
Clinical Performance of Rapid and Point-of-Care Antigen Tests for SARS-CoV-2 Variants of Concern: A Living Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Index Test
2.4. Reference Standard
2.5. Search Strategy
2.6. Study Selection and Data Extraction
2.7. Assessment of Risk of Bias and Applicability
2.8. Statistical Analysis and Data Synthesis
3. Results
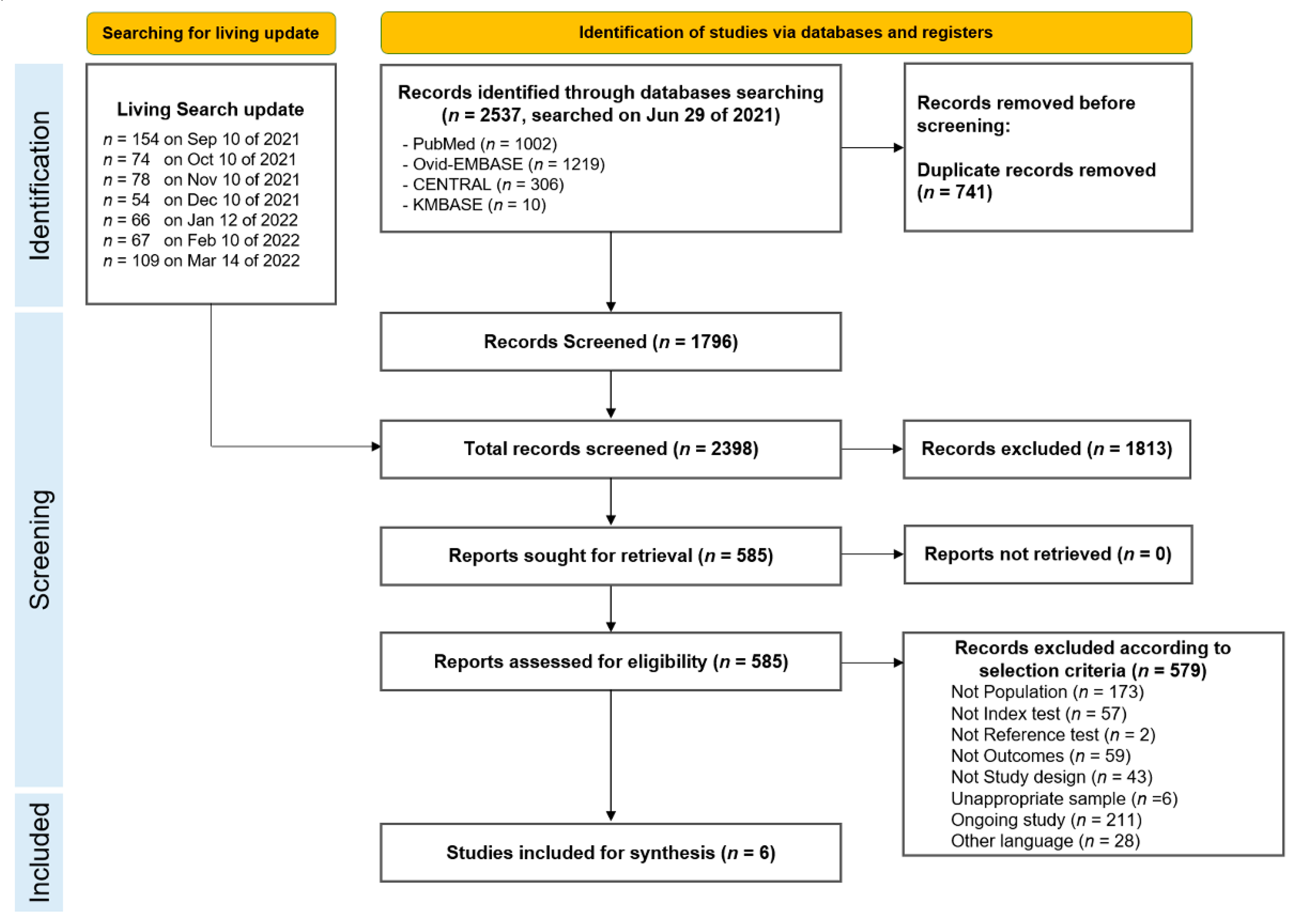
3.1. Identified Studies
3.2. Study Characteristics
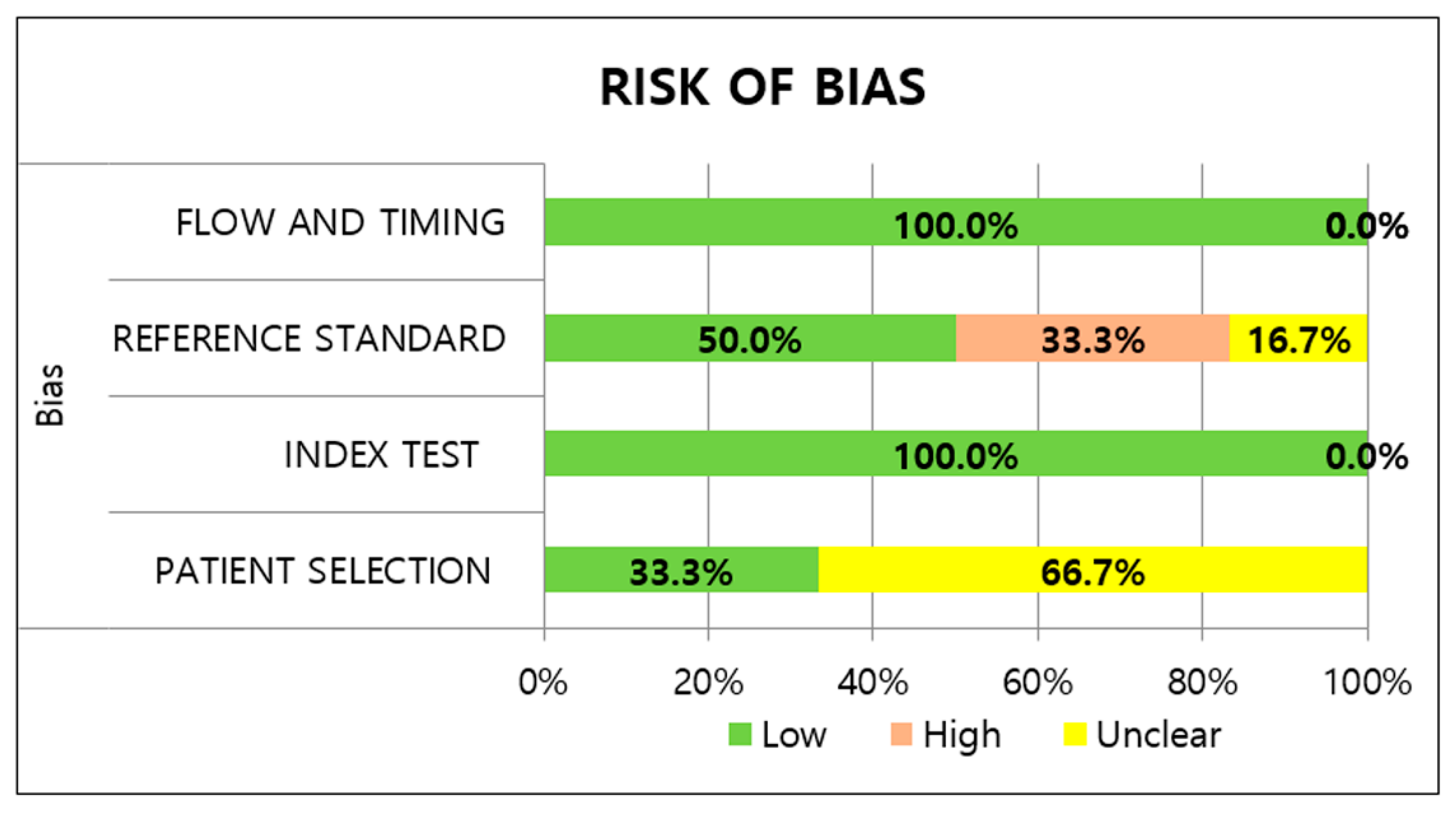
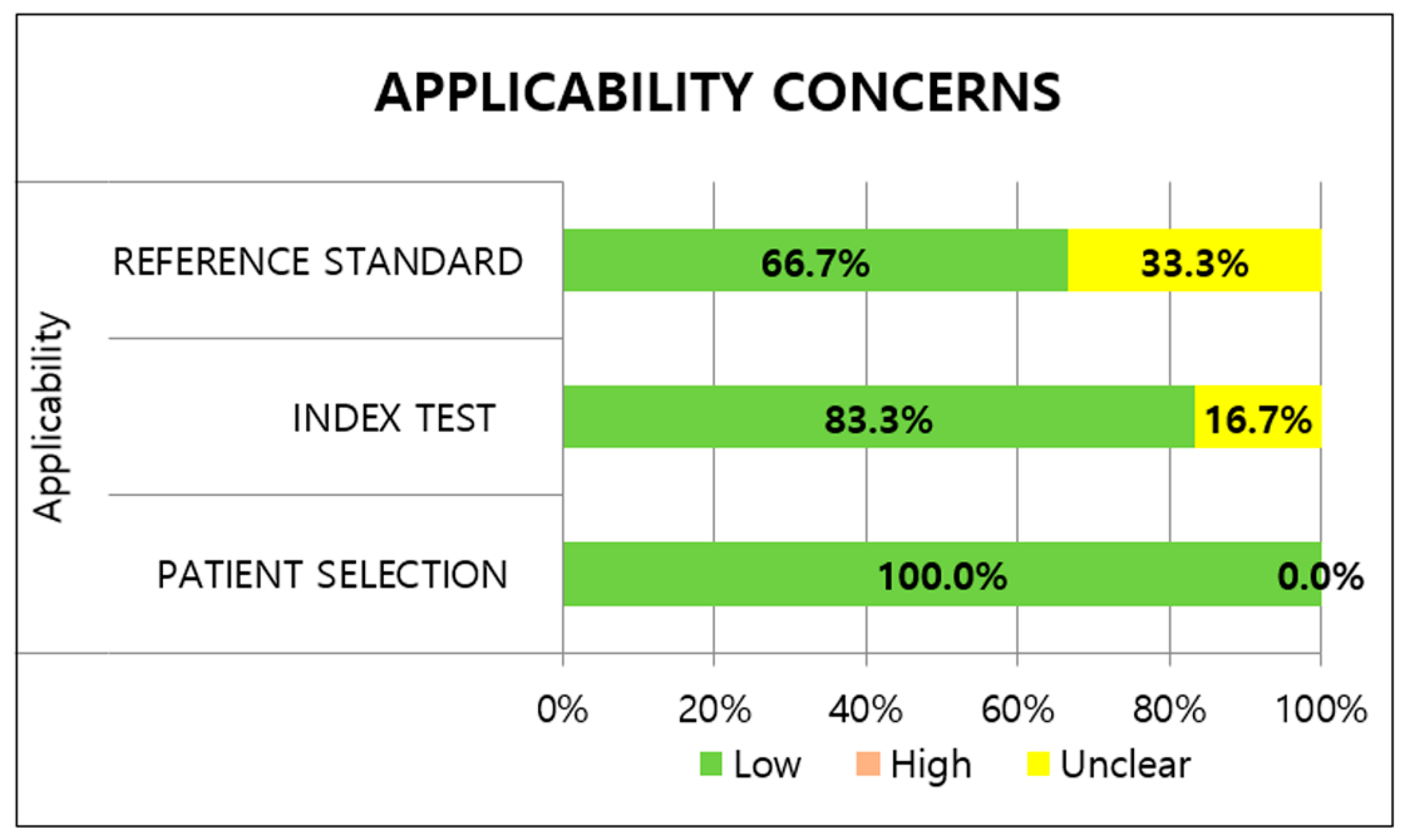
3.3. Methodological Quality of Studies
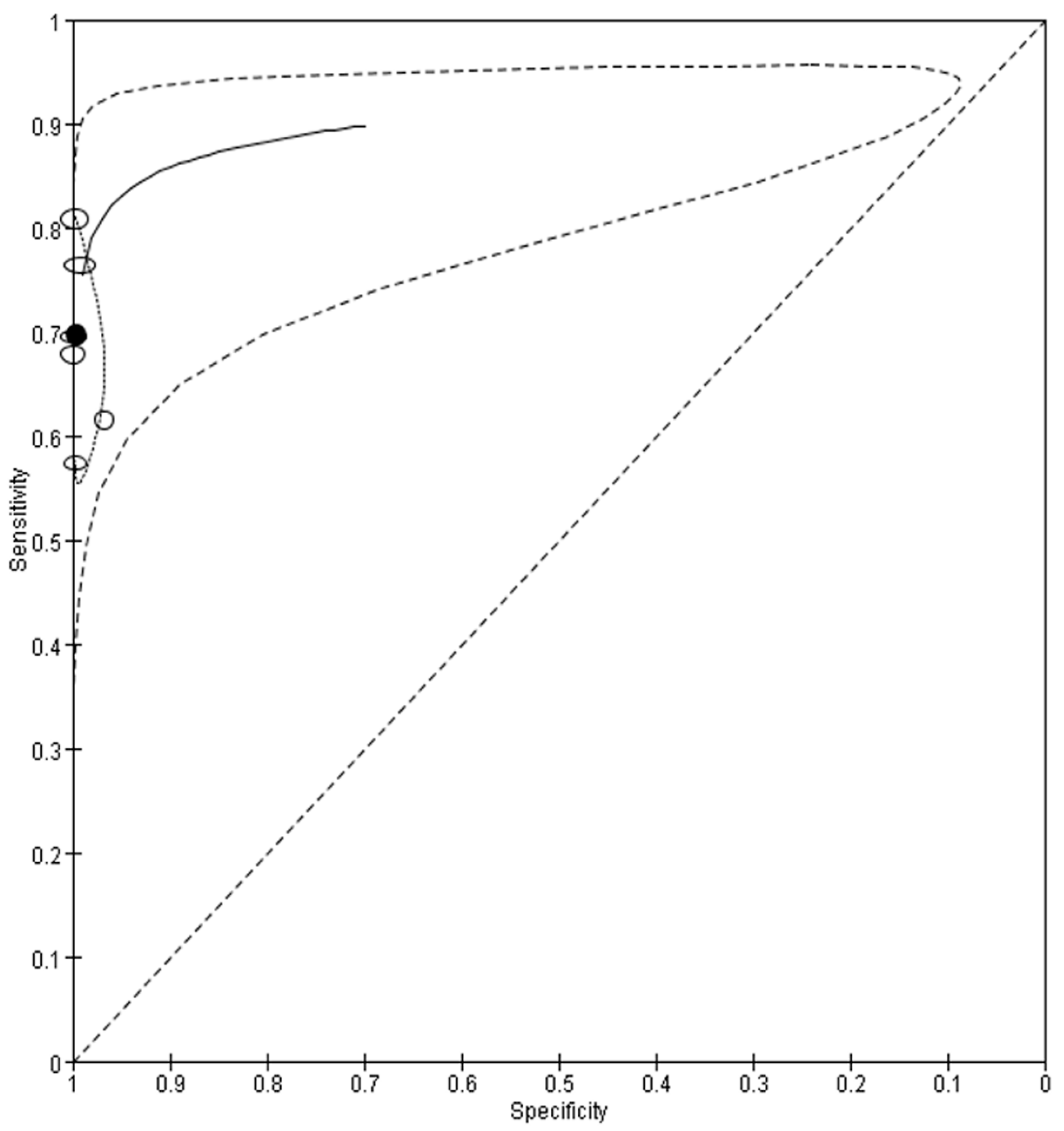
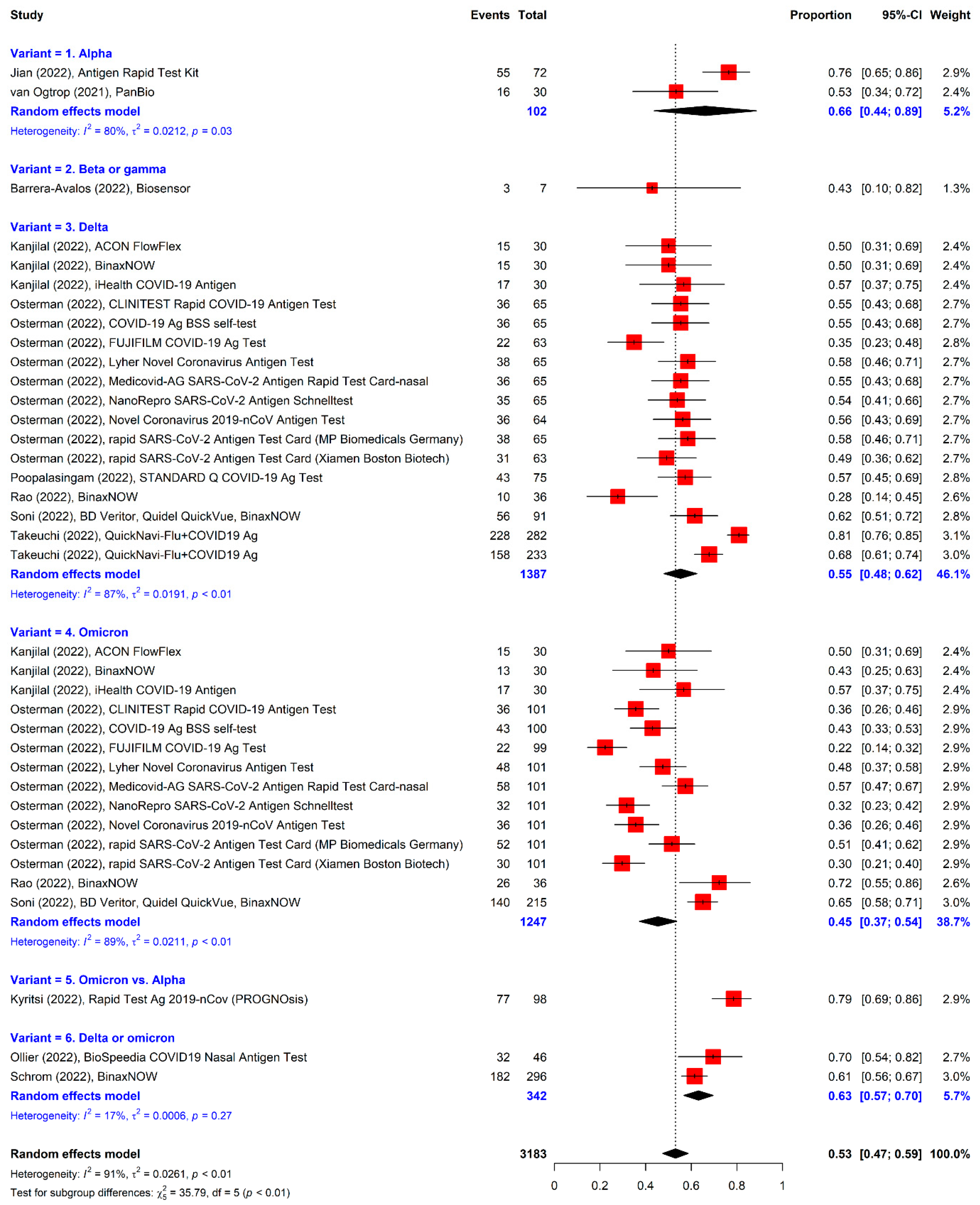
3.4. Meta-Analysis of RATs for Detecting Variants
3.5. Analysis Stratified by the Presence of Symptoms
3.6. Sensitivity Analysis
3.7. Analysis of RATs in Studies with Sensitivity Only
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Avetyan, D.; Hakobyan, S.; Nikoghosyan, M.; Ghukasyan, L.; Khachatryan, G.; Sirunyan, T.; Muradyan, N.; Zakharyan, R.; Chavushyan, A.; Hayrapetyan, V.; et al. Molecular Analysis of SARS-CoV-2 Lineages in Armenia. Viruses 2022, 14, 1074. [Google Scholar] [CrossRef] [PubMed]
- Hirotsu, Y.; Omata, M. Discovery of a SARS-CoV-2 variant from the P.1 lineage harboring K417T/E484K/N501Y mutations in Kofu, Japan. J. Infect. 2021, 82, 276–316. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.; Kmiec, D.; Koepke, L.; Zech, F.; Jacob, T.; Sparrer, K.M.J.; Kirchhoff, F. Omicron: What Makes the Latest SARS-CoV-2 Variant of Concern So Concerning? J. Virol. 2022, 96, e0207721. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Coronnavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 1 April 2022).
- KCDC. KCDC Coronnavirus (COVID-19) Dashboard. Available online: http://ncov.mohw.go.kr/ (accessed on 1 April 2022).
- WHO. Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed on 17 May 2022).
- Islam, F.; Dhawan, M.; Nafady, M.H.; Emran, T.B.; Mitra, S.; Choudhary, O.P.; Akter, A. Understanding the omicron variant (B.1.1.529) of SARS-CoV-2: Mutational impacts, concerns, and the possible solutions. Ann. Med. Surg. 2022, 78, 103737. [Google Scholar] [CrossRef]
- CDC. COVID Data Tracker: Variant Proportions. Available online: https://covid.cdc.gov/covid-data-tracker/#variant-proportions (accessed on 17 May 2022).
- Khandia, R.; Singhal, S.; Alqahtani, T.; Kamal, M.A.; El-Shall, N.A.; Nainu, F.; Desingu, P.A.; Dhama, K. Emergence of SARS-CoV-2 Omicron (B.1.1.529) variant, salient features, high global health concerns and strategies to counter it amid ongoing COVID-19 pandemic. Environ. Res. 2022, 209, 112816. [Google Scholar] [CrossRef]
- Xie, X.; Liu, Y.; Liu, J.; Zhang, X.; Zou, J.; Fontes-Garfias, C.R.; Xia, H.; Swanson, K.A.; Cutler, M.; Cooper, D.; et al. Neutralization of SARS-CoV-2 spike 69/70 deletion, E484K and N501Y variants by BNT162b2 vaccine-elicited sera. Nat. Med. 2021, 27, 620–621. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Rapid Increase of a SARS-CoV-2 Variant with Multiple Spike Protein Mutations Observed in the United Kingdom. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/SARS-CoV-2-variant-multiple-spike-protein-mutations-United-Kingdom.pdf (accessed on 17 May 2022).
- NERVTAG. NERVTAG Meeting on SARS-CoV-2 Variant under Investigation VUI-202012/01. Available online: https://app.box.com/s/3lkcbxepqixkg4mv640dpvvg978ixjtf/file/756963730457 (accessed on 17 May 2022).
- NERVTAG. NERVTAG/SPI-M Extraordinary Meetingon SARS-CoV-2 Variant of Concern 202012/01 (Variant B.1.1.7). Available online: https://app.box.com/s/3lkcbxepqixkg4mv640dpvvg978ixjtf/file/756964987830 (accessed on 13 May 2022).
- Tsang, N.N.Y.; So, H.C.; Ng, K.Y.; Cowling, B.J.; Leung, G.M.; Ip, D.K.M. Diagnostic performance of different sampling approaches for SARS-CoV-2 RT-PCR testing: A systematic review and meta-analysis. Lancet Infect. Dis. 2021, 21, 1233–1245. [Google Scholar] [CrossRef]
- Renzoni, A.; Perez, F.; Ngo Nsoga, M.T.; Yerly, S.; Boehm, E.; Gayet-Ageron, A.; Kaiser, L.; Schibler, M. Analytical Evaluation of Visby Medical RT-PCR Portable Device for Rapid Detection of SARS-CoV-2. Diagnostics 2021, 1, 813. [Google Scholar] [CrossRef]
- Khalid, M.F.; Selvam, K.; Jeffry, A.J.N.; Salmi, M.F.; Najib, M.A.; Norhayati, M.N.; Aziah, I. Performance of Rapid Antigen Tests for COVID-19 Diagnosis: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 110. [Google Scholar] [CrossRef]
- CDC. Antigen Testing Guidelines. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antigen-tests-guidelines.html (accessed on 13 May 2022).
- ECDC. Options for the Use of Rapid Antigen Detection Tests for COVID-19 in the EU/EEA—First Update. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Options-for-the-use-of-rapid-antigen-tests-for-COVID-19-first-update.pdf (accessed on 13 May 2022).
- Ollier, Q.; Pillet, S.; Mory, O.; Gagnaire, J.; Thuiller, C.; Annino, N.; Gagneux-Brunon, A.; Botelho-Nevers, E.; Bourlet, T.; Pozzetto, B.; et al. Prospective evaluation of the point-of-care use of a rapid antigenic SARS-CoV-2 immunochromatographic test in a paediatric emergency department. Clin. Microbiol. Infect. 2022, 28, 734.e1–734.e6. [Google Scholar] [CrossRef]
- Takeuchi, Y.; Akashi, Y.; Kiyasu, Y.; Terada, N.; Kurihara, Y.; Kato, D.; Miyazawa, T.; Muramatsu, S.; Shinohara, Y.; Ueda, A.; et al. A prospective evaluation of diagnostic performance of a combo rapid antigen test QuickNavi-Flu+COVID19 Ag. J. Infect. Chemother. 2022, 28, 840–843. [Google Scholar] [CrossRef] [PubMed]
- Kanjilal, S.; Chalise, S.; Shah, A.S.; Cheng, C.-A.; Senussi, Y.; Uddin, R.; Thiriveedhi, V.; Cho, H.E.; Carroll, S.; Lemieux, J.; et al. Performance of three rapid antigen tests against the SARS-CoV-2 Omicron variant. medRxiv 2022. [Google Scholar] [CrossRef]
- Osterman, A.; Badell, I.; Basara, E.; Stern, M.; Kriesel, F.; Eletreby, M.; Oztan, G.N.; Huber, M.; Autenrieth, H.; Knabe, R.; et al. Impaired detection of omicron by SARS-CoV-2 rapid antigen tests. Med. Microbiol. Immunol. 2022, 211, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Forcelloni, S.; Benedetti, A.; Dilucca, M.; Giansanti, A. Identification of Conserved Epitopes in SARS-CoV-2 Spike and Nucleocapsid Protein. Curr. Genomics 2021, 22, 541–549. [Google Scholar] [CrossRef]
- Brummer, L.E.; Katzenschlager, S.; Gaeddert, M.; Erdmann, C.; Schmitz, S.; Bota, M.; Grilli, M.; Larmann, J.; Weigand, M.A.; Pollock, N.R.; et al. Accuracy of novel antigen rapid diagnostics for SARS-CoV-2: A living systematic review and meta-analysis. PLoS Med. 2021, 18, e1003735. [Google Scholar] [CrossRef]
- WHO. In Vitro Diagnostics Detecting SARS-CoV-2 Nucleic Acid and Rapid Diagnostics Tests Detecting SARS-CoV-2 Antigen. Available online: https://www.who.int/publications/m/item/PQDx-347-version-4 (accessed on 3 May 2022).
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Nyaga, V.N.; Arbyn, M. Metadta: A Stata command for meta-analysis and meta-regression of diagnostic test accuracy data—A tutorial. Arch. Public Health 2022, 80, 95. [Google Scholar] [CrossRef]
- Poopalasingam, N.; Korenkov, M.; Ashurov, A.; Strobel, J.; Fish, I.; Hellmich, M.; Gruell, H.; Lehmann, C.; Heger, E.; Klein, F. Determining the reliability of rapid SARS-CoV-2 antigen detection in fully vaccinated individuals. J. Clin. Virol. 2022, 148, 105119. [Google Scholar] [CrossRef]
- Jian, M.J.; Perng, C.L.; Chung, H.Y.; Chang, C.K.; Lin, J.C.; Yeh, K.M.; Chen, C.W.; Hsieh, S.S.; Pan, P.C.; Chang, H.T.; et al. Clinical assessment of SARS-CoV-2 antigen rapid detection compared with RT-PCR assay for emerging variants at a high-throughput community testing site in Taiwan. Int. J. Infect. Dis. 2022, 115, 30–34. [Google Scholar] [CrossRef]
- Akingba, O.L.; Sprong, K.; Marais, G.; Hardie, D.R. Field performance evaluation of the PanBio rapid SARS-CoV-2 antigen assay in an epidemic driven by the B.1.351 variant in the Eastern Cape, South Africa. J. Clin. Virol. Plus 2021, 1, 100013. [Google Scholar] [CrossRef]
- Schrom, J.; Marquez, C.; Pilarowski, G.; Wang, C.Y.; Mitchell, A.; Puccinelli, R.; Black, D.; Rojas, S.; Ribeiro, S.; Tulier-Laiwa, V.; et al. Comparison of SARS-CoV-2 Reverse Transcriptase Polymerase Chain Reaction and BinaxNOW Rapid Antigen Tests at a Community Site During an Omicron Surge: A Cross-Sectional Study. Ann. Intern. Med. 2022, 175, 682–690. [Google Scholar] [CrossRef] [PubMed]
- Arshadi, M.; Fardsanei, F.; Deihim, B.; Farshadzadeh, Z.; Nikkhahi, F.; Khalili, F.; Sotgiu, G.; Shahidi Bonjar, A.H.; Centis, R.; Migliori, G.B.; et al. Diagnostic Accuracy of Rapid Antigen Tests for COVID-19 Detection: A Systematic Review With Meta-analysis. Front. Med. 2022, 9, 870738. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.C.; Lu, S.C.; Bai, C.H.; Wang, P.Y.; Lee, K.Y.; Wang, Y.H. Diagnostic Accuracy of SARS-CoV-2 Antigen Tests for Community Transmission Screening: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 11451. [Google Scholar] [CrossRef]
- Dinnes, J.; Deeks, J.J.; Adriano, A.; Berhane, S.; Davenport, C.; Dittrich, S.; Emperador, D.; Takwoingi, Y.; Cunningham, J.; Beese, S.; et al. Rapid, point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst. Rev. 2020, 8, CD013705. [Google Scholar] [CrossRef]
- Dinnes, J.; Deeks, J.J.; Berhane, S.; Taylor, M.; Adriano, A.; Davenport, C.; Dittrich, S.; Emperador, D.; Takwoingi, Y.; Cunningham, J.; et al. Rapid, point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst. Rev. 2021, 3, CD013705. [Google Scholar] [CrossRef] [PubMed]
- Khandker, S.S.; Nik Hashim, N.H.H.; Deris, Z.Z.; Shueb, R.H.; Islam, M.A. Diagnostic Accuracy of Rapid Antigen Test Kits for Detecting SARS-CoV-2: A Systematic Review and Meta-Analysis of 17,171 Suspected COVID-19 Patients. J. Clin. Med. 2021, 10, 3493. [Google Scholar] [CrossRef]
- Ricco, M.; Ranzieri, S.; Peruzzi, S.; Valente, M.; Marchesi, F.; Bragazzi, N.L.; Donelli, D.; Balzarini, F.; Ferraro, P.; Gianfredi, V.; et al. Antigen Detection Tests for SARS-CoV-2: A systematic review and meta-analysis on real world data. Acta. Biomed. 2022, 93, e2022036. [Google Scholar] [CrossRef]
- WHO. Criteria for Releasing COVID-19 Patients from Isolation. Available online: https://www.who.int/news-room/commentaries/detail/criteria-for-releasing-covid-19-patients-from-isolation (accessed on 17 May 2022).
- FDA. Template for Developers of Antigen Tests. Available online: https://view.officeapps.live.com/op/view.aspx?src=https%3A%2F%2Fwww.fda.gov%2Fmedia%2F137907%2Fdownload&wdOrigin=BROWSELINK (accessed on 17 May 2022).
- WHO. Antigen-Detection in the Diagnosis of SARS-CoV-2 Infection. Available online: https://www.who.int/publications/i/item/antigen-detection-in-the-diagnosis-of-sars-cov-2infection-using-rapid-immunoassays (accessed on 17 May 2022).
- WHO. Enhancing Readiness for Omicron (B.1.1.529): Technical Brief and Priority Actions for Member States. Available online: https://www.who.int/publications/m/item/enhancing-readiness-for-omicron-(b.1.1.529)-technical-brief-and-priority-actions-for-member-states (accessed on 17 May 2022).
- Pulliam, J.R.C.; van Schalkwyk, C.; Govender, N.; von Gottberg, A.; Cohen, C.; Groome, M.J.; Dushoff, J.; Mlisana, K.; Moultrie, H. Increased risk of SARS-CoV-2 reinfection associated with emergence of the Omicron variant in South Africa. medRxiv 2021. [Google Scholar] [CrossRef]
- Dougherty, K.; Mannell, M.; Naqvi, O.; Matson, D.; Stone, J. SARS-CoV-2 B.1.617.2 (Delta) Variant COVID-19 Outbreak Associated with a Gymnastics Facility—Oklahoma, April–May 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1004–1007. [Google Scholar] [CrossRef]
- PHE. SARS-CoV-2 Variants of Concern and Variants under Investigation in England. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/991343/Variants_of_Concern_VOC_Technical_Briefing_14.pdf (accessed on 17 May 2022).
- Fisman, D.N.; Tuite, A.R. Evaluation of the relative virulence of novel SARS-CoV-2 variants: A retrospective cohort study in Ontario, Canada. CMAJ 2021, 193, E1619–E1625. [Google Scholar] [CrossRef]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, risk of hospital admission, and vaccine effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef]
- Twohig, K.A.; Nyberg, T.; Zaidi, A.; Thelwall, S.; Sinnathamby, M.A.; Aliabadi, S.; Seaman, S.R.; Harris, R.J.; Hope, R.; Lopez-Bernal, J.; et al. Hospital admission and emergency care attendance risk for SARS-CoV-2 delta (B.1.617.2) compared with alpha (B.1.1.7) variants of concern: A cohort study. Lancet Infect. Dis. 2022, 22, 35–42. [Google Scholar] [CrossRef]
- Lee, J.; Kim, K.W.; Choi, S.H.; Huh, J.; Park, S.H. Systematic Review and Meta-Analysis of Studies Evaluating Diagnostic Test Accuracy: A Practical Review for Clinical Researchers-Part II. Statistical Methods of Meta-Analysis. Korean J. Radiol. 2015, 16, 1188–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyritsi, M.A.; Speletas, M.; Mouchtouri, V.; Vachtsioli, E.; Babalis, D.; Kouliou, O.; Tsispara, A.; Tseroni, M.; Hadjichristodoulou, C. Performance Evaluation of a Rapid Antigen Test (RAT) during Omicron Pandemic Wave in Greece, Conducted by Different Personnel, and Comparison with Performance in Previous Wave (Alpha Variant) Period. Diagnostics 2022, 12, 1048. [Google Scholar] [CrossRef]
- Rao, A.; Bassit, L.; Lin, J.; Verma, K.; Bowers, H.B.; Pachura, K.; Greenleaf, M.; Sullivan, J.; Lai, E.; Creager, R.S.; et al. Assessment of the Abbott BinaxNOW SARS-CoV-2 rapid antigen test against viral variants of concern. iScience 2022, 25, 103968. [Google Scholar] [CrossRef]
- Soni, A.; Herbert, C.; Filippaios, A.; Broach, J.; Colubri, A.; Fahey, N.; Woods, K.; Nanavati, J.; Wright, C.; Orwig, T.; et al. Comparison of Rapid Antigen Tests’ Performance between Delta (B.1.61.7; AY.X) and Omicron (B.1.1.529; BA1) Variants of SARS-CoV-2: Secondary Analysis from a Serial Home Self-Testing Study. medRxiv 2022. [Google Scholar] [CrossRef]
- Van Ogtrop, M.L.; van de Laar, T.J.W.; Eggink, D.; Vanhommerig, J.W.; van der Reijden, W.A. Comparison of the Performance of the PanBio COVID-19 Antigen Test in SARS-CoV-2 B.1.1.7 (Alpha) Variants versus non-B.1.1.7 Variants. Microbiol. Spectr. 2021, 9, e0088421. [Google Scholar] [CrossRef]
- Barrera-Avalos, C.; Luraschi, R.; Vallejos-Vidal, E.; Mella-Torres, A.; Hernandez, F.; Figueroa, M.; Rioseco, C.; Valdes, D.; Imarai, M.; Acuna-Castillo, C.; et al. The Rapid Antigen Detection Test for SARS-CoV-2 Underestimates the Identification of COVID-19 Positive Cases and Compromises the Diagnosis of the SARS-CoV-2 (K417N/T, E484K, and N501Y) Variants. Front. Public Health 2021, 9, 780801. [Google Scholar] [CrossRef]
- Korenkov, M.; Poopalasingam, N.; Madler, M.; Vanshylla, K.; Eggeling, R.; Wirtz, M.; Fish, I.; Dewald, F.; Gieselmann, L.; Lehmann, C.; et al. Evaluation of a Rapid Antigen Test To Detect SARS-CoV-2 Infection and Identify Potentially Infectious Individuals. J. Clin. Microbiol. 2021, 59, e0089621. [Google Scholar] [CrossRef]
- Gerges, D.; Kapps, S.; Hernández-Carralero, E.; Freire, R.; Aiad, M.; Schmidt, S.; Winnicki, W.; Reiter, T.; Pajenda, S.; Schmidt, A.; et al. Vaccination with BNT162b2 and ChAdOx1 nCoV-19 Induces Cross-Reactive Anti-RBD IgG against SARS-CoV-2 Variants including Omicron. Viruses 2022, 14, 1181. [Google Scholar] [CrossRef]
- Fujita-Rohwerder, N.; Beckmann, L.; Zens, Y.; Verma, A. Diagnostic accuracy of rapid point-of-care tests for diagnosis of current SARS-CoV-2 infections in children: A systematic review and meta-analysis. BMJ Evid. Based Med. 2022, bmjebm-2021-111828. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.; Yang, D.; Lee, W.; Kim, G.T.; Kim, H.S.; Ahn, H.S.; Kim, H.J. Diagnostic value of screening enzyme immunoassays compared to indirect immunofluorescence for anti-nuclear antibodies in patients with systemic rheumatic diseases: A systematic review and meta-analysis. Semin. Arthritis Rheum. 2018, 48, 334–342. [Google Scholar] [CrossRef]
- Macaskill, P.; Gatsonis, C.; Deeks, J.; Harbord, R.; Takwoingi, Y. Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy; Version 0.9.0.; The Cochrane Collaboration: London, UK, 2010; pp. 36–43. [Google Scholar]
- NECA. COVID-19 Living Guideline. Available online: https://www.neca.re.kr/lay1/bbs/S1T11C174/F/58/view.do?article_seq=8826&cpage=1&rows=10&condition=&keyword=&show=&cat=) (accessed on 17 May 2022).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Population (n) | Enrollment Periods | Sample Type | RATs | rRT-PCR | Study Location |
|---|---|---|---|---|---|---|
| Alpha | ||||||
| Jian et al. [2022] | Mixed (2096) | 2021.5.17~2021.5.22 | NP swab | Antigen Rapid Test Kit | LabTurbo AIO 48 system (LabTurbo Biotech Corporation, Princeton, NJ, USA) | Taiwan |
| Ollier et al. [2022] | Mixed (990) | 2021.1.15~2021.5.28 | NP swab | BioSpeedia COVID19 Nasal Antigen Test (BioSpeedia, Gutenberg, France) | SARS-CoV-2 R-GENE (bioMérieux, Marcy I’Etoile, France) | France |
| Beta | ||||||
| Akingba et al. [2021] | Symptomatic (677) | 2020.11.17~2020.11.20 | NP swab | PanBio SARS-CoV-2 RTD (Abbott, Chicago, IL, USA) | Allplex 2019-nCoV (Seegene, Seoul, South Korea) | South Africa |
| Delta | ||||||
| Poopalasingam et al. [2022] | Mixed (696) | 2021.12.6~2021.12.31 | NP swab | STANDARD Q COVID-19 Ag Test (SD Biosensor, Suwon, Korea) | cobas SARS-CoV-2 (Roche Diagnostics, Mannheim, Germany) | Germany |
| Takeuchi et al. [2022] | Mixed (2372) | 2021.8.2~2021.9.13 | NP and Nasal swabs | QuickNavi-Flu+COVID19 Ag (Denka Co., Tokyo, Japan) | In-house | Japan |
| Delta and Omicron | ||||||
| Schrom et al. [2022] | Mixed (731) | 2022.1 | Nasal swab | BinaxNOW COVID-19 Antigen Self Test (Abbott, Chicago, IL, USA) | In-house | USA |
| Clinical Presentation | Study | Sample Type | RATs | Sensitivity (%) * | Specificity (%) * | Study Location |
|---|---|---|---|---|---|---|
| Mixed | Alpha | |||||
| Jian et al. [2022] | NP swab | Antigen Rapid Test Kit | 76.4 (64.9–85.6) | 99.3 (98.8–99.6) | Taiwan | |
| Ollier et al. [2022] | NP swab | BioSpeedia COVID19 Nasal Antigen Test (BioSpeedia, Gutenberg, France) | 69.6 (54.3–82.3) | 99.9 (99.4–100.0) | France | |
| Delta | ||||||
| Poopalasingam et al. [2022] | NP swab | STANDARD Q COVID-19 Ag Test (SD Biosensor, Suwon, Korea) | 57.3 (46.1–67.9) | 99.9 (99.6–100.0) | German | |
| Takeuchi et al. [2022] | NP swab | QuickNavi-Flu+COVID19 Ag (Denka Co., Tokyo, Japan) | 80.9 (75.8–85.3) | 99.8 (99.3–99.9) | Japan | |
| Takeuchi et al. [2022] | Nasal swab | QuickNavi-Flu+COVID19 Ag (Denka Co., Tokyo, Japan) | 67.8 (61.4–73.8) | 100 (99.1–100.0) | Japan | |
| Delta and Omicron | ||||||
| Schrom et al. [2022] | Nasal swab | BinaxNOW COVID-19 Antigen Self Test (Abbott, Chicago, IL, USA) | 61.5 (55.7–67.1) | 96.8 (94.7–98.2) | USA | |
| Symptomatic | Alpha | |||||
| Ollier et al. [2022] | NP swab | BioSpeedia COVID19 Nasal Antigen Test (BioSpeedia, Gutenberg, France) | 82.9 (66.4–93.4) | 99.8 (98.7–100.0) | France | |
| Beta | ||||||
| Akingba et al. [2021] | NP swab | PanBio SARS-CoV-2 RTD (Abbott, Chicago, IL, USA) | 69.2 (61.4–75.8) | 99.0 (98.8–99.3) | South Africa | |
| Delta | ||||||
| Takeuchi et al. [2022] | NP swab | QuickNavi-Flu+COVID19 Ag (Denka Co., Tokyo, Japan) | 88.3 (82.5–92.7) | 100.0 (98.8–100.0) | Japan | |
| Takeuchi et al. [2022] | Nasal swab | QuickNavi-Flu+COVID19 Ag (Denka Co., Tokyo, Japan) | 73.7 (65.3–80.9) | 100.0 (98.3–100.0) | Japan | |
| Asymptomatic | Alpha | |||||
| Ollier et al. [2022] | NP swab | BioSpeedia COVID19 Nasal Antigen Test (BioSpeedia, Gutenberg, France) | 27.3 (6.1–61.0) | 100.0 (99.3–100.0) | France | |
| Delta | ||||||
| Takeuchi et al. [2022] | NP swab | QuickNavi-Flu+COVID19 Ag (Denka Co., Tokyo, Japan) | 69.4 (59.9–77.8) | 99.6 (98.9–99.9) | Japan | |
| Takeuchi et al. [2022] | Nasal swab | QuickNavi-Flu+COVID19 Ag (Denka Co., Tokyo, Japan) | 60.0 (49.7–69.7) | 100.0 (98.2–100.0) | Japan | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Sung, H.; Lee, H.; Kim, J.-S.; Shin, S.; Jeong, S.; Choi, M.; Lee, H.-J.; on behalf of the Development Committee and Clinical Evidence Research Team in National Evidence-Based Healthcare Collaborating Agency. Clinical Performance of Rapid and Point-of-Care Antigen Tests for SARS-CoV-2 Variants of Concern: A Living Systematic Review and Meta-Analysis. Viruses 2022, 14, 1479. https://doi.org/10.3390/v14071479
Kim J, Sung H, Lee H, Kim J-S, Shin S, Jeong S, Choi M, Lee H-J, on behalf of the Development Committee and Clinical Evidence Research Team in National Evidence-Based Healthcare Collaborating Agency. Clinical Performance of Rapid and Point-of-Care Antigen Tests for SARS-CoV-2 Variants of Concern: A Living Systematic Review and Meta-Analysis. Viruses. 2022; 14(7):1479. https://doi.org/10.3390/v14071479
Chicago/Turabian StyleKim, Jimin, Heungsup Sung, Hyukmin Lee, Jae-Seok Kim, Sue Shin, Seri Jeong, Miyoung Choi, Hyeon-Jeong Lee, and on behalf of the Development Committee and Clinical Evidence Research Team in National Evidence-Based Healthcare Collaborating Agency. 2022. "Clinical Performance of Rapid and Point-of-Care Antigen Tests for SARS-CoV-2 Variants of Concern: A Living Systematic Review and Meta-Analysis" Viruses 14, no. 7: 1479. https://doi.org/10.3390/v14071479
APA StyleKim, J., Sung, H., Lee, H., Kim, J. -S., Shin, S., Jeong, S., Choi, M., Lee, H. -J., & on behalf of the Development Committee and Clinical Evidence Research Team in National Evidence-Based Healthcare Collaborating Agency. (2022). Clinical Performance of Rapid and Point-of-Care Antigen Tests for SARS-CoV-2 Variants of Concern: A Living Systematic Review and Meta-Analysis. Viruses, 14(7), 1479. https://doi.org/10.3390/v14071479