
The Indoor Climate of Hospitals in Tropical Countries: A Systematic Review

 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
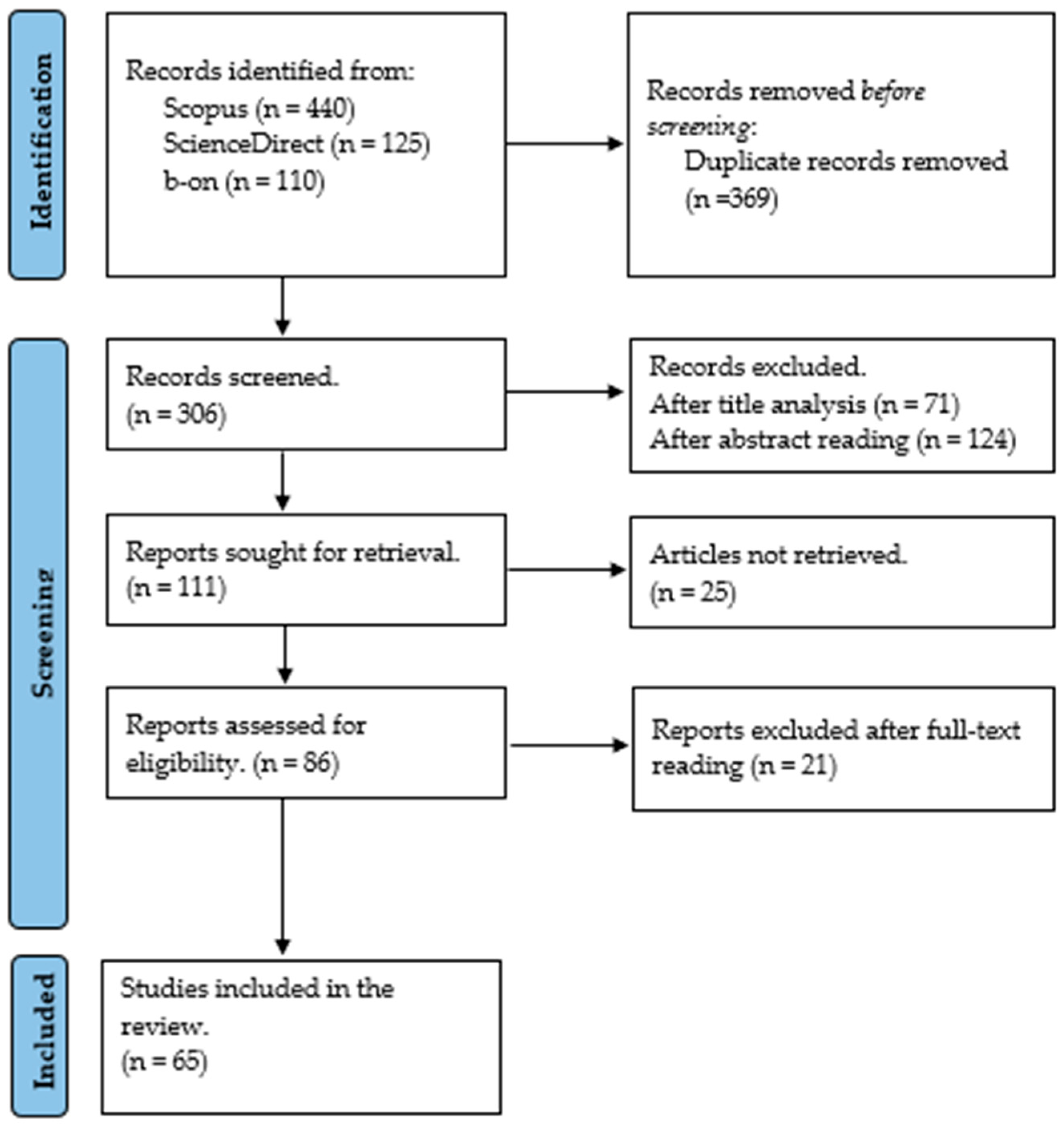
2. Review Methodology
2.1. Inclusion and Exclusion Measures
2.2. Research Questions
- What relevant scientific documentation, studies, and literature are available concerning the IC of hospitals in a tropical climate context and their main findings? (RQ1)
- What aspects of the IC of hospitals in tropical regions have been studied? (RQ2)
- What impacts of the IC conditions on the occupants of hospitals in tropical countries have been reported by the studies? (RQ3)
- What methods were used in these scientific studies of the IC in tropical hospitals? (RQ4)
- What are the areas for further studies concerning the IC of hospital buildings in tropical countries (the research gaps)? (RQ5)
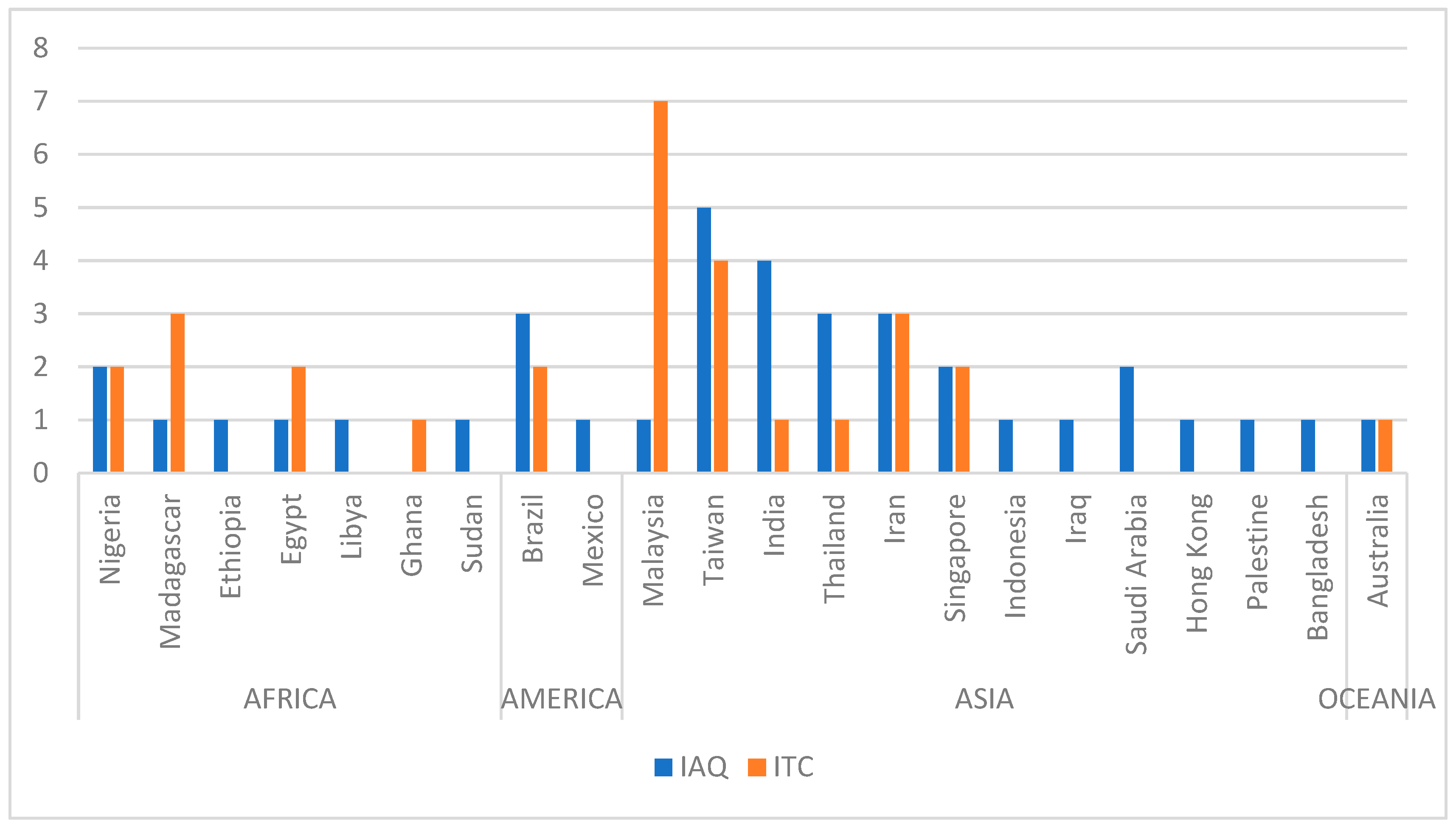
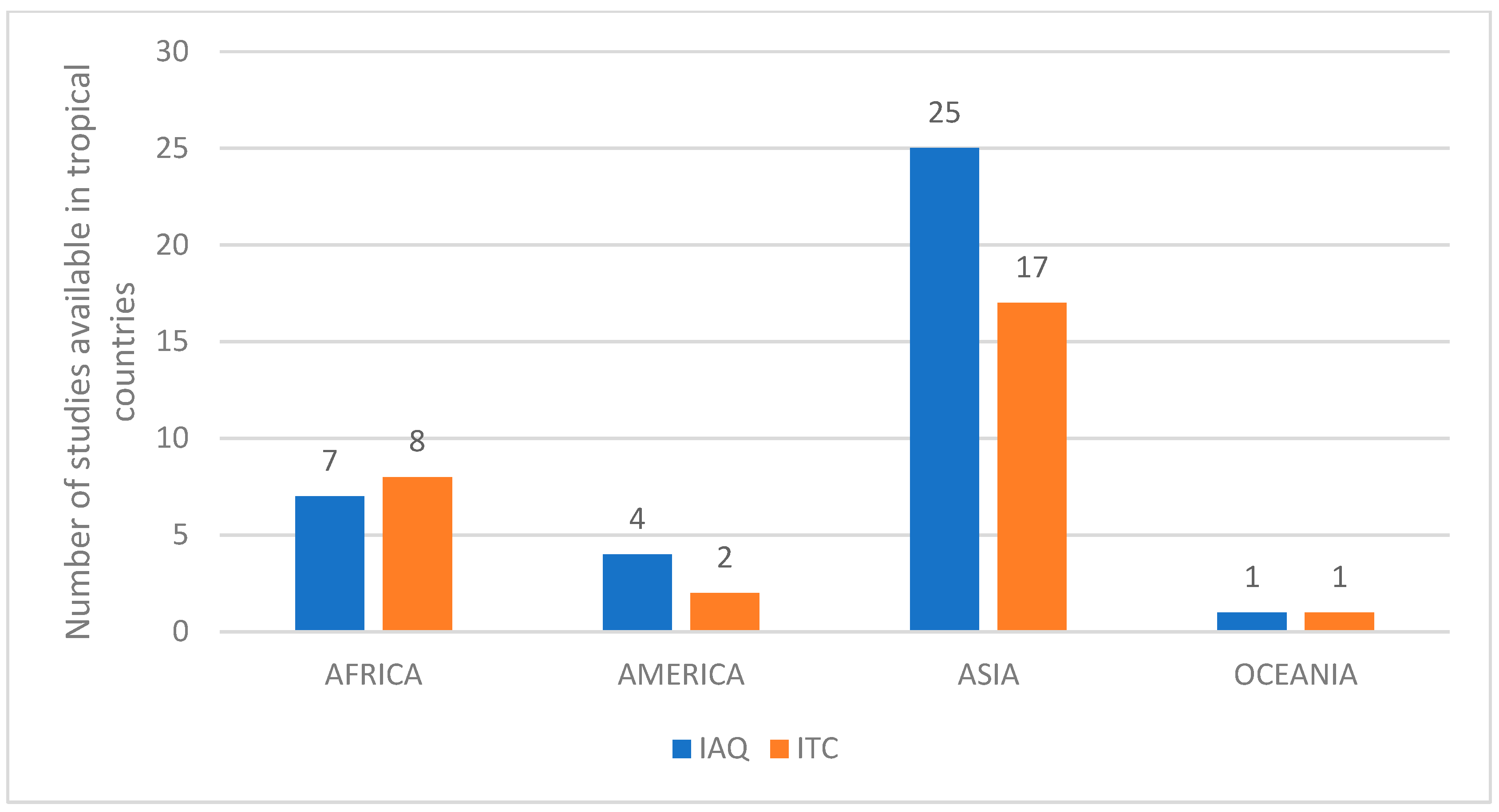
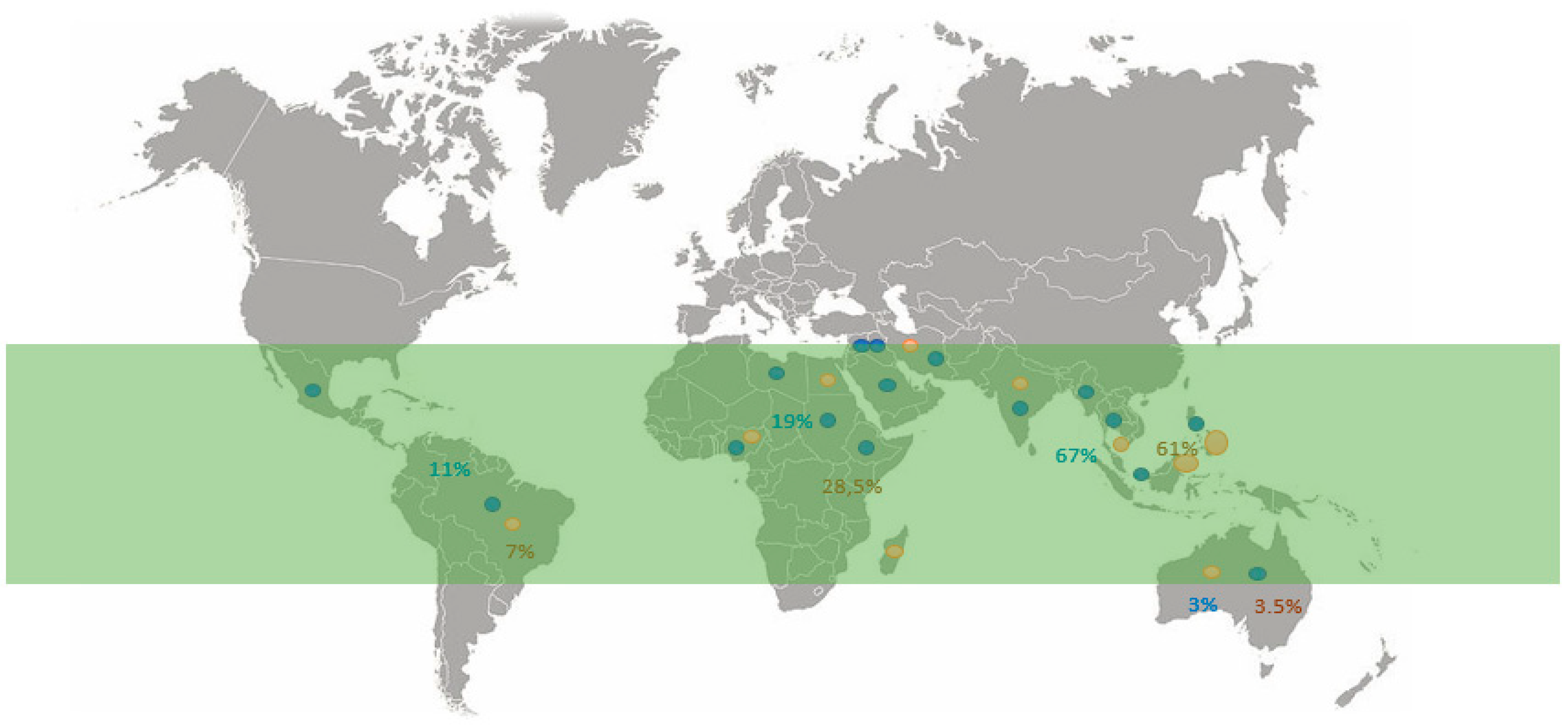
3. Literature Analysis
4. Results and Discussion
4.1. Aspects of IC in Tropical Hospitals
4.2. Implications of Poor IC in Tropical Hospitals
4.2.1. Thermal Comfort Studies
4.2.2. Indoor Air Quality Studies
4.3. Main Methods and Approaches Used in the Reviewed Studies
5. Conclusions
- More studies are required to assess the IC of hospitals with consideration for the outdoor factors, such as the location in industrial zones (exposure to heavy industry operations, mines, mineral processing etc.), commercial zones, and residential zones (ambient traffic and city noise, religious activities). Particular attention should be given to the IC of hospitals in sub-Saharan Africa, such as in the Copperbelt regions.
- Future studies should consider the use of a seasonal assessment in their methodology to evaluate the IEQ parameters by considering the peculiarities of the seasonal differences and effects on the IC. Meanwhile, a seasonal approach for assessing the thermal comfort may be important for considering the peculiarities of occupant’s activities, behaviour, and cultural nuances in developing tropical countries.
- Future studies should pay special attention to the IAQ and comfort parameters, such as the thermal, visual, and acoustic comfort and their impacts on an occupant’s productivity, performance, and behaviour, as well as any behaviour change in the healthcare and schools in tropical countries.
- Future studies should evaluate the gaps and challenges of the IEQ policies, regulations, implementation challenges, and building design practices in developing tropical African countries, with particular attention on the IC of hospitals and schools.
- Future studies should evaluate the IEQ gaps and requirements for the development of well-adapted standards and regulations by considering the climatic, environmental, and infrastructural peculiarities of the tropical countries for the betterment of the IEQ conditions in built and mobile indoor spaces.
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Gómez-Acebo, I.; Llorca, J.; Ortiz-Revuelta, C.; Angulo, B.; Gómez-Álvarez, S.; Dierssen-Sotos, T. Sick building syndrome in a general hospital and the risks for pregnant workers. Int. J. Gynecol. Obstet. 2011, 113, 241–242. [Google Scholar] [CrossRef]
- Akova, I.; Kiliç, E.; Sümer, H.; Keklikçi, T. Prevalence of sick building syndrome in hospital staff and its relationship with indoor environmental quality. Int. J. Environ. Health Res. 2020, 32, 1204–1219. [Google Scholar] [CrossRef]
- Babaoglu, U.T.; Sezgin, F.M.; Yag, F. Sick building symptoms among hospital workers associated with indoor air quality and personal factors. Indoor Built Environ. 2019, 29, 645–655. [Google Scholar] [CrossRef]
- Norbäck, D. An update on sick building syndrome. Curr. Opin. Allergy Clin. Immunol. 2009, 9, 55–59. [Google Scholar] [CrossRef]
- U.S. Environmental Protection Agency and I. Environments Division. Indoor Air Facts No. 4 Sick Building Syndrome. EPA - Air & Radiation (6609J), Research and Development (MD-56). 1991; pp. 1–4. Available online: https://www.epa.gov/sites/production/files/2014-08/documents/sick_building_factsheet.pdf (accessed on 10 April 2023).
- McMichael, A.J. Climate Change and Health: Policy Priorities and Perspectives; Centre on Global Health Security: Washington, DC, USA, 2011; p. 15. [Google Scholar]
- Haines, A.; Smith, K.R.; Anderson, D.; Epstein, P.R.; McMichael, A.J.; Roberts, I.; Wilkinson, P.; Woodcock, J.; Woods, J. Policies for accelerating access to clean energy, improving health, advancing development, and mitigating climate change. Lancet 2007, 370, 1264–1281. [Google Scholar] [CrossRef]
- Fanger, P.O. Analysis and Applications in Environmental Engineering; Danish Technical Press: Copenhagen, Denmark, 1970. [Google Scholar]
- Wang, Y.T.; Chiu, J.C.; Hsu, Y.C.; Wu, T.N.; Shen, Y.H.; Wen, S.B. Investigation on Indoor Air Quality of Public Sites in Tainan Area. Adv. Mater. Res. 2011, 255–260, 1413–1417. [Google Scholar] [CrossRef]
- Van Hoof, J.; Kort, H.; Duijnstee, M.; Rutten, P.; Hensen, J. The indoor environment and the integrated design of homes for older people with dementia. Build. Environ. 2010, 45, 1244–1261. [Google Scholar] [CrossRef]
- Dahlia, Y. Physical and Physiological Thermal Comfort on Indoor Studio. 2018, pp. 19–23. Available online: https://www.thefreelibrary.com/_/print/PrintArticle.aspx?id=601551025 (accessed on 10 April 2023).
- Szczurek, A.; Maciejewska, M.; Połoczański, R.; Teuerle, M.; Wyłomańska, A. Dynamics of carbon dioxide concentration in indoor air. Stoch. Environ. Res. Risk Assess. 2014, 29, 2193–2199. [Google Scholar] [CrossRef]
- Zhang, H.; Xie, X.; Hong, S.; Lv, H. Impact of metabolism and the clothing thermal resistance on inpatient thermal comfort. Energy Built Environ. 2020, 2, 223–232. [Google Scholar] [CrossRef]
- Watkins, E. VOCs and Indoor Air Quality. September 2014. Available online: https://blog.cashins.com/blog-0/bid/194114/VOCs-and-Indoor-Air-Quality (accessed on 10 April 2023).
- Corgnati, S.P.; da Silva, M.G.; Ansaldi, R.I.; Asasi, E.; Costa, J.J.; Filipi, M.; Kaczmarczyk, J.; Melikov, A.K.; Olesen, B.W.; Popiolek, Z. Indoor Climate Quality Assessment; REHVA, Federation of European Heating, Ventilation and Air-conditioning Associations: Brussels, Belgium, 2011. [Google Scholar]
- Fanger, P.O.; Toftum, J. Extension of the PMV model to non-air-conditioned buildings in warm climates. Energy Build. 2002, 34, 533–536. [Google Scholar] [CrossRef]
- Verheyen, J.; Theys, N.; Allonsius, L.; Descamps, F. Thermal comfort of patients: Objective and subjective measurements in patient rooms of a Belgian healthcare facility. Build. Environ. 2011, 46, 1195–1204. [Google Scholar] [CrossRef]
- Rodriguez, C.M.; D’Alessandro, M. Indoor thermal comfort review: The tropics as the next frontier. Urban Clim. 2019, 29, 100488. [Google Scholar] [CrossRef]
- Rajapaksha, I.; Nagai, H.; Okumiya, M. Indoor Thermal Modification of a Ventilated Courtyard House in the Tropics. J. Asian Arch. Build. Eng. 2002, 1, 87–94. [Google Scholar] [CrossRef]
- Kubota, T.; Ahmad, S. Wind Environment Evaluation of Neighborhood Areas in Major Towns of Malaysia. J. Asian Arch. Build. Eng. 2006, 5, 199–206. [Google Scholar] [CrossRef]
- Taylor, J.; Shrubsole, C.; Davies, M.; Biddulph, P.; Das, P.; Hamilton, I.; Vardoulakis, S.; Mavrogianni, A.; Jones, B.; Oikonomou, E. The modifying effect of the building envelope on population exposure to PM2.5 from outdoor sources. Indoor Air 2014, 24, 639–651. [Google Scholar] [CrossRef]
- Van den Berg, A.E. Health Impacts of Healing Environments, a Review of Evidence for Benefits of Nature, Daylight, Fresh Air, and Quiet in Healthcare Settings; UMCG: Hanzeplein, The Netherlands, 2005. [Google Scholar]
- Zborowsky, T.; Kreitzer, M.J. Creating optimal healing environments in a health care setting—PubMed. Minn. Med. 2008, 91, 35–38. Available online: https://pubmed.ncbi.nlm.nih.gov/18438085/ (accessed on 15 September 2021).
- Mayssara, A. Abo Hassanin Supervised, Affiifi. IAQ in Hospitals—Better Health through Indoor Air Quality Awareness. In Paper Knowledge. Toward a Media History of Documents; Duke University Press: Durham, NC, USA, 2014. [Google Scholar]
- Mahbob, N.S.; Kamaruzzaman, S.N.; Salleh, N.; Sulaiman, R. A Correlation Studies of Indoor Environmental Quality (IEQ) Towards Productive Workplace. In Proceedings of the 2nd International Conference on Environmental Science and Technology (ICEST 2011), Singapore, 26–28 February 2011; Volume 6, pp. 434–438. [Google Scholar]
- Sadek, A.H.; Nofal, E.M. Effects of Indoor Environmental Quality on Occupant Satisfaction in Healing Environments. 2013. Available online: https://www.researchgate.net/publication/258510534 (accessed on 10 April 2023).
- Pejtersen, J.; Allermann, L.; Kristensen, T.S.; Poulsen, O.M. Indoor climate, psychosocial work environment and symptoms in open-plan offices. Indoor Air 2006, 16, 392–401. [Google Scholar] [CrossRef]
- Antunes, F.; Safdar, S.; Monteiro, A.; Samsudin, E.Z. Hospital indoor air quality and its relationships with building design, building operation, and occupant-related factors: A mini-review. Front. Public Health 2022, 10, 1067764. [Google Scholar]
- Fonseca, A.; Abreu, I.; Guerreiro, M.J.; Barros, N. Indoor Air Quality in Healthcare Units—A Systematic Literature Review Focusing Recent Research. Sustainability 2022, 14, 967. [Google Scholar] [CrossRef]
- Ramaswamy, M.; Al-Jahwari, F.; Al-Rajhi, S.M.M. IAQ in Hospitals-Better Health through Indoor Air Quality Awareness. 2010. Available online: https://oaktrust.library.tamu.edu/handle/1969.1/94139 (accessed on 10 April 2023).
- Thiam, D.R. Structures of energy resources consumption in Senegal in 2006. J. Energy South. Afr. 2011, 22, 23–34. [Google Scholar] [CrossRef]
- WHO. Energizing Health: Accelerating Electricity Access in Health-Care Facilities; WHO: Geneva, Switzerland, 2023. [Google Scholar]
- Buchanan, T.L.; Barker, K.N.; Tyrone Gibson, J.; Jiang, B.C.; Pearson, R.E. Illumination and Errors in Dispensing. 1991. Available online: https://academic.oup.com/ajhp/article-abstract/48/10/2137/5183010 (accessed on 10 April 2023).
- Davis, R.G.; McCunn, L.J.; Wilkerson, A.; Safranek, S. Nurses’ Satisfaction with Patient Room Lighting Conditions: A Study of Nurses in Four Hospitals With Differences in the Environment of Care. HERD Health Environ. Res. Des. J. 2020, 13, 110–124. [Google Scholar] [CrossRef]
- Juang, D.F.; Lee, C.H.; Yang, T.; Chang, M.C. ABSTRACT: Noise pollution and its effects on medical care workers and patients in hospitals. Int. J. Environ. Sci. Tech. 2010, 7, 705–716. [Google Scholar] [CrossRef]
- Nyembwe, J.-P.K.B.; Ogundiran, J.O.; da Silva, M.G.; Simões, N.A.V. Evaluation of Noise Level in Intensive Care Units of Hospitals and Noise Mitigation Strategies, Case Study: Democratic Republic of Congo. Buildings 2023, 13, 278. [Google Scholar] [CrossRef]
- Ebrahimi-Moghadam, A.; Ildarabadi, P.; Aliakbari, K.; Fadaee, F. Sensitivity analysis and multi-objective optimization of energy consumption and thermal comfort by using interior light shelves in residential buildings. Renew. Energy 2020, 159, 736–755. [Google Scholar] [CrossRef]
- Ebrahimi-Moghadam, A.; Ildarabadi, P.; Aliakbari, K.; Arabkoohsar, A.; Fadaee, F. Performance analysis of light shelves in providing visual and thermal comfort and energy savings in residential buildings. J. Braz. Soc. Mech. Sci. Eng. 2020, 42, 484. [Google Scholar] [CrossRef]
- Lan, L.; Tushar, W.; Otto, K.; Yuen, C.; Wood, K.L. Thermal comfort improvement of naturally ventilated patient wards in Singapore. Energy Build. 2017, 154, 499–512. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Khodakarami, J.; Nasrollahi, N. Thermal comfort in hospitals—A literature review. Renew. Sustain. Energy Rev. 2012, 16, 4071–4077. [Google Scholar] [CrossRef]
- Sodha, M.; Sharma, A.; Singh, S.; Bansal, N.; Kumar, A. Evaluation of an earth—Air tunnel system for cooling/heating of a hospital complex. Build. Environ. 1985, 20, 115–122. [Google Scholar] [CrossRef]
- Chow, T.-T.; Yang, X.-Y. Performance of ventilation system in a non-standard operating room. Build. Environ. 2003, 38, 1401–1411. [Google Scholar] [CrossRef]
- Hwang, R.-L.; Lin, T.-P.; Cheng, M.-J.; Chien, J.-H. Patient thermal comfort requirement for hospital environments in Taiwan. Build. Environ. 2007, 42, 2980–2987. [Google Scholar] [CrossRef]
- Nematchoua, M.K.; Ricciardi, P.; Reiter, S.; Asadi, S.; Demers, C.M. Thermal comfort and comparison of some parameters coming from hospitals and shopping centers under natural ventilation: The case of Madagascar Island. J. Build. Eng. 2017, 13, 196–206. [Google Scholar] [CrossRef]
- Nematchoua, M.K.; Ricciardi, P.; Buratti, C. Statistical analysis of indoor parameters an subjective responses of building occupants in a hot region of Indian ocean; a case of Madagascar island. Appl. Energy 2017, 208, 1562–1575. [Google Scholar] [CrossRef]
- Alfa, M.T. Perceived indoor environmental quality of hospital wards and patients outcomes: A study of a general hospital, minna, Nigeria. Appl. Ecol. Environ. Res. 2019, 17, 8235–8259. [Google Scholar] [CrossRef]
- El Hamid, A.A.; El Helw, M.; Teamah, H.A.M. Three-Dimensional Thermal Comfort Analysis for Hospital Operating Room with the Effect of Door Gradually Opened Part (II) Effect on mean age of the air and predicted mean vote distribution. CFD Lett. 2013, 5, 20–31. [Google Scholar]
- El Hamid, A.A.; El Helw, M.; Teamah, H.A.M. Three-dimensional thermal comfort analysis for hospital operating room with the effect of door gradually opened part (I) effect on velocity and temperature distributions. CFD Lett. 2013, 5, 6–19. [Google Scholar]
- Tartarini, F.; Cooper, P.; Fleming, R. Thermal perceptions, preferences and adaptive behaviours of occupants of nursing homes. Build. Environ. 2018, 132, 57–69. [Google Scholar] [CrossRef]
- Pereira, P.F.D.C.; Broday, E.E.; Xavier, A.A.D.P. Thermal Comfort Applied in Hospital Environments: A Literature Review. Appl. Sci. 2020, 10, 7030. [Google Scholar] [CrossRef]
- Cheong, K.; Chong, K. Development and application of an indoor air quality audit to an air-conditioned building in Singapore. Build. Environ. 2001, 36, 181–188. [Google Scholar] [CrossRef]
- Khodakarami, J.; Knight, I. Required and Current Thermal Conditions for Occupants in Iranian Hospitals. HVAC&R Res. 2008, 14, 175–193. [Google Scholar] [CrossRef]
- Yau, Y.H.; Chew, B.T. Thermal comfort study of hospital workers in Malaysia. Indoor Air 2009, 19, 500–510. [Google Scholar] [CrossRef]
- Pourshaghaghy, A.; Omidvari, M. Examination of thermal comfort in a hospital using PMV–PPD model. Appl. Ergon. 2012, 43, 1089–1095. [Google Scholar] [CrossRef]
- Azizpour, F.; Moghimi, S.; Lim, C.H.; Mat, S.; Salleh, E.; Sopian, K. A Thermal Comfort Investigation of a Facility Department of a Hospital in Hot-Humid Climate: Correlation between Objective and Subjective Measurements. Indoor Built Environ. 2012, 22, 836–845. [Google Scholar] [CrossRef]
- Azizpour, F.; Moghimi, F.S.; Lim, C.; Mat, S.; Zaharim, A.; Sopian, K. Thermal comfort assessment of large-scale hospitals in tropical climates: A case study of University Kebangsaan Malaysia Medical Centre (UKMMC). Energy Build. 2013, 64, 317–322. [Google Scholar] [CrossRef]
- Yau, Y.; Chew, B. Adaptive thermal comfort model for air-conditioned hospitals in Malaysia. Build. Serv. Eng. Res. Technol. 2013, 35, 117–138. [Google Scholar] [CrossRef]
- Khalid, W.; Zaki, S.A.; Rijal, H.B.; Yakub, F. Thermal comfort requirements for different occupants in Malaysian hospital in-patient wards. J. Adv. Res. Fluid Mech. Therm. Sci. 2018, 43, 128–140. [Google Scholar]
- Khalid, W.; Zaki, S.A.; Rijal, H.B.; Yakub, F. Investigation of comfort temperature and thermal adaptation for patients and visitors in Malaysian hospitals. Energy Build. 2018, 183, 484–499. [Google Scholar] [CrossRef]
- Wang, F.; Lee, M.; Cheng, T.; Law, Y. Field evaluation of thermal comfort and indoor environment quality for a hospital in a hot and humid climate. HVAC R Res. 2012, 18, 671–680. [Google Scholar]
- Sattayakorn, S.; Ichinose, M.; Sasaki, R. Clarifying thermal comfort of healthcare occupants in tropical region: A case of indoor environment in Thai hospitals. Energy Build. 2017, 149, 45–57. [Google Scholar] [CrossRef]
- Lawrernce, I.D.; Jayabal, S.; Thirumal, P. Indoor air quality investigations in hospital patient room. Int. J. Biomed. Eng. Technol. 2018, 27, 124. [Google Scholar] [CrossRef]
- Pirsaheb, M.; Sohrabi, Y.; Yarmohammadi, H. Assessment of Thermal Comfort in Hospital Wards of Kermanshah, Iran, based on the Standards. Indian, J. Public Health Res. Dev. 2017, 8, 357. [Google Scholar] [CrossRef]
- Azmoon, H.; Dehghan, H.; Akbari, J.; Souri, S. The Relationship between Thermal Comfort and Light Intensity with Sleep Quality and Eye Tiredness in Shift Work Nurses. J. Environ. Public Health 2013, 2013, 639184. [Google Scholar] [CrossRef]
- Mohammadyan, M.; Keyvani, S.; Bahrami, A.; Charati-Yazdani, J.; Nejad-Yousefi, R. Indoor and ambient air concentrations of respirable particles between two hospitals in Kashan (2014–2015). KAUMAS J. 2017, 21, 66–73. [Google Scholar]
- Shokri, S.; Nikpey, A.; Varyani, A.S. Evaluation of Hospital Wards Indoor Air Quality. J. Air Pollut. Health 2016, 1, 205–214. [Google Scholar]
- Haleem, A.M.; Al-Obaidy, A.H.M.; Haleem, S.M. Air Quality Assessment of Some Selected Hospitals within Baghdad City. Eng. Technol. J. 2019, 37, 59–63. [Google Scholar] [CrossRef]
- Luksamijarulkul, P.; Somjai, N.; Nankongnap, N.; Pataitiemthong, A.; Kongtip, P.; Woskie, S. Indoor air quality at different sites of a governmental hospital, Thailand. Nurs. Palliat. Care 2019, 4, 1–5. [Google Scholar] [CrossRef]
- Tungjai, A.; Kubaha, K. Indoor Air Quality Evaluation of Isolation Room for Hospital in Thailand. Energy Procedia 2017, 138, 858–863. [Google Scholar] [CrossRef]
- Chen, H.-W.; Chuang, C.-Y.; Lin, H.-T. Indoor Air Distribution of Nitrogen Dioxide and Ozone in Urban Hospitals. Bull. Environ. Contam. Toxicol. 2009, 83, 147–150. [Google Scholar] [CrossRef]
- Tang, C.-S.; Wan, G.-H. Air Quality Monitoring of the Post-Operative Recovery Room and Locations Surrounding Operating Theaters in a Medical Center in Taiwan. PLoS ONE 2013, 8, e61093. [Google Scholar] [CrossRef]
- Liu, M.-H.; Tung, T.-H.; Chung, F.-F.; Chuang, L.-C.; Wan, G.-H. High total volatile organic compounds pollution in a hospital dental department. Environ. Monit. Assess. 2017, 189, 571. [Google Scholar] [CrossRef]
- Sen, P.K.; Sen, P. Hospital Indoor Air Quality in Respect to Transmission of Infection. In Indoor Environmental Quality; Springer: Singapore, 2020; pp. 53–66. [Google Scholar] [CrossRef]
- Yulinawati, H.; Khairani, T.; Siami, L. Analysis of indoor and outdoor particulate (PM2.5) at a women and children’s hospital in West Jakarta. IOP Conf. Ser. Earth Environ. Sci. 2021, 737, 012067. [Google Scholar] [CrossRef]
- Lian, K.S.; Inangda, P.S.N.; Ramly, A. Sources of indoor air quality problem in a new hospital in Malaysia. In Proceedings of the IAQVEC 2007 Proceedings–6th International Conference on Indoor Air Quality, Ventilation and Energy Conservation in Buildings: Sustainable Built Environment, Sendai, Japan, 28–31 October 2007; Volume 2, pp. 367–370. [Google Scholar]
- El-Sharkawy, M.F.; Noweir, M.E.H. Indoor air quality levels in a University Hospital in the Eastern Province of Saudi Arabia. J. Fam. Community Med. 2014, 21, 39–47. [Google Scholar] [CrossRef]
- Yousef, B.A.A.; Elshareef, A.A.D.; Ibraheem, M.A.K.; Alsayed, S.S. Assessment of Indoor Air Quality In Medical Facilities In Sudan. Int. J. Sci. Technol. Res. 2013, 2, 92–95. [Google Scholar]
- Gizaw, Z.; Gebrehiwot, M.; Yenew, C. High bacterial load of indoor air in hospital wards: The case of University of Gondar teaching hospital, Northwest Ethiopia. Multidiscip. Respir. Med. 2016, 11, 24. [Google Scholar] [CrossRef]
- Ordinioha, B.; Emuren, K. Physico-chemical assessment of indoor air quality of a tertiary hospital in South–South Nigeria. Port Harcourt Med. J. 2017, 11, 21. [Google Scholar] [CrossRef]
- Ayodele, C.; Fakinle, B.; Jimoda, L.; Sonibare, J. Investigation on the ambient air quality in a hospital environment. Cogent Environ. Sci. 2016, 2, 1215281. [Google Scholar] [CrossRef]
- Gawili, H.; Bodabos, H.A.; Al-Awami, W.A.; Al-Gargouri, A.O.; Alhegazi, Y.F. Indoor Air Quality in Benghazi’s Hospitals and Its Impact among Patients. Asian J. Med. Health 2021, 39–52. [Google Scholar] [CrossRef]
- Quadros, M.E.; Lisboa, H.D.M.; De Oliveira, V.L.; Schirmer, W.N. Qualidade do ar em ambientes internos hospitalares: Estudo de caso e análise crítica dos padrões atuais. Eng. Sanit. Ambient. 2009, 14, 431–438. [Google Scholar] [CrossRef]
- Macedo, J.I.; Kubota, T.H.; Matsumoto, L.S.; Giordani, A.T.; Takayanagui, A.M.M.; Mendes, A.A.; Bertolini, D.A. Air quality in a hospital environment. WIT Trans. Built Environ. 2013, 134, 737–747. [Google Scholar] [CrossRef]
- Aljeesh, Y.; Al Madhoun, W.; Shamh, I.A.; Arcaya, M. Assessment of Indoor Air Quality in Neonatal Intensive Care Units in Government Hospitals in Gaza Strip. Palestine 2016, 6, 24–30. [Google Scholar]
- Zaman, S.U.; Yesmin, M.; Pavel, R.S.; Jeba, F.; Salam, A. Indoor air quality indicators and toxicity potential at the hospitals’ environment in Dhaka, Bangladesh. Environ. Sci. Pollut. Res. 2021, 28, 37727–37740. [Google Scholar] [CrossRef]
- Božić, J.; Ilić, P.; Ilić, S. Indoor Air Quality in the Hospital: The Influence of Heating, Ventilating and Conditioning Systems. Braz. Arch. Biol. Technol. 2019, 62. [Google Scholar] [CrossRef]
- Martínez, F.C.C. Empirical investigation of indoor environmental quality (IEQ) in a hospital building in Merida Yucatan, Mexico. Int. J. Eng. Technol. 2018, 7, 245–249. [Google Scholar] [CrossRef]
- Osman, M.; Ibrahim, H.; Yousef, F.; Elnasr, A.A.; Saeed, Y.; Hameed, A.A. A study on microbiological contamination on air quality in hospitals in Egypt. Indoor Built Environ. 2017, 27, 953–968. [Google Scholar] [CrossRef]
- Taushiba, A.; Dwivedi, S.; Zehra, F.; Shukla, P.N.; Lawrence, A.J. Assessment of indoor air quality and their inter-association in hospitals of northern India—A cross-sectional study. Air Qual. Atmos. Health 2023. [Google Scholar] [CrossRef]
- Udobang, P.C.; Aniekan Otumo, E. Texas Journal of Medical Science Assessment of Thermal Comfort in Hospital Rooms and Health Status of Patients. Peer Rev. Int. J. 2023. Available online: https://zienjournals.com (accessed on 10 April 2023).
- Alghamdi, W.; Neamatallah, A.A.; Alshamrani, M.M.; Al Mehmadi, F.; El-Saed, A. Distribution and the trend of airborne particles and bio-aerosol concentration in pediatric intensive care units with different ventilation setting at two hospitals in Riyadh, Saudi Arabia. J. Infect. Public Health 2023, 16, 588–595. [Google Scholar] [CrossRef]
- Asghar, K.; Ali, A.; Tabassum, A.; Nadeem, S.; Hakim, S.; Amin, M.; Raza, G.; Bashir, S.; Afshan, N.; Usman, N.; et al. Assessment of particulate matter (PM) in ambient air of different settings and its associated health risk in Haripur city, Pakistan. Braz. J. Biol. 2022, 84, e256190. [Google Scholar] [CrossRef]
- Banza, C.L.N.; Nawrot, T.S.; Haufroid, V.; Decrée, S.; De Putter, T.; Smolders, E.; Kabyla, B.I.; Luboya, O.N.; Ilunga, A.N.; Mutombo, A.M.; et al. High human exposure to cobalt and other metals in Katanga, a mining area of the Democratic Republic of Congo. Environ. Res. 2009, 109, 745–752. [Google Scholar] [CrossRef]
- Kurth, L.; Kolker, A.; Engle, M.; Geboy, N.; Hendryx, M.; Orem, W.; McCAWLEY, M.; Crosby, L.; Tatu, C.; Varonka, M.; et al. Atmospheric particulate matter in proximity to mountaintop coal mines: Sources and potential environmental and human health impacts. Environ. Geochem. Health 2014, 37, 529–544. [Google Scholar] [CrossRef]
- Hendryx, M.; Islam, M.S.; Dong, G.-H.; Paul, G. Air Pollution Emissions 2008–2018 from Australian Coal Mining: Implications for Public and Occupational Health. Int. J. Environ. Res. Public Health 2020, 17, 1570. [Google Scholar] [CrossRef]
- Mwaanga, P.; Silondwa, M.; Kasali, G.; Banda, P.M. Preliminary review of mine air pollution in Zambia. Heliyon 2019, 5, e02485. [Google Scholar] [CrossRef]
- Muimba-Kankolongo, A.; Nkulu, C.B.L.; Mwitwa, J.; Kampemba, F.M.; Nabuyanda, M.M. Impacts of Trace Metals Pollution of Water, Food Crops, and Ambient Air on Population Health in Zambia and the DR Congo. J. Environ. Public Health 2022, 2022, 4515115. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Articles that focused on the IAQ and thermal comfort in tropical hospital building indoor environments. | Articles focused on non-tropical countries. |
| Only articles that were written in English. | Duplicated articles in the databases. |
| Publications released from 2000–2023. | Articles that were not written in English. |
| Articles regarding the IC but not hospital buildings. | |
| Published before 2000. |
| References | Title | Year | Country | Environment | Findings |
|---|---|---|---|---|---|
| Yi-Tun Wang et al. [9] | Investigation on indoor air quality of public sites in Tainan area | 2011 | Taiwan | Hospital | Hospitals need air conditioning and CO2 control to maintain a healthy indoor environment. |
| Hualing Zhang [13] | Impact of Metabolism and clothing thermal resistance on inpatient thermal comfort | 2021 | China | The formulation of useful guidelines to facilitate the assessment and management of hospital ward thermal environments | |
| Ramaswamy et al. [30] | IAQ in Hospitals – Better Health through Indoor Air Quality Awareness | 2010 | Oman | Hospital | patients in a controlled environment generally have more rapid physical improvement than do those in an uncontrolled environment |
| Lan et al. [39] | Thermal comfort improvement of naturally ventilated patient wards in Singapore | 2017 | Singapore | Hospital | A tropical warm climate medical ward might employ passive ventilation methods. |
| Khodakarami and Nasrollahi [41] | Thermal comfort in hospitals—A literature review | 2012 | Iran | Hospital | The direct impact of the thermal comfort on health has not been studied. |
| Chow and Yang [43] | Performance of ventilation system in a non-standard operating room | 2003 | Hong Kong | Hospital | The airflow and other design aspects did not meet the specifications. |
| Hwang et al. [44] | Patient thermal comfort requirement for hospital environments in Taiwan | 2007 | Taiwan | Hospital | Patients preferred warmer temperatures to neutral temperatures. This contradicts the office field studies. |
| Nematchoua et al. [45] | Thermal comfort and comparison of some parameters coming from hospitals and shopping centres under natural ventilation: The case of Madagascar Island | 2017 | Madagascar | Hospital | Hospital thermal satisfaction, preferences, and comfort may differ by gender and health. |
| Nematchoua, Ricciardi and Buratti [46] | Statistical analysis of indoor parameters a subjective response of building occupants in a hot region of Indian ocean: A case of Madagascar Island | 2017 | Madagascar | Hospital | Thermal, humidity, and air movement feelings are similar in men and women. |
| Alfa and Öztürk [47] | Perceived indoor environmental quality of hospital wards and patients’ outcomes: A study of a general hospital, Minna, Nigeria | 2019 | Nigeria | Hospital | IEQ enhanced a ward’s well-being. Health satisfaction most positively affected by the IEQ. |
| el Hamid Attia, El Helw and Teamah [48] | Three-dimensional thermal comfort analysis for hospital operating room with the effect of door gradually opened: Part (II) effect on mean age of the air and predicted mean vote distribution | 2013 | Egypt | Hospital | Door opening disrupts the optimal thermal impression by creating hot and humid zones. |
| el Hamid Attia, El Helw and Teamah [49] | Three-dimensional thermal comfort analysis for hospital operating room with the effect of door gradually opened part (I) effect on velocity and temperature distributions | 2013 | Egypt | Hospital | Door opening negatively affects the thermal comfort. Thermal comfort is enhanced by the air curtain. |
| Tartarini, Cooper, and Fleming [50] | Thermal perceptions, preferences, and adaptive behaviours of occupants of nursing homes | 2018 | Australia | Elderly Centre | This study is likely to have practical implications for all the stakeholders in the aged care sector. The residents were more tolerant of temperature variations than staff or visitors. |
| Pedro Filipe et al. [51] | Thermal comfort applied in hospital environments | 2020 | Brazil | Hospital | Professionals and patients demanded adequate temperature conditions. Hospital productivity is inadequate. |
| Cheong and Chong [52] | Development and application of an indoor air quality audit to an air-conditioned building in Singapore | 2001 | Singapore | Hospital | Building air quality assessments showed that the ACMV system decreases pollutants. |
| Khodakarami and Knight [53] | Required and current thermal conditions for occupants in Iranian hospitals | 2008 | Iran | Hospital | The measurements of the hospital thermal comfort conditions were unsatisfactory. |
| Yau et al. [54] | Thermal comfort study of hospital workers in Malaysia | 2009 | Malaysia | Hospital | The tropical hospital thermal comfort temperature range may help services engineers save HVAC energy. |
| Pourshaghaghy and Omidvari [55] | Examination of thermal comfort in a hospital using PMV–PPD model | 2012 | Iran | Hospital | Men and women’s PMV values exceed the ISO’s acceptable range. |
| Azizpour et al. [56] | A thermal comfort investigation of a facility department of a hospital in hot–humid climate: Correlation between objective and subjective measurements | 2013 | Malaysia | Hospital | People in hot–humid climates prefered lower temperatures to neutral temperatures. |
| Azizpour et al. [57] | Thermal comfort assessment of large-scale hospitals in tropical climates: A case study of University Kebangsaan Malaysia Medical Centre (UKMMC) | 2013 | Malaysia | Hospital | Globally, the neutral temperature is higher than the preferred temperature. |
| Yau and Chew [58] | Adaptive thermal comfort model for air-conditioned hospitals in Malaysia | 2013 | Malaysia | Hospital | Tropical hospital adaptive thermal comfort model may save HVAC energy while preserving the thermal comfort. |
| Khalid et al. [59] | Thermal comfort requirements for different occupants in Malaysian hospital in-patient wards | 2018 | Malaysia | Hospital | Patients, visitors, and staff complained about overcooled rooms and nursing stations. |
| Khalid et al. [60] | Investigation of comfort temperature and thermal adaptation for patients and visitors in Malaysian hospitals | 2019 | Malaysia | Hospital | Higher temperatures improve patient comfort in the hospital. |
| Fujen Wang et al. [61] | Field evaluation of thermal comfort and indoor environment quality for a hospital in a hot and humid climate | 2012 | Taiwan | Hospital | The hospital residents prefer lower tropical temperatures. |
| Sattayakorn, Ichinose and Sasaki [62] | Clarifying thermal comfort of healthcare occupants in tropical region: A case of indoor environment in Thai hospitals | 2017 | Thailand | Hospital | Thermal sensitivity differs among the patients, visitors, and hospital personnel. |
| Lawrence, et al. [63] | Indoor air quality investigations in hospital patient room | 2018 | India | Hospital | Hospital patient room active ventilation systems provide thermal comfort indoor air. |
| Pirsaheb, et al. [64] | Assessment of thermal comfort in hospital wards of Kermanshah, Iran, based on the standards | 2017 | Iran | Hospital | None of the sites were within the acceptable temperature and humidity ranges. |
| Azmoon et al. [65] | The relationship between thermal comfort and light intensity with sleep quality and eye tiredness in shift work nurses | 2013 | India | Hospital | Defects in the thermal and light conditions and a lack of a managerial strategy for night shift work nurses are harmful to their physical and mental well-being. |
| Mohammadyan, et al. [66] | Indoor and ambient air concentrations of respirable particles between two hospitals in Kashan | 2016 | Iran | Hospital | WHO/EPA 24-h PM limits were exceeded. Air conditioning may improve the indoor air quality. |
| Sana et al. [67] | Evaluation of hospital wards indoor air quality: the particles concentration | 2016 | Iran | Hospital | Low air exchange and ventilation in hospitals can produce and spread airborne particles that cause hospital infections. |
| Azhar et al. [68] | Air quality assessment of some selected hospitals within Baghdad City | 2019 | Iraq | Hospital | Hospital IAQ is significantly affected by the surrounding environment. |
| Luksamijarulkul et al. [69] | Indoor air quality at different sites of a governmental hospital, Thailand | 2019 | Thailand | Elderly Centre | Bacteria in hospital air may affect patients and workers, particularly nurses. |
| Tungjai Kubaha. [70] | Indoor air quality evaluation of isolation room for hospital in Thailand | 2017 | Thailand | Hospital | The indoor air quality index showed moderate VOC, formaldehyde, PM2.5, and PM10 levels (IAQI). |
| Hong-Wen et al. [71] | Indoor air distribution of nitrogen dioxide and ozone in urban hospitals | 2009 | Taiwan | Hospital | Nitrogen dioxide, PM10, and traffic increased indoor pollution. |
| Chin-Sheng [72] | Air quality monitoring of the post-operative recovery room and locations surrounding operating theaters in a medical centre in Taiwan | 2013 | Taiwan | Hospital | Patients and staff need clean air in the post-operative recovery room. |
| Ming et al. [73] | High total volatile organic compounds pollution in a hospital dental department | 2017 | Taiwan | Hospital | PM10, PM2.5, PM1, and TVOCs were higher in hospitals. Hospital air quality needs attention. |
| Daniel et al. [63] | Indoor air quality investigations in hospital patient room | 2018 | India | Hospital | Predictions for the indoor–outdoor relationship for fresh air supply, temperature flow, and human load. |
| Kumar and Parijat [74] | Hospital indoor air quality in respect to transmission of infection | 2020 | India | Hospital | A hospital HVAC and IAQ regulating structure will enhance the IAQ. |
| H Yulinawati et al. [75] | Analysis of indoor and outdoor particulate (PM2.5) at a women and children’s hospital in West Jakarta | 2021 | Indonesia | Hospital | PM 2.5 levels were higher in hospitals. Thus, a hospital must control the indoor and outdoor PM2.5 concentrations to reduce health risks. |
| Khew et al. [76] | Sources of indoor air quality problem in a new hospital in Malaysia | 2007 | Malaysia | Hospital | Low-level air pollution affects respiratory and cardiovascular health. |
| Mahmoud F et al. [77] | Indoor air quality levels in a University Hospital in the Eastern Province of Saudi Arabia | 2014 | Saudi Arabia | Hospital | Particulate matter (PM 10 and TSP) exceeded the air quality guidelines. |
| Basharia, et al. [78] | Assessment of indoor air quality in medical facilities in Sudan | 2013 | Sudan | Hospital | In hospitals, the window and split units don’t provide adequate ventilation. |
| Zemichael Gizaw et al. [79] | High bacterial load of indoor air in hospital wards: the case of University of Gondar teaching hospital, Northwest Ethiopia | 2016 | Ethiopia | Hospital | Poor ventilation, waste management, temperature, and humidity increase the bacterial load. |
| K. Emuren, B. Ordinioha [80] | Physico-chemical assessment of indoor air quality of a tertiary hospital in South–South Nigeria | 2017 | Nigeria | Hospital | Hospital air pollutants were within the regulatory limits. |
| Ayodele et al. [81] | Investigation on the ambient air quality in a hospital environment | 2016 | Nigeria | Hospital | In the hospital airshed, human activities may degrade the air quality. |
| Hadir Gawili et al. [82] | Indoor air quality in Benghazi’s hospitals and its impact among patients | 2019 | Libya | Hospital | Hospital health was most affected by the temperature, humidity, PM, other chemical pollutants, and noise. |
| Quadros et al. [83] | Indoor air quality in hospitals: A case study and a critical review of current standards | 2009 | Brazil | Hospital | Chemical pollution from cleaning can affect the air quality in hospitals. |
| Macedo et al. [84] | Air quality in a hospital environment | 2013 | Brazil | Hospital | The hallways and NICU have a wide variety of fungi. |
| Yousef et al. [85] | Assessment of indoor air quality in neonatal intensive care units in government hospitals in Gaza Strip, Palestine | 2016 | Palestine | Hospital | Hospital CO2 was higher than recommended. |
| Shahid Zaman et al. [86] | Indoor air quality indicators and toxicity potential at the hospitals’ environment in Dhaka, Bangladesh | 2021 | Bangladesh | Hospital | PM levels were lower indoors than outdoors, but gaseous pollutants were higher, except for NO2. |
| Božić et al. [87] | Indoor air quality in the hospital: The influence of heating, ventilating and conditioning systems | 2019 | Brazil | Hospital | Monitoring proves HVAC systems reduce microbiological contamination. |
| Cocom Martínez [88] | Empirical investigation of indoor environmental quality (IEQ) in a hospital building in Merida Yucatan, Mexico | 2018 | Mexico | Hospital | Hospitals needed cross ventilation in all interior rooms due to poor ventilation. |
| ME Osman [89] | A study on microbiological contamination on air quality in hospitals in Egypt | 2017 | Egypt | Hospital | Airborne germs and fungus in hospitals came from dust on air conditioning filters and floors. |
| Taushiba et al. [90] | Assessment of indoor air quality and their inter-association in hospitals of northern India—a cross-sectional study | 2023 | India | Hospital | The outdoor vehicular load, greenery, industries, etc., play a crucial role in maintaining the IAQ at an acceptable level. |
| Udobang and Otumo [91] | Assessment of thermal comfort in hospital rooms and health status of patients | 2023 | Nigeria/Ghana | Hospital | Thermal comfort can foster the healing process of the patients in hospitals. |
| Alghamdi et al. [92] | Distribution and the trend of airborne particles and bioaerosol concentration in pediatric intensive care units with different ventilation setting at two hospitals in Riyadh, Saudi Arabia | 2023 | Saudi Arabia | Hospital | Advanced filtration system and central HEPA filters play a significant role in the reduction in indoor fine particulates and TBC. |
| Lan et al. [39] | Thermal comfort improvement of naturally ventilated patient wards in Singapore | 2017 | Singapore | Hospital | Ventilation could be used effectively for a patient hospital ward, even in a tropical warm climate. |
| Continent | Country | No. Documents | Population (Millions) | CO2 Emissions (Metric Tons/Capita) | Average Annual Temp. | ||
|---|---|---|---|---|---|---|---|
| IAQ | ITC | 2015 | 2022 | 2019 | (°C) | ||
| AFRICA | Nigeria | 2 | 2 | 181.1 | 218.5 | 0.70 | 27.2 °C |
| Madagascar | 1 | 3 | 24.2 | 27.6 | 0.15 | 23 °C | |
| Ethiopia | 1 | 0 | 100.8 | 123.3 | 0.14 | 22.6 °C | |
| Egypt | 1 | 2 | 92.4 | 110.9 | 2.46 | 22.5 °C | |
| Libya | 1 | 0 | 6.4 | 6.8 | 6.85 | 22.6 °C | |
| Sudan | 1 | 0 | 38.9 | 46.8 | 0.54 | 27 °C | |
| Congo, DR. | 0 | 0 | 76.2 | 99.5 | 0.03 | 26.6 °C | |
| South Africa | 0 | 0 | 55.3 | 59.8 | 8.17 | 18.3 °C | |
| Chad | 0 | 0 | 14.1 | 17.7 | 0.06 | 27.4 °C | |
| Ghana | 0 | 1 | 28.8 | 32.8 | 13.9 | 27.2 °C | |
| Angola | 0 | 0 | 27.8 | 35.5 | 1.19 | 27 °C | |
| Mozambique | 0 | 0 | 27.0 | 32.9 | 0.29 | 24.3 °C | |
| AMERICA | Brazil | 3 | 2 | 204.4 | 215.3 | 2.21 | 25 °C |
| Mexico | 1 | 0 | 121.8 | 127.5 | 3.44 | 20.6 °C | |
| Venezuela | 0 | 0 | 28.3 | 30.3 | 4.09 | 24 °C | |
| Peru | 0 | 0 | 30.3 | 32.9 | 1.68 | 23.5 °C | |
| Colombia | 0 | 0 | 47.5 | 50.8 | 2.03 | 24 °C | |
| Bolivia | 0 | 0 | 10.8 | 11.6 | 1.96 | 20 °C | |
| Cuba | 0 | 0 | 8.3 | 11.3 | 2.29 | 25.2 °C | |
| ASIA | Malaysia | 1 | 6 | 31.5 | 33,9 | 7.83 | 25.4 °C |
| Taiwan | 5 | 4 | 23.4 | 27.5 | 11.05 | 22 °C | |
| India | 4 | 1 | 1.310 | 1.417 | 1.91 | 25 °C | |
| Thailand | 3 | 1 | 68.7 | 69.7 | 4.14 | 26.3 °C | |
| Iran | 3 | 3 | 78.4 | 83.9 | 9.40 | 22 °C | |
| Singapore | 2 | 2 | 5.5 | 5.8 | 6.71 | 26.7 °C | |
| Indonesia | 1 | 0 | 258.3 | 275.5 | 2.28 | 26.5 °C | |
| Iraq | 1 | 0 | 35.5 | 40.2 | 5.63 | 22.6 °C | |
| Saudi Arabia | 2 | 0 | 31.7 | 34.8 | 16.99 | 26.2 °C | |
| Hong Kong | 1 | 0 | 7.2 | 7.5 | 7.5 | 22.6 °C | |
| Philippines | 0 | 0 | 102.1 | 109.5 | 1.33 | 26 °C | |
| Palestine | 1 | 0 | 4.2 | 5.1 | 0.66 | 19.6 °C | |
| Bangladesh | 1 | 0 | 156.2 | 164.6 | 0.63 | 26.1° C | |
| OCEANIA | Australia | 1 | 1 | 23.8 | 26.1 | 16.31 | 22.1° C |
| Solomon Islands | 0 | 0 | 0.6 | 0.7 | 7.64 | 25.65 °C | |
| Papua New Guinea | 0 | 0 | 8.1 | 8.9 | 0.81 | 25 °C | |
| Fiji | 0 | 0 | 0.9 | 0.9 | 2.54 | 24.4 °C | |
| New Caledonia | 0 | 0 | 0.3 | 0.3 | 8.53 | 27.0 °C | |
| French Polynesia | 0 | 0 | 0.3 | 0.3 | 2.98 | 26.1 °C | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nyembwe, J.-P.K.B.; Ogundiran, J.O.; Chenari, B.; Simões, N.A.V.; Gameiro da Silva, M. The Indoor Climate of Hospitals in Tropical Countries: A Systematic Review. Energies 2023, 16, 3513. https://doi.org/10.3390/en16083513
Nyembwe J-PKB, Ogundiran JO, Chenari B, Simões NAV, Gameiro da Silva M. The Indoor Climate of Hospitals in Tropical Countries: A Systematic Review. Energies. 2023; 16(8):3513. https://doi.org/10.3390/en16083513
Chicago/Turabian StyleNyembwe, Jean-Paul Kapuya Bulaba, John Omomoluwa Ogundiran, Behrang Chenari, Nuno Albino Vieira Simões, and Manuel Gameiro da Silva. 2023. "The Indoor Climate of Hospitals in Tropical Countries: A Systematic Review" Energies 16, no. 8: 3513. https://doi.org/10.3390/en16083513
APA StyleNyembwe, J. -P. K. B., Ogundiran, J. O., Chenari, B., Simões, N. A. V., & Gameiro da Silva, M. (2023). The Indoor Climate of Hospitals in Tropical Countries: A Systematic Review. Energies, 16(8), 3513. https://doi.org/10.3390/en16083513