
A Decision Tree Model for Breast Reconstruction of Women with Breast Cancer: A Mixed Method Approach


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Background
1.2. Ethnographic Decision Tree Model
2. Materials and Methods
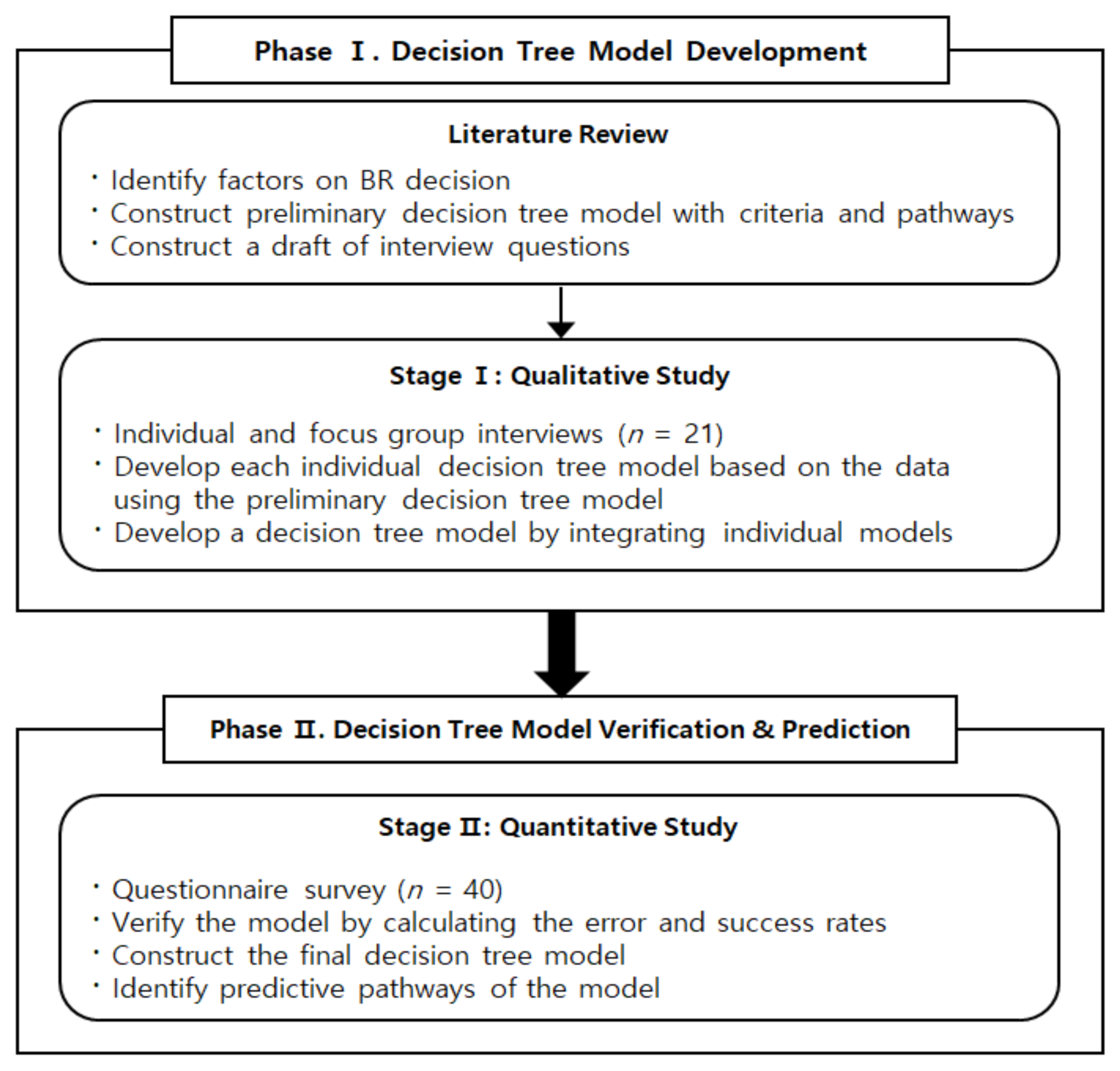
2.1. Design and Process
2.2. Participants
2.3. Data Collection
2.4. Data Analysis
- (1)
- Identify decision-making issues to explore
- (2)
- Specify a set of decision choices
- (3)
- Master ethnographic interview skills: Researchers with experience in qualitative research were asked to participate in data collection and analysis.
- (4)
- Participation observations should be included where possible, including data that manifest themselves as actions.
- (5)
- WBC who underwent decision-making process for BR was selected to ensure the representativeness of the data. Sample numbers were collected until the data was saturated.
- (6)
- Decision-making criteria were derived through inviting participants to recall and explain specific examples of decision-making. If an active objection was identified and confirmed, this was used as criteria.
- (7)
- A decision-making tree was then developed by drawing flows and relationships between the derived criteria. To establish a clear statement stage with each individual decision-making tree and ensure each decision-making tree was appropriate, the researcher used the language and categories utilized by the participants. In developing individual models, group models were constructed by evaluating and modifying them in the following qualitative interviews.
- (8)
- In the final stage, individual trees were combined to form a collective decision model that was revised several times in hierarchical order to ensure it is logical and predictable. The reason for establishing a decision-making tree was placed prior to the obstacle that hindered this choice or behaviour.
2.5. Ethical Considerations
2.6. Rigor
3. Results
3.1. Development of a Decision Tree Model
3.2. Verification and Prediction of the Decision Tree Model
- Predictive pathways to decide to have BR
I had lived without breast about two years. But, you know, I completely lost my self-esteem. I was so depressed that I even thought about suicide. Finally, it came to my mind that I will live as a woman with confidence even if I can live only one day!(Participant 15)
Without breast, I feel like she is not a woman. So I thought that others would think that I am not a woman when they saw me. Honestly, men touch women’s breast. As a wife, I wanted to be a woman to my husband. It seemed to be my pride…(Participant 12)
One day, about two years have passed after mastectomy, I looked at my body and I suddenly realized that I needed to have BR. So, I talked about it in front of my family. And my husband said, “You can have it any time you want! You could have done it from the beginning, but you didn’t do it!” And my daughter said, “Mom, you do it! You know it’s great”. Anyway, I couldn’t decide at that time. But, later on, I just choose to do it as I was being pushed away by my family.(Participant 14)
When I was in hospital for cancer treatment, other patient recommended breast reconstruction… very strongly. “I’m so happy and satisfied with the surgery!” She didn’t say that surgery was difficult at all… she only talked about the good points(Participant 13)
My family thought that my body would be twisted without a breast. “If you don’t have surgery, your body will bend. Are you okay?” My daughter persuaded me to do breast reconstruction by saying so.(Participant 17)
- Predictive pathways to decide against to have BR
Another friend [who had breast reconstruction] told me that she finished her cancer treatment and when she had to decide to have surgery [BR] again, it was very hard in terms of time, effort, and cost she put. And, she said she wouldn’t do it again anymore. When I heard about that, I also didn’t want to have that kind of surgery because I thought ‘what should I do if I would have the same feeling and results like her?’(Participant 18)
The insurance didn’t cover it at that time, and moreover I had to pay VAT on the surgery fees. It was so unfair that I was sick and cost a lot of money. I’m sorry to have had a mastectomy… Should I undergo breast reconstruction while paying the VAT of the surgery… That’s too sad and I am very angry.(Participant 14)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 1–41. [Google Scholar] [CrossRef]
- Korean Breast Cancer Society. 2020 Breast Cancer Facts and Figures. Available online: http://www.kbcs.or.kr/journal/file/210107.pdf (accessed on 20 February 2021).
- Health Insurance Review & Assessment Service. Health Care Big Data Open System. National Interest Medical Practices (Examination and Procedure) Statistics. Available online: http://opendata.hira.or.kr/op/opc/olapMfrnIntrsDiagBhvInfo.do (accessed on 30 June 2020).
- Kummerow, K.L.; Du, L.; Penson, D.F.; Shyr, Y.; Hooks, M.A. Nationwide trends in mastectomy for early-stage breast cancer. JAMA Surg. 2015, 150, 9–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.; Sunu, C.; Pignone, M. Patient-reported outcomes of breast reconstruction after mastectomy: A systematic review. J. Am. Coll. Surg. 2009, 209, 123–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baek, S.H.; Bae, S.J.; Yoon, C.I.; Park, S.E.; Cha, C.H.; Ahn, S.G.; Kim, Y.S.; Roh, T.S.; Jeong, J. Immediate breast reconstruction does not have a clinically significant impact on adjuvant treatment delay and subsequent survival outcomes. J. Breast Cancer 2019, 22, 109–119. [Google Scholar] [CrossRef]
- Jabo, B.; Lin, A.C.; Aljehani, M.A.; Ji, L.; Morgan, J.W.; Selleck, M.J.; Kim, H.Y.; Lum, S.S. Impact of breast reconstruction on time to definitive surgical treatment, adjuvant therapy, and breast cancer outcomes. Ann. Surg. Oncol. 2018, 25, 3096–3105. [Google Scholar] [CrossRef]
- Nam, S.; Park, S.; Lee, D.W.; Song, S.Y.; Park, H.S.; Kim, S.I.; Park, B.W.; Lew, D.H. Clinical outcome of immediate breast reconstruction after mastectomy for breast cancer. J. Breast Dis. 2014, 2, 44–50. [Google Scholar] [CrossRef]
- Ceradini, D.J.; Levine, J.P. Breast cancer reconstruction: More than skin deep. Prim. Psychiatry 2008, 15, 72–80. [Google Scholar]
- Fernández-Delgado, J.; López-Pedraza, M.J.; Blasco, J.A.; Andradas-Aragones, E.; Sánchez-Méndez, J.I.; Sordo-Miralles, G.; Reza, M.M. Satisfaction with and psychological impact of immediate and deferred breast reconstruction. Ann. Oncol. 2008, 19, 1430–1434. [Google Scholar] [CrossRef]
- Kang, H.J.; Kim, S.W.; Noh, D.Y.; Youn, Y.K.; Oh, S.K.; Choe, K.J.; Han, S.B.; Minn, K.W. Immediate breast reconstruction after a mastectomy for breast cancer. J. Korean Surg. Soc. 2000, 59, 584–589. [Google Scholar]
- Sheehan, J.; Sheman, K.A.; Lam, T.; Boyages, J. Association of information satisfaction, psychological distress and monitoring coping style with post-decision regret following breast reconstruction. Psycho-Oncology 2007, 16, 342–351. [Google Scholar] [CrossRef]
- Nissen, M.J.; Swenson, K.K.; Kind, E.A. Quality of life after postmastectomy breast reconstruction. Oncol. Nurs. Forum 2002, 29, 547–553. [Google Scholar] [CrossRef]
- Harcourt, D.; Rumsey, N. Mastectomy patients’ decision-making for or against immediate breast reconstruction. Psycho-Oncology 2004, 13, 106–114. [Google Scholar] [CrossRef]
- Rowland, J.H.; Desmond, K.A.; Meyerowitz, B.E.; Belin, T.R.; Wyatt, G.E.; Ganz, P.A. Role of breast reconstructive surgery in physical and emotional outcomes among breast cancer survivors. J. Natl. Cancer Inst. 2000, 92, 1422–1429. [Google Scholar] [CrossRef] [Green Version]
- Paraskeva, N.; Guest, E.; Lewis-Smith, H.; Harcourt, D. Assessing the effectiveness of interventions to support patient decision making about breast reconstruction: A systematic review. Breast 2018, 40, 97–105. [Google Scholar] [CrossRef]
- Lee, C.N.; Hultman, C.S.; Sepucha, K. What are patients’ goals and concerns about breast reconstruction after mastectomy? Ann. Plastic Surg. 2010, 64, 567–569. [Google Scholar] [CrossRef]
- Wolf, L. The information needs of women who have undergone breast reconstruction. Part I: Decision-making and sources of information. Eur. J. Oncol. Nurs. 2004, 8, 211–223. [Google Scholar] [CrossRef]
- Wolf, L. The information needs of women who have undergone breast reconstruction. Part II: Information giving and content of information. Eur. J. Oncol. Nurs. 2004, 8, 315–324. [Google Scholar] [CrossRef]
- Chung, I.Y.; Kang, E.; Yang, E.J.; Lim, J.Y.; Kim, E.K.; Kim, H.A.; Noh, W.C.; Kim, J.I.; Park, M.H.; Yoon, J.H.; et al. Survey of psychosocial problems facing breast cancer survivors after undergoing a mastectomy and their awareness of breast reconstruction. J. Breast Cancer 2011, 14, S70–S76. [Google Scholar] [CrossRef]
- Yi, M.; Joung, W.J.; Park, E.Y.; Kwon, E.J.; Kim, H.; Seo, J.Y. Decision making experience on breast reconstruction for women with breast cancer. J. Korean Acad. Nurs. 2016, 46, 894–904. [Google Scholar] [CrossRef] [Green Version]
- Somogyi, R.B.; Webb, A.; Baghdikian, N.; Stephenson, J.; Edward, K.L.; Morrison, W. Understanding the factors that influence breast reconstruction decision making in Australian women. Breast 2015, 24, 124–130. [Google Scholar] [CrossRef] [Green Version]
- Rose, F.; Michelle, M.C.; Margaret, C.; Christine, H.R. A qualitative study of breast reconstruction decision-making among Asian immigrant women living in the United States. Plastic Reconstr. Surg. 2017, 139, 360e–368e. [Google Scholar]
- Ng, S.K.; Hare, R.M.; Kuang, R.J.; Smith, K.M.; Brown, B.J.; Hunter-Smith, D.J. Breast reconstruction post mastectomy: Patient satisfaction and decision making. Ann. Plastic Surg. 2016, 76, 640–644. [Google Scholar] [CrossRef]
- Morrow, M.; Li, Y.; Alderman, A.K.; Jagsi, R.; Hamilton, A.S.; Graff, J.J.; Hawley, S.T.; Katz, S.J. Access to breast reconstruction after mastectomy and patient perspectives on reconstruction decision making. JAMA Surg. 2014, 149, 1015–1021. [Google Scholar] [CrossRef] [Green Version]
- Gladwin, C.H. Ethnographic Decision Tree Modeling; Sage Publication: Thousand Oaks, CA, USA, 1989. [Google Scholar]
- Beck, K.A. Ethnographic decision tree modeling: A research method for counseling psychology. J. Couns. Psychol. 2005, 52, 243–249. [Google Scholar] [CrossRef]
- Patton, M.Q. Qualitative Research Methods; Sage Publication: Thousand Oaks, CA, USA, 1990. [Google Scholar]
- Guba, E.G.; Lincoln, Y.S. Effective Evaluation: Improving the Usefulness of Evaluation Results through Responsive and Naturalistic Approaches; Jossey-Bas: San Francisco, CA, USA, 1981. [Google Scholar]
- Manne, S.L.; Topham, N.; Kirstein, L.; Virtue, S.M.; Brill, K.; Devine, K.A.; Gajda, T.; Frederick, S.; Darabos, K.; Sorice, K. Attitudes and decisional conflict regarding breast reconstruction among breast cancer patients. Cancer Nurs. 2016, 39, 427–436. [Google Scholar] [CrossRef] [Green Version]
- Rubin, L.R. Does that make me a woman? Breast cancer, mastectomy, and breast reconstruction decisions among sexual minority women. Psychol. Women Q. 2011, 35, 401–414. [Google Scholar] [CrossRef] [Green Version]
- Fang, S.Y.; Balneaves, L.G.; Shu, B.C. A struggle between vanity and life: The experience of receiving breast reconstruction in women of Taiwan. Cancer Nurs. 2010, 33, E1–E11. [Google Scholar] [CrossRef]
- Wu, S.M.; Chao-Yu, Y.M.; Yang, C.F.; Che, H.L. Decision-making tree for women considering hysterectomy. J. Adv. Nurs. 2005, 51, 361–368. [Google Scholar] [CrossRef]
- Shin, D.W.; Sunwoo, S.; Lee, J. Management of cancer survivors in Korea. J. Korean Med. Assoc. 2015, 58, 216–226. [Google Scholar] [CrossRef]
- Fasse, L.; Flahault, C.; Vioulac, C.; Lamore, K.; Van Wersch, A.; Quintard, B.; Untas, A. The decision-making process for breast reconstruction after cancer surgery: Representations of heterosexual couples in long-standing relationships. Br. J. Health Psychol. 2017, 22, 254–269. [Google Scholar] [CrossRef]
- Oh, H.S.; Park, H.A. Decision tree model of the treatment-seeking behaviors among Korean cancer patients. Cancer Nurs. 2004, 27, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Coburn, N.; Fulton, J.; Pearlman, D.N.; Law, C.; DiPaolo, B.; Cady, B. Treatment variation by insurance status for breast cancer patients. Breast J. 2008, 14, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.N.H.; Deal, A.M.; Huh, R.; Ubel, P.A.; Liu, Y.J.; Blizard, L.; Hunt, C.; Pignone, M.P. Quality of patient decisions about breast reconstruction after mastectomy. JAMA Surg. 2017, 152, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Rosson, G.D.; Singh, N.K.; Ahuja, N.; Jacobs, L.K.; Chang, D.C. Multilevel analysis of the impact of community vs patient factors on access to immediate breast reconstruction following mastectomy in Maryland. Arch. Surg. 2008, 143, 1076–1081. [Google Scholar] [CrossRef] [Green Version]
- Yi, M.; Park, E.Y.; Kim, D.S.; Tae, Y.S.; Chung, B.Y.; So, H.S. Psychosocial adjustment of low-income Koreans with cancer. J. Korean Acad. Nurs. 2011, 41, 225–235. [Google Scholar] [CrossRef] [Green Version]
- Alderman, A.K.; Hawley, S.T.; Waljee, J.; Mujahid, M.; Morrow, M.; Katz, S.J. Understanding the impact of breast reconstruction on the surgical decision-making process for breast cancer. Cancer 2008, 112, 489–494. [Google Scholar] [CrossRef] [Green Version]
- Kadmon, I.; Noy, S.; Billig, A.; Tzur, T. Decision-making styles and levels of involvement concerning breast reconstructive surgery: An Israeli study. Oncol. Nurs. Forum 2016, 43, E1–E7. [Google Scholar] [CrossRef]
- Jeong, Y.S. An efficiency management scheme using big data of healthcare patients using puzzy AHP. J. Digit. Converg. 2015, 13, 227–233. [Google Scholar] [CrossRef]
- Kim, M.Y.; Shin, H.S. Dental hospital selection factors using triangle fuzzy numbers with a focus on supplier factors. J. Korean Acad. Oral Health 2015, 39, 110–118. [Google Scholar] [CrossRef] [Green Version]
- Salabun, W.; Piegat, A. Comparative analysis of MCDM methods for the assessment of mortality in patients with acute coronary syndrome. Artif. Intell. Rev. 2017, 48, 557–571. [Google Scholar] [CrossRef]
- Piegat, A.; Sałabun, W. Comparative analysis of MCDM methods for assessing the severity of chronic liver disease. In Artificial Intelligence and Soft Computing; ICAISC Lecture Notes in Computer Science; Rutkowski, L., Korytkowski, M., Scherer, R., Tadeusiewicz, R., Zadeh, L., Zurada, J., Eds.; Springer: Cham, Switzerland, 2015; Volume 9119. [Google Scholar] [CrossRef]
- Triandis, H. Collectivism v. individualism: A reconceptualisation of a basic concept in cross-cultural social psychology. In Cross-Cultural Studies of Personality, Attitudes and Cognition; Verma, G.K., Bagley, C., Eds.; Palgrave Macmillan: London, UK, 1988; pp. 60–95. [Google Scholar]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, E.Y.; Yi, M.; Kim, H.S.; Kim, H. A Decision Tree Model for Breast Reconstruction of Women with Breast Cancer: A Mixed Method Approach. Int. J. Environ. Res. Public Health 2021, 18, 3579. https://doi.org/10.3390/ijerph18073579
Park EY, Yi M, Kim HS, Kim H. A Decision Tree Model for Breast Reconstruction of Women with Breast Cancer: A Mixed Method Approach. International Journal of Environmental Research and Public Health. 2021; 18(7):3579. https://doi.org/10.3390/ijerph18073579
Chicago/Turabian StylePark, Eun Young, Myungsun Yi, Hye Sook Kim, and Haejin Kim. 2021. "A Decision Tree Model for Breast Reconstruction of Women with Breast Cancer: A Mixed Method Approach" International Journal of Environmental Research and Public Health 18, no. 7: 3579. https://doi.org/10.3390/ijerph18073579
APA StylePark, E. Y., Yi, M., Kim, H. S., & Kim, H. (2021). A Decision Tree Model for Breast Reconstruction of Women with Breast Cancer: A Mixed Method Approach. International Journal of Environmental Research and Public Health, 18(7), 3579. https://doi.org/10.3390/ijerph18073579