
Assessment of Quality of Life in Men Treated for Infertility in Poland

 ,
,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Method
2.1. Study Groups
- 400 men were treated without using assisted reproductive technology (non-ART);
- 400 men were treated with the intrauterine insemination (IUI);
- 400 men were treated using in vitro fertilization (IVF).
2.2. Survey Questionnaire
2.3. Statistical Methods
- Pearson’s chi-square test to compare the categorical variables between study groups;
- analysis of variance F test for to compare continuous variables between study groups. If statistical dependence between study groups was found, post hoc analyses were conducted to compare every pair of study groups and the least significant difference test was used.
3. Results
3.1. Respondents’ Characteristics
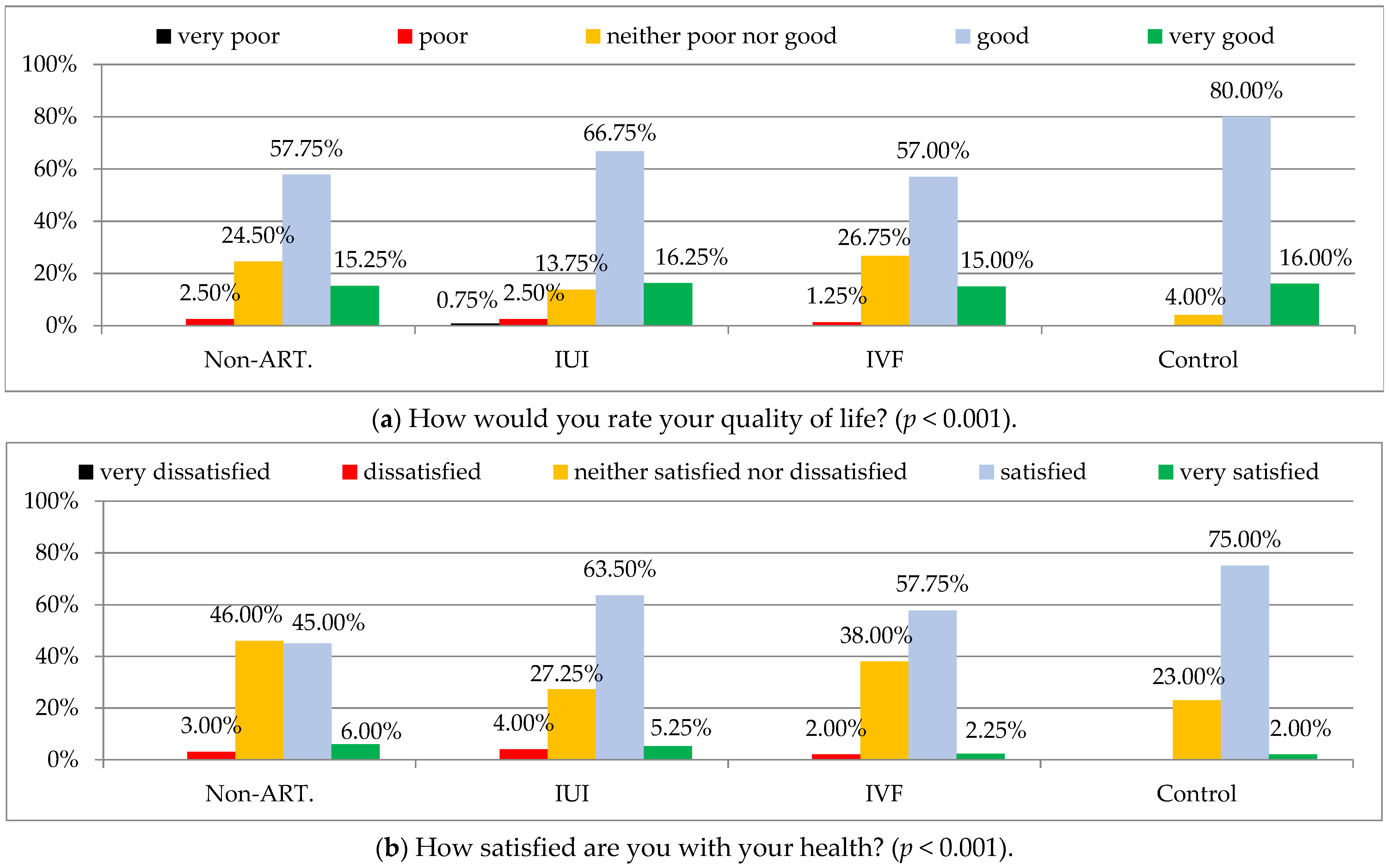
3.2. Comparison of Quality of Life (WHOQoL-Bref) between Respondents with Infertility and Those Who Had Children
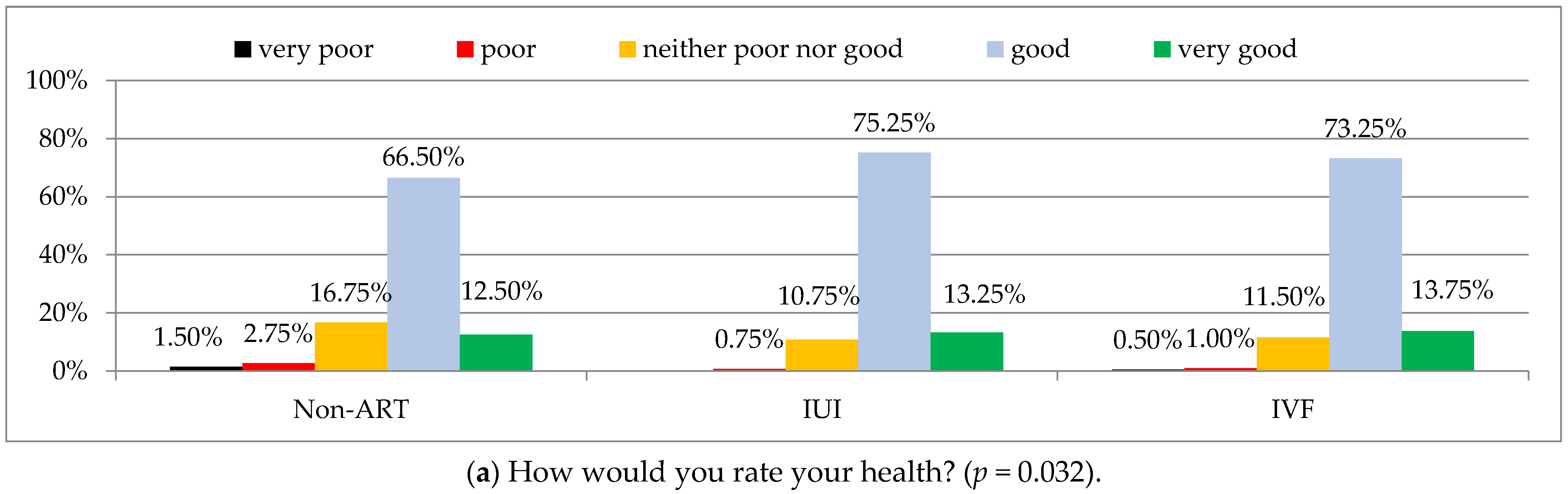
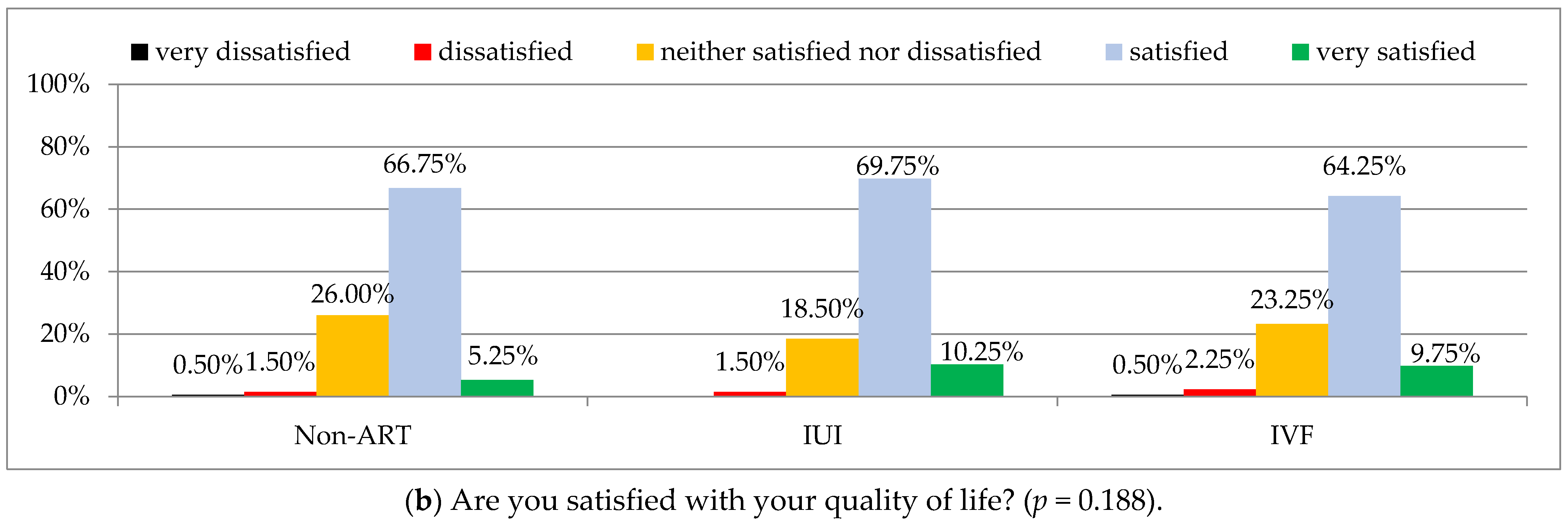
3.3. Comparison of Quality of Life (Acc. to the FertiQoL) between Methods of Infertility Treatment
3.4. Correlations between Characteristics of Study Groups and Quality of Life (Acc. to FertiQoL)
4. Discussion
5. Conclusions
- The quality of life of men treated due to infertility is affected by their reproductive problems.
- The type of treatment had an impact on quality of life in men who were undergoing infertility treatment.
- Rural place of residence, increased BMI, non-ART treatment has a negative impact on quality of life of men treated for infertility.
- Attention should be paid to health, psychological, and environmental factors which deteriorate the quality of life of male patients undergoing infertility treatment, because stress associated with a low quality of life may result in worse outcomes of treatment.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sun, H.; Gong, T.T.; Jiang, Y.T.; Zhang, S.; Zhao, Y.H.; Wu, Q.J. Global, Regional, and National Prevalence and Disability-Adjusted Life-Years for Infertility in 195 Countries and Territories, 1990–2017: Results from a Global Burden of Disease Study, 2017. Aging 2019, 11, 10952. [Google Scholar] [CrossRef]
- Zegers-Hochschild, F.; Dickens, B.M.; Dughman-Manzur, S. Human Rights to in Vitro Fertilization. Int. J. Gynecol. Obstet. 2013, 123, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Ministerstwo Zdrowia Program Kompleksowej Ochrony Zdrowia Prokreacyjnego w Polsce w Latach 2016–2020. Available online: http://www.archiwum.mz.gov.pl/wp-content/uploads/2018/01/2017-program-kompleksowej-ochrony-zdrowia-prokreacyjnego-nowelizacja-24072017.pdf (accessed on 12 December 2021).
- Namdar, A.; Naghizadeh, M.M.; Zamani, M.; Yaghmaei, F.; Sameni, M.H. Quality of Life and General Health of Infertile Women. Health Qual. Life Outcomes 2017, 15, 139. [Google Scholar] [CrossRef] [PubMed]
- Ying, L.Y.; Wu, L.H.; Loke, A.Y. Gender Differences in Experiences with and Adjustments to Infertility: A Literature Review. Int. J. Nurs. Stud. 2015, 52, 1640–1652. [Google Scholar] [CrossRef] [PubMed]
- Petok, W.D. The Psychology of Gender-Specific Infertility Diagnoses. In Infertility Counseling: A Comprehensive Handbook for Clinicians; Cambridge University Press: Cambridge, UK, 2006; pp. 37–60. [Google Scholar] [CrossRef]
- Gao, J.; Zhang, X.; Su, P.; Liu, J.; Shi, K.; Hao, Z.; Zhou, J.; Liang, C. Relationship between Sexual Dysfunction and Psychological Burden in Men with Infertility: A Large Observational Study in China. J. Sex. Med. 2013, 10, 1935–1942. [Google Scholar] [CrossRef]
- Ahmadi, H.; Montaser-Kouhsari, L.; Nowroozi, M.R.; Bazargan-Hejazi, S. Male Infertility and Depression: A Neglected Problem in the Middle East. J. Sex. Med. 2011, 8, 824–830. [Google Scholar] [CrossRef]
- Peronace, L.A.; Boivin, J.; Schmidt, L. Patterns of Suffering and Social Interactions in Infertile Men: 12 Months after Unsuccessful Treatment. J. Psychosom. Obstet. Gynecol. 2007, 28, 105–114. [Google Scholar] [CrossRef]
- Wischmann, T.; Thorn, P. (Male) Infertility: What Does It Mean to Men? New Evidence from Quantitative and Qualitative Studies. Reprod. Biomed. Online 2013, 27, 236–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordkap, L.; Jensen, T.K.; Hansen, Å.M.; Lassen, T.H.; Bang, A.K.; Joensen, U.N.; Jensen, M.B.; Skakkebæk, N.E.; Jørgensen, N. Psychological Stress and Testicular Function: A Cross-Sectional Study of 1215 Danish Men. Fertil. Steril. 2016, 105, 174–187.e2. [Google Scholar] [CrossRef] [Green Version]
- Boivin, J.; Schmidt, L. Infertility-Related Stress in Men and Women Predicts Treatment Outcome 1 Year Later. Fertil. Steril. 2005, 83, 1745–1752. [Google Scholar] [CrossRef]
- Rooney, K.L.; Domar, A.D. The Relationship between Stress and Infertility. Dialogues Clin. Neurosci. 2018, 20, 41. [Google Scholar] [CrossRef] [PubMed]
- Keramat, A.; Masoumi, S.Z.; Mousavi, S.A.; Poorolajal, J.; Shobeiri, F.; Hazavehie, S.M.M. Quality of Life and Its Related Factors in Infertile Couples. J. Res. Health Sci. 2014, 14, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Santoro, N.; Eisenberg, E.; Trussell, J.C.; Craig, L.B.; Gracia, C.; Huang, H.; Alvero, R.; Casson, P.; Christman, G.; Coutifaris, C.; et al. Fertility-Related Quality of Life from Two RCT Cohorts with Infertility: Unexplained Infertility and Polycystic Ovary Syndrome. Hum. Reprod. 2016, 31, 2268–2279. [Google Scholar] [CrossRef] [PubMed]
- Asazawa, K.; Jitsuzaki, M.; Mori, A.; Ichikawa, T.; Shinozaki, K.; Porter, S.E. Quality-of-Life Predictors for Men Undergoing Infertility Treatment in Japan. Jpn. J. Nurs. Sci. 2019, 16, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Wdowiak, A.; Anusiewicz, A.; Bakalczuk, G.; Raczkiewicz, D.; Janczyk, P.; Makara-Studzińska, M. Assessment of Quality of Life in Infertility Treated Women in Poland. Int. J. Environ. Res. Public Health 2021, 18, 4275. [Google Scholar] [CrossRef] [PubMed]
- Zegers-Hochschild, F.; Adamson, G.D.; de Mouzon, J.; Ishihara, O.; Mansour, R.; Nygren, K.; Sullivan, E.; Vanderpoel, S. International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) revised glossary of ART terminology, 2009. Fertil. Steril. 2009, 92, 1520–1524. [Google Scholar] [CrossRef] [PubMed]
- Jaracz, K.; Kalfoss, M.; Górna, K.; Bączyk, G. Quality of life in Polish respondents: Psychometric properties of the Polish WHOQOL–Bref. Scand. J. Caring Sci. 2006, 20, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Boivin, J.; Takefman, J.; Braverman, A. The Fertility Quality of Life (FertiQoL) tool: Development and general psychometric properties. Fertil. Steril. 2011, 96, 409–415.e3. [Google Scholar] [CrossRef] [PubMed]
- Bolsoy, N.; Taspinar, A.; Kavlak, O.; Sirin, A. Differences in Quality of Life between Infertile Women and Men in Turkey. J. Obstet. Gynecol. Neonatal Nurs. JOGNN 2010, 39, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Karaca, A.; Unsal, G. Psychosocial Problems and Coping Strategies among Turkish Women with Infertility. Asian Nurs. Res. 2015, 9, 243–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galhardo, A.; Cunha, M.; Pinto-Gouveia, J.; Matos, M. The Mediator Role of Emotion Regulation Processes on Infertility-Related Stress. J. Clin. Psychol. Med. Settings 2013, 20, 497–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cserepes, R.E.; Kollár, J.; Sápy, T.; Wischmann, T.; Bugán, A. Effects of Gender Roles, Child Wish Motives, Subjective Well-Being, and Marital Adjustment on Infertility-Related Stress: A Preliminary Study with a Hungarian Sample of Involuntary Childless Men and Women. Arch. Gynecol. Obstet. 2013, 288, 925–932. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.Y.; Lin, M.W.; Hwang, J.L.; Lee, M.S.; Wu, M.H. The Fertility Quality of Life (FertiQoL) Questionnaire in Taiwanese Infertilecouples. Taiwan. J. Obstet. Gynecol. 2013, 52, 204–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warchol-Biedermann, K. The Etiology of Infertility Affects Fertility Quality of Life of Males Undergoing Fertility Workup and Treatment. Am. J. Men’s Health 2021, 15, 1557988320982167. [Google Scholar] [CrossRef] [PubMed]
- Wadadekar, G.; Inamdar, D.; Nimbargi, V. Assessment of Impact of Infertility & Its Treatment on Quality of Life of Infertile Couples Using Fertility Quality of Life Questionnaire. J. Hum. Reprod. Sci. 2021, 14, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Agostini, F.; Monti, F.; Andrei, F.; Paterlini, M.; Palomba, S.; La Sala, G.B. Assisted Reproductive Technology Treatments and Quality of Life: A Longitudinal Study among Subfertile Women and Men. J. Assist. Reprod. Genet. 2017, 34, 1307–1315. [Google Scholar] [CrossRef] [PubMed]
- Chachamovich, J.R.; Chachamovich, E.; Ezer, H.; Fleck, M.P.; Knauth, D.; Passos, E.P. Investigating Quality of Life and Health-Related Quality of Life in Infertility: A Systematic Review. J. Psychosom. Obstet. Gynaecol. 2010, 31, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Jahromi, B.N.; Mansouri, M.; Forouhari, S.; Poordast, T.; Salehi, A. Quality of Life and Its Influencing Factors of Couples Referred to An Infertility Center in Shiraz, Iran. Int. J. Fertil. Steril. 2018, 11, 293–297. [Google Scholar] [CrossRef]
- Greil, A.L.; Slauson-Blevins, K.; McQuillan, J. The Experience of Infertility: A Review of Recent Literature. Sociol. Health Illn. 2010, 32, 140–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sexty, R.E.; Hamadneh, J.; Rösner, S.; Strowitzki, T.; Ditzen, B.; Toth, B.; Wischmann, T. Cross-Cultural Comparison of Fertility Specific Quality of Life in German, Hungarian and Jordanian Couples Attending a Fertility Center. Health Qual. Life Outcomes 2016, 14, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korolczuk, E. Niepłodność, Tożsamość, Obywatelstwo. Analiza Społecznej Mobilizacji Wokół Dostępu Do in Vitro w Polsce. Etnogr. Biomed. 2014, 1, 69–70. [Google Scholar] [CrossRef]
- Makara-Studzinśka, M.; Wdowiak, A.; Bakalczuk, G.; Bakalczuk, S.; Krys, K. Emotional Problems among Couples Treated for Infertility [Problemy Emocjonalne Wśród Par Leczonych z Powodu Niepłodności]. Seksuologia Pol. 2012, 10, 28–35. [Google Scholar]
- Aarts, J.W.M.; van Empel, I.W.H.; Boivin, J.; Nelen, W.L.; Kremer, J.A.M.; Verhaak, C.M. Relationship between Quality of Life and Distress in Infertility: A Validation Study of the Dutch FertiQoL. Hum. Reprod. 2011, 26, 1112–1118. [Google Scholar] [CrossRef]
- Banerjee, S.; Mary, M.N. Exploring Quality of Life and Perceived Experiences among Couples Undergoing Fertility Treatment in Western India: A Mixed Methodology. Int. J. Curr. Res. Rev. 2020, 12, 118–123. [Google Scholar] [CrossRef]
- Sexty, R.E.; Griesinger, G.; Kayser, J.; Lallinger, M.; Rösner, S.; Strowitzki, T.; Toth, B.; Wischmann, T. Psychometric Characteristics of the FertiQoL Questionnaire in a German Sample of Infertile Individuals and Couples. Health Qual. Life Outcomes 2018, 16, 233. [Google Scholar] [CrossRef] [PubMed]
- Barry, D.; Pietrzak, R.H.; Petry, N.M. Gender Differences in Associations between Body Mass Index and DSM-IV Mood and Anxiety Disorders: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. Ann. Epidemiol. 2008, 18, 458–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable, Parameter | IU or Category | Infertility Treated Men | Control Group (N = 100) | Comparison between Groups p | ||
|---|---|---|---|---|---|---|
| Non-ART (N = 400) | IUI (N = 400) | IVF (N = 400) | ||||
| Age, Min–Max M ± SD | years | 24–52 34.9 ± 4.5 | 25–54 35.0 ± 5.0 | 26–53 35.6 ± 4.3 | 25–51 34.7 ± 4.6 | 0.104 |
| Place of residence, n (%) | city | 154 (38.50) | 162 (40.50) | 149 (37.25) | 51 (51.00) | 0.055 |
| town | 120 (30.00) | 97 (24.25) | 98 (24.50) | 22 (22.00) | ||
| rural area | 126 (31.50) | 141 (35.25) | 153 (38.25) | 27 (27.00) | ||
| Level of education, n (%) | basic vocational | 63 (15.75) | 40 (10.00) | 46 (11.50) | 16 (16.00) | 0.065 |
| secondary | 128 (32.00) | 152 (38.00) | 132 (33.00) | 40 (40.00) | ||
| tertiary | 209 (52.25) | 208 (52.00) | 222 (55.50) | 44 (44.00) | ||
| BMI, Min–Max M ± SD | kg/m2 | 21.4–36.2 27.2 ± 2.8 | 16.9–38.1 27.0 ± 3.6 | 17.3–42.9 27.1 ± 2.9 | 16.7–36.2 27.5 ± 3.8 | 0.540 |
| BMI, n (%) | underweight | 0 (0.00) | 7 (1.75) | 2 (0.50) | 3 (3.00) | <0.001 |
| normal weight | 102 (25.00) | 103 (25.75) | 80 (20.00) | 21 (21.00) | ||
| overweight | 230 (57.50) | 216 (54.00) | 267 (66.75) | 51 (51.00) | ||
| obesity | 68 (17.00) | 14 (18.50) | 51 (12.75) | 25 (25.00) | ||
| Having children, n (%) | yes, from the current relationship | 20 (5.00) | 40 (10.00) | 30 (7.50) | 100 (100.00) | 0.039 * |
| yes, from a previous relationship | 26 (6.50) | 25 (6.25) | 16 (4.00) | |||
| no | 354 (88.50) | 335 (83.75) | 354 (88.50) | 0 (0.00) | ||
| Time trying to conceive a child, Min–Max M ± SD | years | 1–10 3.2 ± 1.9 | 1–9 3.1 ± 1.9 | 1–14 3.4 ± 2.0 | - | 0.219 |
| Type of job, n (%) | manual | 130 (32.50) | 98 (24.50) | 126 (31.50) | 32 (32.00) | 0.069 |
| non-manual | 151 (37.75) | 145 (36.25) | 146 (36.50) | 33 (33.00) | ||
| mixed | 119 (29.75) | 157 (39.25) | 128 (32.00) | 35 (35.00) | ||
| Working hours, n (%) | fixed | 160 (40.00) | 143 (35.75) | 147 (36.75) | 36 (36.00) | <0.001 |
| shift work | 148 (37.00) | 117 (29.25) | 151 (37.75) | 26 (26.00) | ||
| flexible | 92 (23.00) | 140 (35.00) | 102 (25.50) | 38 (38.00) | ||
| Monthly net income per 1 person in a household (thousand PLN), n (%) | below 1 | 45 (11.25) | 27 (6.75) | 36 (9.00) | 2 (2.00) | <0.001 |
| 1–1.5 | 109 (27.25) | 94 (23.50) | 119 (29.75) | 21 (21.00) | ||
| 1.5–2 | 119 (29.75) | 102 (25.50) | 120 (30.00) | 23 (23.00) | ||
| above 2 | 127 (31.75) | 177 (44.25) | 125 (31.25) | 54 (54.00) | ||
| Domain | Infertility Treated Men | Control Group (N = 100) | Comparison between Groups p | p for Post Hoc Tests | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Non-ART (N = 400) | IUI (N = 400) | IVF (N = 400) | Non-ART vs. Control | IUI vs. Control | IVF vs. Control | Non-ART vs. IUI | Non-ART vs. IVF | IUI vs. IVF | |||
| M ± SD | |||||||||||
| Physical health | 56.0 ± 7.6 | 55.4 ± 7.8 | 54.3 ± 6.2 | 55.7 ± 8.6 | 0.015 | 0.737 | 0.737 | 0.099 | 0.288 | 0.002 | 0.038 |
| Psychological | 66.0 ± 8.4 | 66.7± 7.5 | 67.0 ± 8.5 | 68.0 ± 7.4 | 0.111 | n/a | n/a | n/a | n/a | n/a | n/a |
| Social relationships | 69.3 ± 11.1 | 71.0 ± 11.3 | 71.0 ± 12.5 | 71.8 ± 11.7 | 0.060 | n/a | n/a | n/a | n/a | n/a | n/a |
| Environment | 69.4 ± 7.2 | 68.4 ± 7.2 | 68.5 ± 8.7 | 71.1 ± 7.3 | 0.009 | 0.050 | 0.002 | 0.004 | 0.085 | 0.129 | 0.841 |
| Domain | Infertility Treated Men | Comparison between Groups p | p for Post Hoc Tests | ||||
|---|---|---|---|---|---|---|---|
| Non-ART (N = 400) | IUI (N = 400) | IVF (N = 400) | Non-ART vs. IUI | Non-ART vs. IVF | IUI vs. IVF | ||
| M ± SD | |||||||
| Total FertiQoL | 68.8 ± 11.3 | 71.0 ±11.2 | 69.8 ± 11.8 | 0.029 | 0.008 | 0.204 | 0.162 |
| Core FertiQoL | 67.8 ± 13.1 | 71.1 ± 13.1 | 68.5 ± 12.0 | 0.001 | <0.001 | 0.471 | 0.004 |
| Emotional | 64.2 ± 17.1 | 67.9 ± 17.6 | 66.5 ± 14.9 | 0.006 | 0.001 | 0.050 | 0.217 |
| Mind/body | 69.4 ± 17.7 | 73.6 ± 17.2 | 70.2 ± 15.9 | 0.001 | <0.001 | 0.504 | 0.005 |
| Relational | 72.2 ± 16.7 | 76.2 ± 16.0 | 72.9 ± 15.6 | 0.001 | <0.001 | 0.523 | 0.004 |
| Social | 65.6 ± 14.6 | 66.6 ± 14.9 | 64.4 ± 13.7 | 0.099 | n/a | n/a | n/a |
| Treatment FertiQoL | 69.8 ± 12.2 | 70.9 ±11.7 | 71.2 ± 13.8 | 0.255 | n/a | n/a | n/a |
| Environment | 64.5 ± 13.5 | 64.8 ± 13.9 | 67.2± 13.8 | 0.009 | 0.788 | 0.005 | 0.012 |
| Tolerability | 75.1 ± 15.8 | 77.0 ± 16.7 | 75.2 ± 18.5 | 0.201 | n/a | n/a | n/a |
| Covariate | IU or Category | Infertility Treated Men | |||||
|---|---|---|---|---|---|---|---|
| Non-ART (N = 400) | IUI (N = 400) | IVF (N = 400) | |||||
| b | p | b | p | b | p | ||
| Age | years | 0.12 | 0.360 | 0.35 | 0.002 | −0.44 | 0.001 |
| Place of residence | city | −1.01 | 0.204 | 1.17 | 0.125 | 1.92 | 0.018 |
| town | 2.54 | 0.002 | 2.61 | 0.001 | 1.90 | 0.313 | |
| rural area | reference | ||||||
| Level of education | basic vocational or secondary | 1.81 | 0.015 | 1.70 | 0.007 | 0.64 | 0.350 |
| tertiary | reference | ||||||
| BMI | kg/m2 | −0.60 | 0.005 | −0.80 | <0.001 | −0.58 | 0.004 |
| Having children | yes | 0.03 | 0.974 | 0.35 | 0.635 | −0.46 | 0.630 |
| no | reference | ||||||
| How long trying for a baby | years | −0.69 | 0.024 | −1.08 | <0.001 | −0.27 | 0.391 |
| Type of job | non-manual | reference | |||||
| manual or mixed | −0.59 | 0.439 | 0.73 | 0.270 | −2.81 | <0.001 | |
| Working hours | fixed | 1.63 | 0.010 | 0.97 | 0.096 | −0.81 | 0.229 |
| shift or flexible | reference | ||||||
| Monthly net income per 1 person in a household (thousand PLN) | below 1.5 | reference | |||||
| 1.5–2 | 1.20 | 0.138 | 1.22 | 0.133 | 0.33 | 0.691 | |
| above 2 | −0.17 | 0.838 | −0.57 | 0.429 | 0.20 | 0.816 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makara-Studzińska, M.; Limanin, A.; Anusiewicz, A.; Janczyk, P.; Raczkiewicz, D.; Wdowiak-Filip, A.; Filip, M.; Bojar, I.; Lukaszuk, K.; Wdowiak, A. Assessment of Quality of Life in Men Treated for Infertility in Poland. Int. J. Environ. Res. Public Health 2022, 19, 2950. https://doi.org/10.3390/ijerph19052950
Makara-Studzińska M, Limanin A, Anusiewicz A, Janczyk P, Raczkiewicz D, Wdowiak-Filip A, Filip M, Bojar I, Lukaszuk K, Wdowiak A. Assessment of Quality of Life in Men Treated for Infertility in Poland. International Journal of Environmental Research and Public Health. 2022; 19(5):2950. https://doi.org/10.3390/ijerph19052950
Chicago/Turabian StyleMakara-Studzińska, Marta, Agnieszka Limanin, Agnieszka Anusiewicz, Paula Janczyk, Dorota Raczkiewicz, Anita Wdowiak-Filip, Michał Filip, Iwona Bojar, Krzysztof Lukaszuk, and Artur Wdowiak. 2022. "Assessment of Quality of Life in Men Treated for Infertility in Poland" International Journal of Environmental Research and Public Health 19, no. 5: 2950. https://doi.org/10.3390/ijerph19052950
APA StyleMakara-Studzińska, M., Limanin, A., Anusiewicz, A., Janczyk, P., Raczkiewicz, D., Wdowiak-Filip, A., Filip, M., Bojar, I., Lukaszuk, K., & Wdowiak, A. (2022). Assessment of Quality of Life in Men Treated for Infertility in Poland. International Journal of Environmental Research and Public Health, 19(5), 2950. https://doi.org/10.3390/ijerph19052950