

Analysis of Hospitalization Costs in Patients Suffering from Cerebral Infarction along with Varied Comorbidities

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
- (1)
- According to the International Classification of Diseases, patients with the primary diagnostic disease code I63.900 were included.
- (1)
- Total hospitalization cost was zero;
- (2)
- Data were missing or incorrect (which could not be corrected);
- (3)
- Length of hospital stay was less than 1 day or more than 60 days.
2.2. Variables Extracted
- (1)
- Basic inpatient information: gender, age, ethnicity, marital status, hospital level, and the patient’s chosen medical payment method;
- (2)
- Clinical information: discharge diagnosis, history of comorbidities, length of hospital stay, discharge and admission dates, and operation status;
- (3)
- Information relating to medical costs: total hospitalization costs, drug costs, diagnosis costs, treatment costs, costs of medical consumables, medical service costs, rehabilitation costs, and other costs.
2.3. Statistical Analysis
3. Results
3.1. Basic Information of Inpatients
3.2. Association between Hospitalization Costs and the Number of Comorbidities
3.3. The Status of Hospitalization Costs in Different Types of Comorbidity
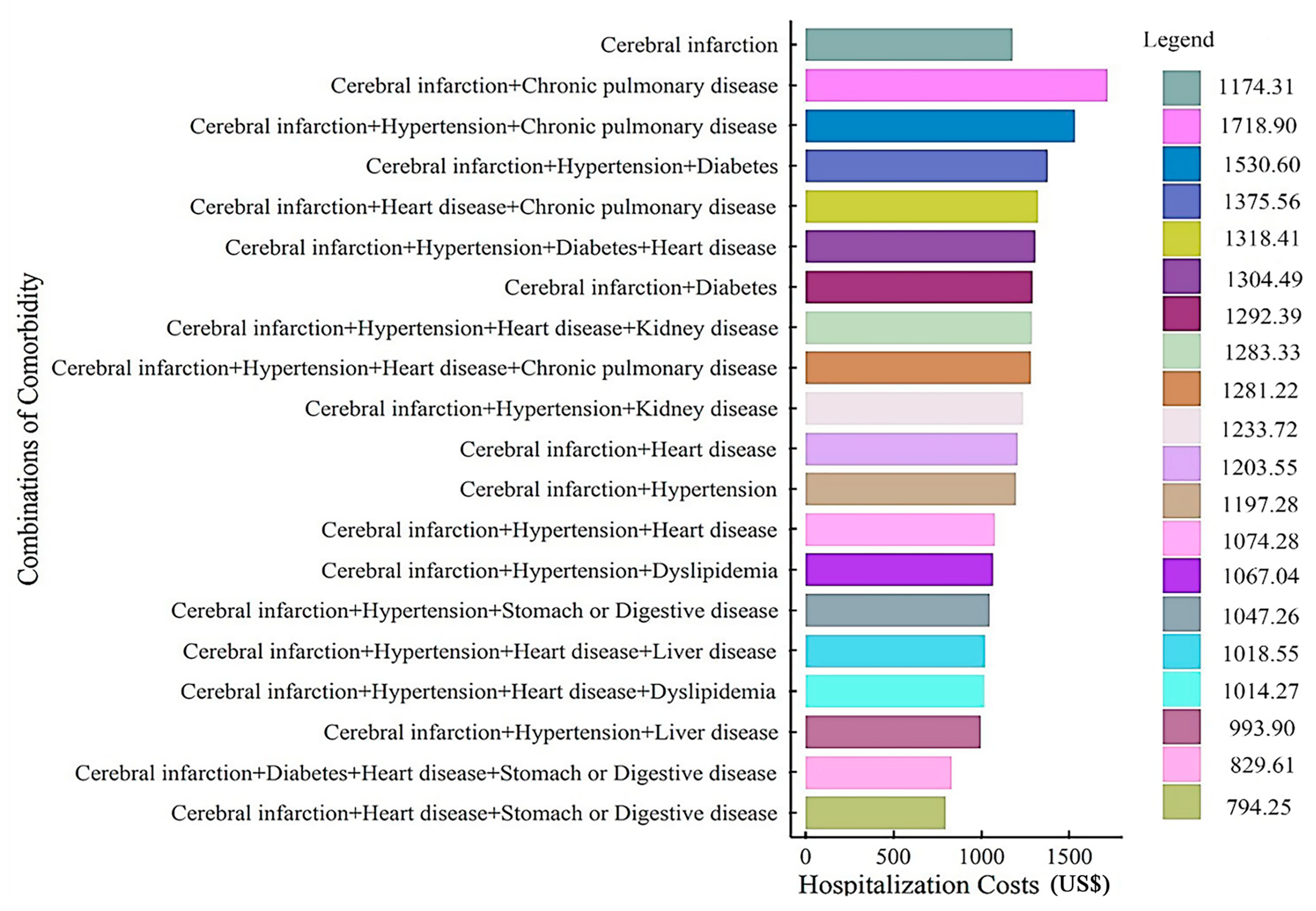
3.4. The Status of Hospitalization Costs in Different Combinations of Comorbidities
3.5. Multiple Linear Regression Analysis of the Impacts of Comorbidities on Hospitalization Costs for Cerebral Infarction Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, J.Y.; Li, J.W.; Zhang, L.H.; Wang, Y.Y.; Mei, J.J.; Guo, J.; Li, R.Q. Research progress of Chinese medicine regulating PI3K/AKT signaling pathway to improve ischemic stroke. Chin. J. Exp. Tradit. Med. Formulae 2022, 28, 265–275. [Google Scholar] [CrossRef]
- Paul, S.; Candelario, J.E. Emerging neuroprotective strategies for the treatment of ischemic stroke: An overview of clinical and preclinical studies. Exp. Neurol. 2021, 335, 113518. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The World Health Report 2008: Primary Health Care Now More than Ever; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Xu, X.B.; Li, D.; Sun, Y.; Shu, Q.; Xiao, L.; Xu, S.R.; Hu, S.; Jiang, Y.S.; Xin, Y.J. Analysis of chronic diseases comorbidity among the elderly in China based on association rules. Chin. J. Prev. Control Chronic Dis. 2021, 29, 808–812. [Google Scholar]
- Cipolla, M.J.; Liebeskind, D.S.; Chan, S.L. The importance of comorbidities in ischemic stroke: Impact of hypertension on the cerebral circulation. J. Cereb. Blood Flow Metab. 2018, 38, 2129–2149. [Google Scholar] [CrossRef]
- Lapchak, P.A.; Zhang, J.H. The High Cost of Stroke and Stroke Cytoprotection Research. Transl. Stroke Res. 2017, 8, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Dong, J.; Zhu, J.; Zhang, R.H.; Tang, M.L.; Shu, Y.; He, W. Analysis on the composition and influencing factors of hospitalization costs for cerebral infarction patients in a tertiary hospital from 2007 to 2011. Chin. J. Health Stat. 2014, 31, 707–709. [Google Scholar]
- Zou, S.; Wang, Z.; Bhura, M.; Zhang, G.; Tang, K. Prevalence and associated socioeconomic factors of multimorbidity in 10 regions of China: An analysis of 0.5 million adults. J. Public Health 2022, 44, 36–50. [Google Scholar] [CrossRef]
- National Bureau of Statistics. Available online: http://www.stats.gov.cn/tjsj/zxfb/202102/t20210227_1814154.html (accessed on 16 August 2020).
- Wang, P.; Sun, Y.; Yi, D.; Xie, Y.; Luo, Y. Clinical features of Chinese patients in different age groups with spontaneous intracerebral hemorrhage based on multicenter inpatient information. Neurol. Res. 2020, 42, 657–664. [Google Scholar] [CrossRef]
- Rosales, J.S.; Alet, M.J.; Lereis, V.A.P.; Ameriso, S.F. Fall in the Proportion of Atherothrombotic Strokes during the Last Decade. J. Stroke Cerebrovasc. Dis. 2020, 29, 105257. [Google Scholar] [CrossRef]
- Gallacher, K.I.; Jani, B.D.; Hanlon, P.; Nicholl, B.I.; Mair, F.S. Multimorbidity in Stroke. Stroke 2019, 50, 1919–1926. [Google Scholar] [CrossRef] [Green Version]
- Yu, B.Q.; Tian, X.; Zhou, S.N.; Wu, S.; Liu, H. Related factors for pulmonary infections in acute stoke patients. Chin. J. Nosocomiol. 2015, 25, 3965–3966+3978. [Google Scholar]
- Chen, B.; Dai, H.E.; Chen, L.X. The Value of Inflammatory Mechanism in Chronic Obstructive Pulmonary Disease with Ischemic Stroke. Shenzhen J. Integr. Tradit. Chin. West. Med. 2019, 29, 5–7. [Google Scholar]
- Wang, H.; Li, S.L.; Bai, J.; Wang, D.X. Perioperative Acute Ischemic Stroke Increases Mortality after Noncardiac, Nonvascular, and Non-Neurologic Surgery: A Retrospective Case Series. J. Cardiothorac. Vasc. Anesth. 2019, 33, 2231–2236. [Google Scholar] [CrossRef] [PubMed]
- Chamorro, A.; Amaro, S.; Vargas, M.; Obach, V.; Cervera, A.; Gómez-Choco, M.; Torres, F.; Planas, A.M. Catecholamines, infection, and death in acute ischemic stroke. J. Neurol. Sci. 2007, 252, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Ding, C.Y.; Wang, X.Y.; Luo, G.C.; Chen, H. Association of peripheral blood NLRP3 inflammasome gene polymorphisms with pulmonary infection in patients with ischemic stroke. Chin. J. Nosocomiol. 2021, 31, 1634–1638. [Google Scholar]
- Babore, A.D.; Tybjerg, A.J.; Andersen, K.K.; Olsen, T.S. Occult lung cancer manifesting within the first year after stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 105023. [Google Scholar] [CrossRef]
- Wolff, J.L.; Starfield, B.; Anderson, G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch. Intern. Med. 2002, 162, 2269–2276. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.S.; Li, S. Studying the influence of comorbidity on the number of outpatient visits, length of hospitalization, and catastrophic health expenditure. Chin. J. Health Policy 2021, 14, 17–24. [Google Scholar]
- Cortaredona, S.; Ventelou, B. The extra cost of comorbidity: Multiple illnesses and the economic burden of non-communicable diseases. BMC Med. 2017, 15, 216. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.E.; Charlson, R.E.; Peterson, J.C.; Marinopoulos, S.S.; Briggs, W.M.; Hollenberg, J.P. The Charlson comorbidity index is adapted to predict costs of chronic disease in primary care patients. J. Clin. Epidemiol. 2008, 61, 1234–1240. [Google Scholar] [CrossRef]
- State Council: More than 50% reimbursement of outpatient medication for hypertension and diabetes under medical insurance. For Your Health 2019, 10, 2.
- Xu, M.M.; Liu, D.; Yang, C.Y. Study on the effect of implementing basic medical insurance+critical illness insurance in Rural areas of China—A case study of hospitalized farmers with heart disease in Men Tou Gou District, Beijing. Price Theory Pract. 2020, 4, 112–115+178. [Google Scholar]
- Lou, P.A.; Yu, J.X.; Zhang, L.; Zhang, N.; Chen, P.P.; Zhang, L.; Han, L.C. Analysis on economic burden of COPD patients in Tongshan County. Chin. J. Dis. Control Prev. 2010, 14, 1129–1131. [Google Scholar]
- Dal Negro, R.; Berto, P.; Tognella, S.; Quareni, L.; Global Outcomes in Lung Disease Study Group. Cost-of-illness of lung disease in the TriVeneto Region, Italy: The GOLD Study. Monaldi Arch. Chest Dis. 2002, 57, 3–9. [Google Scholar]
- Lakshminarayan, K.; Tsai, A.W.; Tong, X.; Vazquez, G.; Peacock, J.M.; George, M.G.; Luepker, R.V.; Anderson, D. Utility of dysphagia screening results in predicting poststroke pneumonia. Stroke 2010, 41, 2849–2854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katzan, I.L.; Cebul, R.D.; Husak, S.H.; Dawson, N.V.; Baker, D.W. The effect of pneumonia on mortality among patients hospitalized for acute stroke. Neurology 2003, 60, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Yuan, M.Z.; Li, F.; Tian, X.; Wang, W.; Jia, M.; Wang, X.F.; Liu, G.W. Risk factors for lung infection in stroke patients: A meta-analysis of observational studies. Expert Rev. Anti Infect. Ther. 2015, 13, 1289–1298. [Google Scholar] [CrossRef]
- Khor, Y.H.; Glaspole, I.; Goh, N.S.L. Therapeutic burden in interstitial lung disease: Lessons to learn. Respirology 2019, 24, 566–571. [Google Scholar] [CrossRef]


{kind=link}
| Variable | No Comorbidity Group | Comorbidity Group | Total | χ2 | p |
|---|---|---|---|---|---|
| Gender | 0.023 | <0.001 | |||
| Male | 7088 (9.26) | 34,312 (44.82) | 41,400 (54.08) | ||
| Female | 5431 (7.09) | 29,732 (38.83) | 35,163 (45.92) | ||
| Age, years | 0.080 | <0.001 | |||
| 19 | 273 (0.36) | 746 (0.97) | 1019 (1.33) | ||
| 40 | 3684 (4.81) | 13,896 (18.15) | 17,580 (22.96) | ||
| 60 | 7636 (9.97) | 42,655 (55.72) | 50,291 (65.69) | ||
| 80 | 926 (1.21) | 6747 (8.81) | 7673 (10.02) | ||
| Ethnicity | −0.036 | <0.001 | |||
| Han | 11,539 (15.07) | 60,504 (79.03) | 72,043 (94.10) | ||
| Ethnic minorities | 980 (1.28) | 3540 (4.62) | 4520 (5.90) | ||
| Marital status | 0.030 | <0.001 | |||
| Unmarried | 1945 (2.54) | 8955 (11.70) | 10,900 (14.24) | ||
| Married | 10,310 (13.47) | 52,637 (68.75) | 62,947 (82.22) | ||
| Divorced/widowed | 264 (0.34) | 2452 (3.20) | 2716 (3.54) | ||
| Hospital level | 0.198 | <0.001 | |||
| First-level hospital | 897 (1.17) | 1279 (1.67) | 2176 (2.84) | ||
| Secondary hospital | 8019 (10.47) | 28,663 (37.44) | 36,682 (47.91) | ||
| Tertiary hospital | 3603 (4.71) | 34,102 (44.54) | 37,705 (49.25) | ||
| Total | 12,519 (16.35) | 64,044 (83.65) | 76,563 (100.00) | ||
| Number of Comorbidities | Hospitalization Costs | Drug Costs | Diagnosis Costs | Treatment Costs | Medical Consumables Costs | Medical Service Costs | Nursing Costs | Rehabilitation Costs | Other Costs |
|---|---|---|---|---|---|---|---|---|---|
| 0 (n = 12,519) | 1174.31 | 352.88 | 314.30 | 188.61 | 115.76 | 67.00 | 46.37 | 66.36 | 23.02 |
| 1 (n = 21,614) | 1224.41 | 398.26 | 338.22 | 176.28 | 115.12 | 90.59 | 60.43 | 40.92 | 4.58 |
| 2 (n = 23,146) | 1237.90 | 402.38 | 330.07 | 180.70 | 139.68 | 85.88 | 58.31 | 33.21 | 7.69 |
| 3 (n = 16,014) | 1247.30 | 393.84 | 364.97 | 169.61 | 120.55 | 91.14 | 59.12 | 45.47 | 2.59 |
| ≥4 (n = 3270) | 1322.27 | 414.56 | 395.28 | 188.15 | 114.46 | 89.65 | 66.36 | 50.83 | 2.98 |
| Total | 1219.66 | 391.77 | 340.04 | 178.66 | 123.27 | 85.48 | 57.51 | 37.19 | 5.74 |
| H | 404.506 | 153.385 | 491.911 | 55.347 | 26.427 | 1236.598 | 427.936 | 258.721 | 379.125 |
| p | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Type of Comorbidity | n | Drug Costs | Treatment Costs | Diagnosis Costs | Material Costs | Medical Service Costs | Nursing Costs | Rehabilitation Costs | Other Costs | Hospitalization Costs | Rank |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cancer | 3253 | 576.05 | 316.59 | 468.05 | 306.84 | 113.42 | 88.74 | 60.05 | 4.28 | 1934.02 | 1 |
| Chronic pulmonary disease | 12,055 | 503.90 | 224.60 | 410.02 | 144.62 | 102.97 | 96.29 | 46.06 | 4.57 | 1533.02 | 2 |
| Asthma | 412 | 508.30 | 225.25 | 445.58 | 118.64 | 96.88 | 68.01 | 23.88 | 1.69 | 1488.22 | 3 |
| Memory-related disease | 1557 | 482.22 | 170.17 | 383.08 | 103.72 | 98.66 | 112.97 | 84.69 | 3.51 | 1439.01 | 4 |
| Diabetes | 11,642 | 439.92 | 196.73 | 409.36 | 127.19 | 84.87 | 65.40 | 62.03 | 5.82 | 1391.31 | 5 |
| Kidney disease | 6719 | 418.68 | 184.62 | 402.24 | 96.40 | 96.74 | 67.21 | 64.14 | 2.32 | 1332.36 | 6 |
| Arthritis or rheumatism disease | 1815 | 346.40 | 204.91 | 316.20 | 186.24 | 91.63 | 46.99 | 29.42 | 2.56 | 1224.34 | 7 |
| Hypertension | 45,626 | 394.25 | 172.19 | 339.44 | 116.05 | 87.12 | 56.28 | 41.12 | 5.82 | 1212.28 | 8 |
| Heart disease | 27,646 | 370.42 | 156.70 | 329.04 | 136.28 | 85.60 | 52.67 | 32.31 | 2.43 | 1165.44 | 9 |
| Liver disease | 7436 | 362.28 | 142.46 | 361.92 | 68.73 | 85.32 | 53.59 | 55.08 | 2.27 | 1131.64 | 10 |
| Dyslipidemia | 5565 | 342.61 | 152.28 | 336.93 | 64.16 | 75.24 | 35.24 | 34.32 | 2.50 | 1043.28 | 11 |
| Stomach or digestive disease | 6826 | 319.16 | 138.54 | 285.17 | 91.57 | 93.86 | 47.74 | 26.20 | 2.50 | 1004.73 | 12 |
| Emotional and psychiatric disorders | 2951 | 274.97 | 130.63 | 284.34 | 52.47 | 122.38 | 45.02 | 28.72 | 1.60 | 940.12 | 13 |
| Variable | Hospitalization Costs | Drug Costs | Diagnosis Costs | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Beta | t | 95% CI | Beta | t | 95% CI | Beta | t | 95% CI | ||||
| (Constant) | 7.356 ** | 504.918 | 7.385 | 7.328 | 5.685 ** | 244.702 | 5.731 | 5.640 | 6.860 ** | 365.512 | 6.896 | 6.823 |
| Gender (Ref. = female) | −0.048 ** | −12.684 | −0.041 | −0.056 | −0.057 ** | −9.398 | −0.045 | −0.069 | −0.029 ** | −5.891 | −0.019 | −0.039 |
| Age (Ref. = 60) | ||||||||||||
| 19 | 0.148 ** | 8.985 | 0.180 | 0.115 | −0.014 | −0.551 | 0.037 | −0.065 | 0.073 * | 3.462 | 0.115 | 0.032 |
| 40 | 0.022 ** | 4.790 | 0.031 | 0.013 | 0.007 | 0.987 | 0.022 | −0.007 | −0.001 | −0.182 | 0.011 | −0.013 |
| 80 | 0.050 ** | 7.822 | 0.063 | 0.038 | 0.073 ** | 7.131 | 0.093 | 0.053 | 0.053 ** | 6.290 | 0.069 | 0.036 |
| LN length of hospital stay | 0.535 ** | 129.207 | 0.543 | 0.527 | 0.822 ** | 122.883 | 0.835 | 0.809 | 0.163 ** | 30.466 | 0.174 | 0.153 |
| Hospital level (Ref. = Tertiary hospital) | ||||||||||||
| First-level hospital | −0.042 ** | −3.771 | −0.020 | −0.064 | −0.042 * | −2.313 | −0.006 | −0.078 | −0.109 ** | −7.446 | −0.081 | −0.138 |
| Secondary hospital | 0.466 ** | 116.274 | 0.474 | 0.458 | 0.405 ** | 63.806 | 0.417 | 0.392 | 0.586 ** | 113.117 | 0.596 | 0.575 |
| Payment (Ref. = medical insurance) | ||||||||||||
| Public expense | 0.029 * | 3.003 | 0.047 | 0.010 | −0.124 ** | −8.304 | −0.095 | −0.154 | 0.044 ** | 3.641 | 0.068 | 0.020 |
| Out-of-pocket | 0.225 ** | 16.228 | 0.252 | 0.197 | 0.125 ** | 5.708 | 0.167 | 0.082 | 0.189 ** | 10.602 | 0.224 | 0.154 |
| Other | 0.067 ** | 4.234 | 0.099 | 0.036 | −0.156 ** | −6.215 | −0.107 | −0.205 | 0.014 | 0.693 | 0.055 | −0.026 |
| Type of comorbidity (Ref. = cerebral infarction) | ||||||||||||
| Hypertension | −0.040 ** | −10.292 | −0.033 | −0.048 | −0.025 ** | −3.954 | −0.012 | −0.037 | −0.077 ** | −15.205 | −0.067 | −0.087 |
| Diabetes | 0.069 ** | 12.976 | 0.080 | 0.059 | 0.003 | 0.402 | 0.020 | −0.013 | 0.143 ** | 20.612 | 0.156 | 0.129 |
| Heart disease | −0.025 ** | −6.230 | −0.017 | −0.033 | 0.041 ** | 6.295 | 0.054 | 0.028 | −0.029 ** | −5.482 | −0.019 | −0.039 |
| Emotional and psychiatric disorders | −0.096 ** | −9.710 | −0.077 | −0.116 | −0.370 ** | −23.669 | −0.340 | −0.401 | −0.149 ** | −11.670 | −0.124 | −0.174 |
| Chronic pulmonary disease | 0.181 ** | 33.911 | 0.191 | 0.170 | 0.144 ** | 16.927 | 0.160 | 0.127 | 0.171 ** | 24.726 | 0.184 | 0.157 |
| Stomach or digestive disease | −0.096 ** | −14.217 | −0.083 | −0.109 | −0.070 ** | −6.448 | −0.049 | −0.092 | −0.108 ** | −12.417 | −0.091 | −0.125 |
| Liver disease | −0.041 ** | −6.198 | −0.028 | −0.053 | −0.110 ** | −10.565 | −0.089 | −0.130 | 0.074 ** | 8.675 | 0.091 | 0.057 |
| Kidney disease | 0.023 * | 3.363 | 0.036 | 0.010 | −0.017 | −1.592 | 0.004 | −0.039 | 0.119 ** | 13.346 | 0.137 | 0.102 |
| Asthma | 0.053 * | 2.016 | 0.104 | 0.001 | 0.132 * | 3.196 | 0.213 | 0.051 | 0.105 * | 3.124 | 0.170 | 0.039 |
| Arthritis or rheumatic disease | 0.012 | 0.928 | 0.036 | −0.013 | −0.084 ** | −4.252 | −0.045 | −0.123 | −0.056 * | −3.462 | −0.024 | −0.087 |
| Memory-related diseases | −0.019 | −1.455 | 0.007 | −0.045 | −0.003 | −0.122 | 0.039 | −0.044 | −0.030 | −1.720 | 0.004 | −0.064 |
| Cancer | 0.156 ** | 16.552 | 0.174 | 0.137 | 0.135 ** | 9.081 | 0.164 | 0.106 | 0.141 ** | 11.589 | 0.165 | 0.117 |
| Dyslipidemia | −0.057 ** | −7.878 | −0.043 | −0.071 | −0.065 ** | −5.690 | −0.043 | −0.088 | 0.035 ** | 3.741 | 0.053 | 0.017 |
| R2 | 0.371 | 0.258 | 0.230 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, Y.; Chen, S.; Chen, Y. Analysis of Hospitalization Costs in Patients Suffering from Cerebral Infarction along with Varied Comorbidities. Int. J. Environ. Res. Public Health 2022, 19, 15053. https://doi.org/10.3390/ijerph192215053
He Y, Chen S, Chen Y. Analysis of Hospitalization Costs in Patients Suffering from Cerebral Infarction along with Varied Comorbidities. International Journal of Environmental Research and Public Health. 2022; 19(22):15053. https://doi.org/10.3390/ijerph192215053
Chicago/Turabian StyleHe, Yongmei, Sixuan Chen, and Yongcong Chen. 2022. "Analysis of Hospitalization Costs in Patients Suffering from Cerebral Infarction along with Varied Comorbidities" International Journal of Environmental Research and Public Health 19, no. 22: 15053. https://doi.org/10.3390/ijerph192215053
APA StyleHe, Y., Chen, S., & Chen, Y. (2022). Analysis of Hospitalization Costs in Patients Suffering from Cerebral Infarction along with Varied Comorbidities. International Journal of Environmental Research and Public Health, 19(22), 15053. https://doi.org/10.3390/ijerph192215053