
The Identification and Management of High Blood Pressure Using Exercise Blood Pressure: Current Evidence and Practical Guidance

 , , ,
, , ,
Abstract
:1. Introduction
1.1. The Blood Pressure Response to Acute Dynamic Incremental Exercise
1.2. Evidence Supporting the Clinical Value of Submaximal Exercise BP Measurement
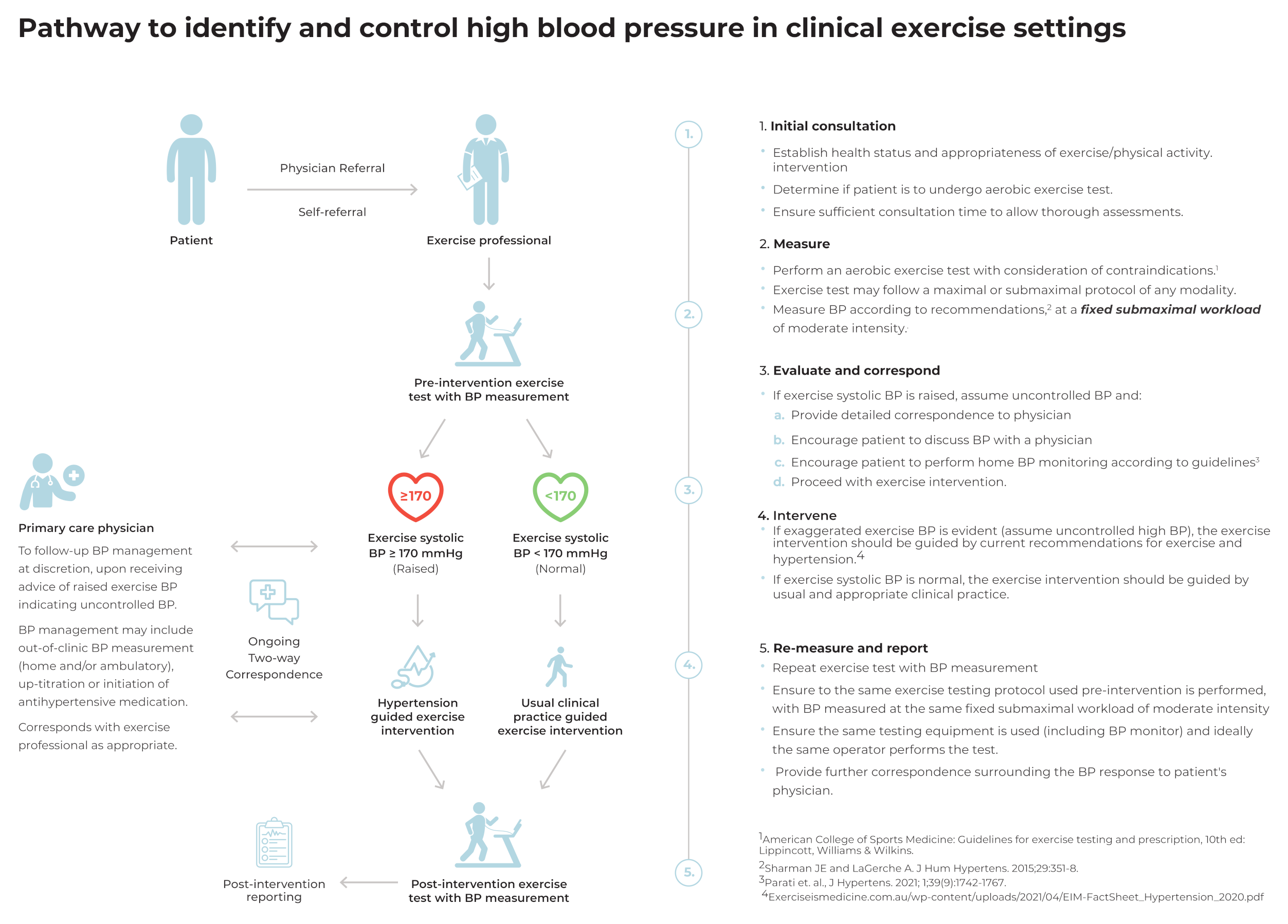
1.3. A Pathway for the Identification and Management of High BP via Exercise BP Measurement within Clinical Exercise Settings
2. Initial Consultation
Key Recommendations
- -
- Establish health status and appropriateness for exercise/physical activity intervention;
- -
- Determine if patient is to undergo an aerobic exercise test;
- -
- Ensure sufficient consultation time to allow thorough assessments.
3. Measure
Key Recommendations
- -
- Perform an aerobic exercise test with consideration of contraindications;
- -
- Exercise test may follow a maximal or submaximal protocol of any modality;
- -
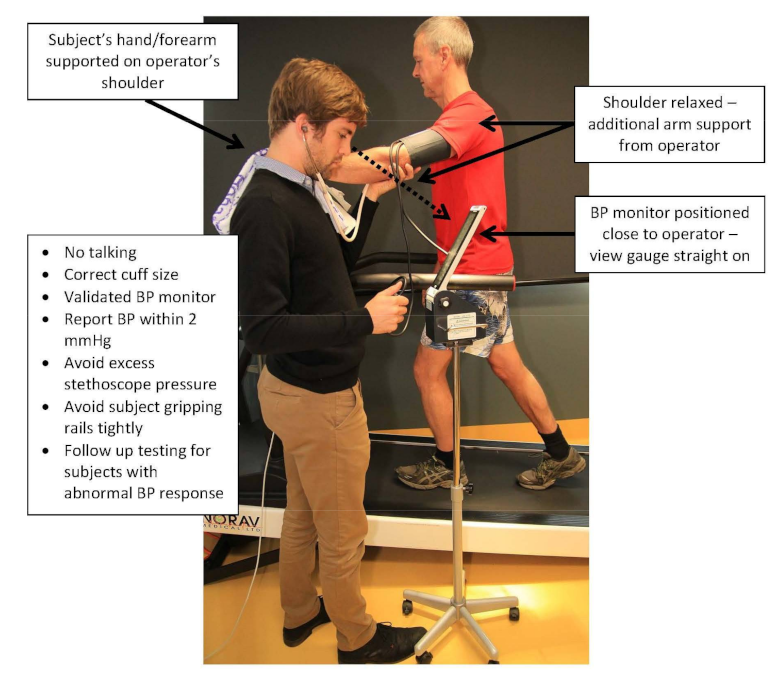
- Measure BP according to recommendations at a fixed submaximal workload of moderate intensity.
4. Evaluate and Correspond
Key Recommendations
- -
- If exercise systolic BP is raised (≥170 mmHg), assume uncontrolled BP and
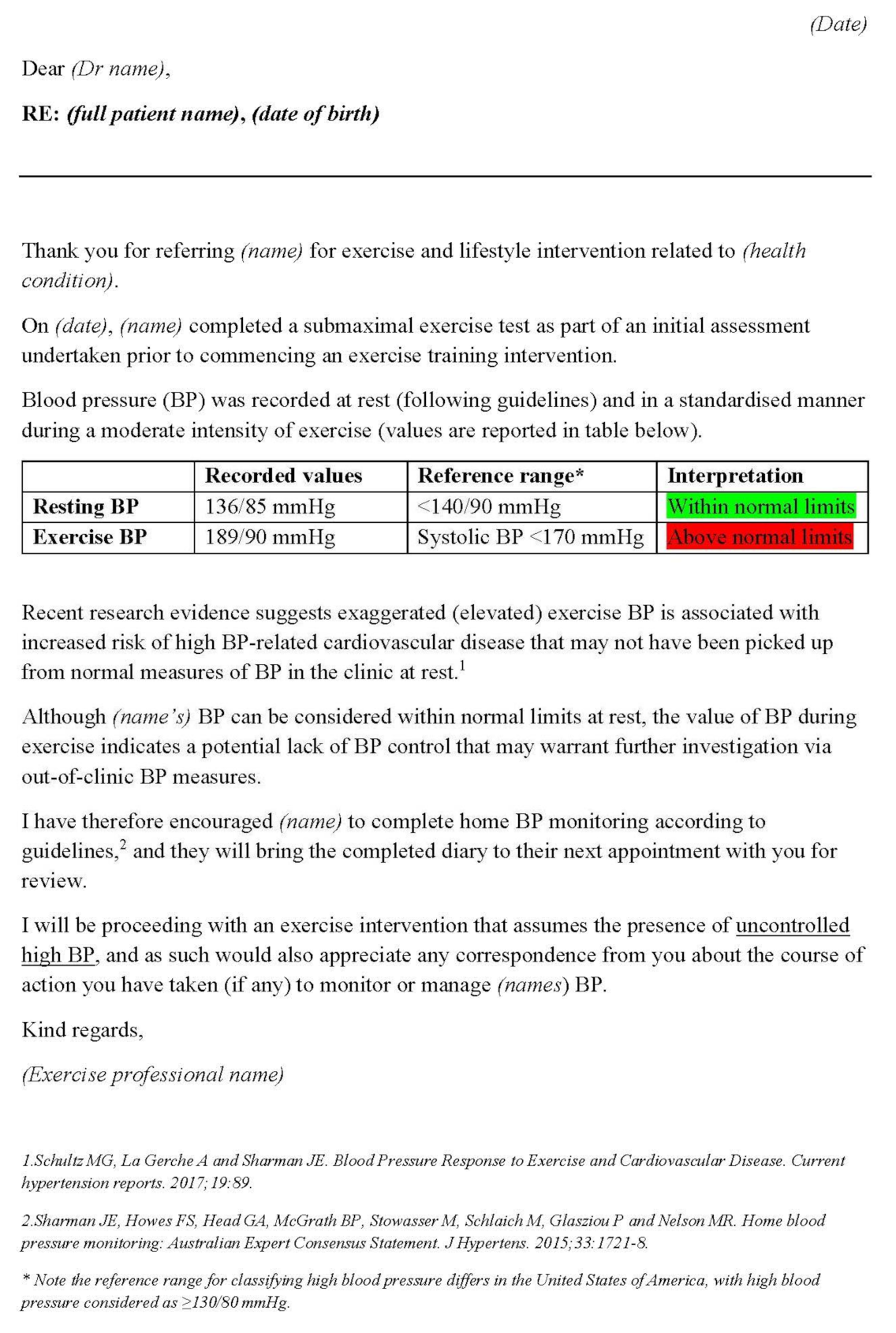
- Provide detailed correspondence to physician;
- Encourage patient to discuss BP with a physician;
- Encourage the patient to perform home BP monitoring according to guidelines;
- Proceed with exercise intervention.
5. Intervene
Key Recommendations
- -
- If EEBP is evident (assume uncontrolled high BP), the exercise intervention should be guided by current recommendations for exercise and hypertension;
- -
- If exercise systolic BP is normal, the exercise intervention should be guided by usual and appropriate clinical practice.
6. Re-Measure and Report
Key Points
- -
- Repeat exercise test with BP measurement;
- -
- Ensure the same exercise testing protocol used pre-intervention is performed, with BP measured at the same fixed submaximal workload at moderate intensity;
- -
- Ensure the same testing equipment is used (including BP monitor) and ideally the same operator performs the test;
- -
- Provide further correspondence surrounding the BP response to patient’s physician.
7. The Physician’s Role
8. Future Needs
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stanaway, J.D.; Afshin, A.; Gakidou, E.; Lim, S.S.; Abate, D.; Abate, K.H.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar]
- Zhou, B.; Bentham, J.; Di Cesare, M.; Bixby, H.; Danaei, G.; Cowan, M.J.; Paciorek, C.J.; Singh, G.; Hajifathalian, K.; Bennett, J.E.; et al. Worldwide trends in blood pressure from 1975 to 2015: A pooled analysis of 1479 population-based measurement studies with 19·1 million participants. Lancet 2017, 389, 37–55. [Google Scholar] [CrossRef] [Green Version]
- Campbell, N.R.C.; Schutte, A.E.; Varghese, C.V.; Ordunez, P.; Zhang, X.H.; Khan, T.; Sharman, J.E.; Whelton, P.K.; Parati, G.; Weber, M.A.; et al. São Paulo call to action for the prevention and control of high blood pressure: 2020. J. Clin. Hypertens. 2019, 21, 1744–1752. [Google Scholar] [CrossRef] [Green Version]
- Bobrie, G.; Clerson, P.; Ménard, J.; Postel-Vinay, N.; Chatellier, G.; Plouin, P.F. Masked hypertension: A systematic review. J. Hypertens. 2008, 26, 1715–1725. [Google Scholar] [CrossRef]
- Schultz, M.G.; Otahal, P.; Cleland, V.J.; Blizzard, L.; Marwick, T.H.; Sharman, J.E. Exercise-induced hypertension, cardiovascular events, and mortality in patients undergoing exercise stress testing: A systematic review and meta-analysis. Am. J. Hypertens. 2013, 26, 357–366. [Google Scholar] [CrossRef] [Green Version]
- Weiss, S.A.; Blumenthal, R.S.; Sharrett, A.R.; Redberg, R.F.; Mora, S. Exercise blood pressure and future cardiovascular death in asymptomatic individuals. Circulation 2010, 121, 2109–2116. [Google Scholar] [CrossRef] [Green Version]
- Mariampillai, J.E.; Liestøl, K.; Kjeldsen, S.E.; Prestgaard, E.E.; Engeseth, K.; Bodegard, J.; Berge, E.; Gjesdal, K.; Erikssen, J.; Grundvold, I.; et al. Exercise Systolic Blood Pressure at Moderate Workload Is Linearly Associated With Coronary Disease Risk in Healthy Men. Hypertension 2020, 75, 44–50. [Google Scholar] [CrossRef]
- Kayrak, M.; Bacaksiz, A.; Vatankulu, M.A.; Ayhan, S.S.; Kaya, Z.; Ari, H.; Sonmez, O.; Gok, H. Exaggerated blood pressure response to exercise—A new portent of masked hypertension. Clin. Exp. Hypertens. 2010, 32, 560–568. [Google Scholar] [CrossRef]
- Schultz, M.G.; Hare, J.L.; Marwick, T.H.; Stowasser, M.; Sharman, J.E. Masked hypertension is “unmasked” by low-intensity exercise blood pressure. Blood Press. 2011, 20, 284–289. [Google Scholar] [CrossRef]
- Schultz, M.G.; Picone, D.S.; Nikolic, S.B.; Williams, A.D.; Sharman, J.E. Exaggerated blood pressure response to early stages of exercise stress testing and presence of hypertension. J. Sci. Med. Sport 2016, 19, 1039–1042. [Google Scholar] [CrossRef]
- Australian Government—Services Australia, Medicare Items Processed from July 2020 to June 2021—Item 10953, Exercise Physiology Services. Available online: http://medicarestatistics.humanservices.gov.au/statistics/mbs_item.jsp (accessed on 21 November 2020).
- Bassett, D.R., Jr.; Howley, E.T. Limiting factors for maximum oxygen uptake and determinants of endurance performance. Med. Sci. Sports Exerc. 2000, 32, 70–84. [Google Scholar] [CrossRef]
- Joyner, M.J.; Casey, D.P. Regulation of increased blood flow (hyperemia) to muscles during exercise: A hierarchy of competing physiological needs. Physiol. Rev. 2015, 95, 549–601. [Google Scholar] [CrossRef] [Green Version]
- Currie, K.D.; Floras, J.S.; La Gerche, A.; Goodman, J.M. Exercise Blood Pressure Guidelines: Time to Re-evaluate What is Normal and Exaggerated? Sports Med. 2018, 48, 1763–1771. [Google Scholar] [CrossRef]
- American College of Sports Medicine: Guidelines for Exercise Testing and Prescription, 9th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013.
- Lauer, M.S.; Levy, D.; Anderson, K.M.; Plehn, J.F. Is there a relationship between exercise systolic blood pressure response and left ventricular mass? The Framingham Heart Study. Ann. Intern. Med. 1992, 116, 203–210. [Google Scholar] [CrossRef]
- Lauer, M.S.; Pashkow, F.J.; Harvey, S.A.; Marwick, T.H.; Thomas, J.D. Angiographic and prognostic implications of an exaggerated exercise systolic blood pressure response and rest systolic blood pressure in adults undergoing evaluation for suspected coronary artery disease. J. Am. Coll. Cardiol. 1995, 26, 1630–1636. [Google Scholar] [CrossRef] [Green Version]
- Allison, T.G.; Cordeiro, M.A.; Miller, T.D.; Daida, H.; Squires, R.W.; Gau, G.T. Prognostic significance of exercise-induced systemic hypertension in healthy subjects. Am. J. Cardiol. 1999, 83, 371–375. [Google Scholar] [CrossRef]
- Le, V.V.; Mitiku, T.; Sungar, G.; Myers, J.; Froelicher, V. The blood pressure response to dynamic exercise testing: A systematic review. Prog. Cardiovasc. Dis. 2008, 51, 135–160. [Google Scholar] [CrossRef]
- Schultz, M.G.; Otahal, P.; Picone, D.S.; Sharman, J.E. Clinical Relevance of Exaggerated Exercise Blood Pressure. J. Am. Coll. Cardiol. 2015, 66, 1843–1845. [Google Scholar] [CrossRef] [Green Version]
- Schultz, M.G.; La Gerche, A.; Sharman, J.E. Cardiorespiratory Fitness, Workload, and the Blood Pressure Response to Exercise Testing. Exerc. Sport Sci. Rev. 2022, 50, 25–30. [Google Scholar] [CrossRef]
- Schultz, M.G.; La Gerche, A.; Sharman, J.E. Blood Pressure Response to Exercise and Cardiovascular Disease. Curr. Hypertens. Rep. 2017, 19, 89. [Google Scholar] [CrossRef]
- Schultz, M.G.; Sharman, J.E. Exercise Hypertension. Pulse 2013, 1, 161–176. [Google Scholar] [CrossRef] [Green Version]
- Sharman, J.E.; LaGerche, A. Exercise blood pressure: Clinical relevance and correct measurement. J. Hum. Hypertens. 2015, 29, 351–358. [Google Scholar] [CrossRef]
- Keller, K.; Stelzer, K.; Ostad, M.A.; Post, F. Impact of exaggerated blood pressure response in normotensive individuals on future hypertension and prognosis: Systematic review according to PRISMA guideline. Adv. Med. Sci. 2017, 62, 317–329. [Google Scholar] [CrossRef]
- Mariampillai, J.E.; Engeseth, K.; Kjeldsen, S.E.; Grundvold, I.; Liestøl, K.; Erikssen, G.; Erikssen, J.; Bodegard, J.; Skretteberg, P.T. Exercise systolic blood pressure at moderate workload predicts cardiovascular disease and mortality through 35 years of follow-up in healthy, middle-aged men. Blood Press. 2017, 26, 229–236. [Google Scholar] [CrossRef]
- Lee, J.; Vasan, R.S.; Xanthakis, V. Association of Blood Pressure Responses to Submaximal Exercise in Midlife With the Incidence of Cardiovascular Outcomes and All-Cause Mortality: The Framingham Heart Study. J. Am. Heart Assoc. 2020, 9, e015554. [Google Scholar] [CrossRef]
- Sharman, J.E.; Hare, J.L.; Thomas, S.; Davies, J.E.; Leano, R.; Jenkins, C.; Marwick, T.H. Association of masked hypertension and left ventricular remodeling with the hypertensive response to exercise. Am. J. Hypertens. 2011, 24, 898–903. [Google Scholar] [CrossRef] [Green Version]
- Huang, Z.; Sharman, J.E.; Fonseca, R.; Park, C.; Chaturvedi, N.; Davey Smith, G.; Howe, L.D.; Lawlor, D.A.; Hughes, A.D.; Schultz, M.G. Masked hypertension and submaximal exercise blood pressure among adolescents from the Avon Longitudinal Study of Parents and Children (ALSPAC). Scand. J. Med. Sci. Sports 2020, 30, 25–30. [Google Scholar] [CrossRef]
- Stergiou, G.S.; Asayama, K.; Thijs, L.; Kollias, A.; Niiranen, T.J.; Hozawa, A.; Boggia, J.; Johansson, J.K.; Ohkubo, T.; Tsuji, I.; et al. Prognosis of white-coat and masked hypertension: International Database of HOme blood pressure in relation to Cardiovascular Outcome. Hypertension 2014, 63, 675–682. [Google Scholar] [CrossRef] [Green Version]
- Franklin, S.S.; Thijs, L.; Li, Y.; Hansen, T.W.; Boggia, J.; Liu, Y.; Asayama, K.; Björklund-Bodegård, K.; Ohkubo, T.; Jeppesen, J.; et al. Masked hypertension in diabetes mellitus: Treatment implications for clinical practice. Hypertension 2013, 61, 964–971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mundal, R.; Kjeldsen, S.E.; Sandvik, L.; Erikssen, G.; Thaulow, E.; Erikssen, J. Clustering of coronary risk factors with increasing blood pressure at rest and during exercise. J. Hypertens. 1998, 16, 19–22. [Google Scholar] [CrossRef]
- Scott, J.A.; Coombes, J.S.; Prins, J.B.; Leano, R.L.; Marwick, T.H.; Sharman, J.E. Patients with type 2 diabetes have exaggerated brachial and central exercise blood pressure: Relation to left ventricular relative wall thickness. Am. J. Hypertens. 2008, 21, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.; Ouyang, P.; Silber, H.A.; Bacher, A.C.; Turner, K.L.; DeRegis, J.R.; Hees, P.S.; Shapiro, E.P.; Stewart, K.J. Exercise blood pressure response is related to left ventricular mass. J. Hum. Hypertens. 2003, 17, 333–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kokkinos, P.; Pittaras, A.; Narayan, P.; Faselis, C.; Singh, S.; Manolis, A. Exercise capacity and blood pressure associations with left ventricular mass in prehypertensive individuals. Hypertension 2007, 49, 55–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schultz, M.G.; Park, C.; Fraser, A.; Howe, L.D.; Jones, S.; Rapala, A.; Davey Smith, G.; Sharman, J.E.; Lawlor, D.A.; Chaturvedi, N.; et al. Submaximal exercise blood pressure and cardiovascular structure in adolescence. Int. J. Cardiol. 2019, 275, 152–157. [Google Scholar] [CrossRef] [Green Version]
- Mottram, P.M.; Haluska, B.; Yuda, S.; Leano, R.; Marwick, T.H. Patients with a hypertensive response to exercise have impaired systolic function without diastolic dysfunction or left ventricular hypertrophy. J. Am. Coll. Cardiol. 2004, 43, 848–853. [Google Scholar] [CrossRef] [Green Version]
- Sarma, S.; Howden, E.; Carrick-Ranson, G.; Lawley, J.; Hearon, C.; Samels, M.; Everding, B.; Livingston, S.; Adams-Huet, B.; Palmer, M.D.; et al. Elevated exercise blood pressure in middle-aged women is associated with altered left ventricular and vascular stiffness. J. Appl. Physiol. 2020, 128, 1123–1129. [Google Scholar] [CrossRef]
- Maiorana, A.J.; Williams, A.D.; Askew, C.D.; Levinger, I.; Coombes, J.; Vicenzino, B.; Davison, K.; Smart, N.A.; Selig, S.E. Exercise Professionals with Advanced Clinical Training Should be Afforded Greater Responsibility in Pre-Participation Exercise Screening: A New Collaborative Model between Exercise Professionals and Physicians. Sports Med. 2018, 48, 1293–1302. [Google Scholar] [CrossRef] [Green Version]
- Whitfield, G.P.; Riebe, D.; Magal, M.; Liguori, G. Applying the ACSM Preparticipation Screening Algorithm to U.S. Adults: National Health and Nutrition Examination Survey 2001-2004. Med. Sci. Sports Exerc. 2017, 49, 2056–2063. [Google Scholar] [CrossRef]
- Warburton, D.E.R.; Jamnik, V.K.; Bredin, S.S.D.; Burr, J.; Charlesworth, S.; Chilibeck, P.; Eves, N.; Foulds, H.; Goodman, J.; Jones, L.; et al. Executive Summary: The 2011 Physical Activity Readiness Questionnaire for Everyone (PAR-Q+) and the Electronic Physical Activity Readiness Medical Examination (ePARmed-X+). Health Amp Fit. J. Can. 2011, 4, 24–25. [Google Scholar]
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.A.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C.; et al. Exercise standards for testing and training: A scientific statement from the American Heart Association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef]
- Norton, K.; Norton, L.; Sadgrove, D. Position statement on physical activity and exercise intensity terminology. J. Sci. Med. Sport 2010, 13, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Coombes, J.; Skinner, T. ESSA’s Student Manual for Health, Exercise and Sport Assessment—eBook; Elsevier: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Currie, K.D.; Soave, K.M.; Slade, J.M. Reliability of blood pressure responses used to define an exaggerated blood pressure response to exercise in young healthy adults. J. Hum. Hypertens. 2021. [Google Scholar] [CrossRef] [PubMed]
- Hedman, K.; Lindow, T.; Elmberg, V.; Brudin, L.; Ekström, M. Age- and gender-specific upper limits and reference equations for workload-indexed systolic blood pressure response during bicycle ergometry. Eur. J. Prev. Cardiol. 2021, 28, 1360–1369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, M.N.; Picone, D.S.; Callisaya, M.L.; Srikanth, V.; Sharman, J.E.; Schultz, M.G. Comparison of manual and automated auscultatory blood pressure during graded exercise among people with type 2 diabetes. J. Clin. Hypertens. 2019, 21, 1872–1878. [Google Scholar] [CrossRef]
- Cameron, J.D.; Stevenson, I.; Reed, E.; McGrath, B.P.; Dart, A.M.; Kingwell, B.A. Accuracy of automated auscultatory blood pressure measurement during supine exercise and treadmill stress electrocardiogram-testing. Blood Press. Monit. 2004, 9, 269–275. [Google Scholar] [CrossRef]
- Pickering, T.G.; Hall, J.E.; Appel, L.J.; Falkner, B.E.; Graves, J.; Hill, M.N.; Jones, D.W.; Kurtz, T.; Sheps, S.G.; Roccella, E.J. Recommendations for blood pressure measurement in humans and experimental animals: Part 1: Blood pressure measurement in humans: A statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Hypertension 2005, 45, 142–161. [Google Scholar]
- Lorbeer, R.; Ittermann, T.; Volzke, H.; Glaser, S.; Ewert, R.; Felix, S.B.; Dorr, M. Assessing cutoff values for increased exercise blood pressure to predict incident hypertension in a general population. J. Hypertens. 2015, 33, 1386–1393. [Google Scholar] [CrossRef]
- Zafrir, B.; Aker, A.; Asaf, Y.; Saliba, W. Blood pressure response during treadmill exercise testing and the risk for future cardiovascular events and new-onset hypertension. J. Hypertens. 2022, 40, 143–152. [Google Scholar] [CrossRef]
- Jae, S.Y.; Franklin, B.A.; Choo, J.; Choi, Y.H.; Fernhall, B. Exaggerated Exercise Blood Pressure Response during Treadmill Testing as a Predictor of Future Hypertension in Men: A Longitudinal Study. Am. J. Hypertens. 2015, 28, 1362–1367. [Google Scholar] [CrossRef] [Green Version]
- Miyai, N.; Arita, M.; Morioka, I.; Miyashita, K.; Nishio, I.; Takeda, S. Exercise BP response in subjects with high-normal BP: Exaggerated blood pressure response to exercise and risk of future hypertension in subjects with high-normal blood pressure. J. Am. Coll. Cardiol. 2000, 36, 1626–1631. [Google Scholar] [CrossRef] [Green Version]
- Parati, G.; Stergiou, G.S.; Bilo, G.; Kollias, A.; Pengo, M.; Ochoa, J.E.; Agarwal, R.; Asayama, K.; Asmar, R.; Burnier, M.; et al. Home blood pressure monitoring: Methodology, clinical relevance and practical application: A 2021 position paper by the Working Group on Blood Pressure Monitoring and Cardiovascular Variability of the European Society of Hypertension. J. Hypertens. 2021, 39, 1742–1767. [Google Scholar] [CrossRef]
- Sharman, J.E.; Howes, F.S.; Head, G.A.; McGrath, B.P.; Stowasser, M.; Schlaich, M.; Glasziou, P.; Nelson, M.R. Home blood pressure monitoring: Australian Expert Consensus Statement. J. Hypertens. 2015, 33, 1721–1728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picone, D.S.; Padwal, R.; Campbell, N.R.C.; Boutouyrie, P.; Brady, T.M.; Olsen, M.H.; Delles, C.; Lombardi, C.; Mahmud, A.; Meng, Y.; et al. How to check whether a blood pressure monitor has been properly validated for accuracy. J. Clin. Hypertens. 2020, 22, 2167–2174. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.H.; Wong, F.K. The association between time spent in sedentary behaviors and blood pressure: A systematic review and meta-analysis. Sports Med. 2015, 45, 867–880. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.; Zhang, D.; Chen, S.; Duan, G. The association of cardiorespiratory fitness and the risk of hypertension: A systematic review and dose-response meta-analysis. J. Hum. Hypertens. 2021. [Google Scholar] [CrossRef]
- Cornelissen, V.A.; Smart, N.A. Exercise training for blood pressure: A systematic review and meta-analysis. J. Am. Heart Assoc. 2013, 2, e004473. [Google Scholar] [CrossRef] [Green Version]
- Kelley, G.A.; Kelley, K.S. Progressive resistance exercise and resting blood pressure: A meta-analysis of randomized controlled trials. Hypertension 2000, 35, 838–843. [Google Scholar] [CrossRef] [PubMed]
- Cornelissen, V.A.; Buys, R.; Smart, N.A. Endurance exercise beneficially affects ambulatory blood pressure: A systematic review and meta-analysis. J. Hypertens. 2013, 31, 639–648. [Google Scholar] [CrossRef]
- Barone, B.B.; Wang, N.Y.; Bacher, A.C.; Stewart, K.J. Decreased exercise blood pressure in older adults after exercise training: Contributions of increased fitness and decreased fatness. Br. J. Sports Med. 2009, 43, 52–56. [Google Scholar] [CrossRef] [Green Version]
- Naci, H.; Salcher-Konrad, M.; Dias, S.; Blum, M.R.; Sahoo, S.A.; Nunan, D.; Ioannidis, J.P.A. How does exercise treatment compare with antihypertensive medications? A network meta-analysis of 391 randomised controlled trials assessing exercise and medication effects on systolic blood pressure. Br. J. Sports Med. 2019, 53, 859–869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pescatello, L.S.; Wu, Y.; Gao, S.; Livingston, J.; Sheppard, B.B.; Chen, M.H. Do the combined blood pressure effects of exercise and antihypertensive medications add up to the sum of their parts? A systematic meta-review. BMJ Open Sport Exerc. Med. 2021, 7, e000895. [Google Scholar] [CrossRef] [PubMed]
- Pescatello, L.S.; Franklin, B.A.; Fagard, R.; Farquhar, W.B.; Kelley, G.A.; Ray, C.A. American College of Sports Medicine position stand. Exercise and hypertension. Med. Sci. Sports Exerc. 2004, 36, 533–553. [Google Scholar] [CrossRef] [PubMed]
- Sharman, J.E.; Smart, N.A.; Coombes, J.S.; Stowasser, M. Exercise and sport science australia position stand update on exercise and hypertension. J. Hum. Hypertens. 2019, 33, 837–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rognmo, Ø.; Moholdt, T.; Bakken, H.; Hole, T.; Mølstad, P.; Myhr, N.E.; Grimsmo, J.; Wisløff, U. Cardiovascular risk of high- versus moderate-intensity aerobic exercise in coronary heart disease patients. Circulation 2012, 126, 1436–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, E.C.; Hay, J.L.; Kehler, D.S.; Boreskie, K.F.; Arora, R.C.; Umpierre, D.; Szwajcer, A.; Duhamel, T.A. Effects of High-Intensity Interval Training Versus Moderate-Intensity Continuous Training On Blood Pressure in Adults with Pre- to Established Hypertension: A Systematic Review and Meta-Analysis of Randomized Trials. Sports Med. 2018, 48, 2127–2142. [Google Scholar] [CrossRef] [PubMed]
- Leal, J.M.; Galliano, L.M.; Del Vecchio, F.B. Effectiveness of High-Intensity Interval Training Versus Moderate-Intensity Continuous Training in Hypertensive Patients: A Systematic Review and Meta-Analysis. Curr. Hypertens. Rep. 2020, 22, 26. [Google Scholar] [CrossRef] [PubMed]
- Severin, R.; Sabbahi, A.; Albarrati, A.; Phillips, S.A.; Arena, S. Blood Pressure Screening by Outpatient Physical Therapists: A Call to Action and Clinical Recommendations. Phys. Ther. 2020, 100, 1008–1019. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| General: |
|
|
|
| For manual measurement: |
|
|
|
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schultz, M.G.; Currie, K.D.; Hedman, K.; Climie, R.E.; Maiorana, A.; Coombes, J.S.; Sharman, J.E. The Identification and Management of High Blood Pressure Using Exercise Blood Pressure: Current Evidence and Practical Guidance. Int. J. Environ. Res. Public Health 2022, 19, 2819. https://doi.org/10.3390/ijerph19052819
Schultz MG, Currie KD, Hedman K, Climie RE, Maiorana A, Coombes JS, Sharman JE. The Identification and Management of High Blood Pressure Using Exercise Blood Pressure: Current Evidence and Practical Guidance. International Journal of Environmental Research and Public Health. 2022; 19(5):2819. https://doi.org/10.3390/ijerph19052819
Chicago/Turabian StyleSchultz, Martin G., Katharine D. Currie, Kristofer Hedman, Rachel E. Climie, Andrew Maiorana, Jeff S. Coombes, and James E. Sharman. 2022. "The Identification and Management of High Blood Pressure Using Exercise Blood Pressure: Current Evidence and Practical Guidance" International Journal of Environmental Research and Public Health 19, no. 5: 2819. https://doi.org/10.3390/ijerph19052819
APA StyleSchultz, M. G., Currie, K. D., Hedman, K., Climie, R. E., Maiorana, A., Coombes, J. S., & Sharman, J. E. (2022). The Identification and Management of High Blood Pressure Using Exercise Blood Pressure: Current Evidence and Practical Guidance. International Journal of Environmental Research and Public Health, 19(5), 2819. https://doi.org/10.3390/ijerph19052819