
SARS-CoV-2 Infection and Pregnancy: Maternal and Neonatal Outcomes and Placental Pathology Correlations
 , , , , , , , ,
, , , , , , , ,  , ,
, ,  ,
,  , add
Show full author list
, add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
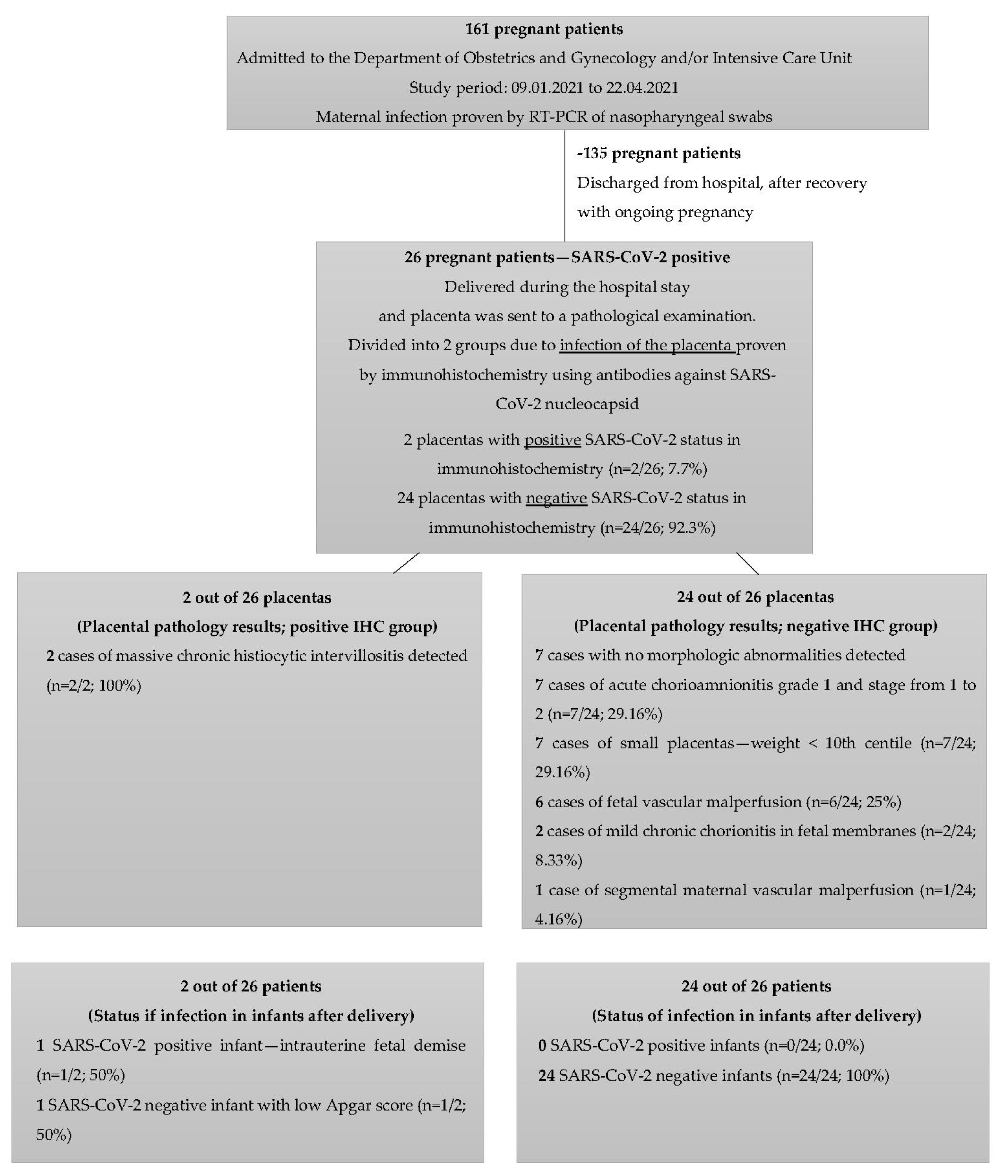
2.1. Study Population and Procedures
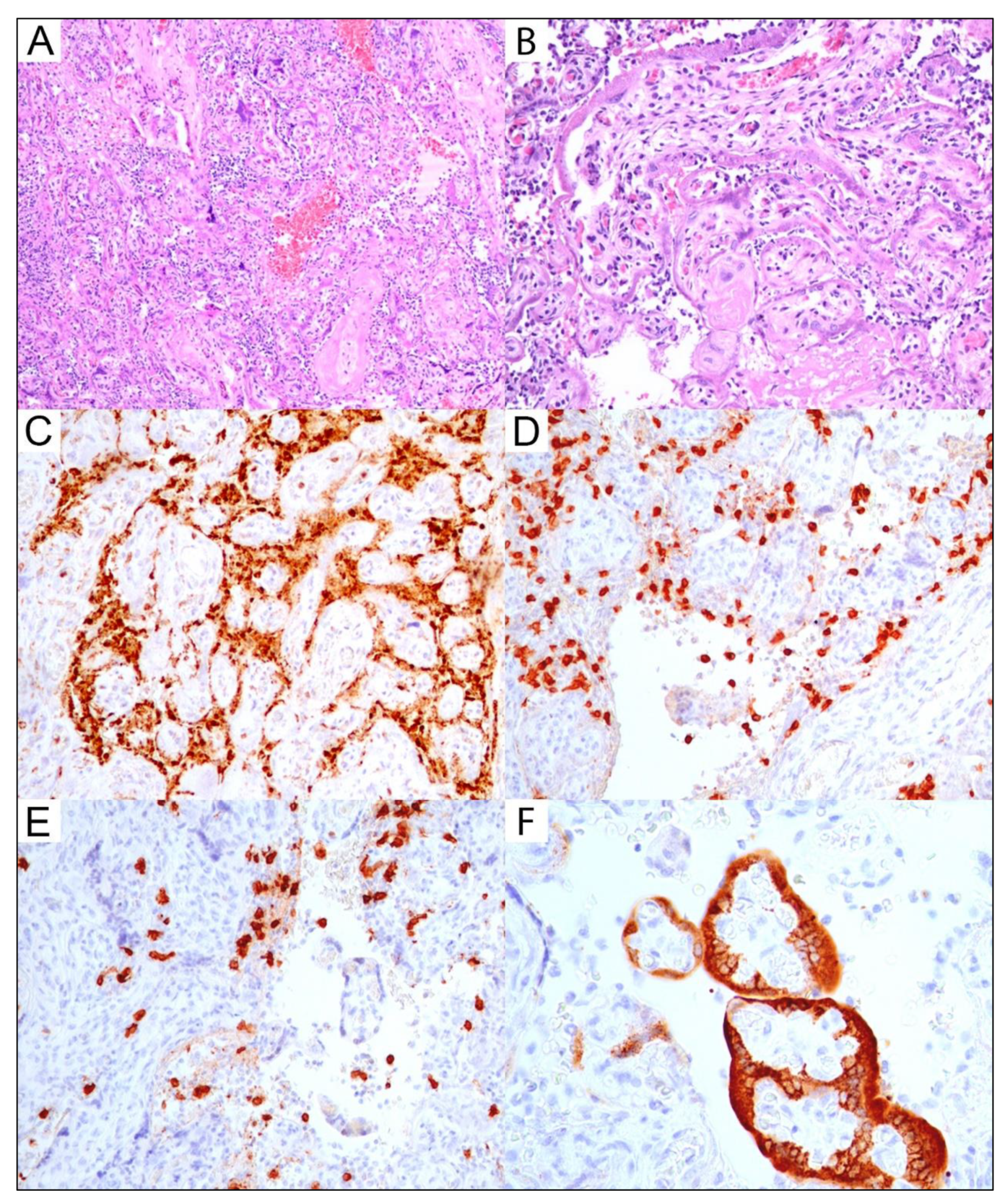
2.2. Placental Pathology and SARS-CoV-2 Immunoexpression Studies
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Karimi-Zarchi, M.; Neamatzadeh, H.; Dastgheib, S.A.; Abbasi, H.; Mirjalili, S.R.; Behforouz, A.; Ferdosian, F.; Bahrami, R. Vertical Transmission of Coronavirus Disease 19 (COVID-19) from Infected Pregnant Mothers to Neonates: A Review. Fetal Pediatric Pathol. 2020, 39, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Duran, P.; Berman, S.; Niermeyer, S.; Jaenisch, T.; Forster, T.; Ponce de Leon, R.G.; de Mucio, B.; Serruya, S. COVID-19 and newborn health: Systematic review. Pan Am. J. Public Health 2020, 44, 2020. [Google Scholar] [CrossRef] [PubMed]
- Fenizia, C.; Biasin, M.; Cetin, I.; Vergani, P.; Mileto, D.; Spinillo, A.; Gismondo, M.R.; Perotti, F.; Callegari, C.; Mancon, A.; et al. Analysis of SARS-CoV-2 vertical transmission during pregnancy. Nat. Commun. 2020, 11, 5128. [Google Scholar] [CrossRef]
- Jamieson, D.J.; Rasmussen, S.A. An update on COVID-19 and pregnancy. Am. J. Obstet. Gynecol. 2022, 226, 177–186. [Google Scholar] [CrossRef]
- World Health Organisation. Definition and Categorization of the Timing of Mother-to-Child Transmission of SARS-CoV-2; Scientific brief, 8 February 2021; WHO: Geneva, Switzerland, 2021.
- Blumberg, D.A.; Underwood, M.A.; Hedriana, H.L.; Lakshminrusimha, S. Vertical Transmission of SARS-CoV-2: What is the Optimal Definition? Am. J. Perinatol. 2020, 37, 769–772. [Google Scholar] [CrossRef]
- Edlow, A.G.; Li, J.Z.; Collier, A.Y.; Atyeo, C.; James, K.E.; Boatin, A.A.; Gray, K.J.; Bordt, E.A.; Shook, L.L.; Yonker, L.M.; et al. Assessment of Maternal and Neonatal SARS-CoV-2 Viral Load, Transplacental Antibody Transfer, and Placental Pathology in Pregnancies During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2030455. [Google Scholar] [CrossRef]
- Zdanowski, W.; Waśniewski, T. Evaluation of SARS-CoV-2 spike protein antibody titers in cord blood after COVID-19 vaccination during pregnancy in polish healthcare workers: Preliminary results. Vaccines 2021, 9, 675. [Google Scholar] [CrossRef]
- Fox, H.; Sebire, N.J. Pathology of the Placenta, 3rd ed.; Saunders Elsevier: Philadelphia, PA, USA, 2007. [Google Scholar]
- Baergen, R.N.; Burton, G.J.; Kaplan, C.G. Benirschke’s Pathology of the Human Placenta, 7th ed.; Springer: Cham, Switzerland, 2022. [Google Scholar]
- Wong, Y.P.; Khong, T.Y.; Tan, G.C. The Effects of COVID-19 on Placenta and Pregnancy: What Do We Know So Far? Diagnostics 2021, 11, 94. [Google Scholar] [CrossRef]
- Krasemann, S.; Dittmayer, C.; von Stillfried, S.; Meinhardt, J.; Heinrich, F.; Hartmann, K.; Pfefferle, S.; Thies, E.; von Manitius, R.; Aschman, T.A.D.; et al. Assessing and improving the validity of COVID-19 autopsy studies—A multicentre approach to establish essential standards for immunohistochemical and ultrastructural analyses. EBioMedicine 2022, 83, 104193. [Google Scholar] [CrossRef]
- Sharps, M.C.; Hayes, D.J.L.; Lee, S.; Zou, Z.; Brady, C.A.; Almoghrabi, Y.; Kerby, A.; Tamber, K.K.; Jones, C.J.; Adams Waldorf, K.M.; et al. A structured review of placental morphology and histopathological lesions associated with SARS-CoV-2 infection. Placenta 2020, 101, 13–29. [Google Scholar] [CrossRef] [PubMed]
- Di Girolamo, R.; Khalil, A.; Alameddine, S.; D’Angelo, E.; Galliani, C.; Matarrelli, B.; Buca, D.; Liberati, M.; Rizzo, G.; D’Antonio, F. Placental histopathology after SARS-CoV-2 infection in pregnancy: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2021, 3, 100468. [Google Scholar] [CrossRef] [PubMed]
- Baergen, R.N.; Heller, D.S. Placental Pathology in COVID-19 Positive Mothers: Preliminary Findings. Pediatr. Dev. Pathol. 2020, 23, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Rebutini, P.Z.; Zanchettin, A.C.; Stonoga, E.T.S.; Prá, D.M.M.; de Oliveira, A.L.P.; Dezidério, F.D.S.; Fonseca, A.S.; Dagostini, J.C.H.; Hlatchuk, E.C.; Furuie, I.N.; et al. Association Between COVID-19 Pregnant Women Symptoms Severity and Placental Morphologic Features. Front. Immunol. 2021, 12, 685919. [Google Scholar] [CrossRef]
- Chew, B.S.; Ghazali, R.; Othman, H.; Ismail, N.A.M.; Othman, A.S.; Laim, N.M.S.T.; Wong, Y.P.; Tan, G.C. Endocan expression in placenta of women with hypertension. J. Obstet. Gynaecol. Res. 2019, 45, 345–351. [Google Scholar] [CrossRef]
- Baergen, R.N. Manual of the Pathology of the Human Placenta, 2nd ed.; Springer: New York, NY, USA, 2011. [Google Scholar]
- Hecht, J.L.; Quade, B.; Deshpande, V.; Mino-Kenudson, M.; Ting, D.T.; Desai, N.; Dygulska, B.; Heyman, T.; Salafia, C.; Shen, D.; et al. SARS-CoV-2 can infect the placenta and is not associated with specific placental histopathology: A series of 19 placentas from COVID-19-positive mothers. Mod. Pathol. 2020, 33, 2092–2103. [Google Scholar] [CrossRef]
- Zeng, H.; Xu, C.; Fan, J.; Tang, Y.; Deng, Q.; Zhang, W.; Long, X. Antibodies in Infants Born to Mothers With COVID-19 Pneumonia. JAMA 2020, 323, 1848–1849. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M.; Henry, B.M. Thrombocytopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A meta-analysis. Clin. Chim. Acta Int. J. Clin. Chem. 2020, 506, 145–148. [Google Scholar] [CrossRef]
- Khong, T.Y.; Mooney, E.E.; Ariel, I.; Balmus, N.C.; Boyd, T.K.; Brundler, M.A.; Derricott, H.; Evans, M.J.; Faye-Petersen, O.M.; Gillan, J.E.; et al. Sampling and Definitions of Placental Lesions: Amsterdam Placental Workshop Group Consensus Statement. Arch. Pathol. Lab. Med. 2016, 140, 698–713. [Google Scholar] [CrossRef]
- Konstantinidou, A.E.; Angelidou, S.; Havaki, S.; Paparizou, K.; Spanakis, N.; Chatzakis, C.; Sotiriadis, A.; Theodora, M.; Donoudis, C.; Daponte, A.; et al. Stillbirth due to SARS-CoV-2 placentitis without evidence of intrauterine transmission to fetus: Association with maternal risk factors. Ultrasound Obstet. Gynecol. 2022, 59, 813–822. [Google Scholar] [CrossRef]
- Carsetti, R.; Quintarelli, C.; Quinti, I.; Piano Mortari, E.; Zumla, A.; Ippolito, G.; Locatelli, F. The immune system of children: The key to understanding SARS-CoV-2 susceptibility? Lancet Child Adolesc. Health 2020, 4, 414–416. [Google Scholar] [CrossRef]
- Mullins, E.; Evans, D.; Viner, R.M.; O’Brien, P.; Morris, E. Coronavirus in pregnancy and delivery: Rapid review. Ultrasound Obstet. Gynecol. 2020, 55, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Zaigham, M.; Andersson, O. Maternal and perinatal outcomes with COVID-19: A systematic review of 108 pregnancies. Acta Obstet. Gynecol. Scand. 2020, 99, 823–829. [Google Scholar] [CrossRef]
- Linehan, L.; O’Donoghue, K.; Dineen, S.; White, J.; Higgins, J.R.; Fitzgerald, B. SARS-CoV-2 placentitis: An uncommon complication of maternal COVID-19. Placenta 2021, 15, 261–266. [Google Scholar] [CrossRef]
- Walker, K.F.; O’Donoghue, K.; Grace, N.; Dorling, J.; Comeau, J.L.; Li, W.; Thornton, J.G. Maternal transmission of SARS-CoV-2 to the neonate, and possible routes for such transmission: A systematic review and critical analysis. BJOG 2020, 127, 1324–1336. [Google Scholar] [CrossRef] [PubMed]
- Marchaudon, V.; Devisme, L.; Petit, S.; Ansart-Franquet, H.; Vaast, P.; Subtil, D. Chronic histiocytic intervillositis of unknown etiology: Clinical features in a consecutive series of 69 cases. Placenta 2011, 32, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Bos, M.; Nikkels, P.G.J.; Cohen, D.; Schoones, J.W.; Bloemenkamp, K.W.M.; Bruijn, J.A.; Baelde, H.J.; van der Hoorn, M.L.P.; Turner, R.J. Towards standardized criteria for diagnosing chronic intervillositis of unknown etiology: A systematic review. Placenta 2018, 61, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Bwire, G.M.; Majigo, M.V.; Njiro, B.J.; Mawazo, A. Detection profile of SARS-CoV-2 using RT-PCR in different types of clinical specimens: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 719–725. [Google Scholar] [CrossRef]
- Cavaliere, A.F.; Marchi, L.; Aquilini, D.; Brunelli, T.; Vasarri, P.L. Passive immunity in newborn from SARS-CoV-2-infected mother. J. Med. Virol. 2020, 93, 1810–1813. [Google Scholar] [CrossRef]
- Giannis, D.; Ziogas, I.; Gianni, P. Coagulation disorders in coronavirus infected patients: COVID-19, SARS-CoV-1, MERS-CoV and lessons from the past. J. Clin. Virol. 2020, 127, 104362. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. China Medical Treatment Expert Group for COVID-19.Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | |
|---|---|
| Weeks of gestation at delivery | 37 (Mean), 25 week (Minimum), 41 (Maximum), |
| Delivery route | n = 6, 23% Vaginal; n = 19, 73% Cesarean; n = 1, 4% Spontaneous Abortion |
| PCR of amniotic fluid | n = 1, 4% Positive; n = 11, 42% Negative; n = 14, 54% Not Confirmed |
| PCR of infant | n = 1, 4% Positive; n = 25, 96% Negative |
| IHC of placenta | n = 2, 8% Positive; n = 24, 92% Negative |
| Maternal Anti-SARS-CoV-2 IgG | n = 3, 11% Positive; n = 5, 19% Negative; n = 18, 70% Not examined |
| Infant Anti-SARS-CoV-2 IgG | n = 3; 12% Positive; n = 6, 23% Negative; n = 17, 65% Not examined |
| Placental Diagnosis | Further Morphological Findings | Number of Cases Detected in Placental Subgroup; No (%) |
|---|---|---|
| Massive Chronic Histiocytic Intervillositis (MCHI) | All cases of MCHI in the study were detected in IHC SARS-CoV-2-positive placenta subgroup. Massive inflammatory infiltrate involving >30% percent of placental parenchyma was highlighted by CD68/CD3/CD8/CD138 panel of antibodies. | 2/26 (7.69%) |
| Acute chorioamnionitis (ACA) of fetal membranes | Grade 1 and stage 1-2 of maternal inflammatory response was detected in all of ACA cases | 8/26 (30.77%) |
| Placenta weight < 10th centile | All cases of small placenta were detected in IHC SARS-CoV-2-negative placenta subgroup | 7/26 (26.92%) |
| Fetal vascular malperfusion (FVM) | Detected FVM included abnormal placental insertion site or hypercoiling of the umbilical cord with subsequent low-grade global FVM morphologically manifested as small foci of karyorrhectic villi | 6/26 (23.07%) |
| Chronic chorionitis of fetal membranes | Mild chronic chorionitis of fetal membranes with CD3/CD8-positive inflammatory infiltrate was diagnosed, without morphologic evidence of villitis of unknown etiology | 2/26 (7.69%) |
| Maternal vascular malperfusion (MVM) | One case of segmental MVM manifested by single villous infarct involving <5% of placental parenchyma was found | 1/26 (3.84%) |
| No morphological abnormalities | All cases with no morphologic abnormalities were detected in IHC-SARS-CoV-2-negative placental subgroup | 7/26 (26.92%) |
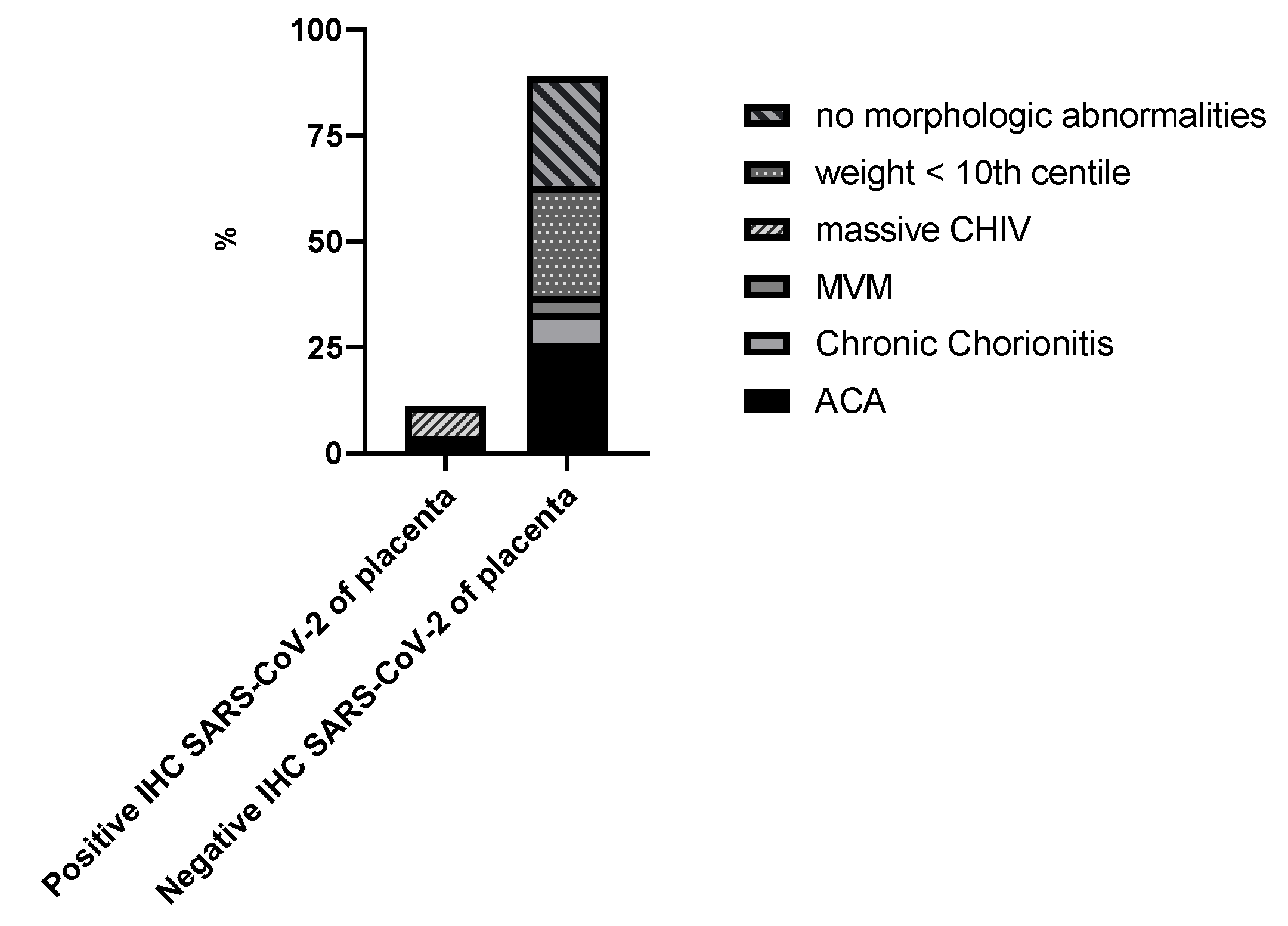
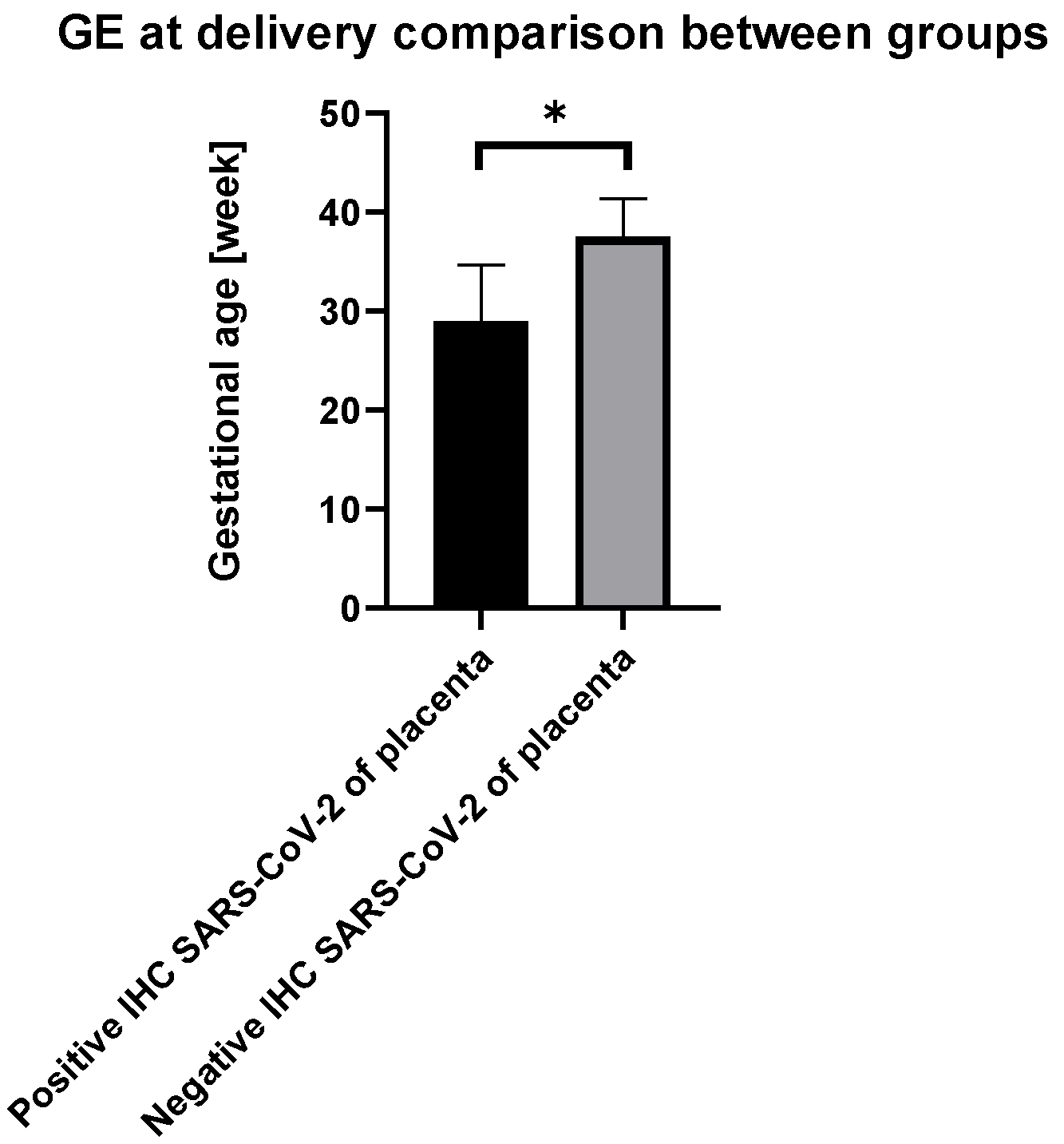
| Additional notes regarding positive placental SARS-CoV-2 status in IHC | All placentas with positive SARS-CoV-2 status in IHC (n = 2/2; 100%) had MCHI. In all these cases adverse perinatal outcomes were found, one with intrauterine fetal demise and one with low Apgar score. One of SARS-CoV-2-positive placentas had ACA co-existing. Morphologic features of MVM or FVM were not detected in that subgroup. In any placenta with negative IHC SARS-CoV-2 status, morphologic features of chronic histiocytic intervillositis were not diagnosed. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pomorski, M.; Trzeszcz, M.; Matera-Witkiewicz, A.; Krupińska, M.; Fuchs, T.; Zimmer, M.; Zimmer-Stelmach, A.; Rosner-Tenerowicz, A.; Budny-Wińska, J.; Tarczyńska-Podraza, A.; et al. SARS-CoV-2 Infection and Pregnancy: Maternal and Neonatal Outcomes and Placental Pathology Correlations. Viruses 2022, 14, 2043. https://doi.org/10.3390/v14092043
Pomorski M, Trzeszcz M, Matera-Witkiewicz A, Krupińska M, Fuchs T, Zimmer M, Zimmer-Stelmach A, Rosner-Tenerowicz A, Budny-Wińska J, Tarczyńska-Podraza A, et al. SARS-CoV-2 Infection and Pregnancy: Maternal and Neonatal Outcomes and Placental Pathology Correlations. Viruses. 2022; 14(9):2043. https://doi.org/10.3390/v14092043
Chicago/Turabian StylePomorski, Michał, Martyna Trzeszcz, Agnieszka Matera-Witkiewicz, Magdalena Krupińska, Tomasz Fuchs, Mariusz Zimmer, Aleksandra Zimmer-Stelmach, Anna Rosner-Tenerowicz, Joanna Budny-Wińska, Anna Tarczyńska-Podraza, and et al. 2022. "SARS-CoV-2 Infection and Pregnancy: Maternal and Neonatal Outcomes and Placental Pathology Correlations" Viruses 14, no. 9: 2043. https://doi.org/10.3390/v14092043
APA StylePomorski, M., Trzeszcz, M., Matera-Witkiewicz, A., Krupińska, M., Fuchs, T., Zimmer, M., Zimmer-Stelmach, A., Rosner-Tenerowicz, A., Budny-Wińska, J., Tarczyńska-Podraza, A., Radziejewska, K., Królak-Olejnik, B., Szczygieł, A., Augustyniak-Bartosik, H., Kuriata-Kordek, M., Skalec, K., Smoła, I., Morgiel, E., Gawryś, J., ... Madziarska, K. (2022). SARS-CoV-2 Infection and Pregnancy: Maternal and Neonatal Outcomes and Placental Pathology Correlations. Viruses, 14(9), 2043. https://doi.org/10.3390/v14092043