
The Effects of Adding Art Therapy to Ongoing Antidepressant Treatment in Moderate-to-Severe Major Depressive Disorder: A Randomized Controlled Study


Abstract
:1. Introduction
2. Materials and Methods
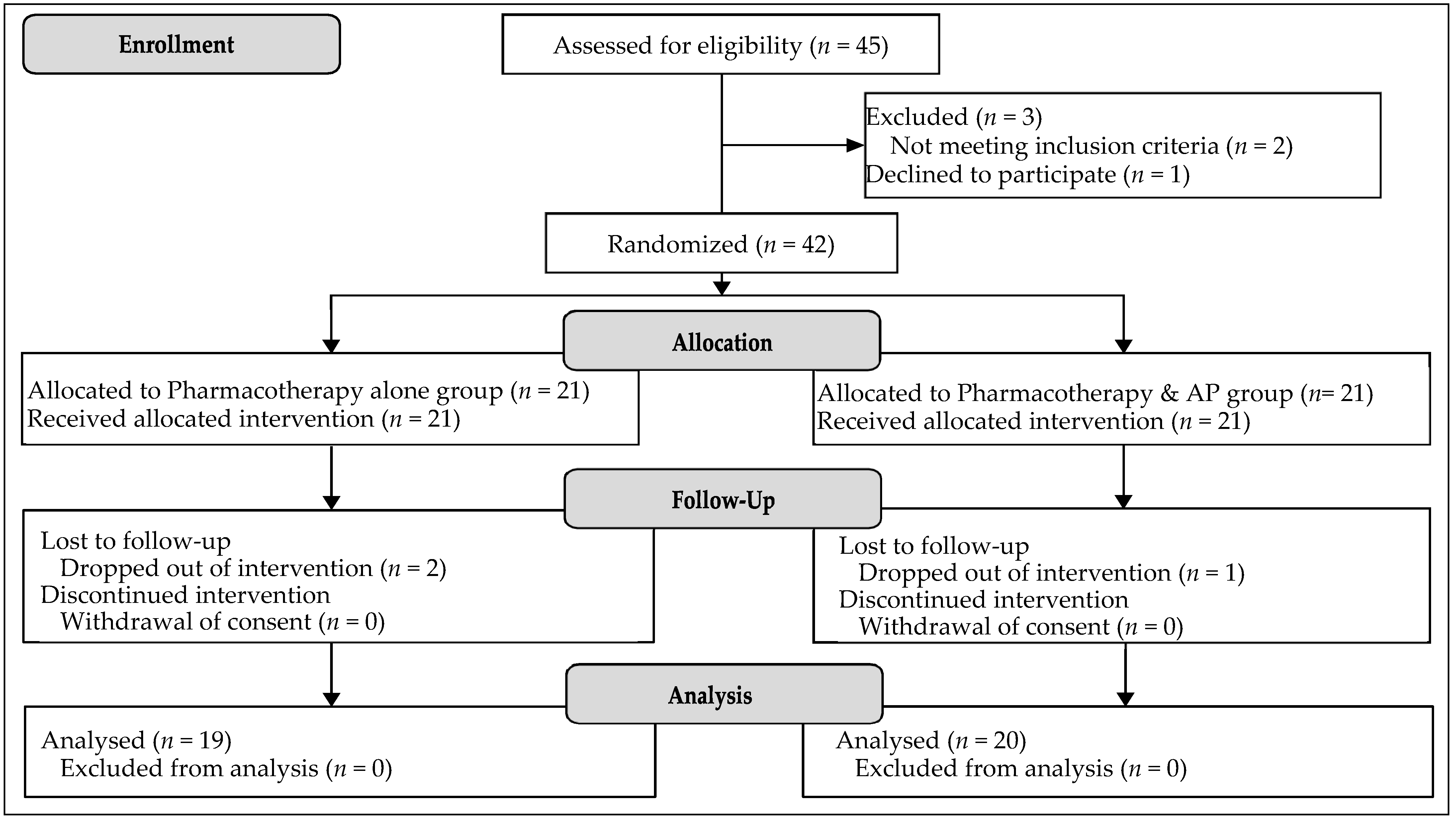
2.1. Design
2.2. Sample Size
2.3. Sample
2.4. Intervention
2.5. Assessments
2.6. Procedure
2.7. Statistical Analyses
3. Results
3.1. Demographic Characteristics between the Experimental and Control Groups
3.2. Primary Outcomes: Experimental versus Control
3.3. Secondary Outcomes: Moderate MDD versus Severe MDD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gutiérrez-Rojas, L.; Porras-Segovia, A.; Dunne, H.; Andrade-González, N.; Cervilla, J.A. Prevalence and correlates of major depressive disorder: A systematic review. Rev. Bras. de Psiquiatr. 2020, 42, 657–672. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, M.H. Major Depressive Disorder in Primary Care: Strategies for Identification. J. Clin. Psychiatry 2020, 81. [Google Scholar] [CrossRef]
- AFSP. Suicide Risk Factors and Warning Signs. Available online: https://afsp.org/risk-factors-protective-factors-and-warning-signs#risk-factors (accessed on 26 February 2022).
- CDCP. Risk and Protective Factors. Available online: https://www.cdc.gov/suicide/factors/ (accessed on 26 February 2022).
- NIMH. Suicide Prevention. Available online: https://www.nimh.nih.gov/health/topics/suicide-prevention#part_153178 (accessed on 26 February 2022).
- World Health Organisation. Suicide: Key Facts. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 16 February 2021).
- Yang, L.; Zhao, Y.; Wang, Y.; Liu, L.; Zhang, X.; Li, B.; Cui, R. The Effects of Psychological Stress on Depression. Curr. Neuropharmacol. 2015, 13, 494–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciasca, E.C.; Ferreira, R.C.; Santana, C.L.; Forlenza, O.V.; dos Santos, G.D.; Brum, P.S.; Nunes, P.V. Art therapy as an adjuvant treatment for depression in elderly women: A randomized controlled trial. Rev. Bras. de Psiquiatr. 2018, 40, 256–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hays, R.D.; Wells, K.B.; Sherbourne, C.D.; Rogers, W.; Spritzer, K. Functioning and Well-being Outcomes of Patients With Depression Compared With Chronic General Medical Illnesses. Arch. Gen. Psychiatry 1995, 52, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Ishak, W.W.; James, D.M.; Mirocha, J.; Youssef, H.; Tobia, G.; Pi, S.; Collison, K.L.; Cohen, R.M. Patient-reported functioning in major depressive disorder. Ther. Adv. Chronic Dis. 2016, 7, 160–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumiyoshi, T.; Watanabe, K.; Noto, S.; Sakamoto, S.; Moriguchi, Y.; Hammer-Helmich, L.; Fernandez, J. Relationship of Subjective Cognitive Impairment with Psychosocial Function and Relapse of Depressive Symptoms in Patients with Major Depressive Disorder: Analysis of Longitudinal Data from PERFORM-J. Neuropsychiatr. Dis. Treat. 2021, 17, 945–955. [Google Scholar] [CrossRef] [PubMed]
- Fava, G.A.; Park, S.K.; Sonino, N. Treatment of recurrent depression. Expert Rev. Neurother. 2006, 6, 1735–1740. [Google Scholar] [CrossRef]
- Limosin, F.; Mekaoui, L.; Hautecouverture, S. Stratégies thérapeutiques prophylactiques dans la dépression unipolaire. La Presse Médicale 2007, 36, 1627–1633. [Google Scholar] [CrossRef]
- Culpepper, L.; Muskin, P.R.; Stahl, S.M. Major Depressive Disorder: Understanding the Significance of Residual Symptoms and Balancing Efficacy with Tolerability. Am. J. Med. 2015, 128, S1–S15. [Google Scholar] [CrossRef]
- Eaton, W.W.; Shao, H.; Nestadt, G.; Lee, B.H.; Bienvenu, J.; Zandi, P. Population-Based Study of First Onset and Chronicity in Major Depressive Disorder. Arch. Gen. Psychiatry 2008, 65, 513–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuijpers, P.; Huibers, M.J.H.; Furukawa, T. The Need for Research on Treatments of Chronic Depression. JAMA Psychiatry 2017, 74, 242–243. [Google Scholar] [CrossRef] [PubMed]
- Köhler, S.; Wiethoff, K.; Ricken, R.; Stamm, T.; Baghai, T.C.; Fisher, R.; Seemüller, F.; Brieger, P.; Cordes, J.; Malevani, J.; et al. Characteristics and differences in treatment outcome of inpatients with chronic vs. episodic major depressive disorders. J. Affect. Disord. 2014, 173, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Turner, E.H.; Mohr, D.C.; Hofmann, S.G.; Andersson, G.; Berking, M.; Coyne, J. Comparison of psychotherapies for adult depression to pill placebo control groups: A meta-analysis. Psychol. Med. 2013, 44, 685–695. [Google Scholar] [CrossRef] [Green Version]
- Panel, AHCPR Depression Guideline. Clinical Practice Guideline Number 5. Depression in Primary Care. Volume 2: Treatment of Major Depression. AHCPR Publication no. 93-0550. Rockville (MD): Agency for Health Care Policy and Research; Public Health Services, US Department of Health and Human Services: Washington, DC, USA, 1993.
- Gelenberg, A.J.; Freeman, M.P.; Markowitz, J.C.; Rosenbaum, J.F.; Thase, M.E.; Trivedi, M.H.; Van Rhoads, R.S. American Psychiatric Association Practice Guideline for the Treatment of Patients With Major Depressive Disorder, Third Edition. Am. J. Psychiatry 2010, 167, 9–118. [Google Scholar]
- Management of Major Depressive Disorder Working Group. Clinical Practice Guideline for the Management of Major Depressive Disorder in Adults, Version 2.0; Veterans Health Administration/Department of Defense: Washington, DC, USA, 2000.
- Driessen, E.; Cuijpers, P.; de Maat, S.C.; Abbass, A.A.; de Jonghe, F.; Dekker, J.J. The efficacy of short-term psychodynamic psychotherapy for depression: A meta-analysis. Clin. Psychol. Rev. 2010, 30, 25–36. [Google Scholar] [CrossRef]
- Karyotaki, E.; Smit, Y.; Henningsen, K.H.; Huibers, M.; Robays, J.; de Beurs, D.; Cuijpers, P. Combining pharmacotherapy and psychotherapy or monotherapy for major depression? A meta-analysis on the long-term effects. J. Affect. Disord. 2016, 194, 144–152. [Google Scholar] [CrossRef] [Green Version]
- Pampallona, S.; Bollini, P.; Tibaldi, G.; Kupelnick, B.; Munizza, C. Combined pharmacotherapy and psychological treatment for depression: A systematic review. Arch. Gen. Psychiatry 2004, 61, 714–719. [Google Scholar] [CrossRef] [Green Version]
- von Wolff, A.; Hölzel, L.P.; Westphal, A.; Härter, M.; Kriston, L. Combination of pharmacotherapy and psychotherapy in the treatment of chronic depression: A systematic review and meta-analysis. BMC Psychiatry 2012, 12, 61. [Google Scholar] [CrossRef] [Green Version]
- Cuijpers, P.; Noma, H.; Karyotaki, E.; Vinkers, C.H.; Cipriani, A.; Furukawa, T.A. A network meta-analysis of the effects of psychotherapies, pharmacotherapies and their combination in the treatment of adult depression. World Psychiatry 2020, 19, 92–107. [Google Scholar] [CrossRef] [Green Version]
- Cuijpers, P.; Oud, M.; Karyotaki, E.; Noma, H.; Quero, S.; Cipriani, A.; Arroll, B.; Furukawa, T.A. Psychologic Treatment of Depression Compared With Pharmacotherapy and Combined Treatment in Primary Care: A Network Meta-Analysis. Ann. Fam. Med. 2021, 19, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Bekhuis, E.; Schoevers, R.; De Boer, M.; Peen, J.; Dekker, J.; Van, H.; Boschloo, L. Symptom-Specific Effects of Psychotherapy versus Combined Therapy in the Treatment of Mild to Moderate Depression: A Network Approach. Psychother. Psychosom. 2018, 87, 121–123. [Google Scholar] [CrossRef] [PubMed]
- Segal, Z.; Vincent, P.; Levitt, A. Efficacy of combined, sequential and crossover psychotherapy and pharmacotherapy in improving outcomes in depression. J. Psychiatry Neurosci. 2002, 27, 281–290. [Google Scholar]
- Ijaz, S.; Davies, P.; Williams, C.J.; Kessler, D.; Lewis, G.; Wiles, N. Psychological therapies for treatment-resistant depression in adults. Cochrane Database Syst. Rev. 2018, 2018, CD010558. [Google Scholar] [CrossRef] [Green Version]
- Mohacsy, I. Nonverbal communication and its place in the therapy session. Arts Psychother. 1995, 22, 31–38. [Google Scholar] [CrossRef]
- Malchiodi, C.A. Expressive Therapies: History, Theory and Practice; McGraw-Hill: New York, NY, USA, 2005. [Google Scholar]
- Haeyen, S.; Chakhssi, F.; Van Hooren, S. Benefits of Art Therapy in People Diagnosed With Personality Disorders: A Quantitative Survey. Front. Psychol. 2020, 11, 686. [Google Scholar] [CrossRef] [PubMed]
- Mercer, A.; Warson, E.; Zhao, J. Visual journaling: An intervention to influence stress, anxiety and affect levels in medical students. Arts Psychother. 2010, 37, 143–148. [Google Scholar] [CrossRef]
- Kramer, E. Art as Therapy: Collected Papers; Jessica Kingsley Publishers: London, UK, 2001. [Google Scholar]
- Hanevik, H.; Hestad, K.A.; Lien, L.; Teglbjaerg, H.S.; Danbolt, L.J. Expressive art therapy for psychosis: A multiple case study. Arts Psychother. 2013, 40, 312–321. [Google Scholar] [CrossRef] [Green Version]
- Nan, J.K.; Ho, R.T. Effects of clay art therapy on adults outpatients with major depressive disorder: A randomized controlled trial. J. Affect. Disord. 2017, 217, 237–245. [Google Scholar] [CrossRef]
- Korostiy, V.; Hmain, S. Influence of art therapy in complex treatment on the quality of remission in patients with recurrent depressive disorder. Eur. Psychiatry 2016, 33, S559. [Google Scholar] [CrossRef]
- Choi, H.; Jung, D.-J.; Jeon, Y.-H.; Kim, M.J. The effects of combining art psychotherapy with pharmacotherapy in treating major depressive disorder: Randomized control study. Arts Psychother. 2020, 70, 101689. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Gilmer, W.S.; Trivedi, M.H.; Rush, A.; Wisniewski, S.; Luther, J.; Howland, R.H.; Yohanna, D.; Khan, A.; Alpert, J. Factors associated with chronic depressive episodes: A preliminary report from the STAR-D project. Acta Psychiatr. Scand. 2005, 112, 425–433. [Google Scholar] [CrossRef]
- Nieuwsma, J.A.; Trivedi, R.B.; McDuffie, J.; Kronish, I.; Benjamin, D.; Williams Jr, J.W. Brief psychotherapy for depression: A systematic review and meta-analysis. Int. J. Psychiatry Med. 2012, 43, 129–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klerman, G.L.; Weissman, M.M. Interpersonal Psychotherapy of Depression: A Brief, Focused, Specific Strategy; Jason Aronson, Incorporated: Lanham, MD, USA, 1994. [Google Scholar]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Beck Depression Inventory (BDI-II); Pearson: London, UK, 1996; Volume 10. [Google Scholar]
- Riedel, M.; Möller, H.-J.; Obermeier, M.; Schennach-Wolff, R.; Bauer, M.; Adli, M.; Kronmüller, K.; Nickel, T.; Brieger, P.; Laux, G.; et al. Response and remission criteria in major depression—A validation of current practice. J. Psychiatr. Res. 2010, 44, 1063–1068. [Google Scholar] [CrossRef]
- Zimmerman, M.; Chelminski, I.; Posternak, M. A review of studies of the Hamilton depression rating scale in healthy controls: Implications for the definition of remission in treatment studies of depression. J. Nerv. Ment. Dis. 2004, 192, 595–601. [Google Scholar] [CrossRef]
- DeRubeis, R.J.; Hollon, S.D.; Amsterdam, J.D.; Shelton, R.C.; Young, P.R.; Salomon, R.; O’Reardon, J.P.; Lovett, M.L.; Gladis, M.M.; Brown, L.L.; et al. Cognitive Therapy vs Medications in the Treatment of Moderate to Severe Depression. Arch. Gen. Psychiatry 2005, 62, 409–416. [Google Scholar] [CrossRef] [Green Version]
- Zu, S.; Xiang, Y.T.; Liu, J.; Zhang, L.; Wang, G.; Ma, X.; Kilbourne, A.M.; Ungvari, G.S.; Chiu, H.F.K.; Li, Z.J.; et al. A comparison of cognitive-behavioral therapy, antidepressants, their combination and standard treatment for Chinese patients with moderate–severe major depressive disorders. J. Affect. Disord. 2014, 152, 262–267. [Google Scholar] [CrossRef]
- Uttley, L.; Scope, A.; Stevenson, M.; Rawdin, A.; Buck, E.T.; Sutton, A.; Stevens, J.; Kaltenthaler, E.; Dent-Brown, K.; Wood, C. Systematic review and economic modelling of the clinical effectiveness and cost-effectiveness of art therapy among people with non-psychotic mental health disorders. Heal. Technol. Assess. 2015, 19, 18. [Google Scholar] [CrossRef] [Green Version]
- Springham, N.; Huet, V. Facing our shadows: Understanding harm in the arts therapies. Int. J. Art Ther. 2020, 25, 5–18. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Sub-Variables | M (SD) | χ2 or t | p | |
|---|---|---|---|---|---|
| Experimental Group | Control Group | ||||
| Age | 36.92 (12.4) | 40.62 (14.02) | −0.695 | 0.494 | |
| Gender | Male | 7 (36.8%) | 6 (30.0%) | 0.205 | 0.650 |
| Female | 12 (63.2%) | 14 (92.3%) | |||
| Depression Severity (HDRS) | Moderate | 10 (52.6) | 8 (40.0) | 0.626 | 0.429 |
| Severe | 9 (47.4) | 12 (60.0) | |||
| Duration of illness | Less than a month | 3 (15.8%) | 2 (10.0%) | 0.680 | 0.711 |
| Less than a year | 9 (47.4%) | 12 (60.0%) | |||
| Between 1 and 2 years | 7 (36.8%) | 6 (30.0%) | |||
| Variables | Group | M (SD) | t | p | d 3 | |
|---|---|---|---|---|---|---|
| Pre | Post | |||||
| HDRS 1 | Experimental | 21.58 (5.09) | 15.50 (5.00) | 6.304 *** | 0.001 | 1.81 |
| Control | 25.70 (7.29) | 23.60 (7.65) | 2.272 * | 0.049 | 0.72 | |
| BDI-II 2 | Experimental | 29.75 (5.96) | 22.92 (5.11) | 5.556 *** | 0.001 | 1.60 |
| Control | 33.33 (6.91) | 31.56 (6.93) | 1.497 | 0.173 | 0.50 | |
| Variables | Experimental Group | n | M (SD) | t | p | d 3 | |
|---|---|---|---|---|---|---|---|
| Pre | Post | ||||||
| HDRS 1 | Moderate | 10 | 15.45 (1.75) | 11.91 (2.59) | 4.485 *** | 0.001 | 1.35 |
| Severe | 9 | 25.09 (4.04) | 18.18 (3.79) | 6.820 *** | 0.001 | 2.06 | |
| BDI-II 2 | Moderate | 11 | 24.00 (2.54) | 20.70 (5.29) | 2.810 * | 0.020 | 0.89 |
| Severe | 8 | 35.64 (7.75) | 28.55 (8.44) | 5.722 *** | 0.001 | 1.73 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, M.; Choi, H.; Shin, J.; Suh, H.-S. The Effects of Adding Art Therapy to Ongoing Antidepressant Treatment in Moderate-to-Severe Major Depressive Disorder: A Randomized Controlled Study. Int. J. Environ. Res. Public Health 2023, 20, 91. https://doi.org/10.3390/ijerph20010091
Lee M, Choi H, Shin J, Suh H-S. The Effects of Adding Art Therapy to Ongoing Antidepressant Treatment in Moderate-to-Severe Major Depressive Disorder: A Randomized Controlled Study. International Journal of Environmental Research and Public Health. 2023; 20(1):91. https://doi.org/10.3390/ijerph20010091
Chicago/Turabian StyleLee, Myungjoo, Han Choi, Jiwon Shin, and Ho-Suk Suh. 2023. "The Effects of Adding Art Therapy to Ongoing Antidepressant Treatment in Moderate-to-Severe Major Depressive Disorder: A Randomized Controlled Study" International Journal of Environmental Research and Public Health 20, no. 1: 91. https://doi.org/10.3390/ijerph20010091
APA StyleLee, M., Choi, H., Shin, J., & Suh, H. -S. (2023). The Effects of Adding Art Therapy to Ongoing Antidepressant Treatment in Moderate-to-Severe Major Depressive Disorder: A Randomized Controlled Study. International Journal of Environmental Research and Public Health, 20(1), 91. https://doi.org/10.3390/ijerph20010091