
Change over Time in the Risk of Death among Japanese COVID-19 Cases Caused by the Omicron Variant Depending on Prevalence of Sublineages

 , , add
Show full author list
, , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Calculation of Case Fatality Rate

2.3. Causes of Death
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosed Period | Number of Cases | Number of Death | Age-Standardized Fatality Rate | 95%CI (Lower-Upper) |
|---|---|---|---|---|
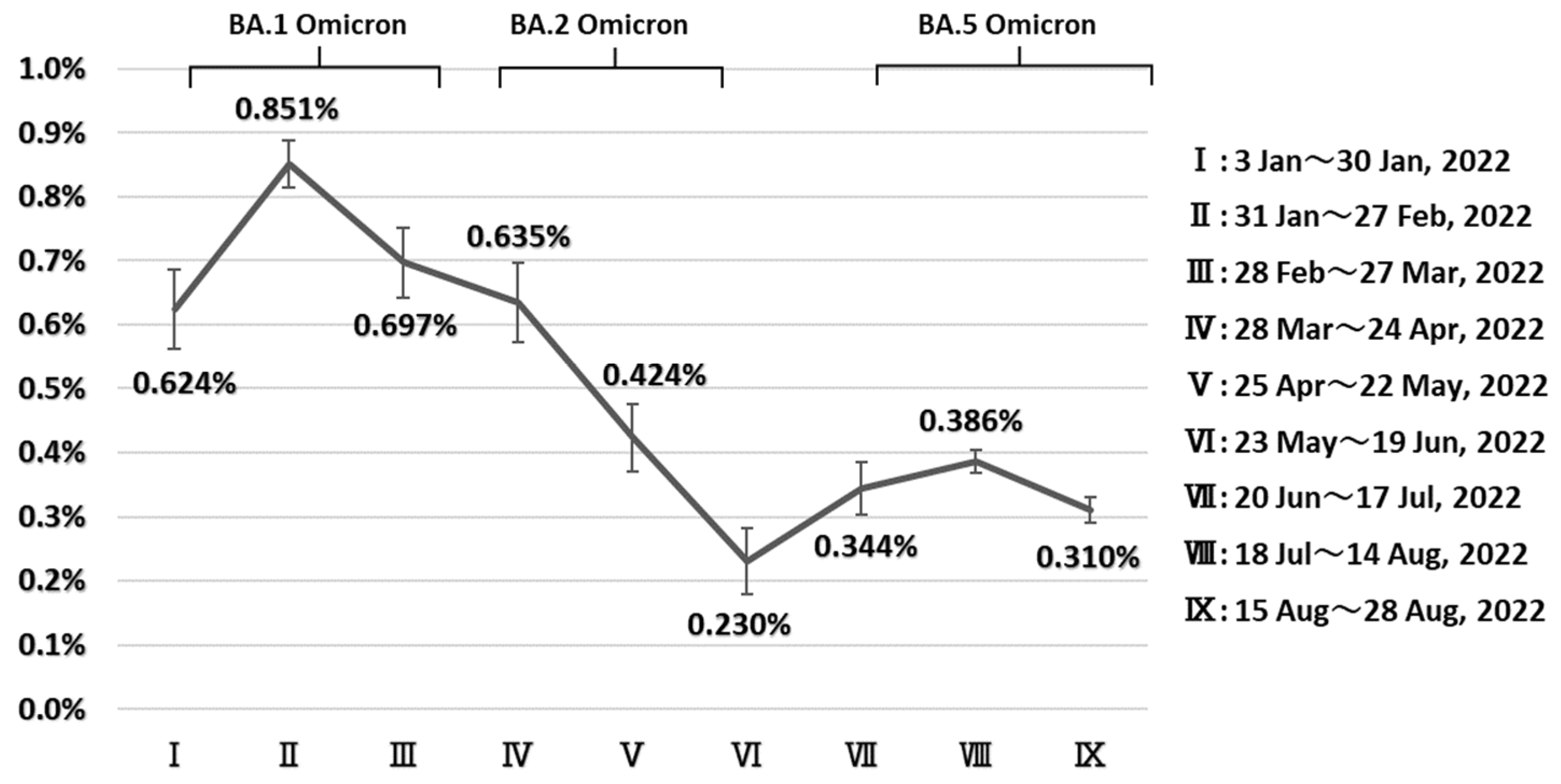
| I (3 January~30 January 2022) | 27,674 | 108 | 0.624% | (0.563%–0.685%) |
| II (31 January~27 February 2022) | 80,101 | 557 | 0.851% | (0.814%–0.888%) |
| III (28 February~27 March 2022) | 39,303 | 169 | 0.697% | (0.642%–0.752%) |
| IV (28 March~24 April 2022) | 34,113 | 110 | 0.635% | (0.572%–0.697%) |
| V (25 April~22 May 2022) | 24,358 | 71 | 0.424% | (0.371%–0.477%) |
| VI (23 May~19 June 2022) | 14,182 | 21 | 0.230% | (0.179%–0.281%) |
| VII (20 June~17 July 2022) | 33,463 | 72 | 0.344% | (0.302%–0.385%) |
| VIII (18 July~14 August 2022) | 182,366 | 474 | 0.386% | (0.368%–0.404%) |
| IX (15 August~28 August 2022) | 117,021 | 254 | 0.310% | (0.290%–0.330%) |
| Diagnosed Period | Cases of COVID-19 Related Deaths | Cases of COVID-19 Non-Related Deaths | Cause of Death Not Known | Total |
|---|---|---|---|---|
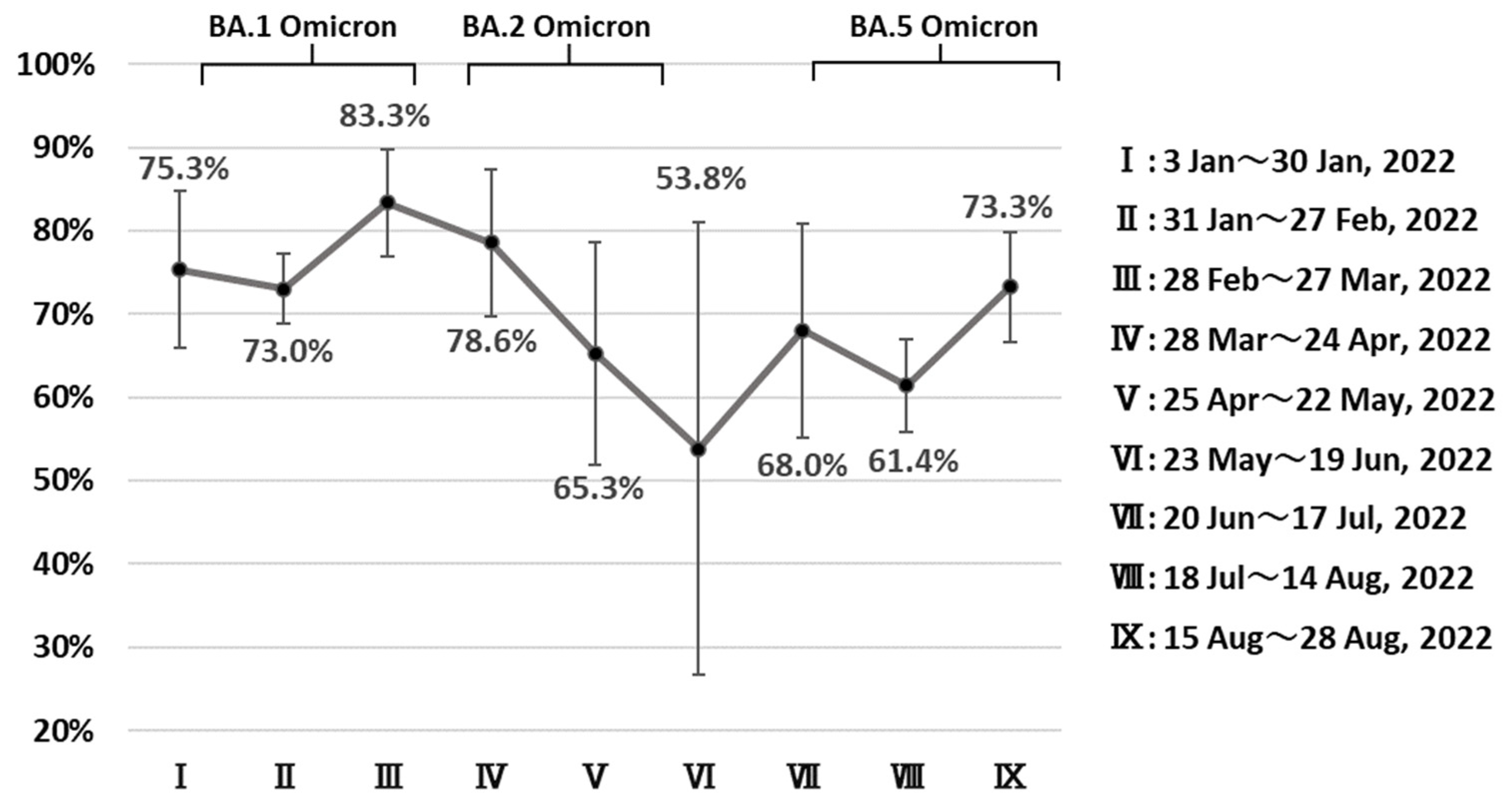
| Ⅰ (3 January~30 January 2022) | 61 | 20 | 27 | 108 |
| Ⅱ (31 January~27 February 2022) | 314 | 116 | 127 | 557 |
| Ⅲ (28 February~27 March 2022) | 110 | 22 | 37 | 169 |
| Ⅳ (28 March~24 April 2022) | 66 | 18 | 26 | 110 |
| Ⅴ (25 April~22 May 2022) | 32 | 17 | 22 | 71 |
| Ⅵ (23 May~19 June 2022) | 7 | 6 | 8 | 21 |
| Ⅶ (20 June~17 July 2022) | 34 | 16 | 22 | 72 |
| Ⅷ (18 July~14 August 2022) | 183 | 115 | 176 | 474 |
| Ⅸ (15 August~28 August 2022) | 126 | 46 | 82 | 254 |
| BA.1(B.1.1.529.1) *1 | BA.2(B.1.1.529.2) *2 | BA.5(B.1.1.529.5) *3 | p-Value (1) *4 | p-Value (2) *4 | |
|---|---|---|---|---|---|
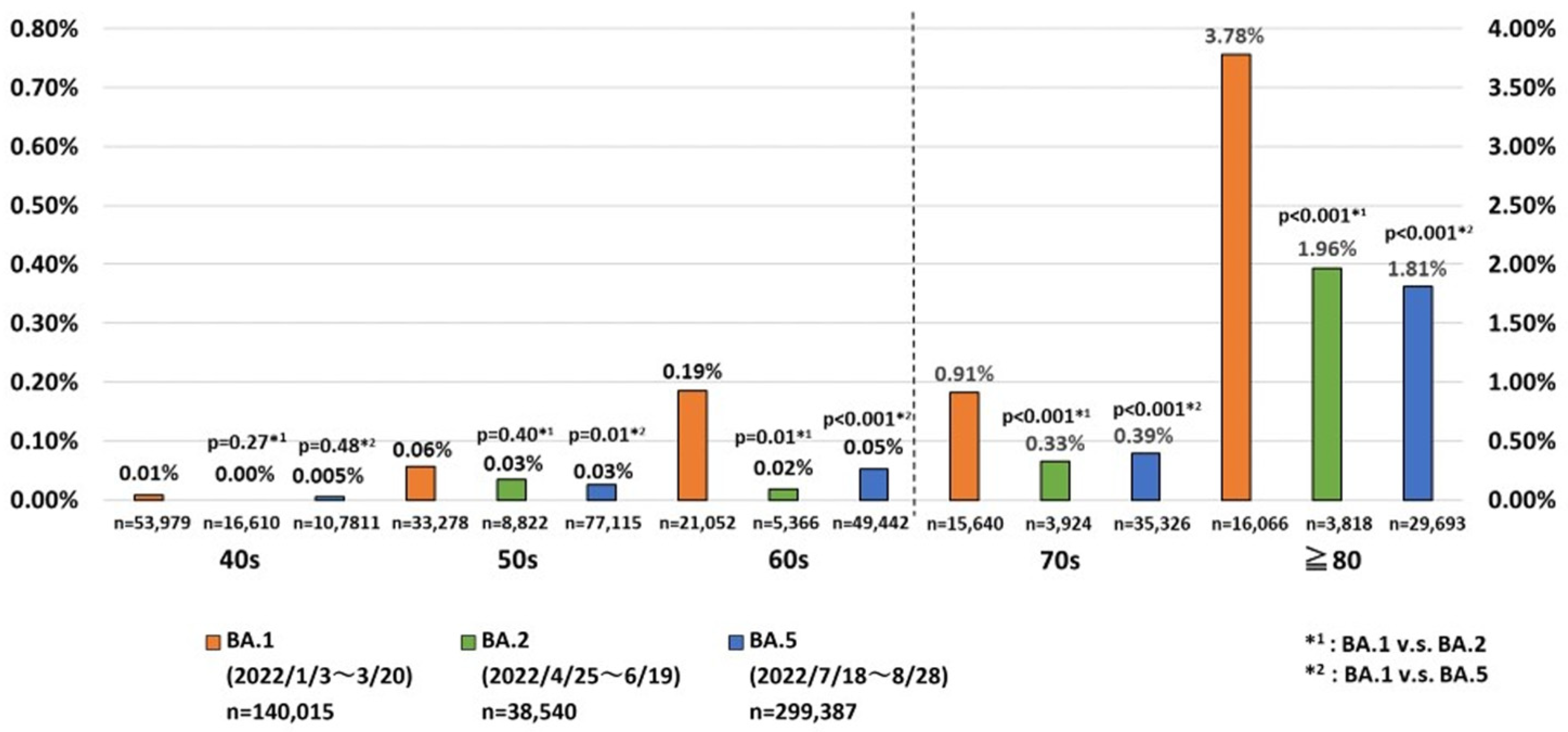
| 40s | 4/53979 (0.00741%) | 0/16610 (0.00%) | 5/107811 (0.00464%) | 0.27 | 0.48 |
| 50s | 19/33278 (0.0571%) | 3/8822 (0.0340%) | 20/77115 (0.0259%) | 0.40 | 0.01 |
| 60s | 39/21052 (0.185%) | 1/5366 (0.0186%) | 26/49442 (0.0526%) | 0.01 | <0.001 |
| 70s | 143/15640 (0.914%) | 13/3924 (0.331%) | 139/35326 (0.393%) | <0.001 | <0.001 |
| ≧80 | 607/16066 (3.78%) | 75/3818 (1.96%) | 538/29693 (1.81%) | <0.001 | <0.001 |
References
- World Health Organization. Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 11 December 2022).
- GISAID. Tracking of HCoV-19 Variants. Available online: https://www.re3data.org/repository/r3d100010126 (accessed on 11 December 2022).
- National Institute of Infectious Diseases. About SARS-CoV-2 Variants. Available online: https://www.niid.go.jp/niid/ja/2019-ncov/2551-cepr/10745-cepr-topics.html (accessed on 11 December 2022).
- Ogata, T.; Tanaka, H.; Tanaka, E.; Osaki, N.; Noguchi, E.; Osaki, Y.; Tono, A.; Wada, K. Increased Secondary Attack Rates among the Household Contacts of Patients with the Omicron Variant of the Coronavirus Disease 2019 in Japan. Int. J. Environ. Res. Public Health 2022, 19, 8068. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, S.B.; Nygård, K.; Kacelnik, O.; Telle, K. Secondary Attack Rates for Omicron and Delta Variants of SARS-CoV-2 in Norwegian Households. JAMA 2022, 327, 1610–1611. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative Analysis of the Risks of Hospitalisation and Death Associated with SARS-CoV-2 Omicron (B.1.1.529) and Delta (B.1.617.2) Variants in England: A Cohort Study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- Auvigne, V.; Vaux, S.; Strat, Y.L.; Schaeffer, J.; Fournier, L.; Tamandjou, C.; Montagnat, C.; Coignard, B.; Levy-Bruhl, D.; Parent du Châtelet, I. Severe Hospital Events Following Symptomatic Infection with Sars-CoV-2 Omicron and Delta Variants in France, December 2021–January 2022: A Retrospective, Population-Based, Matched Cohort Study. eClinicalMedicine 2022, 48, 101455. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, F.; Myers, J.; Basu, D.; Tintinger, G.; Ueckermann, V.; Mathebula, M.; Ramlall, R.; Spoor, S.; de Villiers, T.; Van der Walt, Z.; et al. Decreased Severity of Disease during the First Global Omicron Variant Covid-19 Outbreak in a Large Hospital in Tshwane, South Africa. Int. J. Infect. Dis. 2022, 116, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Liu, B.; Zhang, S.; Huang, N.; Zhao, T.; Lu, Q.-B.; Cui, F. Differences in Incidence and Fatality of COVID-19 by SARS-CoV-2 Omicron Variant versus Delta Variant in Relation to Vaccine Coverage: A World-Wide Review. J. Med. Virol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Esper, F.P.; Adhikari, T.M.; Tu, Z.J.; Cheng, Y.-W.; El-Haddad, K.; Farkas, D.H.; Bosler, D.; Rhoads, D.; Procop, G.W.; Ko, J.S.; et al. Alpha to Omicron: Disease Severity and Clinical Outcomes of Major SARS-CoV-2 Variants. J. Infect. Dis. 2022, 227, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, A.; Kerr, S.; Woolhouse, M.; McMenamin, J.; Robertson, C.; Simpson, C.R.; Millington, T.; Shi, T.; Agrawal, U.; Shahul Hameed, S.; et al. Severity of Omicron Variant of Concern and Effectiveness of Vaccine Boosters against Symptomatic Disease in Scotland (EAVE II): A National Cohort Study with Nested Test-Negative Design. Lancet Infect. Dis. 2022, 22, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Xue, L.; Jing, S.; Zhang, K.; Milne, R.; Wang, H. Infectivity versus Fatality of SARS-CoV-2 Mutations and Influenza. Int. J. Infect. Dis. 2022, 121, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Gram, M.A.; Emborg, H.-D.; Schelde, A.B.; Friis, N.U.; Nielsen, K.F.; Moustsen-Helms, I.R.; Legarth, R.; Lam, J.U.H.; Chaine, M.; Malik, A.Z.; et al. Vaccine Effectiveness against SARS-CoV-2 Infection or COVID-19 Hospitalization with the Alpha, Delta, or Omicron SARS-CoV-2 Variant: A Nationwide Danish Cohort Study. PLoS Med. 2022, 19, e1003992. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, U.; Bedston, S.; McCowan, C.; Oke, J.; Patterson, L.; Robertson, C.; Akbari, A.; Azcoaga-Lorenzo, A.; Bradley, D.T.; Fagbamigbe, A.F.; et al. Severe COVID-19 Outcomes after Full Vaccination of Primary Schedule and Initial Boosters: Pooled Analysis of National Prospective Cohort Studies of 30 Million Individuals in England, Northern Ireland, Scotland, and Wales. Lancet 2022, 400, 1305–1320. [Google Scholar] [CrossRef] [PubMed]
- McConeghy, K.W. Effectiveness of a Second COVID-19 Vaccine Booster Dose Against Infection, Hospitalization, or Death Among Nursing Home Residents—19 States, March 29–July 25, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 1235–1238. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.J.; Hakim, A.J.; Leung, G.M.; Xu, W.; Schluter, W.W.; Novak, R.T.; Marston, B.; Hersh, B.S. COVID-19 Mortality and Vaccine Coverage—Hong Kong Special Administrative Region, China, January 6, 2022-March 21, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 545–548. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.-A.; Kassanjee, R.; Rosseau, P.; Morden, E.; Johnson, L.; Solomon, W.; Hsiao, N.-Y.; Hussey, H.; Meintjes, G.; Paleker, M.; et al. Outcomes of Laboratory-Confirmed SARS-CoV-2 Infection in the Omicron-Driven Fourth Wave Compared with Previous Waves in the Western Cape Province, South Africa. medRxiv 2022. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare Approval Information of a Medical Product for Extracorporeal Checks of New-Style Coronavirus Infectious Disease (Check Kit). Available online: https://www.mhlw.go.jp/stf/newpage_11331.html (accessed on 29 January 2023).
- Jacques, E.; Ellen, B.; Luc, R. Statistical Methods in Cancer Research Volume IV: Descriptive Epidemiology; The International Agency for Research on Cancer: Lyon, France, 1994; ISBN 978-92-832-2128-9. [Google Scholar]
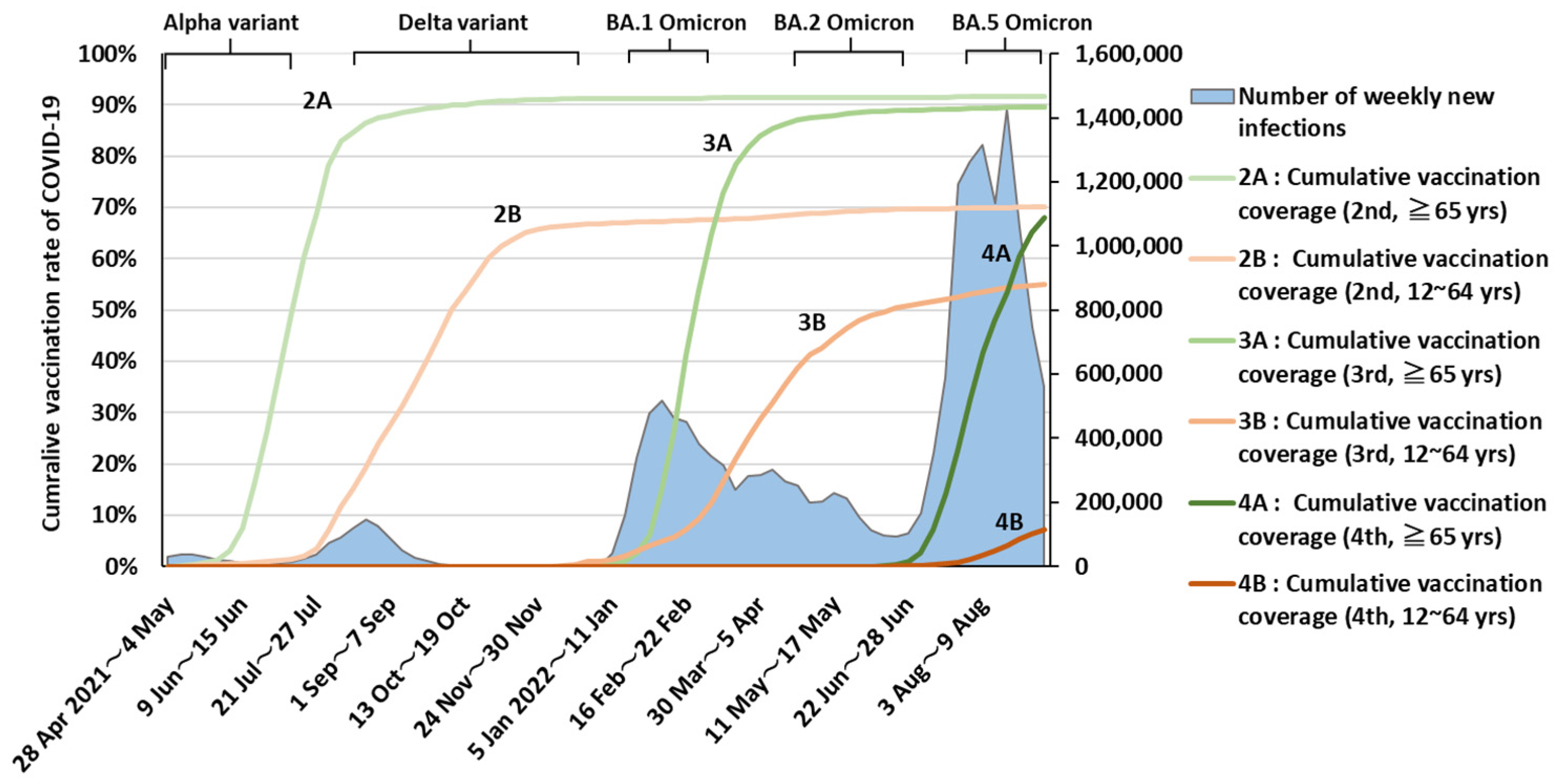
- Prime Minister’s Office of Japan. COVID-19 Vaccines. Available online: https://japan.kantei.go.jp/ongoingtopics/vaccine.html (accessed on 11 December 2022).
- Ministry of Health, Labour and Welfare. General Information about the First Time Inoculation (It’s Inoculated the 1st Time the 2nd Time.). Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000121431_00218.html (accessed on 31 January 2023).
- Ministry of Health, Labour and Welfare. About Special Case Approval of a New-Style Coronavirus Vaccine Based on a Medical Product Medical Device Mood. Available online: https://www.mhlw.go.jp/stf/newpage_16734.html (accessed on 29 January 2023).
- Ministry of Health, Labour and Welfare. About Special Case Approval of a New-Style Coronavirus Vaccine Based on a Medical Product Medical Device Mood. Available online: https://www.mhlw.go.jp/stf/newpage_18787.html (accessed on 31 January 2023).
- Ministry of Health, Labour and Welfare. About Making and Selling Approval of a New-Style Coronavirus Vaccine. Available online: https://www.mhlw.go.jp/stf/newpage_25294.html (accessed on 31 January 2023).
- Ministry of Health, Labour and Welfare. About Special Case Approval of New-Style Coronavirus Medicine. Available online: https://www.mhlw.go.jp/stf/newpage_23047.html (accessed on 11 December 2022).
- Ministry of Health, Labour and Welfare. About Special Case Approval of New-Style Coronavirus Medicine. Available online: https://www.mhlw.go.jp/stf/newpage_23815.html (accessed on 11 December 2022).
- Ministry of Health, Labour and Welfare. Visualizing the Data: Information on COVID-19 Infections. Available online: https://covid19.mhlw.go.jp/en/ (accessed on 11 December 2022).
- Ministry of Health, Labour and Welfare. About an Investigation about the Recuperation Situation etc. and the Inpatient Acceptance Number of Beds, etc. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/newpage_00023.html (accessed on 11 December 2022).
- Lin, D.-Y.; Gu, Y.; Xu, Y.; Wheeler, B.; Young, H.; Sunny, S.K.; Moore, Z.; Zeng, D. Association of Primary and Booster Vaccination and Prior Infection With SARS-CoV-2 Infection and Severe COVID-19 Outcomes. JAMA 2022, 328, 1415–1426. [Google Scholar] [CrossRef] [PubMed]
- knoema®. World and National Data, Maps & Ranking. Available online: https://jp.knoema.com/atlas (accessed on 11 December 2022).
- Madaniyazi, L.; Armstrong, B.; Chung, Y.; Ng, C.F.S.; Seposo, X.; Kim, Y.; Tobias, A.; Guo, Y.; Sera, F.; Honda, Y.; et al. Seasonal Variation in Mortality and the Role of Temperature: A Multi-Country Multi-City Study. Int. J. Epidemiol. 2022, 51, 122–133. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Shinjo, M.; Tsukuma, H.; Kawazuma, Y.; Shimoji, S.; Kinoshita, N.; Morita, T. Seasonal Variation in Mortality from Ischemic Heart Disease and Cerebrovascular Disease in Okinawa and Osaka: The Possible Role of Air Temperature. J. Epidemiol. 2000, 10, 392–398. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takahashi, Y.; Tanaka, H.; Koga, Y.; Takiguchi, S.; Ogimoto, S.; Inaba, S.; Matsuoka, H.; Miyajima, Y.; Takagi, T.; Irie, F.; et al. Change over Time in the Risk of Death among Japanese COVID-19 Cases Caused by the Omicron Variant Depending on Prevalence of Sublineages. Int. J. Environ. Res. Public Health 2023, 20, 2779. https://doi.org/10.3390/ijerph20042779
Takahashi Y, Tanaka H, Koga Y, Takiguchi S, Ogimoto S, Inaba S, Matsuoka H, Miyajima Y, Takagi T, Irie F, et al. Change over Time in the Risk of Death among Japanese COVID-19 Cases Caused by the Omicron Variant Depending on Prevalence of Sublineages. International Journal of Environmental Research and Public Health. 2023; 20(4):2779. https://doi.org/10.3390/ijerph20042779
Chicago/Turabian StyleTakahashi, Yuki, Hideo Tanaka, Yoshitaka Koga, Shunichi Takiguchi, Shigeru Ogimoto, Shizuyo Inaba, Hiroyuki Matsuoka, Yuka Miyajima, Takeshi Takagi, Fujiko Irie, and et al. 2023. "Change over Time in the Risk of Death among Japanese COVID-19 Cases Caused by the Omicron Variant Depending on Prevalence of Sublineages" International Journal of Environmental Research and Public Health 20, no. 4: 2779. https://doi.org/10.3390/ijerph20042779
APA StyleTakahashi, Y., Tanaka, H., Koga, Y., Takiguchi, S., Ogimoto, S., Inaba, S., Matsuoka, H., Miyajima, Y., Takagi, T., Irie, F., Bamba, Y., Yoshimi, F., Suzuki, T., Araki, I., Shirai, C., Matsumoto, S., Shimizu, M., Shibata, T., Nagai, H., ... Ogata, T. (2023). Change over Time in the Risk of Death among Japanese COVID-19 Cases Caused by the Omicron Variant Depending on Prevalence of Sublineages. International Journal of Environmental Research and Public Health, 20(4), 2779. https://doi.org/10.3390/ijerph20042779