Feasibility of Implementation and the Impact of a Digital Prehabilitation Service in Patients Undergoing Treatment for Oesophago-Gastric Cancer

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Recruitment
2.2. Study Interventions
2.2.1. Digital Prehabilitation Service
2.2.2. In-Person Prehabilitation Service
2.3. Study Outcomes
- Cardio-respiratory fitness assessed by performing the 1 min sit-to-stand test and measuring the heart rate at rest and at the end of the test and 1 min after recovery [13]. Heart rate recovery (HRR) was end of exercise heart rate (beats per minute) minus the heart rate at 1 min recovery. Higher values are associated with improvements following exercise-based cardiac rehabilitation programmes [14].
- Lower limb muscle strength assessed using the 30 s ‘sit-to-stand test’ [15].
2.4. Consent and Regulatory Approvals
2.5. Statistical Analysis
3. Results
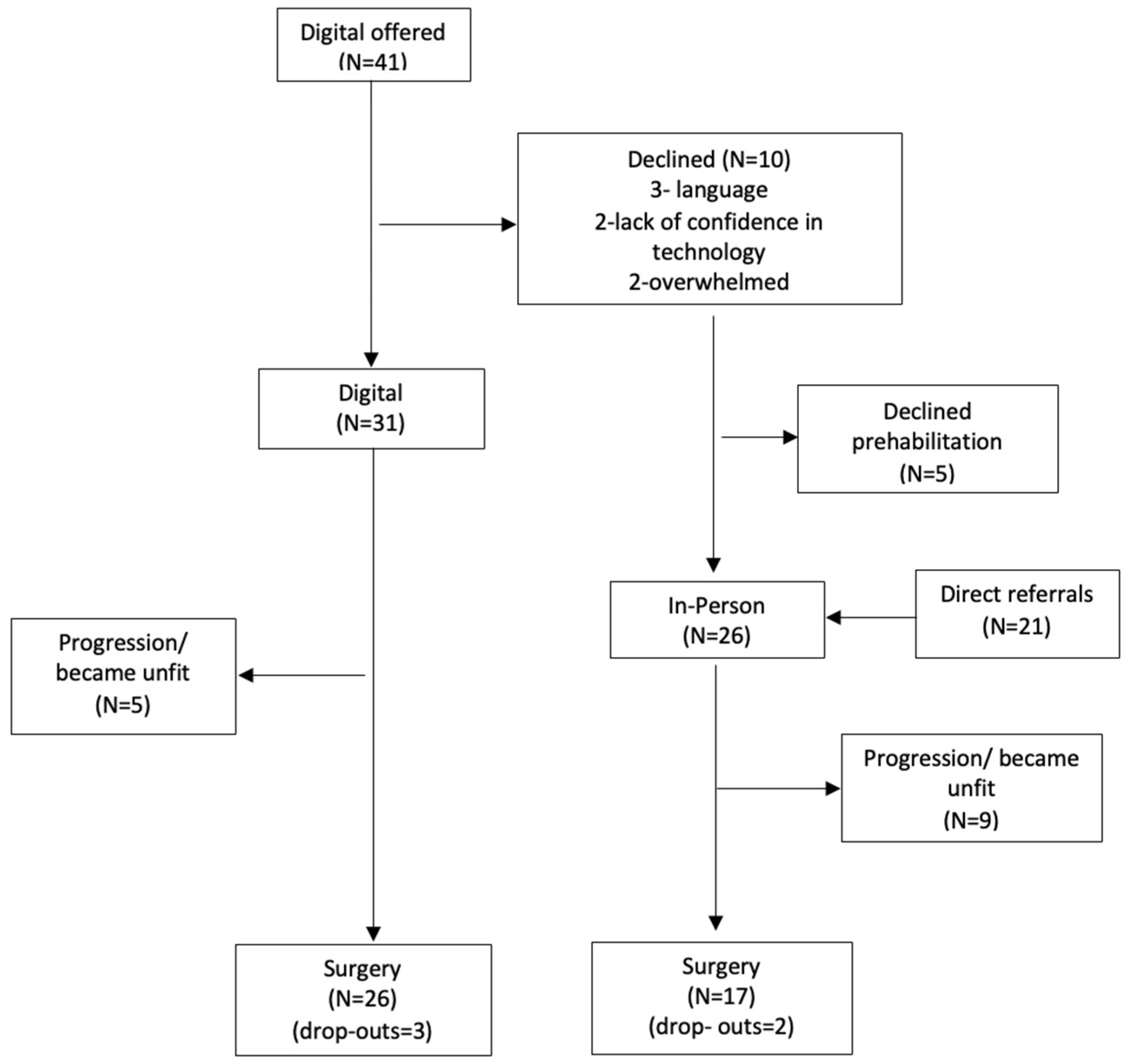
3.1. Recruitment and Retention
3.2. Engagement with Digital Prehabilitation
3.3. Physical Activity, Fitness, and Psychological Wellbeing
3.4. Comparison of Postoperative Outcomes with In-Person Programme
4. Discussion
5. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Low, D.E.; Kuppusamy, M.K.; Alderson, D.; Cecconello, I.; Chang, A.C.; Darling, G.; Davies, A.; D’Journo, X.B.; Gisbertz, S.S.; Griffin, S.M.; et al. Benchmarking Complications Associated with Esophagectomy. Ann. Surg. 2019, 269, 291–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varagunam, M.; Park, M.H.; Sinha, S.; Cromwell, D.; Maynard, N.; Crosby, T.; Trudgill, N.; Michalowski, J.; Salvador, A.; Napper, R. National Oesophago-Gastric Cancer Audit 2018. 2019. An Audit of the Care Received by People with Oesophago-Gastric Cancer in England and Wales 2018 Annual Report. March 2019. Available online: https://www.nogca.org.uk/content/uploads/2019/04/NOGCA-2018-Annual-Report-V2.pdf (accessed on 22 March 2022).
- Paul, S.; Altorki, N. Outcomes in the management of esophageal cancer. J. Surg. Oncol. 2014, 110, 599–610. [Google Scholar] [CrossRef]
- Doorakkers, E.; Konings, P.; Mattsson, F.; Lagergren, J.; Brusselaers, N. Early Complications Following Oesophagectomy for Cancer in Relation to Long-Term Healthcare Utilisation: A Prospective Population-Based Cohort Study. PLoS ONE 2015, 10, e0121080. [Google Scholar] [CrossRef] [PubMed]
- Rutegård, M.; Lagergren, P.; Rouvelas, I.; Mason, R.; Lagergren, J. Surgical complications and long-term survival after esophagectomy for cancer in a nationwide Swedish cohort study. Eur. J. Surg. Oncol. 2012, 38, 555–561. [Google Scholar] [CrossRef]
- Carli, F.; Silver, J.K.; Feldman, L.S.; McKee, A.; Gilman, S.; Gillis, C.; Scheede-Bergdahl, C.; Gamsa, A.; Stout, N.; Hirsch, B. Surgical Prehabilitation in Patients with Cancer. Phys. Med. Rehabil. Clin. N. Am. 2017, 28, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Halliday, L.J.; Doganay, E.; Wynter-Blyth, V.; Osborn, H.; Buckley, J.; Moorthy, K. Adherence to Pre-operative Exercise and the Response to Prehabilitation in Oesophageal Cancer Patients. J. Gastrointest. Surg. 2021, 25, 890–899. [Google Scholar] [CrossRef] [Green Version]
- Halliday, L.J.; Doganay, E.; Wynter-Blyth, V.A.; Hanna, G.B.; Moorthy, K. The Impact of Prehabilitation on Post-operative Outcomes in Oesophageal Cancer Surgery: A Propensity Score Matched Comparison. J. Gastrointest. Surg. 2020, 25, 2733–2741. [Google Scholar] [CrossRef]
- MacMillan-Cancer-Support. Principles and Guidance for Prehabilitation within the Management and Support of People with Cancer. 2020. Available online: https://www.macmillan.org.uk/healthcare-professionals/news-and-resources/guides/principles-and-guidance-for-prehabilitation (accessed on 22 March 2022).
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Courneya, K.S.; Friedenreich, C.M.; Quinney, H.A.; Fields, A.L.A.; Jones, L.W.; Fairey, A.S. Predictors of adherence and contamination in a randomized trial of exercise in colorectal cancer survivors. Psycho-Oncology 2004, 13, 857–866. [Google Scholar] [CrossRef]
- Owusu, C.; Margevicius, S.; Schluchter, M.; Koroukian, S.M.; Berger, N.A. Short Physical Performance Battery, usual gait speed, grip strength and Vulnerable Elders Survey each predict functional decline among older women with breast cancer. J. Geriatr. Oncol. 2017, 8, 356–362. [Google Scholar] [CrossRef]
- Giallauria, F.; Maresca, L.; Vitelli, A.; Santucci De Magistris, M.; Chiodini, P.; Mattiello, A.; Gentile, M.; Mancini, M.; Grieco, A.; Russo, A.; et al. Exercise training improves heart rate recovery in women with breast cancer. SpringerPlus 2015, 4, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giallauria, F.; Lucci, R.; Pietrosante, M.; Gargiulo, G.; De Lorenzo, A.; D’Agostino, M.; Gerundo, G.; Abete, P.; Rengo, F.; Vigorito, C. Exercise-Based Cardiac Rehabilitation Improves Heart Rate Recovery in Elderly Patients after Acute Myocardial Infarction. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 713–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W. Test-retest reliability of the five-repetition sit-to-stand test: A systematic review of the literature involving adults. J. Strength Cond. Res. 2011, 25, 3205–3207. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.J.; Baker-Glenn, E.A.; Granger, L.; Symonds, P. Can the Distress Thermometer be improved by additional mood domains? Part I. Initial validation of the Emotion Thermometers tool. Psycho-Oncology 2010, 19, 125–133. [Google Scholar] [CrossRef]
- Low, D.E.; Alderson, D.; Cecconello, I.; Chang, A.C.; Darling, G.E.; D’Journo, X.B.; Griffin, S.M.; Hölscher, A.H.; Hofstetter, W.L.; Jobe, B.A.; et al. International Consensus on Standardization of Data Collection for Complications Associated With Esophagectomy: Esophagectomy Complications Consensus Group (ECCG). Ann. Surg. 2015, 262, 286–294. [Google Scholar] [CrossRef] [PubMed]
- NHS-Digital. What We Mean by Digital Inclusion. Available online: https://digital.nhs.uk/about-nhs-digital/our-work/digital-inclusion/what-digital-inclusion-is#people-likely-to-be-digitally-excluded (accessed on 22 March 2022).
- Peek, N.; Sujan, M.; Scott, P. Digital health and care in pandemic times: Impact of COVID-19. BMJ Health Care Inform. 2020, 27, e100166. [Google Scholar] [CrossRef]
- Meyerowitz-Katz, G.; Ravi, S.; Arnolda, L.; Feng, X.; Maberly, G.; Astell-Burt, T. Rates of Attrition and Dropout in App-Based Interventions for Chronic Disease: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2020, 22, e20283. [Google Scholar] [CrossRef]
- Perski, O.; Blandford, A.; West, R.; Michie, S. Conceptualising engagement with digital behaviour change interventions: A systematic review using principles from critical interpretive synthesis. Transl. Behav. Med. 2017, 7, 254–267. [Google Scholar] [CrossRef] [Green Version]
- Keller, R.; Hartmann, S.; Teepe, G.W.; Lohse, K.-M.; Alattas, A.; Tudor Car, L.; Müller-Riemenschneider, F.; Von Wangenheim, F.; Mair, J.L.; Kowatsch, T. Digital Behavior Change Interventions for the Prevention and Management of Type 2 Diabetes: Systematic Market Analysis. J. Med. Internet Res. 2022, 24, e33348. [Google Scholar] [CrossRef]
- Aapro, M.; Bossi, P.; Dasari, A.; Fallowfield, L.; Gascón, P.; Geller, M.; Jordan, K.; Kim, J.; Martin, K.; Porzig, S. Digital health for optimal supportive care in oncology: Benefits, limits, and future perspectives. Support. Care Cancer 2020, 28, 4589–4612. [Google Scholar] [CrossRef]
- Spahrkäs, S.S.; Looijmans, A.; Sanderman, R.; Hagedoorn, M. Beating cancer-related fatigue with the Untire mobile app: Results from a waiting-list randomized controlled trial. Psycho-Oncology 2020, 29, 1823–1834. [Google Scholar] [CrossRef] [PubMed]
- Resurrección, D.M.; Motrico, E.; Rubio-Valera, M.; Mora-Pardo, J.A.; Moreno-Peral, P. Reasons for dropout from cardiac rehabilitation programs in women: A qualitative study. PLoS ONE 2018, 13, e0200636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mina, D.S.; Petrella, A.; Currie, K.L.; Bietola, K.; Alibhai, S.M.H.; Trachtenberg, J.; Ritvo, P.; Matthew, A.G. Enablers and Barriers in Delivery of a Cancer Exercise Program: The Canadian Experience. Curr. Oncol. 2015, 22, 374–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghisi, G.L.D.M.; Xu, Z.; Liu, X.; Mola, A.; Gallagher, R.; Babu, A.S.; Yeung, C.; Marzolini, S.; Buckley, J.; Oh, P.; et al. Impacts of the COVID-19 Pandemic on Cardiac Rehabilitation Delivery around the World. Glob. Heart 2021, 16, 43. [Google Scholar] [CrossRef] [PubMed]
- People Are Avoiding Hospital Because They Are Nervous of Catching COVID-19. The Health Foundation. 2020. Available online: https://www.health.org.uk/news-and-comment/news/people-are-avoiding-hospital-because-they-are-nervous-of-catching-covid (accessed on 23 June 2020).
- Grace, S.L.; Mcdonald, J.; Fishman, D.; Caruso, V. Patient Preferences for Home-based Versus Hospital-based Cardiac Rehabilitation. J. Cardiopulm. Rehabil. 2005, 25, 24–29. [Google Scholar] [CrossRef]
- Stout, N.L.; Baima, J.; Swisher, A.K.; Winters-Stone, K.M.; Welsh, J. A Systematic Review of Exercise Systematic Reviews in the Cancer Literature (2005-2017). PMR 2017, 9, S347–S384. [Google Scholar] [CrossRef]
- Sell, N.M.; Silver, J.K.; Rando, S.; Draviam, A.C.; Mina, D.S.; Qadan, M. Prehabilitation Telemedicine in Neoadjuvant Surgical Oncology Patients during the Novel COVID-19 Coronavirus Pandemic. Ann Surg 2020, 272, e81–e83. [Google Scholar] [CrossRef]
- Courneya, K.S. Exercise Interventions During Cancer Treatment: Biopsychosocial Outcomes. Exerc. Sport Sci. Rev. 2001, 29, 60–64. [Google Scholar]
- Schueller, S.M. Grand Challenges in Human Factors and Digital Health. Front. Digit. Health. 2021, 3, 635112. [Google Scholar] [CrossRef]
- Kemp, E.; Trigg, J.; Beatty, L.; Christensen, C.; Dhillon, H.M.; Maeder, A.; Williams, P.A.H.; Koczwara, B. Health literacy, digital health literacy and the implementation of digital health technologies in cancer care: The need for a strategic approach. Health Promot. J. Aust. 2021, 32, 104–114. [Google Scholar] [CrossRef]
- Schmidt, K.; Vogt, L.; Thiel, C.; Jäger, E.; Banzer, W. Validity of the Six-Minute Walk Test in Cancer Patients. Int. J. Sport. Med. 2013, 34, 631–636. [Google Scholar] [CrossRef]
- Lai, A.G.; Pasea, L.; Banerjee, A.; Hall, G.; Denaxas, S.; Chang, W.H.; Katsoulis, M.; Williams, B.; Pillay, D.; Noursadeghi, M.; et al. Estimated impact of the COVID-19 pandemic on cancer services and excess 1-year mortality in people with cancer and multimorbidity: Near real-time data on cancer care, cancer deaths and a population-based cohort study. BMJ Open 2020, 10, e043828. [Google Scholar] [CrossRef] [PubMed]
- Adjekum, A.; Blasimme, A.; Vayena, E. Elements of Trust in Digital Health Systems: Scoping Review. J. Med. Internet Res. 2018, 20, e11254. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.; Byles, J.E.; Inder, K.J. Equity of access to cardiac rehabilitation: The role of system factors. Int. J. Equity Health 2010, 9, 2. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Pre | Post | p Values | |
|---|---|---|---|
| 30 s STS Median (IQR) | 14.5 (10.5–15.5) | 16 (16–22) | 0.02 |
| HRR Median (IQR) | 10.5 (7.5–14) | 15.5 (11–20) | 0.24 |
| Self-reported PA METs mins per week Mean (sd) | 346.5 (362) | 407 (400) | 0.64 |
| Step count Mean (sd) | 5179 (3204) | 4550 (3061) | 0.55 |
| Distress Median (IQR) | 3 (0.5) | 1 (0–2) | 0.04 |
| Anxiety Median (IQR) | 3 (0–5) | 2 (0–3) | 0.22 |
| Depression Median (IQR) | 1 (0–3) | 1 (0–2) | 0.41 |
| Digital (31) | In-Person (26) | p Values | |
|---|---|---|---|
| Age (y, mean (sd)) | 67.4 (8.9) | 65 (10.1) | 0.37 |
| Sex (male) | 26 (84%) | 17 (65%) | 0.06 |
| Stage | 4-1 3-24 2-4 1-2 | 4-3 3-19 2-3 1-1 | 0.70 |
| ASA | 3–17 2–14 | 3–15 2–11 | 0.33 |
| CCI (interquartile range) | 4 (3–5) | 5 (3–6) | 0.08 |
| NAC | 29 (93%) | 23 (88%) | 0.51 |
| Cancer (oesophagus/gastric, GOJ) | O-26 (84%) S-5 GOJ-0 | O-16 (62%) S-5 GOJ-5 | 0.04 |
| Procedures | |||
| - Oesophagectomy | 19 (73%) | 10 (59%) | 0.11 |
| - Gastrectomy | 7 (27%) | 7 (41%) | |
| Postoperative outcomes | |||
| - All complications | 13 (50%) | 11 (64%) | 0.30 |
| - Postoperative pneumonia | 6 (23%) | 7 (41%) | 0.12 |
| - Hospital stay (median (IQR)) | 10.5 (9–18) | 17 (12.25–26) | 0.07 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moorthy, K.; Halliday, L.J.; Noor, N.; Peters, C.J.; Wynter-Blyth, V.; Urch, C.E. Feasibility of Implementation and the Impact of a Digital Prehabilitation Service in Patients Undergoing Treatment for Oesophago-Gastric Cancer. Curr. Oncol. 2023, 30, 1673-1682. https://doi.org/10.3390/curroncol30020128
Moorthy K, Halliday LJ, Noor N, Peters CJ, Wynter-Blyth V, Urch CE. Feasibility of Implementation and the Impact of a Digital Prehabilitation Service in Patients Undergoing Treatment for Oesophago-Gastric Cancer. Current Oncology. 2023; 30(2):1673-1682. https://doi.org/10.3390/curroncol30020128
Chicago/Turabian StyleMoorthy, Krishna, Laura J. Halliday, Nigel Noor, Christopher J Peters, Venetia Wynter-Blyth, and Catherine E Urch. 2023. "Feasibility of Implementation and the Impact of a Digital Prehabilitation Service in Patients Undergoing Treatment for Oesophago-Gastric Cancer" Current Oncology 30, no. 2: 1673-1682. https://doi.org/10.3390/curroncol30020128
APA StyleMoorthy, K., Halliday, L. J., Noor, N., Peters, C. J., Wynter-Blyth, V., & Urch, C. E. (2023). Feasibility of Implementation and the Impact of a Digital Prehabilitation Service in Patients Undergoing Treatment for Oesophago-Gastric Cancer. Current Oncology, 30(2), 1673-1682. https://doi.org/10.3390/curroncol30020128