


A Recreational Swimming Intervention during the Whole School Year Improves Fitness and Cardiometabolic Risk in Children and Adolescents with Overweight and Obesity
Abstract
:1. Introduction
2. Materials and Methods
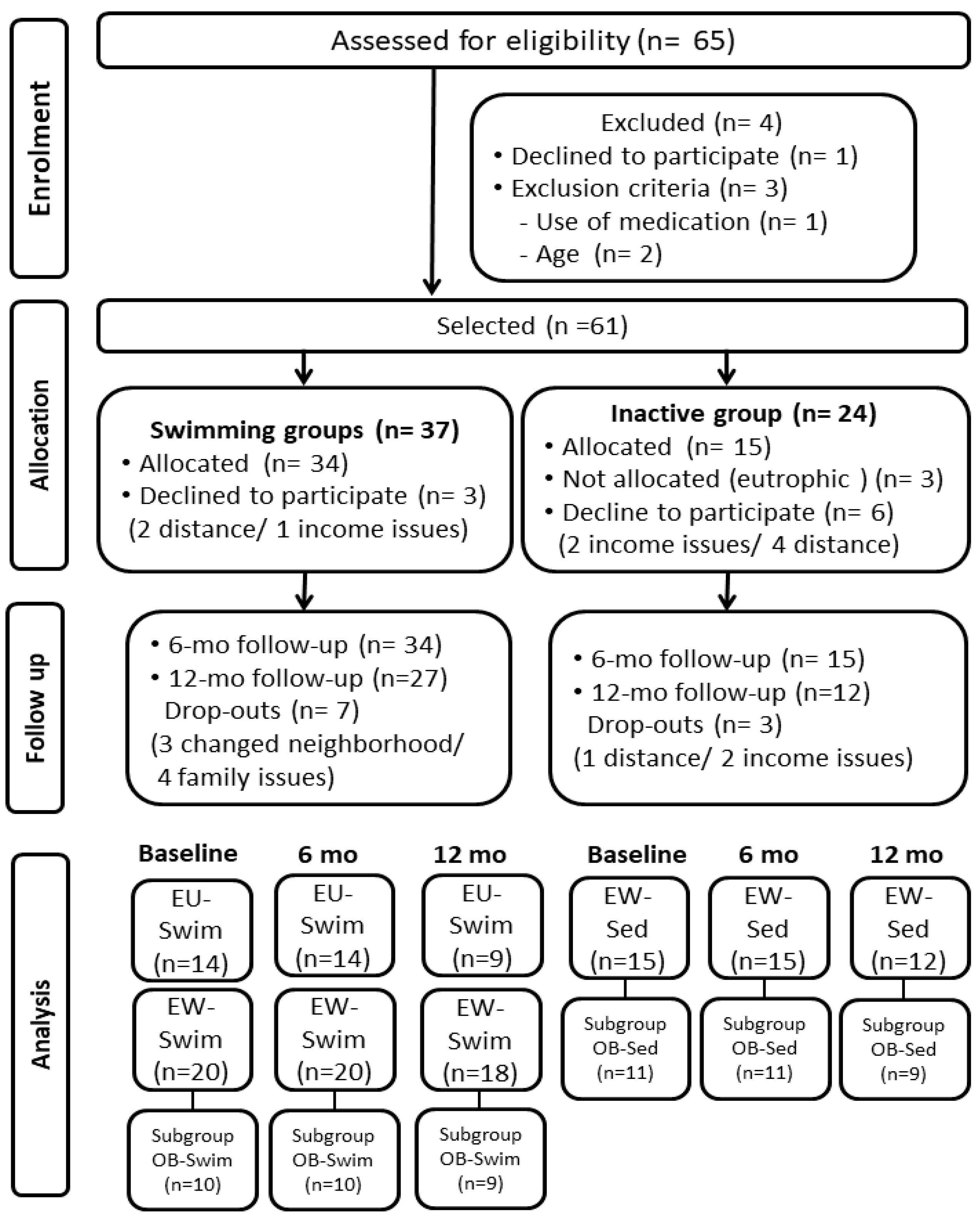
2.1. Subjects
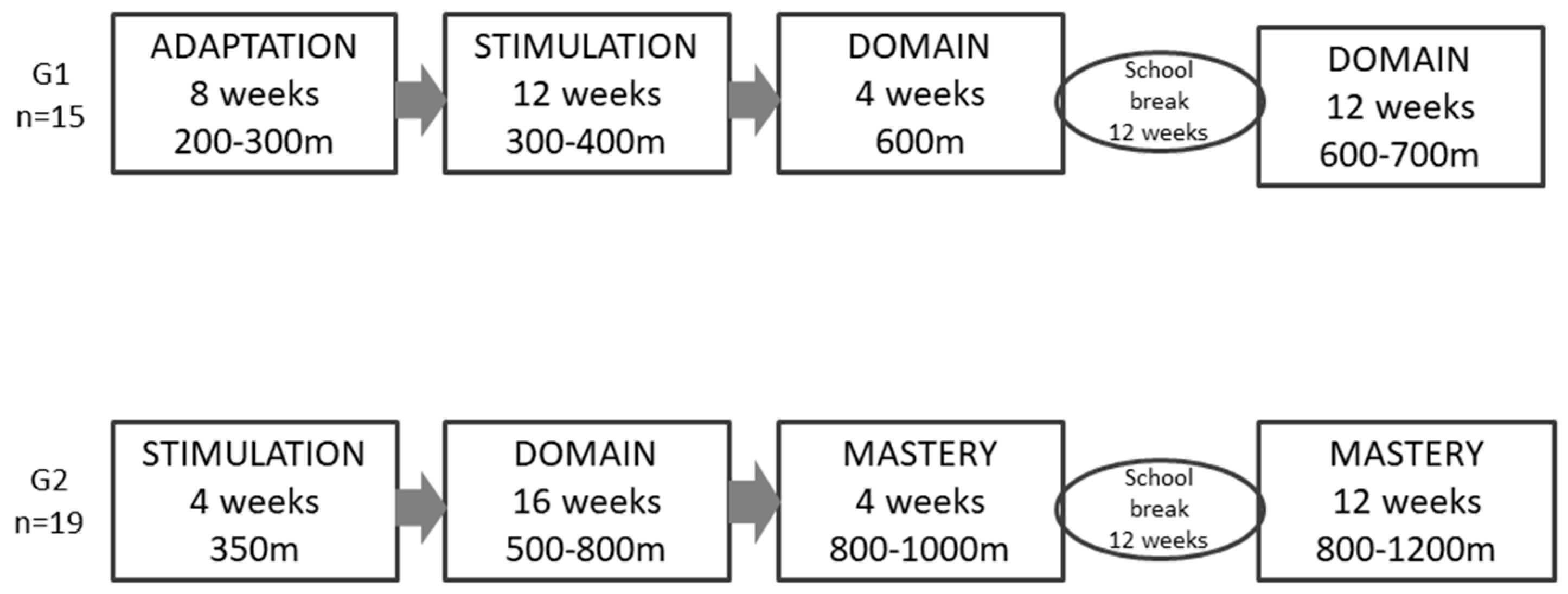
2.2. Experimental Design
2.3. Clinical and Anthropometric Outcomes
2.4. Physical Activity Level and Cardiorespiratory Fitness
2.5. Biochemical Analysis
2.6. Blood Pressure, Peripheral Arterial Tonometry, Venous Occlusion Plethysmography, and Heart Rate Variability
2.7. Ultrasound Assessments
2.8. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lambourne, K.; Donnelly, J.E. The role of physical activity in pediatric obesity. Pediatr. Clin. 2011, 58, 1481–1491. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; McAuley, P.; Lavie, C.J.; Despres, J.P.; Arena, R.; Kokkinos, P. Physical Activity and Cardiorespiratory Fitness as Major Markers of Cardiovascular Risk: Their Independent and Interwoven Importance to Health Status. Prog. Cardiovasc. Dis. 2015, 57, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Telama, R. Tracking of physical activity from childhood to adulthood: A review. Obes. Facts 2009, 2, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Venn, A.J.; Thomson, R.J.; Schmidt, M.D.; Cleland, V.J.; Curry, B.A.; Gennat, H.C.; Dwyer, T. Overweight and obesity from childhood to adulthood: A follow-up of participants in the 1985 Australian Schools Health and Fitness Survey. Med. J. Aust. 2007, 186, 458–460. [Google Scholar] [CrossRef] [PubMed]
- Geserick, M.; Vogel, M.; Gausche, R.; Lipek, T.; Spielau, U.; Keller, E.; Pfäffle, R.; Kiess, W.; Körner, A. Acceleration of BMI in Early Childhood and Risk of Sustained Obesity. N. Engl. J. Med. 2018, 379, 1303–1312. [Google Scholar] [CrossRef]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.; Martin, B.W.; Lancet Physical Activity Series Working Group. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Alberga, A.S.; Sigal, R.J.; Sweet, S.N.; Doucette, S.; Russell-Mayhew, S.; Tulloch, H.; Kenny, G.P.; Prud'homme, D.; Hadjiyannakis, S.; Goldfield, G.S. Understanding low adherence to an exercise program for adolescents with obesity: The HEARTY trial. Obes. Sci. Pract. 2019, 5, 437–448. [Google Scholar] [CrossRef] [Green Version]
- Stankov, I.; Olds, T.; Cargo, M. Overweight and obese adolescents: What turns them off physical activity? Int. J. Behav. Nutr. Phys. Act. 2012, 9, 53. [Google Scholar] [CrossRef] [Green Version]
- Vasconcellos, F.; Seabra, A.; Katzmarzyk, P.T.; Kraemer-Aguiar, L.G.; Bouskela, E.; Farinatti, P. Physical activity in overweight and obese adolescents: Systematic review of the effects on physical fitness components and cardiovascular risk factors. Sport. Med. 2014, 44, 1139–1152. [Google Scholar] [CrossRef]
- Vasconcellos, F.; Seabra, A.; Katzmarzyk, P.T.; Kraemer-Aguiar, L.G.; Bouskela, E.; Farinatti, P. Health markers in obese adolescents improved by a 12-week recreational soccer program: A randomised controlled trial. J. Sport. Sci. 2016, 34, 564–575. [Google Scholar] [CrossRef]
- Brasil, I.; Monteiro, W.; Lima, T.; Seabra, A.; Farinatti, P. Effects of judo training upon body composition, autonomic function, and cardiorespiratory fitness in overweight or obese children aged 8- to 13 years. J. Sport. Sci. 2020, 38, 2508–2516. [Google Scholar] [CrossRef] [PubMed]
- Chase, N.L.; Sui, X.; Blair, S.N. Comparison of the Health Aspects of Swimming with Other Types of Physical Activity and Sedentary Lifestyle Habits. Int. J. Aquat. Res. Educ. 2008, 2, 7. [Google Scholar] [CrossRef] [Green Version]
- Oral, O. Effects of Aquatic Exercise in the Treatment of Obesity. Biomed. J. Sci. Tech. Res. 2021, 33, 25423–25426. [Google Scholar] [CrossRef]
- Pharr, J.; Irwin, C.; Layne, T.; Irwin, R. Predictors of swimming ability among children and adolescents in the United States. Sports 2018, 6, 17. [Google Scholar] [CrossRef] [Green Version]
- Lee, B.-A.; Oh, D.-J. The effects of aquatic exercise on body composition, physical fitness, and vascular compliance of obese elementary students. J. Exerc. Rehabil. 2014, 10, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Onis, M.D.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Tanner, J.M. Growth at Adolescence: With a General Consideration of the Effects of Hereditary and Environmental Factors upon Growth and Maturation from Birth to Maturity, 2nd ed.; Blackwell Scientific Publications: Oxford, UK, 1962; 325p. [Google Scholar]
- Burke, J.P.; Hale, D.E.; Hazuda, H.P.; Stern, M.P. A quantitative scale of acanthosis nigricans. Diabetes Care 1999, 22, 1655–1659. [Google Scholar] [CrossRef] [PubMed]
- Guedes, D.P.; Guedes, J.E.R.P. Medida da atividade física em jovens brasileiros: Reprodutibilidade e validade do PAQ-C e do PAQ-A. Rev. Bras. Med. Esporte 2015, 21, 425–432. [Google Scholar] [CrossRef] [Green Version]
- Crocker, P.R.; Bailey, D.A.; Faulkner, R.A.; Kowalski, K.C.; McGrath, R. Measuring general levels of physical activity: Preliminary evidence for the physical activity questionnaire for older children. Med. Sci. Sports Exerc. 1997, 29, 1344–1349. [Google Scholar] [CrossRef]
- Malina, R.M.; Eisenmann, J.C.; Cumming, S.P.; Ribeiro, B.; Aroso, J. Maturity-associated variation in the growth and functional capacities of youth football (soccer) players 13–15 years. Eur. J. Appl. Physiol. 2004, 91, 555–562. [Google Scholar] [CrossRef]
- Sociedade Brasileira de Pediatria—Departamento de Nutrologia. Obesidade na infância e adolescência. In Manual de Orientação/Sociedade Brasileira de Pediatria. Departamento Científico de Nutrologia, 3rd ed.; SBP: São Paulo, Brazil, 2019; 236p. [Google Scholar]
- Flynn, J.T.; Falkner, B.E. New clinical practice guideline for the management of high blood pressure in children and adolescents. Hypertension 2017, 70, 683–686. [Google Scholar] [CrossRef] [PubMed]
- Tierney, E.S.S.; Newburger, J.W.; Gauvreau, K.; Geva, J.; Coogan, E.; Colan, S.D.; de Ferranti, S.D. Endothelial Pulse Amplitude Testing: Feasibility and Reproducibility in Adolescents. J. Pediatr. 2009, 154, 901–905. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, I.B.; Webb, D.J. Venous occlusion plethysmography in cardiovascular research: Methodology and clinical applications. Br. J. Clin. Pharmacol. 2001, 52, 631–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erre, G.L.; Piga, M.; Fedele, A.L.; Mura, S.; Piras, A.; Cadoni, M.L.; Cangemi, I.; Dessi, M.; Di Sante, G.; Tolusso, B.; et al. Prevalence and Determinants of Peripheral Microvascular Endothelial Dysfunction in Rheumatoid Arthritis Patients: A Multicenter Cross-Sectional Study. Mediat. Inflamm. 2018, 2018, 6548715. [Google Scholar] [CrossRef]
- Pumprla, J.; Howorka, K.; Groves, D.; Chester, M.; Nolan, J. Functional assessment of heart rate variability: Physiological basis and practical applications. Int. J. Cardiol. 2002, 84, 1–14. [Google Scholar] [CrossRef]
- Ponti, F.; De Cinque, A.; Fazio, N.; Napoli, A.; Guglielmi, G.; Bazzocchi, A. “Ultrasound imaging, a stethoscope for body composition assessment. ” Quant. Imaging Med. Surg. 2020, 10, 1699–1722. [Google Scholar] [CrossRef]
- Yang, X.Z.; Liu, Y.; Mi, J.; Tang, C.S.; Du, J.B. Totally, Pre-clinical atherosclerosis evaluated by carotid artery intimamedia thickness and the risk factors in children. Chin. Med. J. 2007, 120, 359–362. [Google Scholar] [CrossRef]
- Cristi-Montero, C.; Chillon, P.; Labayen, I.; Casajus, J.A.; Gonzalez-Gross, M.; Vanhelst, J.; Manios, Y.; Moreno, L.A.; Ortega, F.B.; Ruiz, J.R.; et al. Cardiometabolic risk through an integrative classification combining physical activity and sedentary behavior in European adolescents: HELENA study. J. Sport Health Sci. 2019, 8, 55–62. [Google Scholar] [CrossRef]
- Machado, E.A.; Farinatti, P.; Sicuro, F.L.; Rodrigues Jr, F.; Bouskela, E.; Collett-Solberg, P.F. Daily physical activity, cardiorespiratory fitness, nutritional status, endothelial function, and autonomic modulation in school-age adolescents: A principal component analysis. Obes. Res. Clin. Pract. 2021, 15, 205–211. [Google Scholar] [CrossRef]
- Dias, I.; Farinatti, P.; de Souza, M.D.G.C.; Manhanini, D.P.; Balthazar, E.; Dantas, D.L.S.; Pinto, E.H.D.A.; Bouskela, E.; Kraemer-Aguiar, L.G. Effects of Resistance Training on Obese Adolescents. Med. Sci. Sport. Exerc. 2015, 47, 2636–2644. [Google Scholar] [CrossRef]
- Gaesser, G.A.; Angadi, S.S.; Sawyer, B.J. Exercise and Diet, Independent of Weight Loss, Improve Cardiometabolic Risk Profile in Overweight and Obese Individuals. Phys. Sportsmed. 2011, 39, 87–97. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour; WHO: Geneva, Switzerland, 2020; 104p. [Google Scholar]
- Lee, C.M.Y.; Huxley, R.R.; Wildman, R.P.; Woodward, M. Indices of abdominal obesity are better discriminators of cardiovascular risk factors than BMI: A meta-analysis. J. Clin. Epidemiol. 2008, 61, 646–653. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Libman, I.; Hughan, K.S.; Kuk, J.L.; Barinas-Mitchell, E.; Chung, H.; Arslanian, S. Effects of exercise modality on body composition and cardiovascular disease risk factors in adolescents with obesity: A randomized clinical trial. Appl. Physiol. Nutr. Metab. 2020, 45, 1377–1386. [Google Scholar] [CrossRef] [PubMed]
- Verheggen, R.J.H.M.; Maessen, M.F.H.; Green, D.J.; Hermus, A.R.M.M.; Hopman, M.T.E.; Thijssen, D.H.T. A systematic review and meta-analysis on the effects of exercise training versus hypocaloric diet: Distinct effects on body weight and visceral adipose tissue. Obes Rev. 2016, 17, 664–690. [Google Scholar] [CrossRef]
- Pescatello, L.S.; Buchner, D.M.; Jakicic, J.M.; Powell, K.E.; Kraus, W.E.; Bloodgood, B.; Campbell, W.W.; Dietz, S.; DiPietro, L.; George, S.M.; et al. Physical Activity to Prevent and Treat Hypertension: A Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1314–1323. [Google Scholar] [CrossRef] [PubMed]
- Canoy, D.; Nazarzadeh, M.; Copland, E.; Bidel, Z.; Rao, S.; Li, Y.; Rahimi, K. How Much Lowering of Blood Pressure Is Required to Prevent Cardiovascular Disease in Patients With and Without Previous Cardiovascular Disease? Curr. Cardiol. Rep. 2022, 24, 851–860. [Google Scholar] [CrossRef]
- García-Hermoso, A.; Saavedra, J.M.; Escalante, Y. Effects of exercise on resting blood pressure in obese children: A meta-analysis of randomized controlled trials. Obes. Rev. 2013, 14, 919–928. [Google Scholar] [CrossRef]
- Meyer, A.A.; Kundt, G.; Lenschow, U.; Schuff-Werner, P.; Kienast, W. Improvement of Early Vascular Changes and Cardiovascular Risk Factors in Obese Children After a Six-Month Exercise Program. J. Am. Coll. Cardiol. 2006, 48, 1865–1870. [Google Scholar] [CrossRef] [Green Version]
- Kelley, G.A.; Kelley, K.S.; Pate, R.R. Exercise and Cardiovascular Disease Risk Factors in Children and Adolescents With Obesity: A Systematic Review With Meta-Analysis of Randomized Controlled Trials. Am. J. Lifestyle Med. 2021, 16, 485–510. [Google Scholar] [CrossRef]
- Ramezani, A.; Gaeini, A.A.; Hosseini, M.; Mohammadi, J.; Mohammadi, B. Effects of three methods of exercise training on cardiovascular risk factors in obese boys. Iran. J. Pediatr. 2017, 27, e7145. [Google Scholar] [CrossRef]
- Racil, G.; Ben Ounis, O.; Hammouda, O.; Kallel, A.; Zouhal, H.; Chamari, K.; Amri, M. Effects of high vs. Moderate exercise intensity during interval training on lipids and adiponectin levels in obese young females. Eur. J. Appl. Physiol. 2013, 113, 2531–2540. [Google Scholar] [CrossRef]
- Karacabey, K. The effect of exercise on leptin, insulin, cortisol and lipid profiles in obese children. J. Int. Med. Res. 2009, 37, 1472–1478. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.S.; Im, J.A.; Kim, K.C.; Park, J.H.; Suh, S.H.; Kang, E.S.; Kim, S.H.; Jekal, Y.; Lee, C.W.; Yoon, Y.J.; et al. Improved insulin sensitivity and adiponectin level after exercise training in obese Korean youth. Obesity 2007, 15, 3023–3030. [Google Scholar] [CrossRef]
- Madeira, I.R.; Carvalho, C.N.; Gazolla, F.M.; Pinto, L.W.; Borges, M.A.; Bordallo, M.A.N. Impact of obesity on metabolic syndrome components and adipokines in prepubertal children. J. Pediatr. 2009, 85, 261–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maguolo, A.; Maffeis, C. Acanthosis nigricans in childhood: A cutaneous marker that should not be underestimated, especially in obese children. Acta Paediatr. Int. J. Paediatr. 2020, 109, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Fuster, J.J.; Walsh, K. Adipokines: A link between obesity and cardiovascular disease. J. Cardiol. 2014, 63, 250–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galic, S.; Oakhill, J.S.; Steinberg, G.R. Adipose tissue as an endocrine organ. Mol. Cell. Endocrinol. 2010, 316, 129–139. [Google Scholar] [CrossRef]
- Park, J.H.; Miyashita, M.; Kwon, Y.C.; Park, H.T.; Kim, E.H.; Park, J.K.; Park, K.B.; Yoon, S.R.; Chung, J.W.; Nakamura, Y.; et al. A 12-week after-school physical activity programme improves endothelial cell function in overweight and obese children: A randomised controlled study. BMC Pediatr. 2012, 12, 111. [Google Scholar] [CrossRef] [Green Version]
- Sethi, J.K.; Hotamisligil, G.S. Metabolic Messengers: Tumour necrosis factor. Nat. Metab. 2021, 3, 1302–1312. [Google Scholar] [CrossRef]
- Han, Y.; Liu, Y.; Zhao, Z.; Zhen, S.; Chen, J.; Ding, N.; Ma, Y.; Wen, D. Does physical activity-based intervention improve systemic proinflammatory cytokine levels in overweight or obese children and adolescents? Insights from a meta-Analysis of randomized control trials. Obes. Facts 2019, 12, 653–668. [Google Scholar] [CrossRef]
- Ryder, J.R.; O'Connell, M.; Bosch, T.A.; Chow, L.; Rudser, K.D.; Dengel, D.R.; Fox, C.K.; Steinberger, J.; Kelly, A.S. Impaired cardiac autonomic nervous system function is associated with pediatric hypertension independent of adiposity. Pediatr. Res. 2016, 79, 49–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, R.S.; Barker, A.R.; Wilkinson, K.M.; Abbott, R.A.; Williams, C.A. Is cardiac autonomic function associated with cardiorespiratory fitness and physical activity in children and adolescents? A systematic review of cross-sectional studies. Int. J. Cardiol. 2017, 236, 113–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Penha, J.T.; Gazolla, F.M.; de Miranda Carvalho, C.N.; Madeira, I.R.; Rodrigues-Júnior, F.; de Amorim Machado, E.; Sicuro, F.L.; Farinatti, P.; Bouskela, E.; Collett-Solberg, P.F. Physical fitness and activity, metabolic profile, adipokines and endothelial function in children. J. Pediatr. 2019, 95, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Gazolla, F.M.; Bordallo, M.A.N.; Madeira, I.R.; de Miranda Carvalho, C.N.; Monteiro, A.M.V.; Rodrigues, N.C.P.; Borges, M.A.; Collett-Solberg, P.F.; Muniz, B.M.; de Oliveira, C.L.; et al. Association between cardiovascular risk factors and carotid intima-media thickness in prepubertal Brazilian children. J. Pediatr. Endocrinol. Metab. 2015, 28, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Groner, J.A.; Joshi, M.; Bauer, J.A. Pediatric precursors of adult cardiovascular disease: Noninvasive assessment of early vascular changes in children and adolescents. Pediatrics 2006, 118, 1683–1691. [Google Scholar] [CrossRef] [PubMed]
- Farpour-Lambert, N.J.; Aggoun, Y.; Marchand, L.M.; Martin, X.E.; Herrmann, F.R.; Beghetti, M. Physical Activity Reduces Systemic Blood Pressure and Improves Early Markers of Atherosclerosis in Pre-Pubertal Obese Children. J. Am. Coll. Cardiol. 2009, 54, 2396–2406. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Outcome | EU-Swim | EW-Swim | EW-Sed |
|---|---|---|---|
| N | 14 | 20 | 15 |
| Age (y) | 9.6 ± 1.5 | 10.3 ±1.8 | 10.9 ±2.1 |
| Female/male (n) | 9/5 | 11/9 | 10/5 |
| Nutritional status (n) | |||
| Eutrophic | 14 | 0 | 0 |
| Overweight | 0 | 10 | 4 |
| Obesity | 0 | 10 | 11 |
| Pubertal stage (n) | |||
| Prepubertal (T1) | 8 | 5 | 6 |
| Beginning of puberty (T2 and T3) | 4 | 12 | 5 |
| End of puberty (T4 and T5) | 2 | 3 | 4 |
| Acanthosenigricans (yes/no) | 0/0 | 5/15 | 10/5 |
| Elevated blood pressure (≥90th percentile, n) | 4 | 7 | 8 |
| Outcome | EU-Swim | EW-Swim | EW-Sed | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline (n = 14) | 6 Months (n = 14) | 12 Months (n = 9) | Baseline (n = 20) | 6 Months (n = 20) | 12 Months (n = 18) | Baseline (n = 15) | 6 Months (n = 15) | 12 Months (n = 12) | |
| z-BMI | 0.26 ± 0.64 *,ϕ,12 | 0.26 ± 0.69 *,ϕ | 0.10 ± 0.83 | 1.98 ± 0.69 ϕ, 12 | 1.84 ± 0.64 *,ϕ | 1.67 ± 0.48 ϕ | 2.91 ± 1.06 | 2.56 ± 0.56 | 2.95 ± 0.96 |
| W/H | 0.42 ± 0.02 *,ϕ | 0.42 ± 0.02 *,ϕ | 0.42 ± 0.03 ϕ | 0.51 ±0.06 ϕ, 6, 12 | 0.48 ±0.04 ϕ | 0.47 ±0.04 ϕ | 0.57 ± 0.06 | 0.54 ± 0.03 | 0.58 ± 0.11 |
| PAQ-C (score) | 2.2 ± 0.5 6 | 2.6 ± 0.5 *,ϕ | 2.4 ± 0.6 | 1.9 ± 0.4 6, 12 | 2.9 ± 0.5 ϕ, 12 | 2.6 ± 0.4 ϕ | 2.1 ± 0.5 | 2.0 ± 0.5 | 2.0 ± 0.5 |
| Screen time (h) | 5.6 ± 2.3 6, 12 | 4.6 ± 2.8 | 4.9 ± 3.5 | 3.4 ± 1.8 | 3.6 ± 1.9 | 3.9 ± 2.5 | 4.2 ± 1.9 | 4.0 ± 2.6 | 3.8 ± 1.8 |
| Yoyo test (m) | 506 ± 200 *,ϕ, 6, 12 | 641 ± 266 *,ϕ, 12 | 531 ± 93 | 337 ± 98 ϕ, 6, 12 | 438 ± 117 ϕ | 474 ± 96 ϕ | 307 ± 108 | 338 ± 103 | 326 ± 117 |
| SBP (mmHg) | 106.4 ± 11.2 ϕ,6,12 | 97.4 ± 7.8 ϕ | 97.1 ± 6.5 ϕ | 108.4 ± 8.5 ϕ,6,12 | 100.3 ± 4.8 ϕ | 102.3 ± 4.8 | 118.2 ± 15.0 6,12 | 110.2 ± 13.3 | 111.7 ± 14.4 |
| DBP (mmHg) | 60.6 ± 8.5 6 | 54.4 ± 5.6 | 54.8 ± 5.2 | 62.2 ± 9.1 6,12 | 56.9 ± 5.8 ϕ | 56.0 ± 4.9 | 64.4 ± 7.0 | 63.2 ± 13.4 | 63.9 ± 10.5 |
| Glucose (mg/dL) | 91.1 ± 6.8 | 91.4 ± 7.7 ϕ | 89.9 ± 7.5 | 94.1 ± 11.7 | 91.1 ± 5.3 ϕ | 89.8 ± 4.1 | 95.1 ± 7.7 | 97.1 ± 9.1 | 92.4 ± 7.7 |
| Insulin (μlU/mL) | 8.8 ± 4.2 ϕ | 9.2 ± 4.3 ϕ | 11.3 ± 5.1 ϕ | 17.5 ± 8.3 ϕ | 14.7 ± 7.6 ϕ | 17.9 ± 7.6 ϕ | 30.0 ± 8.7 | 29.9 ± 6.0 | 31.8 ± 3.2 |
| TG (mg/dL) | 93.2 ± 44.5 ϕ | 89.9 ± 59.0 ϕ | 85.6 ± 33.8 ϕ | 91.9 ± 35.3 ϕ | 93.1 ± 38.9 ϕ | 89.5 ± 26.7 | 153.9 ± 18.4 12 | 174.6 ± 10.9 | 116.7 ± 64.8 |
| HDL (mg/dL) | 51.8 ± 10.7 ϕ | 48.5 ± 10.6 ϕ | 49.3 ± 7.7 | 50.3 ± 13.9 ϕ | 47.3 ± 8.5 ϕ | 47.9 ± 9.1 | 40.3 ± 6.9 | 35.2 ± 6.9 | 39.9 ± 6.0 |
| LDL (mg/dL) | 86.3 ± 17.3 12 | 85.3 ± 25.5 | 99.0 ± 24.5 | 94.8 ± 26.0 | 83.1 ± 23.2 12 | 100.6 ± 29.4 | 96.2 ± 20.4 | 82.2 ± 21.6 12 | 105.2 ± 20.3 |
| TNF-α (pg/mL) | - | - | - | 1.07 ± 0.55 | - | 0.96 ± 0.21 | 1.06 ± 0.23 | - | 1.08 ± 0.12 |
| Adiponectin (µg/mL) | 10.3 ± 4.1 *ϕ | 9.3 ± 3.2 12 | 12.2 ± 5.1 ϕ | 7.9 ± 5.4 | 7.6 ± 4.8 | 8.3 ± 4.0 | 5.4 ± 3.5 | 5.5 ± 3.4 | 6.0 ± 3.7 |
| Leptin (ng/mL) | 11.0 ± 6.0 *,ϕ | 11.6 ± 9.2 *,ϕ | 14.1 ± 8.1 *,ϕ | 26.4 ± 14.0 6,12 | 22.8 ± 10.6 ϕ | 21.6 ± 9.1 ϕ | 37.7 ± 21.8 | 32.2 ± 22.9 | 42.3 ± 25.2 |
| % Increment | 323.9 ± 206.2 ϕ | 389.6 ± 123.9 12 | 265.9 ± 112.3 | 238.2 ± 94.8 6,12 | 334.6 ± 190.6 | 300.0 ± 136.8 | 209.3 ± 150.0 | 305.0 ± 156.3 | 347.1 ± 112.6 |
| LnRHI | 0.31 ± 0.14 *,ϕ,6,12 | 0.51 ± 0.24 | 0.57 ± 0.33 | 0.47 ± 0.24 | 0.58 ± 0.23 | 0.57 ± 0.22 | 0.54 ± 0.21 | 0.60 ± 0.17 | 0.64 ± 0.21 |
| RR (ms) | 818.6 ± 98.5 | 851.7 ± 89.8 | 826.0 ± 81.4 | 796.7 ± 68.9 6 | 874.0 ± 121.9 12 | 831.0 ± 133.6 | 847.4 ± 77.9 | 875.6 ± 77.9 | 910.6 ± 154.2 |
| RMSSD (ms) | 78.8 ± 30.7 ϕ | 82.6 ± 25.8 ϕ | 77.0 ± 20.1 ϕ | 68.7 ± 28.2 ϕ,6 | 94.2 ± 43.2 12 | 71.4 ± 25.6 ϕ | 92.4 ± 40.8 6 | 110.9 ± 75.5 | 105.0 ± 57.2 |
| SAT (cm) | 1.32 ± 0.67 *,ϕ | - | 2.88 ± 1.63 | 2.50 ± 1.03 12 | - | 2.34 ± 0.71 ϕ | 3.35 ± 1.27 | - | 3.61 ± 1.13 |
| VAT (cm) | 2.71 ± 0.31 *,ϕ | - | 3.09 ± 0.52 ϕ | 4.05 ± 1.08 12 | - | 3.39 ± 1.01 ϕ | 4.61 ± 1.35 | - | 4.74 ± 0.91 |
| cIMT right (cm) | 0.060 ± 0.005 12 | - | 0.043 ± 0.010 *,ϕ | 0.057 ± 0.012 | - | 0.058 ± 0.011 | 0.061 ± 0.001 | - | 0.056 ± 0.010 |
| cIMT left (cm) | 0.063 ± 0.004 12 | - | 0.047 ± 0.013 *,ϕ | 0.058 ± 0.012 ϕ | - | 0.059 ± 0.011 | 0.064 ± 0.010 | - | 0.057 ± 0.011 |
| Outcome | OB-Swim | OB-Sed | ||||
|---|---|---|---|---|---|---|
| Baseline (n = 10) | 6 Months (n=10) | 12 Months (n = 9) | Baseline (n = 11) | 6 Months (n = 11) | 12 Months (n = 9) | |
| z-BMI | 2.56 ± 0.42 *,12 | 2.37 ± 0.39 *,12 | 2.00 ± 0.36* | 3.29 ± 0.98 | 2.84 ± 0.53 | 3.24 ± 0.91 |
| W/H | 0.55 ± 0.06 6,12 | 0.51 ± 0.03 * | 0.50 ± 0.04 * | 0.59 ± 0.05 | 0.57 ± 0.03 | 0.60 ± 0.11 |
| PAQ-C (score) | 1.9 ± 0.5 6 | 2.8 ± 0.6 *,12 | 2.2 ± 0.4 | 2.1 ± 0.5 | 2.0 ± 0.5 | 2.1 ± 0.6 |
| Screen time (h) | 3.5 ± 2.0 | 3.7 ± 1.8 | 3.7 ± 2.9 | 4.4 ± 2.0 | 3.7 ± 2.6 | 4.0 ± 2.1 |
| Yoyo test (m) | 324 ± 101 6,12 | 416 ± 75 12 | 462 ± 75 * | 290 ± 101 6,12 | 331 ± 85 | 320 ± 113 |
| SBP (mmHg) | 111.8 ± 7.6 *,6,12 | 99.0 ± 4.6 *,12 | 104.1 ± 4.2 * | 121.6 ± 15.0 | 118.0 ± 8.6 | 115.7 ± 12.5 |
| DBP (mmHg) | 62.8 ± 7.2 6,12 | 56.5 ± 7.4 * | 56.2 ± 5.5 | 66.2 ± 5.5 | 67.6 ± 15.0 | 65.9 ± 11.4 |
| Glucose (mg/dL) | 92.8 ± 5.1 | 91.1 ± 3.6 * | 88.7 ± 4.9 | 92.7 ± 6.8 | 96.8 ± 10.2 | 90.6 ± 7.4 |
| Insulin (μlU/mL) | 19.9 ± 9.1 | 19.4 ± 9.0 | 19.5 ± 9.5 | 26.7 ± 11.4 | 24.3 ± 12.1 | 23.6 ± 11.9 |
| TG (mg/dL) | 107.8 ± 38.3 | 120.1 ± 38.1 | 93.2 ± 32.9 | 161.4 ± 119.3 | 212.3 ± 122.5 | 127.5 ± 71.8 |
| HDL (mg/dL) | 46.2 ± 12.5 | 46.3 ± 7.7 | 48.9 ± 7.3 | 39.0 ± 7.0 | 37.0 ± 7.7 | 40.3 ± 5.0 |
| LDL (mg/dL) | 103.8 ± 27.8 | 88.6 ± 23.8 | 111.1 ± 32.3 | 96.9 ± 23.4 | 89.2 ± 24.9 | 110.3 ± 17.3 |
| TNF-α (pg/mL) | 1.11 ± 0.15 12 | - | 0.92 ± 0.18 * | 1.07 ± 0.24 | - | 1.12 ± 0.09 |
| Adiponectin (µg/mL) | 5.7 ± 3.5 12 | 5.8 ± 3.1 12 | 7.0 ± 2.9 * | 4.8 ± 3.1 | 5.0 ± 3.4 | 5.5 ± 3.2 |
| Leptin (ng/mL) | 33.8 ± 15.2 6,12 | 29.3 ± 10.7 * | 23.0 ± 8.9 * | 43.8 ± 21.8 | 43.2 ± 18.6 | 45.0 ± 18.0 |
| % Increment | 207.8 ± 75.8 | 296.1 ± 119.2 | 282.8 ± 120.6 | 199.8 ± 143.4 | 292.4 ± 119.8 | 383.0 ± 100.5 |
| LnRHI | 0.46 ± 0.22 | 0.63 ± 0.21 | 0.52 ± 0.23 | 0.58 ± 0.21 | 0.62 ± 0.12 | 0.68 ± 0.19 |
| RR (ms) | 815.8 ± 79.5 | 930.3 ± 144.5 | 895.9 ± 144.9 | 855.4 ± 73.7 | 862.3 ± 137.8 | 945.5 ± 174.8 |
| RMSSD (ms) | 84.1 ± 28.5 | 114.9 ± 44.4 | 85.5 ± 22.4 | 89.6 ± 35.1 | 94.2 ± 65.7 | 95.7 ± 46.3 |
| SAT (cm) | 3.09 ± 1.10 12 | - | 2.70 ± 0.70 * | 3.54 ± 1.35 | - | 4.06 ± 1.06 |
| VAT (cm) | 4.65 ± 1.04 12 | - | 3.69 ± 1.01 | 4.68 ± 1.27 | - | 4.44 ± 0.75 |
| cIMT right (cm) | 0.061 ± 0.008 | - | 0.059 ± 0.012 | 0.061 ± 0.003 | - | 0.057 ± 0.011 |
| cIMT left (cm) | 0.059 ± 0.009 | - | 0.061 ± 0.008 | 0.064 ± 0.006 | - | 0.059 ± 0.008 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machado, E.; Jannuzzi, F.; Telles, S.; Oliveira, C.; Madeira, I.; Sicuro, F.; Souza, M.d.G.; Monteiro, A.; Bouskela, E.; Collett-Solberg, P.; et al. A Recreational Swimming Intervention during the Whole School Year Improves Fitness and Cardiometabolic Risk in Children and Adolescents with Overweight and Obesity. Int. J. Environ. Res. Public Health 2022, 19, 17093. https://doi.org/10.3390/ijerph192417093
Machado E, Jannuzzi F, Telles S, Oliveira C, Madeira I, Sicuro F, Souza MdG, Monteiro A, Bouskela E, Collett-Solberg P, et al. A Recreational Swimming Intervention during the Whole School Year Improves Fitness and Cardiometabolic Risk in Children and Adolescents with Overweight and Obesity. International Journal of Environmental Research and Public Health. 2022; 19(24):17093. https://doi.org/10.3390/ijerph192417093
Chicago/Turabian StyleMachado, Elisabeth, Fernanda Jannuzzi, Silvio Telles, Cecilia Oliveira, Isabel Madeira, Fernando Sicuro, Maria das Graças Souza, Alexandra Monteiro, Eliete Bouskela, Paulo Collett-Solberg, and et al. 2022. "A Recreational Swimming Intervention during the Whole School Year Improves Fitness and Cardiometabolic Risk in Children and Adolescents with Overweight and Obesity" International Journal of Environmental Research and Public Health 19, no. 24: 17093. https://doi.org/10.3390/ijerph192417093
APA StyleMachado, E., Jannuzzi, F., Telles, S., Oliveira, C., Madeira, I., Sicuro, F., Souza, M. d. G., Monteiro, A., Bouskela, E., Collett-Solberg, P., & Farinatti, P. (2022). A Recreational Swimming Intervention during the Whole School Year Improves Fitness and Cardiometabolic Risk in Children and Adolescents with Overweight and Obesity. International Journal of Environmental Research and Public Health, 19(24), 17093. https://doi.org/10.3390/ijerph192417093