
Persistence of SARS-CoV-2-Specific Antibodies for 13 Months after Infection

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort and Sample Collection
2.2. Statistical Analysis
2.3. Laboratory Testing of Blood Specimens
3. Results
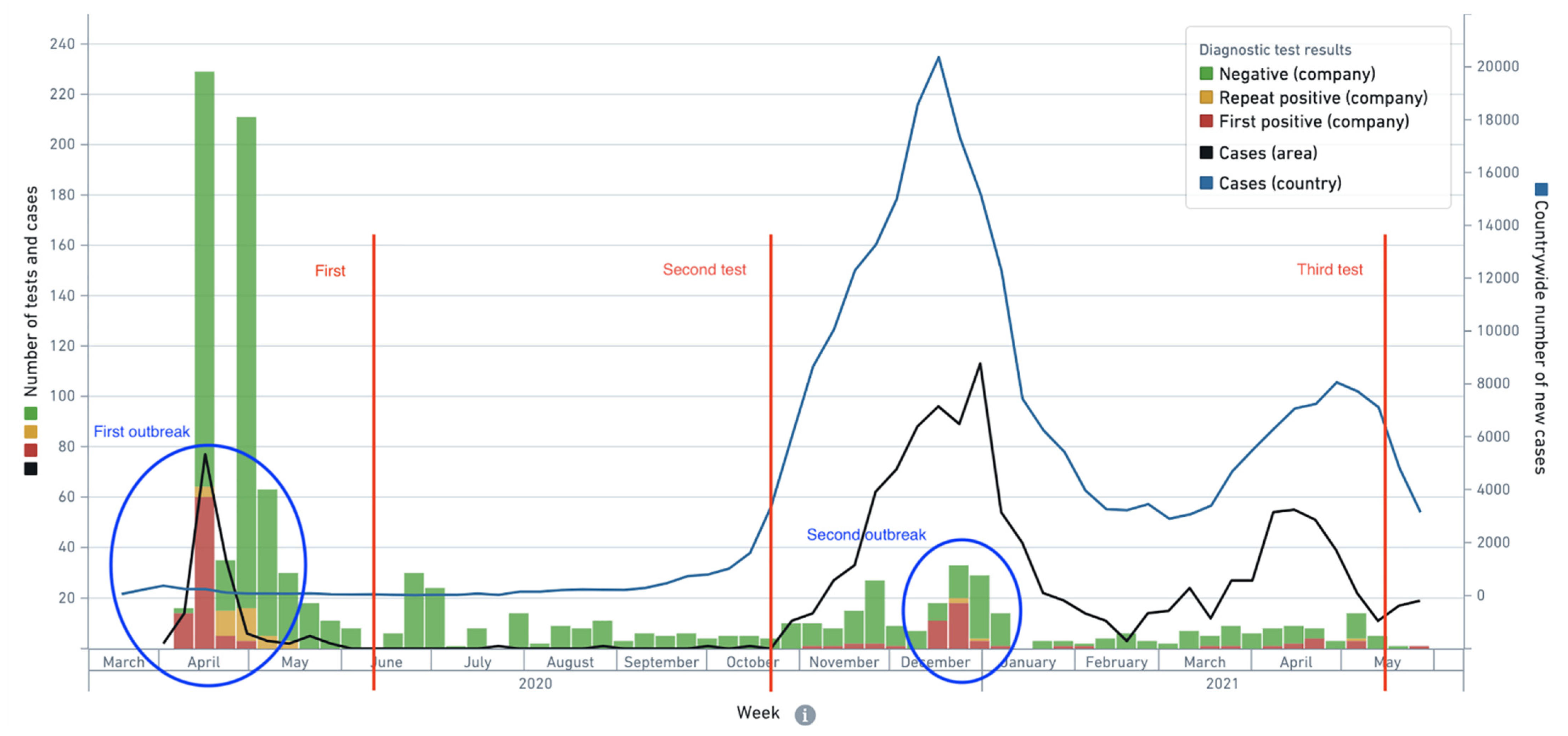
3.1. Epidemiological Context
3.2. Characterization of the Study Cohort
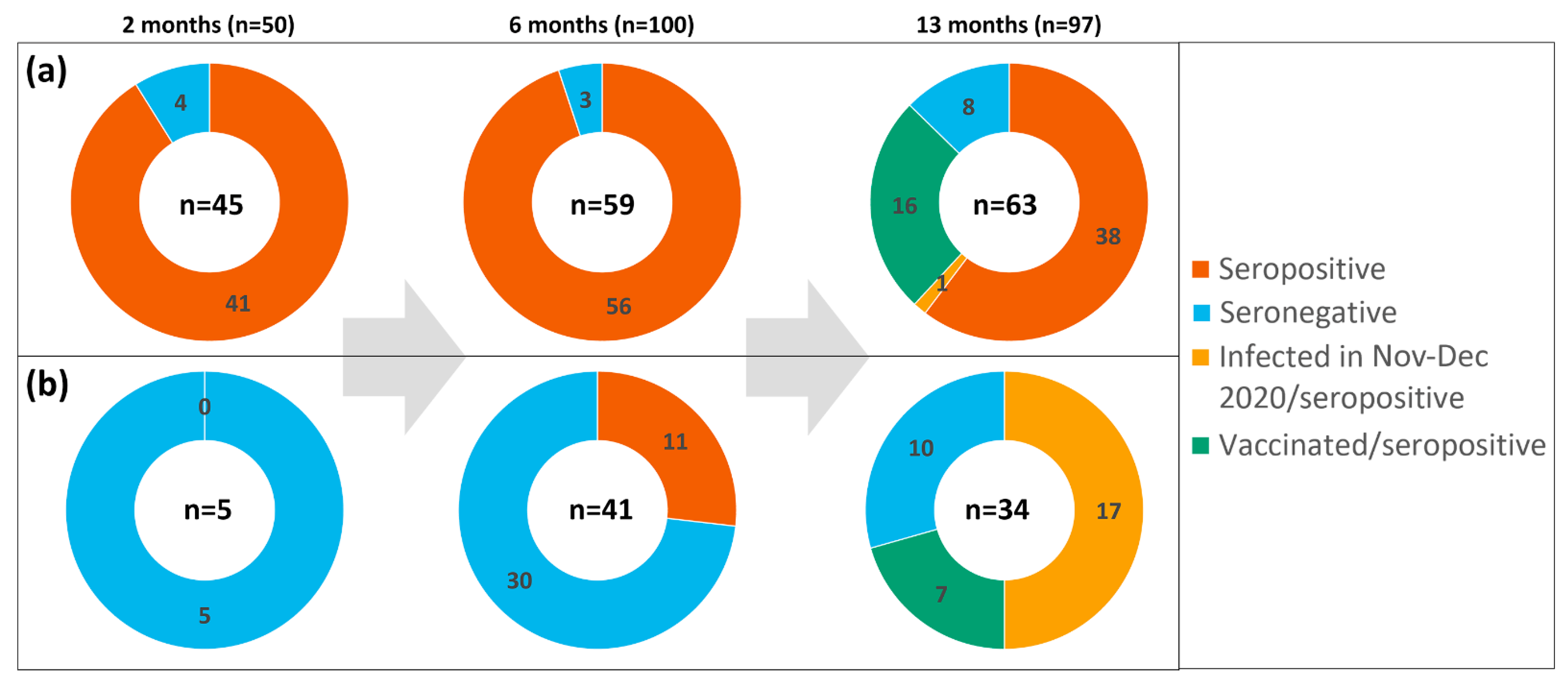
3.3. Seropositivity Pattern 2 Months after the Outbreak
3.4. Seropositivity Pattern 6 Months after the Outbreak
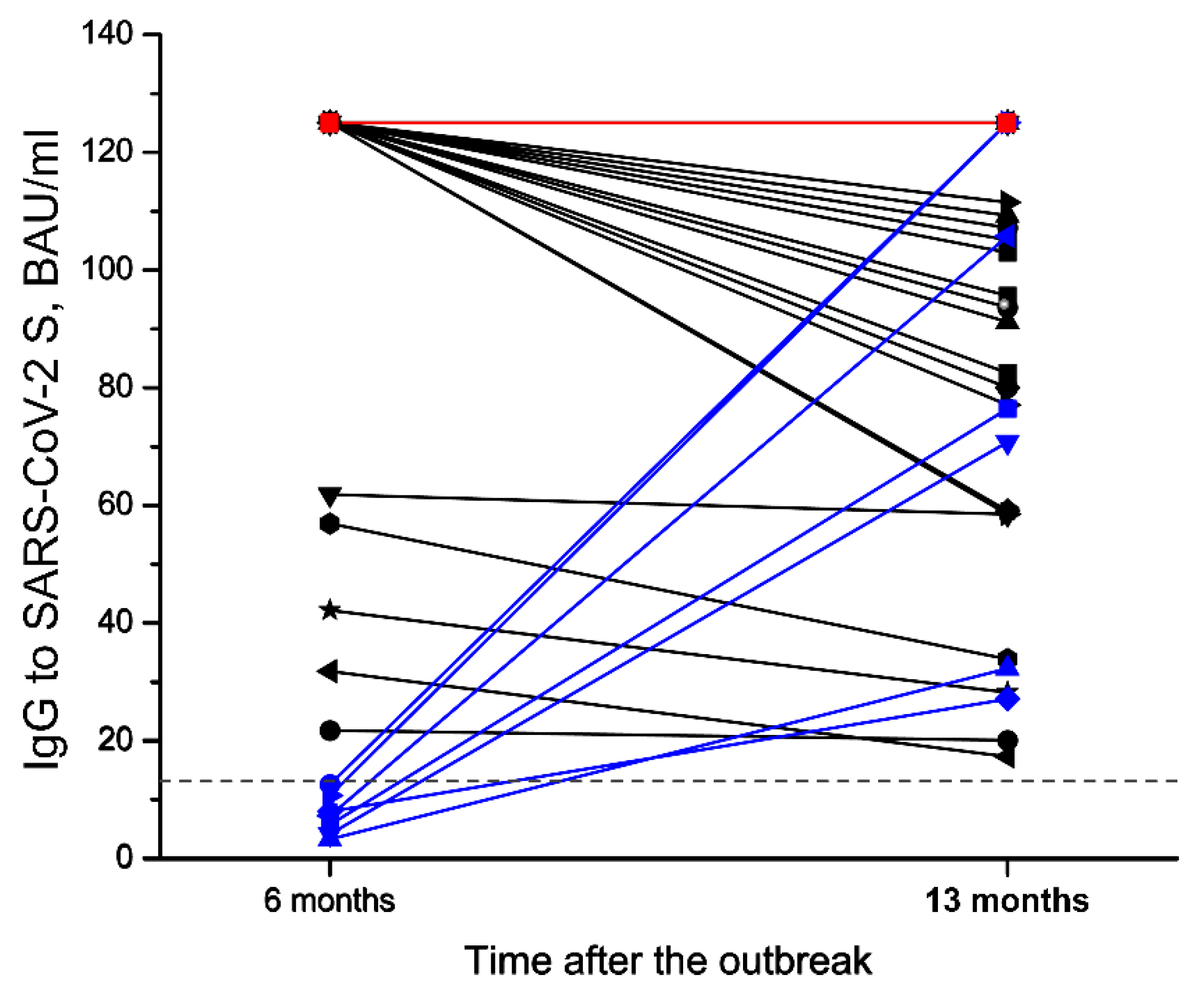
3.5. Seropositivity Pattern 13 Months after the Outbreak
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Xiao, A.T.; Gao, C.; Zhang, S. Profile of specific antibodies to SARS-CoV-2: The first report. J. Infect. 2020, 81, 147–178. [Google Scholar] [CrossRef]
- Beaudoin-Bussières, G.; Laumaea, A.; Anand, S.P.; Prévost, J.; Gasser, R.; Goyette, G.; Medjahed, H.; Perreault, J.; Tremblay, T.; Lewin, A.; et al. Decline of humoral responses against SARS-CoV-2 spike in convalescent individuals. MBio 2020, 11, e02590–e02620. [Google Scholar] [CrossRef] [PubMed]
- Peeling, R.W.; Wedderburn, C.J.; Garcia, P.J.; Boeras, D.; Fongwen, N.; Nkengasong, J.; Sall, A.; Tanuri, A.; Heymann, D.L. Serology testing in the COVID-19 pandemic response. Lancet Infect. Dis. 2020, 20, e245–e249. [Google Scholar] [CrossRef]
- Long, Q.-X.; Liu, B.-Z.; Deng, H.-J.; Wu, G.-C.; Deng, K.; Chen, Y.-K.; Liao, P.; Qiu, J.-F.; Lin, Y.; Cai, X.-F.; et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat. Med. 2020, 26, 845–848. [Google Scholar] [CrossRef]
- Iyer, A.S.; Jones, F.K.; Nodoushani, A.; Kelly, M.; Becker, M.; Slater, D.; Mills, R.; Teng, E.; Kamruzzaman, M.; Garcia-Beltran, W.F.; et al. Persistence and decay of human antibody responses to the receptor binding domain of SARS-CoV-2 spike protein in COVID-19 patients. Sci. Immunol. 2020, 5, eabe0367. [Google Scholar] [CrossRef] [PubMed]
- Röltgen, K.; Powell, A.E.; Wirz, O.F.; Stevens, B.A.; Hogan, C.A.; Najeeb, J.; Hunter, M.; Wang, H.; Sahoo, M.K.; Huang, C.H.; et al. Defining the features and duration of antibody responses to SARS-CoV-2 infection associated with disease severity and outcome. Sci. Immunol. 2020, 5, eabe0240. [Google Scholar] [CrossRef]
- Crawford, K.H.D.; Dingens, A.S.; Eguia, R.; Wolf, C.R.; Wilcox, N.; Logue, J.K.; Shuey, K.; Casto, A.M.; Fiala, B.; Wrenn, S.; et al. Dynamics of Neutralizing Antibody Titers in the Months After Severe Acute Respiratory Syndrome Coronavirus 2 Infection. J. Infect. Dis. 2021, 223, 197–205. [Google Scholar] [CrossRef]
- Isho, B.; Abe, K.T.; Zuo, M.; Jamal, A.J.; Rathod, B.; Wang, J.H.; Li, Z.; Chao, G.; Rojas, O.L.; Bang, Y.M.; et al. Persistence of serum and saliva antibody responses to SARS-CoV-2 spike antigens in COVID-19 patients. Sci. Immunol. 2020, 5, eabe5511. [Google Scholar] [CrossRef]
- Wang, H.; Yuan, Y.; Xiao, M.; Chen, L.; Zhao, Y.; Zhang, H.; Long, P.; Zhou, Y.; Xu, X.; Lei, Y.; et al. Dynamics of the SARS-CoV-2 antibody response up to 10 months after infection. Cell. Mol. Immunol. 2021, 18, 1832–1834. [Google Scholar] [CrossRef]
- Wang, K.; Long, Q.-X.; Deng, H.-J.; Hu, J.; Gao, Q.-Z.; Zhang, G.-J.; He, C.-L.; Huang, L.-Y.; Hu, J.-L.; Chen, J.; et al. Longitudinal Dynamics of the Neutralizing Antibody Response to Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection. Clin. Infect. Dis. 2020, 73, e531–e539. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Yu, X.; Gao, C.; Zhang, L.; Zhai, H.; Hu, Y.; Liu, E.; Wang, Q.; Gao, Y.; Wei, D.; et al. Characterization of antibody responses to SARS-CoV-2 in convalescent COVID-19 patients. J. Med. Virol. 2021, 93, 2227–2233. [Google Scholar] [CrossRef]
- Feng, C.; Shi, J.; Fan, Q.; Wang, Y.; Huang, H.; Chen, F.; Tang, G.; Li, Y.; Li, P.; Li, J.; et al. Protective humoral and cellular immune responses to SARS-CoV-2 persist up to 1 year after recovery. Nat. Commun. 2021, 12, 4984. [Google Scholar] [CrossRef]
- Gallais, F.; Gantner, P.; Bruel, T.; Velay, A.; Planas, D.; Wendling, M.-J.; Bayer, S.; Solis, M.; Laugel, E.; Reix, N.; et al. Evolution of antibody responses up to 13 months after SARS-CoV-2 infection and risk of reinfection. EBioMedicine 2021, 71, 103561. [Google Scholar] [CrossRef]
- Lumley, S.F.; Wei, J.; O’Donnell, D.; Stoesser, N.E.; Matthews, P.C.; Howarth, A.; Hatch, S.B.; Marsden, B.D.; Cox, S.; James, T.; et al. The Duration, Dynamics, and Determinants of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Antibody Responses in Individual Healthcare Workers. Clin. Infect. Dis. 2021, 73, e699–e709. [Google Scholar] [CrossRef]
- Petersen, M.S.; Hansen, C.B.; Kristiansen, M.F.; Fjallsbak, J.P.; Larsen, S.; Hansen, J.L.; Jarlhelt, I.; Pérez-Alós, L.; á Steig, B.; Christiansen, D.H.; et al. SARS-CoV-2 Natural Antibody Response Persists for at Least 12 Months in a Nationwide Study From the Faroe Islands. Open Forum Infect. Dis. 2021, 8, ofab378. [Google Scholar] [CrossRef]
- Varona, J.F.; Madurga, R.; Peñalver, F.; Abarca, E.; Almirall, C.; Cruz, M.; Ramos, E.; Castellano-Vazquez, J.M. Kinetics of anti-SARS-CoV-2 antibodies over time. Results of 10 month follow up in over 300 seropositive Health Care Workers. Eur. J. Intern. Med. 2021, 89, 97–103. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef]
- Anand, S.P.; Prévost, J.; Nayrac, M.; Beaudoin-Bussières, G.; Benlarbi, M.; Gasser, R.; Brassard, N.; Laumaea, A.; Gong, S.Y.; Bourassa, C.; et al. Longitudinal analysis of humoral immunity against SARS-CoV-2 Spike in convalescent individuals up to 8 months post-symptom onset. Cell Rep. Med. 2021, 2, 100290. [Google Scholar] [CrossRef]
- Duysburgh, E.; Mortgat, L.; Barbezange, C.; Dierick, K.; Fischer, N.; Heyndrickx, L.; Hutse, V.; Thomas, I.; Van Gucht, S.; Vuylsteke, B.; et al. Persistence of IgG response to SARS-CoV-2. Lancet Infect. Dis. 2021, 21, 163–164. [Google Scholar] [CrossRef]
- Choudhry, N.; Drysdale, K.; Usai, C.; Leighton, D.; Sonagara, V.; Buchanan, R.; Nijjar, M.; Thomas, S.; Hopkins, M.; Cutino-Moguel, T.; et al. Disparities of SARS-CoV-2 Nucleoprotein-Specific IgG in Healthcare Workers in East London, UK. Front. Med. 2021, 8, 642723. [Google Scholar] [CrossRef]
- Wisnivesky, J.P.; Stone, K.; Bagiella, E.; Doernberg, M.; Mendu, D.R.; Lin, J.J.; Kale, M. Long-term Persistence of Neutralizing Antibodies to SARS-CoV-2 Following Infection. J. Gen. Intern. Med. 2021, 36, 3289–3291. [Google Scholar] [CrossRef]
- Stringhini, S.; Zaballa, M.-E.; Pullen, N.; de Mestral, C.; Perez-Saez, J.; Dumont, R.; Picazio, A.; Pennacchio, F.; Dibner, Y.; Yerly, S.; et al. Large variation in anti-SARS-CoV-2 antibody prevalence among essential workers in Geneva, Switzerland. Nat. Commun. 2021, 12, 3455. [Google Scholar] [CrossRef] [PubMed]
- Mattiuzzo, G.; Bentley, E.M.; Hassall, M.; Routley, S.; Richardson, S.; Bernasconi, V.; Kristiansen, P.; Harvala, H.; Roberts, D.; Semple, M.G.; et al. Establishment of the WHO International Standard and Reference Panel for anti-SARS-CoV-2 antibody on behalf of the ISARIC4C Investigators. In Proceedings of the Expert Committee On Biological Standardization, Geneva, Switzerland, 9–10 December 2020. [Google Scholar]
- Seow, J.; Graham, C.; Merrick, B.; Acors, S.; Pickering, S.; Steel, K.J.A.; Hemmings, O.; O’Byrne, A.; Kouphou, N.; Galao, R.P.; et al. Longitudinal observation and decline of neutralizing antibody responses in the three months following SARS-CoV-2 infection in humans. Nat. Microbiol. 2020, 5, 1598–1607. [Google Scholar] [CrossRef]
- Wajnberg, A.; Amanat, F.; Firpo, A.; Altman, D.R.; Bailey, M.J.; Mansour, M.; McMahon, M.; Meade, P.; Mendu, D.R.; Muellers, K.; et al. Robust neutralizing antibodies to SARS-CoV-2 infection persist for months. Science 2020, 370, 1227. [Google Scholar] [CrossRef]
- Horton, D.B.; Barrett, E.S.; Roy, J.; Gennaro, M.L.; Andrews, T.; Greenberg, P.; Bruiners, N.; Datta, P.; Ukey, R.; Velusamy, S.K.; et al. Determinants and Dynamics of SARS-CoV-2 Infection in a Diverse Population: 6-Month Evaluation of a Prospective Cohort Study. J. Infect. Dis. 2021, 224, 1345–1356. [Google Scholar] [CrossRef] [PubMed]
- Robertson, L.J.; Moore, J.S.; Blighe, K.; Ng, K.Y.; Quinn, N.; Jennings, F.; Warnock, G.; Sharpe, P.; Clarke, M.; Maguire, K.; et al. Evaluation of the IgG antibody response to SARS-CoV-2 infection and performance of a lateral flow immunoassay: Cross-sectional and longitudinal analysis over 11 months. BMJ Open 2021, 11, e048142. [Google Scholar] [CrossRef]
- Sarantopoulos, A.; Brown, D.; Wiedermann, U.; Dominguez, C.A.; Bogdan, C.; Gürsel, İ.; Janković, S.; LeClerc, C.; Locati, M.; Spurkland, A.; et al. The EFIS vaccination task force expert report. Eur. J. Immunol. 2021, 51, 1023–1027. [Google Scholar] [CrossRef]
- The Use of Antibody Tests for SARS-COV-2 in the Context of Digital Green Certificates. Available online: https://www.ecdc.europa.eu/en/publications-data/use-antibody-tests-sars-cov-2-context-digital-green-certificates (accessed on 30 September 2021).
- Jiang, X.L.; Wang, G.L.; Zhao, X.N.; Yan, F.H.; Yao, L.; Kou, Z.Q.; Ji, S.X.; Zhang, X.L.; Li, C.B.; Duan, L.J.; et al. Lasting antibody and T cell responses to SARS-CoV-2 in COVID-19 patients three months after infection. Nat. Commun. 2021, 12, 897. [Google Scholar] [CrossRef]
- Secchi, M.; Bazzigaluppi, E.; Brigatti, C.; Marzinotto, I.; Tresoldi, C.; Rovere-Querini, P.; Poli, A.; Castagna, A.; Scarlatti, G.; Zangrillo, A.; et al. COVID-19 survival associates with the immunoglobulin response to the SARS-CoV-2 spike receptor binding domain. J. Clin. Investig. 2020, 130, 6366–6378. [Google Scholar] [CrossRef]
- Gaebler, C.; Wang, Z.; Lorenzi, J.C.C.; Muecksch, F.; Finkin, S.; Tokuyama, M.; Cho, A.; Jankovic, M.; Schaefer-Babajew, D.; Oliveira, T.Y.; et al. Evolution of antibody immunity to SARS-CoV-2. Nature 2021, 591, 639–644. [Google Scholar] [CrossRef]
- Ibarrondo, F.J.; Fulcher, J.A.; Goodman-Meza, D.; Elliott, J.; Hofmann, C.; Hausner, M.A.; Ferbas, K.G.; Tobin, N.H.; Aldrovandi, G.M.; Yang, O.O. Rapid Decay of Anti–SARS-CoV-2 Antibodies in Persons with Mild COVID-19. Engl. J. Med. 2020, 383, 1085–1087. [Google Scholar] [CrossRef]
- Ward, H.; Cooke, G.; Atchison, C.; Whitaker, M.; Elliott, J.; Moshe, M.; Brown, J.C.; Flower, B.; Daunt, A.; Ainslie, K.; et al. Declining prevalence of antibody positivity to SARS-CoV-2: A community study of 365,000 adults. medRxiv 2020. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Gadi, N.; Wu, S.C.; Spihlman, A.P.; Moulton, V.R. What’s Sex Got to Do With COVID-19? Gender-Based Differences in the Host Immune Response to Coronaviruses. Front. Immunol. 2020, 11, 2147. [Google Scholar] [CrossRef] [PubMed]
- Zeng, F.; Dai, C.; Cai, P.; Wang, J.; Xu, L.; Li, J.; Hu, G.; Wang, Z.; Zheng, F.; Wang, L. A comparison study of SARS-CoV-2 IgG antibody between male and female COVID-19 patients: A possible reason underlying different outcome between sex. J. Med. Virol. 2020, 92, 2050–2054. [Google Scholar] [CrossRef]
- Grzelak, L.; Velay, A.; Madec, Y.; Gallais, F.; Staropoli, I.; Schmidt-Mutter, C.; Wendling, M.J.; Meyer, N.; Planchais, C.; Rey, D.; et al. Sex Differences in the Evolution of Neutralizing Antibodies to Severe Acute Respiratory Syndrome Coronavirus 2. J. Infect. Dis. 2021, 224, 983–988. [Google Scholar] [CrossRef]
- Takahashi, T.; Ellingson, M.K.; Wong, P.; Israelow, B.; Lucas, C.; Klein, J.; Silva, J.; Mao, T.; Oh, J.E.; Tokuyama, M.; et al. Sex differences in immune responses that underlie COVID-19 disease outcomes. Nature 2020, 588, 315–320. [Google Scholar] [CrossRef]
- Zeng, F.; Wu, M.; Wang, J.; Li, J.; Hu, G.; Wang, L. Over 1-year duration and age difference of SARS-CoV-2 antibodies in convalescent COVID-19 patients. J. Med. Virol. 2021, 93, 6506–6511. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.; Waight, P.A.; Andrews, N.J.; McOwat, K.; Brown, K.E.; Höschler, K.; Ijaz, S.; Letley, L.; Haskins, D.; Sinnathamby, M.; et al. Transmission of SARS-CoV-2 in the household setting: A prospective cohort study in children and adults in England. J. Infect. 2021, 83, 483–489. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Testing Date | Sample Size | Age of Study Participants | % of Female Participants | ||||
|---|---|---|---|---|---|---|---|
| Mean Age | SD | Median Age | IQR | Range (Years) | |||
| 17 June 2020 | 50 | 45.0 | 10.8 | 46 | 40–53 | 18–65 | 89.66 |
| 20 October 2020 | 100 | 45.1 | 10.8 | 46 | 40–53 | 18–65 | 88.89 |
| 12 May 2021 | 97 | 46.1 | 10.8 | 47 | 41–54 | 18–66 | 83.50 |
| The Results of SARS-CoV-2-Specific RT-PCR Test at the Time of the Outbreak (April 2020) | ||||||
|---|---|---|---|---|---|---|
| Negative | Positive | |||||
| Classification of Symptoms | None | None | Very Mild | Mild | Moderate | Severe |
| Group Size | n = 5 | n = 12 | n = 13 | n = 9 | n = 8 | n = 3 |
| Only IgG+ | 0 | 4 | 8 | 3 | 3 | 1 |
| Only IgM+ | 0 | 0 | 0 | 0 | 0 | 0 |
| IgG+/IgM+ | 0 | 5 | 5 | 5 | 5 | 2 |
| IgG−/IgM− | 5 | 3 | 0 | 1 | 0 | 0 |
| The number of seropositive individuals | 0 | 9 | 13 | 8 | 8 | 3 |
| Seropositivity rate, % | 0 | 75 | 100 | 89 | 100 | 100 |
| Total number of participants of the second serologic testing | 100 |
| The number of participants with a previous * positive RT-PCR result | 59 |
| The number of participants with a previous * negative RT-PCR result | 41 |
| Among them, identified as seropositive | 11 |
| Among them, identified as seronegative | 30 |
| The number of seropositive participants | 67 |
| The number of seronegative participants | 33 |
| Seropositive with a previous * positive RT-PCR result | 56 |
| Self-reported asymptomatic infection | 11 |
| Self-reported mild or very mild symptoms | 33 |
| Self-reported moderate or severe symptoms | 12 |
| Seropositive with a previous * negative RT-PCR result | 11 |
| Both IgG+/IgM+ | 24 |
| Only IgM+ | 0 |
| Only IgG+ | 43 |
| The number of participants enrolled both into the first (2 months after the outbreak) and the second (6 months after the outbreak) serologic testing | 39 |
| Seronegative both in the first and the second serologic testing | 5 |
| Seropositive in the second serologic testing | 34 |
| Seropositive in the first serologic testing | 34 |
| Only IgM+ in the first serologic testing | 0 |
| Only IgG+ in the first serologic testing | 13 |
| From them, only IgG+ in the second serologic testing | 13 |
| Both IgG+/IgM+ in the first serologic testing | 21 |
| From them, both IgG+/IgM+ in the second serologic testing | 14 |
| From them, only IgG+ positive in the second serologic testing | 7 |
| Total Number of Participants of the Third Serologic Testing | 97 |
|---|---|
| The number of participants with a previous * negative RT-PCR result | 34 |
| No confirmed SARS-CoV-2 infection and vaccination record | 10 |
| Confirmed SARS-CoV-2 infection in November‒December 2020 | 17 |
| Vaccinated in April–May 2021 | 7 |
| The number of participants with a previous * positive RT-PCR result | 63 |
| Vaccinated in April–May 2021 | 16 |
| Non-vaccinated by the date of the third serologic testing | 47 |
| Confirmed SARS-CoV-2 infection in December 2020 | 1 |
| Seropositive | 38 |
| Seronegative | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kučinskaitė-Kodzė, I.; Simanavičius, M.; Šimaitis, A.; Žvirblienė, A. Persistence of SARS-CoV-2-Specific Antibodies for 13 Months after Infection. Viruses 2021, 13, 2313. https://doi.org/10.3390/v13112313
Kučinskaitė-Kodzė I, Simanavičius M, Šimaitis A, Žvirblienė A. Persistence of SARS-CoV-2-Specific Antibodies for 13 Months after Infection. Viruses. 2021; 13(11):2313. https://doi.org/10.3390/v13112313
Chicago/Turabian StyleKučinskaitė-Kodzė, Indrė, Martynas Simanavičius, Aistis Šimaitis, and Aurelija Žvirblienė. 2021. "Persistence of SARS-CoV-2-Specific Antibodies for 13 Months after Infection" Viruses 13, no. 11: 2313. https://doi.org/10.3390/v13112313
APA StyleKučinskaitė-Kodzė, I., Simanavičius, M., Šimaitis, A., & Žvirblienė, A. (2021). Persistence of SARS-CoV-2-Specific Antibodies for 13 Months after Infection. Viruses, 13(11), 2313. https://doi.org/10.3390/v13112313