
We Are Not Islands: The Role of Social Support in the Relationship between Perceived Stress during the COVID-19 Pandemic and Psychological Distress

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Ethics
2.4. Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Szkody, E.; Stearns, M.; Stanhope, L.; McKinney, C. Stress-Buffering Role of Social Support during COVID-19. Fam. Process 2021, 60, 1002–1015. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S. Perceived stress in a probability sample of the United States. In The Social Psychology of Health; Spacapan, S., Oskamp, S., Eds.; Sage: New York, NY, USA, 1988; pp. 31–67. [Google Scholar]
- Yan, L.; Gan, Y.; Ding, X.; Wu, J.; Duan, H. The relationship between perceived stress and emotional distress during the COVID-19 outbreak: Effects of boredom proneness and coping style. J. Anxiety Disord. 2021, 77, 102328. [Google Scholar] [CrossRef]
- Robinson, E.; Sutin, A.R.; Daly, M.; Jones, A. A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic in 2020. J. Affect. Disord. 2022, 296, 567–576. [Google Scholar] [CrossRef]
- Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2021, 281, 91–98. [Google Scholar] [CrossRef]
- Magnúsdóttir, I.; Lovik, A.; Unnarsdóttir, A.B.; McCartney, D.; Ask, H.; Kõiv, K.; Christoffersen, L.A.N.; Johnson, S.U.; Hauksdóttir, A.; Fawns-Ritchie, C.; et al. Acute COVID-19 severity and mental health morbidity trajectories in patient populations of six nations: An observational study. Lancet Public Health 2022, 7, e406–e416. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Lucock, M. The mental health of university students during the COVID-19 pandemic: An online survey in the UK. PLoS ONE 2022, 17, e0262562. [Google Scholar] [CrossRef]
- Padmanabhanunni, A.; Pretorius, T. Behaviour is the key in a pandemic: The direct and indirect effects of COVID-19-related variables on psychological wellbeing. Psychol. Rep. 2022, 125, 2456–2469. [Google Scholar] [CrossRef]
- Elharake, J.A.; Akbar, F.; Malik, A.A.; Gilliam, W.; Omer, S.B. Mental Health Impact of COVID-19 among Children and College Students: A Systematic Review. Child Psychiatry Hum. Dev. 2022, 1–13. [Google Scholar] [CrossRef]
- Torales, J.; Ríos-González, C.; Barrios, I.; O’Higgins, M.; González, I.; García, O.; Castaldelli-Maia, J.M.; Ventriglio, A. Self-Perceived Stress During the Quarantine of COVID-19 Pandemic in Paraguay: An Exploratory Survey. Front. Psychiatry 2020, 11, 558691. [Google Scholar] [CrossRef] [PubMed]
- Valikhani, A.; Kashani, V.O.; Rahmanian, M.; Sattarian, R.; Rahmati Kankat, L.; Mills, P.J. Examining the mediating role of perceived stress in the relationship between mindfulness and quality of life and mental health: Testing the mindfulness stress buffering model. Anxiety Stress Coping 2020, 33, 311–325. [Google Scholar] [CrossRef]
- Stamatis, C.A.; Broos, H.C.; Hudiburgh, S.E.; Dale, S.K.; Timpano, K.R. A longitudinal investigation of COVID-19 pandemic experiences and mental health among university students. Br. J. Clin. Psychol. 2022, 61, 385–404. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, A.P.; Sonar, N.S.; Tr, J.; Banerjee, M.; Yadav, S. Impact of the COVID-19 Pandemic on the Mental Health of College Students in India: Cross-sectional Web-Based Study. JMIRx Med 2021, 2, e28158. [Google Scholar] [CrossRef] [PubMed]
- Faisal, R.A.; Jobe, M.C.; Ahmed, O.; Sharker, T. Mental Health Status, Anxiety, and Depression Levels of Bangladeshi University Students During the COVID-19 Pandemic. Int. J. Ment. Health Addict. 2022, 20, 1500–1515. [Google Scholar] [CrossRef]
- Grey, I.; Arora, T.; Thomas, J.; Saneh, A.; Tohme, P.; Abi-Habib, R. The role of perceived social support on depression and sleep during the COVID-19 pandemic. Psychiatry Res. 2020, 293, 113452. [Google Scholar] [CrossRef] [PubMed]
- Riepenhausen, A.; Veer, I.M.; Wackerhagen, C.; Reppmann, Z.C.; Köber, G.; Ayuso-Mateos, J.L.; Bögemann, S.A.; Corrao, G.; Felez-Nobrega, M.; Abad, J.M.H.; et al. Coping with COVID: Risk and resilience factors for mental health in a German representative panel study. Psychol. Med. 2022, 1–11. [Google Scholar] [CrossRef]
- Chew, Q.H.; Wei, K.C.; Vasoo, S.; Chua, H.C.; Sim, K. Narrative synthesis of psychological and coping responses towards emerging infectious disease outbreaks in the general population: Practical considerations for the COVID-19 pandemic. Singap. Med. J. 2020, 61, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Song, E.; Yoo, H.J. Impact of Social Support and Social Trust on Public Viral Risk Response: A COVID-19 Survey Study. Int. J. Environ. Res. Public Health 2020, 17, 6589. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Luo, S.; Mu, W.; Li, Y.; Ye, L.; Zheng, X.; Xu, B.; Ding, Y.; Ling, P.; Zhou, M.; et al. Effects of sources of social support and resilience on the mental health of different age groups during the COVID-19 pandemic. BMC Psychiatry 2021, 21, 16. [Google Scholar] [CrossRef]
- Wang, J.; Mann, F.; Lloyd-Evans, B.; Ma, R.; Johnson, S. Associations between loneliness and perceived social support and outcomes of mental health problems: A systematic review. BMC Psychiatry 2018, 18, 156. [Google Scholar] [CrossRef]
- Okabayashi, H.; Liang, J.; Krause, N.; Akiyama, H.; Sugisawa, H. Mental health among older adults in Japan: Do sources of social support and negative interaction make a difference? Soc. Sci. Med. 2004, 59, 2259–2270. [Google Scholar] [CrossRef]
- Alsubaie, M.M.; Stain, H.J.; Webster, L.A.D.; Wadman, R. The role of sources of social support on depression and quality of life for university students. Int. J. Adolesc. Youth 2019, 24, 484–496. [Google Scholar] [CrossRef]
- Qi, M.; Zhou, S.-J.; Guo, Z.-C.; Zhang, L.-G.; Min, H.-J.; Li, X.-M.; Chen, J.-X. The Effect of Social Support on Mental Health in Chinese Adolescents During the Outbreak of COVID-19. J. Adolesc. Health 2020, 67, 514–518. [Google Scholar] [CrossRef]
- Alnazly, E.; Khraisat, O.M.; Al-Bashaireh, A.M.; Bryant, C.L. Anxiety, depression, stress, fear and social support during COVID-19 pandemic among Jordanian healthcare workers. PLoS ONE 2021, 16, e0247679. [Google Scholar] [CrossRef]
- Labrague, L.J. Psychological resilience, coping behaviours and social support among health care workers during the COVID-19 pandemic: A systematic review of quantitative studies. J. Nurs. Manag. 2021, 29, 1893–1905. [Google Scholar] [CrossRef] [PubMed]
- Ifdil, I.; Fadli, R.P.; Suranata, K.; Zola, N.; Ardi, Z. Online mental health services in Indonesia during the COVID-19 outbreak. Asian J. Psychiatry 2020, 51, 102153. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.U.M.; Safri, S.N.A.; Thevadas, R.; Noordin, N.K.; Rahman, A.A.; Sekawi, Z.; Ideris, A.; Sultan, M.T.H. COVID-19 outbreak in Malaysia: Actions taken by the Malaysian government. Int. J. Infect. Dis. 2020, 97, 108–116. [Google Scholar] [CrossRef]
- Kennelly, B.; O’Callaghan, M.; Coughlan, D.; Cullinan, J.; Doherty, E.; Glynn, L.; Moloney, E.; Queally, M. The COVID-19 pandemic in Ireland: An overview of the health service and economic policy response. Health Policy Technol. 2020, 9, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Schulder, T.; Rudenstine, S.; Bhatt, K.J.; McNeal, K.; Ettman, C.K.; Galea, S. A multilevel approach to social support as a determinant of mental health during COVID-19. J. Community Psychol. 2022. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: Berlin, Germany, 1984. [Google Scholar]
- Cohen, S.; Wills, T.A. Stress, Social Support, and the Buffering Hypothesis. Psychol. Bull. 1985, 98, 310–357. [Google Scholar] [CrossRef]
- Bekiros, S.; Jahanshahi, H.; Munoz-Pacheco, J.M. A new buffering theory of social support and psychological stress. PLoS ONE 2022, 17, e0275364. [Google Scholar] [CrossRef]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The Multidimensional Scale of Perceived Social Support. J. Personal. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef]
- Zhang, W.; O’Brien, N.; Forrest, J.I.; Salters, K.A.; Patterson, T.L.; Montaner, J.S.G.; Hogg, R.S.; Lima, V.D. Validating a shortened depression scale (10 item CES-D) among HIV-positive people in British Columbia, Canada. PLoS ONE 2012, 7, e40793. [Google Scholar] [CrossRef]
- Zsido, A.N.; Teleki, S.A.; Csokasi, K.; Rozsa, S.; Bandi, S.A. Development of the short version of the spielberger state—Trait anxiety inventory. Psychiatry Res. 2020, 291, 113223. [Google Scholar] [CrossRef] [PubMed]
- Balsamo, M.; Carlucci, L.; Innamorati, M.; Lester, D.; Pompili, M. Further Insights Into the Beck Hopelessness Scale (BHS): Unidimensionality Among Psychiatric Inpatients. Front. Psychiatry 2020, 11, 727. [Google Scholar] [CrossRef] [PubMed]
- Bruwer, B.; Emsley, R.; Kidd, M.; Lochner, C.; Seedat, S. Psychometric properties of the Multidimensional Scale of Perceived Social Support in youth. Compr. Psychiatry 2008, 49, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Makhubela, M. Assessing psychological stress in South African university students: Measurement validity of the perceived stress scale (PSS-10) in diverse populations. Curr. Psychol. 2022, 41, 2802–2809. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Pretorius, T.B.; Padmanabhanunni, A. Validation of the Connor-Davidson Resilience Scale-10 in South Africa: Item Response Theory and Classical Test Theory. Psychol. Res. Behav. Manag. 2022, 15, 1235–1245. [Google Scholar] [CrossRef]
- Spielberger, C.D. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Beck, A.T.; Weissman, A.; Lester, D.; Trexler, L. The measurement of pessimism: The hopelessness scale. J. Consult. Clin. Psychol. 1974, 42, 861. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Ghafari, R.; Mirghafourvand, M.; Rouhi, M.; Osouli Tabrizi, S. Mental health and its relationship with social support in Iranian students during the COVID-19 pandemic. BMC Psychol. 2021, 9, 81. [Google Scholar] [CrossRef]
- Zhang, R. The stress-buffering effect of self-disclosure on Facebook: An examination of stressful life events, social support, and mental health among college students. Comput. Hum. Behav. 2017, 75, 527–537. [Google Scholar] [CrossRef]
- Lauren, M.S.; Robert, H.P.; Dennis, S.C.; Linda, C.M.; Steven, M.S. How does social support enhance resilience in the trauma-exposed individual? Ecol. Soc. 2015, 20, 10. [Google Scholar] [CrossRef]
- Elmer, T.; Mepham, K.; Stadtfeld, C. Students under lockdown: Comparisons of students’ social networks and mental health before and during the COVID-19 crisis in Switzerland. PLoS ONE 2020, 15, e0236337. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Haigh, E.A.P. Advances in Cognitive Theory and Therapy: The Generic Cognitive Model. Annu. Rev. Clin. Psychol. 2014, 10, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Grupe, D.W.; Nitschke, J.B. Uncertainty and anticipation in anxiety: An integrated neurobiological and psychological perspective. Nat. Rev. Neurosci. 2013, 14, 488–501. [Google Scholar] [CrossRef] [PubMed]
- Harandi, T.F.; Taghinasab, M.M.; Nayeri, T.D. The correlation of social support with mental health: A meta-analysis. Electron. Physician 2017, 9, 5212–5222. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | Categories | n | % |
|---|---|---|---|
| Gender | Women | 248 | 77 |
| Men | 68 | 21.1 | |
| Transgender | 2 | 0.6 | |
| Non-binary | 4 | 0.2 | |
| Area of residence | Urban | 281 | 87.3 |
| Rural | 41 | 12.7 | |
| Do you know people who have been infected with the coronavirus? | Yes | 279 | 86.6 |
| No | 30 | 9.3 | |
| Don’t know | 13 | 4.0 | |
| Have you ever tested positive for COVID-19? | Yes | 82 | 25.5 |
| No | 177 | 55.0 | |
| Suspected COVID-19 | 63 | 19.6 | |
| Have you received a COVID-19 vaccine? | Yes | 279 | 86.6 |
| No | 43 | 13.4 | |
| Have you lost a family member due to COVID-19? | Yes | 131 | 40.7 |
| No | 191 | 59.3 | |
| Age | Mean = 26.01 | SD = 10.19 |
| Variable/Scale | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| 1. Perceived stress | |||||||
| 2. Support from significant others | −0.29 ** | ||||||
| 3. Support from family | −0.30 ** | 0.61 ** | |||||
| 4. Support from friends | −0.28 ** | 0.55 ** | 0.49 ** | ||||
| 5. Hopelessness | 0.47 ** | −0.30 ** | −0.33 ** | −0.22 ** | |||
| 6. Depression | 0.66 ** | −0.35 ** | −0.35 ** | −0.32 ** | 0.50 ** | ||
| 7. Anxiety | 0.60 ** | −0.22 ** | −0.24 | −0.21 ** | 0.46 ** | 0.66 ** | |
| Mean | 23.9 | 19.0 | 17.8 | 17.6 | 2.3 | 14.1 | 12.4 |
| SD | 6.3 | 7.3 | 6.9 | 7.0 | 2.4 | 6.8 | 4.1 |
| Alpha | 0.85 | 0.93 | 0.92 | 0.94 | 0.84 | 0.84 | 0.88 |
| Omega | 0.86 | 0.93 | 0.92 | 0.94 | 0.84 | 0.85 | 0.88 |
| Effect | B | SE | 95% CI | β | p |
|---|---|---|---|---|---|
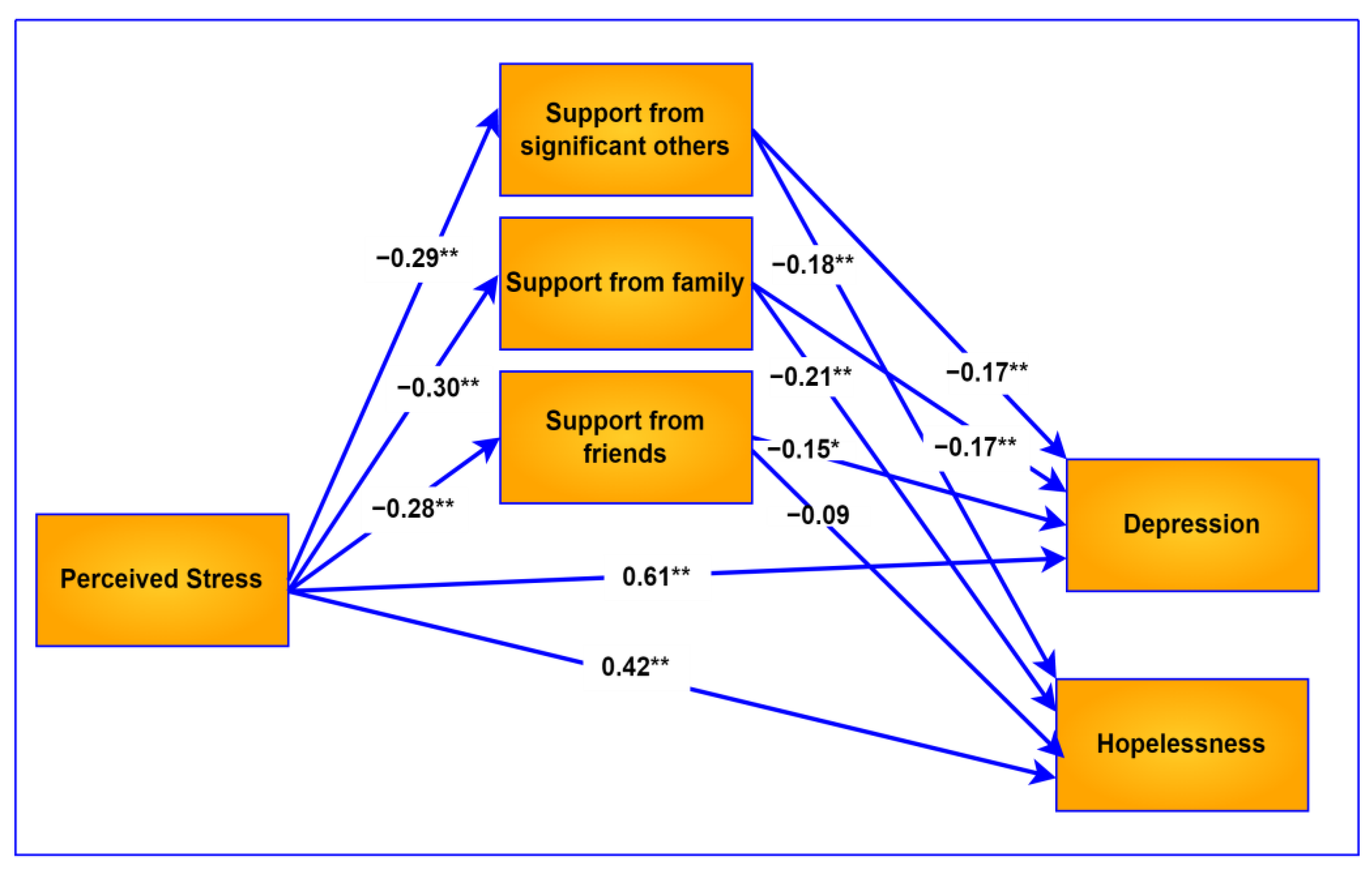
| Direct effects | |||||
| Perceived stress -> depression | 0.660 | 0.046 | [0.569, 0.751] | 0.612 | <0.001 |
| Perceived stress -> hopelessness | 0.164 | 0.020 | [0.126, 0.203] | 0.422 | <0.001 |
| Perceived stress -> anxiety | 0.389 | 0.031 | [0.328, 0.449] | 0.590 | <0.001 |
| Support from significant others -> depression | −0.157 | 0.040 | [−0.235, −0.078] | −0.168 | <0.001 |
| Support from significant others -> hopelessness | −0.060 | 0.017 | [−0.094, −0.027] | −0.180 | <0.001 |
| Support from significant others -> anxiety | −0.028 | 0.026 | [−0.080, 0.024] | −0.049 | 0.294 |
| Support from family -> depression | −0.161 | 0.042 | [−0.244, −0.078 | −0.165 | <0.001 |
| Support from family -> hopelessness | −0.073 | 0.018 | [−0.108, −0.038] | −0.207 | <0.001 |
| Support from family -> anxiety | −0.039 | 0.028 | [−0.094, 0.015] | −0.066 | 0.159 |
| Support from friends -> depression | −0.145 | 0.042 | [−0.227, −0.064] | 0.151 | <0.001 |
| Support from friends -> hopelessness | −0.033 | 0.018 | [−0.068, 0.002] | −0.093 | 0.068 |
| Support from friends -> anxiety | −0.024 | 0.027 | [−0.078, 0.030] | −0.040 | 0.387 |
| Indirect effects | |||||
| Perceived stress -> support from significant others -> depression | 0.053 | 0.017 | [0.023, 0.091] | 0.049 | — |
| Perceived stress -> support from family -> depression | 0.053 | 0.018 | [0.020, 0.093] | 0.050 | — |
| Perceived stress -> support from friends -> depression | 0.046 | 0.017 | [0.015, 0.082] | 0.042 | — |
| Perceived stress -> support from significant others -> hopelessness | 0.020 | 0.007 | [0.008, 0.036] | 0.052 | — |
| Perceived stress -> support from family -> hopelessness | 0.024 | 0.008 | [0.011, 0.041] | 0.062 | — |
| Perceived stress-> support from friends -> hopelessness | 0.010 | 0.006 | [0.000, 0.022] | 0.026 | — |
| Perceived stress -> support from significant others -> anxiety | 0.009 | 0.010 | [−0.010, 0.029] | 0.014 | |
| Perceived stress -> support from family -> anxiety | 0.013 | 0.010 | [−0.006, 0.035] | 0.020 | |
| Perceived stress -> support from friends -> anxiety | 0.007 | 0.009 | [−0.010, 0.027] | 0.011 |
| Variable | B | SE | 95% CI | p |
|---|---|---|---|---|
| Anxiety as outcome variable | ||||
| Perceived Stress | 0.402 | 0.030 | [0.343, 0.460] | <0.001 |
| Support from significant others | −0.042 | 0.026 | [−0.093, 0.008] | 0.100 |
| Support from family | −0.044 | 0.028 | [−0.098, 0.011] | 0.116 |
| Support from friends | −0.032 | 0.027 | [−0.085, 0.021] | 0.235 |
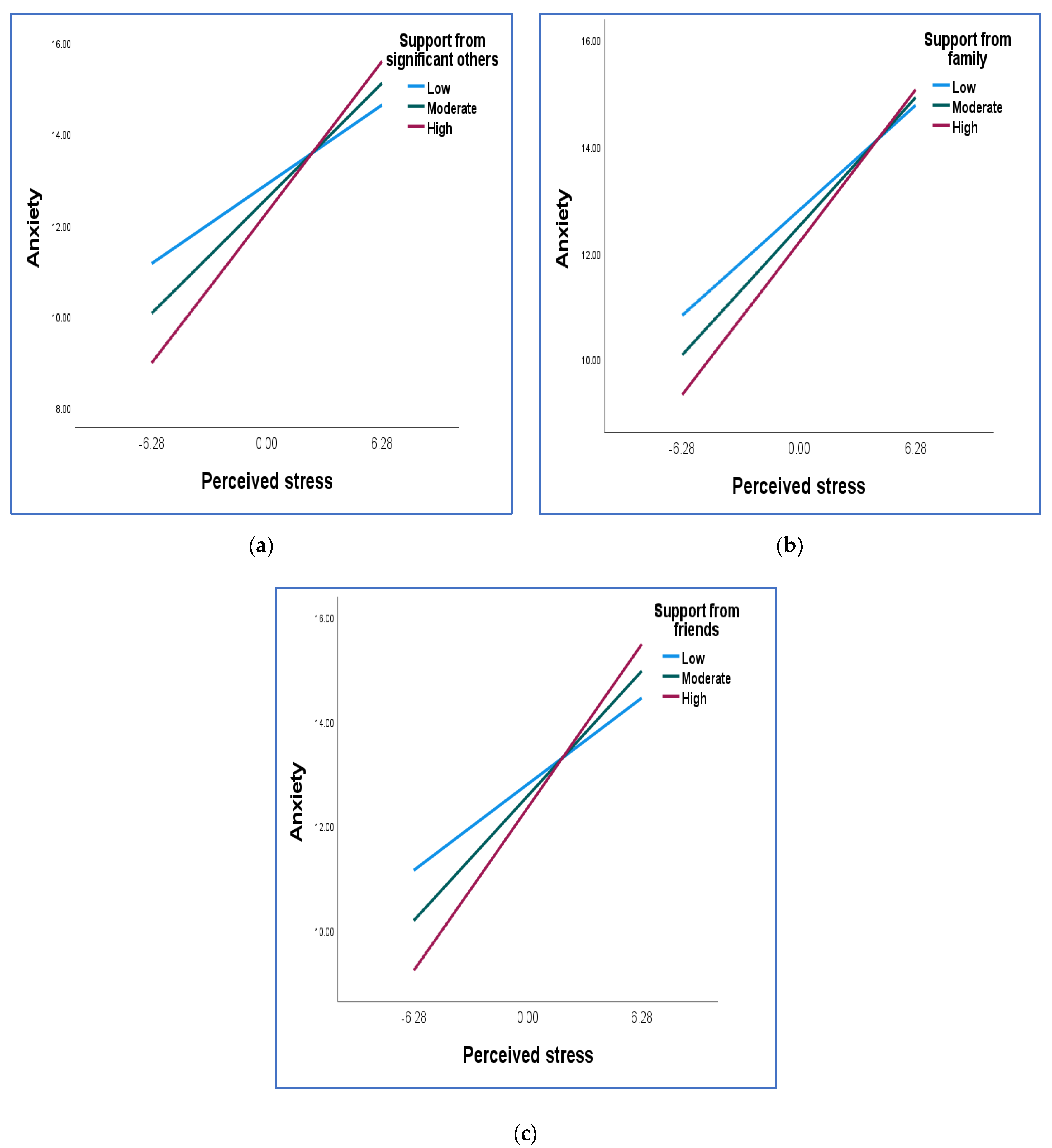
| Perceived stress X support from significant others | 0.017 | 0.004 | [0.010, 0.024] | <0.001 |
| Perceived stress X support from family | 0.010 | 0.004 | [0.002, 0.018] | 0.012 |
| Perceived stress X support from friends | 0.017 | 0.004 | [0.008, 0.025] | <0.001 |
| Values of Social Support | Effect | SE | 95% CI | p |
|---|---|---|---|---|
| Support from significant others | ||||
| Low (mean − 1 SD) | 0.276 | 0.038 | [0.201,0.351] | <0.001 |
| Moderate (mean) | 0.402 | 0.030 | [0.343, 0.460] | <0.001 |
| High (mean + 1 SD) | 0.527 | 0.042 | [0.445, 0.609] | <0.001 |
| Support from family | ||||
| Low (mean − 1 SD) | 0.315 | 0.041 | [0.234, 0.396] | <0.001 |
| Moderate (mean) | 0.386 | 0.030 | [0.326, 0.446] | <0.001 |
| High (mean + 1 SD) | 0.458 | 0.042 | [0.375, 0.540] | <0.001 |
| Support from friends | ||||
| Low (mean − 1 SD) | 0.263 | 0.045 | [0.175, 0.351] | <0.001 |
| Moderate (mean) | 0.381 | 0.030 | [0.322, 0.440] | <0.001 |
| High (mean + 1 SD) | 0.499 | 0.041 | [0.418, 0.580] | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padmanabhanunni, A.; Pretorius, T.B.; Isaacs, S.A. We Are Not Islands: The Role of Social Support in the Relationship between Perceived Stress during the COVID-19 Pandemic and Psychological Distress. Int. J. Environ. Res. Public Health 2023, 20, 3179. https://doi.org/10.3390/ijerph20043179
Padmanabhanunni A, Pretorius TB, Isaacs SA. We Are Not Islands: The Role of Social Support in the Relationship between Perceived Stress during the COVID-19 Pandemic and Psychological Distress. International Journal of Environmental Research and Public Health. 2023; 20(4):3179. https://doi.org/10.3390/ijerph20043179
Chicago/Turabian StylePadmanabhanunni, Anita, Tyrone B. Pretorius, and Serena Ann Isaacs. 2023. "We Are Not Islands: The Role of Social Support in the Relationship between Perceived Stress during the COVID-19 Pandemic and Psychological Distress" International Journal of Environmental Research and Public Health 20, no. 4: 3179. https://doi.org/10.3390/ijerph20043179
APA StylePadmanabhanunni, A., Pretorius, T. B., & Isaacs, S. A. (2023). We Are Not Islands: The Role of Social Support in the Relationship between Perceived Stress during the COVID-19 Pandemic and Psychological Distress. International Journal of Environmental Research and Public Health, 20(4), 3179. https://doi.org/10.3390/ijerph20043179