
Effects of Low-Volume High-Intensity Interval Exercise on 24 h Movement Behaviors in Inactive Female University Students



Abstract
:1. Introduction
2. Materials and Methods
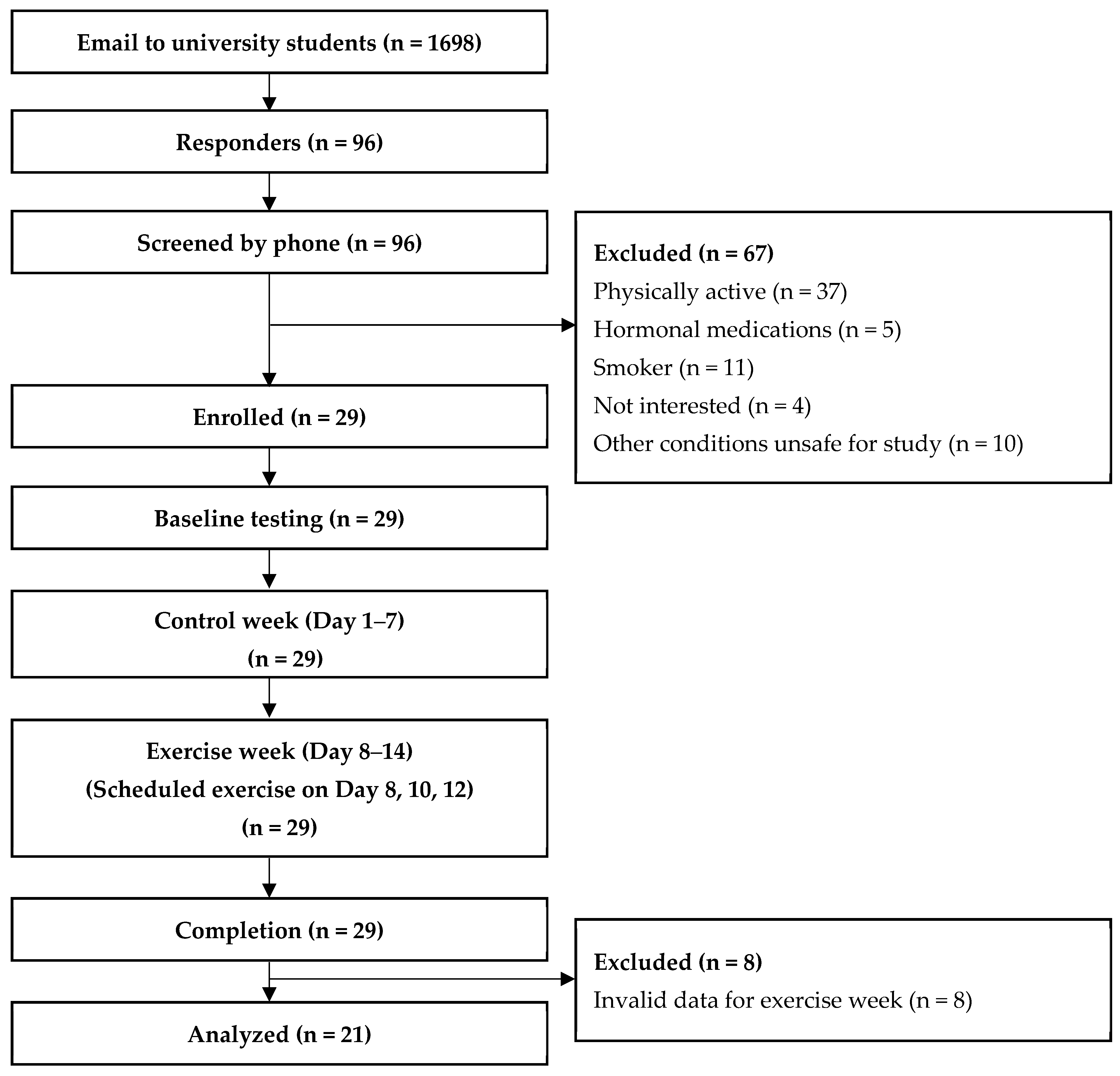
2.1. Participants
2.2. Procedures
2.3. Measurement
- Anthropometry
- Aerobic capacity
- Movement behaviors
- Exercise exertion
- Exercise protocol
2.4. Statistical Analysis
3. Results
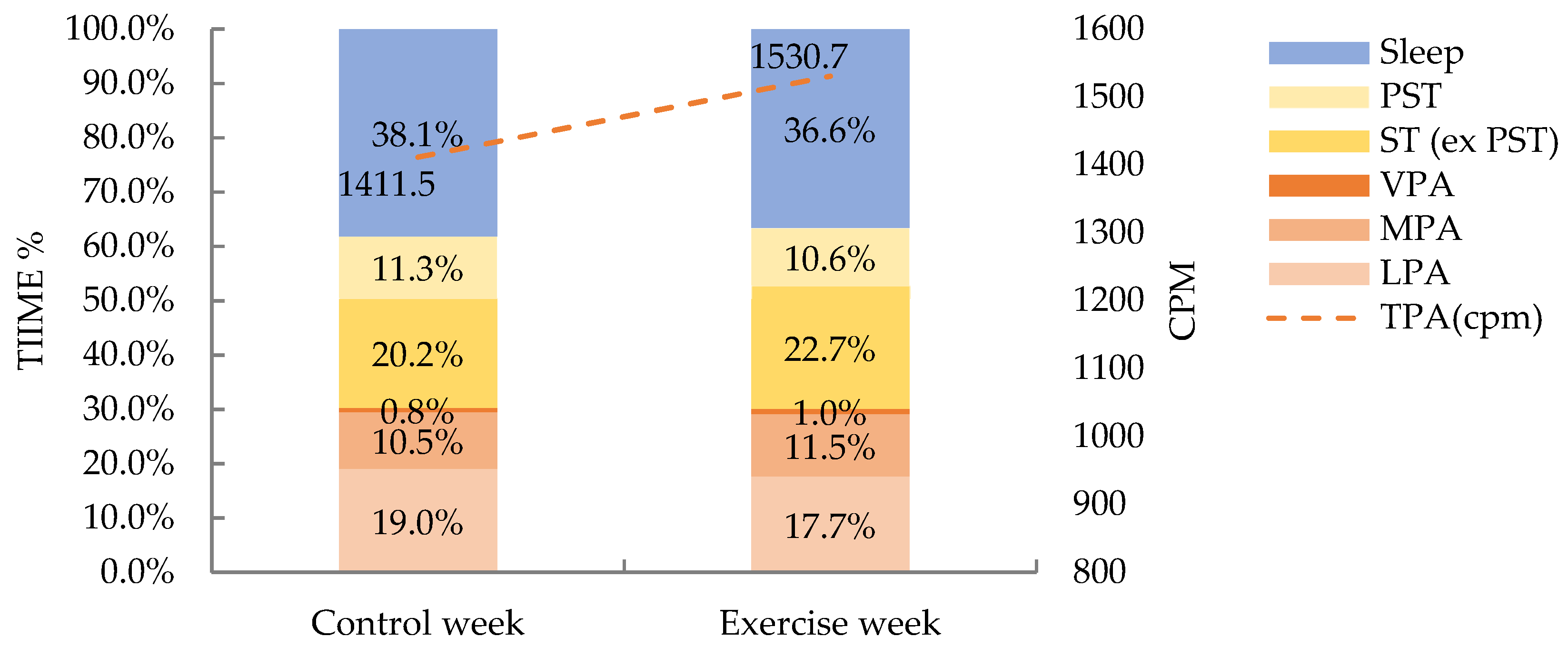
- Weekly basis analysis
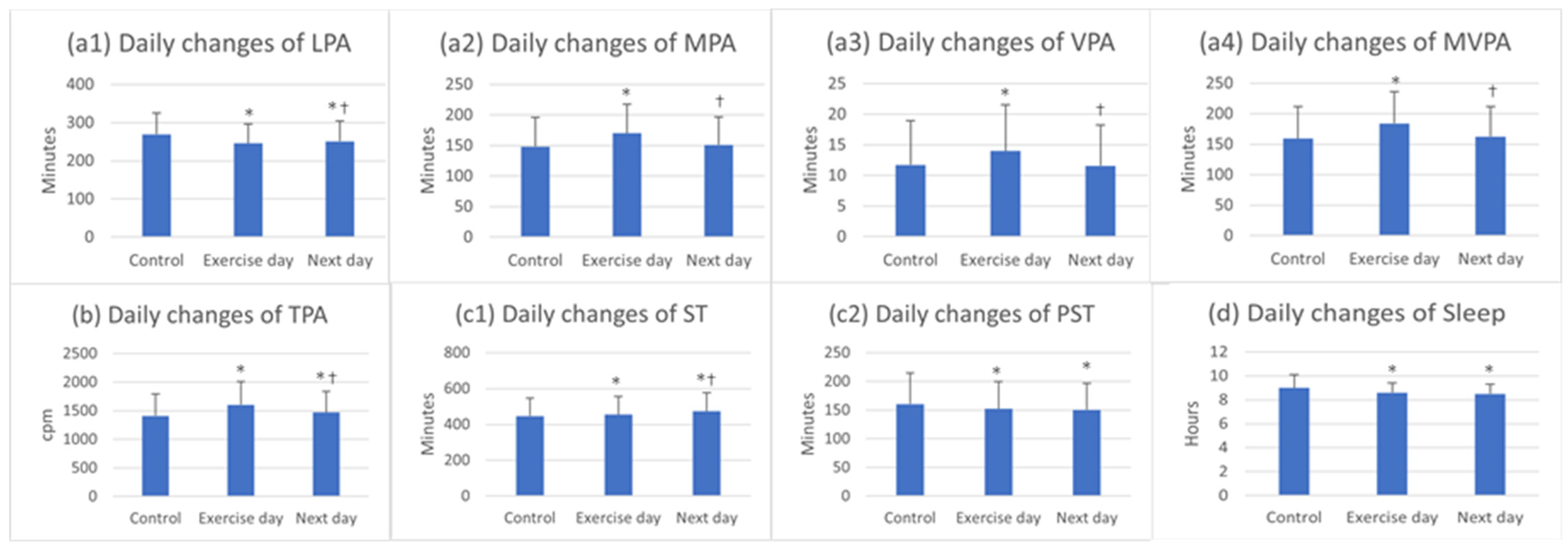
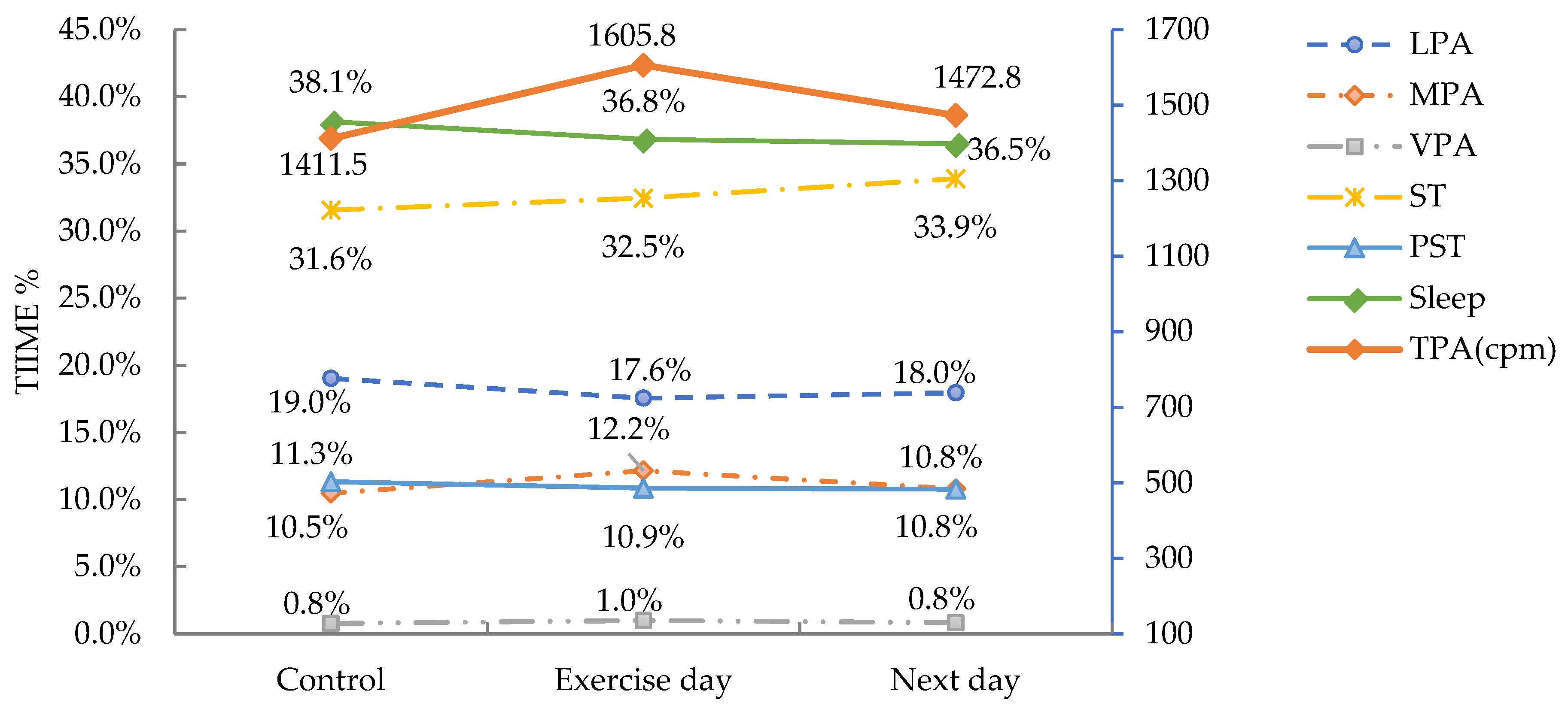
- Daily basis analysis
- Exercise fidelity and exertion
- Linear regression modeling
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | ||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | LPA | – | ||||||||
| 2 | MPA | 0.666 ** | – | |||||||
| 3 | VPA | 0.498 * | 0.579 ** | – | ||||||
| 4 | MVPA | 0.677 ** | 0.994 * | 0.668 ** | – | |||||
| 5 | TPA | 0.430 | 0.911 ** | 0.537 * | 0.907 ** | – | ||||
| 6 | ST | −0.567 ** | −0.818 ** | −0.258 | −0.782 ** | −0.748 ** | – | |||
| 7 | PST | −0.060 | −0.251 | −0.077 | −0.24 | −0.365 | 0.398 | – | ||
| 8 | Sleep | −0.443 * | −0.117 | −0.493 * | −0.175 | 0.003 | −0.382 | −0.325 | −0.270 | – |
References
- Alessa, H.B.; Chomistek, A.K.; Hankinson, S.E.; Barnett, J.B.; Rood, J.; Matthews, C.E.; Rimm, E.B.; Willett, W.C.; Hu, F.B.; Tobias, D.K. Objective measures of physical activity and cardiometabolic and endocrine biomarkers. Med. Sci. Sports Exerc. 2017, 49, 1817–1825. [Google Scholar] [CrossRef] [PubMed]
- Balducci, S.; Haxhi, J.; Sacchetti, M.; Orlando, G.; Cardelli, P.; Vitale, M.; Mattia, L.; Carla, I.; Bollanti, L.; Conti, F.; et al. Relationships of changes in physical activity and sedentary behavior with changes in physical fitness and cardiometabolic risk profile in individuals with type 2 diabetes: The italian diabetes and exercise study 2 (IDES_2). Diabetes Care 2022, 45, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, R.B.; Dos Santos Amorim, P.R.; Marins, J.C.B.; de LX Martins, Y.; de Souza Magalhães Marques, S.; Aguiar, V.P.R.; Palotás, A.; Lima, L.M. Physical inactivity is liable to the increased cardiovascular risk and impaired cognitive profile. Curr. Alzheimer Res. 2020, 17, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, C.; O’ Sullivan, R.; Caserotti, P.; Tully, M.A. Consequences of physical inactivity in older adults: A systematic review of reviews and meta-analyses. Scand. J. Med. Sci. Sports 2020, 30, 816–827. [Google Scholar] [CrossRef] [PubMed]
- Whitlock, G.; Lewington, S.; Sherliker, P.; Clarke, R.; Emberson, J.; Halsey, J.; Qizilbash, N.; Collins, R.; Peto, R. Body-mass index and cause-specific mortality in 900 000 adults: Collaborative analyses of 57 prospective studies. Lancet 2009, 373, 1083–1096. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- Vella-Zarb, R.A.; Elgar, F.J. The ‘freshman 5’: A meta-analysis of weight gain in the freshman year of college. J. Am. Coll. Health 2009, 58, 161–166. [Google Scholar] [CrossRef]
- Kwan, M.Y.; Cairney, J.; Faulkner, G.E.; Pullenayegum, E.E. Physical activity and other health-risk behaviors during the transition into early adulthood: A longitudinal cohort study. Am. J. Prev. Med. 2012, 42, 14–20. [Google Scholar] [CrossRef]
- Kljajević, V.; Stanković, M.; Đorđević, D.; Trkulja-Petković, D.; Jovanović, R.; Plazibat, K.; Oršolić, M.; Čurić, M.; Sporiš, G. Physical activity and physical fitness among university students—A systematic review. Int. J. Environ. Res. Public Health 2021, 19, 158. [Google Scholar] [CrossRef]
- Grasdalsmoen, M.; Eriksen, H.R.; Lønning, K.J.; Sivertsen, B. Physical exercise and body-mass index in young adults: A national survey of Norwegian university students. BMC Public Health 2019, 19, 1354. [Google Scholar] [CrossRef]
- Cotten, E.; Prapavessis, H. Increasing nonsedentary behaviors in university students using text messages: Randomized controlled trial. JMIR mHealth uHealth 2016, 4, e99. [Google Scholar] [CrossRef] [PubMed]
- Carballo-Fazanes, A.; Rico-Díaz, J.; Barcala-Furelos, R.; Rey, E.; Rodríguez-Fernández, J.E.; Varela-Casal, C.; Abelairas-Gómez, C. Physical activity habits and determinants, sedentary behaviour and lifestyle in university students. Int. J. Environ. Res. Public Health 2020, 17, 3272. [Google Scholar] [CrossRef] [PubMed]
- Dias, K.A.; Ingul, C.B.; Tjønna, A.E.; Keating, S.E.; Gomersall, S.R.; Follestad, T.; Hosseini, M.S.; Hollekim-Strand, S.M.; Ro, T.B.; Haram, M.; et al. Effect of high-intensity interval training on fitness, fat mass and cardiometabolic biomarkers in children with obesity: A randomised controlled trial. Sports Med. 2018, 48, 733–746. [Google Scholar] [CrossRef] [PubMed]
- Sultana, R.N.; Sabag, A.; Keating, S.E.; Johnson, N.A. The effect of low-volume high-intensity interval training on body composition and cardiorespiratory fitness: A systematic review and meta-analysis. Sports Med. 2019, 49, 1687–1721. [Google Scholar] [CrossRef] [PubMed]
- Batacan, R.B., Jr.; Duncan, M.J.; Dalbo, V.J.; Tucker, P.S.; Fenning, A.S. Effects of high-intensity interval training on cardiometabolic health: A systematic review and meta-analysis of intervention studies. Br. J. Sports Med. 2017, 51, 494–503. [Google Scholar] [CrossRef]
- Jelleyman, C.; Yates, T.; O’Donovan, G.; Gray, L.J.; King, J.A.; Khunti, K.; Davies, M.J. The effects of high-intensity interval training on glucose regulation and insulin resistance: A meta-analysis. Obes. Rev. 2015, 16, 942–961. [Google Scholar] [CrossRef]
- Kessler, H.S.; Sisson, S.B.; Short, K.R. The potential for high-intensity interval training to reduce cardiometabolic disease risk. Sports Med. Auckl. 2012, 42, 489–509. [Google Scholar] [CrossRef]
- Rowland, T.W. The biological basis of physical activity. Med. Sci. Sports Exerc. 1998, 30, 392–399. [Google Scholar] [CrossRef]
- King, N.A.; Caudwell, P.; Hopkins, M.; Byrne, N.M.; Colley, R.; Hills, A.P.; Stubbs, J.R.; Blundell, J.E. Metabolic and behavioral compensatory responses to exercise interventions: Barriers to weight loss. Obesity 2007, 15, 1373–1383. [Google Scholar] [CrossRef]
- Rangan, V.V.; Willis, L.H.; Slentz, C.A.; Bateman, L.A.; Shields, A.T.; Houmard, J.A.; Kraus, W.E. Effects of an 8-month exercise training program on off-exercise physical activity. Med. Sci. Sports Exerc. 2011, 43, 1744–1751. [Google Scholar] [CrossRef]
- Cooper, A.R.; Page, A.S.; Foster, L.J.; Qahwaji, D. Commuting to school: Are children who walk more physically active? Am. J. Prev. Med. 2003, 25, 273–276. [Google Scholar] [CrossRef]
- Goodman, A.; Mackett, R.L.; Paskins, J. Activity compensation and activity synergy in British 8–13 year olds. Prev. Med. 2011, 53, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Long, M.W.; Sobol, A.M.; Cradock, A.L.; Subramanian, S.V.; Blendon, R.J.; Gortmaker, S.L. School-day and overall physical activity among youth. Am. J. Prev. Med. 2013, 45, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Maillard, F.; Pereira, B.; Boisseau, N. Effect of high-intensity interval training on total, abdominal and visceral fat mass: A meta-analysis. Sports Med. 2018, 48, 269–288. [Google Scholar] [CrossRef] [PubMed]
- Astorino, T.A.; Allen, R.P.; Roberson, D.W.; Jurancich, M. Effect of high-intensity interval training on cardiovascular function, VO2max, and muscular force. J. Strength Cond. Res. 2012, 26, 138–145. [Google Scholar] [CrossRef]
- De Revere, J.L.; Clausen, R.D.; Astorino, T.A. Changes in VO2max and cardiac output in response to short-term high-intensity interval training in Caucasian and Hispanic young women: A pilot study. PLoS ONE 2021, 16, e0244850. [Google Scholar] [CrossRef]
- Gibala, M.J. Interval training for cardiometabolic health: Why such a HIIT? Curr. Sports Med. Rep. 2018, 17, 148–150. [Google Scholar] [CrossRef]
- Skovgaard, E.L.; Obling, K.; Maindal, H.T.; Rasmussen, C.; Overgaard, K. Unprompted vigorous physical activity is associated with higher levels of subsequent sedentary behaviour in participants with low cardiorespiratory fitness: A cross-sectional study. Eur. J. Sport Sci. 2019, 19, 1004–1013. [Google Scholar] [CrossRef]
- Paravidino, V.B.; Mediano, M.F.F.; Sichieri, R. Does a single bout of exercise influence subsequent physical activity and sedentary time in overweight boys? Physiol. Behav. 2017, 173, 231–235. [Google Scholar] [CrossRef]
- Nugent, S.F.; Jung, M.E.; Bourne, J.E.; Loeppky, J.; Arnold, A.; Little, J.P. The influence of high-intensity interval training and moderate-intensity continuous training on sedentary time in overweight and obese adults. Appl. Physiol. Nutr. Metab. 2018, 43, 747–750. [Google Scholar] [CrossRef]
- Sjöros, T.; Vähä-Ypyä, H.; Laine, S.; Garthwaite, T.; Lahesmaa, M.; Laurila, S.M.; Latva-Rasku, A.; Savolainen, A.; Miikkulainen, A.; Löyttyniemi, E.; et al. Both sedentary time and physical activity are associated with cardiometabolic health in overweight adults in a 1 month accelerometer measurement. Sci. Rep. 2020, 10, 20578. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Tian, X.Y.; Sun, F.H.; Huang, W.Y.; Sheridan, S.; Wu, Y.; Wong, S.H.S. Associations of Sedentary patterns with cardiometabolic biomarkers in physically active young males. Med. Sci. Sports Exerc. 2021, 53, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Itani, O.; Jike, M.; Watanabe, N.; Kaneita, Y. Short sleep duration and health outcomes: A systematic review, meta-analysis, and meta-regression. Sleep Med. 2017, 32, 246–256. [Google Scholar] [CrossRef] [PubMed]
- Peltzer, K.; Pengpid, S. Sleep duration and health correlates among university students in 26 countries. Psychol. Health Med. 2016, 21, 208–220. [Google Scholar] [CrossRef] [PubMed]
- Zhu, G.; Cassidy, S.; Hiden, H.; Woodman, S.; Trenell, M.; Gunn, D.A.; Catt, M.; Birch-Machin, M.; Anderson, K.N. Exploration of sleep as a specific risk factor for poor metabolic and mental health: A uk biobank study of 84,404 participants. Nat. Sci. Sleep 2021, 13, 1903–1912. [Google Scholar] [CrossRef]
- Bakker, E.A.; Lee, D.C.; Hopman, M.T.E.; Oymans, E.J.; Watson, P.M.; Thompson, P.D.; Thijssen, D.H.J.; Eijsvogels, T.M.H. Dose-response association between moderate to vigorous physical activity and incident morbidity and mortality for individuals with a different cardiovascular health status: A cohort study among 142,493 adults from the Netherlands. PLoS Med. 2021, 18, e1003845. [Google Scholar] [CrossRef]
- Liu, Q.; Liu, F.C.; Huang, K.Y.; Li, J.X.; Yang, X.L.; Wang, X.Y.; Chen, J.C.; Liu, X.Q.; Cao, J.; Shen, C.; et al. Beneficial effects of moderate to vigorous physical activity on cardiovascular disease among Chinese adults. J. Geriatr. Cardiol. 2020, 17, 85–95. [Google Scholar] [CrossRef]
- Wu, F.; Wills, K.; Laslett, L.L.; Oldenburg, B.; Jones, G.; Winzenberg, T. Moderate-to-vigorous physical activity but not sedentary time is associated with musculoskeletal health outcomes in a cohort of australian middle-aged women. J. Bone Miner. Res. 2017, 32, 708–715. [Google Scholar] [CrossRef]
- Batacan, R.B., Jr.; Duncan, M.J.; Dalbo, V.J.; Tucker, P.S.; Fenning, A.S. Effects of light intensity activity on cvd risk factors: A systematic review of intervention studies. Biomed. Res. Int. 2015, 2015, 596367. [Google Scholar] [CrossRef]
- Chastin, S.F.M.; De Craemer, M.; De Cocker, K.; Powell, L.; Van Cauwenberg, J.; Dall, P.; Hamer, M.; Stamatakis, E. How does light-intensity physical activity associate with adult cardiometabolic health and mortality? Systematic review with meta-analysis of experimental and observational studies. Br. J. Sports Med. 2019, 53, 370–376. [Google Scholar] [CrossRef]
- German, C.; Makarem, N.; Fanning, J.; Redline, S.; Elfassy, T.; McClain, A.; Abdalla, M.; Aggarwal, B.; Allen, N.; Carnethon, M. Sleep, sedentary behavior, physical activity, and cardiovascular health: MESA. Med. Sci. Sports Exerc. 2021, 53, 724–731. [Google Scholar] [CrossRef]
- McGregor, D.E.; Carson, V.; Palarea-Albaladejo, J.; Dall, P.M.; Tremblay, M.S.; Chastin, S.F.M. Compositional analysis of the associations between 24-h movement behaviours and health indicators among adults and older adults from the canadian health measure survey. Int. J. Environ. Res. Public Health 2018, 15, 1779. [Google Scholar] [CrossRef]
- McGregor, D.E.; Palarea-Albaladejo, J.; Dall, P.M.; Del Pozo Cruz, B.; Chastin, S.F.M. Compositional analysis of the association between mortality and 24-hour movement behaviour from NHANES. Eur. J. Prev. Cardiol. 2021, 28, 791–798. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Carson, V.; Chaput, J.P.; Connor Gorber, S.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-hour movement guidelines for children and youth: An integration of physical activity, sedentary behaviour, and sleep. Appl. Physiol. Nutr. Metab. 2016, 41, S311–S327. [Google Scholar] [CrossRef]
- Riebe, D.; Ehrman, J.K.; Liguori, G.; Magal, M. (Eds.) ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2018. [Google Scholar]
- Skender, S.; Ose, J.; Chang-Claude, J.; Paskow, M.; Brühmann, B.; Siegel, E.M.; Steindorf, K.; Ulrich, C.M. Accelerometry and physical activity questionnaires—A systematic review. BMC Public Health 2016, 16, 515. [Google Scholar] [CrossRef]
- Stavrinou, P.S.; Bogdanis, G.C.; Giannaki, C.D.; Terzis, G.; Hadjicharalambous, M. High-intensity interval training frequency: Cardiometabolic effects and quality of life. Int. J. Sports Med. 2018, 39, 210–217. [Google Scholar] [CrossRef]
- Beekley, M.D.; Brechue, W.F.; de Hoyos, D.V.; Garzarella, L.; Werber-Zion, G.; Pollock, M.L. Cross-validation of the YMCA submaximal cycle ergometer test to predict VO2max. Res. Q. Exerc. Sport 2004, 75, 337–342. [Google Scholar] [CrossRef]
- Trost, S.G.; McIver, K.L.; Pate, R.R. Conducting accelerometer-based activity assessments in field-based research. Med. Sci. Sports Exerc. 2005, 37, S531–S543. [Google Scholar] [CrossRef]
- Barreira, T.V.; Redmond, J.G.; Brutsaert, T.D.; Schuna, J.M.; Mire, E.F.; Katzmarzyk, P.T.; Tudor-Locke, C. Can an automated sleep detection algorithm for waist-worn accelerometry replace sleep logs? Appl. Physiol. Nutr. Metab. 2018, 43, 1027–1032. [Google Scholar] [CrossRef]
- Choi, L.; Liu, Z.; Matthews, C.E.; Buchowski, M.S. Validation of accelerometer wear and nonwear time classification algorithm. Med. Sci. Sports Exerc. 2011, 43, 357–364. [Google Scholar] [CrossRef]
- Slater, J.; Kruger, R.; Douwes, J.; O’Brien, W.J.; Corbin, M.; Miles-Chan, J.L.; Breier, B.H. Objectively measured physical activity is associated with body composition and metabolic profiles of pacific and New Zealand european women with different metabolic disease risks. Front. Physiol. 2021, 12, 684782. [Google Scholar] [CrossRef] [PubMed]
- Dunstan, D.W.; Kingwell, B.A.; Larsen, R.; Healy, G.N.; Cerin, E.; Hamilton, M.T.; Shaw, J.E.; Bertovic, D.A.; Zimmet, P.Z.; Salmon, J.; et al. Breaking up prolonged sitting reduces postprandial glucose and insulin responses. Diabetes Care 2012, 35, 976–983. [Google Scholar] [CrossRef] [PubMed]
- Tabata, I. Tabata training: One of the most energetically effective high-intensity intermittent training methods. J. Physiol. Sci. 2019, 69, 559–572. [Google Scholar] [CrossRef] [PubMed]
- Goncin, N.; Linares, A.; Lloyd, M.; Dogra, S. Does sedentary time increase in older adults in the days following participation in intense exercise? Aging Clin. Exp. Res. 2020, 32, 2517–2527. [Google Scholar] [CrossRef]
- Baggett, C.D.; Stevens, J.; Catellier, D.J.; Evenson, K.R.; McMurray, R.G.; He, K.; Treuth, M.S. Compensation or displacement of physical activity in middle-school girls: The trial of activity for adolescent girls. Int. J. Obes. 2010, 34, 1193–1199. [Google Scholar] [CrossRef]
- Fedewa, M.V.; Hathaway, E.D.; Williams, T.D.; Schmidt, M.D. Effect of exercise training on non-exercise physical activity: A systematic review and meta-analysis of randomized controlled trials. Sports Med. 2017, 47, 1171–1182. [Google Scholar] [CrossRef]
- Castro, E.A.; Júdice, P.B.; Silva, A.M.; Teixeira, P.J.; Benito, P.J. Sedentary behavior and compensatory mechanisms in response to different doses of exercise-a randomized controlled trial in overweight and obese adults. Eur. J. Clin. Nutr. 2017, 71, 1393–1398. [Google Scholar] [CrossRef]
- De Moura, B.P.; Marins, J.C.; Franceschini Sdo, C.; Reis, J.S.; Amorim, P.R. Aerobic exercise did not have compensatory effects on physical activity levels in type 2 diabetes patients. J. Sports Sci. 2015, 33, 545–551. [Google Scholar] [CrossRef]
- Church, T.S.; Earnest, C.P.; Skinner, J.S.; Blair, S.N. Effects of different doses of physical activity on cardiorespiratory fitness among sedentary, overweight or obese postmenopausal women with elevated blood pressure: A randomized controlled trial. JAMA 2007, 297, 2081–2091. [Google Scholar] [CrossRef]
- Ridgers, N.D.; Timperio, A.; Cerin, E.; Salmon, J. Compensation of physical activity and sedentary time in primary school children. Med. Sci. Sports Exerc. 2014, 46, 1564–1569. [Google Scholar] [CrossRef]
- Sigmund, E.; Sigmundová, D.; Hamrik, Z.; Madarásová Gecková, A. Does participation in physical education reduce sedentary behaviour in school and throughout the day among normal-weight and overweight-to-obese Czech children aged 9–11 years? Int. J. Environ. Res. Public Health 2014, 11, 1076–1093. [Google Scholar] [CrossRef] [PubMed]
- Chevance, G.; Baretta, D.; Romain, A.J.; Godino, J.G.; Bernard, P. Day-to-day associations between sleep and physical activity: A set of person-specific analyses in adults with overweight and obesity. J. Behav. Med. 2021, 45, 14–27. [Google Scholar] [CrossRef] [PubMed]
- Mendelson, M.; Borowik, A.; Michallet, A.S.; Perrin, C.; Monneret, D.; Faure, P.; Levy, P.; Pépin, J.L.; Wuyam, B.; Flore, P. Sleep quality, sleep duration and physical activity in obese adolescents: Effects of exercise training. Pediatric Obes. 2016, 11, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Quist, J.S.; Rosenkilde, M.; Gram, A.S.; Blond, M.B.; Holm-Petersen, D.; Hjorth, M.F.; Stallknecht, B.; Sjödin, A. Effects of exercise domain and intensity on sleep in women and men with overweight and obesity. J. Obes. 2019, 2019, 2189034. [Google Scholar] [CrossRef]
- Kakinami, L.; O’Loughlin, E.K.; Brunet, J.; Dugas, E.N.; Constantin, E.; Sabiston, C.M.; O’Loughlin, J. Associations between physical activity and sedentary behavior with sleep quality and quantity in young adults. Sleep Health 2017, 3, 56–61. [Google Scholar] [CrossRef]
- Smiley, A.; King, D.; Bidulescu, A. The association between sleep duration and metabolic syndrome: The NHANES 2013/2014. Nutrients 2019, 11, 2582. [Google Scholar] [CrossRef] [PubMed]
- Scherr, J.; Wolfarth, B.; Christle, J.W.; Pressler, A.; Wagenpfeil, S.; Halle, M. Associations between Borg’s rating of perceived exertion and physiological measures of exercise intensity. Eur. J. Appl. Physiol. 2013, 113, 147–155. [Google Scholar] [CrossRef]
- Kossi, O.; Lacroix, J.; Ferry, B.; Batcho, C.S.; Julien-Vergonjanne, A.; Mandigout, S. Reliability of ActiGraph GT3X+ placement location in the estimation of energy expenditure during moderate and high-intensity physical activities in young and older adults. J. Sports Sci. 2021, 39, 1489–1496. [Google Scholar] [CrossRef]




| Variables | Mean ± SD |
|---|---|
| Age (years) | 25.4 ± 1.0 |
| Weight (kg) | 60.9 ± 4.9 |
| Height (m) | 165.4 ± 3.9 |
| Body mass index (kg/m2) | 22.3 ± 1.9 |
| VO2max (mL/kg/min) | 36.8 ± 4.3 |
| Accelerometry (days) | 13.9 ± 0.3 |
| Wear time (h/d) | 23.6 ± 0.2 |
| Movement behaviors: | |
| LPA (min/d) | 269.4 ± 55.5 |
| MPA (min/d) | 148.3 ± 47.4 |
| VPA (min/d) | 11.1 ± 7.2 |
| MVPA (min/d) | 159.5 ± 52.0 |
| TPA (cpm) | 1411.5 ± 381.5 |
| ST (min/d) | 446.7 ± 98.9 |
| PST (min/d) | 160.4 ± 54.4 |
| Sleep (h/d) | 9.0 ± 1.1 |
| Variables | Control Week | Exercise Week | Mean Change | 95% CI | % Change | p Value | Effect Size (Cohens’d) | |
|---|---|---|---|---|---|---|---|---|
| LPA (min/d) | 269.4 ± 55.5 | 246.0 ± 54.5 | −23.4 ± 44.3 * | −43.5 | −3.2 | −7.3 ± 16.7% | p < 0.05 | −0.53 |
| MPA (min/d) | 148.3 ± 47.4 | 159.8 ± 44.8 | 11.5 ± 12.6 *** | 5.7 | 17.2 | 9.9 ± 11.7% | p < 0.001 | 0.91 |
| VPA (min/d) | 11.1 ± 7.2 | 13.8 ± 7.6 | 2.6 ± 2.7 *** | 1.4 | 3.8 | 35.2 ± 40.6% | p < 0.001 | 0.96 |
| MVPA (min/d) | 159.5 ± 52.0 | 173.6 ± 49.1 | 14.1 ± 13.1 *** | 8.2 | 20.1 | 11.1 ± 11.6% | p < 0.001 | 1.06 |
| TPA (cpm) | 1411.5 ± 381.5 | 1530.7 ± 384.3 | 119.2 ± 70.9 *** | 86.9 | 151.5 | 9.1 ± 5.6% | p < 0.001 | 1.68 |
| ST (min/d) | 446.7 ± 98.9 | 464.1 ± 95.5 | 17.5 ± 25.9 ** | 5.7 | 29.3 | 4.4 ± 6.0% | p < 0.01 | 0.68 |
| PST (min/d) | 160.4 ± 54.4 | 148.1 ± 50.1 | −12.3 ± 24.7 * | −23.5 | −1.0 | −5.1 ± 20.6% | p < 0.05 | −0.49 |
| Sleep (h/d) | 9.0 ± 1.1 | 8.5 ± 0.7 | −0.5 ± 0.7 ** | −0.8 | −0.2 | −5.0 ± 7.5% | p < 0.01 | −0.71 |
| Variables | Control | Exercise Day | Next Day | p-Value | η2 |
|---|---|---|---|---|---|
| LPA (min/d) | 269.4 ± 55.5 | 245.9 ± 50.8 * | 250.9 ± 53.1 *† | <0.001 | 0.615 |
| MPA (min/d) | 148.3 ± 47.4 | 170.2 ± 46.9 * | 151.0 ± 45.5 † | <0.001 | 0.784 |
| VPA (min/d) | 11.1 ± 7.2 | 14.0 ± 7.5 * | 11.6 ± 6.6 † | <0.001 | 0.735 |
| MVPA (min/d) | 159.5 ± 52.0 | 184.2 ± 51.6 * | 162.6 ± 48.9 † | <0.001 | 0.816 |
| TPA (cpm) | 1411.5 ± 381.5 | 1605.8 ± 401.4 * | 1472.8 ± 366.4 *† | <0.001 | 0.784 |
| ST (min/d) | 446.7 ± 98.9 | 454.6 ± 101.3 * | 473.6 ± 103.3 *† | <0.001 | 0.462 |
| PST (min/d) | 160.4 ± 54.4 | 152 ± 47.5 * | 150.5 ± 45.8 * | <0.001 | 0.35 |
| Sleep (h/d) | 9.0 ± 1.1 | 8.6 ± 0.8 * | 8.5 ± 0.8 * | <0.001 | 0.419 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, Y.; Wiltshire, H.D.; Baker, J.S.; Wang, Q. Effects of Low-Volume High-Intensity Interval Exercise on 24 h Movement Behaviors in Inactive Female University Students. Int. J. Environ. Res. Public Health 2022, 19, 7177. https://doi.org/10.3390/ijerph19127177
Lu Y, Wiltshire HD, Baker JS, Wang Q. Effects of Low-Volume High-Intensity Interval Exercise on 24 h Movement Behaviors in Inactive Female University Students. International Journal of Environmental Research and Public Health. 2022; 19(12):7177. https://doi.org/10.3390/ijerph19127177
Chicago/Turabian StyleLu, Yining, Huw D. Wiltshire, Julien S. Baker, and Qiaojun Wang. 2022. "Effects of Low-Volume High-Intensity Interval Exercise on 24 h Movement Behaviors in Inactive Female University Students" International Journal of Environmental Research and Public Health 19, no. 12: 7177. https://doi.org/10.3390/ijerph19127177
APA StyleLu, Y., Wiltshire, H. D., Baker, J. S., & Wang, Q. (2022). Effects of Low-Volume High-Intensity Interval Exercise on 24 h Movement Behaviors in Inactive Female University Students. International Journal of Environmental Research and Public Health, 19(12), 7177. https://doi.org/10.3390/ijerph19127177