
Estimation of Tinnitus-Related Socioeconomic Costs in Germany

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Ethical Statement
2.2. Data Acquisition
2.3. Calculation of Socioeconomic Costs
2.4. Statistics
3. Results
3.1. Patient Statistics
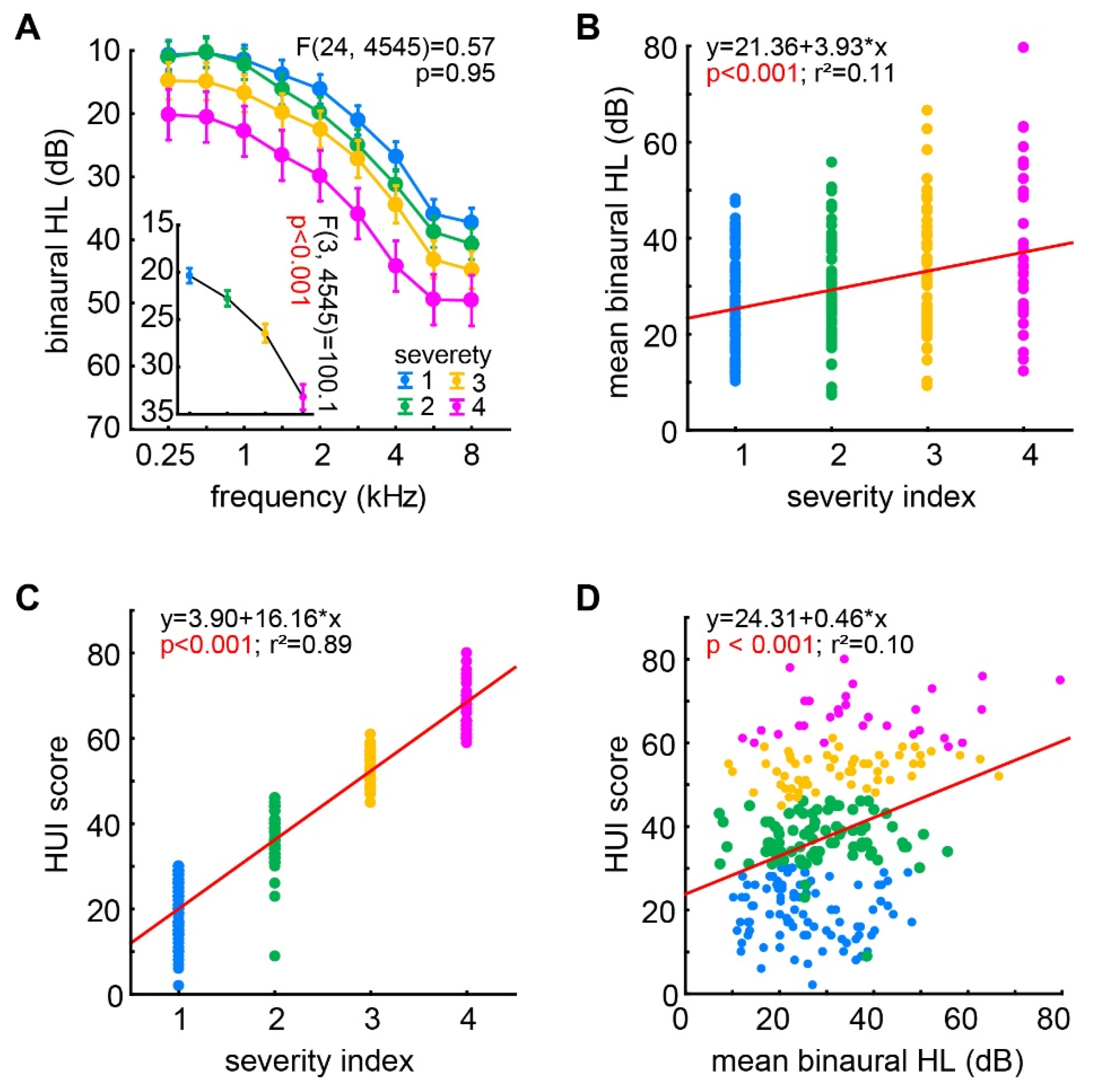
3.2. Audiological and HUI Dependencies
3.3. Socioeconomic Cost of Tinnitus
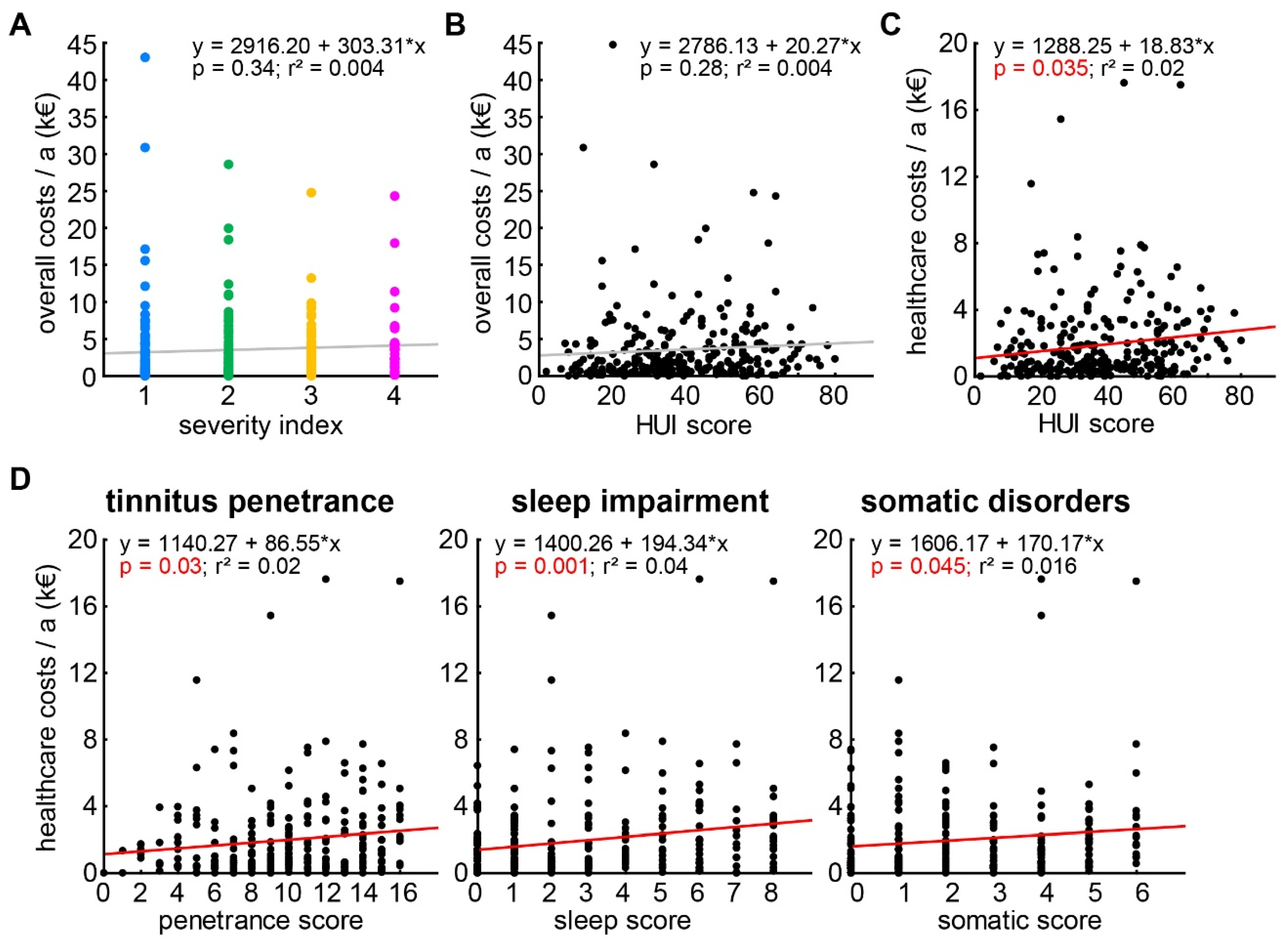
3.4. Dependencies of the Socioeconomic Costs on Other Variables
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Biesinger, E.; Goebel, G.; Hesse, G.; Kießling, J.; Laubert, A.; Mazurek, B.; Michel, O.; Schaaf, H.; Szczepek, A.J. Tinnitus; Georg Thieme Verlag: Leipzig, Germany, 2016. [Google Scholar]
- Biswas, R.; Lugo, A.; Akeroyd, M.A.; Schlee, W.; Gallus, S.; Hall, D.A. Tinnitus prevalence in Europe: A multi-country cross-sectional population study. Lancet Reg. Health Eur. 2022, 12, 100250. [Google Scholar] [CrossRef] [PubMed]
- Lockwood, A.H.; Salvi, R.J.; Burkard, R.F. Tinnitus. New Engl. J. Med. 2002, 347, 904–910. [Google Scholar] [CrossRef] [PubMed]
- Hebert, S.; Canlon, B.; Hasson, D.; Hanson, L.L.M.; Westerlund, H.; Theorell, T. Tinnitus severity is reduced with reduction of depressive mood--a prospective population study in Sweden. PLoS ONE 2012, 7, e37733. [Google Scholar]
- Henry, J.A.M.; Gilbert, A. Audiometric correlates of tinnitus pitch: Insights from the Tinnitus Data Registry. In Proceedings of the Sixth International Tinnitus Seminar, Cambridge, UK, 5–9 September 1999; Hazell, J., Ed.; The Tinnitus and Hyperacusis Centre: London, UK, 1999; pp. 51–57. [Google Scholar]
- Di Stadio, A.; Dipietro, L.; Ricci, G.; della Volpe, A.; Minni, A.; Greco, A.; de Vincentiis, M.; Ralli, M. Hearing loss, tinnitus, hyperacusis, and diplacusis in professional musicians: A systematic review. Int. J. Environ. Res. Public Health 2018, 15, 2120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, J.J.; Chen, K. The relationship of tinnitus, hyperacusis, and hearing loss. Ear Nose Throat J. 2004, 83, 472–476. [Google Scholar] [CrossRef] [Green Version]
- Ryu, I.S.; Ahn, J.H.; Lim, H.W.; Joo, K.Y.; Chung, J.W. Evaluation of masking effects on speech perception in patients with unilateral chronic tinnitus using the hearing in noise test. Otol. Neurotol. 2012, 33, 1472–1476. [Google Scholar] [CrossRef]
- Niewiarowicz, M.; Wicher, A.; Sęk, A.; Górecki, T. Speech intelligibility deterioration for normal hearing and hearing impaired patients with different types of tinnitus. Speech Commun. 2022, 139, 35–44. [Google Scholar] [CrossRef]
- Møller, A.R. Epidemiology of Tinnitus in Adults. In Textbook of Tinnitus; Møller, A.R.L., De Ridder, B.D., Kleinjung, T., Eds.; Springer: New York, NY, USA, 2011; pp. 29–37. [Google Scholar]
- Coles, R.R. Epidemiology of tinnitus: (1) prevalence. J. Laryngol. Otol. Suppl. 1984, 9, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Langguth, B.; Landgrebe, M.; Kleinjung, T.; Sand, G.P.; Hajak, G. Tinnitus and depression. World J. Biol. Psychiatry 2011, 12, 489–500. [Google Scholar] [CrossRef]
- Lewis, J.E.; Stephens, S.D.; McKenna, L. Tinnitus and suicide. Clin. Otolaryngol. Allied Sci. 1994, 19, 50–54. [Google Scholar] [CrossRef]
- Eggermont, J.J. Central tinnitus. Auris Nasus Larynx 2003, 30, S7–S12. [Google Scholar] [CrossRef]
- Eggermont, J.J.; Roberts, L.E. The neuroscience of tinnitus. Trends Neurosci. 2004, 27, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Gerken, G.M. Central tinnitus and lateral inhibition: An auditory brainstem model. Hear Res. 1996, 97, 75–83. [Google Scholar] [CrossRef]
- Knipper, M.; Ruettiger, L.; Schick, B.; Dlugaiczyk, J. Glycine Receptor Agonists for the Treatment of Phantom Phenomena. U.S. Patent Application No. 12/818,391, 31 March 2011. [Google Scholar]
- Ruttiger, L.; Singer, W.; Panford-Walsh, R.; Matsumoto, M.; Lee, S.C.; Zuccotti, A.; Zimmermann, U.; Jaumann, M.; Rohbock, K.; Xiong, H.; et al. The reduced cochlear output and the failure to adapt the central auditory response causes tinnitus in noise exposed rats. PLoS ONE 2013, 8, e57247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaette, R.; McAlpine, D. Tinnitus with a normal audiogram: Physiological evidence for hidden hearing loss and computational model. J. Neurosci. 2011, 31, 13452–13457. [Google Scholar] [CrossRef] [Green Version]
- Engineer, N.D.; Riley, J.R.; Seale, J.D.; Vrana, W.A.; Shetake, J.A.; Sudanagunta, S.P.; Borland, M.S.; Kilgard, M.P. Reversing pathological neural activity using targeted plasticity. Nature 2011, 470, 101–104. [Google Scholar] [CrossRef]
- Weisz, N.; Hartmann, T.; Dohrmann, K.; Schlee, W.; Norena, A. High-frequency tinnitus without hearing loss does not mean absence of deafferentation. Hear. Res. 2006, 222, 108–114. [Google Scholar] [CrossRef] [Green Version]
- Savastano, M. Tinnitus with or without hearing loss: Are its characteristics different? Eur. Arch. Otorhinolaryngol. 2008, 265, 1295–1300. [Google Scholar] [CrossRef]
- Hickox, A.E.; Liberman, M.C. Is noise-induced cochlear neuropathy key to the generation of hyperacusis or tinnitus? J. Neurophysiol. 2014, 111, 552–564. [Google Scholar] [CrossRef] [Green Version]
- Krauss, P.; Tziridis, K.; Metzner, C.; Schilling, A.; Hoppe, U.; Schulze, H. Stochastic Resonance Controlled Upregulation of Internal Noise after Hearing Loss as a Putative Cause of Tinnitus-Related Neuronal Hyperactivity. Front Neurosci. 2016, 10, 597. [Google Scholar] [CrossRef]
- Tziridis, K.; Forster, J.; Buchheidt-Dorfler, I.; Krauss, P.; Schilling, A.; Wendler, O.; Sterna, E.; Schulze, H. Tinnitus development is associated with synaptopathy of inner hair cells in Mongolian gerbils. Eur. J. Neurosci. 2021, 54, 4768–4780. [Google Scholar] [CrossRef] [PubMed]
- Tziridis, K.; Brunner, S.; Schilling, A.; Krauss, P.; Schulze, H. Spectrally Matched Near-Threshold Noise for Subjective Tinnitus Loudness Attenuation Based on Stochastic Resonance. Front. Neurosci. 2022, 16, 831581. [Google Scholar] [CrossRef] [PubMed]
- Schilling, A.; Tziridis, K.; Schulze, H.; Krauss, P. The stochastic resonance model of auditory perception: A unified explanation of tinnitus development, Zwicker tone illusion, and residual inhibition. In Progress in Brain Research; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Krauss, P.; Schilling, A.; Tziridis, K.; Schulze, H. Modelle der Tinnitusentstehung. HNO 2019, 67, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Trochidis, I.; Lugo, A.; Borroni, E.; Cederroth, C.R.; Cima, R.; Kikidis, D.; Langguth, B.; Schlee, W.; Gallus, S. Systematic review on healthcare and societal costs of tinnitus. Int. J. Environ. Res. Public Health 2021, 18, 6881. [Google Scholar] [CrossRef]
- Cederroth, C.R.; Canlon, B.; Langguth, B. Hearing loss and tinnitus—Are funders and industry listening? Nat. Biotechnol. 2013, 31, 972–974. [Google Scholar] [CrossRef]
- Rademaker, M.M.; Stegeman, I.; Hooiveld, M.; Stokroos, R.J.; Smit, A.L. Patients with tinnitus use more primary healthcare compared to people without tinnitus. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef]
- Maes, I.H.; Cima, R.F.; Vlaeyen, J.W.; Anteunis, L.J.; Joore, M.A. Tinnitus: A cost study. Ear Hear. 2013, 34, 508–514. [Google Scholar] [CrossRef] [Green Version]
- Ehring, F.S.; Köster, A.-D. Gesundheitssysteme im Vergleich. Die Gesundheitsreformen in den Niederlanden und in der Schweiz als Vorbild für Deutschland. Available online: https://www.sozialpolitik-aktuell.de/files/sozialpolitik-aktuell/_Politikfelder/Gesundheitswesen/Dokumente/pkv-doku_no29_12w.pdf (accessed on 1 July 2022).
- Van Asselt, A.; Dirksen, C.D.; Arntz, A.; Severens, J.L. The cost of borderline personality disorder: Societal cost of illness in BPD-patients. Eur. Psychiatry 2007, 22, 354–361. [Google Scholar] [CrossRef]
- Acarturk, C.; Smit, F.; de Graaf, R.; van Straten, A.; Have, M.T.; Cuijpers, P. Economic costs of social phobia: A population-based study. J. Affect. Disord. 2009, 115, 421–429. [Google Scholar] [CrossRef]
- Lambeek, L.C.; van Tulder, M.W.; Swinkels, I.C.; Koppes, L.L.; Anema, J.R.; van Mechelen, W. The trend in total cost of back pain in The Netherlands in the period 2002 to 2007. Spine 2011, 36, 1050–1058. [Google Scholar] [CrossRef] [Green Version]
- Furlong, W.J.; Feeny, D.H.; Torrance, G.W.; Barr, R.D. The Health Utilities Index (HUI®) system for assessing health-related quality of life in clinical studies. Ann. Med. 2001, 33, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Goebel, G.; Hiller, W. Tinnitus-Fragebogen (TF). Standardinstrument zur Graduierung des Tinnitusschweregrades. Erbebnisse einer Multicenterstudie mit dem Tinnitus-Fragebogen (TF). HNO 1994, 42, 166–172. [Google Scholar] [PubMed]
- Neumeier, S. Regionale Erreichbarkeit von Ausgewählten Fachärzten, Apotheken, Ambulanten Pflege-Diensten und Weiteren Ausgewählten Medizin-Dienstleistungen in Deutschland—Abschätzung auf Basis des Thünen-Erreichbar-Keitsmodells; Thünen Working Paper 77; Thünen-Institut für Ländliche Räume: Braunschweig, Germany, 2017. [Google Scholar]
- Beck, C.H. Steuerrichtlinien; Verlag C.H.BECK: Munich, Germany, 2021. [Google Scholar]
- Volkswirtschaftliche Kosten durch Arbeitsunfähigkeit 2017; Bundesanstalt für Arbeitsschutz und Arbeitsmedizin: Dortmund, Germany, 2017.
- Einheitlicher Bewertungsmaßstab; Kassenärztliche Bundesvereinigung: Berlin, Germany, 2022.
- Hermanns, P.M.; Diep, G.; Mattig, W. GOÄ 2019 Kommentar, IGeL-Abrechnung; Gebührenordnung für Ärzte; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Hörgeräte: Übernahme der Kosten, Verbraucherzentrale Bundesverband. 2021. Available online: https://www.verbraucherzentrale.de/wissen/gesundheit-pflege/krankenversicherung/hoergeraete-uebernahme-der-kosten-11470 (accessed on 1 July 2022).
- Vertrag über die Versorgung der Versicherten ab Vollendung des 18. Lebensjahres mit Hörsystemen gemäß § 127 Abs. 1 SGB V. 2019. Available online: https://www.aok.de/gp/fileadmin/user_upload/Hilfsmittel/Hoerhilfen/bw_hoerhilfen_verbandsvertrag_who_2_3.pdf (accessed on 1 July 2022).
- Vertrag zur Komplettversorgung mit Hörsystemen Zwischen der Innung für Hörakustik und Verschiedenen Ersatzkassen; Logos Verlag: Berlin, Germany, 2015.
- Freitag, M. Krankenkassen-Zuschuss bei Hörgeräten. Wie viel übernimmt die Krankenkasse bei Hörgeräten? Audibene: Berlin, Germany, 2021. [Google Scholar]
- Zirke, N.; Seydel, C.; Szczepek, A.J.; Olze, H.; Haupt, H.; Mazurek, B. Psychological comorbidity in patients with chronic tinnitus: Analysis and comparison with chronic pain, asthma or atopic dermatitis patients. Qual. Life Res. 2013, 22, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Heilmittelrichtline des Gemeinsamen Bundesaussusses Deutscher Verband Ergotherapie; Deutscher Verband Ergotherapie: Karlsbad-Ittersbach, Germany, 2021.
- Bösel, C. Einfluss Funktionstherapeutischer Maßnahmen auf die Tinnitusbelastung beiPatienten mit Chronischem Tinnitus und Symptomen Einer CraniomandibulärenDysfunktion. Ph.D. Thesis, Universitätsmedizin Berlin, Berlin, Germany, 2006. [Google Scholar]
- Gebührenverzeichnisse der Kassenzahnärztlichen Bundesvereinigung; Kassenärztliche Bundesvereinigung: Berlin, Germany, 2022.
- Terrahe, K. The cervico-cranial syndrome in the practice of the otorhinolaryngologist. Laryngol. Rhinol. Otol. 1985, 64, 292–299. [Google Scholar] [CrossRef]
- Reisshauer, A.; Mathiske-Schmidt, K.; Küchler, I.; Umland, G.; Klapp, B.; Mazurek, B. Functional disturbances of the cervical spine in tinnitus. HNO 2006, 54, 125–131. [Google Scholar]
- Biesinger, E.; Reisshauer, A.; Mazurek, B. Die Rolle der Halswirbelsäule und des Kiefergelenks bei Tinnitus. HNO 2008, 56, 673–677. [Google Scholar] [CrossRef]
- Heilmittelrichtlinie; Kassenärztliche Bundesvereinigung: Berlin, Germany, 2021.
- Buchner, R. Wie man angemessene Privatpreise durchsetzt. Ergopraxis 2019, 12, 10–12. [Google Scholar] [CrossRef] [Green Version]
- Bispinck, R.; Dribbusch, H.; Öz, F.; Stoll, E.T. Was Verdienen Sozialpädagoginnen und Sozial-Pädagogen? Projekt Lohnspiegel.de; Hans Böckler Stiftung: Düsseldorf, Germany, 2015. [Google Scholar]
- Bundesamt, S. Qualität der Arbeit—Krankenstand; Statistisches Bundesamt: Berlin, Germany, 2019. [Google Scholar]
- Mazurek, B.; Szczepek, A.; Hebert, S. Stress and tinnitus. HNO 2015, 63, 258–265. [Google Scholar] [CrossRef]
- Pinto, P.C.L.; Sanchez, T.G.; Tomita, S. The impact of gender, age and hearing loss on tinnitus severity. Braz. J. Otorhinolaryngol. 2010, 76, 18–24. [Google Scholar] [CrossRef] [Green Version]
- Martines, F.; Bentivegna, D.; di Piazza, F.; Martines, E.; Sciacca, V.; Martinciglio, G. Investigation of tinnitus patients in Italy: Clinical and audiological characteristics. Int. J. Otolaryngol. 2010, 2010, 265861. [Google Scholar] [CrossRef] [Green Version]
- Seydel, C.; Haupt, H.; Olze, H.; Szczepek, A.J.; Mazurek, B. Gender and chronic tinnitus: Differences in tinnitus-related distress depend on age and duration of tinnitus. Ear Hear. 2013, 34, 661–672. [Google Scholar] [CrossRef] [PubMed]
- Kauhl, B.; Maier, W.; Schweikart, J.; Keste, A.; Moskwyn, M. Who is where at risk for Chronic Obstructive Pulmonary Disease? A spatial epidemiological analysis of health insurance claims for COPD in Northeastern Germany. PLoS ONE 2018, 13, e0190865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wacker, M.E.; Jörres, R.A.; Schulz, H.; Heinrich, J.; Karrasch, S.; Karch, A.; Koch, A.; Peters, A.; Leidl, R.; Vogelmeier, C.; et al. Direct and indirect costs of COPD and its comorbidities: Results from the German COSYCONET study. Respir. Med. 2016, 111, 39–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirsch, F.; Teuner, C.; Menn, P.; Leidl, R. Costs of illness for asthma and COPD in adults in Germany. Gesundheitswesen 2013, 75, 413–423. [Google Scholar]
- Heidemann, C.; Scheidt-Nave, C. Prevalence, incidence and mortality of diabetes mellitus in adults in Germany—A review in the framework of the diabetes Surveillanc. J. Health Monit. 2017, 2, 98–121. [Google Scholar]
- Köster, I.; Huppertz, E.; Hauner, H.; Schubert, I. Direct costs of diabetes mellitus in Germany—CoDiM 2000–2007. Exp. Clin. Endocrinol. Diabetes 2011, 119, 377–385. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Severity Index | Number of Patients | Compensated/Uncompensated Tinnitus Patients |
|---|---|---|
| 1 | 90 | 172 |
| 2 | 82 | |
| 3 | 56 | 86 |
| 4 | 30 |
| Visit at Specific Medical Personal or Service | Mean Public Health Care Insurance Costs (EUR) | Mean Private Health Care Insurance Costs (EUR) |
|---|---|---|
| General practitioner (GP) | 13.60 | 37.12 |
| House call GP | 45.11 | 60.14 |
| Emergency service | 21.10 | 49.06 |
| ENT specialist | 56.48 | 74.62 |
| ENT clinic | 98.90 | 138.05 |
| Neurologist | 81.25 | 212.06 |
| Audiologist | 255.00 | 500.00 |
| Psychiatrist | 25.44 | 67.04 |
| Psychotherapist | 86.38 | 107.69 |
| Occupational therapist | 65.72 | 118.30 |
| Dentist | 72.46 | 102.26 |
| Physiotherapist | 30.64 | 51.55 |
| Social worker | 8.59 | 8.59 |
| Medical officer | 6.75 | 6.75 |
| Severity 1 | Severity 2 | Severity 3 + 4 | All Patients | |||||
|---|---|---|---|---|---|---|---|---|
| Mean Visits | Mean Costs (EUR) | Mean Visits | Mean Costs (EUR) | Mean Visits | Mean Costs (EUR) | Mean Visits | Mean Costs (EUR) | |
| GP | 9.69 | 198.67 | 13.26 | 229.79 | 16.70 | 278.34 | 13.21 | 238.64 |
| House call GP | 0.04 | 2.00 | 0.10 | 4.40 | 0.08 | 4.20 | 0.12 | 6.27 |
| Emerg. service | - | - | 0.10 | 2.06 | 0.14 | 2.94 | 0.12 | 3.90 |
| ENT specialist | 3.87 | 233.71 | 4.63 | 273.24 | 6.33 | 364.86 | 4.96 | 292.33 |
| ENT clinic | 3.56 | 396.52 | 2.54 | 198.50 | 1.67 | 147.10 | 2.59 | 249.48 |
| Neurologist | 0.53 | 60.77 | 0.59 | 47.56 | 1.67 | 196.89 | 0.93 | 101.55 |
| Audiologist | 1.07 | 413.56 | 1.12 | 345.85 | 1.35 | 446.51 | 1.17 | 401.47 |
| Psychiatrist/ | 2.00 | 188.86 | 3.51 | 352.24 | 4.05 | 367.38 | 3.15 | 299.13 |
| Psychotherapist | 0.89 | 37.40 | 1.46 | 85.93 | 0.56 | 18.07 | 0.96 | 46.20 |
| Occupat. thera. | 0.27 | 17.53 | 0.05 | 3.21 | 0.56 | 44.02 | 0.29 | 21.72 |
| Dentist | 0.31 | 27.84 | 1.07 | 82.12 | 1.12 | 80.89 | 0.82 | 62.53 |
| Physiotherapist | 5.07 | 206.36 | 6.78 | 251.61 | 11.07 | 387.81 | 7.58 | 280.14 |
| Social worker | - | - | - | - | 0.70 | 5.99 | 0.23 | 1.99 |
| Medical officer | 0.09 | 0.60 | 0.15 | 0.99 | 0.14 | 0.94 | 0.14 | 0.94 |
| Others | 0.3 | 28.88 | 0.92 | 159.12 | 0.81 | 340.49 | 0.75 | 173.48 |
| Prescr. Drugs * | 0.17 | 25.98 | 0.18 | 19.57 | 0.31 | 39.26 | 0.22 | 28.28 |
| Complete costs | 27.68 | 1838.69 | 36.46 | 2056.20 | 47.27 | 2725.69 | 38.92 | 2206.95 |
| Active Ingredient or Drug® | Pack Size (No. of Pills) | Lowest Found Price (EUR) |
|---|---|---|
| Amitriptylin | 50 | 14.35 |
| Carbamazepin | 200 | 29.13 |
| Diazepam | 50 | 12.57 |
| Ginkgo biloba | 60 | 28.79 |
| Lorazepam | 50 | 14.30 |
| Magnesium | 50 | 9.95 |
| Oxazepam | 50 | 12.59 |
| Zinc sulphate | 20 | 3.49 |
| Zolpidem | 20 | 14.29 |
| Amioxid-neurax® | 50 | 12.70 |
| Betavert® | 50 | 17.99 |
| Cinnarizin® | 50 | 28.52 |
| Laif 900® | 60 | 23.26 |
| Mirtazapin® | 50 | 24.32 |
| Prednisolon® | 50 | 16.35 |
| Seroxat® | 50 | 47.95 |
| Venlafaxin® | 20 | 20.90 |
| Zoloft® | 50 | 32.25 |
| First Variable | Second Variable | Linear Equation | r2 Value | p Value |
|---|---|---|---|---|
| individual overall costs | Severity index | y = 2916.2 + 303.3 × x | 0.004 | 0.34 |
| HUI score (complete) | y = 2786.1 + 20.2 × x | 0.004 | 0.28 | |
| HUI: emotions | y = 3080.8 + 47.6 × x | 0.003 | 0.40 | |
| HUI: cognition | y = 3273.8 + 45.1 × x | 0.001 | 0.57 | |
| HUI: penetrance | y = 3254.2 + 31.4 × x | 0.0005 | 0.71 | |
| HUI: auditory | y = 3093.5 + 82.0 × x | 0.004 | 0.33 | |
| HUI: sleep | y = 2766.5 + 258.2 × x | 0.02 | 0.04 | |
| HUI: somatic | y = 3261.5 + 131.2 × x | 0.002 | 0.46 | |
| individual healthcare costs | Severity index | y = 1389.0 + 291.3 × x | 0.014 | 0.058 |
| HUI score (complete) | y = 1288.3 + 18.8 × x | 0.02 | 0.035 | |
| HUI: emotions | y = 1731.5 + 26.6 × x | 0.004 | 0.33 | |
| HUI: cognition | y = 1652.1 + 53.9 × x | 0.008 | 0.16 | |
| HUI: penetrance | y = 1140.3 + 86.6 × x | 0.02 | 0.03 | |
| HUI: auditory | y = 1690.9 + 54.0 × x | 0.007 | 0.18 | |
| HUI: sleep | y = 1400.3 + 194.3 ×x | 0.04 | 0.001 | |
| HUI: somatic | y = 1606.2 + 170.2 × x | 0.016 | 0.045 | |
| individual private costs | Severity index | y = 396.1 + 62.1 × x | 0.002 | 0.51 |
| HUI score (complete) | y = 259.2 + 7.1 × x | 0.006 | 0.20 | |
| HUI: emotions | y = 314.5 + 21.1 × x | 0.006 | 0.21 | |
| HUI: cognition | y = 472.9 + 8.8 × x | 0.0005 | 0.71 | |
| HUI: penetrance | y = 495.5 + 3.5 × x | 0.0001 | 0.89 | |
| HUI: auditory | y = 302.0 + 39.5 × x | 0.01 | 0.11 | |
| HUI: sleep | y = 342.7 + 60.5 × x | 0.01 | 0.16 | |
| HUI: somatic | y = 311.9 + 97.7 × x | 0.01 | 0.073 | |
| individual economic costs | Severity index | y = 1131.1 − 50.1 × x | 0.0002 | 0.83 |
| HUI score (complete) | y = 1238.7 − 5.6 × x | 0.0007 | 0.68 | |
| HUI: emotions | y = 1034.7 − 0.1 × x | <0.0001 | 0.99 | |
| HUI: cognition | y = 1148.8 − 17.6 × x | 0.0003 | 0.77 | |
| HUI: penetrance | y = 1618.4 − 58.6 × x | 0.003 | 0.35 | |
| HUI: auditory | y = 1100.6 − 11.5 × x | 0.0001 | 0.85 | |
| HUI: sleep | y = 1023.5 + 3.4 × x | <0.0001 | 0.97 | |
| HUI: somatic | y = 1343.4 − 132.7 × x | 0.001 | 0.31 |
| First Variable | Second Variable | F Value of Slope | R2 Value | p Value |
|---|---|---|---|---|
| individual overall costs | Severity index | 0.44 | 0.005 | 0.72 |
| HUI score (complete) | 1.19 | 0.005 | 0.27 | |
| HUI: emotions | 0.70 | 0.003 | 0.40 | |
| HUI: cognition | 0.32 | 0.001 | 0.57 | |
| HUI: penetrance | 0.14 | 0.0005 | 0.71 | |
| HUI: auditory | 0.97 | 0.004 | 0.33 | |
| HUI: sleep | 4.24 | 0.016 | 0.04 | |
| HUI: somatic | 0.55 | 0.002 | 0.46 | |
| individual healthcare costs | Severity index | 1.66 | 0.02 | 0.18 |
| HUI score (complete) | 4.48 | 0.017 | 0.035 | |
| HUI: emotions | 0.94 | 0.004 | 0.33 | |
| HUI: cognition | 1.95 | 0.008 | 0.16 | |
| HUI: penetrance | 4.54 | 0.018 | 0.034 | |
| HUI: auditory | 1.81 | 0.007 | 0.18 | |
| HUI: sleep | 10.57 | 0.040 | 0.001 | |
| HUI: somatic | 4.05 | 0.016 | 0.045 | |
| individual private costs | Severity index | 1.59 | 0.018 | 0.19 |
| HUI score (complete) | 1.65 | 0.006 | 0.20 | |
| HUI: emotions | 1.58 | 0.006 | 0.21 | |
| HUI: cognition | 0.14 | 0.0005 | 0.71 | |
| HUI: penetrance | 0.02 | <0.0001 | 0.89 | |
| HUI: auditory | 2.57 | 0.01 | 0.11 | |
| HUI: sleep | 2.63 | 0.01 | 0.11 | |
| HUI: somatic | 3.24 | 0.01 | 0.07 | |
| individual economic costs | Severity index | 0.34 | 0.004 | 0.79 |
| HUI score (complete) | 0.17 | 0.0006 | 0.68 | |
| HUI: emotions | 0.00 | 0.00 | 1.00 | |
| HUI: cognition | 0.09 | 0.0003 | 0.77 | |
| HUI: penetrance | 0.88 | 0.003 | 0.35 | |
| HUI: auditory | 0.03 | 0.0001 | 0.85 | |
| HUI: sleep | 0.001 | <0.0001 | 0.97 | |
| HUI: somatic | 1.04 | 0.004 | 0.31 |
| Compensated Tinnitus Patients | Uncompensated Tinnitus Patients | p Value | |
|---|---|---|---|
| Overall costs | 3657.40 [2742.72, 6089.08] | 4912.02 [3314.84, 6346.34] | 0.007 |
| Healthcare costs | 1857.64 [1430.65, 3270.50] | 2835.04 [1668.20, 4272.80] | 0.005 |
| Private costs | 153.54 [113.03, 439.46] | 242.92 [135.25, 541.48] | 0.009 |
| Economic costs | 2250.57 [0, 4142.90] | 2158.62 [0, 5031.60] | 0.34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tziridis, K.; Friedrich, J.; Brüeggemann, P.; Mazurek, B.; Schulze, H. Estimation of Tinnitus-Related Socioeconomic Costs in Germany. Int. J. Environ. Res. Public Health 2022, 19, 10455. https://doi.org/10.3390/ijerph191610455
Tziridis K, Friedrich J, Brüeggemann P, Mazurek B, Schulze H. Estimation of Tinnitus-Related Socioeconomic Costs in Germany. International Journal of Environmental Research and Public Health. 2022; 19(16):10455. https://doi.org/10.3390/ijerph191610455
Chicago/Turabian StyleTziridis, Konstantin, Jana Friedrich, Petra Brüeggemann, Birgit Mazurek, and Holger Schulze. 2022. "Estimation of Tinnitus-Related Socioeconomic Costs in Germany" International Journal of Environmental Research and Public Health 19, no. 16: 10455. https://doi.org/10.3390/ijerph191610455
APA StyleTziridis, K., Friedrich, J., Brüeggemann, P., Mazurek, B., & Schulze, H. (2022). Estimation of Tinnitus-Related Socioeconomic Costs in Germany. International Journal of Environmental Research and Public Health, 19(16), 10455. https://doi.org/10.3390/ijerph191610455