
Association of Food Desert Residency and Preterm Birth in the United States



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
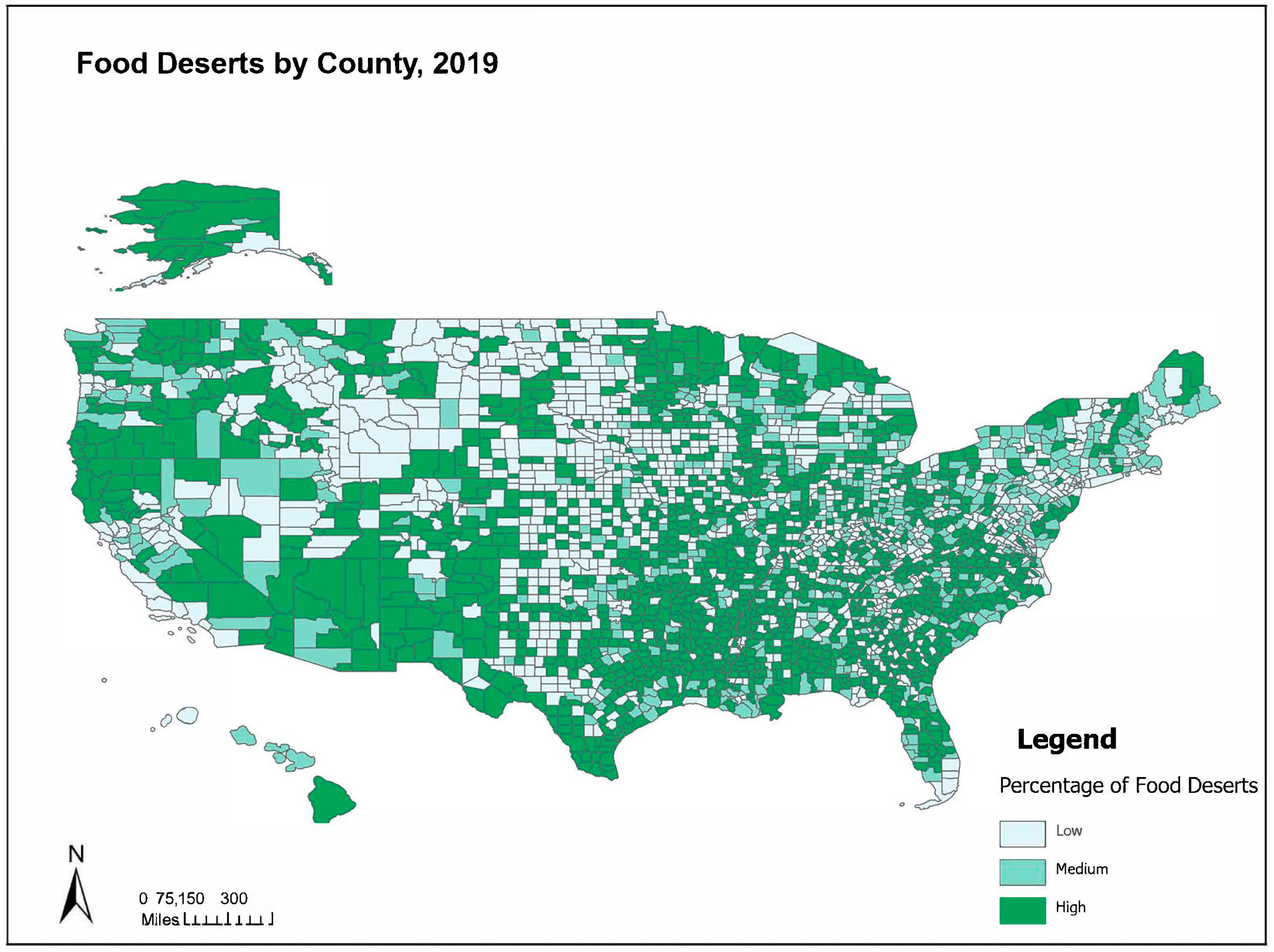
2.2. Exposure Variable
2.3. Outcome
2.4. Individual-Level Covariates
2.5. County-Level Covariates
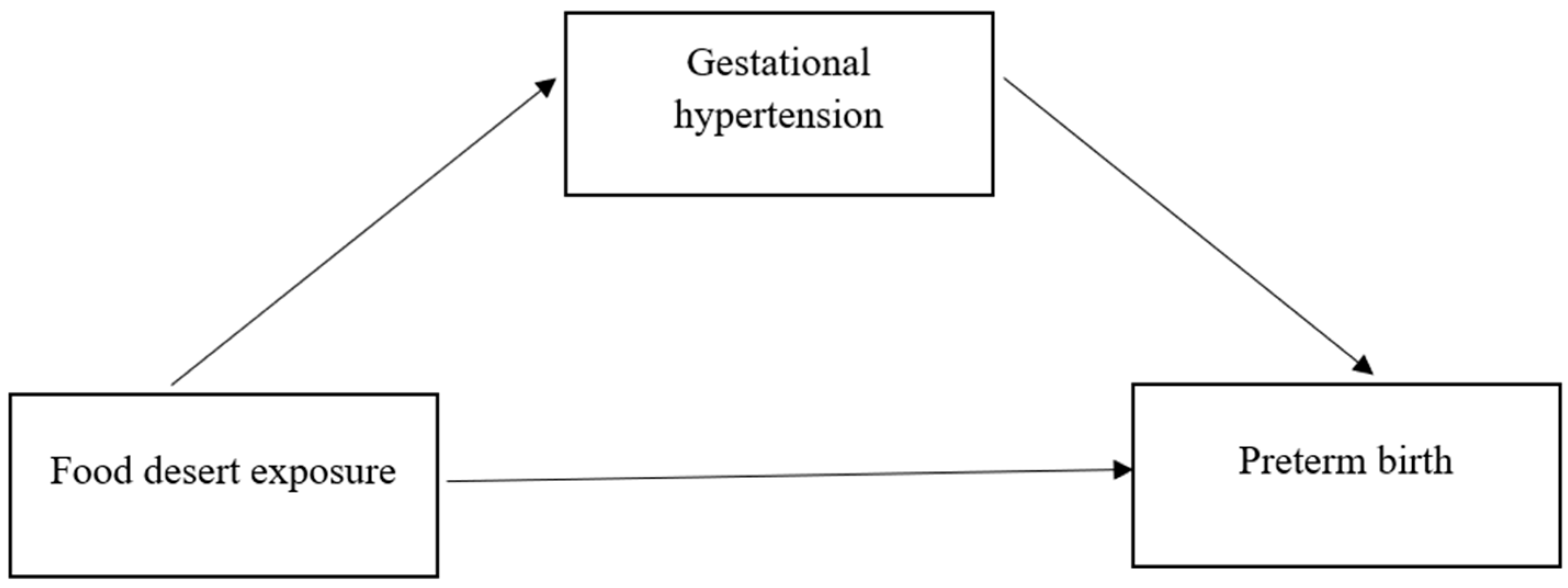
2.6. Mediator
2.7. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giang, T.; Karpyn, A.; Laurison, H.B.; Hillier, A.; Perry, R.D. Closing the Grocery Gap in Underserved Communities: The Creation of the Pennsylvania Fresh Food Financing Initiative. J. Public Health Manag. Pract. 2008, 14, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Singleton, C.R.; Li, Y.; Duran, A.C.; Zenk, S.N.; Odoms-Young, A.; Powell, L.M. Food and Beverage Availability in Small Food Stores Located in Healthy Food Financing Initiative Eligible Communities. Int. J. Environ. Res. Public Health 2017, 14, 1242. [Google Scholar] [CrossRef] [PubMed]
- Agriculture Organization of the United States. The State of Food Insecurity in the World 2013: The Multiple Dimensions of Food Security; FAO: Rome, Italy, 2013. [Google Scholar]
- Goodman, M.; Thomson, J.; Landry, A. Food Environment in the Lower Mississippi Delta: Food Deserts, Food Swamps and Hot Spots. Int. J. Environ. Res. Public Health 2020, 17, 3354. [Google Scholar] [CrossRef]
- Yang, M.; Wang, H.; Qiu, F. Neighbourhood food environments revisited: When food deserts meet food swamps. Can. Geogr./Le Géographe Can. 2020, 64, 135–154. [Google Scholar] [CrossRef]
- Cooksey-Stowers, K.; Schwartz, M.B.; Brownell, K.D. Food Swamps Predict Obesity Rates Better Than Food Deserts in the United States. Int. J. Environ. Res. Public Health 2017, 14, 1366. [Google Scholar] [CrossRef] [PubMed]
- Cooksey Stowers, K.; Jiang, Q.; Atoloye, A.T.; Lucan, S.; Gans, K. Racial Differences in Perceived Food Swamp and Food Desert Exposure and Disparities in Self-Reported Dietary Habits. Int. J. Environ. Res. Public Health 2020, 17, 7143. [Google Scholar] [CrossRef]
- Nagata, J.M.; Palar, K.; Gooding, H.C.; Garber, A.K.; Bibbins-Domingo, K.; Weiser, S.D. Food Insecurity and Chronic Disease in US Young Adults: Findings from the National Longitudinal Study of Adolescent to Adult Health. J. Gen. Intern. Med. 2019, 34, 2756–2762. [Google Scholar] [CrossRef] [PubMed]
- Tipton, M.J.; Wagner, S.A.; Dixon, A.; Westbay, L.; Darji, H.; Graziano, S. Association of Living in a Food Desert with Pregnancy Morbidity. Obstet. Gynecol. 2020, 136, 140–145. [Google Scholar] [CrossRef]
- Bower, K.M.; Thorpe, R.J., Jr.; Rohde, C.; Gaskin, D.J. The intersection of neighborhood racial segregation, poverty, and urbanicity and its impact on food store availability in the United States. Prev. Med. 2014, 58, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Ohri-Vachaspati, P.; DeWeese, R.S.; Acciai, F.; DeLia, D.; Tulloch, D.; Tong, D.; Lorts, C.; Yedidia, M.J. Healthy Food Access in Low-Income High-Minority Communities: A Longitudinal Assessment—2009–2017. Int. J. Environ. Res. Public Health 2019, 16, 2354. [Google Scholar] [CrossRef] [PubMed]
- Singleton, C.R.; Wright, L.A.; McDonald, M.; Archer, I.G.; Bell, C.N.; McLoughlin, G.M.; Houghtaling, B.; Stowers, K.C.; Steeves, E.A. Structural racism and geographic access to food retailers in the United States: A scoping review. Health Place 2023, 83, 103089. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Xie, X.; Yuan, T.; Wang, Y.; Zhao, F.; Zhou, Z.; Zhang, H. Epidemiological trends of maternal hypertensive disorders of pregnancy at the global, regional, and national levels: A population-based study. BMC Pregnancy Childbirth 2021, 21, 364. [Google Scholar] [CrossRef] [PubMed]
- Hutcheon, J.A.; Lisonkova, S.; Joseph, K. Epidemiology of pre-eclampsia and the other hypertensive disorders of pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2011, 25, 391–403. [Google Scholar] [CrossRef]
- Roberts, J.M.; August, P.A.; Bakris, G.; Barton, J.R.; Bernstein, I.M.; Druzin, M.; Ngaiza, K. Hypertension in pregnancy: Executive Summary. Obstet. Gynecol. 2013, 122, 1122–1131. [Google Scholar] [CrossRef]
- Shen, M.; Smith, G.N.; Rodger, M.; White, R.R.; Walker, M.C.; Wen, S.W. Comparison of risk factors and outcomes of gestational hypertension and pre-eclampsia. PLoS ONE 2017, 12, e0175914. [Google Scholar] [CrossRef] [PubMed]
- Arfandi, M.A.; Ansariadi, A.; Amiruddin, R.; Wahiduddin, W.; Salmah, A.U.; Salam, A. Preterm birth risk in mother with hypertensive disorders of pregnancy. Int. J. Public Health Sci. 2023, 12, 590–597. [Google Scholar] [CrossRef]
- Martin, J.; Osterman, M. Shifts in the Distribution of Births by Gestational Age, United States, 2014–2022; National Center for Health Statistics (U.S.): Hyattsville, MD, USA, 2023. [CrossRef]
- Hug, L.; Alexander, M.; You, D.; Alkema, L. National, regional, and global levels and trends in neonatal mortality between 1990 and 2017, with scenario-based projections to 2030: A systematic analysis. Lancet Glob. Health 2019, 7, e710–e720. [Google Scholar] [CrossRef]
- Perin, J.; Mulick, A.; Yeung, D.; Villavicencio, F.; Lopez, G.; Strong, K.L.; Prieto-Merino, D.; Cousens, S.; E Black, R.; Liu, L. Global, regional, and national causes of under-5 mortality in 2000–19: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet Child Adolesc. Health 2022, 6, 106–115. [Google Scholar] [CrossRef]
- Vogel, J.P.; Chawanpaiboon, S.; Moller, A.-B.; Watananirun, K.; Bonet, M.; Lumbiganon, P. The global epidemiology of preterm birth. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 52, 3–12. [Google Scholar] [CrossRef]
- Hamilton, B.E.; Martin, J.A.; Osterman, M.J.K. Births: Provisional Data for 2020. In Vital Stat Rapid Release; National Center for Health Statistics: Hyattsville, MD, USA, 2021; Volume 12. [Google Scholar] [CrossRef]
- Vaccaro, J.A.; Huffman, F.G. Sex and Race/Ethnic Disparities in Food Security and Chronic Diseases in U.S. Older Adults. Geriatr. Med. 2017, 3, 2333721417718344. [Google Scholar] [CrossRef] [PubMed]
- Hill-Briggs, F.; Ephraim, P.L.; Vrany, E.A.; Davidson, K.W.; Pekmezaris, R.; Salas-Lopez, D.; Alfano, C.M.; Gary-Webb, T.L. Social Determinants of Health, Race, and Diabetes Population Health Improvement: Black/African Americans as a Population Exemplar. Curr. Diabetes Rep. 2022, 22, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Squires, G.D. Furthering Fair Housing: Prospects for Racial Justice in America’s Neighborhoods; Steil, J.P., Kelly, N.F., Vale, L.J., Woluchem, M.S., Eds.; Temple University Press: Philadelphia, PA, USA, 2021. [Google Scholar] [CrossRef]
- Bowen, S.; Elliott, S.; Hardison-Moody, A. The structural roots of food insecurity: How racism is a fundamental cause of food insecurity. Sociol. Compass 2021, 15, e12846. [Google Scholar] [CrossRef]
- Rhone, A.; Williams, R.; Dicken, C. Low-Income and Low-Foodstore-Access Census Tracts, 2015–19; 323869; Economic Information Bulletin; United States Department of Agriculture, Economic Research Service: Washington, DC, USA, 2022. [CrossRef]
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Ishaku, S. Hypertensive Disorders of Pregnancy. Hypertension 2018, 72, 24–43. [Google Scholar] [CrossRef] [PubMed]
- Whitfield, K.E.; Allaire, J.C.; Belue, R.; Edwards, C.L. Are Comparisons the Answer to Understanding Behavioral Aspects of Aging in Racial and Ethnic Groups? J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2008, 63, P301–P308. [Google Scholar] [CrossRef]
- Valeri, L.; VanderWeele, T.J. SAS Macro for Causal Mediation Analysis with Survival Data. Epidemiology 2015, 26, e23–e24. [Google Scholar] [CrossRef]
- Willingham, L.; Gordon, J.; Stokes, E.; Scott, W.; Fleenor, R. 402: Association between food deserts and pregnancy outcomes. Am. J. Obstet. Gynecol. 2020, 222, S265–S266. [Google Scholar] [CrossRef]
- Wood, E.K.; Stamos, G.; Mitchell, A.J.; Gonoud, R.; Horgan, A.M.; Nomura, O.; Young, A.; Nigg, J.T.; Gustafsson, H.C.; Sullivan, E.L. The association between food desert severity, socioeconomic status, and metabolic state during pregnancy in a prospective longitudinal cohort. Sci. Rep. 2023, 13, 7197. [Google Scholar] [CrossRef]
- Smith, M.A.B.; Tanner, J.P.; Campos, A.; Wilson, R.; Fryer, K.; Jacques, A.L. Food Desert Residence and the Effect on Breastfeeding Initiation [A199]. Obstet. Gynecol. 2022, 139, 58S. [Google Scholar] [CrossRef]
- Braveman, P.; Dominguez, T.P.; Burke, W.; Dolan, S.M.; Stevenson, D.K.; Jackson, F.M.; Collins, J.W.; Driscoll, D.A.; Haley, T.; Acker, J.; et al. Explaining the Black-White Disparity in Preterm Birth: A Consensus Statement from a Multi-Disciplinary Scientific Work Group Convened by the March of Dimes. Front. Reprod. Health 2021, 3, 684207. [Google Scholar] [CrossRef]
- Giurgescu, C.; Zenk, S.N.; Dancy, B.L.; Park, C.G.; Dieber, W.; Block, R. Relationships among Neighborhood Environment, Racial Discrimination, Psychological Distress, and Preterm Birth in African American Women. J. Obstet. Gynecol. Neonatal Nurs. 2012, 41, E51–E61. [Google Scholar] [CrossRef]
- Chaparro, M.P.; Cruthirds, S.; Bell, C.N.; Wallace, M.E. State-Level Socioeconomic Racial Inequity and Food Insecurity in the U.S. Am. J. Prev. Med. 2022, 63, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Odoms-Young, A.M. Examining the Impact of Structural Racism on Food Insecurity: Implications for Addressing Racial/Ethnic Disparities. Fam. Community Health 2019, 41, S3–S6. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, S.; Toussaint, E.C. Food access in crisis: Food security and COVID-19. Ecol. Econ. 2021, 180, 106859. [Google Scholar] [CrossRef]
- Dubowitz, T.; Dastidar, M.G.; Troxel, W.M.; Beckman, R.; Nugroho, A.; Siddiqi, S.; Cantor, J.; Baird, M.; Richardson, A.S.; Hunter, G.P.; et al. Food Insecurity in a Low-Income, Predominantly African American Cohort Following the COVID-19 Pandemic. Am. J. Public Health 2021, 111, 494–497. [Google Scholar] [CrossRef] [PubMed]
- An, H.; Jin, M.; Li, Z.; Zhang, L.; Li, H.; Zhang, Y.; Ye, R.; Li, N. Impact of gestational hypertension and pre-eclampsia on preterm birth in China: A large prospective cohort study. BMJ Open 2022, 12, e058068. [Google Scholar] [CrossRef]
- Ford, N.D. Hypertensive Disorders in Pregnancy and Mortality at Delivery Hospitalization—United States, 2017–2019. MMWR. Morb. Mortal. Wkly. Rep. 2022, 71, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Gary-Webb, T.L.; Bear, T.M.; Mendez, D.D.; Schiff, M.D.; Keenan, E.; Fabio, A. Evaluation of a Mobile Farmer’s Market Aimed at Increasing Fruit and Vegetable Consumption in Food Deserts: A Pilot Study to Determine Evaluation Feasibility. Health Equity 2018, 2, 375–383. [Google Scholar] [CrossRef]
- Crowe, J.; Lacy, C.; Columbus, Y. Barriers to Food Security and Community Stress in an Urban Food Desert. Urban Sci. 2018, 2, 46. [Google Scholar] [CrossRef]
- Abeykoon, A.H.; Engler-Stringer, R.; Muhajarine, N. Health-related outcomes of new grocery store interventions: A systematic review. Public Health Nutr. 2017, 20, 2236–2248. [Google Scholar] [CrossRef]
- Dubowitz, T.; Ghosh-Dastidar, M.; Cohen, D.A.; Beckman, R.; Steiner, E.D.; Hunter, G.P.; Flórez, K.R.; Huang, C.; Vaughan, C.A.; Sloan, J.C.; et al. Diet and Perceptions Change with Supermarket Introduction in a Food Desert, but Not Because of Supermarket Use. Health Aff. 2015, 34, 1858–1868. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Descriptive Statistics (n = 7,533,086) | ||
|---|---|---|
| n (%) | ||
| Gestational age at birth | ||
| >37 weeks | 6,771,501 (89.8) | |
| <37 weeks | 762,838 (10.1) | |
| Missing | 4913 (0.1) | |
| Previous preterm birth | ||
| Yes | 270,492 (3.6) | |
| No | 7,262,594 (10.1) | |
| Missing | 4913 (0.1) | |
| Maternal race/ethnicity | ||
| Non-Hispanic White | 3,872,325 (51.4) | |
| Non-Hispanic Black | 1,100,104 (14.6) | |
| Hispanic | 1,172,677 (23.5) | |
| Multiracial/other | 724,518 (9.6) | |
| Missing | 69,628 (0.9) | |
| Education attainment | ||
| Less than high school | 928,864 (12.3) | |
| High School | 1,932,708 (25.6) | |
| High school diploma/equivalent | 1,479,970 (19.6) | |
| College educated | 3,094,596 (41.0) | |
| Missing | 103,114 (1.4) | |
| Maternal age | ||
| 19 and under | 355,068 (4.7) | |
| 20–34 | 5,788,083 (76.8) | |
| 35 and up | 1,396,101 (18.5) | |
| Prenatal care initiated | ||
| No prenatal care | 131,340 (1.7) | |
| 1st trimester | 5,706,639 (75.7) | |
| 2nd trimester | 1,189,864 (15.8) | |
| 3rd trimester | 331,259 (4.4) | |
| Missing | 180,150 (2.4) | |
| Urban residence | ||
| Yes | 6,603,752 (87.6) | |
| No | 934,025 (12.4) | |
| Missing | 1475 (0.0) | |
| Mean (SD) | ||
| Food desert indicator 1 mile (urban) and 10 miles (rural) | 13.01 (12.2) | |
| Median income | 67,599.83 (18,390.1) | |
| Level of family poverty | 9.44 (4.2) | |
| Exposure Variable | Total Crude OR (95% C.I.) | Total Adjusted OR (95% C.I.) |
|---|---|---|
| n = 7,533,319 | n = 7,533,319 | |
| Food desert indicator (1 and 10) | ||
| Low % | Ref | Ref |
| Mid-range % | 1.08 (1.04–1.12) | 1.04 (1.01–1.07) |
| High % | 1.17 (1.14–1.22) | 1.07 (1.03–1.11) |
| NH White n = 3,773,576 | NH Black n = 1,050,925 | |||
|---|---|---|---|---|
| Exposure Variable | Crude | Adjusted | Crude | Adjusted |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Food desert indicator (1 and 10) | ||||
| Low % | Ref | Ref | Ref | Ref |
| Mid-range % | 1.07 (1.04–1.11) | * 1.03 (1.00–1.04) | 1.06 (1.00–1.12) | 1.06 (1.01–1.11) |
| High % | 1.15 (1.12–1.19) | 1.06 (1.01–1.07) | 1.16 (1.10–1.21) | 1.10 (1.04–1.16) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haley, C.O.; Singleton, C.R.; King, L.E.; Dyer, L.; Theall, K.P.; Wallace, M. Association of Food Desert Residency and Preterm Birth in the United States. Int. J. Environ. Res. Public Health 2024, 21, 412. https://doi.org/10.3390/ijerph21040412
Haley CO, Singleton CR, King LE, Dyer L, Theall KP, Wallace M. Association of Food Desert Residency and Preterm Birth in the United States. International Journal of Environmental Research and Public Health. 2024; 21(4):412. https://doi.org/10.3390/ijerph21040412
Chicago/Turabian StyleHaley, Chanell O., Chelsea R. Singleton, Lily E. King, Lauren Dyer, Katherine P. Theall, and Maeve Wallace. 2024. "Association of Food Desert Residency and Preterm Birth in the United States" International Journal of Environmental Research and Public Health 21, no. 4: 412. https://doi.org/10.3390/ijerph21040412
APA StyleHaley, C. O., Singleton, C. R., King, L. E., Dyer, L., Theall, K. P., & Wallace, M. (2024). Association of Food Desert Residency and Preterm Birth in the United States. International Journal of Environmental Research and Public Health, 21(4), 412. https://doi.org/10.3390/ijerph21040412