
Comparing Virtual and Center-Based Cardiac Rehabilitation on Changes in Frailty

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
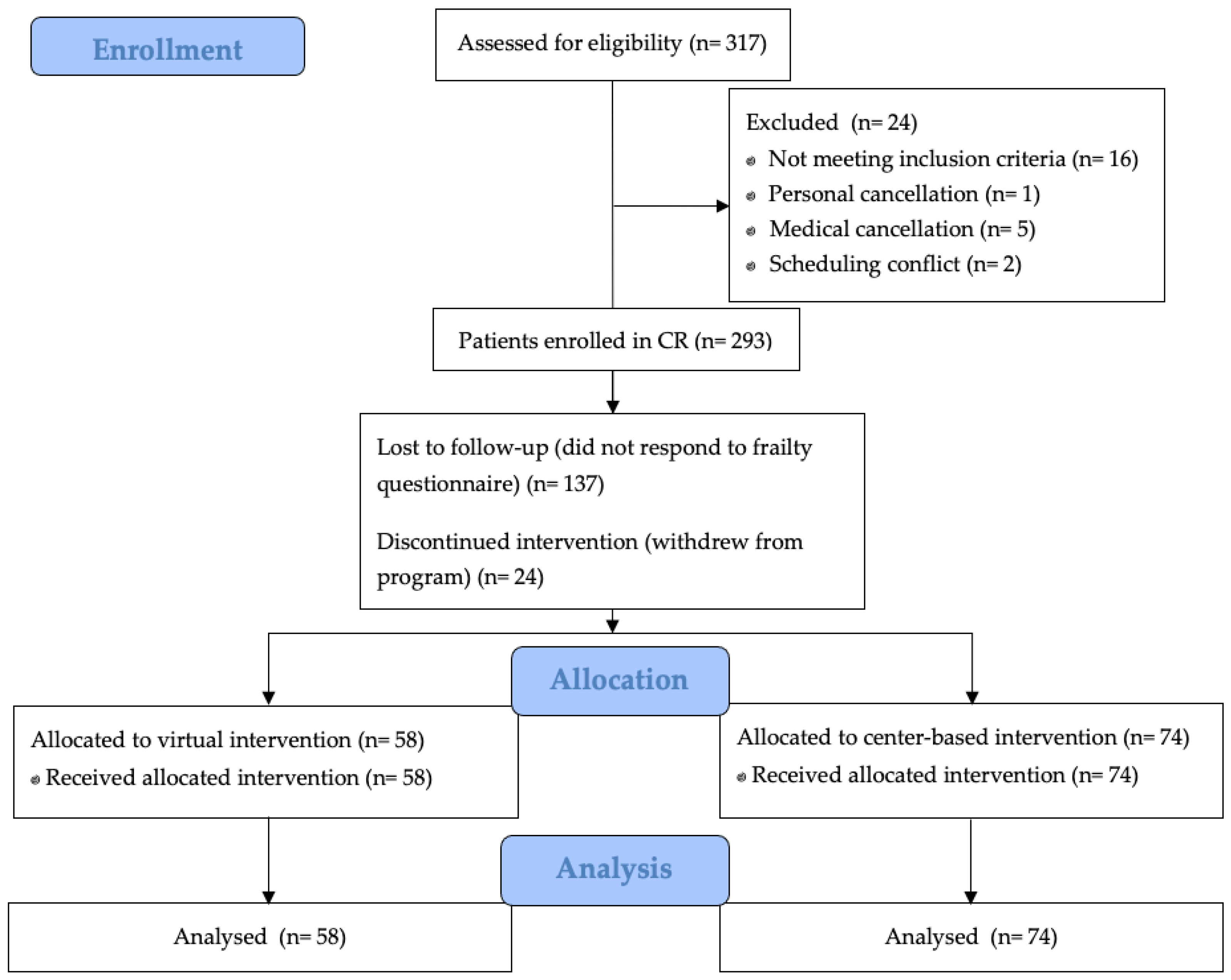
2.1. Study Design
2.2. Cardiac Rehabilitation
2.3. Frailty Index
2.4. Cardiovascular Outcomes
2.5. Statistical Analyses
2.6. Sensitivity Analyses
3. Results
3.1. Description of Participants
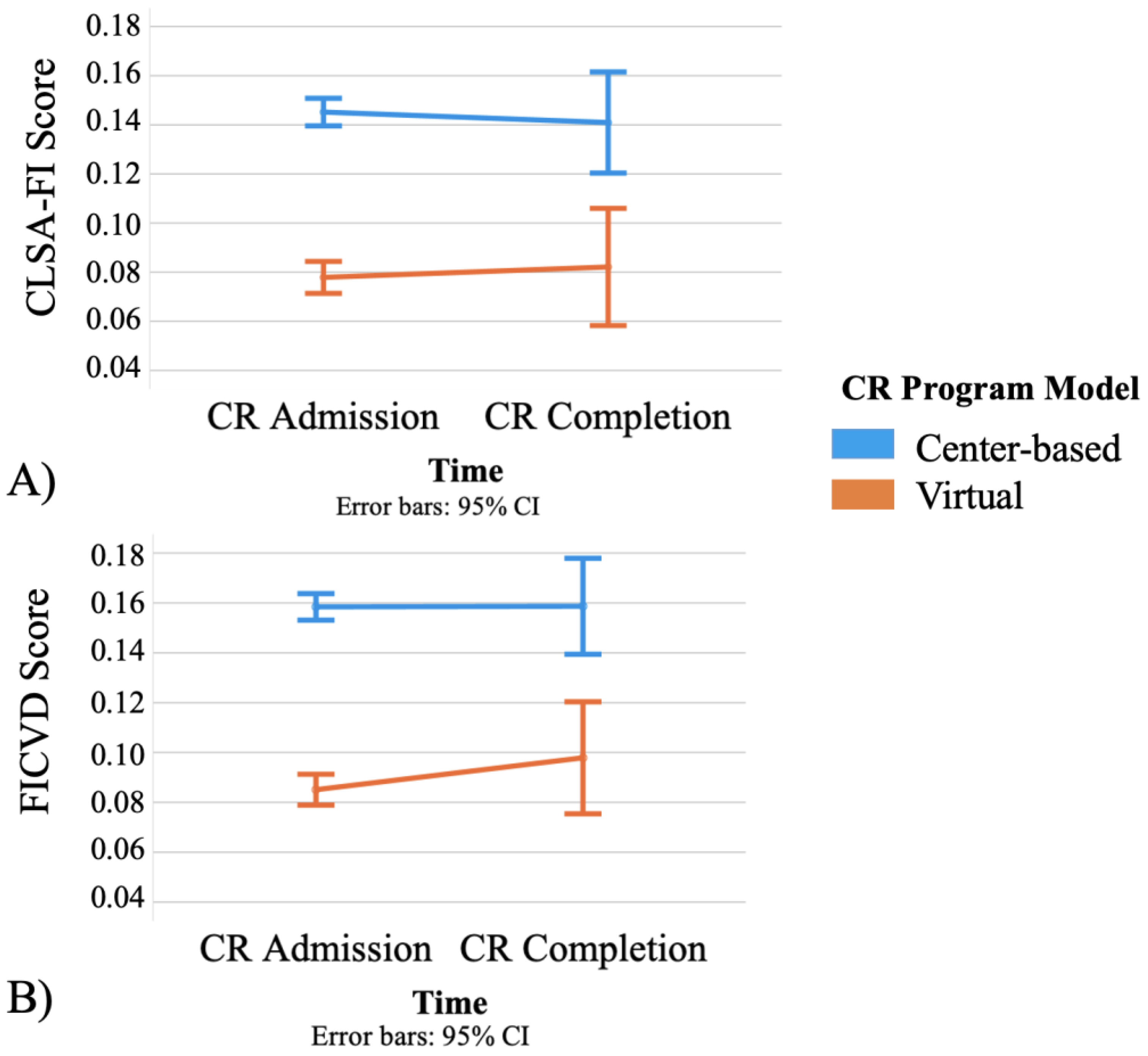
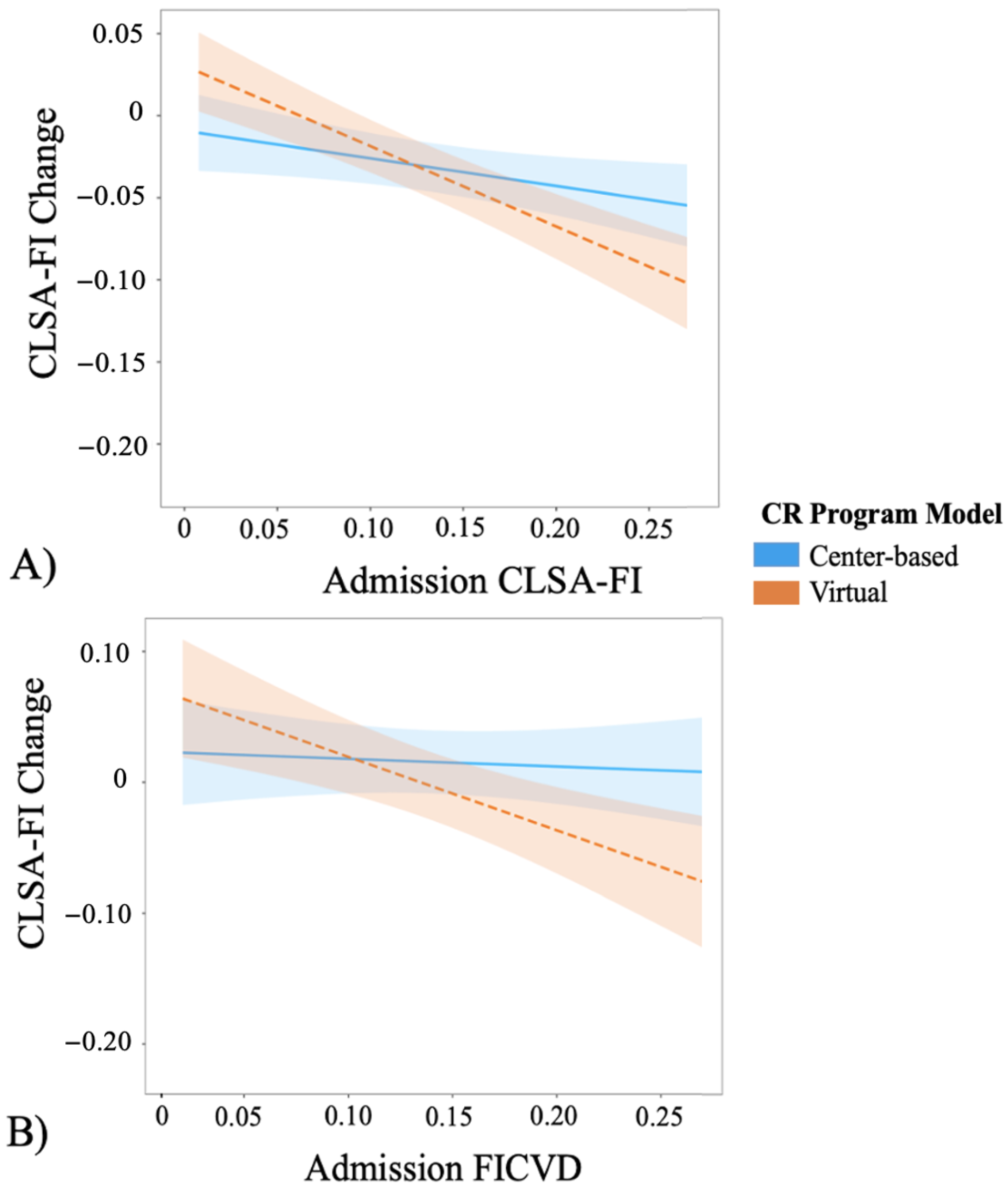
3.2. Change in Frailty between Virtual and Center-Based CR
3.3. Cardiovascular Biomarkers
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- …dress and undress yourself (including picking out clothes and putting on socks and shoes)?
- …take care of your own appearance, combing your hair, shaving?
- …walk?
- …get in and out of bed?
- …take a bath or shower (including getting in and out of the tub)?
- Yes, without help.
- Yes, with some help.
- No, unable to do so.
- …use the telephone, including looking up numbers and dialing?
- …get to places out of walking distance (i.e., you drive your own car, or travel alone on buses, or taxis)?
- …go shopping for groceries or clothes (taking care of all shopping needs yourself)?
- …prepare your own meals (i.e., you plan and cook full meals yourself)?
- …do your housework (i.e., you can clean floors, etc.)?
- …take your own medicine (in the right doses at the right time)?
- …handle your own money (i.e., you write cheques, pay bills, etc.)?
- Yes, without help.
- Yes, with some help.
- No, unable to do so.
- Reaching or extending your arms above your shoulders?
- Stooping, crouching, or kneeling down?
- Pushing or pulling large objects like a living room chair?
- Lifting 10 lbs. (or 4.5 kg) from the floor, like a heavy bag of groceries?
- Handling small objects, like picking up a coin from a table?
- Standing for a long period, around 15 min?
- Standing up after sitting in a chair?
- Walking alone up and down a flight of stairs?
- Walking 2–3 neighborhood blocks?
- Making a bed?
- Washing your back?
- Using a knife to cut food?
- Recreational or work activities in which you take some force or impact through your arm, shoulder, or hand (e.g., golf, hammering, tennis, typing, etc.)?
- No.
- Yes, a little difficult.
- Yes, somewhat difficult.
- Yes, very difficult.
- Unable to do so.
- Do not do on doctor’s orders.
- In general, would you say your health is…?
- Is your eyesight, using glasses or corrective lens if you use them…?
- Is your hearing, using a hearing aid if you use one…?
- Excellent.
- Very Good.
- Good.
- Fair.
- Poor.
- Overweight.
- Underweight.
- Just about right.
- None.
- Once.
- Twice or more.
- …that everything you did was an effort?
- …lonely?
- …that you could not “get going”?
- Rarely or never (less than 1 day).
- Some of the time (1–2 days).
- Occasionally (3–4 days).
- All of the time (5–7 days).
- Pneumonia?
- Urinary Tract Infection (UTI)?
- (Yes or no questions)
- …have osteoarthritis in the knee?
- …have osteoarthritis in the hip?
- …have osteoarthritis in one or both hands?
- …have rheumatoid arthritis?
- …have any other type of arthritis?
- …have/had any of the following- emphysema, chronic bronchitis, chronic obstructive pulmonary disease (COPD), or chronic changes in lungs due to smoking?
- …have high blood pressure or hypertension?
- …have diabetes, borderline diabetes or that your blood sugar is high?
- …have heart disease (including congestive heart failure or CHF)?
- …have angina (or chest pain due to heart disease)?
- …have had a heart attack, or myocardial infarction?
- …have peripheral vascular disease or poor circulation in your limbs?
- …have experienced a stroke or CVA (cerebrovascular accident)?
- …have experienced a mini-stroke or TIA (transient ischemic attack)?
- …have a memory problem?
- …have dementia or Alzheimer’s disease?
- …had parkinsonism or Parkinson’s disease?
- …have intestinal or stomach ulcers?
- …have a bowel disorder such as Crohn’s disease, ulcerative colitis, or irritable bowel syndrome?
- …experience bowel incontinence?
- …experience urinary incontinence?
- …have cataracts?
- …have glaucoma?
- …have macular degeneration?
- …had cancer?
- …have osteoporosis, sometimes called low bone mineral density, or thin, brittle, or weak bones?
- …have back problems, excluding fibromyalgia and arthritis?
- …have an UNDER-active thyroid gland (sometimes called hypothyroidism or myxedema)?
- …have an OVER-active thyroid gland (sometimes called hyperthyroidism or Graves’ disease?
- …have kidney disease or kidney failure?
- (Yes or no questions)
References
- Botly, L.C.P.; Lindsay, M.P.; Mulvagh, S.L.; Hill, M.D.; Goia, C.; Martin-Rhee, M.; Casaubon, L.K.; Yip, C.Y.Y. Recent Trends in Hospitalizations for Cardiovascular Disease, Stroke, and Vascular Cognitive Impairment in Canada. Can. J. Cardiol. 2020, 36, 1081–1090. [Google Scholar] [CrossRef] [PubMed]
- Yazdanyar, A.; Newman, A.B. The burden of cardiovascular disease in the elderly: Morbidity, mortality, and costs. Clin. Geriatr. Med. 2009, 25, 563–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitnitski, A.B.; Mogilner, A.J.; Rockwood, K. Accumulation of deficits as a proxy measure of aging. Sci. World J. 2001, 1, 323–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ijaz, N.; Buta, B.; Xue, Q.L.; Mohess, D.T.; Bushan, A.; Tran, H.; Batchelor, W.; de Filippi, C.R.; Walston, J.D.; Bandeen-Roche, K.; et al. Interventions for Frailty among Older Adults with Cardiovascular Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022, 79, 482–503. [Google Scholar] [CrossRef]
- Afilalo, J.; Karunananthan, S.; Eisenberg, M.J.; Alexander, K.P.; Bergman, H. Role of frailty in patients with cardiovascular disease. Am. J. Cardiol. 2009, 103, 1616–1621. [Google Scholar] [CrossRef]
- Forman, D.E.; Alexander, K.P. Frailty: A Vital Sign for Older Adults with Cardiovascular Disease. Can. J. Cardiol. 2016, 32, 1082–1087. [Google Scholar] [CrossRef]
- Afilalo, J.; Alexander, K.P.; Mack, M.J.; Maurer, M.S.; Green, P.; Allen, L.A.; Popma, J.J.; Ferrucci, L.; Forman, D.E. Frailty assessment in the cardiovascular care of older adults. J. Am. Coll. Cardiol. 2014, 63, 747–762. [Google Scholar] [CrossRef] [Green Version]
- Aida, K.; Kamiya, K.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Ichikawa, T.; Nakamura, T.; Yamashita, M.; Maekawa, E.; Yamaoka-Tojo, M.; et al. Usefulness of the Simplified Frailty Scale in Predicting Risk of Readmission or Mortality in Elderly Patients Hospitalized with Cardiovascular Disease. Int. Heart J. 2020, 61, 571–578. [Google Scholar] [CrossRef]
- Marinus, N.; Vigorito, C.; Giallauria, F.; Haenen, L.; Jansegers, T.; Dendale, P.; Feys, P.; Meesen, R.; Timmermans, A.; Spildooren, J.; et al. Frailty is highly prevalent in specific cardiovascular diseases and females, but significantly worsens prognosis in all affected patients: A systematic review. Ageing Res. Rev. 2021, 66, 101233. [Google Scholar] [CrossRef]
- Anderson, L.; Oldridge, N.; Thompson, D.R.; Zwisler, A.D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-Based Cardiac Rehabilitation for Coronary Heart Disease: Cochrane Systematic Review and Meta-Analysis. J. Am. Coll. Cardiol. 2016, 67, 1–12. [Google Scholar] [CrossRef]
- Kehler, D.S.; Giacomantonio, N.; Firth, W.; Blanchard, C.M.; Rockwood, K.; Theou, O. Association Between Cardiac Rehabilitation and Frailty. Can. J. Cardiol. 2020, 36, 482–489. [Google Scholar] [CrossRef]
- Mudge, A.M.; Pelecanos, A.; Adsett, J.A. Frailty implications for exercise participation and outcomes in patients with heart failure. J. Am. Geriatr. Soc. 2021, 69, 2476–2485. [Google Scholar] [CrossRef]
- Lutz, A.H.; Delligatti, A.; Allsup, K.; Afilalo, J.; Forman, D.E. Cardiac Rehabilitation Is Associated with Improved Physical Function in Frail Older Adults with Cardiovascular Disease. J. Cardiopulm. Rehabil. Prev. 2020, 40, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Ushijima, A.; Morita, N.; Hama, T.; Yamamoto, A.; Yoshimachi, F.; Ikari, Y.; Kobayashi, Y. Effects of cardiac rehabilitation on physical function and exercise capacity in elderly cardiovascular patients with frailty. J. Cardiol. 2020, 77, 424–431. [Google Scholar] [CrossRef]
- Toshie Tanaka, T.; Furukawa, S.; Nakaike, R.; Teshima, K.; Koga, H.; Yamada, A. Effect of outpatient cardiac rehabilitation program on outcome of elderly patients, especially in frailty status. Eur. J. Prev. Cardiol. 2018, 25, S138. [Google Scholar]
- Huang, K.; Liu, W.; He, D.; Huang, B.; Xiao, D.; Peng, Y.; He, Y.; Hu, H.; Chen, M.; Huang, D. Telehealth interventions versus center-based cardiac rehabilitation of coronary artery disease: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2015, 22, 959–971. [Google Scholar] [CrossRef]
- Batalik, L.; Filakova, K.; Batalikova, K.; Dosbaba, F. Remotely monitored telerehabilitation for cardiac patients: A review of the current situation. World J. Clin. Cases 2020, 8, 1818–1831. [Google Scholar] [CrossRef] [PubMed]
- Wongvibulsin, S.; Habeos, E.E.; Huynh, P.P.; Xun, H.; Shan, R.; Porosnicu Rodriguez, K.A.; Wang, J.; Gandapur, Y.K.; Osuji, N.; Shah, L.M.; et al. Digital Health Interventions for Cardiac Rehabilitation: Systematic Literature Review. J. Med. Internet Res. 2021, 23, e18773. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.; Yamabayashi, C.; Syed, N.; Kirkham, A.; Camp, P.G. Exercise Telemonitoring and Telerehabilitation Compared with Traditional Cardiac and Pulmonary Rehabilitation: A Systematic Review and Meta-Analysis. Physiother. Can. 2016, 68, 242–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spindler, H.; Leerskov, K.; Joensson, K.; Nielsen, G.; Andreasen, J.J.; Dinesen, B. Conventional Rehabilitation Therapy Versus Telerehabilitation in Cardiac Patients: A Comparison of Motivation, Psychological Distress, and Quality of Life. Int. J. Environ. Res. Public Health 2019, 16, 512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, R.J.; Beatty, A.L.; Beckie, T.M.; Brewer, L.C.; Brown, T.M.; Forman, D.E.; Franklin, B.A.; Keteyian, S.J.; Kitzman, D.W.; Regensteiner, J.G.; et al. Home-Based Cardiac Rehabilitation: A Scientific Statement from the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology. Circulation 2019, 140, e69–e89. [Google Scholar] [CrossRef] [PubMed]
- Moulson, N.; Bewick, D.; Selway, T.; Harris, J.; Suskin, N.; Oh, P.; Coutinho, T.; Singh, G.; Chow, C.M.; Clarke, B.; et al. Cardiac Rehabilitation during the COVID-19 Era: Guidance on Implementing Virtual Care. Can. J. Cardiol. 2020, 36, 1317–1321. [Google Scholar] [CrossRef]
- Searle, S.D.; Mitnitski, A.; Gahbauer, E.A.; Gill, T.M.; Rockwood, K. A standard procedure for creating a frailty index. BMC Geriatr. 2008, 8, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Zepeda, M.U.; Godin, J.; Armstrong, J.J.; Andrew, M.K.; Mitnitski, A.; Kirkland, S.; Rockwood, K.; Theou, O. Frailty among middle-aged and older Canadians: Population norms for the frailty index using the Canadian Longitudinal Study on Aging. Age Ageing 2020, 50, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Theou, O.; van der Valk, A.M.; Godin, J.; Andrew, M.K.; McElhaney, J.E.; McNeil, S.A.; Rockwood, K. Exploring Clinically Meaningful Changes for the Frailty Index in a Longitudinal Cohort of Hospitalized Older Patients. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1928–1934. [Google Scholar] [CrossRef]
- Jang, I.Y.; Jung, H.W.; Lee, H.Y.; Park, H.; Lee, E.; Kim, D.H. Evaluation of Clinically Meaningful Changes in Measures of Frailty. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1143–1147. [Google Scholar] [CrossRef]
- Vigorito, C.; Abreu, A.; Ambrosetti, M.; Belardinelli, R.; Corrà, U.; Cupples, M.; Davos, C.H.; Hoefer, S.; Iliou, M.C.; Schmid, J.P.; et al. Frailty and cardiac rehabilitation: A call to action from the EAPC Cardiac Rehabilitation Section. Eur. J. Prev. Cardiol. 2017, 24, 577–590. [Google Scholar] [CrossRef] [Green Version]
- Aamot, I.-L.; Forbord, S.H.; Gustad, K.; Løckra, V.; Stensen, A.; Berg, A.T.; Dalen, H.; Karlsen, T.; Støylen, A. Home-based versus hospital-based high-intensity interval training in cardiac rehabilitation: A randomized study. Eur. J. Prev. Cardiol. 2020, 21, 1070–1078. [Google Scholar] [CrossRef]
- Rawstorn, J.C.; Gant, N.; Direito, A.; Beckmann, C.; Maddison, R. Telehealth exercise-based cardiac rehabilitation: A systematic review and meta-analysis. Heart 2016, 102, 1183–1192. [Google Scholar] [CrossRef]
- Kimber, D.E.; Kehler, D.S.; Lytwyn, J.; Boreskie, K.F.; Jung, P.; Alexander, B.; Hiebert, B.M.; Dubiel, C.; Hamm, N.C.; Stammers, A.N.; et al. Pre-Operative Frailty Status Is Associated with Cardiac Rehabilitation Completion: A Retrospective Cohort Study. J. Clin. Med. 2018, 7, 560. [Google Scholar] [CrossRef] [Green Version]
- Frederix, I.; Van Driessche, N.; Hansen, D.; Berger, J.; Bonne, K.; Alders, T.; Dendale, P. Increasing the medium-term clinical benefits of hospital-based cardiac rehabilitation by physical activity telemonitoring in coronary artery disease patients. Eur. J. Prev. Cardiol. 2015, 22, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Varnfield, M.; Karunanithi, M.; Lee, C.K.; Honeyman, E.; Arnold, D.; Ding, H.; Smith, C.; Walters, D.L. Smartphone-based home care model improved use of cardiac rehabilitation in postmyocardial infarction patients: Results from a randomised controlled trial. Heart 2014, 100, 1770–1779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lear, S.A.; Singer, J.; Banner-Lukaris, D.; Horvat, D.; Park, J.E.; Bates, J.; Ignaszewski, A. Improving access to cardiac rehabilitation using the internet: A randomized trial. Stud. Health Technol. Inform. 2015, 209, 58–66. [Google Scholar] [PubMed]
- Twisk, J.W.; Rijnhart, J.J.; Hoekstra, T.; Schuster, N.A.; Ter Wee, M.M.; Heymans, M.W. Intention-to-treat analysis when only a baseline value is available. Contemp. Clin. Trials Commun. 2020, 20, 100684. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Cardiac Rehabilitation Model | p Value | |
|---|---|---|---|
| Center-Based | Virtual | ||
Sex
| 47 (63.5%) 27 (46.5%) | 37 (63.7%) 21 (46.3%) | 0.974 |
| Mean age | 63.1 ± 10.6 | 66.4 ± 10.1 | 0.069 |
Unadjusted admission CLSA-FI a
| 0.11 ± 0.07 35 (47.2%) 32 (43.2%) 5 (6.7%) 2 (2.7%) 0.14 ± 0.003 | 0.11 ± 0.06 29 (50%) 24 (41.3%) 4 (6.8%) 1 (1.7%) 0.07 ± 0.003 | 0.946 0.001 * |
| Exercise session attendance | 88.9% ± 17.9 | 88.9% ± 22.2 | 0.975 |
Cardiovascular biomarkers a
| 1.76 ± 1.01 3.74 ± 1.07 1.10 ± 0.28 1.85 ± 0.84 110.15 ± 64.48 86.65 ± 35.41 6.70 ± 16.57 122.72 ± 19.84 72.19 ± 10.11 66.89 ± 10.82 | 1.54 ± 0.76 3.43 ± 0.76 1.13 ± 0.24 1.59 ± 0.65 115.10 ± 75.66 77.28 ± 15.32 4.03 ± 5.25 125.53 ± 15.02 71.64 ± 9.05 65.45 ± 10.73 | 0.168 0.062 0.579 0.053 0.685 0.062 0.240 0.371 0.746 0.447 |
Smoking status
| 11 (14.8%) 34 (43.6%) 29 (39.1%) 2 (2.7%) | 8 (13.8%) 24 (41.3%) 22 (37.9% 2 (3.4%) | 0.884 0.603 0.863 |
History of CVDs a
| 19 (24.3%) 9 (12.2%) 32 (43.2%) 4 (5.1%) 3 (3.8%) 28 (37.8%) 3 (3.8%) | 6 (10.3%) 5 (8.6%) 30 (51.7%) 17 (29.3%) 2 (3.4%) 23 (39.7%) 1 (1.7%) | 0.026 * 0.515 0.336 0.004 * 0.858 0.833 0.442 |
CVD risk factors
| 58 (78.4%) 62 (83.8%) 37 (50.0%) 22 (29.7%) 13 (17.5%) 13 (17.5%) 41 (55.4%) | 44 (75.8%) 56 (96.5%) 23 (39.7%) 16 (27.5%) 14 (24.1%) 6 (10.3%) 39 (67.2%) | 0.734 0.018 * 0.239 0.789 0.357 0.244 0.170 |
| Cardiovascular Biomarker | R Square | Beta 95% CI | F-Statistic | p Value | |
|---|---|---|---|---|---|
| Beta | Lower | Upper | |||
| Simple slope analysis | |||||
| (Reference is center-based CR) | |||||
Triglycerides
| 0.130 0.210 −0.033 −0.277 −0.522 −0.766 | −0.001 −0.280 −0.392 −0.655 −1.053 −1.508 | 0.099 0.701 0.324 0.099 0.009 −0.025 | 1.156 (116, 15) | 0.054 0.392 0.851 0.143 0.051 0.040 * |
Total cholesterol
| 0.251 0.408 0.051 −0.304 −0.660 −1.017 | −0.125 −0.117 0.330 −0.706 −1.229 −1.811 | −0.017 0.933 0.433 0.097 −0.092 −0.222 | 2.602 (116, 15) | 0.009 * 0.123 0.786 0.132 0.021 * 0.011 * |
HDL-cholesterol a
| 0.390 −0.131 −0.108 −0.084 −0.061 −0.037 | −0.015 −0.328 −0.252 −0.236 −0.275 −0.335 | 0.024 0.065 0.036 0.067 0.152 0.260 | 4.951 (116, 15) | 0.643 0.185 0.136 0.267 0.569 0.901 |
LDL-cholesterol a
| 0.178 −0.409 −0.354 −0.300 −0.246 −0.192 | −0.054 −1.027 −0.806 −0.776 −0.918 −1.130 | 0.076 0.209 0.096 0.175 0.425 0.745 | 1.683 (116, 15) | 0.734 0.188 0.118 0.209 0.464 0.682 |
Creatine kinase
| 0.135 27.446 −14.774 −56.994 −99.215 −141.436 | −18.739 −72.421 −87.629 −134.080 −208.194 −293.457 | 1.851 127.313 58.080 20.090 9.763 10.585 | 1.212 (116, 15) | 0.104 0.583 0.685 0.141 0.071 0.065 |
Creatinine
| 0.054 15.163 12.385 9.608 6.830 4.052 | −10.558 −83.244 −60.246 −67.003 −100.248 −144.490 | 9.447 113.571 85.017 86.219 113.909 152.596 | 0.447 (116, 15) | 0.912 0.758 0.733 0.802 0.898 0.956 |
C-Reactive protein
| 0.254 −3.534 −3.215 −2.895 −2.577 −2.258 | −1.374 −17.556 −13.471 −13.718 −17.822 −23.496 | 1.501 10.488 7.041 7.925 12.667 18.979 | 2.638 (116, 15) | 0.929 0.615 0.531 0.593 0.735 0.821 |
Systolic BP
| 0.185 −6.403 −5.105 −3.807 −2.509 −1.211 | −0.749 −16.091 −12.238 −11.476 −13.355 −16.290 | 1.268 3.284 2.027 3.860 8.336 13.867 | 1.760 (115, 16) | 0.607 0.188 0.154 0.322 0.644 0.872 |
Diastolic BP
| 0.219 2.468 1.125 0.040 −1.173 −2.388 | −0.835 −3.337 −2.975 −4.389 −7.410 −11.089 | 0.349 8.275 5.484 4.469 5.062 6.313 | 2.174 (115, 16) | 0.413 0.396 0.554 0.985 0.707 0.584 |
Resting pulse
| 0.152 0.125 −3.232 −6.589 −9.947 −13.305 | −1.731 −10.291 −10.831 −14.534 −21.109 −28.867 | 0.387 10.543 4.367 1.354 1.213 2.256 | 1.386 (115, 16) | 0.207 0.980 0.396 0.099 0.077 0.089 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MacEachern, E.; Giacomantonio, N.; Theou, O.; Quach, J.; Firth, W.; Abel-Adegbite, I.; Kehler, D.S. Comparing Virtual and Center-Based Cardiac Rehabilitation on Changes in Frailty. Int. J. Environ. Res. Public Health 2023, 20, 1554. https://doi.org/10.3390/ijerph20021554
MacEachern E, Giacomantonio N, Theou O, Quach J, Firth W, Abel-Adegbite I, Kehler DS. Comparing Virtual and Center-Based Cardiac Rehabilitation on Changes in Frailty. International Journal of Environmental Research and Public Health. 2023; 20(2):1554. https://doi.org/10.3390/ijerph20021554
Chicago/Turabian StyleMacEachern, Evan, Nicholas Giacomantonio, Olga Theou, Jack Quach, Wanda Firth, Ifedayo Abel-Adegbite, and Dustin Scott Kehler. 2023. "Comparing Virtual and Center-Based Cardiac Rehabilitation on Changes in Frailty" International Journal of Environmental Research and Public Health 20, no. 2: 1554. https://doi.org/10.3390/ijerph20021554
APA StyleMacEachern, E., Giacomantonio, N., Theou, O., Quach, J., Firth, W., Abel-Adegbite, I., & Kehler, D. S. (2023). Comparing Virtual and Center-Based Cardiac Rehabilitation on Changes in Frailty. International Journal of Environmental Research and Public Health, 20(2), 1554. https://doi.org/10.3390/ijerph20021554