

The Healing Environment of Dental Clinics through the Eyes of Patients and Healthcare Professionals: A Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical and Data Analysis
3. Results
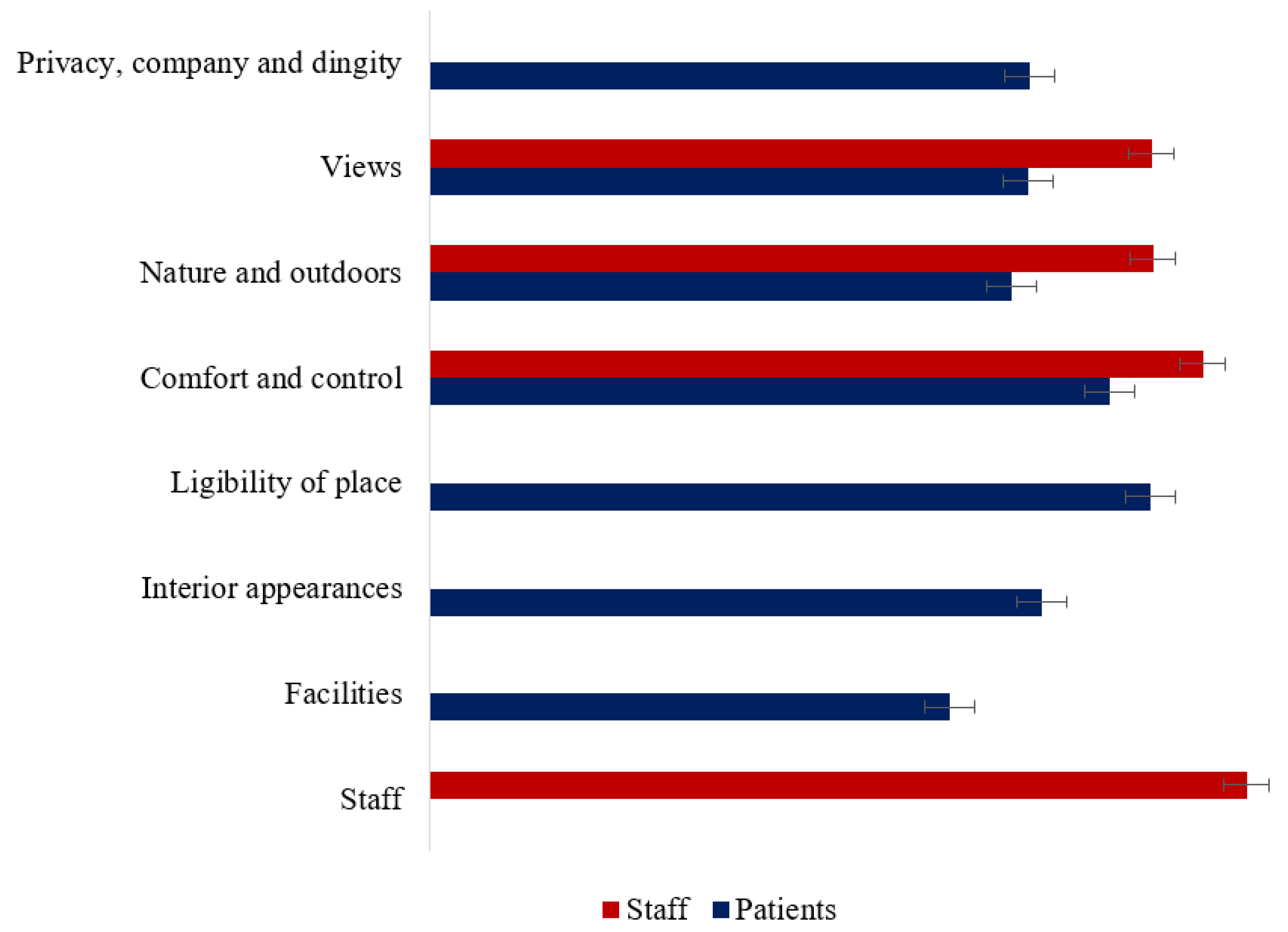
3.1. Healing Environment for Staff
3.2. Healing Environment for Patients
4. Discussion
5. Conclusions
6. Limitations of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jackson, L.E. The Relationship of Urban Design to Human Health and Condition. Landsc. Urban Plan. 2003, 64, 191–200. [Google Scholar] [CrossRef]
- Whitehouse, S.; Varni, J.W.; Seid, M.; Cooper-marcus, C.; Ensberg, M.J.; Jacobs, J.R.; Mehlenbeck, R.S. Evaluating a children’s hospital garden environment: Utilization and consumer satisfaction. J. Environ. Psychol. 2001, 21, 301–314. [Google Scholar] [CrossRef] [Green Version]
- Devlin, A.S.; Arneill, A.B. Health Care Environments and Patient Outcomes: A Review of the Literature. Environ. Behav. 2003, 35, 665–694. [Google Scholar] [CrossRef]
- Jin, L.J.; Lamster, I.B.; Greenspan, J.S.; Pitts, N.B.; Scully, C.; Warnakulasuriya, S. Global Burden of Oral Diseases: Emerging Concepts, Management and Interplay with Systemic Health. Oral Dis. 2016, 22, 609–619. [Google Scholar] [CrossRef]
- How Often do You Visit a Dentist? Available online: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/ddn-20191205-1 (accessed on 27 June 2022).
- Gallagher, J.E.; Hutchinson, L. Analysis of human resources for oral health globally: Inequitable distribution. Int. Dent. J. 2018, 68, 183–189. [Google Scholar] [CrossRef]
- Munson, B.; Vujicic, M. Projected Supply of Dentists in the United States, 2020–2040. Health Policy Institute Research Brief. American Dental Association. May 2021. Available online: https://www.ada.org/-/media/project/adaorganization/ada/ada-org/files/resources/research/hpi/hpibrief_0521_1.pdf (accessed on 27 June 2022).
- Dijkstra, K.; Pieterse, M.; Pruyn, A. Physical Environmental Stimuli That Turn Healthcare Facilities into Healing Environments through Psychologically Mediated Effects: Systematic Review. J. Adv. Nurs. 2006, 56, 166–181. [Google Scholar] [CrossRef]
- Zborowsky, T.; Kreitzer, M.J. Creating Optimal Healing Environments in a Health Care Setting. Minn. Med. 2008, 91, 35–38. [Google Scholar]
- Andrade, C.; Lima, M.L.; Fornara, F.; Bonaiuto, M. Users’ Views of Hospital Environmental Quality: Validation of the Perceived Hospital Environment Quality Indicators (PHEQIs). J. Environ. Psychol. 2012, 32, 97–111. [Google Scholar] [CrossRef]
- Aboulfotouh, A.K.; Tolba, O.; Ezzeldin, S. The Impact of Workspace Location and Indoor Environmental Quality on Employees’ Satisfaction within Office Buildings: A Case Study in Cairo. Indoor Built Environ. 2020, 31, 1420326X20944561. [Google Scholar] [CrossRef]
- Aalto, L.; Lappalainen, S.; Salonen, H.; Reijula, K. Usability Evaluation (IEQ Survey) in Hospital Buildings. Int. J. Workplace Health Manag. 2017, 10, 265–282. [Google Scholar] [CrossRef]
- Nimlyat, P.S.; Kandar, M.Z. Appraisal of Indoor Environmental Quality (IEQ) in Healthcare Facilities: A Literature Review. Sustain. Cities Soc. 2015, 17, 61–68. [Google Scholar] [CrossRef]
- Chaudhury, H.; Mahmood, A.; Valente, M. The Effect of Environmental Design on Reducing Nursing Errors and Increasing Efficiency in Acute Care Settings: A Review and Analysis of the Literature. Environ. Behav. 2009, 41, 755–786. [Google Scholar] [CrossRef]
- Gharaveis, A.; Hamilton, D.K.; Pati, D. The Impact of Environmental Design on Teamwork and Communication in Healthcare Facilities: A Systematic Literature Review. HERD 2018, 11, 119–137. [Google Scholar] [CrossRef] [Green Version]
- Huisman, E.R.C.M.; Morales, E.; van Hoof, J.; Kort, H.S.M. Healing Environment: A Review of the Impact of Physical Environmental Factors on Users. Build. Environ. 2012, 58, 70–80. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.; Zhu, Y.; Ouyang, Q.; Cao, B. A Study on the Effects of Thermal, Luminous, and Acoustic Environments on Indoor Environmental Comfort in Offices. Build. Environ. 2012, 49, 304–309. [Google Scholar] [CrossRef]
- Yasin, Y.M.; Kerr, M.S.; Wong, C.A.; Bélanger, C.H. Factors Affecting Nurses’ Job Satisfaction in Rural and Urban Acute Care Settings: A PRISMA Systematic Review. J. Adv. Nurs. 2020, 76, 963–979. [Google Scholar] [CrossRef] [Green Version]
- Hafeez, I.; Yingjun, Z.; Hafeez, S.; Mansoor, R.; Rehman, K.U. Impact of Workplace Environment on Employee Performance: Mediating Role of Employee Health. Bus. Manag. Econ. Eng. 2019, 17, 173–193. [Google Scholar] [CrossRef]
- Andriani, A.D.; Mulyana, D.; Dida, S.; Wahyudin, U. The Role of Healing Environment in Reducing the Stress of Patients with Non-Communicable Disease. J. Nat. Sci. Biol. Med. 2021, 12, 300–306. [Google Scholar] [CrossRef]
- Bernhardt, J.; Lipson-Smith, R.; Davis, A.; White, M.; Zeeman, H.; Pitt, N.; Shannon, M.; Crotty, M.; Churilov, L.; Elf, M. Why Hospital Design Matters: A Narrative Review of Built Environments Research Relevant to Stroke Care. Int. J. Stroke. 2022, 17, 370–377. [Google Scholar] [CrossRef]
- Fux-Noy, A.; Zohar, M.; Herzog, K.; Shmueli, A.; Halperson, E.; Moskovitz, M.; Ram, D. The Effect of the Waiting Room’s Environment on Level of Anxiety Experienced by Children Prior to Dental Treatment: A Case Control Study. BMC Oral Health 2019, 19, 294. [Google Scholar] [CrossRef] [Green Version]
- Panda, A.; Garg, I.; Shah, M. Children’s Preferences Concerning Ambiance of Dental Waiting Rooms. Eur. Arch. Paediatr. Dent. 2015, 16, 27–33. [Google Scholar] [CrossRef]
- Münevveroğlu, P.A.; Akgöl, B.B.; Erol, T. Assessment of the Feelings and Attitudes of Children towards Their Dentist and Their Association with Oral Health. ISRN Dent. 2014, 2014, 867234. [Google Scholar] [CrossRef]
- Alsarheed, M. Children’s Perception of Their Dentists. Eur. J. Dent. 2011, 5, 186–190. [Google Scholar] [CrossRef] [Green Version]
- Jayakaran, T.G.; Rekha, C.V.; Annamalai, S.; Baghkomeh, P.N.; Sharmin, D.D. Preferences and Choices of a Child Concerning the Environment in a Pediatric Dental Operatory. Dent. Res. J. (Isfahan) 2017, 14, 183–187. [Google Scholar] [CrossRef]
- Oliveira, L.B.; Massignan, C.; De Carvalho, R.M.; Savi, M.G.; Bolan, M.; Porporatti, A.L.; Luca Canto, G.D. Children’s Perceptions of Dentist’s Attire and Environment: A Systematic Review and Meta-Analysis. Int. J. Clin. Pediatr. Dent. 2020, 13, 700–716. [Google Scholar] [CrossRef]
- Asiri, R.S.M.; Ain, T.S.; Hunaif, A.M.A.; Alshehri, E.S.A.; Aldashnan, S.S.; Sahman, L.A.A.; Togoo, R.A. Children’s Perception of Dentist and Clinical Environment—An Observational Study. Saudi J. Health Sci. 2020, 9, 61. [Google Scholar] [CrossRef]
- Ierardo, G.; Vozza, I.; Luzzi, V.; Nardacci, G.; Brugnoletti, O.; Sfasciotti, G.L.; Polimeni, A. Healing Environment in Pediatric Dentistry: Strategies Adopted by “Sapienza” University of Rome. Senses Sci. 2017, 4, 338–342. [Google Scholar]
- Motalebi, G.; Vojdanzadeh, L. Effect of Physical Environmental of Medical Space in Reducing Patients’ Anxiety and Stress (Case Study: A Dental Office). Honar-Ha-Ye-Ziba Memary Va Shahrsazi 2015, 20, 35–46. [Google Scholar] [CrossRef]
- De Ruijter, R.A.G.; Stegenga, B.; Schaub, R.M.H.; Reneman, M.F.; Middel, B. Determinants of Physical and Mental Health Complaints in Dentists: A Systematic Review. Community Dent. Oral Epidemiol. 2015, 43, 86–96. [Google Scholar] [CrossRef] [Green Version]
- Jonker, D.; Rolander, B.; Balogh, I. Relation between Perceived and Measured Workload Obtained by Long-Term Inclinometry among Dentists. Appl. Erg. 2009, 40, 309–315. [Google Scholar] [CrossRef]
- Marklund, S.; Huang, K.; Zohouri, D.; Wahlström, J. Dentists Working Conditions—Factors Associated with Perceived Workload. Acta Odontol. Scand. 2021, 79, 296–301. [Google Scholar] [CrossRef]
- Biddiss, E.; Knibbe, T.J.; McPherson, A. The Effectiveness of Interventions Aimed at Reducing Anxiety in Health Care Waiting Spaces: A Systematic Review of Randomized and Nonrandomized Trials. Anesth. Analg. 2014, 119, 433–448. [Google Scholar] [CrossRef]
- Sarapultseva, M.; Hu, D.; Sarapultsev, A. SARS-CoV-2 Seropositivity among Dental Staff and the Role of Aspirating Systems. JDR Clin. Trans. Res. 2021, 6, 132–138. [Google Scholar] [CrossRef]
- Brambilla, A.; Capolongo, S. Healthy and Sustainable Hospital Evaluation—A Review of POE Tools for Hospital Assessment in an Evidence-Based Design Framework. Buildings 2019, 9, 76. [Google Scholar] [CrossRef] [Green Version]
- Department of Health. Achieving Excellence Design Evaluation Toolkit (AEDET Evolution) and A Staff and Patient Environment Calibration Tool (ASPECT). 2008. Available online: https://webarchive.nationalarchives.gov.uk (accessed on 4 February 2019).
- Amankwah, O.; Weng-Wai, C.; Mohammed, A.H. Modelling the Mediating Effect of Health Care Healing Environment on Core Health Care Delivery and Patient Satisfaction in Ghana. Env. Health Insights 2019, 13, 1178630219852115. [Google Scholar] [CrossRef]
- Sebba, R. The Landscapes of Childhood: The Reflection of Childhood’s Environment in Adult Memories and in Children’s Attitudes. Environ. Behav. 1991, 23, 395–422. [Google Scholar] [CrossRef]
- Van den Bogerd, N.; Dijkstra, S.C.; Seidell, J.C.; Maas, J. Greenery in the University Environment: Students’ Preferences and Perceived Restoration Likelihood. PLoS ONE 2018, 13, e0192429. [Google Scholar] [CrossRef]
- Holt, E.W.; Lombard, Q.K.; Best, N.; Smiley-Smith, S.; Quinn, J.E. Active and Passive Use of Green Space, Health, and Well-Being amongst University Students. Int. J. Env. Res. Public Health 2019, 16, 424. [Google Scholar] [CrossRef] [Green Version]
- Lawton, E.; Brymer, E.; Clough, P.; Denovan, A. The Relationship between the Physical Activity Environment, Nature Relatedness, Anxiety, and the Psychological Well-Being Benefits of Regular Exercisers. Front. Psychol. 2017, 8, 1058. [Google Scholar] [CrossRef] [Green Version]
- Ulrich, R.S.; Simons, R.F.; Losito, B.D.; Fiorito, E.; Miles, M.A.; Zelson, M. Stress Recovery during Exposure to Natural and Urban Environments. J. Environ. Psychol. 1991, 11, 201–230. [Google Scholar] [CrossRef]
- Devlin, A.S. Environmental Psychology and Human Well-Being: Effects of Built and Natural Settings; Academic Press: Cambridge, MA, USA, 2018; ISBN 978-0-12-811482-7. [Google Scholar]
- Chang, C.-H.; Chiao, Y.-C.; Tsai, Y. Identifying Competitive Strategies to Improve the Performance of Hospitals in a Competitive Environment. BMC Health Serv. Res. 2017, 17, 756. [Google Scholar] [CrossRef] [Green Version]
- Mosadeghrad, A.M. Factors Influencing Healthcare Service Quality. Int. J. Health Policy Manag. 2014, 3, 77–89. [Google Scholar] [CrossRef]
- Rimmer, A. Lack of Mental Health Support in the Public Sector. BMJ 2017, 357, j2731. [Google Scholar] [CrossRef]
- Andrade, C.C.; Devlin, A.S.; Pereira, C.R.; Lima, M.L. Do the Hospital Rooms Make a Difference for Patients’ Stress? A Multilevel Analysis of the Role of Perceived Control, Positive Distraction, and Social Support. J. Environ. Psychol. 2017, 53, 63–72. [Google Scholar] [CrossRef]
- Sharma, A.; Chhabra, K.G.; Bhandari, S.S.; Poddar, G.; Dany, S.S.; Chhabra, C.; Goyal, A. Emotional Well-Being of Dentists and the Effect of Lockdown during the COVID-19 Pandemic: A Nationwide Study. J. Educ. Health Promot. 2021, 10, 344. [Google Scholar] [CrossRef]
- Barthwal, P. A Comparative Study of Mental Health among Private and Public Sector Employees. Indian J. Health Wellbeing 2011, 2, 818–820. [Google Scholar]
- Ramstetter, L.; Habersack, F. Do Women Make a Difference? Analysing Environmental Attitudes and Actions of Members of the European Parliament. Environ. Politics 2020, 29, 1063–1084. [Google Scholar] [CrossRef]
- Wallhagen, M.; Eriksson, O.; Sörqvist, P. Gender Differences in Environmental Perspectives among Urban Design Professionals. Buildings 2018, 8, 59. [Google Scholar] [CrossRef] [Green Version]
- Mourshed, M.; Zhao, Y. Healthcare Providers’ Perception of Design Factors Related to Physical Environments in Hospitals. J. Environ. Psychol. 2012, 32, 362–370. [Google Scholar] [CrossRef] [Green Version]
- Ulrich, R.S. Effects of Interior Design on Wellness: Theory and Recent Scientific Research. J. Health Care Inter. Des. 1991, 3, 97–109. [Google Scholar]
- Ulrich, R.S.; Zimring, C.; Zhu, X.; DuBose, J.; Seo, H.-B.; Choi, Y.-S.; Quan, X.; Joseph, A. A Review of the Research Literature on Evidence-Based Healthcare Design. HERD 2008, 1, 61–125. [Google Scholar] [CrossRef]
- Ulrich, R.S. A Theory of Supportive Design for Healthcare Facilities. J. Healthc. Des. 1997, 9, 3–7; discussion 21–24. [Google Scholar]
- Bock, E.P.; Nilsson, S.; Jansson, P.-A.; Wijk, H.; Alexiou, E.; Lindahl, G.; Berghammer, M.; Degl’Innocenti, A. Literature Review: Evidence-Based Health Outcomes and Perceptions of the Built Environment in Pediatric Hospital Facilities. J. Pediatr. Nurs. Nurs. Care Child. Fam. 2021, 61, e42–e50. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Staff (n = 58) | Patients (n = 94) | |
|---|---|---|
| Age, mean (SD) | 39.57 (9.15) | 34.61 (8.59) |
| Sex | ||
| Male, n (%) | 8 (13.8) | 34 (36.2) |
| Female, n (%) | 50 (86.2) | 60 (63.8) |
| Clinic | ||
| Private, n (%) | 36 (62.1) | 43 (45.7) |
| State, n (%) | 22 (37.9) | 51 (54.3) |
| Experience, mean (SD) | 16.77 (8.92) | n/a |
| Work position | ||
| Dentist, n (%) | 18 (31) | n/a |
| Dentist assistant, n (%) | 12 (20.7) | n/a |
| Dental auxiliaries, n (%) | 28 (48.3) | n/a |
| Healing environment | ||
| Privacy, company, and dignity, mean (SD) | n/a | 3.72 (1.37) |
| Views, mean (SD) | 4.47 (0.70) | 3.71 (1.36) |
| Nature and outdoors, mean (SD) | 4.48 (0.91) | 3.60 (1.27) |
| Comfort and control, mean (SD) | 4.79 (0.88) | 4.21 (1.21) |
| Legibility of place, mean (SD) | n/a | 4.46 (1.10) |
| Interior appearances, mean (SD) | n/a | 3.79 (1.16) |
| Facilities, mean (SD) | n/a | 3.22 (1.16) |
| Staff, mean (SD) | 5.06 (0.98) | n/a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarapultseva, M.; Zolotareva, A.; Nasretdinova, N.; Sarapultsev, A. The Healing Environment of Dental Clinics through the Eyes of Patients and Healthcare Professionals: A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 13516. https://doi.org/10.3390/ijerph192013516
Sarapultseva M, Zolotareva A, Nasretdinova N, Sarapultsev A. The Healing Environment of Dental Clinics through the Eyes of Patients and Healthcare Professionals: A Pilot Study. International Journal of Environmental Research and Public Health. 2022; 19(20):13516. https://doi.org/10.3390/ijerph192013516
Chicago/Turabian StyleSarapultseva, Maria, Alena Zolotareva, Natal’ya Nasretdinova, and Alexey Sarapultsev. 2022. "The Healing Environment of Dental Clinics through the Eyes of Patients and Healthcare Professionals: A Pilot Study" International Journal of Environmental Research and Public Health 19, no. 20: 13516. https://doi.org/10.3390/ijerph192013516
APA StyleSarapultseva, M., Zolotareva, A., Nasretdinova, N., & Sarapultsev, A. (2022). The Healing Environment of Dental Clinics through the Eyes of Patients and Healthcare Professionals: A Pilot Study. International Journal of Environmental Research and Public Health, 19(20), 13516. https://doi.org/10.3390/ijerph192013516