
Mother-Child Bond through Feeding: A Prospective Study including Neuroticism, Pregnancy Worries and Post-Traumatic Symptomatology

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedures
2.2. Ethics
2.3. Measures
2.3.1. Sociodemographic and Clinical Data
2.3.2. First Trimester of Pregnancy
Neuroticism
2.3.3. Third Trimester of Pregnancy
Pregnancy Worries
2.3.4. Four Months Postpartum
P-PTSD Symptoms
Mother-Baby Bonding during Feeding
2.3.5. Covariates
2.4. Statistical Analysis
3. Results
3.1. Correlations among Variables (Considering All Four Worry Factors)
3.2. Correlations among Variables (Considering Specific Worries Contained in the Statistically Significant Worry Factors)
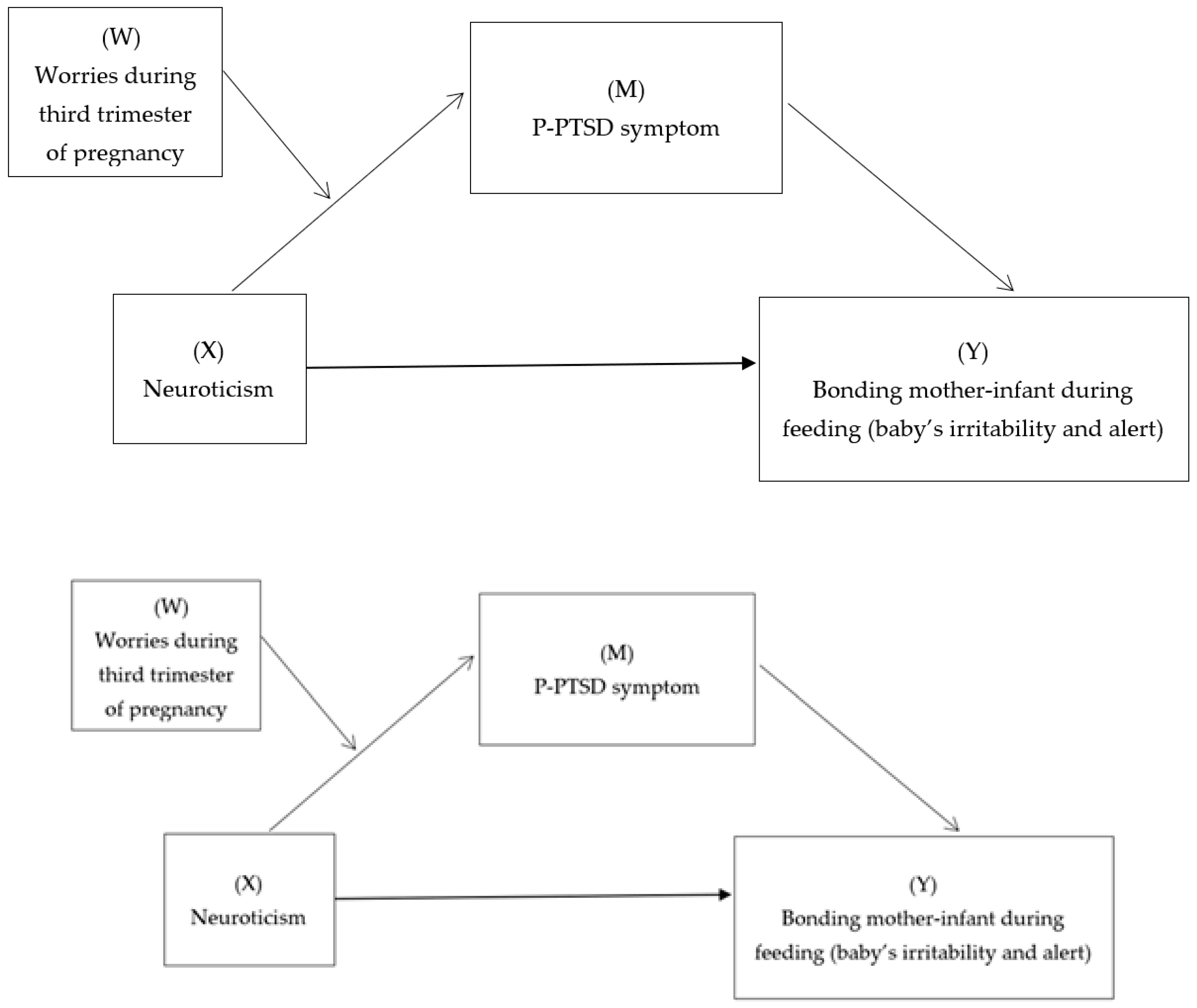
3.3. Testing the Mediation Effect of P-PTSD Symptoms between Neuroticism and Infant Irritability
3.4. Testing the Moderated-Mediation Model Neuroticism- P-PTSD Symptom-Infant Irritability (Worries as Moderator)
4. Discussion
4.1. Limitations
4.2. Implications for Clinical Practice, Policy and Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bicking Kinsey, C.; Hupcey, J.E. State of the science of maternal–infant bonding: A principle-based concept analysis. Midwifery 2013, 29, 1314–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muzik, M.; Bocknek, E.L.; Broderick, A.; Richardson, P.; Rosenblum, K.L.; Thelen, K.; Seng, J.S. Mother–infant bonding impairment across the first 6 months postpartum: The primacy of psychopathology in women with childhood abuse and neglect histories. Arch. Women’s Ment. Health 2013, 16, 29–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, L.; Hipwell, A.; Hooper, R. The cognitive development of 5-year-old children of postnatally depressed mothers. J. Child Psychol. Psychiatry 1996, 37, 927–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teicher, M.H.; Samson, J.A.; Anderson, C.M.; Ohashi, K. The effects of childhood maltreatment on brain structure, function and connectivity. Nat. Rev. Neurosci. 2016, 17, 652–666. [Google Scholar] [CrossRef] [PubMed]
- Else-Quest, N.M.; Hyde, J.S.; Clark, R. Breastfeeding, Bonding, and the Mother-Infant Relationship. Merrill-Palmer Q. 2003, 49, 495–517. [Google Scholar] [CrossRef]
- Mezzacappa, E.S.; Katkin, E.S. Breast-feeding is associated with reduced perceived stress and negative mood in mothers. Health Psychol. 2002, 21, 187–193. [Google Scholar] [CrossRef]
- Brockington, I.F.; Oates, J.; George, S. A screening questionnaire for mother-infant bonding disorders. Arch. Women’s Ment. Health 2001, 3, 133–140. [Google Scholar] [CrossRef]
- Mascheroni, E.; Ionio, C. The efficacy of interventions aimed at improving post-partum bonding: A review of interventions addressing parent-infant bonding in healthy and at risk populations. J. Neonatal Nurs. 2019, 25, 61–68. [Google Scholar] [CrossRef]
- Martone, D.J.; Nash, B.R. Initial differences in postpartum attachment behavior in breastfeeding and bottle-feeding mothers. J. Obstet. Gynecol. Neonatal Nurs. 1988, 17, 212–213. [Google Scholar] [CrossRef]
- Hairston, I.S.; Handelzalts, J.E.; Lehman-Inbar, T.; Kovo, M. Mother-infant bonding is not associated with feeding type: A community study sample. BMC Pregnancy Childbirth 2019, 19, 125. [Google Scholar] [CrossRef]
- Kendall-Tackett, K. Birth trauma: The causes and consequences of childbirth-related trauma and PTSD. In Women’s Reproductive Mental Health Across the Lifespan; Barnes, D.L., Ed.; Springer Publishing: Basel, Switzerland, 2015. [Google Scholar]
- Dekel, S.; Stuebe, C.; Dishy, G. Childbirth induced posttraumatic stress syndrome: A systematic review of prevalence and risk factors. Front. Psychol. 2017, 8, 560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yildiz, P.D.; Ayers, S.; Phillips, L. The prevalence of posttraumatic stress disorder in pregnancy and after birth: A systematic review and meta-analysis. J. Affect. Disord. 2017, 208, 634–645. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Grekin, R.; O’Hara, M.W. Prevalence and risk factors of postpartum posttraumatic stress disorder: A meta-analysis. Clin. Psychol. Rev. 2014, 34, 389–401. [Google Scholar] [CrossRef] [PubMed]
- Horsch, A.; Brooks, C.; Fletcher, H. Maternal coping, appraisals and adjustment following diagnosis of fetal anomaly. Prenat. Diagn. 2013, 33, 1137–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Heumen, M.A.; Hollander, M.H.; van Pampus, M.G.; van Dillen, J.; Stramrood, C.A. Psychosocial predictors of postpartum posttraumatic stress disorder in women with a traumatic childbirth experience. Front. Psychiatry 2018, 9, 348. [Google Scholar] [CrossRef] [Green Version]
- Oddo-Sommerfeld, S.; Hain, S.; Louwen, F.; Schermelleh-Engel, K. Longitudinal effects of dysfunctional perfectionism and avoidant personality style on postpartum mental disorders: Pathways through antepartum depression and anxiety. J. Affect. Disord. 2016, 191, 280–288. [Google Scholar] [CrossRef]
- Davies, S.M.; Silverio, S.A.; Christiansen, P.; Fallon, V. Maternal-infant bonding and perceptions of infant temperament: The mediating role of maternal mental health. J. Affect. Disord. 2021, 282, 1323–1329. [Google Scholar] [CrossRef]
- Deans, C.L. Maternal sensitivity, its relationship with child outcomes, and interventions that address it: A systematic literature review. Early Child Dev. Care 2020, 190, 252–275. [Google Scholar] [CrossRef]
- Vedova, A.M.D. Maternal psychological state and infant’s temperament at three months. J. Reprod. Infant Psychol. 2014, 32, 520–534. [Google Scholar] [CrossRef]
- Widiger, T.A.; Oltmanns, J.R. Neuroticism is a fundamental domain of personality with enormous public health implications. World Psychiatry 2017, 16, 144–145. [Google Scholar] [CrossRef]
- Dudek, D.; Jaeschke, R.; Siwek, M.; Mączka, G.; Topǒr-Mądry, R.; Rybakowski, J. Postpartum depression: Identifying associations with bipolarity and personality traits. Preliminary results from a cross-sectional study in Poland. Psychiatry Res. 2014, 215, 69–74. [Google Scholar] [CrossRef]
- Iliadis, S.I.; Koulouris, P.; Gingnell, M.; Sylvén, S.M.; Sundström-Poromaa, I.; Ekselius, L.; Papadopoulos, F.C.; Skalkidou, A. Personality and risk for postpartum depressive symptoms. Arch. Women’s Ment. Health 2015, 18, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Marín-Morales, D.; Carmona-Monge, F.J.; Peñacoba-Puente, C. Relationship between personality and postpartum depression in Spanish pregnant. Annu. Psychol. 2014, 30, 908–915. [Google Scholar]
- Handelzalts, J.E.; Hairston, I.S.; Muzik, M.; Matatyahu Tahar, A.; Levy, S. A paradoxical role of childbirth-related posttraumatic stress disorder (PTSD) symptoms in the association between personality factors and mother-infant bonding: A cross-sectional study. Psychol. Trauma 2022, 14, 1066–1072. [Google Scholar] [CrossRef] [PubMed]
- Puente, C.P.; Carmona Monge, F.J.; Abellán, I.C.; Morales, D.M. Effects of personality on psychiatric and somatic symptoms in pregnant women: The role of pregnancy worries. Psychol. Women Q. 2011, 35, 293–302. [Google Scholar] [CrossRef]
- Tamir, M. Don’t worry, be happy? Neuroticism, trait consistent affect regulation, and performance. J. Personal. Soc. Psychol. 2005, 89, 449–461. [Google Scholar] [CrossRef] [Green Version]
- Osborne, L.M.; Voegtline, K.; Standeven, L.R.; Sundel, B.; Pangtey, M.; Hantsoo, L.; Payne, J.L. High worry in pregnancy predicts postpartum depression. J. Affect. Disord. 2021, 294, 701–706. [Google Scholar] [CrossRef]
- Seisdedos, N. Inventario NEO Reducido de Cinco Factores (NEO-FFI). Manual Profesional [NEO-FFI Inventory. Proffesional Manual]; TEA Ediciones: Madrid, Spain, 1999. [Google Scholar]
- Ludtke, O.; Trautwein, U.; Nagy, G.; Koller, O. A validation of the NEO-FFI in a sample of young adults: Effects of the response format, factorial validity, and relations with indicators of academic achievement. Diagnostica 2004, 50, 134–144. [Google Scholar]
- Carmona Monge, F.J.; Peñacoba-Puente, C.; Marín Morales, D.; Carretero Abellán, I. Factor structure, validity and reliability of the Spanish version of the Cambridge Worry Scale. Midwifery 2012, 28, 112–119. [Google Scholar] [CrossRef]
- Hernández-Martínez, A.; Martínez-Vázquez, S.; Rodríguez-Almagro, J.; Khan, K.S.; Delgado-Rodríguez, M.; Martínez-Galiano, J.M. Validation of perinatal post-traumatic stress disorder questionnaire for Spanish women during the postpartum period. Sci. Rep. 2021, 11, 5567. [Google Scholar] [CrossRef]
- Wolke, D.; James-Roberts, I.S. Multi-Method Measurement of the Early Parent-Infant System with Easy and Difficult Newborns. Adv. Psychol. 1987, 46, 49–70. [Google Scholar]
- Bayri Bingol, F.; Demirgoz Bal, M. The risk factors for postpartum posttraumatic stress disorder and depression. Perspect. Psychiatr. Care 2020, 56, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Dekel, S.; Ein-Dor, T.; Dishy, G.A.; Mayopoulos, P.A. Beyond postpartum depression: Posttraumatic stress-depressive response following childbirth. Arch. Women’s Ment. Health 2020, 23, 557–564. [Google Scholar] [CrossRef] [PubMed]
- González de Rivera, J.L.; Derogatis, L.R.; De las Cuevas, C.; Gracia Marco, R.; Rodríguez-Pulido, F.; Henry-Benítez, M.; Monterrey, A.L. The Spanish Version of the SCL-90-R. Normative Data in the GENERAL Population; Clinical Psychometric Research: Towson, MD, USA, 1989. [Google Scholar]
- Robles, J.I.; Andreu, J.M.; Peña, M.E. SCL-90: Aplicación y análisis de sus propiedades psicométricas en una muestra de sujetos clínicos españoles [SCL-90: An analysis of its psychometric properties in a clinical sample of Spanish subjects]. Psicopatología Clínica Leg. Forense 2002, 2, 1–19. [Google Scholar]
- Hayes, A.F. Mediation, Moderation and Conditional Process Analysis. A Regression-Based Approach, 3rd ed.; Guildford Press: New York, NY, USA, 2017. [Google Scholar]
- Cassidy, J.; Jones, J.D.; Shaver, P.R. Contributions of attachment theory and research: A framework for future research, translation, and policy. Dev. Psychopathol. 2013, 25, 1415–1434. [Google Scholar] [CrossRef]
- Siddiqui, A.; Hagglof, B. Does maternal prenatal attachment predict postnatal mother–infant interaction? Early Hum. Dev. 2000, 59, 13–25. [Google Scholar] [CrossRef]
- Brandäo, T.; Brites, R.; Nunes, O.; Pires, M.; Hipólito, J. Anxiety and depressive symptoms during pregnancy, perceived control and posttraumatic stress symptoms after childbirth: A longitudinal mediation analysis. J. Health Psychol. 2020, 25, 2085–2095. [Google Scholar] [CrossRef]
- Catala, P.; Suso-Ribera, C.; Marin, D.; Peñacoba, C. Predicting postpartum post-traumatic stress and depressive symptoms in low-risk women from distal and proximal factors: A biopsychosocial prospective study using structural equation modeling. Arch. Gynecol. Obstet. 2021, 303, 1415–1423. [Google Scholar] [CrossRef]
- Breslau, N.; Schultz, L. Neuroticism and post-traumatic stress disorder: A prospective investigation. Psychol. Med. 2013, 43, 1697–1702. [Google Scholar] [CrossRef]
- Hirschfeld, R.M.; Klerman, G.L.; Clayton, P.J.; Keller, M.B.; McDonald-Scott, P.; Larkin, B.H. Assessing personality: Effects of the depressive state on trait measurement. Am. J. Psychiatry 1983, 140, 695–699. [Google Scholar]
- Cook, N.; Ayers, S.; Horsch, A. Maternal posttraumatic stress disorder during the perinatal period and child outcomes: A systematic review. J. Affect. Disord. 2018, 225, 18–31. [Google Scholar] [CrossRef] [PubMed]
- Tietz, A.; Zietlow, A.L.; Reck, C. Maternal bonding in mothers with postpartum anxiety disorder: The crucial role of subclinical depressive symptoms and maternal avoidance behaviour. Arch. Women’s Ment. Health 2014, 17, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Peñacoba-Puente, C.; Monge, F.J.; Morales, D.M. Pregnancy worries: A longitudinal study of Spanish women. Acta Obstet. Et Gynecol. Scand. 2011, 90, 1030–1035. [Google Scholar] [CrossRef] [PubMed]
- Biaggi, A.; Conroy, S.; Pawlby, S.; Pariante, C.M. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect. Disord. 2016, 191, 62–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, S.M.; Haber, E.; Frey, B.N.; McCabe, R.E. Cognitive–behavioral group treatment for perinatal anxiety: A pilot study. Arch. Women’s Ment. Health 2015, 18, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Bolier, L.; Haverman, M.; Westerhof, G.J.; Riper, H.; Smit, F.; Bohlmeijer, E. Positive psychology interventions: A meta-analysis of randomized controlled studies. BMC Public Health 2013, 13, 119–138. [Google Scholar] [CrossRef] [Green Version]
- Gelaye, B.; Addae, G.; Neway, B.; Larrabure-Torrealva, G.T.; Qiu, C.; Stoner, L.; Luque Fernandez, M.A.; Sanchez, S.E.; Williams, M.A. Poor sleep quality, antepartum depression and suicidal ideation among pregnant women. J. Affect. Disord. 2017, 209, 195–200. [Google Scholar] [CrossRef] [Green Version]
- Morris, A.R.; Aviv, E.C.; Khaled, M.; Corner, G.W.; Saxbe, D.E. Prenatal romantic relationship satisfaction predicts parent-infant bonding for fathers, but not mothers. Couple Fam. Psychol. 2022, 11, 244–253. [Google Scholar] [CrossRef]
- Prinzie, P.; Stams, G.J.; Deković, M.; Reijntjes, A.H.; Belsky, J. The relations between parents’ Big Five personality factors and parenting: A meta-analytic review. J. Personal. Soc. Psychol. 2009, 97, 351–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staehelin, K.; Bertea, P.C.; Stutz, E.Z. Length of maternity leave and health of mother and child—A review. Int. J. Public Health 2007, 52, 202–209. [Google Scholar] [CrossRef]
- Tohme, P.; Habib, R.A. Correlates of work productivity and maternal competence after having a baby: The roles of mother-infant bonding and maternal subjective experiences. BMC Women’s Health 2022, 22, 392. [Google Scholar] [CrossRef] [PubMed]
- Alderdice, F.; McNeil, J.; Lynn, F. A systematic review of systematic reviews of interventions to improve maternal mental health and well-being. Midwifery 2013, 29, 389–399. [Google Scholar] [CrossRef]
- Glover, V. Maternal depression, anxiety and stress during pregnancy and child outcome; what needs to be done. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Feldman, R.; Weller, A.; Zagoory-Sharon, O.; Levine, A. Evidence for a neuroendocrinological foundation of human affiliation: Plasma oxytocin levels across pregnancy and the postpartum period predict mother-infant bonding. Psychol. Sci. 2007, 18, 965–970. [Google Scholar] [CrossRef] [PubMed]
- Ugartemendia, L.; De Guzman, R.M.; Cai, J.; Rajamanickam, S.; Jiang, Z.; Tao, J.; Zuloaga, D.G.; Justice, N.J. A subpopulation of oxytocin neurons initiate expression of CRF receptor 1 (CRFR1) in females post parturition. Psychoneuroendocrinology 2022, 145, 105918. [Google Scholar] [CrossRef]


{kind=link}
| Time | Participants | Participants Excluded | Percentage of Excluded | Reasons |
|---|---|---|---|---|
| Assessed for eligibility | 290 | 5 | 1.72% |
|
| First trimester | 285 | 162 | 56.84% |
|
| Third trimester | 123 | 3 | 2.43% |
|
| Postpartum | 120 | 0 | 0% | |
| Analysis | 120 | 0 | 0% |
| M (SD) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|---|
| 1.Neuroticism | 18.05 (7.26) | -- | |||||||
| 2.Worries about giving birth | 2.22 (1.26) | 0.129 | -- | ||||||
| 3.Worries related to hospital visits | 0.74 (0.06) | 0.143 | 0.023 | -- | |||||
| 4.Worries related to medical examinations | 1.05 (1.00) | 0.274 ** | 0.229 * | 0.553 ** | -- | ||||
| 5.Worries related to coping in caring for the baby | 1.85 (0.51) | 0.316 * | 0.469 ** | 0.239 ** | 0.369 ** | -- | |||
| 6. P-PTSD symptoms | 7.90 (0.50) | 0.428 ** | 0.116 | 0.010 | 0.139 | 0.272 * | -- | ||
| 7.Irritability during feeding | 7.02 (2.38) | 0.217 * | 0.179 | −0.034 | −0.095 | 0.388 ** | 0.362 ** | -- | |
| 8.Alertness during feeding | 27.84 (11.02) | −0.128 | −0.035 | −0.009 | −0.072 | −0.161 | −0.311 ** | 0.540 ** | -- |
| Variables | B | SE | t | p | LLCI | ULCI |
|---|---|---|---|---|---|---|
| Direct and total effect a path, Neuroticism → P-PTSD symptoms | 0.431 | 0.085 | 5.075 | <0.001 | 0.262 | 0.600 |
| b path, P-PTSD symptoms → Infant irritability during feeding | 0.273 | 0.072 | 3.364 | 0.011 | 0.975 | 0.377 |
| c’ path, Neuroticism → Infant irritability during feeding (Direct effect) | 0.053 | 0.070 | 1.76 | 0.044 | 0.087 | 0.192 |
| c path, Neuroticism → Infant irritability during feeding (Total effect) | 0.165 | 0.06 | 2.35 | 0.020 | 0.021 | 0.280 |
| Indirect effect of Neuroticism (X) on Infant irritability during feeding (Y) through P-PTSD symptoms | 0.102 | 0.035 | 0.038 | 0.176 |
| Predictor | Infant Irritability during Feeding | |||||
|---|---|---|---|---|---|---|
| B | SE | t | p | LLCI | ULCI | |
| Neuroticism | 0.059 | 0.153 | 0.873 | 0.045 | 0.256 | 0.355 |
| Neuroticism x Worries related to coping in caring for the baby | 0.136 | 0.045 | 2.029 | 0.046 | 0.077 | 0.158 |
| Postpartum PTSD symptoms | 0.207 | 0.199 | 1.044 | 0.003 | 0.197 | 0.377 |
| [Model R = 0.391 | ||||||
| R2 = 0.201 F = 8.858 p = 0.006] | ||||||
| Effect of covariates | ||||||
| Type of delivery | 0.665 | 1.034 | 1.221 | 0.240 | −3.451 | 0.921 |
| Choice-feeding | −0.612 | 1.047 | 0.813 | 0.430 | −11.820 | 5.242 |
| Type of anesthesia | −0.751 | 1.723 | 0.570 | 0.580 | −2.663 | 4.625 |
| First minute Apgar test | 0.659 | 0.340 | 0.289 | 0.776 | −2.438 | 3.213 |
| Fifth minute Apgar test | 0.296 | 0.951 | 0.100 | 0.922 | −5.923 | 6.520 |
| Depressive symptoms first trimester | 1.820 | 0.420 | 2.49 | 0.016 | 2.314 | 0.251 |
| Anxious symptoms first trimester | 1.262 | 1.515 | 0.058 | 0.563 | −5.577 | 3.058 |
| Age | −0.124 | 0.184 | −0.675 | 0.502 | −0.491 | 0.242 |
| Conditional indirect effect of Neuroticism (X) on Infant irritability during feeding (Y) by different levels of worries related to coping in caring for the baby (W) through the effect of Postpartum PTSD symptoms (M) | ||||||
| Low level of worries | 0.257 | 0.110 | 2.332 | 0.061 | 0.038 | 0.476 |
| Medium level of worries | 0.301 | 0.120 | 3.874 | 0.065 | 0.333 | 0.801 |
| High level of worries | 0.413 | 0.084 | 4.783 | 0.006 | 0.245 | 0.581 |
| Indirect effect of Neuroticism (X) on Infant irritability during feeding (Y) through Postpartum PTSD (M) | 0.061 | 0.033 | 0.004 | 0.130 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutiérrez Hermoso, L.; Catalá Mesón, P.; Écija Gallardo, C.; Marín Morales, D.; Peñacoba Puente, C. Mother-Child Bond through Feeding: A Prospective Study including Neuroticism, Pregnancy Worries and Post-Traumatic Symptomatology. Int. J. Environ. Res. Public Health 2023, 20, 2115. https://doi.org/10.3390/ijerph20032115
Gutiérrez Hermoso L, Catalá Mesón P, Écija Gallardo C, Marín Morales D, Peñacoba Puente C. Mother-Child Bond through Feeding: A Prospective Study including Neuroticism, Pregnancy Worries and Post-Traumatic Symptomatology. International Journal of Environmental Research and Public Health. 2023; 20(3):2115. https://doi.org/10.3390/ijerph20032115
Chicago/Turabian StyleGutiérrez Hermoso, Lorena, Patricia Catalá Mesón, Carmen Écija Gallardo, Dolores Marín Morales, and Cecilia Peñacoba Puente. 2023. "Mother-Child Bond through Feeding: A Prospective Study including Neuroticism, Pregnancy Worries and Post-Traumatic Symptomatology" International Journal of Environmental Research and Public Health 20, no. 3: 2115. https://doi.org/10.3390/ijerph20032115
APA StyleGutiérrez Hermoso, L., Catalá Mesón, P., Écija Gallardo, C., Marín Morales, D., & Peñacoba Puente, C. (2023). Mother-Child Bond through Feeding: A Prospective Study including Neuroticism, Pregnancy Worries and Post-Traumatic Symptomatology. International Journal of Environmental Research and Public Health, 20(3), 2115. https://doi.org/10.3390/ijerph20032115