
Changes in Prevalence and Seasonality of Pathogens Identified in Acute Respiratory Tract Infections in Hospitalised Individuals in Rural and Urban Settings in South Africa; 2018–2022
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Sample Size
2.3. Specimen Collection and Processing
2.4. Nucleic Acid Extraction
2.5. Multiplex Real-Time PCR for Nucleic Acids Extracted from Nasopharyngeal and Oropharyngeal Swabs
2.6. Data Analysis and Management
3. Results
3.1. Enrolment and Baseline Characteristics
3.2. Detection of Respiratory Pathogens in NP/OP Swabs from RTI Cases
3.3. Association between Age, Province, and the Prevalence of Respiratory Pathogens among Cases Relative to Controls
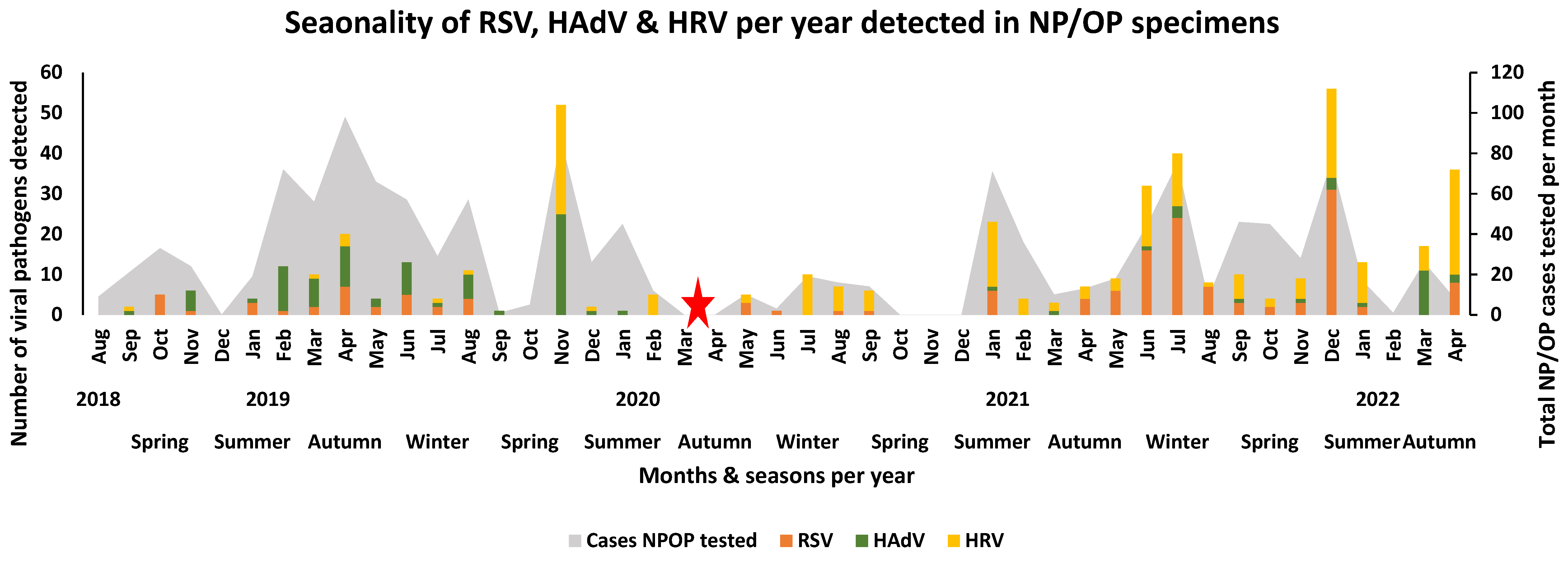
3.4. Seasonality of Respiratory Pathogens Detected in NP/OP Swabs of Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Troeger, C.; Blacker, B.; Khalil, I.A.; Rao, P.C.; Cao, J.; Zimsen, S.R.; Albertson, S.B.; Deshpande, A.; Farag, T.; Abebe, Z. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef]
- Dheda, K.; Gumbo, T.; Maartens, G.; Dooley, K.E.; Murray, M.; Furin, J.; Nardell, E.A.; Warren, R.M.; Esmail, A.; Nardell, E. The Lancet Respiratory Medicine Commission: 2019 update: Epidemiology, pathogenesis, transmission, diagnosis, and management of multidrug-resistant and incurable tuberculosis. Lancet Respir. Med. 2019, 7, 820–826. [Google Scholar] [CrossRef]
- Nicholson, K.G.; Kent, J.; Hammersley, V.; Cancio, E. Acute viral infections of upper respiratory tract in elderly people living in the community: Comparative, prospective, population based study of disease burden. BMJ 1997, 315, 1060–1064. [Google Scholar] [CrossRef]
- Grief, S.N. Upper respiratory infections. Prim. Care Clin. Off. Pract. 2013, 40, 757–770. [Google Scholar] [CrossRef]
- Arroll, B.; Kenealy, T.; Falloon, K. Are antibiotics indicated as an initial treatment for patients with acute upper respiratory tract infections? A review. N. Z. Med. J. 2008, 121, 64–70. [Google Scholar]
- Wolter, N.; Tempia, S.; Cohen, C.; Madhi, S.A.; Venter, M.; Moyes, J.; Walaza, S.; Malope-Kgokong, B.; Groome, M.; du Plessis, M. High nasopharyngeal pneumococcal density, increased by viral coinfection, is associated with invasive pneumococcal pneumonia. J. Infect. Dis. 2014, 210, 1649–1657. [Google Scholar] [CrossRef]
- Murray, J.; Cohen, A.; Walaza, S.; Groome, M.; Madhi, S.; Variava, E.; Kahn, K.; Dawood, H.; Tempia, S.; Tshangela, A. Determining the provincial and national burden of influenza-associated severe acute respiratory illness in South Africa using a rapid assessment methodology. PLoS ONE 2015, 10, e0132078. [Google Scholar] [CrossRef]
- Cohen, C.; Walaza, S.; Treurnicht, F.K.; McMorrow, M.; Madhi, S.A.; McAnerney, J.M.; Tempia, S. In-and out-of-hospital mortality associated with seasonal and pandemic influenza and respiratory syncytial virus in South Africa, 2009–2013. Clin. Infect. Dis. 2018, 66, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Tempia, S.; Walaza, S.; Moyes, J.; Cohen, A.L.; Von Mollendorf, C.; Treurnicht, F.K.; Venter, M.; Pretorius, M.; Hellferscee, O.; Mtshali, S. Risk factors for influenza-associated severe acute respiratory illness hospitalization in South Africa, 2012–2015. In Open Forum Infectious Diseases; Oxford University Press: Oxford, UK, 2017; p. ofw262. [Google Scholar]
- Pal, M.; Berhanu, G.; Desalegn, C.; Kandi, V. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2): An update. Cureus 2020, 12, e7423. [Google Scholar] [CrossRef] [PubMed]
- Pillai, J.; Motloba, P.; Motaung, K.; Ozougwu, L.; Ikalafeng, B.; Marinda, E.; Lukhele, M.; Basu, D. The effect of lockdown regulations on SARS-CoV-2 infectivity in Gauteng Province, South Africa. SAMJ South Afr. Med. J. 2020, 110, 1119–1123. [Google Scholar] [CrossRef] [PubMed]
- Schubert, G.; Achi, V.; Ahuka, S.; Belarbi, E.; Bourhaima, O.; Eckmanns, T.; Johnstone, S.; Kabore, F.; Kra, O.; Mendes, A. The African network for improved diagnostics, epidemiology and management of common infectious agents. BMC Infect. Dis. 2021, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- El Bcheraoui, C.; Mimche, H.; Miangotar, Y.; Krish, V.S.; Ziegeweid, F.; Krohn, K.J.; Ekat, M.H.; Nansseu, J.R.; Dimbuene, Z.T.; Olsen, H.E. Burden of disease in francophone Africa, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Glob. Health 2020, 8, e341–e351. [Google Scholar] [CrossRef]
- Giandhari, J.; Pillay, S.; Wilkinson, E.; Tegally, H.; Sinayskiy, I.; Schuld, M.; Lourenço, J.; Chimukangara, B.; Lessells, R.; Moosa, Y. Early transmission of SARS-CoV-2 in South Africa: An epidemiological and phylogenetic report. Int. J. Infect. Dis. 2021, 103, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Perofsky, A.C.; Tempia, S.; Bingham, J.; Maslo, C.; Toubkin, M.; Laubscher, A.; Walaza, S.; Pulliam, J.R.; Viboud, C.; Cohen, C. Direct and Indirect Effects of the Coronavirus Disease 2019 Pandemic on Private Healthcare Utilization in South Africa, March 2020–September 2021. Clin. Infect. Dis. 2022, 75, e1000–e1010. [Google Scholar] [CrossRef]
- McCarthy, K.M.; Tempia, S.; Kufa, T.; Kleynhans, J.; Wolter, N.; Jassat, W.; Ebonwu, J.; Von Gottberg, A.; Erasmus, L.; Muchengeti, M. The importation and establishment of community transmission of SARS-CoV-2 during the first eight weeks of the South African COVID-19 epidemic. EClinicalMedicine 2021, 39, 101072. [Google Scholar] [CrossRef] [PubMed]
- du Plessis, E.; van Niekerk, D.; Rosenkranz, B.; Preiser, W. After the COVID-19 state of disaster in South Africa. Nat. Hum. Behav. 2022, 6, 901. [Google Scholar] [CrossRef]
- Moonasar, D.; Pillay, A.; Leonard, E.; Naidoo, R.; Mngemane, S.; Ramkrishna, W.; Jamaloodien, K.; Lebese, L.; Chetty, K.; Bamford, L. COVID-19: Lessons and experiences from South Africa’s first surge. BMJ Glob. Health 2021, 6, e004393. [Google Scholar] [CrossRef]
- Kenmoe, S.; Tcharnenwa, C.; Monamele, G.C.; Kengne, C.N.; Ripa, M.N.; Whitaker, B.; Alroy, K.A.; Balajee, S.A.; Njouom, R. Comparison of FTD® respiratory pathogens 33 and a singleplex CDC assay for the detection of respiratory viruses: A study from Cameroon. Diagn. Microbiol. Infect. Dis. 2019, 94, 236–242. [Google Scholar] [CrossRef]
- O’Brien, K.L.; Baggett, H.C.; Brooks, W.A.; Feikin, D.R.; Hammitt, L.L.; Higdon, M.M.; Howie, S.R.; Knoll, M.D.; Kotloff, K.L.; Levine, O.S. Causes of severe pneumonia requiring hospital admission in children without HIV infection from Africa and Asia: The PERCH multi-country case-control study. Lancet 2019, 394, 757–779. [Google Scholar] [CrossRef]
- Tempia, S.; Walaza, S.; Moyes, J.; Cohen, A.L.; Von Mollendorf, C.; McMorrow, M.L.; Treurnicht, F.K.; Venter, M.; Pretorius, M.; Hellferscee, O. Attributable fraction of influenza virus detection to mild and severe respiratory illnesses in HIV-infected and HIV-uninfected patients, South Africa, 2012–2016. Emerg. Infect. Dis. 2017, 23, 1124. [Google Scholar] [CrossRef]
- Pretorius, M.A.; Tempia, S.; Walaza, S.; Cohen, A.L.; Moyes, J.; Variava, E.; Dawood, H.; Seleka, M.; Hellferscee, O.; Treurnicht, F. The role of influenza, RSV and other common respiratory viruses in severe acute respiratory infections and influenza-like illness in a population with a high HIV sero-prevalence, South Africa 2012–2015. J. Clin. Virol. 2016, 75, 21–26. [Google Scholar] [CrossRef]
- Sundell, N.; Andersson, L.-M.; Brittain-Long, R.; Lindh, M.; Westin, J. A four year seasonal survey of the relationship between outdoor climate and epidemiology of viral respiratory tract infections in a temperate climate. J. Clin. Virol. 2016, 84, 59–63. [Google Scholar] [CrossRef]
- Staadegaard, L.; Caini, S.; Wangchuk, S.; Thapa, B.; de Almeida, W.A.F.; de Carvalho, F.C.; Fasce, R.A.; Bustos, P.; Kyncl, J.; Novakova, L. Defining the seasonality of respiratory syncytial virus around the world: National and subnational surveillance data from 12 countries. Influenza Other Respir. Viruses 2021, 15, 732–741. [Google Scholar] [CrossRef]
- Gessner, B.D.; Shindo, N.; Briand, S. Seasonal influenza epidemiology in sub-Saharan Africa: A systematic review. Lancet Infect. Dis. 2011, 11, 223–235. [Google Scholar] [CrossRef]
- Lee, H.; Lee, H.; Song, K.-H.; Kim, E.S.; Park, J.S.; Jung, J.; Ahn, S.; Jeong, E.K.; Park, H.; Kim, H.B. Impact of public health interventions on seasonal influenza activity during the COVID-19 outbreak in Korea. Clin. Infect. Dis. 2021, 73, e132–e140. [Google Scholar] [CrossRef]
- Tempia, S.; Walaza, S.; Bhiman, J.N.; McMorrow, M.L.; Moyes, J.; Mkhencele, T.; Meiring, S.; Quan, V.; Bishop, K.; McAnerney, J.M. Decline of influenza and respiratory syncytial virus detection in facility-based surveillance during the COVID-19 pandemic, South Africa, January to October 2020. Eurosurveillance 2021, 26, 2001600. [Google Scholar] [CrossRef] [PubMed]
- Jassat, W.; Mudara, C.; Ozougwu, L.; Tempia, S.; Blumberg, L.; Davies, M.-A.; Pillay, Y.; Carter, T.; Morewane, R.; Wolmarans, M. Difference in mortality among individuals admitted to hospital with COVID-19 during the first and second waves in South Africa: A cohort study. Lancet Glob. Health 2021, 9, e1216–e1225. [Google Scholar] [CrossRef]
- Kuitunen, I.; Artama, M.; Mäkelä, L.; Backman, K.; Heiskanen-Kosma, T.; Renko, M. Effect of social distancing due to the COVID-19 pandemic on the incidence of viral respiratory tract infections in children in Finland during early 2020. Pediatr. Infect. Dis. J. 2020, 39, e423–e427. [Google Scholar] [CrossRef] [PubMed]
- Nolen, L.D.; Seeman, S.; Bruden, D.; Klejka, J.; Desnoyers, C.; Tiesinga, J.; Singleton, R. Impact of social distancing and travel restrictions on non-coronavirus disease 2019 (non-COVID-19) respiratory hospital admissions in young children in Rural Alaska. Clin. Infect. Dis. 2021, 72, 2196–2198. [Google Scholar] [CrossRef]
- Cissé, A.; Milucky, J.; Ilboudo, A.K.; Waller, J.L.; Bicaba, B.; Medah, I.; Mirza, S.; Whitney, C.G.; Tarnagda, Z. Comparison of performance between Fast Track Diagnostics Respiratory Kit and the CDC global reference laboratory for influenza rRT-PCR panel for detection of influenza A and influenza B. Influenza Other Respir. Viruses 2021, 15, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Ntshoe, G.M.; McAnerney, J.M.; Tempia, S.; Blumberg, L.; Moyes, J.; Buys, A.; Naidoo, D.; Venter, M.; Besselaar, T.; Schoub, B.D. Influenza epidemiology and vaccine effectiveness among patients with influenza-like illness, viral watch sentinel sites, South Africa, 2005–2009. PLoS ONE 2014, 9, e94681. [Google Scholar] [CrossRef]
- Eguia, R.T.; Crawford, K.H.; Stevens-Ayers, T.; Kelnhofer-Millevolte, L.; Greninger, A.L.; Englund, J.A.; Boeckh, M.J.; Bloom, J.D. A human coronavirus evolves antigenically to escape antibody immunity. PLoS Pathog. 2021, 17, e1009453. [Google Scholar] [CrossRef]
- Venter, M.; Lassaunière, R.; Kresfelder, T.L.; Westerberg, Y.; Visser, A. Contribution of common and recently described respiratory viruses to annual hospitalizations in children in South Africa. J. Med. Virol. 2011, 83, 1458–1468. [Google Scholar] [CrossRef]
- Leotte, J.; Trombetta, H.; Faggion, H.Z.; Almeida, B.M.; Nogueira, M.B.; Vidal, L.R.; Raboni, S.M. Impact and seasonality of human rhinovirus infection in hospitalized patients for two consecutive years. J. De Pediatr. 2017, 93, 294–300. [Google Scholar] [CrossRef]
- Basu, G.; Rossouw, J.; Sebunya, T.; Gashe, B.; De Beer, M.; Dewar, J.; Steele, A. Prevalence of rotavirus, adenovirus and astrovirus infection in young children with gastroenteritis in Gaborone, Botswana. East Afr. Med. J. 2003, 80, 652–655. [Google Scholar] [CrossRef] [PubMed]
- Dey, S.; Hoq, I.; Okitsu, S.; Hayakawa, S.; Ushijima, H. Prevalence, seasonality, and peak age of infection of enteric adenoviruses in Japan, 1995–2009. Epidemiol. Infect. 2013, 141, 958–960. [Google Scholar] [CrossRef]
- Brueggemann, A.B.; van Rensburg, M.J.J.; Shaw, D.; McCarthy, N.; Jolley, K.A.; Maiden, M.C.; van der Linden, M.P.; Amin-Chowdhury, Z.; Bennett, D.E.; Borrow, R. The invasive respiratory infection surveillance (IRIS) Initiative reveals significant reductions in invasive bacterial infections during the COVID-19 pandemic. medRxiv 2020. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1a. Overall patients enrolled and tested | ||||
|---|---|---|---|---|
| Cases (%) | Controls (%) | Total | ||
| Patients enrolled | 3121 | 939 | 4060 | |
| Patients tested | 2595 | 442 | 3037 | |
| NP/OP | Patients enrolled | 1713 (55) | 482 (51) | 2195 |
| Specimens tested | 1540 (52) | 336 (76) | 1876 | |
| 1b. Demographic characteristics of individuals with NP/OP specimens tested for respiratory pathogens | ||||
| Cases, N = 1540 (%) a | Control, N = 336 (%) a | Total | ||
| Province | Gauteng | 789 (51) | 174 (52) | 963 |
| Mpumalanga | 751 (49) | 162 (48) | 913 | |
| Year | 2018 | 178 (11.5) | 0 (0) | 178 |
| 2019 | 634 (41) | 46 (14) | 680 | |
| 2020 | 308 (20) | 42 (12) | 350 | |
| 2021 | 412 (27) | 174 (52) | 586 | |
| 2022 | 8 (0.5) | 74 (22) | 82 | |
| Age | <1 years | 603 (39) | 45 (13) | 648 |
| 1–4 years | 367 (24) | 60 (18) | 427 | |
| 5–14 years | 67 (4) | 57 (17) | 124 | |
| 15–54 years | 277 (18) | 150 (45) | 427 | |
| ≥55 years | 222 (14) | 24 (7) | 246 | |
| Gender | Male | 736 (48) | 176 (52) | 912 |
| Female | 789 (51) | 158 (47) | 944 | |
| RTI Cases | Years, n (%), N = 1540 | ||||||
|---|---|---|---|---|---|---|---|
| 2018 | 2019 | 2020 | 2021 | 2022 | Total | p-Value a | |
| Viral Pathogens | |||||||
| HAdV | 17 (1.10) | 79 (5.12) | 12 (0.78) | 18 (1.17) | 1 (0.06) | 127 (8.24) | 0.000 * |
| HboV | 16 (1.03) | 76 (4.92) | 3 (0.19) | 19 (1.23) | 1 (0.06) | 115 (7.46) | 0.000 * |
| hCoV 229e | 37 (2.40) | 148 (9.61) | 2 (0.12) | 0 (0) | 0 (0) | 187 (12.14) | 0.000 * |
| hCoV HKU1 | 1 (0.06) | 22 (1.42) | 1 (0.06) | 0 (0) | 0 (0) | 24 (1.55) | 0.000 * |
| hCoV NL63 | 1 (0.06) | 19 (1.22) | 2 (0.12) | 7 (0.45) | 0 (0) | 29 (1.88) | 0.077 |
| hCoV OC43 | 4 (0.25) | 8 (0.52) | 8 (0.51) | 10 (0.64) | 0 (0) | 30 (1.94) | 0.447 |
| EV | 6 (0.38) | 9 (0.58) | 15 (0.97) | 8 (0.52) | 0 (0) | 38 (2.46) | 0.045 |
| IAV | 3 (0.19) | 45 (2.92) | 1 (0.06) | 15 (0.97) | 1 (0.06) | 65 (4.22) | 0.000 * |
| IAV H1N1 | 2 (0.12) | 8 (0.51) | 0 (0) | 13 (0.84) | 1 (0.06) | 24 (1.55) | 0.002 * |
| IBV | 35 (2.27) | 6 (0.39) | 0 (0) | 7 (0.45) | 0 (0) | 48 (3.11) | 0.000 * |
| ICV | 4 (0.25) | 5 (0.32) | 3 (0.19) | 1 (0.06) | 0 (0) | 13 (0.84) | 0.159 |
| HMPV A&B | 9 (0.58) | 30 (1.94) | 10 (0.64) | 20 (1.29) | 0 (0) | 69 (4.48) | 0.779 |
| HPIV 1 | 6 (0.38) | 13 (0.84) | 4 (0.25) | 3 (0.19) | 0 (0) | 26 (1.68) | 0.165 |
| HPIV 2 | 2 (0.13) | 8 (0.52) | 0 (0) | 1 (0.06) | 0 (0) | 11 (0.71) | 0.117 |
| HPIV 3 | 9 (0.58) | 23 (1.49) | 1 (0.06) | 21 (1.36) | 0 (0) | 54 (3.51) | 0.001 * |
| HPIV 4 | 9 (0.58) | 19 (1.23) | 11 (0.71) | 7 (0.45) | 0 (0) | 46 (2.98) | 0.208 |
| HpeV | 3 (0.19) | 11 (0.71) | 6 (0.38) | 3 (0.19) | 0 (0) | 23 (1.49) | 0.507 |
| HRV | 3 (0.19) | 49 (3.18) | 114 (7.40) | 61 (3.96) | 1 (0.06) | 228 (14.80) | 0.000 * |
| RSV | 12 (0.77) | 30 (1.94) | 48 (3.11) | 86 (5.58) | 0 (0) | 176 (11.42) | 0.000 * |
| Bacterial Pathogens | |||||||
| Haemophilus influenzae | 59 (3.83) | 199 (12.92) | 72 (4.67) | 71 (4.61) | 5 (0.32) | 406 (26.33) | 0.000 * |
| Haemophilus influenzae b | 4 (0.25) | 3 (0.19) | 2 (0.12) | 4 (0.25) | 0 (0) | 13 (0.84) | 0.214 |
| Bordetella spp. | 7 (0.45) | 124 (8.05) | 4 (0.24) | 1 (0.06) | 0 (0) | 136 (8.83) | 0.000 * |
| Chlamydophila pneumoniae | 47 (3.05) | 152 (9.87) | 0 (0) | 0 (0) | 0 (0) | 199 (12.92) | 0.000 * |
| Klesiella pneumoniae | 62 (0.38) | 203 (12.18) | 26 (1.68) | 22 (1.42) | 1 (0.06) | 314 (20.39) | 0.000 * |
| Legionella | 2 (0.13) | 4 (0.25) | 2 (0.12) | 0 (0) | 0 (0) | 8 (0.52) | 0.220 |
| Moraxella catarrhalis | 18 (1.17) | 48 (3.11) | 84 (5.45) | 91 (5.90) | 1 (0.06) | 242 (15.71) | 0.000 * |
| Mycoplasma pneumoniae | 4 (0.25) | 53 (3.44) | 1 (0.06) | 0 (0) | 0 (0) | 58 (3.76) | 0.000 * |
| Pneumocystis jirovecii | 12 (0.77) | 34 (2.20) | 27 (1.75) | 15 (0.97) | 0 (0) | 88 (5.71) | 0.057 |
| Salmonella | 1 (0.06) | 4 (0.25) | 1 (0.06) | 0 (0) | 0 (0) | 6 (0.38) | 0.394 |
| Staphylococcus aureus | 36 (2.33) | 167 (10.84) | 98 (6.36) | 108 (7.01) | 1(0.06) | 410 (26.62) | 0.067 |
| Streptococcus pneumoniae | 43 (2.79) | 177 (11.49) | 103 (6.68) | 116 (7.53) | 0 (0) | 439 (28.50) | 0.072 |
| Respiratory Pathogens | Cases (%); n = 1540 | Controls (%); n = 336 | Univariate Logistic Regression | Multivariate Logistic Regression Controlling for Age and Site | ||||
|---|---|---|---|---|---|---|---|---|
| ORa | 95% CI | p-Value | OR | 95% CI | p-Value | |||
| HAdV | 127 (8.3) | 12 (3.6) | 2.41 | 1.32–4.41 | 0.004 | 1.8 | 0.97–3.33 | 0.06 |
| HboV | 115 (7.5) | 11 (3.3) | 2.37 | 1.26–4.45 | 0.007 | 1.95 | 1.03–3.68 | 0.041 |
| HRV | 228 (14.8) | 22 (6.6) | 2.46 | 1.56–3.88 | 0 | 2.01 | 1.32–3.32 | 0.002 * |
| RSV | 176 (11.4) | 3 (0.9) | 14.24 | 4.52–44.85 | 0 | 11.36 | 3.59–35.97 | <0.001 * |
| hCoV 229e | 187 (12.1) | 2 (0.6) | 22.94 | 5.67–92.89 | 0 | 18.91 | 4.66–79.75 | <0.001 * |
| hCoV HKU1 | 24 (1.6) | 2 (0.6) | 2.63 | 0.62–11.17 | 0.191 | 2.66 | 0.62–11.47 | 0.188 |
| hCoV NL63 | 29 (1.9) | 4 (1.2) | 1.58 | 0.55–4.53 | 0.392 | 1.23 | 0.43–3.57 | 0.7 |
| hCoV OC43 | 30 (2.0) | 4 (1.2) | 1.64 | 0.57–4.68 | 0.356 | 1.42 | 0.49–4.10 | 0.519 |
| EV | 38 (2.5) | 11 (3.3) | 1.03 | 0.70–1.52 | 0.865 | 0.95 | 0.66–1.35 | 0.766 |
| IAV | 65 (4.2) | 0 (0.0) | omitted | omitted | ||||
| IAV H1N1 | 24 (1.6) | 2 (0.6) | 2.63 | 0.62–11.17 | 0.19 | 2.16 | 0.50–9.27 | 0.301 |
| IBV | 48 (3.1) | 1 (0.3) | 10.71 | 1.47–77.89 | 0.019 | 12.02 | 1.64–88.01 | 0.014 * |
| ICV | 13 (0.8) | 4 (1.2) | 0.7 | 0.23–2.17 | 0.539 | 0.69 | 0.22–2.18 | 0.53 |
| HMPV A&B | 69 (4.5) | 4 (1.2) | 3.87 | 1.40–10.68 | 0.009 | 2.85 | 1.02–7.91 | 0.045 * |
| HPIV 1 | 26 (1.7) | 1 (0.3) | 5.72 | 0.77–42.29 | 0.088 | 5.62 | 0.75–42.42 | 0.092 |
| HPIV 2 | 11 (0.7) | 0 (0.0) | omitted | omitted | ||||
| HPIV 3 | 54 (3.5) | 5 (1.5) | 2.39 | 0.95–6.02 | 0.064 | 1.68 | 0.66–4.27 | 0.278 |
| HPIV 4 | 46 (3.0) | 7 (2.1) | 1.44 | 0.64–3.21 | 0.376 | 1.3 | 0.57–2.95 | 0.53 |
| HPeV | 23 (1.5) | 0 (0.0) | omitted | omitted | ||||
| Bordetella | 136 (8.8) | 1 (0.3) | 32.26 | 4.49–231.48 | 0.001 | 23.04 | 3.20–165.91 | 0.002 * |
| Chlamydophila pneumoniae | 199 (12.9) | 1 (0.3) | 49.42 | 6.90–353.83 | 0 | 38.44 | 5.36–275.85 | <0.001 * |
| Haemophilus influenzae | 406 (26.4) | 34 (10.1) | 3.16 | 2.18–4.59 | 0 | 2.69 | 1.84–0.92 | 0 |
| Haemophilus influenzae b | 13 (0.8) | 2 (0.6) | 1.41 | 0.32–6.29 | 0.65 | 1.48 | 0.32–6.8 | 0.612 |
| Klebsiella pneumoniae | 314 (20.4) | 17 (5.1) | 4.78 | 2.89–7.90 | 0 | 4.25 | 2.56–7.06 | <0.001 * |
| Legionella | 8 (0.5) | 0 (0.0) | omitted | omitted | ||||
| Moraxella catarrhalis | 242 (15.7) | 48 (14.3) | 1.11 | 0.79–1.55 | 0.539 | 0.84 | 0.59–1.19 | 0.333 |
| Mycoplasma pneumoniae | 58 (3.8) | 1 (0.3) | 13.03 | 1.80–94.42 | 0.011 | 9.19 | 0.26–66.88 | 0.028 |
| Pneumocystis jirovecii | 88 (5.7) | 4 (1.2) | 5 | 1.82–13.72 | 0.002 | 5.12 | 1.85–14.14 | 0.002 * |
| Salmonella | 6 (0.4) | 2 (0.6) | 0.65 | 0.13–3.23 | 0.598 | 0.64 | 0.12–3.3 | 0.591 |
| Staphylococcus aureus | 410 (26.6) | 56 (16.7) | 1.8 | 1.32–2.45 | 0 | 1.66 | 1.21–2.26 | 0.002 * |
| Streptococcus pneumoniae | 439 (28.5) | 54 (16.1) | 2.07 | 1.51–2.82 | 0 | 1.67 | 1.21–2.30 | 0.002 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davids, M.; Johnstone, S.; Mendes, A.; Brecht, G.; Avenant, T.; du Plessis, N.; de Villiers, M.; Page, N.; Venter, M. Changes in Prevalence and Seasonality of Pathogens Identified in Acute Respiratory Tract Infections in Hospitalised Individuals in Rural and Urban Settings in South Africa; 2018–2022. Viruses 2024, 16, 404. https://doi.org/10.3390/v16030404
Davids M, Johnstone S, Mendes A, Brecht G, Avenant T, du Plessis N, de Villiers M, Page N, Venter M. Changes in Prevalence and Seasonality of Pathogens Identified in Acute Respiratory Tract Infections in Hospitalised Individuals in Rural and Urban Settings in South Africa; 2018–2022. Viruses. 2024; 16(3):404. https://doi.org/10.3390/v16030404
Chicago/Turabian StyleDavids, Michaela, Siobhan Johnstone, Adriano Mendes, Gadean Brecht, Theunis Avenant, Nicolette du Plessis, Maryke de Villiers, Nicola Page, and Marietjie Venter. 2024. "Changes in Prevalence and Seasonality of Pathogens Identified in Acute Respiratory Tract Infections in Hospitalised Individuals in Rural and Urban Settings in South Africa; 2018–2022" Viruses 16, no. 3: 404. https://doi.org/10.3390/v16030404
APA StyleDavids, M., Johnstone, S., Mendes, A., Brecht, G., Avenant, T., du Plessis, N., de Villiers, M., Page, N., & Venter, M. (2024). Changes in Prevalence and Seasonality of Pathogens Identified in Acute Respiratory Tract Infections in Hospitalised Individuals in Rural and Urban Settings in South Africa; 2018–2022. Viruses, 16(3), 404. https://doi.org/10.3390/v16030404