
Changes in Physical Activity Patterns Due to the Covid-19 Pandemic: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search Strategy
2.4. Selection Process
2.5. Data Collection Process and Data Items
2.6. Risk of Bias and Quality Assessment
2.7. Summary Measures
2.8. Additional Analyses and Synthesis of Results
2.9. Synthesis Method
3. Results
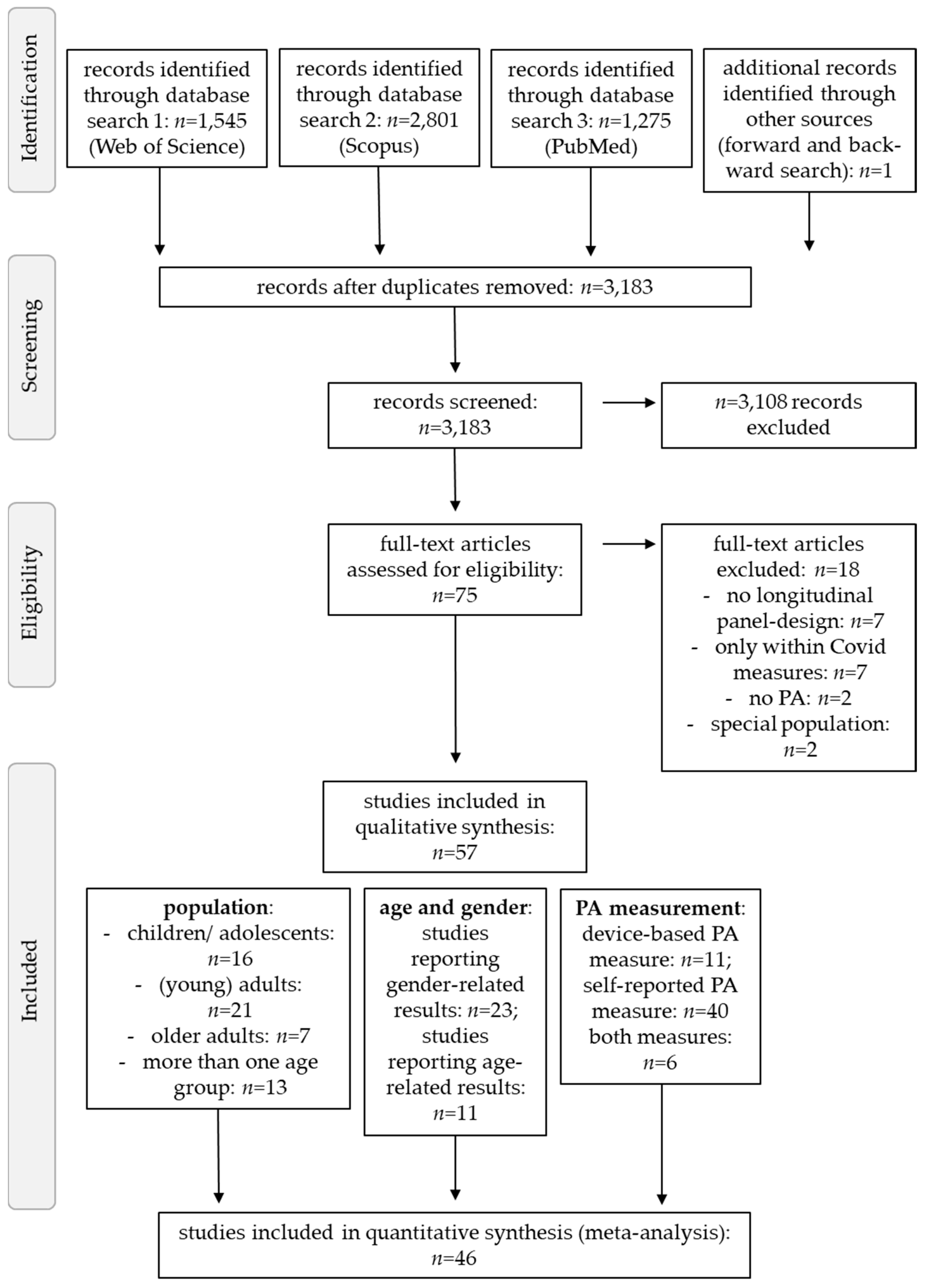
3.1. Study Selection
3.2. Study Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author(s) (Year)/Country [Ref] | Sample Characteristics/Population | PA Related Aim | Sample Size, Age (SD) | PA Measurement | Sampling Timepoints | Central/Overall Results | Absolute Change |
|---|---|---|---|---|---|---|---|
| Aegerter et al. (2021)/Switzerland [68] | Office workers from two Swiss organizations | (...) to quantify the effect of the COVID-19 pandemic on PA levels among Swiss office workers | n = 76 (54 female); 42.7 ± 9.2 years | SR: IPAQ-SF | T0: January 2020 T1: April 2020 | No sig. change in total PA, walking, MPA, VPA | descriptive study |
| Al-Musharaf et al. (2021)/Saudi Arabia [51] | Healthy female students or graduates of King Saud University (19–30 years) | (...) to assess lifestyle changes (a.o. PA) from before COVID-19 to during lockdown | n = 297 (female); 20.7 ± 1.4 years | SR: GPAQ | T0: February–April 2019 T1: April–May 2020 | Total PA: − | Total PA: −126.7 MET-min/week |
| Alonso-Martinez et al. (2021)/Spain [69] | Preschoolers (4–6 years) from 3 schools in Pamplona | (...) to examine the effects of the COVID-19 lockdown on device-measured PA (...) | n = 268 (125 female); 4.28 ± 0.80 years | DB: GENEActiv (accelerometer) | T0: September–December 2019 T1: March–April 2020 | Total PA and MVPA: − | Total PA: −43.3 min/day MVPA: −17.0 min/day |
| Baceviciene and Jankauskiene (2021)/Lithuania [70] | Lithuanian students from a previous, large study | (...) to assess the impact of COVID-19-related lockdown period on PA in university-aged Lithuanian students of both genders (...) | n = 230 (182 female); 23.9 ± 5.4 years | SR: LTQE | T0: October 2019 T1: 9 February 2021 | Males’ leisure-time PA: − | Males: −20 points Females: −6.01 points |
| Barone Gibbset al. (2021)/USA [71] | Desk workers, ≥20 h of deskwork and <150 min MVPA per week | (...) to study the longitudinal impact of COVID-19 on lifestyle among desk workers during shelter-at-home restrictions | n = 112 (77 female); 45.4 ± 12.3 years | SR: Paffenbarger Physical Activity Questionnaire | T0: 2018–2019 T1: May–June 2020 | No sig. change in MPA, VPA, MVPA | MPA: +20 min/week VPA: +/−0 MVPA: +15 min/week |
| Bartlett et al. (2021)/Australia [72] | Adults (>50 years) who engaged in a public health program targeting dementia risk reduction | (...) to examine longitudinal change on dementia risk factors in a sample of middle-aged and older Tasmanian residents | n = 1671 (female 1218); 63.4 ± 7.17 years | SR: min/week for walking, MPA, VPA, TPA | T0: October 2019 T1: April–June 2020 | Total PA: + | Total PA: +300.06 min/week |
| Bronikowska et al. (2021)/Poland [73] | Randomly selected school class from six secondary schools from the urban area of the Wielkopolska region (Greater Poland) | (...) to compare PA levels before and during a pandemic lockdown among adolescent Polish youths (...) | n = 127 (66 female); 15.4 ± 0.5 years | SR: Physical Activity Screening Measure | T0: February 2020 T1: June 2020 | MVPA WHO rec.: + (n = 13), − (n = 15) maintained not meeting (n = 84) maintained meeting (n = 15) | + MVPA WHO rec.: +2.8 days/week −MVPA WHO rec.: −2.4 days/week maintained not meeting rec.: −0.3 days/week maintained meeting rec.: +0.3 days/week |
| Buoite Stella et al. (2021)/Italia [74] | Healthy adults (>18 years) in Italy during the COVID-19 lockdown | (...) to investigate changes occurring in daily life and their effects on health during the COVID-19 lockdown (...) | n = 400 (277 female); 35 ± 15 years | SR: self-designed online-survey | T0: January 2020 T1: 23–29 March 2020 | Step count: − | Ø −4990 steps/day |
| Chaffee et al. (2021)/USA [75] | Ninth- and tenth-grade students high schools in Northern California | (...) to compare adolescents’ PA behaviors before and after stay-at-home restrictions | n = 1006 (623 female); age not reported | SR: Single questionnaire item | T0: March 2019–February 2020 T1: September 2019–September 2020 | Total PA: − | descriptive study |
| Chen et al. (2021)/Sweden [64] | 15-year-old adolescents in Sweden | (...) to investigate the impacts of COVID-19 on health behaviors | n = 584 (311 female); 15.5 ± 04 years | SR: Web questionnaire | T0: September 2015–June 2019 T1: February 2020–November 2020 | PA 60 min/day (days/week): − Weekly duration of LTE: no changes | PA 60 min/day (days/week): −0.2 days/week Weekly duration of LTE: no changes |
| Cheval et al. (2020)/Switzerland [76] | Participants living in France or Switzerland (76% French) | (...) to assess changes in PA during commuting and leisure during the COVID-19 lockdown (...) | n = 110 (76 female); 43 ± 9 years | SR: IPAQ | T1: 30 March 2020 T2: 13 April 2020 | PA when commuting, VPA: − Walking, MPA: + | PA when commuting: −16 min/day VPA: −6 min/day walking: +5 min/day MPA: +4 min/day |
| Curtis et al. (2021)/Australia [77] | Community-based sample of healthy adults from Adelaide, South Australia | (...) to examine changes in recreational PA before and during COVID-19 restrictions in a group of adults in Adelaide, Australia | n = 61 (40 female); 41.3 ± 5.8 years | SR: HABITATDB: Fitbit Charge 3 | T1: 10–23 February 2020 T2: 14–27 April 2020 | LPA, swimming, team sports, boating/sailing: −MVPA: no changecycling: +PA with others in park, running, weights, exercise class, golf, tennis, yoga/pilates/tai chi/qigong, home-based exercise, water activities, PA with others on a beach: no sig. change | LPA: −50 min MVPA: no change; Cycling: +0.35 pt; Swimming: −0.64 pt; Team sports: −0.36 pt; Boating/sailing: −0.13 pt; PA with others in park: −0.32 pt; running: −0.28 pt; weights: −0.31 pt; exercise class: −0.13 pt; golf: −0.03 pt; tennis: +0.04 pt; yoga/pilates/tai chi/qigong: +0.05 pt; home-based exercise: +0.32 pt; water activities: −0.03 pt; PA with others on a beach: −0.11 pt |
| Di Sebastiano et al. (2021)/Canada [78] | Canadian users (≥18 years) PA tracking app (PAC app) | (...) to investigate changes in the PA of Canadians before and after restrictions in Canada, using data from the ParticipACTION app | n = 2338 (2109 female); age range: 18–65 years | DB: PAC app | T1: 10–16 February 2020 T2: 13–19 April 2020 | MVPA, LPA, and steps: − | MVPA: −17.5 min/week LPA: −126.4 min/week steps: −5230 steps/week |
| Ding et al. (2021)/China [79] | Healthy participants (>18 years) from 11 workplaces in Shanghai, | (...) to determine the change in daily steps in response to the lockdown and reopening during the COVID-19 pandemic in China (...) | n = 815 (530 female); age range: 20–50+ years | SR: IPAQ-SF DB: WeRun via WeChat (accelerometer) | T0: December 2019–23 January 2020 T1: 24 January–22 March 2020 | Step count 1: − (24 January 2020) Step count 2: + (25 January–22 March 2020) | step count 1: −3796 steps/day step count 2: +34 steps/day |
| Elnaggar et al. (2020)/Saudi Arabia [80] | Healthy adolescents (14–18 years) | (...) to document PA changes in adolescents living in Saudi Arabia | n = 63 (29 female); 15.54 ± 1.16 years | SR: PAQ-A | Not reported | PAL: − | PAL: −0.28 PAL |
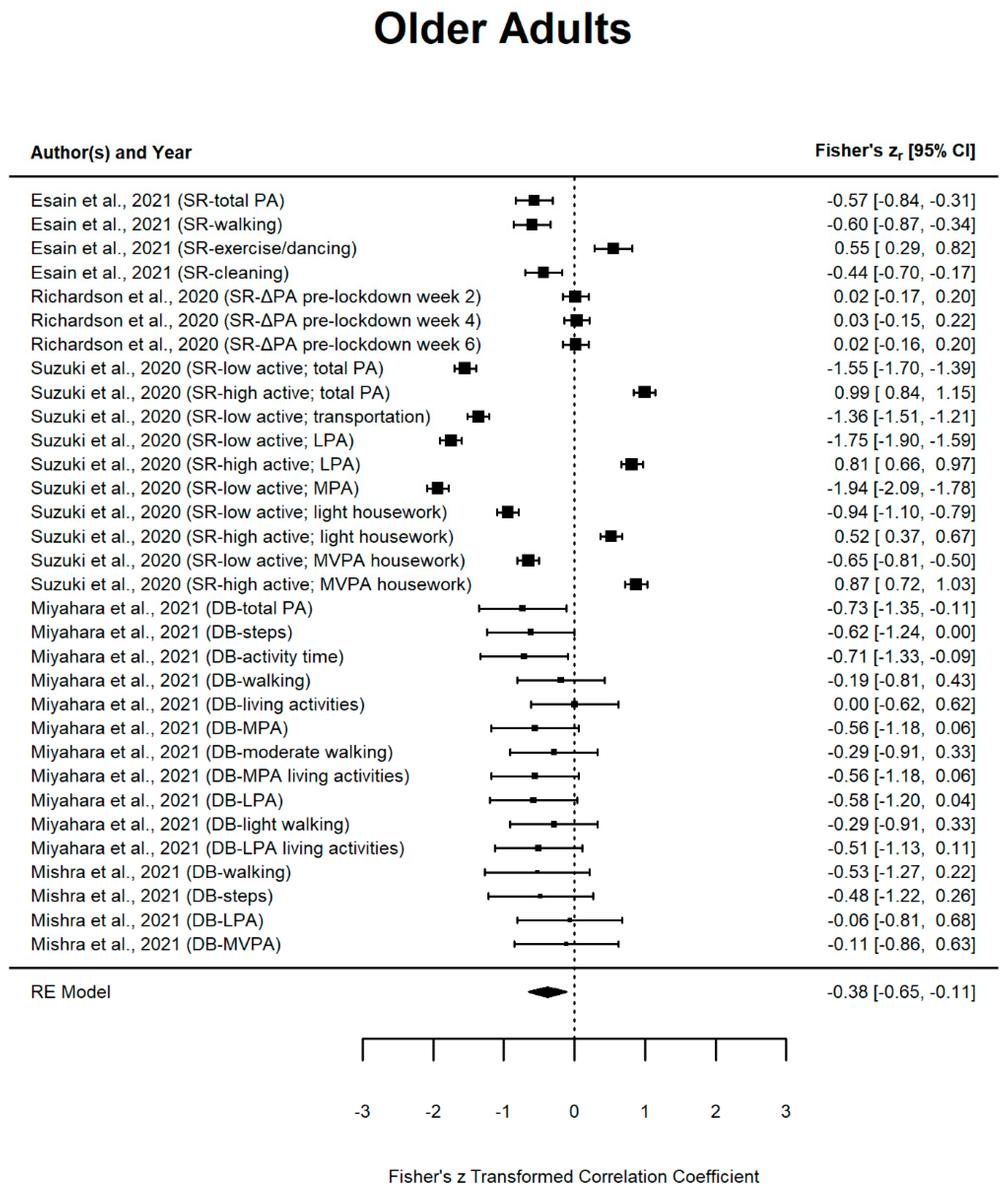
| Esain et al. (2021)/Spain [81] | Community-dwelling adults (>65 years) from Getxo (Basque Country) | (...) to analyze the effect of social distancing measures on PA levels in Spanish older adults (...) | n = 58 (45 female); 76.24 ± 6 years | SR: MLTPAQ-SF | T0: October 2019 T1: June 2020 | Total PA, walking, cleaning: − Exercising or dancing: + | total PA: −2304.74 MET/week walking: −220.00 MET/week cleaning: −210.08 MET/week exercise/dancing: +109.21 MET/week |
| Folk et al. (2021)/USA [82] | Participants of the EAT 2010–2018 study, who attended middle and high schools in Minnesota in 2009/2010 | (...) to understand how PA changed during the time of the COVID-19 pandemic in a diverse sample of emerging adults in the US | n = 720 (447 female); 24.7 ± 2 years | SR: Godin-Shepherd Questionnaire | T0: 2018 T1: April–October 2020 | Total PA, MVPA, mild PA: − | Total PA: −1.47 h/week MVPA: −0.93 h/week Mild PA: −0.52 h/week |
| Franco et al. (2021)/Spain [83] | Spanish office employees who participated in the 5th “Healthy Cities” challenge | (...) to analyze how PA among workers has been affected during confinement and whether certain covariates could have influenced the effect of the confinement on the PA among participants | n = 297 (148 female); 42.76 ± 7.79 years | SR: IPAQ-SF | T0: October 2019 T1: May 2020 | Total PA and MPA: + VPA and walking: no change | Total PA: +463.71 METs MPA: +327.83 METs VPA: +44.32 METs walking: −91.58 METs |
| Gallego-Gomez et al. (2020)/Spain [84] | Nursing students from the Catholic University of Murcia (Spain) | (...) to identify how PE affected the level of stress of Nursing students before and during the lockdown | n = 138 (108 female); 20 years (no SD provided) | SR: Single questionnaire item | T0: 3 February 2020 T1: 24 March 2020 T2: 24 April 2020 | PE and median hours of PE: + | Practice of PE: +26 students Median hours of PE/week: +2 h/week |
| Gilic et al. (2020)/Bosnia and Herzegovina [85] | Adolescents from three counties in B&H attending High school | (...) to evaluate the dynamics of changes in PAL among adolescents from Bosnia and Herzegovina before and during the imposed lockdown | n = 688 (322 female); age range: 15–18 years | SR: PAQ-A | T0: 6–12 January 2020 T1: 20–26 April 2020 | PAL: − | PAL: −0.67 PAL |
| Gilic et al. (2021)/Bosnia and Herzegovina [86] | Healthy high school students (<18 years) from 4 counties in B&H | (...) to examine the influence during the COVID-19 pandemic among adolescents from Bosnia and Herzegovina on PALs | n = 661 (292 female); age range: 15–18 years | SR: PAQ-A | T0: 6–12 January 2020 T1: 20–26 April 2020 | PAL (BL): 48% had sufficient PAL PAL (FU): 24% had sufficient PAL | descriptive study |
| Giuntella et al. (2021)/USA [87] | Students from the University of Pittsburgh | (...) to examine how PA has evolved during the pandemic compared to pre-pandemic levels and to prior cohorts | n = 217 (163 female); 19.22 ± 1.53 years | DB: Fitbit Alta HR | T0: February 2020 T1: April 2020 | Step count: − Active hours: − | Step count: −5400 steps/day Active hours: −1.5 h/day |
| He et al. (2020)/China [88] | Adults from any province of China except Hubei Province (epicenter of the outbreak) | (...) to study the relationships between body weight changes with changes in PA and lifestyle during quarantine | n = 339 (181 female); males: 36.4 ± 11.9 years; female: 37.6 ± 12.4 years | DB: Smartphone health software | T0: 23 December 2019–26 January 2020 T1: 27 January–1 March 2020 | Step count: − MVPA: − | male steps: −4593 steps male MVPA: −11.8 min/day female steps: −3297 steps female MVPA: −8.6 min/day |
| Hino et al. (2021)/Japan [66] | Participants (≥18 years) of the YWPP | (...) to analyze the fluctuation of the step counts of citizens in Yokohama city, Japan, in the first half of 2020 compared to the previous year | n = 18,817 (9083 female); 53.9 ± 7.7 years | DB: Omron HJ-326F (pedometer) | Week 2–26 in 2019 and 2020 T0: Week 15–21, 2019 T1: Week 15–21, 2020 | Step count year-on-year ratio: − | descriptive study |
| Koohsari et al. (2021a)/Japan [89] | Company workers (20–59 years) | (...) to examine the changes in PA of company workers during the COVID-19 outbreak in Japan (...) | n = 2466 (1212 female); 39.6 ± 10.7 years | SR: GPAQ | T0: February 2019 T1: July 2020 | Total PA, VLPA: − VWPA, MWPA, TPA, MLPA: no sig. change | VWPA: −0.02 h/day MWPA: −0.05 h/day TPA: −0.04 h/day VLPA: −0.05 h/day MLPA: −0.04 h/day Total PA: −0.20 h/day |
| Martinez-de-Quel et al. (2020)/Spain [90] | Students (>18 years); at University Madrid, Léon, Vigo, or University Isabel I or others | (...) to show the impact that the lockdown period had on the PA levels to a sample of Spanish individuals due to COVID-19 | n = 161 (60 female); 35 ± 11.2 years | SR: MLTPAQ | T0: 16–31 March 2020 T1: 30 April and 11 May 2020 | Total PA: − | Total PA: - 3462.2 MET min/Week |
| McCarthy et al. (2021)/United Kingdom [58] | Individuals (≥14 years) in the UK registered with BetterPoints (free, publicly available, smartphone-based program) | (...) to explore patterns of tracked activity in the UK before, during, and after the COVID-19 restrictions and to explore variations by demographic characteristics | n = 5395 (3274 female); 41.02 ± 12.2 years | DB: BetterPoints smartphone app | T0: 22 January 2020 T1: 11 March 2020 T1.1: 18 March 2020 T1.2: 25 March 2020 T1.3: 13 May 2020 T2: 17 June 2020 | Total PA: − | Total PA (BL to T1): −30 min/week Total PA (BL to T2): −67 min/week Total PA (BL to T3): −95 min/week Total PA (BL to T4): −69 min/week Total PA (BL to T5): −71 min/week |
| Medrano et al. (2020)/Spain [91] | Cohort of children of the MUGI project in Navarra (8–16 years) | (...) to examine the effects of the COVID-19 confinement on lifestyle behaviors in a cohort of Spanish children (...) | n = 113 (55 female); 12.0 ± 2.6 years | SR: YAP | T0: September–December 2019 T1: March–April 2020 | Total PA: − | Total PA: −91 min/day |
| Mishra et al. (2021)/USA [55] | Community-dwelling older adults (≥75 years) or aged 65 years older with a high risk of falling | (...) to examine changes from pre- to post-pandemic in mobility performance, including walking characteristics (...) | n = 10 (4 female); 77.3 ± 1.9 years | DB: PAMSys (pendant sensor) | Not reported | daily walking duration and step count: − LPA and MVPA: no change | walking duration: −52.2% Step count: −3256 steps/day LPA: −0.3 min/day MVPA: −3.7 min/day |
| Miyahara et al. (2021)/Japan [92] | Elderly people residing in Asakita Ward, Hiroshima City | (...) to elucidate how much self-restraint from activity by the elderly with diseases reduces PA | n = 13 (11 female); 77.5 ± 3.5 years | DB: HJA-750C OMRON (accelerometer) | T0: October 2019 T1: April 2020 | Steps, AT, MPA, MLAPA, LPA, LWAPA, LLAPA, total PA: − Walking, LA, MWAPA: no change | Steps: −2236, 1 steps/d; AT: −98.4 min/d; MPA: −1.8 METs h/d; MLAPA: −1.3 METs h/d; LPA: −2.4 METs h/d; LWAPA: −0.3 METs h/d; LLAPA: −2.1 METs h/d; Total PA: −4.2 METs h/d; Walking: −0.1 METs; LA: no change; MWAPA: −0.5 METs h/d |
| Munasinghe et al. (2020)/Australia [63] | Young people from the general population (13–19 years) of Western Sydney | (...) to investigate whether the physical distancing policies were associated with changes in PA in the state of New South Wales (Australia) | n = 582 (465 female); median age: 17 years | SR: PACE + Adolescent PA Measures DB: Smartphone sensors | T0: 8 November 2019–23 March 2020 T1: 24 March–19 April 2020 | Total PA: − Step count: − MBAR: − | descriptive study |
| Nigg et al. (2021)/Germany [93] | Children and adolescents (4–17 years) living in Germany | (...) to investigate whether participants living in areas with higher population density demonstrate less positive PA changes | n = 1711 (852 female); 11.34 ± 4.06 years | SR: MoMo-PAQ | T0: August 2018–March 2020 T1: 20 April–1 May 2020 | Active days/week, daily life PA: + sports-related PA: − | Active days: +0.47 days/week Sport-related PA: −68.33 min/week Daily life PA: +37.74 min/day |
| Nyström et al. (2020)/Sweden [57] | Preschoolers (3–5 years) from Stockholm County and County of Östergötland | (...) to assess how movement behaviors have been affected in Swedish preschool children during the COVID-19 pandemic | n = 100 (42 female); 4.0 ± 0.5 years | SR: Self-developed questionnaire DB: ActiGraph | T0: March–May 2019 T1: May–June 2020 | Total PA, time spent outside weekdays and weekends: + | Total PA: +53 min/day Time spent outside (weekdays): +124 min/day Time spent outside (weekend): +68 min/day |
| Obuchi et al. (2021)/Japan [94] | Subscribers to a life insurance plan from a private insurance service in Japan | (...) to determine the effects of self-restraints on daily walking parameters | n = 3901 (2969 female); 60.3 ± 28.9 years | DB: Smartphone application | T0: 2 March–15 June 2019 T1: 2 March–15 June 2020 | Step count: − | steps: −1000 steps/week |
| Okely et al. (2021)/14 countries [50] | Children (3–5 years) of the SUNRISE study | (...) to examine how the COVID-19 pandemic influenced PA among preschoolers (...) | n = 948 (466 female); 5.2 ± 0.6 years | SR: Parent/Caregiver survey | T0: April 2019–March 2020 T1: May–June 2020, | No significant changes | Total PA: +17 min/day MVPA: −5 min/day |
| Okely et al. (2020)/United Kingdom [95] | Participants rom the Lothian Birth Cohort 1936 (LBC1936) study, all born in 1936 | (...) to examine changes in PA among older people during COVID-19 lockdown, and if participant characteristics were related to more positive or negative changes during the lockdown | n = 137 (66 female); 84 years | SR: Single questionnaire item | T0: 2017–2019 T1: 27 May 2020 | Total PA: − Minimal PA: + | descriptive study |
| Ong et al. (2020)/Singapore [96] | Young adults (21–40 years) working in the Central Business District in Singapore | (...) to characterize how COVID-19-associated mobility restrictions shifted PA patterns from previously established baselines | n = 1824 (941 female); 30.94 ± 4.62 years | DB: Fitbit API | T0: 2–22 January 2020 T1: 17 March–6 April 2020 T2: 7–27 April 2020 | Step count and MVPA: − | Steps WD (T0–T1): −1548 steps Steps WE (T0–T1): −1569 steps MVPA WD (T0–T1): −4.1 min MVPA WE (T0–T1): −4.9 min Steps WD (T0–T2): −4060 steps Steps WE (T0–T2): −3560 steps MVPA WD (T0–T2): −13.2 min MVPA WE (T0–T2): −13.7 min |
| Park et al. (2021)/South Korea [97] | Adults (>18 years) in South Korea | (...) to investigate the changes in health-related behaviors and outcomes pre-COVID-19 and during COVID-19 (...) | n = 834 (380 female); 23.7 ± 6.0 years | DB: Data from smartphone health app | T0: January 2019–February 2020 and May 2020 T1: June, July, & October 2020 T2: March, April, & August 2020 T3: September 2020 | Step count: − | Step count: −935 steps (mean decrease) T0–T1: −539 steps T0–T2: −1131 steps T0–T3: −1136 steps |
| Perez et al. (2021)/Spain [98] | Nondisabled frail older adults from the +ÀGIL Barcelona project | (...) to describe PA changes due to mobility restrictions in community-dwelling, frail older persons from Barcelona, who had not been diagnosed with COVID-19 | n = 98 (65 female); 82.4 ± 6.1 years | SR: BPAAT | T0: May 2019 T1: May 2020 | Total PA: − sufficient PA: − | Total PA: −1.1/8 points sufficient PA: −32.2% |
| Riberiro de Lima et al. (2021)/Brazil [52] | Physically inactive females (50–70 years) | (...) to analyze the effects of this pandemic period on PA in women aged 50 to 70 years | n = 34 (female); 58.5 ± 6.0 years | SR: MBQO | T0: January–February 2020 T1: June–July 2020 | Domestic PA, free time PA: − Sports PA, total PA (MBQO score): no sig. changes | Domestic PA: −5.8% Free time PA: −83.2% Sports PA: −7.1% Total MBQO score: −19.9% |
| Richardson et al. (2020)/United Kingdom [99] | Older adults (≥70 years) recruited throughout the UK by self-selection, through online advertisements | (...) to examine the impact that COVID-19 measures in the UK, had on individuals aged 70 and over in terms of their PA levels | n = 117 (65 female); 75 ± 4 years | SR: IPAQ-E | T0: 11 March–28 March T1: 4 April T2: 18 April T3: 2 May | Total PA: no sig. change | T0–T1: +87 MET-minutes T0–T2: +185 MET-minutes T0–T3: +109 MET-minutes |
| Romero-Blanco et al. (2020)/Spain [100] | First- to fourth-year health sciences students | (...) to analyze the PA university students did before and during the lockdown and to look at changes resulting from sociodemographic characteristics | n = 213 (172 female); 20.5 ± 4.56 years | SR: IPAQ-SF | T0: 15–30 January 2020 T1: 1–15 April 2020 | Days of VPA and MPA, total minutes of PA: + | Days of VPA: +1.21 days Days of MPA: +1.41 days Total minutes of PA: +159.87 min/week |
| Sanudo et al. (2020)/Spain [101] | College students from different schools in Seville | (...) to determine to what extent PA changed during the COVID-19 lockdown | n = 20 (9 female); 22.6 ± 3.4 years | SR: IPAQ DB: Xiaomi Mi Band 2 (accelerometer) | T0: February 2020 T1: 24 March–3 April 2020 | walking time, MPA, VPA, MVPA, step count: − | walking time: −335 min/week MPA: −263 min/week VPA: −188 min/week MVPA: −451 min/week Step count: −5771 steps/day |
| Savage et al. (2021)/United Kingdom [102] | University students in the UK | (...) to investigate the changes in PA in university students from before to after the COVID-19 pandemic | n = 255 (193 female); 18.97 years (no SD provided) | SR: EVS | T0: 14 October–4 November 2019 T1: 19 October–1 November 2020 | MVPA: − | MVPA: −50 min/week |
| Savage et al. (2020)/United Kingdom [103] | Students of a UK University who were part of the Student Health Study | (...) to investigate changes in PA in UK university students before, in week one, and five weeks into the lockdown (...) | n = 214 (154 female); 20.0 years (no SD provided) | SR: EVS | T0: October 2019 T1: January 2020 T2: March 2020 T3: April 2020 | MVPA: − | MVPA: −30 min/week |
| Schmidt et al. (2020)/Germany [104] | Children and adolescents (4–17 years) living in Germany | (...) to investigate how PA in children and adolescents in Germany changed from before to during the COVID-19 lockdown | n = 1711 (852 female); 11.34 ± 4.06 years | SR: MoMo-PAQ | T0: August 2018–March 2020 T1: 20 April–1 May 2020 | Days active, adherence to the WHO PA guidelines, nonorganized sports, playing outside, gardening, housework, total HA: + Organized sports, total amount of sports: − walking and cycling: no sig. change | days active: +0.44 days/week adherence to PA guidelines: descriptive organized sports: −28.5 min/day nonorganized sports: +17.7 min/day total amount of sports: −10.8 min/day playing outside: +21.4 min/day walking and cycling: +1.8 min/day gardening: +6.7 min/day housework: +4.0 min/day total amount of HA: +36.2 min/day |
| Sekulic et al. (2020)/Croatia [105] | Adolescents attending high school from Split, Dalmatia County | (...) to evaluate the level of changes in PALs among adolescents from southern Croatia (...) | n = 388 (126 female); 16.4 ± 1.9 years | SR: PAQ-A | T0: February 2020 T1: 5–10 April 2020 | PAL: − | PAL: −0.32 |
| Suzuki et al. (2020)/Japan [65] | Randomly selected patients (>65 years) from the patient database of a rehabilitation hospital in Kure city, | (...) to understand the impact of public health restrictions on community-dwelling older adults concerning the changes in PA (...) | n = 165 (115 female) 78.6 ± 8.0 years | SR: PAQ-EJ | T0: 20 March–15 April 2020 T1: 16 April–13 May 2020 | less active group: transportation, light exercise/sports activity, moderate/strenuous exercise/sports, light housework, moderate/heavy housework, total PA: − resistance exercise/sports, labor: no change more active group: light exercise/sports activity, light housework, moderate/heavy housework, total PA: + transportation, moderate/ strenuous exercise/ sports, resistance exercise/sports, labor: no change | less active group: transportation: −3.0 MET h/week light exercise/sports: −6.0 MET h/week moderate/strenuous exercise/sports: −4.1 MET h/week light housework: −4.7 MET h/week moderate/heavy housework: −2.4 MET h/week total PA: −23 MET h/week more active group: light exercise/sports activity: +2.9 MET h/week light housework: +3.7 MET h/week moderate/heavy housework: + 6.9 MET h/week total PA: +24.7 MET h/week |
| To et al. (2021)/Australia [56] | Registered members of the 10,000 Steps program | (...) to investigate changes in PA reported through the 10,000 Steps program during the COVID-19 pandemic | n = 60,560 (40,583 female); age range: 18–45 years | SR: manually registered steps DB: steps automatically synced from activity trackers | Ongoing between 1 January 2018, and 30 June 2020 T1: 1 December 2019 T2: 25 January 2020 T3: 5 February 2020 T4: 2 March 2020 T5: 8 May 2020 | Step count (T1, Ø of 30 d; T2, Ø of 7 d; T3, Ø of 7 d; T4, Ø of 7 d, Ø of 30 d): − Step count (T5, Ø of 7 d; T5, Ø of 30 d): + No change: T1, Ø of 7 d; T2, Ø of 30 d; T3, Ø of 30 d | T1: steps: −99 steps (Ø of 7 d); −174 steps (Ø of 30 d) T2: steps: −144 steps (Ø of 7 d); −39 steps (Ø of 30 d) T3: steps: −69 steps (Ø of 7 d); +13 steps (Ø of 30 d) T4: steps: −325 steps (Ø of 7 d); −485 steps (Ø of 30 d) T5: steps: +130 steps (Ø of 7 d); +356 steps (Ø of 30 d) |
| Wang et al. (2020)/China [106] | Participants (≥40 years) from Step Study 2018 in Changsha, China | (...) to determine if there was any change in daily steps and examine risk factors for frequent low daily steps during the COVID-19 epidemic | n = 3544 (1226 female); 51.6 ± 8.9 years | DB: Accelerometer sensor in the smartphone via WeChat | T0: 22 December 2019–20 January 2020 T1: 22 January–20 February 2020 | Step count: − | Step count: −2657 steps/d |
| Wilson et al. (2021)/USA [107] | Undergraduates enrolled in general health and wellness classes | (...) to examine the impact that COVID-19 had on PA among college students by comparing temporal changes in PA over the course of the US spring academic semester | n = 187 (128 female); 20.9 ± 1.5 years | SR: GPAQ | T0: January 2020 T1: April 2020 | MPA, VPA, MET, active travel, strength training: − | male: MPA: −60 min/week VPA: −75.7 min/week MET: 845.7 min/week AT: −174 min/week ST: −0.6 days/week female:MPA: −52.7 min/week VPA: −18.8 min/weekv MET: 361.1 min/week AT: −266.7 min/week ST: −0.1 days/week |
| Woodruff et al. (2021)/Canada [108] | Participants (≥18 years) who regularly wear activity trackers | (...) to investigate how PA changed within the first month of the COVID-19 pandemic | n = 121 (96 female); 36.2 ± 13.12 years | SR: Data from wearable activity tracker filled into a calendar | T0 and T1 were determined for each participant individually (M T1 = 16 March 2020, SD = 4.7 days, range = 13–31 days). | Step count: − | steps: −1012 steps/day |
| Wunsch et al. (2021)/Germany [109] | Children and adolescents (4–17 years) living in Germany | (...) to examine the direct influence of the COVID-19 lockdown on PA in a nationwide child and adolescent sample in Germany | n = 1711 (961 female); 10.36 ± 4.04 years | SR: MoMo-PAQ | T0: August 2018–March 2020 T1: April 2020 | days/week with at least 60 min of PA (4–10-year-olds, 11–17-year-old girls): + 11–17-year-old boys: no change | days/week with at least 60 min of PA: 4–10-year-old boys: +0.65 days/week 11–17-year-old boys: +0.18 days/week 4–10-year-old girls: +0.65 days/week 11–17-year-old girls: +0.41 days/week |
| Yang and Koenigstorfer (2020)/USA [110] | Healthy U.S. residents (18–65 years) | (...) to investigate the change in PA during the Covid-19-caused lockdown with a focus on PA app use and the features of these apps | n = 431 (211 female); 39.1 ± 10.6 years | SR: IPAQ-SF | T0: 12 March–17 March 2020 T1: 4 weeks after restrictions implemented, different in states; Ø: 43.7 (±4.7) days | MPA, VPA, active PA, PA MET: − walking: no sig. change | MPA: −10.4 min/day VPA: −8.5 min/day active PA: −23.4 min/day PA MET: −605.1 MET min/week walking: −4.5 min/day |
| Zenic et al. (2020)/Croatia [53] | Adolescents attending high school from Split-Dalmatia County | (...) to explore the changes in PALs that occurred because of COVID-19 and social distancing measures in adolescents from Croatia (...) | n = 823 (no gender provided); 16.5 ± 2.1 years | SR: PAQ-A | T0: 1–10 March 2020 T1: 5–10 April 2020 | PAL: − | PAL: −0.34 |
| Zheng et al. (2020)/China [54] | No information provided | (...) to investigate PA levels in Hong Kong young adults during the COVID-19 pandemic and the changes after the COVID-19 outbreak | n = 70 young adults; age not reported | SR: IPAQ | T0: 2019 T1: not provided | MPA, VPA, walking: − | MPA: −5.7 min/day VPA: −3.5 min/day walking: −19.9 min/day |
| Znazen et al. (2021)/Saudi Arabia [111] | Saudi Arabian university students (18–22 years) | (...) to determine the impact of COVID-19-induced home confinement on lifestyle behaviors | n = 144 (90 female); 19.3 ± 1.8 years | SR: SLIQ | T0 & T1: Before and during 75 days of confinement (not specified when) | Total PA: − | Total PA: −3.08 points (activity raw score) |
3.3. Risk of Bias within Studies
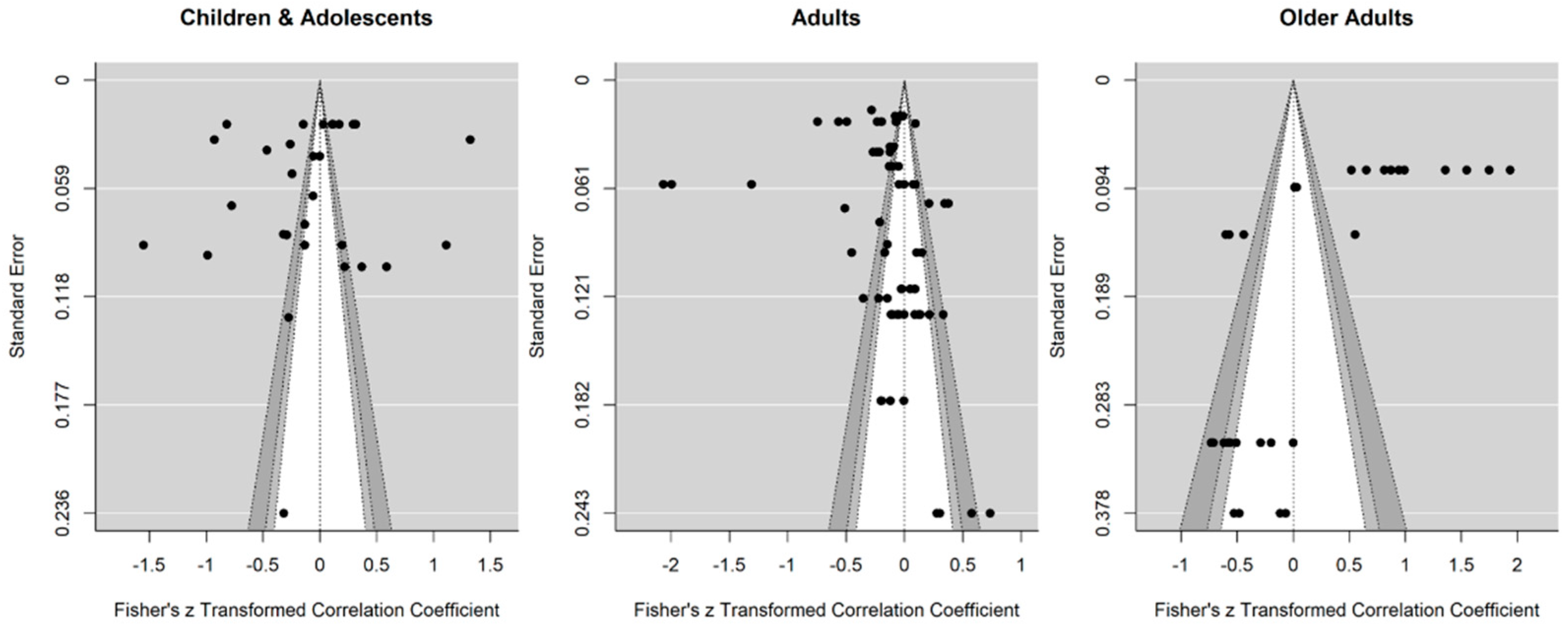
3.4. Risk of Bias across Studies
3.5. Results of Individual Studies
3.6. Results of Synthesis
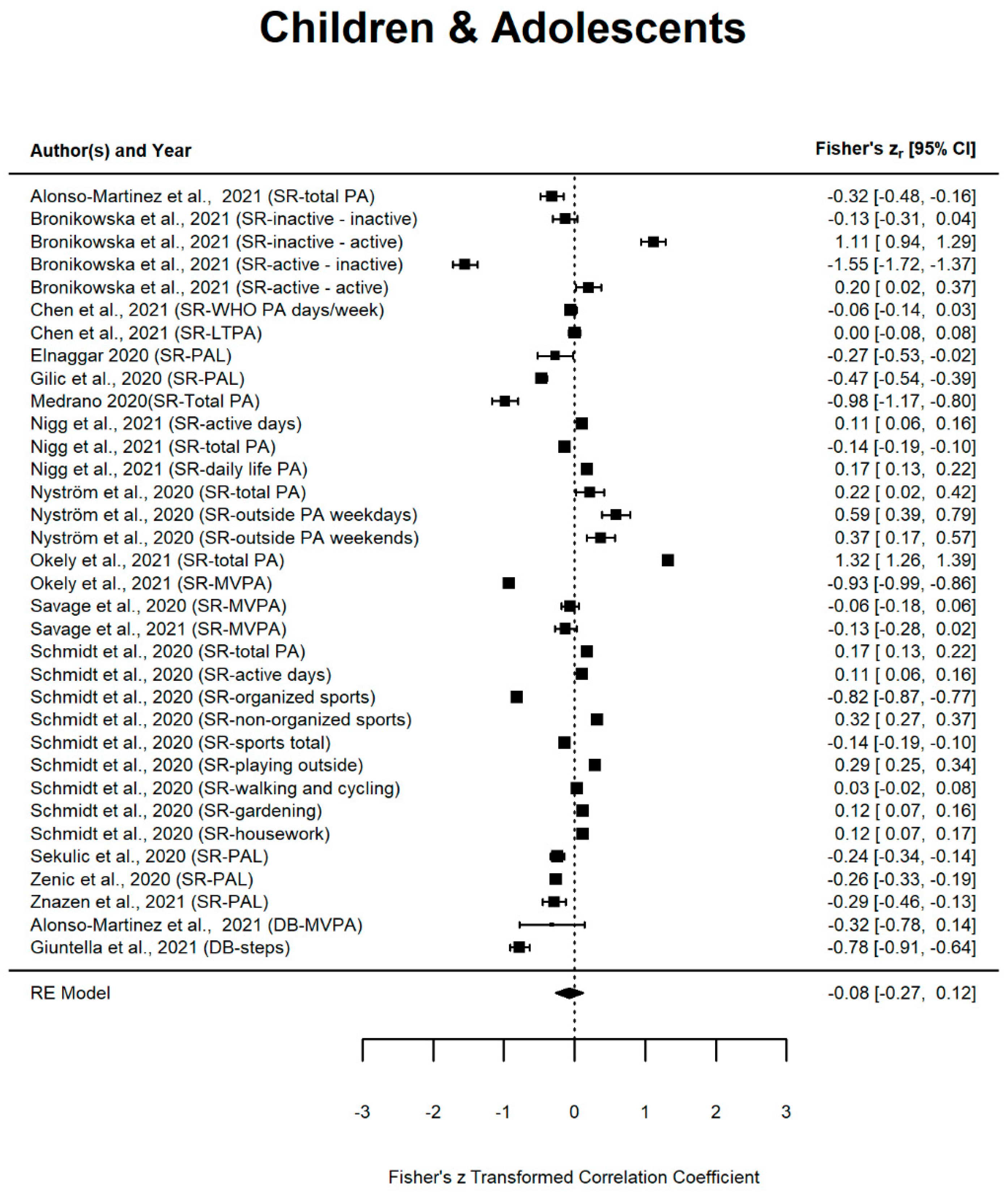
3.6.1. Children and Adolescents
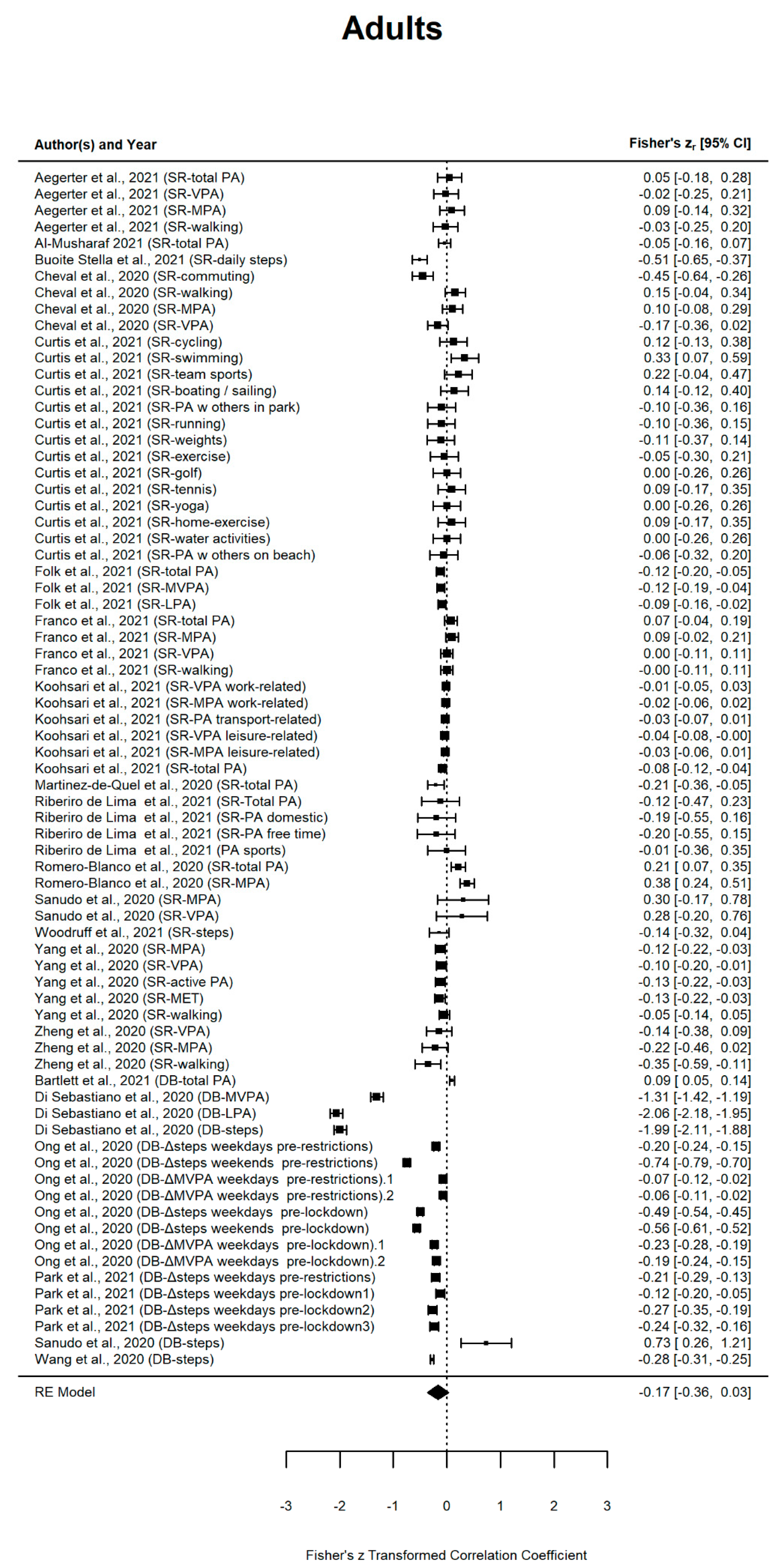
3.6.2. Adults
3.6.3. Older Adults
3.6.4. Results Based on Mixed-Age Groups
3.7. Meta-Analysis
4. Discussion
4.1. Changes in PA according to Age
4.1.1. Children and Adolescents
4.1.2. Adults
4.1.3. Older Adults
4.1.4. Larger Age Ranges
4.2. Change in PA according to Measurement Methods
4.3. Change in PA in Males and Females
4.4. Additional Influencing Factors on PA during the Covid-19 Pandemic
4.5. Summary of Discussion and Comparison
4.6. Strengths and Limitations
5. Conclusions and Implications
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Listings of WHO’s Response to COVID-19. Available online: https://www.who.int/news/item/29-06-2020-covidtimeline (accessed on 5 May 2021).
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. WHO Announces COVID-19 Outbreak a Pandemic. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic (accessed on 12 February 2022).
- Johns Hopkins University, Center for Systems Science and Engineering. COVID-19 Dashboard. Available online: https://gisanddata.maps.arcgis.com/apps/dashboards/bda7594740fd40299423467b48e9ecf6 (accessed on 12 February 2022).
- European Centre for Disease Prevention and Control. Data on Country Response Measures to COVID-19. Available online: https://www.ecdc.europa.eu/en/publications-data/download-data-response-measures-covid-19 (accessed on 28 May 2021).
- Brazendale, K.; Beets, M.W.; Weaver, R.G.; Pate, R.R.; Turner-McGrievy, G.M.; Kaczynski, A.T.; Chandler, J.L.; Bohnert, A.; von Hippel, P.T. Understanding differences between summer vs. school obesogenic behaviors of children: The structured days hypothesis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 100. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 home confinement on eating behaviour and physical activity: Results of the ECLB-COVID19 international online survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical activity change during COVID-19 confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef] [PubMed]
- Franco, I.; Bianco, A.; Bonfiglio, C.; Sorino, P.; Mirizzi, A.; Campanella, A.; Buongiorno, C.; Liuzzi, R.; Osella, A.R. Decreased levels of physical activity: Results from a cross-sectional study in southern Italy during the COVID-19 lockdown. J. Sports Med. Phys. Fit. 2021, 61, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Ruíz-Roso, M.B.; de Carvalho Padilha, P.; Matilla-Escalante, D.C.; Brun, P.; Ulloa, N.; Acevedo-Correa, D.; Ferreira Peres, W.A.; Martorell, M.; Bousquet Carrilho, T.R.; De Oliveira Cardoso, L.; et al. Changes of physical activity and ultra-processed food consumption in adolescents from different countries during Covid-19 pandemic: An observational study. Nutrients 2020, 12, 2289. [Google Scholar] [CrossRef] [PubMed]
- González, K.; Fuentes, J.; Márquez, J.L. Physical inactivity, sedentary behavior and chronic diseases. Korean J. Fam. Med. 2017, 38, 111–115. [Google Scholar] [CrossRef] [Green Version]
- Gaetano, A. Relationship between physical inactivity and effects on individual health status. J. Phys. Educ. Sport 2016, 16, 1069–1074. [Google Scholar] [CrossRef]
- Knight, J.A. Physical inactivity: Associated diseases and disorders. Ann. Clin. Lab. Sci. 2012, 42, 320–337. [Google Scholar]
- Puccinelli, P.J.; da Costa, T.S.; Seffrin, A.; de Lira, C.A.B.; Vancini, R.L.; Nikolaidis, P.T.; Knechtle, B.; Rosemann, T.; Hill, L.; Andrade, M.S. Reduced level of physical activity during COVID-19 pandemic is associated with depression and anxiety levels: An internet-based survey. BMC Public Health 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Löllgen, H.; Löllgen, D. Risikoreduktion kardiovaskulärer Erkrankungen durch körperliche Aktivität. Internist 2011, 53, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Reiner, M.; Niermann, C.; Jekauc, D.; Woll, A. Long-term health benefits of physical activity—A systematic review of longitudinal studies. BMC Public Health 2013, 13, 813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhodes, R.E.; Janssen, I.; Bredin, S.S.; Warburton, D.E.; Bauman, A. Physical activity: Health impact, prevalence, correlates and interventions. Psychol. Health 2017, 32, 942–975. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.-H.; Meyer, A.; Langguth, N. Körperliche Aktivität und psychische Gesundheit. Bundesgesundheitsblatt-Gesundheitsforsch.-Gesundheitsschutz 2012, 55, 55–65. [Google Scholar] [CrossRef]
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during Covid-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef]
- de Sousa, R.A.L.; Improta-Caria, A.C.; Aras-Júnior, R.; de Oliveira, E.M.; Soci, Ú.P.R.; Cassilhas, R.C. Physical exercise effects on the brain during COVID-19 pandemic: Links between mental and cardiovascular health. Neurol. Sci. 2021, 42, 1325–1334. [Google Scholar] [CrossRef]
- Nigro, E.; Polito, R.; Alfieri, A.; Mancini, A.; Imperlini, E.; Elce, A.; Krustrup, P.; Orrù, S.; Buono, P.; Daniele, A. Molecular mechanisms involved in the positive effects of physical activity on coping with COVID-19. Eur. J. Appl. Physiol. 2020, 120, 2569–2582. [Google Scholar] [CrossRef]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]
- López-Valenciano, A.; Suárez-Iglesias, D.; Sanchez-Lastra, M.A.; Ayán, C. Impact of COVID-19 pandemic on university students’ physical activity levels: An early systematic review. Front. Psychol. 2021, 11, 3787. [Google Scholar] [CrossRef]
- Rossi, L.; Behme, N.; Breuer, C. Physical activity of children and adolescents during the COVID-19 pandemic—A scoping review. Int. J. Environ. Res. Public Health 2021, 18, 11440. [Google Scholar] [CrossRef]
- de Looze, M.; Elgar, F.J.; Currie, C.; Kolip, P.; Stevens, G.W. Gender inequality and sex differences in physical fighting, physical activity, and injury among adolescents across 36 countries. J. Adolesc. Health 2019, 64, 657–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boraita, R.J.; Ibort, E.G.; Torres, J.M.D.; Alsina, D.A. Gender differences relating to lifestyle habits and health-related quality of life of adolescents. Child Indic. Res. 2020, 13, 1937–1951. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Corder, K.; Winpenny, E.; Love, R.; Brown, H.E.; White, M.; Van Sluijs, E. Change in physical activity from adolescence to early adulthood: A systematic review and meta-analysis of longitudinal cohort studies. Br. J. Sports Med. 2019, 53, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Westerterp, K.R. Changes in physical activity over the lifespan: Impact on body composition and sarcopenic obesity. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2018, 19 (Suppl. 1), 8–13. [Google Scholar] [CrossRef] [Green Version]
- Varma, V.R.; Dey, D.; Leroux, A.; Di, J.; Urbanek, J.; Xiao, L.; Zipunnikov, V. Re-evaluating the effect of age on physical activity over the lifespan. Prev. Med. 2017, 101, 102–108. [Google Scholar] [CrossRef]
- Hall, K.S.; Cohen, H.J.; Pieper, C.F.; Fillenbaum, G.G.; Kraus, W.E.; Huffman, K.M.; Cornish, M.A.; Shiloh, A.; Flynn, C.; Sloane, R.; et al. Physical performance across the adult life span: Correlates with age and physical activity. J. Gerontol. Ser. A 2016, 72, 572–578. [Google Scholar] [CrossRef] [Green Version]
- Prince, S.A.; Adamo, K.B.; Hamel, M.E.; Hardt, J.; Gorber, S.C.; Tremblay, M. A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 56. [Google Scholar] [CrossRef] [Green Version]
- Dowd, K.P.; Szeklicki, R.; Minetto, M.A.; Murphy, M.H.; Polito, A.; Ghigo, E.; Van Der Ploeg, H.; Ekelund, U.; Maciaszek, J.; Stemplewski, R.; et al. A systematic literature review of reviews on techniques for physical activity measurement in adults: A DEDIPAC study. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 1–33. [Google Scholar] [CrossRef]
- Reilly, J.J.; Penpraze, V.; Hislop, J.; Davies, G.; Grant, S.; Paton, J. Objective measurement of physical activity and sedentary behaviour: Review with new data. Arch. Dis. Child. 2008, 93, 614–619. [Google Scholar] [CrossRef]
- Rudolf, K.; Schaller, A.; Frick, F.; Grieben, C.; Froböse, I. Erfassung der Selbsteinschätzung körperlicher Aktivität von jungen Erwachsenen. Prävent. Gesundh. 2016, 11, 20–26. [Google Scholar] [CrossRef]
- Hagstromer, M.; Ainsworth, B.E.; Oja, P.; Sjostrom, M. Comparison of a subjective and an objective measure of physical activity in a population sample. J. Phys. Act. Health 2010, 7, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014. [Google Scholar]
- RStudio Team. RStudio: Integrated Development for R; RStudio: Boston, MA, USA, 2020. [Google Scholar]
- National Heart, Lung, and Blood Institute. Study Quality Assessment Tools: Quality Assessment Tool for before-after (Pre-Post) Studies with No Control Group. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 29 May 2021).
- Raaijmakers, L.C.H.; Pouwels, S.; Thomassen, S.E.M.; Nienhuijs, S.W. Quality of life and bariatric surgery: A systematic review of short- and long-term results and comparison with community norms. Eur. J. Clin. Nutr. 2016, 71, 441–449. [Google Scholar] [CrossRef]
- Lenhard, W.; Lenhard, A. Computation of effect sizes. Psychometrica 2017. [Google Scholar] [CrossRef]
- Cochran, W.G. The combination of estimates from different experiments. Biometrics 1954, 10, 101–129. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- Fearnbach, S.N.; Flanagan, E.W.; Höchsmann, C.; Beyl, R.A.; Altazan, A.D.; Martin, C.K.; Redman, L.M. Factors protecting against a decline in physical activity during the COVID-19 pandemic. Med. Sci. Sports Exerc. 2021, 53, 1391–1399. [Google Scholar] [CrossRef]
- Gallo, L.A.; Gallo, T.F.; Young, S.L.; Moritz, K.M.; Akison, L.K. The impact of isolation measures due to COVID-19 on energy intake and physical activity levels in Australian university students. Nutrients 2020, 12, 1865. [Google Scholar] [CrossRef]
- Bohn, L.; Barros, D.; Borges-Machado, F.; Carrapatoso, S.; Pizarro, A.N.; Carvalho, J. Active older adults keep aerobic capacity and experience small reductions in body strength during confinement due to COVID-19 outbreak. J. Aging Phys. Act. 2021, 29, 1034–1041. [Google Scholar] [CrossRef] [PubMed]
- Cordovil, R.; Ribeiro, L.; Moreira, M.; Pombo, A.; Rodrigues, L.P.; Luz, C.; Veiga, G.; Lopes, F. Effects of the COVID-19 pandemic on preschool children and preschools in Portugal. J. Phys. Educ. Sport 2021, 21, 492–499. [Google Scholar] [CrossRef]
- Okely, A.D.; Kariippanon, K.E.; Guan, H.; Taylor, E.K.; Suesse, T.; Cross, P.L.; Chong, K.H.; Suherman, A.; Turab, A.; Staiano, A.E.; et al. Global effect of COVID-19 pandemic on physical activity, sedentary behaviour and sleep among 3- to 5-year-old children: A longitudinal study of 14 countries. BMC Public Health 2021, 21, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Al-Musharaf, S.; Aljuraiban, G.; Bogis, R.; Alnafisah, R.; Aldhwayan, M.; Tahrani, A. Lifestyle changes associated with COVID-19 quarantine among young Saudi women: A prospective study. PLoS ONE 2021, 16, e0250625. [Google Scholar] [CrossRef] [PubMed]
- de Lima, J.G.R.; Abud, G.F.; de Freitas, E.C.; Júnior, C.R.B. Effects of the COVID-19 pandemic on the global health of women aged 50 to 70 years. Exp. Gerontol. 2021, 150, 111349. [Google Scholar] [CrossRef] [PubMed]
- Zenic, N.; Taiar, R.; Gilic, B.; Blazevic, M.; Maric, D.; Pojskic, H.; Sekulic, D. Levels and changes of physical activity in adolescents during the COVID-19 pandemic: Contextualizing urban vs. rural living environment. Appl. Sci. 2020, 10, 3997. [Google Scholar] [CrossRef]
- Zheng, C.; Huang, W.Y.; Sheridan, S.; Sit, C.H.-P.; Chen, X.-K.; Wong, S.H.-S. COVID-19 pandemic brings a sedentary lifestyle in young adults: A cross-sectional and longitudinal study. Int. J. Environ. Res. Public Health 2020, 17, 6035. [Google Scholar] [CrossRef]
- Mishra, R.; Park, C.; York, M.; Kunik, M.; Wung, S.-F.; Naik, A.; Najafi, B. Decrease in mobility during the COVID-19 pandemic and its association with increase in depression among older adults: A longitudinal remote mobility monitoring using a wearable sensor. Sensors 2021, 21, 3090. [Google Scholar] [CrossRef]
- To, Q.G.; Duncan, M.J.; Van Itallie, A.; Vandelanotte, C. Impact of COVID-19 on physical activity among 10,000 steps members and engagement with the program in Australia: Prospective study. J. Med. Internet Res. 2021, 23, e23946. [Google Scholar] [CrossRef]
- Nyström, C.D.; Alexandrou, C.; Henström, M.; Nilsson, E.; Okely, A.D.; El Masri, S.W.; Löf, M. International study of movement behaviors in the early years (SUNRISE): Results from SUNRISE Sweden’s pilot and COVID-19 study. Int. J. Environ. Res. Public Health 2020, 17, 8491. [Google Scholar] [CrossRef]
- McCarthy, H.; Potts, H.W.W.; Fisher, A. Physical activity behavior before, during, and after COVID-19 restrictions: Longitudinal smartphone-tracking study of adults in the United Kingdom. J. Med. Internet Res. 2021, 23, e23701. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voss, C.; Dean, P.H.; Gardner, R.F.; Duncombe, S.L.; Harris, K.C. Validity and reliability of the Physical Activity Questionnaire for Children (PAQ-C) and Adolescents (PAQ-A) in individuals with congenital heart disease. PLoS ONE 2017, 12, e0175806. [Google Scholar] [CrossRef] [PubMed]
- Laeremans, M.; Dons, E.; Avila-Palencia, I.; Carrasco-Turigas, G.; Orjuela, J.P.; Anaya, E.; Brand, C.; Cole-Hunter, T.; de Nazelle, A.; Götschi, T.; et al. Physical activity and sedentary behaviour in daily life: A comparative analysis of the Global Physical Activity Questionnaire (GPAQ) and the SenseWear armband. PLoS ONE 2017, 12, e0177765. [Google Scholar] [CrossRef] [Green Version]
- Jekauc, D.; Wagner, M.; Kahlert, D.; Woll, A. Reliability and validity of MoMo-Physical-Activity-Questionnaire for Adolescents (MoMo-AFB). Diagnostica 2013, 59, 100–111. [Google Scholar] [CrossRef] [Green Version]
- Munasinghe, S.; Sperandei, S.; Freebairn, L.; Conroy, E.; Jani, H.; Marjanovic, S.; Page, A. The impact of physical distancing policies during the COVID-19 pandemic on health and well-being among Australian adolescents. J. Adolesc. Health 2020, 67, 653–661. [Google Scholar] [CrossRef]
- Chen, Y.; Osika, W.; Henriksson, G.; Dahlstrand, J.; Friberg, P. Impact of COVID-19 pandemic on mental health and health behaviors in Swedish adolescents. Scand. J. Public Health 2021, 50, 26–32. [Google Scholar] [CrossRef]
- Suzuki, Y.; Maeda, N.; Hirado, D.; Shirakawa, T.; Urabe, Y. Physical activity changes and its risk factors among community-dwelling Japanese older adults during the COVID-19 epidemic: Associations with subjective well-being and health-related quality of life. Int. J. Environ. Res. Public Health 2020, 17, 6591. [Google Scholar] [CrossRef]
- Hino, K.; Asami, Y. Change in walking steps and association with built environments during the COVID-19 state of emergency: A longitudinal comparison with the first half of 2019 in Yokohama, Japan. Health Place 2021, 69, 102544. [Google Scholar] [CrossRef]
- Wikipedia. COVID-19 Lockdowns. Available online: https://en.wikipedia.org/wiki/COVID-19_lockdowns#Countries_and_territories_without_lockdowns (accessed on 6 December 2021).
- Aegerter, A.M.; Deforth, M.; Sjøgaard, G.; Johnston, V.; Volken, T.; Luomajoki, H.; Dratva, J.; Dressel, H.; Distler, O.; Melloh, M.; et al. No evidence for a decrease in physical activity among swiss office workers during COVID-19: A longitudinal study. Front. Psychol. 2021, 12. [Google Scholar] [CrossRef]
- Alonso-Martínez, A.; Ramírez-Vélez, R.; García-Alonso, Y.; Izquierdo, M.; García-Hermoso, A. Physical activity, sedentary behavior, sleep and self-regulation in Spanish preschoolers during the COVID-19 lockdown. Int. J. Environ. Res. Public Health 2021, 18, 693. [Google Scholar] [CrossRef] [PubMed]
- Baceviciene, M.; Jankauskiene, R. Changes in sociocultural attitudes towards appearance, body image, eating attitudes and behaviours, physical activity, and quality of life in students before and during COVID-19 lockdown. Appetite 2021, 166, 105452. [Google Scholar] [CrossRef]
- Barone Gibbs, B.; Kline, C.E.; Huber, K.A.; Paley, J.L.; Perera, S. Covid-19 shelter-at-home and work, lifestyle and well-being in desk workers. Occup. Med. 2021, 71, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, L.; Brady, J.J.R.; Farrow, M.; Kim, S.; Bindoff, A.; Fair, H.; Vickers, J.C.; Sinclair, D. Change in modifiable dementia risk factors during COVID-19 lockdown: The experience of over 50s in Tasmania, Australia. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2021, 7, e12169. [Google Scholar] [CrossRef] [PubMed]
- Bronikowska, M.; Krzysztoszek, J.; Łopatka, M.; Ludwiczak, M.; Pluta, B. Comparison of physical activity levels in youths before and during a pandemic lockdown. Int. J. Environ. Res. Public Health 2021, 18, 5139. [Google Scholar] [CrossRef] [PubMed]
- Buoite Stella, A.; Ajčević, M.; Furlanis, G.; Cillotto, T.; Menichelli, A.; Accardo, A.; Manganotti, P. Smart technology for physical activity and health assessment during COVID-19 lockdown. J. Sports Med. Phys. Fit. 2021, 61, 452–460. [Google Scholar] [CrossRef]
- Chaffee, B.W.; Cheng, J.; Couch, E.T.; Hoeft, K.S.; Halpern-Felsher, B. Adolescents’ substance use and physical activity before and during the COVID-19 pandemic. JAMA Pediatr. 2021, 175, 715–722. [Google Scholar] [CrossRef]
- Cheval, B.; Sivaramakrishnan, H.; Maltagliati, S.; Fessler, L.; Forestier, C.; Sarrazin, P.; Orsholits, D.; Chalabaev, A.; Sander, D.; Ntoumanis, N.; et al. Relationships between changes in self-reported physical activity, sedentary behaviour and health during the coronavirus (COVID-19) pandemic in France and Switzerland. J. Sports Sci. 2020, 39, 699–704. [Google Scholar] [CrossRef]
- Curtis, R.G.; Olds, T.; Ferguson, T.; Fraysse, F.; Dumuid, D.; Esterman, A.; Hendrie, G.A.; Brown, W.J.; Lagiseti, R.; Maher, C.A. Changes in diet, activity, weight, and wellbeing of parents during COVID-19 lockdown. PLoS ONE 2021, 16, e0248008. [Google Scholar] [CrossRef]
- Di Sebastiano, K.M.; Chulak-Bozzer, T.; Vanderloo, L.M.; Faulkner, G. Don’t walk so close to me: Physical distancing and adult physical activity in Canada. Front. Psychol. 2020, 11, 1895. [Google Scholar] [CrossRef]
- Ding, D.; Cheng, M.; del Cruz, B.P.; Lin, T.; Sun, S.; Zhang, L.; Yang, Q.; Ma, Z.; Wang, J.; Jia, Y.; et al. How COVID-19 lockdown and reopening affected daily steps: Evidence based on 164,630 person-days of prospectively collected data from Shanghai, China. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Elnaggar, R.K.; Alqahtani, B.A.; Mahmoud, W.S.; ElFakharany, M.S. Physical activity in adolescents during the social distancing policies of the COVID-19 pandemic. Asia Pac. J. Public Health 2020, 32, 491–494. [Google Scholar] [CrossRef] [PubMed]
- Esain, I.; Gil, S.; Duñabeitia, I.; Rodriguez-Larrad, A.; Bidaurrazaga-Letona, I. Effects of COVID-19 lockdown on physical activity and health-related quality of life in older adults who regularly exercise. Sustainability 2021, 13, 3771. [Google Scholar] [CrossRef]
- Folk, A.L.; Wagner, B.E.; Hahn, S.L.; Larson, N.; Barr-Anderson, D.J.; Neumark-Sztainer, D. Changes to physical activity during a global pandemic: A mixed methods analysis among a diverse population-based sample of emerging adults in the U.S. Int. J. Environ. Res. Public Health 2021, 18, 3674. [Google Scholar] [CrossRef]
- Franco, E.; Urosa, J.; Barakat, R.; Refoyo, I. Physical activity and adherence to the Mediterranean diet among Spanish employees in a health-promotion program before and during the COVID-19 pandemic: The sanitas-healthy cities challenge. Int. J. Environ. Res. Public Health 2021, 18, 2735. [Google Scholar] [CrossRef]
- Gallego-Gómez, J.I.; Campillo-Cano, M.; Carrión-Martínez, A.; Balanza, S.; Rodríguez-González-Moro, M.T.; Simonelli-Muñoz, A.J.; Rivera-Caravaca, J.M. The COVID-19 pandemic and its impact on homebound nursing students. Int. J. Environ. Res. Public Health 2020, 17, 7383. [Google Scholar] [CrossRef] [PubMed]
- Gilic, B.; Ostojic, L.; Corluka, M.; Volaric, T.; Sekulic, D. Contextualizing parental/familial influence on physical activity in adolescents before and during COVID-19 pandemic: A prospective analysis. Children 2020, 7, 125. [Google Scholar] [CrossRef]
- Gilic, B.; Zenic, N.; Separovic, V.; Savicevic, A.J.; Sekulic, D. Evidencing the influence of pre-pandemic sports participation and substance misuse on physical activity during the COVID-19 lockdown: A prospective analysis among older adolescents. Int. J. Occup. Med. Environ. Health 2021, 34, 151–163. [Google Scholar] [CrossRef]
- Giuntella, O.; Hyde, K.; Saccardo, S.; Sadoff, S. Lifestyle and mental health disruptions during COVID-19. Proc. Natl. Acad. Sci. USA 2021, 118, e2016632118. [Google Scholar] [CrossRef]
- He, M.; Xian, Y.; Lv, X.; He, J.; Ren, Y. Changes in body weight, physical activity, and lifestyle during the semi-lockdown period after the outbreak of COVID-19 in China: An online survey. Disaster Med. Public Health Prep. 2020, 15, e23–e28. [Google Scholar] [CrossRef]
- Koohsari, M.J.; Nakaya, T.; McCormack, G.R.; Shibata, A.; Ishii, K.; Oka, K. Changes in workers’ sedentary and physical activity behaviors in response to the COVID-19 pandemic and their relationships with fatigue: Longitudinal online study. JMIR Public Health Surveill. 2021, 7, e26293. [Google Scholar] [CrossRef]
- Martínez-De-Quel, Ó.; Suárez-Iglesias, D.; López-Flores, M.; Pérez, C.A. Physical activity, dietary habits and sleep quality before and during COVID-19 lockdown: A longitudinal study. Appetite 2020, 158, 105019. [Google Scholar] [CrossRef] [PubMed]
- Medrano, M.; Cadenas-Sanchez, C.; Oses, M.; Arenaza, L.; Amasene, M.; Labayen, I. Changes in lifestyle behaviours during the COVID-19 confinement in Spanish children: A longitudinal analysis from the MUGI project. Pediatr. Obes. 2020, 16, e12731. [Google Scholar] [CrossRef] [PubMed]
- Miyahara, S.; Tanikawa, Y.; Hirai, H.; Togashi, S. Impact of the state of emergency enacted due to the COVID-19 pandemic on the physical activity of the elderly in Japan. J. Phys. Ther. Sci. 2021, 33, 345–350. [Google Scholar] [CrossRef]
- Nigg, C.; Oriwol, D.; Wunsch, K.; Burchartz, A.; Kolb, S.; Worth, A.; Woll, A.; Niessner, C. Population density predicts youth’s physical activity changes during Covid-19—Results from the MoMo study. Health Place 2021, 70, 102619. [Google Scholar] [CrossRef] [PubMed]
- Obuchi, S.P.; Kawai, H.; Ejiri, M.; Ito, K.; Murakawa, K. Change in outdoor walking behavior during the coronavirus disease pandemic in Japan: A longitudinal study. Gait Posture 2021, 88, 42–46. [Google Scholar] [CrossRef]
- Okely, J.A.; Corley, J.; Welstead, M.; Taylor, A.M.; Page, D.; Skarabela, B.; Redmond, P.; Cox, S.R.; Russ, T.C. Change in physical activity, sleep quality, and psychosocial variables during COVID-19 lockdown: Evidence from the Lothian Birth Cohort 1936. Int. J. Environ. Res. Public Health 2020, 18, 210. [Google Scholar] [CrossRef]
- Ong, J.L.; Lau, T.; Massar, S.A.A.; Chong, Z.T.; Ng, B.K.L.; Koek, D.; Zhao, W.; Yeo, B.T.T.; Cheong, K.; Chee, M.W.L. COVID-19-related mobility reduction: Heterogenous effects on sleep and physical activity rhythms. Sleep 2020, 44, zsaa179. [Google Scholar] [CrossRef]
- Park, J.-H.; Yoo, E.; Kim, Y.; Lee, J.-M. What happened pre- and during COVID-19 in South Korea? Comparing physical activity, sleep time, and body weight status. Int. J. Environ. Res. Public Health 2021, 18, 5863. [Google Scholar] [CrossRef]
- Pérez, L.M.; Castellano-Tejedor, C.; Cesari, M.; Soto-Bagaria, L.; Ars, J.; Zambom-Ferraresi, F.; Baró, S.; Díaz-Gallego, F.; Vilaró, J.; Enfedaque, M.; et al. Depressive symptoms, fatigue and social relationships influenced physical activity in frail older community-dwellers during the Spanish lockdown due to the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2021, 18, 808. [Google Scholar] [CrossRef]
- Richardson, D.L.; Duncan, M.J.; Clarke, N.D.; Myers, T.D.; Tallis, J. The influence of COVID-19 measures in the United Kingdom on physical activity levels, perceived physical function and mood in older adults: A survey-based observational study. J. Sports Sci. 2020, 39, 887–899. [Google Scholar] [CrossRef] [PubMed]
- Romero-Blanco, C.; Rodríguez-Almagro, J.; Onieva-Zafra, M.D.; Parra-Fernández, M.L.; del Prado-Laguna, M.C.; Hernández-Martínez, A. Physical activity and sedentary lifestyle in university students: Changes during confinement due to the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6567. [Google Scholar] [CrossRef] [PubMed]
- Sañudo, B.; Fennell, C.; Sánchez-Oliver, A.J. Objectively-assessed physical activity, sedentary behavior, smartphone use, and sleep patterns pre- and during-COVID-19 quarantine in young adults from Spain. Sustainability 2020, 12, 5890. [Google Scholar] [CrossRef]
- Savage, M.J.; Hennis, P.J.; Magistro, D.; Donaldson, J.; Healy, L.C.; James, R.M. Nine months into the COVID-19 pandemic: A longitudinal study showing mental health and movement behaviours are impaired in UK students. Int. J. Environ. Res. Public Health 2021, 18, 2930. [Google Scholar] [CrossRef]
- Savage, M.J.; James, R.; Magistro, D.; Donaldson, J.; Healy, L.C.; Nevill, M.; Hennis, P.J. Mental health and movement behaviour during the COVID-19 pandemic in UK university students: Prospective cohort study. Ment. Health Phys. Act. 2020, 19, 100357. [Google Scholar] [CrossRef]
- Schmidt, S.C.E.; Anedda, B.; Burchartz, A.; Eichsteller, A.; Kolb, S.; Nigg, C.; Niessner, C.; Oriwol, D.; Worth, A.; Woll, A. Physical activity and screen time of children and adolescents before and during the COVID-19 lockdown in Germany: A natural experiment. Sci. Rep. 2020, 10, 21780. [Google Scholar] [CrossRef]
- Sekulic, D.; Blazevic, M.; Gilic, B.; Kvesic, I.; Zenic, N. Prospective analysis of levels and correlates of physical activity during COVID-19 pandemic and imposed rules of social distancing: Gender specific study among adolescents from southern Croatia. Sustainability 2020, 12, 4072. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, Y.; Bennell, K.; White, D.K.; Wei, J.; Wu, Z.; He, H.; Liu, S.; Luo, X.; Hu, S.; et al. Physical distancing measures and walking activity in middle-aged and older residents in Changsha, China, during the COVID-19 epidemic period: Longitudinal observational study. J. Med. Internet Res. 2020, 22, e21632. [Google Scholar] [CrossRef]
- Wilson, O.W.; Holland, K.E.; Elliott, L.D.; Duffey, M.; Bopp, M. The Impact of the COVID-19 pandemic on US college students’ physical activity and mental health. J. Phys. Act. Health 2021, 18, 272–278. [Google Scholar] [CrossRef]
- Woodruff, S.J.; Coyne, P.; St-Pierre, E. Stress, physical activity, and screen-related sedentary behaviour within the first month of the COVID-19 pandemic. Appl. Psychol. Health Well-Being 2021, 13, 454–468. [Google Scholar] [CrossRef]
- Wunsch, K.; Nigg, C.; Niessner, C.; Schmidt, S.C.; Oriwol, D.; Hanssen-Doose, A.; Burchartz, A.; Eichsteller, A.; Kolb, S.; Worth, A.; et al. The impact of COVID-19 on the interrelation of physical activity, screen time and health-related quality of life in children and adolescents in Germany: Results of the Motorik-Modul study. Children 2021, 8, 98. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Koenigstorfer, J. Determinants of physical activity maintenance during the COVID-19 pandemic: A focus on fitness apps. Transl. Behav. Med. 2020, 10, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Znazen, H.; Slimani, M.; Bragazzi, N.L.; Tod, D. The relationship between cognitive function, lifestyle behaviours and perception of stress during the COVID-19 induced confinement: Insights from correlational and mediation analyses. Int. J. Environ. Res. Public Health 2021, 18, 3194. [Google Scholar] [CrossRef] [PubMed]
- Guan, H.; Okely, A.D.; Aguilar-Farias, N.; Del Pozo Cruz, B.; Draper, C.E.; El Hamdouchi, A.; Florindo, A.A.; Jáuregui, A.; Katzmarzyk, P.T.; Kontsevaya, A.; et al. Promoting healthy movement behaviours among children during the COVID-19 pandemic. Lancet Child Adolesc. Health 2020, 4, 416–418. [Google Scholar] [CrossRef]
- Androutsos, O.; Perperidi, M.; Georgiou, C.; Chouliaras, G. Lifestyle changes and determinants of children’s and adolescents’ body weight increase during the first COVID-19 lockdown in Greece: The COV-EAT study. Nutrients 2021, 13, 930. [Google Scholar] [CrossRef]
- Dunton, G.F.; Do, B.; Wang, S.D. Early effects of the COVID-19 pandemic on physical activity and sedentary behavior in children living in the U.S. BMC Public Health 2020, 20, 1351. [Google Scholar] [CrossRef]
- Moore, S.A.; Faulkner, G.; Rhodes, R.E.; Brussoni, M.; Chulak-Bozzer, T.; Ferguson, L.J.; Mitra, R.; O’Reilly, N.; Spence, J.C.; Vanderloo, L.M.; et al. Impact of the COVID-19 virus outbreak on movement and play behaviours of Canadian children and youth: A national survey. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 85. [Google Scholar] [CrossRef]
- Press and Information Office of the Federal Government. Agreement: Guidelines to Slow the Spread of the Coronavirus. Available online: https://www.bundesregierung.de/breg-en/news/guidelines-to-slow-the-spread-of-the-coronavirus-1731708 (accessed on 12 February 2022).
- Saint-Maurice, P.F.; Welk, G.J. Validity and calibration of the youth activity profile. PLoS ONE 2015, 10, e0143949. [Google Scholar] [CrossRef] [Green Version]
- Welk, G.J.; Kim, Y.; Stanfill, B.; Osthus, D.A.; Calabro, M.A.; Nusser, S.M.; Carriquiry, A. Validity of 24-h physical activity recall: Physical activity measurement survey. Med. Sci. Sports Exerc. 2014, 46, 2014–2024. [Google Scholar] [CrossRef] [Green Version]
- Gaede-Illig, C.; Zachariae, S.; Menzel, C.; Alfermann, D. Physical activity assessment—A comparison between IPAQ-SF and SenseWear Pro Armband. Dtsch. Z. Sportmed. 2014, 65, 154–159. [Google Scholar] [CrossRef]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandic, S.; Wilson, H.; Clark-Grill, M.; O’Neill, D. Medical students’ awareness of the links between physical activity and health. Montenegrin J. Sports Sci. Med. 2017, 6, 5–12. [Google Scholar] [CrossRef] [Green Version]
- Bertrand, L.; Shaw, M.K.; Ko, J.; Deprez, D.; Chilibeck, P.D.; Zello, G.A. The impact of the coronavirus disease 2019 (COVID-19) pandemic on university students’ dietary intake, physical activity, and sedentary behaviour. Appl. Physiol. Nutr. Metab. 2021, 46, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Srivastav, A.K.; Sharma, N.; Samuel, A.J. Impact of Coronavirus disease-19 (COVID-19) lockdown on physical activity and energy expenditure among physiotherapy professionals and students using web-based open E-survey sent through WhatsApp, Facebook and Instagram messengers. Clin. Epidemiol. Glob. Health 2021, 9, 78–84. [Google Scholar] [CrossRef]
- Karuc, J.; Sorić, M.; Radman, I.; Mišigoj-Duraković, M. Moderators of change in physical activity levels during restrictions due to COVID-19 pandemic in young urban adults. Sustainability 2020, 12, 6392. [Google Scholar] [CrossRef]
- Górnicka, M.; Drywień, M.E.; Zielinska, M.A.; Hamułka, J. Dietary and lifestyle changes during COVID-19 and the subsequent lockdowns among Polish adults: A cross-sectional online survey PLifeCOVID-19 study. Nutrients 2020, 12, 2324. [Google Scholar] [CrossRef]
- Bourdas, D.I.; Zacharakis, E.D. Impact of COVID-19 lockdown on physical activity in a sample of Greek adults. Sports 2020, 8, 139. [Google Scholar] [CrossRef]
- Robert Koch Institut. Informationen und Hilfestellungen für Personen mit einem höheren Risiko für einen schweren COVID-19-Krankheitsverlauf. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Risikogruppen.html (accessed on 12 February 2022).
- König, R.; Seifert, A.; Doh, M. Internet use among older Europeans: An analysis based on SHARE data. Univers. Access Inf. Soc. 2018, 17, 621–633. [Google Scholar] [CrossRef]
- Seifert, A. The digital exclusion of older adults during the COVID-19 pandemic. J. Gerontol. Soc. Work 2020, 63, 674–676. [Google Scholar] [CrossRef]
- Hunsaker, A.; Hargittai, E. A review of Internet use among older adults. N. Media Soc. 2018, 20, 3937–3954. [Google Scholar] [CrossRef]
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Otobe, Y.; Suzuki, M.; Koyama, S.; Kikychi, T.; Kusumi, H.; Arai, H. Effect of the COVID-19 epidemic on physical activity in community-dwelling older adults in Japan: A cross-sectional online survey. J. Nutr. Health Aging 2020, 24, 948–950. [Google Scholar] [CrossRef] [PubMed]
- Trabelsi, K.; Ammar, A.; Masmoudi, L.; Boukhris, O.; Chtourou, H.; Bouaziz, B.; Brach, M.; Bentlage, E.; How, D.; Ahmed, M.; et al. Sleep quality and physical activity as predictors of mental wellbeing variance in older adults during COVID-19 lockdown: ECLB COVID-19 international online survey. Int. J. Environ. Res. Public Health 2021, 18, 4329. [Google Scholar] [CrossRef] [PubMed]
- García-Esquinas, E.; Ortolá, R.; Gine-Vázquez, I.; Carnicero, J.A.; Mañas, A.; Lara, E.; Alvarez-Bustos, A.; Vicente-Rodriguez, G.; Sotos-Prieto, M.; Olaya, B.; et al. Changes in health behaviors, mental and physical health among older adults under severe lockdown restrictions during the COVID-19 pandemic in Spain. Int. J. Environ. Res. Public Health 2021, 18, 7067. [Google Scholar] [CrossRef] [PubMed]
- van Uffelen, J.G.Z.; Khan, A.; Burton, N.W. Gender differences in physical activity motivators and context preferences: A population-based study in people in their sixties. BMC Public Health 2017, 17, 624. [Google Scholar] [CrossRef]
- García-Tascón, M.; Sahelices-Pinto, C.; Mendaña-Cuervo, C.; Magaz-González, A.M. The impact of the COVID-19 confinement on the habits of PA practice according to gender (male/female): Spanish case. Int. J. Environ. Res. Public Health 2020, 17, 6961. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Larrad, A.; Mañas, A.; Labayen, I.; González-Gross, M.; Espin, A.; Aznar, S.; Serrano-Sánchez, J.A.; Vera-Garcia, F.J.; González-Lamuño, D.; Ara, I.; et al. Impact of COVID-19 confinement on physical activity and sedentary behaviour in Spanish university students: Role of gender. Int. J. Environ. Res. Public Health 2021, 18, 369. [Google Scholar] [CrossRef]
- Beck, A.; Gilbert, A.; Duncan, D.; Wiedenman, E. A cross-sectional comparison of physical activity during COVID-19 in a sample of rural and non-rural participants in the US. Int. J. Environ. Res. Public Health 2021, 18, 4991. [Google Scholar] [CrossRef]
- McGrath, A.; Murphy, N.; Richardson, N. The impact of the COVID-19 pandemic on the wellbeing of Irish Men’s Shed members. Health Promot. Int. 2020, 36, 1007–1019. [Google Scholar] [CrossRef]
- Rice, W.L.; Mateer, T.J.; Reigner, N.; Newman, P.; Lawhon, B.; Taff, B.D. Changes in recreational behaviors of outdoor enthusiasts during the COVID-19 pandemic: Analysis across urban and rural communities. J. Urban Ecol. 2020, 6, juaa020. [Google Scholar] [CrossRef]
- Fan, J.X.; Wen, M.; Kowaleski-Jones, L. Rural–urban differences in objective and subjective measures of physical activity: Findings from the National Health and Nutrition Examination Survey (NHANES) 2003–2006. Prev. Chronic Dis. 2014, 11, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Forbes, C.C.; Yu, Z.M.; Cui, Y.; Declercq, V.; Grandy, S.A.; Parker, L.; Sweeney, E.; Dummer, T.J.B.; Keats, M.R. Rural-urban disparities in total physical activity, body composition, and related health indicators: An Atlantic PATH study. J. Rural Health 2020, 36, 111–119. [Google Scholar] [CrossRef] [PubMed]
- McCrorie, P.; Mitchell, R.; Macdonald, L.; Jones, A.; Coombes, E.; Schipperijn, J.; Ellaway, A. The relationship between living in urban and rural areas of Scotland and children’s physical activity and sedentary levels: A country-wide cross-sectional analysis. BMC Public Health 2020, 20, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, R.E.; Liu, S.; Lithopoulos, A.; Zhang, C.; Garcia-Barrera, M.A. Correlates of perceived physical activity transitions during the COVID-19 pandemic among Canadian adults. Appl. Psychol. Health Well-Being 2020, 12, 1157–1182. [Google Scholar] [CrossRef] [PubMed]
- López-Bueno, R.; Calatayud, J.; Casaña, J.; Casajús, J.A.; Smith, L.; Tully, M.A.; Andersen, L.L.; López-Sánchez, G.F. COVID-19 confinement and health risk behaviors in Spain. Front. Psychol. 2020, 11, 1426. [Google Scholar] [CrossRef] [PubMed]
- López-Bueno, R.; Calatayud, J.; Andersen, L.L.; Balsalobre-Fernández, C.; Casaña, J.; Casajús, J.A.; Smith, L.; López-Sánchez, G.F. Immediate impact of the COVID-19 confinement on physical activity levels in Spanish adults. Sustainability 2020, 12, 5708. [Google Scholar] [CrossRef]
- Mon-López, D.; Bernardez-Vilaboa, R.; Fernandez-Balbuena, A.A.; Sillero-Quintana, M. The influence of COVID-19 isolation on physical activity habits and its relationship with convergence insufficiency. Int. J. Environ. Res. Public Health 2020, 17, 7406. [Google Scholar] [CrossRef]
- Sánchez-Sánchez, E.; Ramírez-Vargas, G.; Avellaneda-López, Y.; Orellana-Pecino, J.I.; García-Marín, E.; Díaz-Jimenez, J. Eating habits and physical activity of the Spanish population during the COVID-19 pandemic period. Nutrients 2020, 12, 2826. [Google Scholar] [CrossRef]
- Faulkner, J.; O’Brien, W.J.; McGrane, B.; Wadsworth, D.; Batten, J.; Askew, C.D.; Badenhorst, C.; Byrd, E.; Coulter, M.; Draper, N.; et al. Physical activity, mental health and well-being of adults during initial COVID-19 containment strategies: A multi-country cross-sectional analysis. J. Sci. Med. Sport 2021, 24, 320–326. [Google Scholar] [CrossRef]
- Ruiz, M.C.; Devonport, T.J.; Chen-Wilson, C.H.J.; Nicholls, W.; Cagas, J.Y.; Fernandez-Montalvo, J.; Choi, Y.; Robazza, C. A cross-cultural exploratory study of health behaviors and wellbeing during COVID-19. Front. Psychol. 2021, 11, 608216. [Google Scholar] [CrossRef]
- Spence, J.C.; Rhodes, R.E.; McCurdy, A.; Mangan, A.; Hopkins, D.; Mummery, W.K. Determinants of physical activity among adults in the United Kingdom during the COVID-19 pandemic: The DUK-COVID study. Br. J. Health Psychol. 2020, 26, 588–605. [Google Scholar] [CrossRef]
- MET Office. May 2020 Becomes the Sunniest Calendar Month on Record. Available online: https://www.metoffice.gov.uk/about-us/press-office/news/weather-and-climate/2020/2020-spring-and-may-stats (accessed on 12 February 2022).
- Cleland, C.; Ferguson, S.; Ellis, G.; Hunter, R.F. Validity of the International Physical Activity Questionnaire (IPAQ) for assessing moderate-to-vigorous physical activity and sedentary behaviour of older adults in the United Kingdom. BMC Med. Res. Methodol. 2018, 18, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burchartz, A.; Anedda, B.; Auerswald, T.; Giurgiu, M.; Hill, H.; Ketelhut, S.; Kolb, S.; Mall, C.; Manz, K.; Nigg, C.R.; et al. Assessing physical behavior through accelerometry—State of the science, best practices and future directions. Psychol. Sport Exerc. 2020, 49, 101703. [Google Scholar] [CrossRef]
- Mell, L.K.; Tran, P.T.; James, B.Y. Principles of Clinical Cancer Research; Springer: Berlin, Germany, 2018; ISBN 1617052396. [Google Scholar]
- Caruana, E.J.; Roman, M.; Hernández-Sánchez, J.; Solli, P. Longitudinal studies. J. Thorac. Dis. 2015, 7, E537. [Google Scholar] [PubMed]
- Terwee, C.B.; Mokkink, L.B.; van Poppel, M.; Chinapaw, M.J.M.; van Mechelen, W.; de Vet, H.C.W. Qualitative attributes and measurement properties of physical activity questionnaires: A checklist. Sports Med. 2010, 40, 525–537. [Google Scholar] [CrossRef] [PubMed]
- Danner, D. Reliabilität—Die Genauigkeit einer Messung; Leibniz-Instiut für Sozialwissenschaften (GESIS): Mannheim, Germany, 2015; pp. 1–12. [Google Scholar]
- Werneck, A.O.; Silva, D.R.; Malta, D.C.; Souza-Júnior, P.R.; Azevedo, L.O.; Barros, M.B.; Szwarcwald, C.L. Physical inactivity and elevated TV-viewing reported changes during the COVID-19 pandemic are associated with mental health: A survey with 43,995 Brazilian adults. J. Psychosom. Res. 2021, 140, 110292. [Google Scholar] [CrossRef]
- Association for Aerosol Research. Position paper of the Gesellschaft für Aerosolforschung on Understanding the Role of Aerosol Particles in SARS-CoV-2 Infection. Available online: https://www.info.gaef.de/positionspapier (accessed on 29 May 2021).
- Wilson, D.; Driller, M.; Johnston, B.; Gill, N. The effectiveness of a 17-week lifestyle intervention on health behaviors among airline pilots during COVID-19. J. Sport Health Sci. 2020, 10, 333–340. [Google Scholar] [CrossRef]
- Parker, K.; Uddin, R.; Ridgers, N.D.; Brown, H.; Veitch, J.; Salmon, J.; Timperio, A.; Sahlqvist, S.; Cassar, S.; Toffoletti, K.; et al. The use of digital platforms for adults’ and adolescents’ physical activity during the COVID-19 pandemic (our life at home): Survey study. J. Med. Internet Res. 2021, 23, e23389. [Google Scholar] [CrossRef]
- Hoseini, R. How to exercise during Coronavirus quarantine? Casp. J. Intern. Med. 2020, 11, 479–483. [Google Scholar] [CrossRef]
- Khatri, S.M.; Patil, M. Indoor activities for physical fitness during lockdown. Indian J. Forensic Med. Toxicol. 2021, 15, 456–463. [Google Scholar] [CrossRef]
- King, K.M.; Hartson, K.; Della, L.J.; de Paleville, D.T. Promoting physical activity during the COVID-19 pandemic. Available online: https://www.tandfonline.com/doi/full/10.1080/23750472.2020.1757494 (accessed on 12 February 2022).
- Hammami, A.; Harrabi, B.; Mohr, M.; Krustrup, P. Physical activity and coronavirus disease 2019 (COVID-19): Specific recommendations for home-based physical training. Manag. Sport Leis. 2020, 1–6. [Google Scholar] [CrossRef]





| Inclusion | Exclusion | |
|---|---|---|
| Population | Healthy human subjects: no restriction on age, demographic variables, or geographical region | Groups of special interest not representing the general population (e.g., professional athletes) as well as studies in specialized settings (e.g., hospitals) |
| Intervention | Quasi-experimental: during the Covid-19 pandemic | If (1) only a single measurement was taken (cross-sectional) or if (2) multiple measurements were taken, but conducting retrospective assessments (i.e., asking within the pandemic questions about before the pandemic) |
| Comparison | Change in PA from before- to within-Covid-19 pandemic | |
| Outcome | Any form of PA, either subjectively (self-reports) or objectively (i.e., accelerometry) measured | Studies investigating other health-related behaviors and not reporting PA. For the meta-analysis, studies not providing information for effect size estimation were also excluded. |
| Study type | Only longitudinal studies with at least one measurement before the Covid-19 pandemic, as well as at least one measurement within the Covid-19 pandemic, were included: Observational studies, cohort studies, and pre-post tests were included. | Literature reviews, abstracts and conference proceedings, study protocols, editorials or commentaries, and letters to the editors not including any original data were excluded. |
| Author(s) (Year) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | Quality Rating |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aegerter et al. (2021) [68] | Y | Y | Y | Y | Y | Y | Y | NA | N | Y | Y | NA | Good |
| Al-Musharaf et al. (2021) [51] | Y | Y | Y | Y | Y | Y | Y | NA | N | Y | N | NA | Good |
| Alonso-Martinez et al. (2021) [69] | Y | Y | Y | Y | CD | Y | Y | NA | N | Y | N | NA | Fair |
| Baceviciene and Jankauskiene (2021) [70] | Y | Y | Y | N | CD | Y | Y | NA | N | Y | N | NA | Poor |
| Barone Gibbset al. (2021) [71] | Y | Y | Y | Y | CD | Y | Y | NA | N | Y | N | NA | Fair |
| Bartlett et al. (2021) [72] | Y | Y | Y | Y | CD | Y | Y | NA | N | Y | Y | NA | Good |
| Bronikowska et al. (2021) [73] | Y | Y | Y | Y | Y | Y | Y | NA | N | Y | N | NA | Good |
| Buoite Stella et al. (2021) [74] | Y | Y | Y | Y | CD | Y | N | Y | Y | Y | Y | NA | Good |
| Chaffee et al. (2021) [75] | Y | Y | Y | Y | Y | Y | Y | NA | N | Y | Y | NA | Good |
| Chen et al. (2021) [64] | Y | Y | Y | Y | CD | Y | N | NA | N | Y | Y | NA | Poor |
| Cheval et al. (2020) [76] | Y | Y | Y | Y | Y | Y | Y | NA | N | Y | N | NA | Good |
| Curtis et al. (2021) [77] | Y | Y | Y | Y | CD | Y | Y | NA | N | Y | Y | NA | Good |
| Di Sebastiano et al. (2021) [78] | Y | Y | Y | Y | CD | Y | Y | NA | N | Y | Y | NA | Good |
| Ding et al. (2021) [79] | Y | Y | Y | Y | CD | Y | Y | NA | N | Y | Y | NA | Good |
| Elnaggar et al. (2020) [80] | Y | N | Y | CD | CD | N | Y | NA | NR | Y | Y | NA | Poor |
| Esain et al. (2021) [81] | Y | Y | Y | Y | CD | Y | Y | NA | N | Y | Y | NA | Good |
| Folk et al. (2021) [82] | Y | Y | Y | Y | CD | Y | Y | NA | N | Y | Y | NA | Good |
| Franco et al. (2021) [83] | Y | Y | Y | Y | CD | Y | Y | NA | N | Y | N | NA | Fair |
| Gallego-Gomez et al. (2020) [84] | Y | Y | Y | Y | CD | Y | N | NA | Y | Y | Y | NA | Fair |
| Gilic et al. (2020) [85] | Y | Y | Y | Y | CD | Y | Y | NA | Y | Y | N | NA | Good |
| Gilic et al. (2021) [86] | Y | Y | Y | Y | CD | Y | Y | NA | Y | Y | N | NA | Good |
| Giuntella et al. (2021) [87] | N | Y | N | Y | CD | Y | Y | NA | NR | Y | Y | NA | Poor |
| He et al. (2020) [88] | Y | Y | Y | Y | CD | Y | N | NA | Y | Y | Y | NA | Good |
| Hino et al. (2021) [66] | Y | Y | Y | N | N | Y | Y | NA | Y | N | Y | NA | Fair |
| Koohsari et al. (2021a) [89] | Y | Y | Y | N | CD | Y | Y | NA | N | Y | N | NA | Poor |
| Martinez-de-Quel et al. (2020) [90] | Y | Y | Y | Y | CD | Y | Y | NA | N | Y | N | NA | Fair |
| McCarthy et al. (2021) [58] | Y | Y | Y | Y | CD | Y | Y | NA | NA | Y | Y | NA | Good |
| Medrano et al. (2020) [91] | Y | Y | Y | Y | Y | Y | Y | NA | N | Y | N | NA | Good |
| Mishra et al. (2021) [55] | Y | Y | Y | N | CD | Y | Y | NA | Y | Y | N | NA | Fair |
| Miyahara et al. (2021) [92] | Y | N | N | N | CD | Y | Y | NA | N | N | N | NA | Poor |
| Munasinghe et al. (2020) [63] | Y | Y | Y | Y | CD | Y | N | NA | N | Y | Y | NA | Fair |
| Nigg et al. (2021) [93] | Y | Y | N | Y | Y | Y | Y | NA | Y | Y | Y | NA | Good |
| Nyström et al. (2020) [57] | Y | Y | Y | Y | CD | Y | N | NA | Y | Y | Y | NA | Fair |
| Obuchi et al. (2021) [94] | Y | Y | Y | N | CD | Y | Y | NA | Y | Y | Y | NA | Good |
| Okely et al. (2021) [50] | Y | Y | Y | N | Y | Y | N | NA | NR | Y | N | NA | Poor |
| Okely et al. (2020) [95] | Y | Y | Y | Y | CD | Y | N | NA | N | Y | N | NA | Poor |
| Ong et al. (2020) [96] | Y | Y | Y | Y | CD | Y | Y | NA | Y | Y | Y | NA | Good |
| Park et al. (2021) [97] | Y | Y | N | Y | CD | Y | Y | NA | N | Y | N | NA | Poor |
| Perez et al. (2021) [98] | Y | Y | Y | N | CD | Y | Y | NA | Y | Y | N | NA | Good |
| Riberiro de Lima et al. (2021) [52] | Y | Y | Y | CD | CD | Y | Y | NA | NR | Y | N | NA | Fair |
| Richardson et al. (2020) [99] | Y | Y | Y | Y | CD | Y | Y | NA | Y | Y | Y | NA | Good |
| Romero-Blanco et al. (2020) [100] | Y | Y | Y | Y | Y | Y | Y | NA | Y | Y | N | NA | Good |
| Sanudo et al. (2020) [101] | Y | Y | Y | Y | CD | Y | Y | NA | N | Y | Y | NA | Fair |
| Savage et al. (2021) [102] | Y | Y | Y | N | CD | Y | Y | NA | N | Y | N | NA | Poor |
| Savage et al. (2020) [103] | Y | Y | Y | Y | CD | Y | Y | NA | N | Y | Y | NA | Good |
| Schmidt et al. (2020) [104] | Y | Y | Y | Y | CD | Y | Y | NA | N | Y | N | NA | Good |
| Sekulic et al. (2020) [105] | Y | Y | Y | NR | CD | Y | Y | NA | NR | Y | N | NA | Poor |
| Suzuki et al. (2020) [65] | Y | Y | Y | Y | CD | Y | N | NA | Y | Y | N | NA | Fair |
| To et al. (2021) [56] | Y | Y | Y | Y | CD | Y | N | NA | Y | Y | Y | NA | Poor |
| Wang et al. (2020) [106] | Y | Y | Y | Y | CD | Y | Y | NA | Y | Y | Y | NA | Good |
| Wilson et al. (2021) [107] | Y | Y | Y | CD | CD | Y | Y | NA | NR | Y | N | NA | Poor |
| Woodruff et al. (2021) [108] | Y | Y | Y | CD | CD | Y | N | NA | N | Y | Y | NA | Poor |
| Wunsch et al. (2021) [109] | Y | Y | Y | N | CD | Y | Y | NA | N | Y | N | NA | Poor |
| Yang and Koenigstorfer (2020) [110] | Y | Y | Y | Y | Y | Y | Y | NA | N | Y | N | NA | Good |
| Zenic et al. (2020) [53] | Y | Y | Y | NR | CD | Y | Y | NA | NR | Y | N | NA | Poor |
| Zheng et al. (2020) [54] | Y | Y | N | Y | CD | Y | Y | NA | Y | Y | N | NA | Fair |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wunsch, K.; Kienberger, K.; Niessner, C. Changes in Physical Activity Patterns Due to the Covid-19 Pandemic: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 2250. https://doi.org/10.3390/ijerph19042250
Wunsch K, Kienberger K, Niessner C. Changes in Physical Activity Patterns Due to the Covid-19 Pandemic: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(4):2250. https://doi.org/10.3390/ijerph19042250
Chicago/Turabian StyleWunsch, Kathrin, Korbinian Kienberger, and Claudia Niessner. 2022. "Changes in Physical Activity Patterns Due to the Covid-19 Pandemic: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 4: 2250. https://doi.org/10.3390/ijerph19042250
APA StyleWunsch, K., Kienberger, K., & Niessner, C. (2022). Changes in Physical Activity Patterns Due to the Covid-19 Pandemic: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(4), 2250. https://doi.org/10.3390/ijerph19042250