
Associations between Hip Fracture Operation Waiting Time and Complications in Asian Geriatric Patients: A Taiwan Medical Center Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
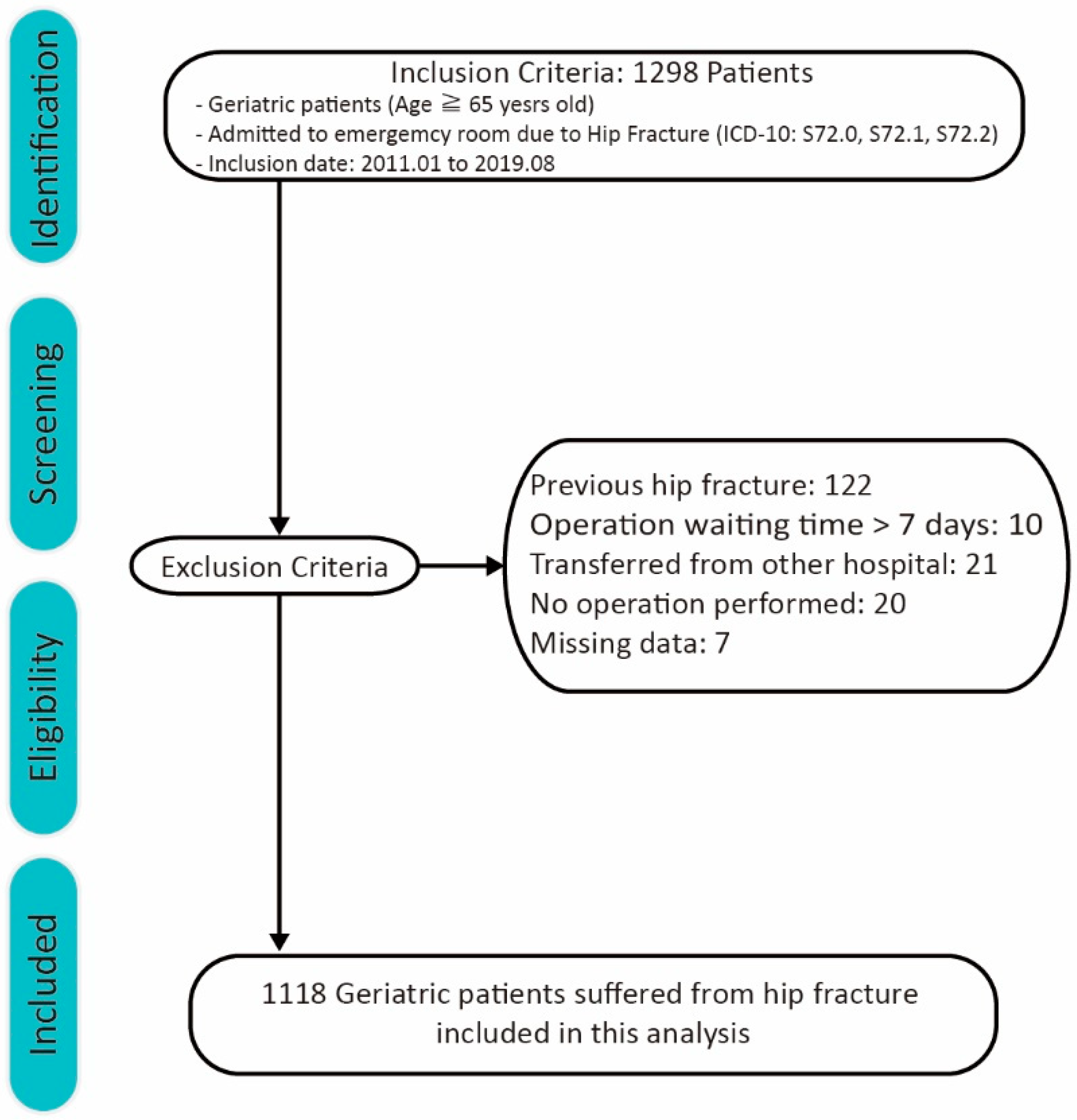
2.1. Patients
2.2. Main Variable
2.3. Covariates
2.4. Statistical Analysis
2.5. Clinical Outcomes
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Chie, W.C.; Yang, R.S.; Liu, J.P.; Tsai, K.S. High incidence rate of hip fracture in Taiwan: Estimated from a nationwide health insurance database. Osteoporos. Int. 2004, 15, 998–1002. [Google Scholar] [CrossRef]
- Hagino, H.; Endo, N.; Harada, A.; Iwamoto, J.; Mashiba, T.; Mori, S.; Ohtori, S.; Sakai, A.; Takada, J.; Yamamoto, T. Survey of hip fractures in Japan: Recent trends in prevalence and treatment. J. Orthop. Sci. 2017, 22, 909–914. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.-L.; Bin Ang, S.; Chadha, M.; Chow, E.S.-L.; Chung, Y.-S.; Hew, F.L.; Jaisamrarn, U.; Ng, H.; Takeuchi, Y.; Wu, C.-H.; et al. An updated hip fracture projection in Asia: The Asian Federation of Osteoporosis Societies study. Osteoporos. Sarcopenia 2018, 4, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-M.; Moon, Y.-W.; Lim, S.-J.; Yoon, B.-K.; Min, Y.-K.; Lee, D.-Y.; Park, Y.-S. Prediction of survival, second fracture, and functional recovery following the first hip fracture surgery in elderly patients. Bone 2012, 50, 1343–1350. [Google Scholar] [CrossRef]
- Dash, S.K.; Panigrahi, R.; Palo, N.; Priyadarshi, A.; Biswal, M. Fragility hip fractures in elderly patients in bhubaneswar, India (2012–2014): A prospective multicenter study of 1031 elderly patients. Geriatr. Orthop. Surg. Rehabil. 2015, 6, 11–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pincus, D.; Ravi, B.; Wasserstein, D.; Huang, A.; Paterson, J.M.; Nathens, A.B.; Kreder, H.J.; Jenkinson, R.J.; Wodchis, W.P. Association between wait Time and 30-Day Mortality in Adults Undergoing Hip Fracture Surgery. JAMA 2017, 318, 1994–2003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasabuchi, Y.; Matsui, H.; Lefor, A.K.; Fushimi, K.; Yasunaga, H. Timing of surgery for hip fractures in the elderly: A retro-spective cohort study. Injury 2018, 49, 1848–1854. [Google Scholar] [CrossRef]
- Wendt, K.; Heim, D.; Josten, C.; Kdolsky, R.; Oestern, H.J.; Palm, H.; Sintenie, J.B.; Komadina, R.; Copuroglu, C. Recommendations on hip fractures. Eur. J. Trauma Emerg. Surg. 2016, 42, 425–431. [Google Scholar] [CrossRef] [Green Version]
- Roberts, K.C.; Brox, W.T.; Jevsevar, D.S.; Sevarino, K. Management of Hip Fractures in the Elderly. J. Am. Acad. Orthop. Surg. 2015, 23, 131–137. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- RStudioTeam. RStudio: Integrated Development for R.; PBC: Boston, MA, USA, 2020. [Google Scholar]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Gauthier, J.; Wu, Q.V.; Gooley, T.A. Cubic splines to model relationships between continuous variables and outcomes: A guide for clinicians. Bone Marrow Transplant. 2019, 55, 675–680. [Google Scholar] [CrossRef] [Green Version]
- IBM Corp. IBM Spss Statistics for Windows, Version 26.0; IBM Corp.: Armonk, NY, USA, 2019. [Google Scholar]
- Ringdal, K.G.; Coats, T.J.; Lefering, R.; Di Bartolomeo, S.; Steen, P.A.; Roise, O.; Handolin, L.; Lossius, H.M.; Utstein TCD Expert Panel. The Utstein template for uniform reporting of data following major trauma: A joint revision by SCANTEM, TARN, DGU-TR and RITG. Scand. J. Trauma Resusc. Emerg. Med. 2008, 16, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brinck, T.; Heinänen, M.; Handolin, L.; Söderlund, T. Trauma-registry survival outcome follow up: 30 days is mandatory and appears sufficient. Injury 2021, 52, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Leizorovicz, A.; Turpie, A.G.; Cohen, A.T.; Wong, L.; Yoo, M.C.; Dans, A.; Group, S.S. Epidemiology of venous thromboem-bolism in Asian patients undergoing major orthopedic surgery without thromboprophylaxis. The smart study. J. Thromb. Haemost. 2005, 3, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Kim, J.S. The 2007 john charnley award. Factors leading to low prevalence of dvt and pulmonary embolism after THA: Analysis of genetic and prothrombotic factors. Clin. Orthop. Relat. Res. 2007, 465, 33–39. [Google Scholar] [CrossRef]
- Ho, C.-A.; Li, C.-Y.; Hsieh, K.-S.; Chen, H.-F. Factors determining the 1-year survival after operated hip fracture: A hospital-based analysis. J. Orthop. Sci. 2010, 15, 30–37. [Google Scholar] [CrossRef]
- Aqil, A.; Hossain, F.; Sheikh, H.; Aderinto, J.; Whitwell, G.; Kapoor, H. Achieving hip fracture surgery within 36 h: An investigation of risk factors to surgical delay and recommendations for practice. J. Orthop. Traumatol. 2015, 17, 207–213. [Google Scholar] [CrossRef] [Green Version]
- Neufeld, M.E.; O’Hara, N.N.; Zhan, M.; Zhai, Y.; Lefaivre, K.A.; Slobogean, G.P.; Broekhuyse, H.M.; Abzug, J.M. Timing of Hip Fracture Surgery and 30-Day Outcomes. Orthopedics 2016, 39, 361–368. [Google Scholar] [CrossRef] [Green Version]
- Cha, Y.-H.; Yoo, J.-I.; Min, Y.-S.; Lee, Y.-K.; Koo, K.-H. Effect of causes of surgical delay on early and late mortality in patients with proximal hip fracture. Arch. Orthop. Trauma Surg. 2017, 137, 625–630. [Google Scholar] [CrossRef]
- Liu, S.K.; Ho, A.W.; Wong, S. Early surgery for Hong Kong Chinese elderly patients with hip fracture reduces short-term and long-term mortality. Hong Kong Med. J. 2017, 23, 374–380. [Google Scholar] [CrossRef]
- Maheshwari, K.; Planchard, J.; You, J.; Sakr, W.A.; George, J.; Higuera-Rueda, C.A.; Saager, L.; Turan, A.; Kurz, A. Early Surgery Confers 1-Year Mortality Benefit in Hip-Fracture Patients. J. Orthop. Trauma 2018, 32, 105–110. [Google Scholar] [CrossRef]
- Mitchell, S.M.; Chung, A.S.; Walker, J.B.; Hustedt, J.W.; Russell, G.V.; Jones, C.B. Delay in Hip Fracture Surgery Prolongs Postoperative Hospital Length of Stay but Does Not Adversely Affect Outcomes at 30 Days. J. Orthop. Trauma 2018, 32, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, M.; Devereaux, P.J.; Swiontkowski, M.F.; Tornetta, P., 3rd; Obremskey, W.; Koval, K.J.; Nork, S.; Sprague, S.; Schemitsch, E.H.; Guyatt, G.H. Internal fixation compared with arthroplasty for displaced fractures of the femoral neck. A meta-analysis. J. Bone Joint Surg. Am. 2003, 85, 1673–1681. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, M.; Swiontkowski, M. Management of Acute Hip Fracture. N. Engl. J. Med. 2017, 377, 2053–2062. [Google Scholar] [CrossRef] [PubMed]
- Daugaard, C.L.; Jorgensen, H.L.; Riis, T.; Lauritzen, J.B.; Duus, B.R.; Van der Mark, S. Is mortality after hip fracture associated with surgical delay or admission during weekends and public holidays? A retrospective study of 38,020 patients. Acta Orthop. 2012, 83, 609–613. [Google Scholar] [CrossRef] [PubMed]
- Kristiansen, N.S.; Kristensen, P.K.; Nørgård, B.M.; Mainz, J.; Johnsen, S.P. Off-hours admission and quality of hip fracture care: A nationwide cohort study of performance measures and 30-day mortality. Int. J. Qual. Health Care 2016, 28, 324–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Early Surgery Group n = 827 | Delay Surgery Group n = 291 | All Patient n = 1118 | p-Value | ||
|---|---|---|---|---|---|
| Operation wait time, mean ± SD | 19.87 ± 6.9 | 55.79 ± 15.44 | 29.22 ± 19.55 | ||
| Basic Characteristics | 0.143 | ||||
| Gender, n (%) | Male | 246 (0.29) | 100 (0.34) | 346 (0.31) | |
| Female | 581 (0.71) | 191 (0.66) | 772 (0.69) | ||
| Age, mean ± SD | 80.69 ± 7.51 | 81.16 ± 7.66 | 80.81 ± 7.55 | 0.519 | |
| Hypertension, n (%) | 301 (36) | 110 (37) | 411 (37) | 0.67 | |
| Diabetes Mellitus, n (%) | 319 (38) | 132 (45) | 451 (40) | <0.05 (0.042) | |
| Hemoglobin, mean ± SD | 11.76 ± 4.4 | 11.33 ± 2.1 | 11.65 ± 3.9 | 0.63 | |
| AST (aspartate aminotransferase), mean ± SD | 28.56 ± 16.6 | 30.13 ± 20.5 | 28.96 ± 17.7 | 0.28 | |
| Estimated GFR a, mean ± SD | 61.51 ± 33.70 | 53.43 ± 27.57 | 59.41 ± 32.40 | 0.94 | |
| INR (international normalized ratio), mean ± SD | 1.11 ± 0.96 | 1.12 ± 0.79 | 1.11 ± 0.92 | 0.76 | |
| Emergency Room Characteristics | |||||
| GCS, mean ± SD | 14.96 ± 0.26 | 14.86 ± 0.89 | <0.05 | ||
| Level of Triage, n (%) | 0.69 | ||||
| Level 1 | 1 (0.1%) | 1 (0.3%) | 2 (0.2%) | ||
| Level 2 | 72 (8.7%) | 30 (10%) | 102 (9%) | ||
| Level 3 | 745 (90%) | 256 (88%) | 1001 (90%) | ||
| Level 4 | 9 (1%) | 4 (1.4%) | 13 (1.2%) | ||
| ISS, mean ± SD | 9.11 ± 1.39 | 9.21 ± 1.02 | 9.14 ± 1.31 | 0.43 | |
| Date of Emergency Room visit, n (%) | <0.05 | ||||
| Weekdays | 650 (78.6%) | 138 (47.4%) | 788 (70.5%) | ||
| Weekends | 177 (21.4%) | 153 (52.6%) | 330 (29.5%) | ||
| Fracture Characteristics | |||||
| Fracture Type, n (%) | 0.428 | ||||
| Femoral neck | 418 (50.5) | 160 (55) | 578 (51.7) | ||
| Intertrochanteric | 378 (45.7) | 121 (41.6) | 499 (44.6) | ||
| Subtrochanteric | 31 (3.7) | 10 (3.4) | 41 (3.7) | ||
| Operation Type, n (%) | 0.157 | ||||
| Internal Fixation | 508 (61) | 165 (57) | 673 (60) | ||
| Arthroplasty | 319 (39) | 126 (43) | 445 (40) | ||
| Timing of Operation, n (%) | 0.521 | ||||
| Working hours | 774 (93.6) | 274 (94.2) | |||
| Evening | 44 (5.3) | 12 (4.1) | |||
| Overnight | 9 (1.1) | 5 (1.7) |
| Early Surgery Group n = 827 | Delay Surgery Group n = 291 | p-Value | Multivariate Analysis * | ||
|---|---|---|---|---|---|
| Pneumonia | |||||
| 30 days | 36 (4.4%) | 23 (7.9%) | <0.05 | <0.05 | |
| 90 days | 51 (6.2%) | 31 (10.7%) | <0.05 | <0.05 | |
| 365 days | 106 (12.8%) | 50 (17.2%) | 0.07 | 0.13 | |
| Acute Myocardial Infarction | |||||
| 30 days | 25 (3%) | 21 (7.2%) | <0.05 | <0.05 | |
| 90 days | 47 (5.7%) | 27 (9.3%) | <0.05 | <0.05 | |
| 365 days | 72 (8.7%) | 35 (12%) | 0.10 | 0.11 | |
| Heart Failure | |||||
| 30 days | 126 (15.2%) | 78 (26.8%) | <0.05 | <0.05 | |
| 90 days | 134 (16.2%) | 83 (28.5%) | <0.05 | <0.05 | |
| 365 days | 162 (19.6%) | 95 (32.6%) | <0.05 | <0.05 | |
| Deep Vein Thrombosis | |||||
| 30 days | 8 (1%) | 6 (2.1%) | 0.22 | 0.14 | |
| 90 days | 9 (1.1%) | 7 (2.4%) | 0.15 | 0.09 | |
| 365 days | 14 (1.7%) | 10 (3.4%) | 0.09 | 0.07 | |
| Pulmonary Embolism | |||||
| 30 days | 3 (0.4%) | 0 (0%) | 0.57 | 0.31 | |
| 90 days | 4 (0.5%) | 0 (0%) | 0.58 | 0.24 | |
| 365 days | 5 (0.6%) | 0 (0%) | 0.18 | 0.19 | |
| Mortality (30 days) | 3 (0.4%) | 3 (1%) | 0.19 | ||
| Length of Stay | 7.4 (3.6) | 9.6 (6.1) | <0.05 | ||
| Operation time | 115.4 (37.1) | 104.9 (40.0) | 0.40 | ||
| Operation blood loss | 211.3 (227.5) | 177.8 (148.3) | 0.26 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, C.-Y.; Hsiao, C.-H.; Tsai, W.; Chang, W.-H.; Chen, T.-H. Associations between Hip Fracture Operation Waiting Time and Complications in Asian Geriatric Patients: A Taiwan Medical Center Study. Int. J. Environ. Res. Public Health 2021, 18, 2848. https://doi.org/10.3390/ijerph18062848
Shen C-Y, Hsiao C-H, Tsai W, Chang W-H, Chen T-H. Associations between Hip Fracture Operation Waiting Time and Complications in Asian Geriatric Patients: A Taiwan Medical Center Study. International Journal of Environmental Research and Public Health. 2021; 18(6):2848. https://doi.org/10.3390/ijerph18062848
Chicago/Turabian StyleShen, Ching-Yi, Chien-Han Hsiao, Weide Tsai, Wen-Han Chang, and Tse-Hao Chen. 2021. "Associations between Hip Fracture Operation Waiting Time and Complications in Asian Geriatric Patients: A Taiwan Medical Center Study" International Journal of Environmental Research and Public Health 18, no. 6: 2848. https://doi.org/10.3390/ijerph18062848
APA StyleShen, C. -Y., Hsiao, C. -H., Tsai, W., Chang, W. -H., & Chen, T. -H. (2021). Associations between Hip Fracture Operation Waiting Time and Complications in Asian Geriatric Patients: A Taiwan Medical Center Study. International Journal of Environmental Research and Public Health, 18(6), 2848. https://doi.org/10.3390/ijerph18062848