
Elimination of Hepatitis C in Southern Italy: A Model of HCV Screening and Linkage to Care among Hospitalized Patients at Different Hospital Divisions

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
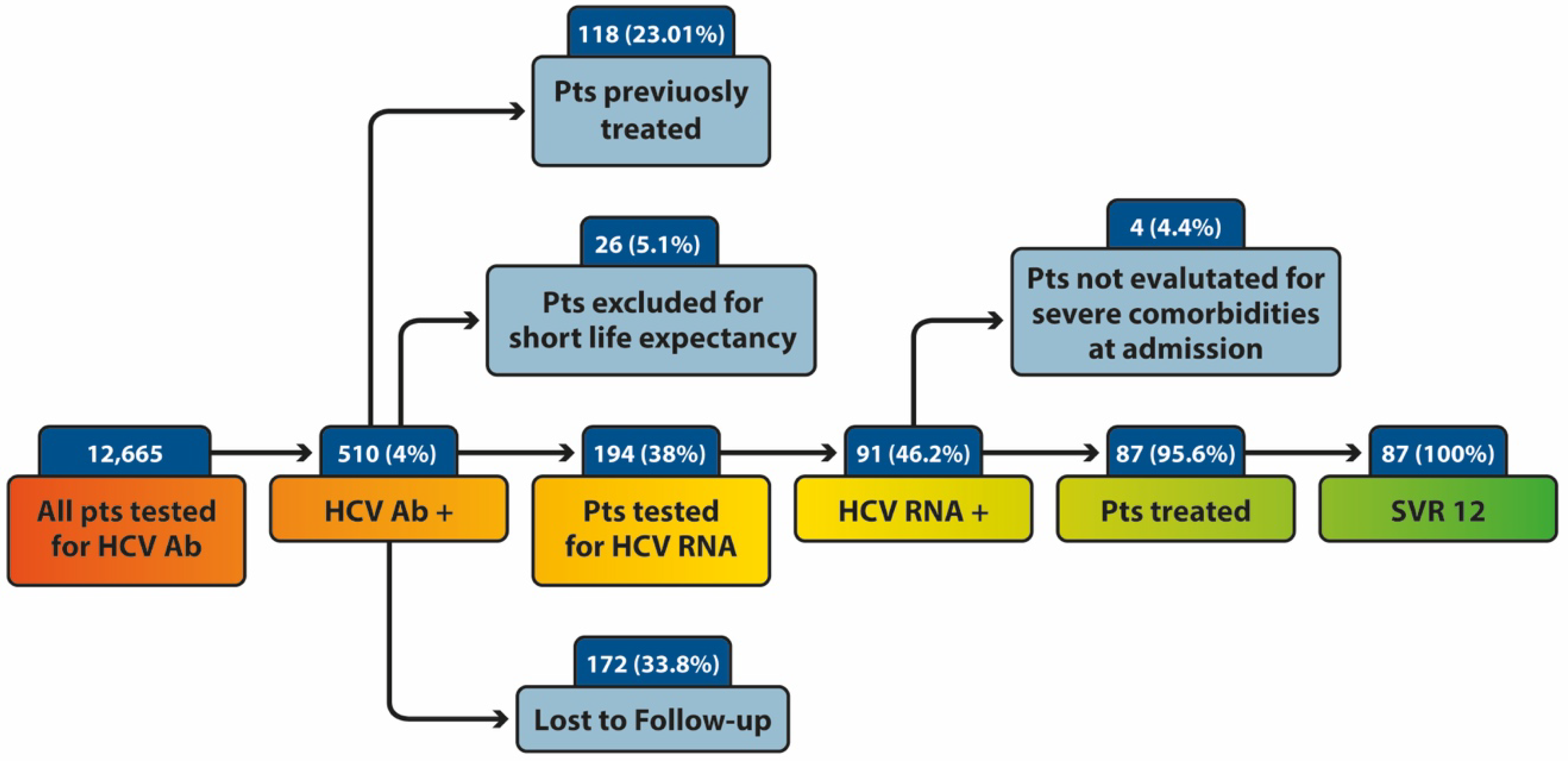
3.1. Study Population
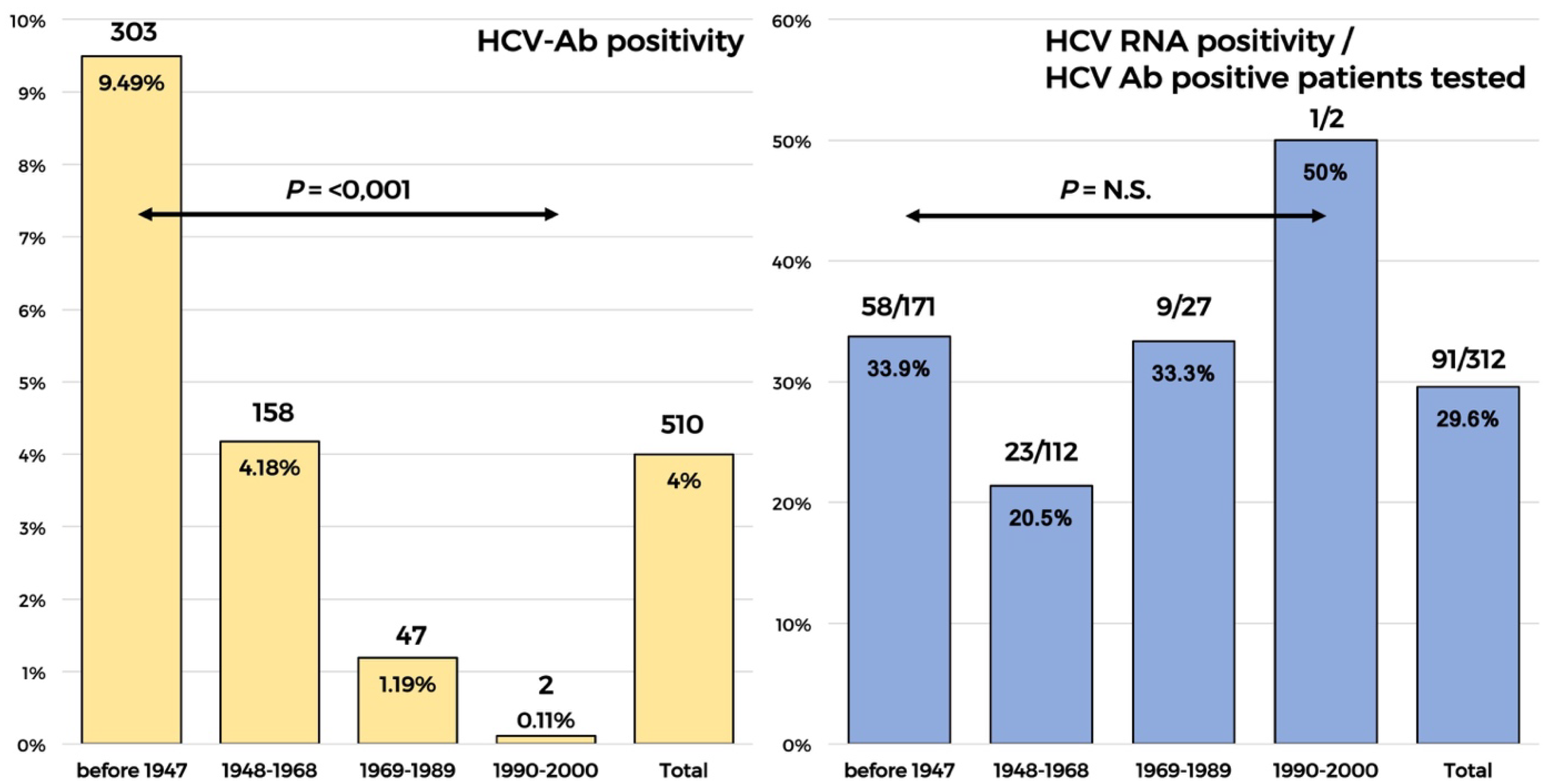
3.2. Rate of Infection among the Hospiral Divisions
3.3. Biochemical Characteristics of Patients with Active Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Polaris Observatory, Global change in hepatitis C virus prevalence and cascade of care between 2015 and 2020: A modelling study. Lancet Gastroenterol. Hepatol. 2022. [CrossRef]
- ec.europa.eu/eurostat. Available online: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/EDN-20190726-1 (accessed on 28 March 2022).
- aifa.gov.it. Available online: https://www.aifa.gov.it/documents/20142/847506/Aggiornamento_dati_Registri_AIFA_DAAs-28-03-2022.pdf (accessed on 28 March 2022).
- Kondili, L.A.; Robbins, S.; Blach, S.; Gamkrelidze, I.; Zignego, A.L.; Brunetto, M.R.; Raimondo, G.; Taliani, G.; Iannone, A.; Russo, F.P.; et al. Forecasting Hepatitis C liver disease burden on real-life data. Does the hidden iceberg matter to reach the elimination goals? Liver Int. 2018, 38, 2190–2198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondili, L.A.; Andreoni, M.; Alberti, A.; Lobello, S.; Babudieri, S.; Roscini, A.S.; Merolla, R.; Marrocco, W.; Craxi, A. Estimated prevalence of undiagnosed HCV infected individuals in Italy: A mathematical model by route of transmission and fibrosis progression. Epidemics 2021, 34, 100442. [Google Scholar] [CrossRef]
- Kondili, L.A.; Andreoni, M.; Alberti, A.; Lobello, S.; Babudieri, S.; De Michina, A.; Merolla, R.; Marrocco, W.; Craxi, A. A mathematical model by route of transmission and fibrosis progression to estimate undiagnosed individuals with HCV in different Italian regions. BMC Infect. Dis. 2022, 22, 58. [Google Scholar] [CrossRef]
- Morisco, F.; Loperto, I.; Stroffolini, T.; Lombardo, F.L.; Cossiga, V.; Guarino, M.; De Feo, A.; Caporaso, N. Prevalence and risk factors of HCV infection in a metropolitan area in southern Italy: Tail of a cohort infected in past decades. J. Med. Virol. 2017, 89, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Andriulli, A.; Stroffolini, T.; Mariano, A.; Valvano, M.R.; Grattagliano, I.; Ippolito, A.M.; Grossi, A.; Brancaccio, G.; Coco, C.; Russello, M.; et al. Declining prevalence and increasing awareness of HCV infection in Italy: A population-based survey in five metropolitan areas. Eur. J. Intern. Med. 2018, 53, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Kondili, L.A.; Gamkrelidze, I.; Blach, S.; Marcellusi, A.; Galli, M.; Petta, S.; Puoti, M.; Vella, S.; Razavi, H.; Craxi, A.; et al. Optimization of hepatitis C virus screening strategies by birth cohort in Italy. Liver Int. 2020, 40, 1545–1555. [Google Scholar] [CrossRef] [Green Version]
- Kondili, L.A.; Aghemo, A.; Andreoni, M.; Galli, M.; Rossi, A.; Babudieri, S.; Nava, F.; Leonardi, C.; Mennini, F.S.; Gardini, I.; et al. Milestones to reach Hepatitis C Virus (HCV) elimination in Italy: From free-of-charge screening to regional roadmaps for an HCV-free nation. Dig. Liver Dis. 2022, 54, 237–242. [Google Scholar] [CrossRef]
- Kondili, L.A.; Craxi, A.; Aghemo, A. Absolute targets for HCV elimination and national health policy paradigms: Foreseeing future requirements. Liver Int. 2021, 41, 649–655. [Google Scholar] [CrossRef]
- Ponziani, F.R.; Aghemo, A.; Cabibbo, G.; Masarone, M.; Montagnese, S.; Petta, S.; Russo, F.P.; Lai, Q.; The AISF COVID-19 Survey Group. Management of liver disease in Italy after one year of the SARS-CoV-2 pandemic: A web-based survey. Liver Int. 2021, 41, 2228–2232. [Google Scholar] [CrossRef]
- Coppola, C.; Masarone, M.; Bartoli, M.; Staiano, L.; Coppola, R.; Torre, P.; Conforti, M.; Amoruso, D.; Gardini, I.; Persico, M. Associated screening for HCV and SARS-Cov2 infection in an urban area of Southern Italy: A cohort study. J. Viral Hepat. 2022, 29, 171–173. [Google Scholar] [CrossRef] [PubMed]
- Giacomelli, A.; Pagani, G.; Conti, F.; Bassoli, C.; Galli, M. Detecting HCV infection by means of mass population SARS-CoV-2 screening: A pilot experience in Northern Italy. J. Hepatol. 2021, 75, 484–486. [Google Scholar] [CrossRef] [PubMed]
- Stroffolini, T.; Menchinelli, M.; Taliani, G.; Dambruoso, V.; Poliandri, G.; Bozza, A.; Lecce, R.; Clementi, C.; Ippolito, F.M.; Compagnoni, A.; et al. High prevalence of hepatitis C virus infection in a small central Italian town: Lack of evidence of parenteral exposure. Ital. J. Gastroenterol. 1995, 27, 235–238. [Google Scholar] [PubMed]
- Guadagnino, V.; Stroffolini, T.; Rapicetta, M.; Costantino, A.; Kondili, L.A.; Menniti-Ippolito, F.; Caroleo, B.; Costa, C.; Griffo, G.; Loiacono, L.; et al. Prevalence, risk factors, and genotype distribution of hepatitis C virus infection in the general population: A community-based survey in southern Italy. Hepatology 1997, 26, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, R.; Stroffolini, T.; Ferraro, D.; Usticano, A.; Valenza, L.M.; Montalbano, L.; Pomara, G.; Craxi, A. Endemic hepatitis C virus infection in a Sicilian town: Further evidence for iatrogenic transmission. J. Med. Virol. 2002, 67, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Piazzolla, A.V.; Paroni, G.; Bazzocchi, F.; Cassese, M.; Cisternino, A.; Ciuffreda, L.; Gorgoglione, F.; Gorgoglione, L.; Palazzo, V.; Scianname, N.; et al. High Rates of Hidden HCV Infections among Hospitalized Patients Aged 55-85. Pathogens 2021, 10, 695. [Google Scholar] [CrossRef] [PubMed]
- Minutolo, R.; Ravera, M.; Cupisti, A.; Nappi, F.; Mandreoli, M.; Soragna, G.; Ferraro, P.M.; Nicola, L. Prevalence of hepatitis C virus infection in non-dialysis CKD patients: A multicentre study in renal clinics. Nephrol. Dial. Transplant 2021, 36, 2348–2350. [Google Scholar] [CrossRef]
- Cammarota, S.; Citarella, A.; Guida, A.; Conti, V.; Iannaccone, T.; Flacco, M.E.; Bravi, F.; Naccarato, C.; Piscitelli, A.; Piscitelli, R.; et al. The inpatient hospital burden of comorbidities in HCV-infected patients: A population-based study in two Italian regions with high HCV endemicity (The BaCH study). PLoS ONE 2019, 14, e0219396. [Google Scholar] [CrossRef] [Green Version]
- Adinolfi, L.E.; Petta, S.; Fracanzani, A.L.; Coppola, C.; Narciso, V.; Nevola, R.; Rinaldi, L.; Calvaruso, V.; Staiano, L.; Di Marco, V.; et al. Impact of hepatitis C virus clearance by direct-acting antiviral treatment on the incidence of major cardiovascular events: A prospective multicentre study. Atherosclerosis 2020, 296, 40–47. [Google Scholar] [CrossRef] [Green Version]
- Deuffic-Burban, S.; Deltenre, P.; Buti, M.; Stroffolini, T.; Parkes, J.; Muhlberger, N.; Siebert, U.; Moreno, C.; Hatzakis, A.; Rosenberg, W.; et al. Predicted effects of treatment for HCV infection vary among European countries. Gastroenterology 2012, 143, 974–985. [Google Scholar] [CrossRef] [Green Version]
- Andreoni, M.; Giacometti, A.; Maida, I.; Meraviglia, P.; Ripamonti, D.; Sarmati, L. HIV-HCV co-infection: Epidemiology, pathogenesis and therapeutic implications. Eur. Rev. Med. Pharmacol. Sci 2012, 16, 1473–1483. [Google Scholar] [PubMed]
- SEIEVA (Sistema Epidemiologico Integrato dell’epatite Virale Acuta). Available online: https://www.epicentro.iss.it/epatite/seieva (accessed on 28 March 2022).
- Kondili, L.A.; Andreoni, M.; Mennini, F.S.; Razavi, H. Opportunistic co-screening for HCV and COVID-19-related services: A creative response with a need for thoughtful reflection. Liver Int. 2022; in press. [Google Scholar]
- Casas, M.P.; Garcia, F.; Freyre-Carrillo, C.; Montiel, N.; de la Iglesia, A.; Viciana, I.; Dominguez, A.; Guillot, V.; Munoz, A.; Cantudo, P.; et al. Towards the elimination of hepatitis C: Implementation of reflex testing in Andalusia. Rev. Esp. Enferm. Dig. 2020, 112, 515–519. [Google Scholar] [CrossRef] [PubMed]
- Evans, H.; Balasegaram, S.; Douthwaite, S.; Hunter, L.; Kulasegaram, R.; Wong, T.; Querol-Rubiera, A.; Nebbia, G. An innovative approach to increase viral hepatitis diagnoses and linkage to care using opt-out testing and an integrated care pathway in a London Emergency Department. PLoS ONE 2018, 13, e0198520. [Google Scholar] [CrossRef] [PubMed]
- Marcellusi, A.; Mennini, F.S.; Ruf, M.; Galli, C.; Aghemo, A.; Brunetto, M.R.; Babudieri, S.; Craxi, A.; Andreoni, M.; Kondili, L.A. Optimizing diagnostic algorithms to advance Hepatitis C elimination in Italy: A cost effectiveness evaluation. Liver Int. 2022, 42, 26–37. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age Groups | Cardiology | Gynecology Senology | Liver Unit | ICU | Medicine | Ophthalmology | Orthopedics | Surgery |
|---|---|---|---|---|---|---|---|---|
| Beyond 1990 | 0 | 0/1 (100) | 1/1 (100) | 0 | 0 | 0 | 0 | 0 |
| 1989–1969 | 0 | 0/3 (0) | 1/7 (14.2) | 1/2 (50) | 2/3 (66.6) | 0 | 2/4 (50) | 3/6 (50) |
| 1948–1968 | 2/7 (28.5) | 1/9 (11.1) | 10/39 (25.6) | 1/1 (100) | 2/10 (20) | 2/21 (9.5) | 4/11 (36.3) | 1/14 (7.1) |
| Before 1947 | 3/14 (21.4) | 3/8 (37.5) | 23/52 (44.2) | 3/9 (33.3) | 6/25 (24) | 6/33 (18.1) | 7/16 (43.7) | 7/15 (46.6) |
| Total | 5/21 (23.8) | 4/22 (18.1) | 35/99 (35.3) | 5/12 (41.6) | 10/38 (26.3) | 8/54 (14.8) | 13/31 (42) | 11/35 (31.4) |
| Other Hospital Divisions | Liver Unit | p-Value | |
|---|---|---|---|
| n | 56 | 35 | |
| Age (year) | 72 (±14) | 74 (±13) | 0.379 |
| male | 24 (42.8) | 21 (60) | 0.184 |
| ALT (U/L) | 35 (±34) | 153 (±595) | 0.385 |
| AST (U/L) | 45 (±58) | 119 (±300) | 0.016 |
| Increased transaminase values * | 25 (44.6) | 22 (62.8) | 0.056 |
| GGT (U/L) | 76 (±128) | 106 (±119) | 0.092 |
| Platelets (103/mL) | 182 (±77) | 151 (±77) | 0.033 |
| Bilirubin (mg/dL) | 0.79 (±1.85) | 2.29 (±4.47) | 0.003 |
| FIB-4 > 3.25 | 16 (28.5) | 23 (65.7) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosato, V.; Kondili, L.A.; Nevola, R.; Perillo, P.; Mastrocinque, D.; Aghemo, A.; Claar, E. Elimination of Hepatitis C in Southern Italy: A Model of HCV Screening and Linkage to Care among Hospitalized Patients at Different Hospital Divisions. Viruses 2022, 14, 1096. https://doi.org/10.3390/v14051096
Rosato V, Kondili LA, Nevola R, Perillo P, Mastrocinque D, Aghemo A, Claar E. Elimination of Hepatitis C in Southern Italy: A Model of HCV Screening and Linkage to Care among Hospitalized Patients at Different Hospital Divisions. Viruses. 2022; 14(5):1096. https://doi.org/10.3390/v14051096
Chicago/Turabian StyleRosato, Valerio, Loreta A. Kondili, Riccardo Nevola, Pasquale Perillo, Davide Mastrocinque, Alessio Aghemo, and Ernesto Claar. 2022. "Elimination of Hepatitis C in Southern Italy: A Model of HCV Screening and Linkage to Care among Hospitalized Patients at Different Hospital Divisions" Viruses 14, no. 5: 1096. https://doi.org/10.3390/v14051096
APA StyleRosato, V., Kondili, L. A., Nevola, R., Perillo, P., Mastrocinque, D., Aghemo, A., & Claar, E. (2022). Elimination of Hepatitis C in Southern Italy: A Model of HCV Screening and Linkage to Care among Hospitalized Patients at Different Hospital Divisions. Viruses, 14(5), 1096. https://doi.org/10.3390/v14051096