
Topical Photodynamic Therapy with Different Forms of 5-Aminolevulinic Acid in the Treatment of Actinic Keratosis


 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Study Formulations
2.3. Treatment Protocol
2.3.1. Application of Study Formulations
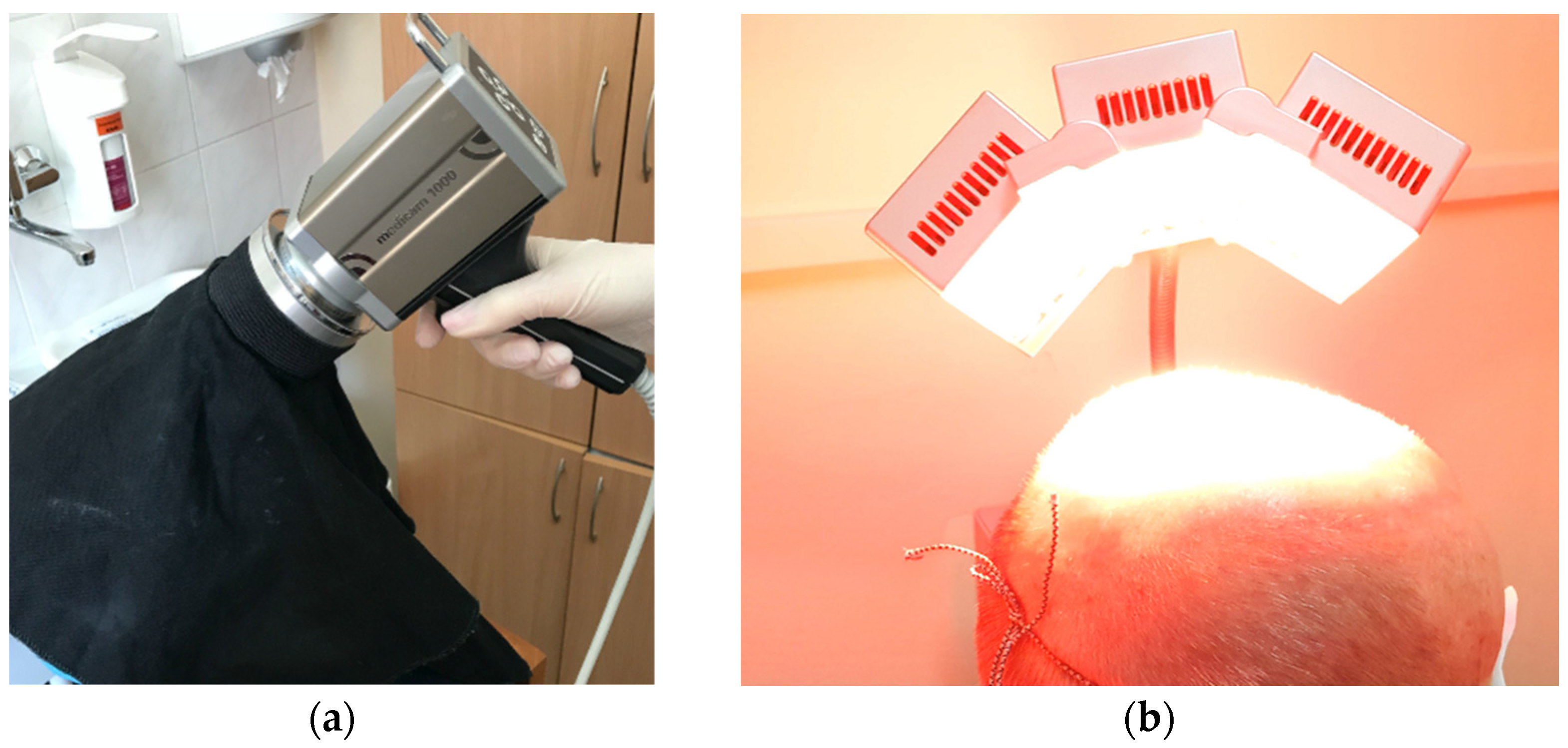
2.3.2. Assessment of Skin Fluorescence Following Application of Study Formulations
2.3.3. Irradiation with Red Light 630 ± 5 nm
2.3.4. PDT with Study Formulations Efficacy Assessment
2.3.5. PDT with Study Formulations Cosmetic Outcome and Patient Satisfaction Assessment
2.3.6. PDT with Study Formulations Tolerability Assessment
2.4. Statistical Methods
3. Results
3.1. Characteristics of the Study Group
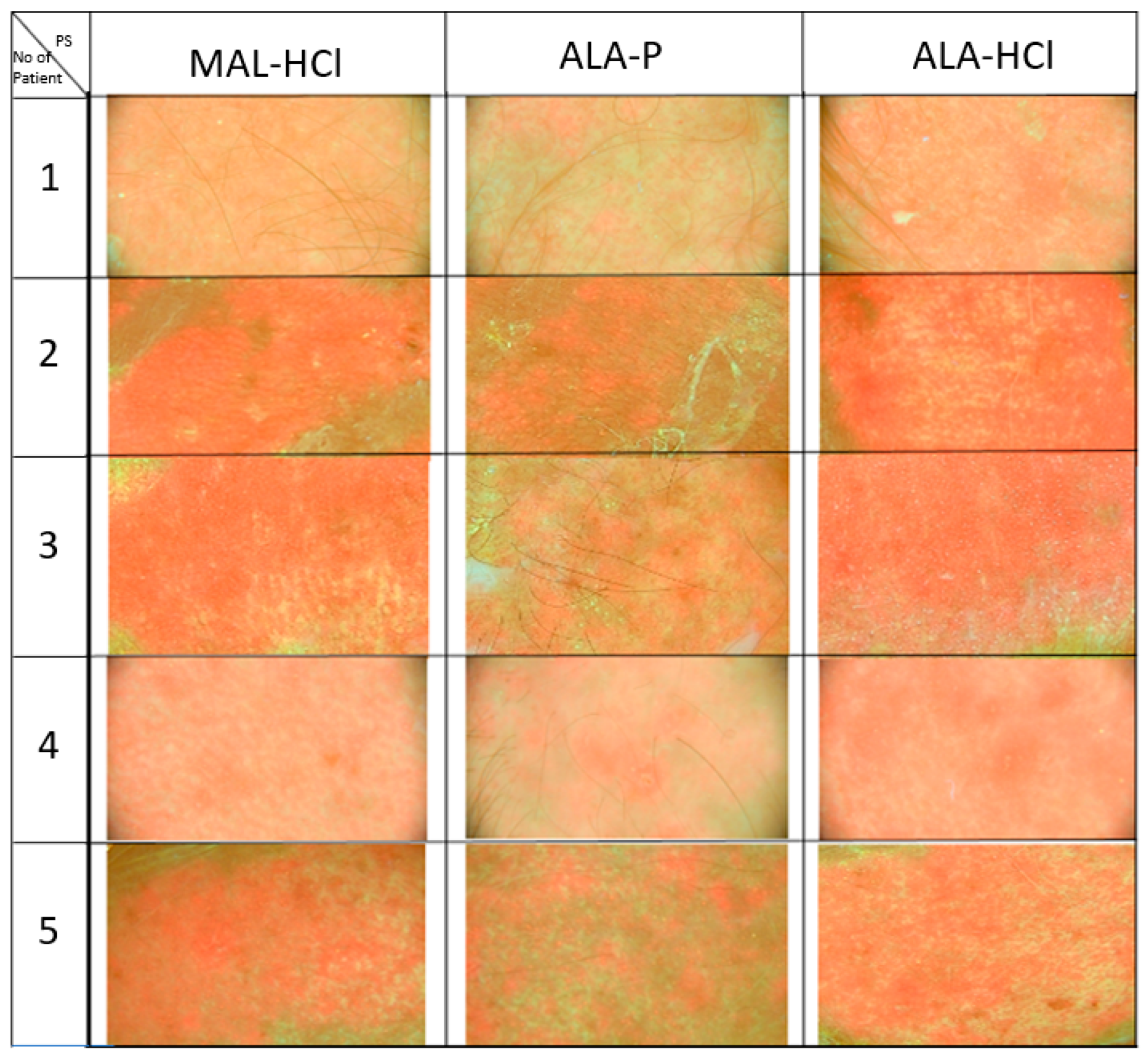
3.2. Fluorescence Assessment Following Application of Study Formulations
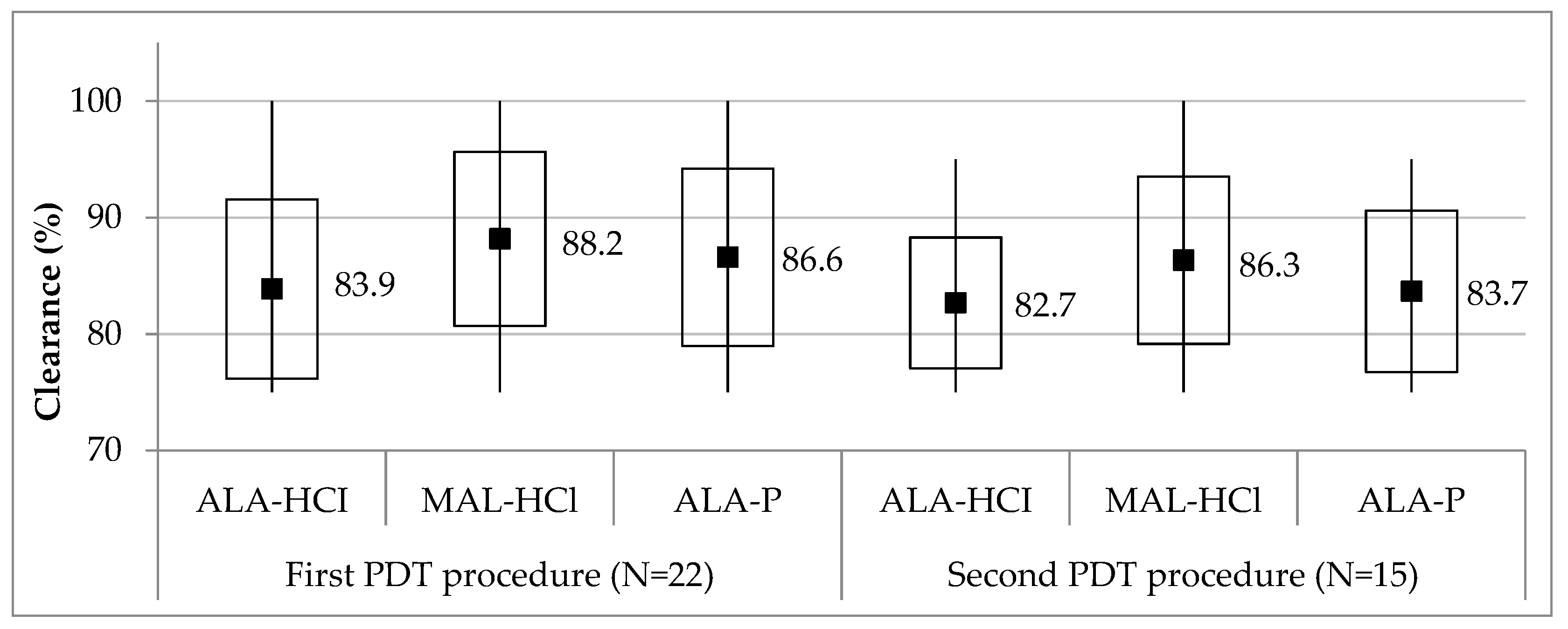
3.3. PDT with Study Formulations Efficacy
3.4. PDT with Study Formulations COSMETIC Outcome and Patient Satisfaction
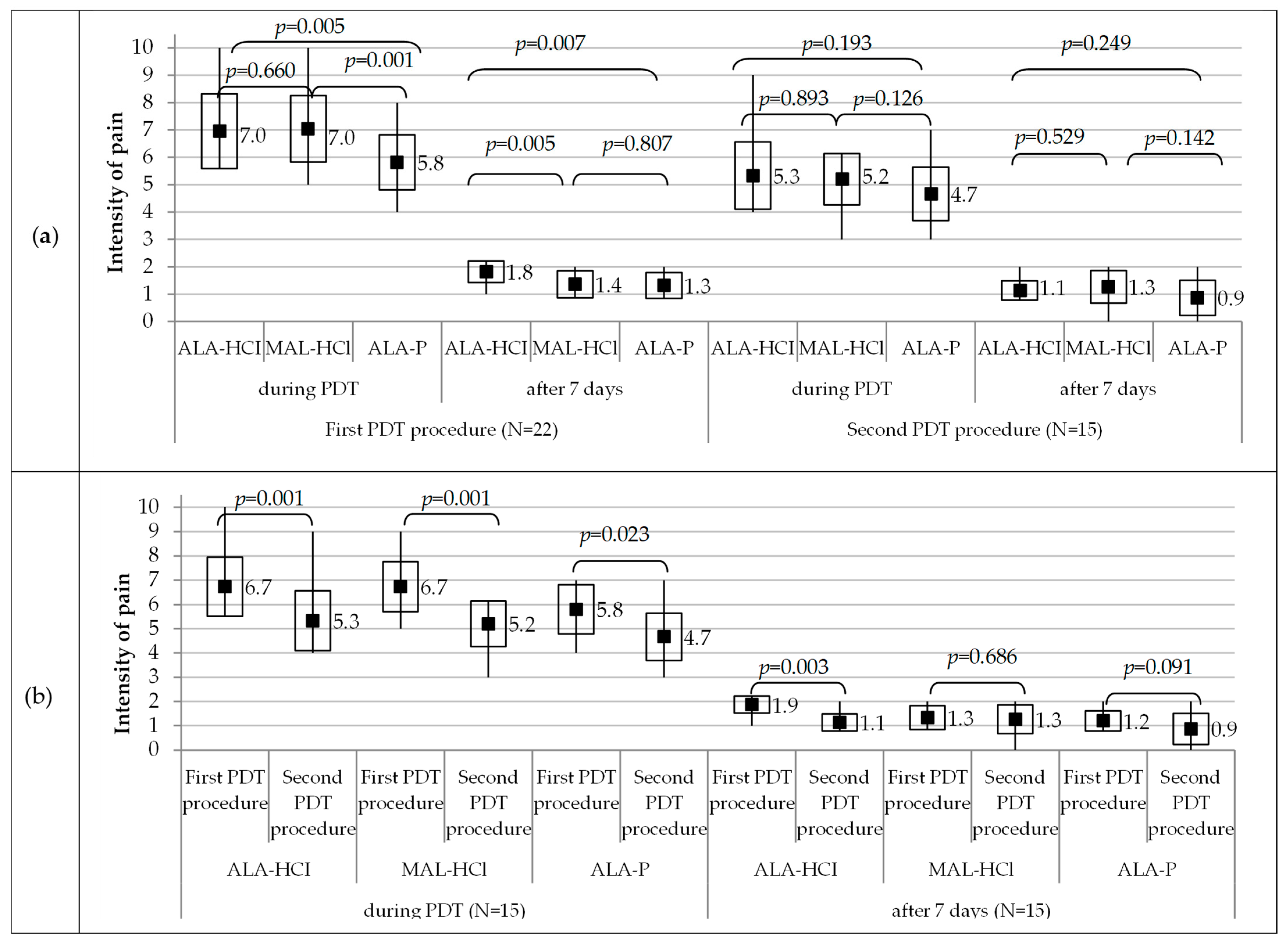
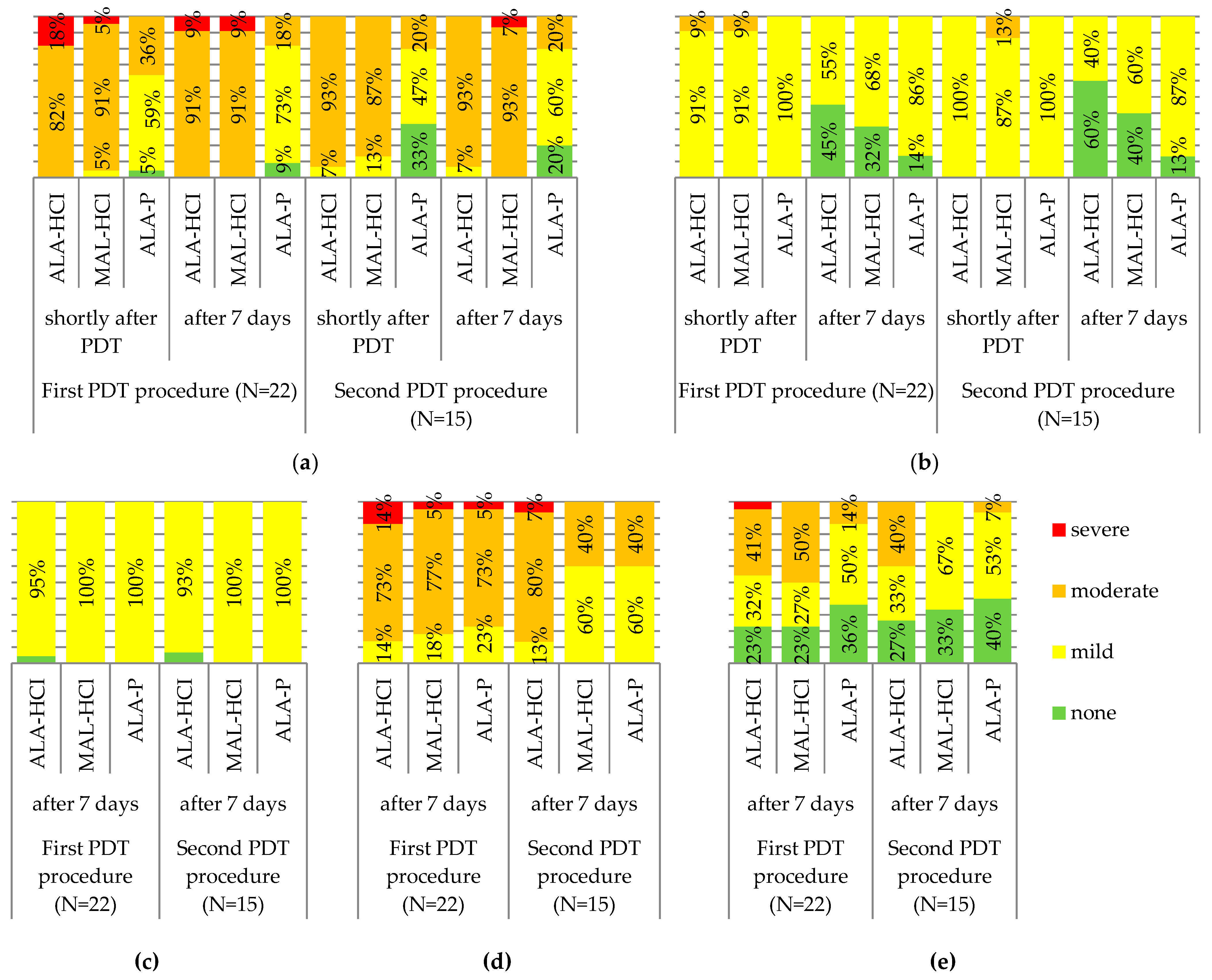
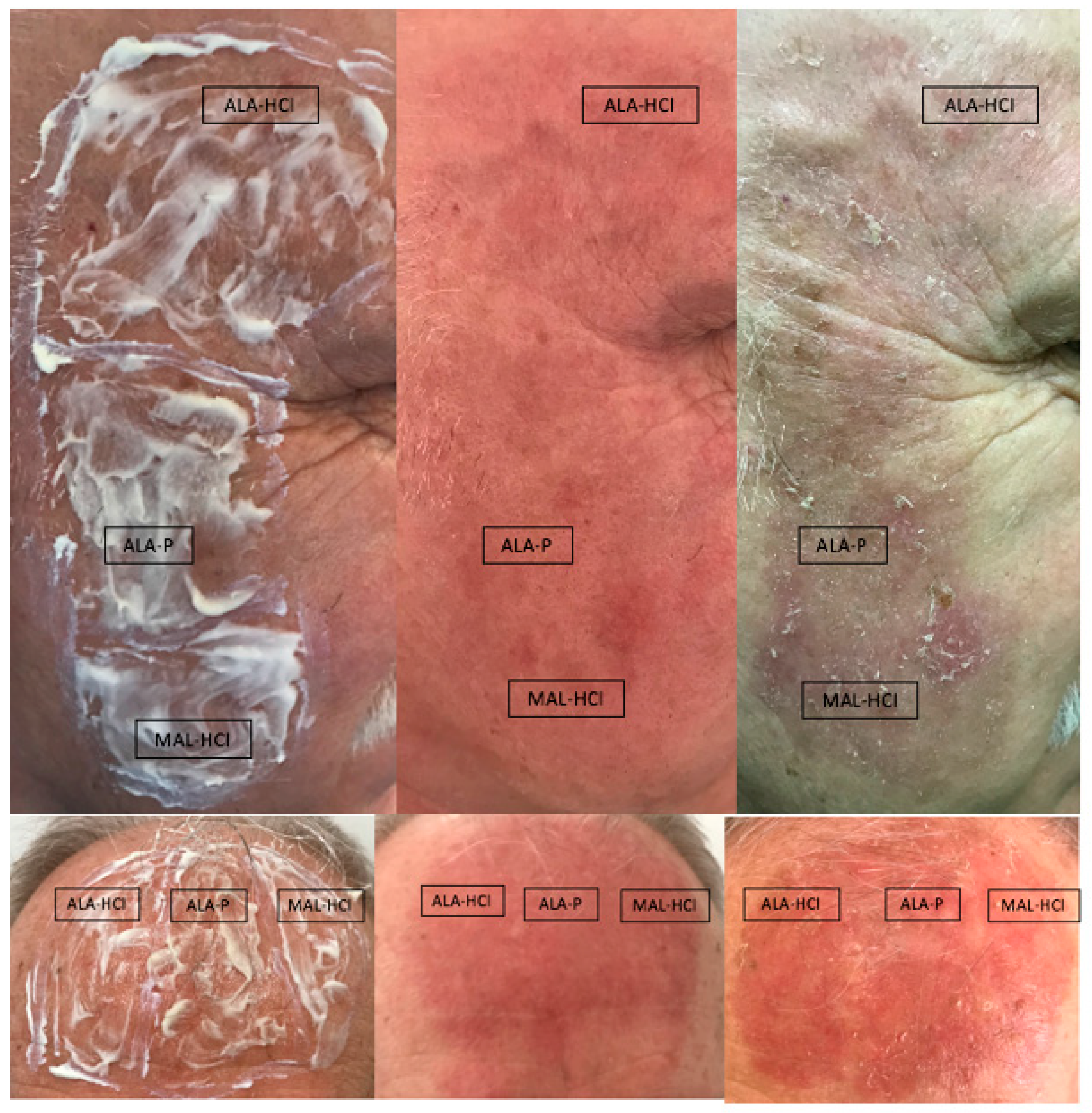
3.5. PDT with Study Formulations Tolerability
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Linos, E.; Katz, K.A.; Colditz, G.A. Skin cancer-the importance of prevention. JAMA Intern. Med. 2016, 176, 1435–1436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, X.; Elkin, E.E.; Marghoob, A.A. Burden of basal cell carcinoma in USA. Future Oncol. 2015, 11, 2967–2974. [Google Scholar] [CrossRef] [PubMed]
- Combalia, A.; Carrera, C. Squamous cell carcinoma: An update on diagnosis and treatment. Dermatol. Pract. Concept. 2020, 10, e2020066. [Google Scholar] [CrossRef] [PubMed]
- Dianzani, C.; Conforti, C.; Giuffrida, R.; Corneli, P.; di Meo, N.; Farinazzo, E.; Moret, A.; Magaton Rizzi, G.; Zalaudek, I. Current therapies for actinic keratosis. Int. J. Dermatol. 2020, 59, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Criscione, V.D.; Weinstock, M.A.; Naylor, M.F.; Luque, C.; Eide, M.J.; Bingham, S.F. Department of veteran affairs topical tretinoin chemoprevention trial group. Actinic keratoses: Natural history and risk of malignant transformation in the veterans affairs topical tretinoin chemoprevention trial. Cancer 2009, 115, 2523–2530. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Figueras, M.T.; Carrato, C.; Sáenz, X.; Puig, L.; Musulen, E.; Ferrándiz, C.; Ariza, A. Actinic keratosis with atypical basal cells (AK I) is the most common lesion associated with invasive squamous cell carcinoma of the skin. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Stockfleth, E. From a new vision of actinic keratosis to imiquimod 3.75%, the new treatment standard. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1–2. [Google Scholar] [CrossRef]
- Jetter, N.; Chandan, N.; Wang, S.; Tsoukas, M. Field cancerization therapies for management of actinic keratosis: A narrative review. Am. J. Clin. Dermatol. 2018, 19, 543–557. [Google Scholar] [CrossRef]
- Kwaśny, M. Photodynamic therapy in dermatology. Forum. Derm. 2018, 4, 138–147. [Google Scholar] [CrossRef]
- Piquero-Casals, J.; Morgado-Carrasco, D.; Gilaberte, Y.; Del Rio, R.; Macaya-Pascual, A.; Granger, C.; López-Estebaranz, J.L. Management pearls on the treatment of actinic keratoses and field cancerization. Dermatol. Ther. 2020, 10, 903–915. [Google Scholar] [CrossRef]
- Ritter, C.G.; Kuhl, I.C.; Lenhardt, C.; Weissbluth, M.L.; Bakos, R.M. Photodynamic therapy with delta-aminolevulinic acid and light-emitting diodes in actinic keratosis. An. Bras. Dermatol. 2010, 85, 639–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conforti, C.; Corneli, P.; Harwood, C.; Zalaudek, I. Evolving role of systemic therapies in non-melanoma skin cancer. Clin. Oncol. 2019, 31, 759–768. [Google Scholar] [CrossRef] [PubMed]
- Champeau, M.; Vignoud, S.; Mortier, L.; Mordon, S. Photodynamic therapy for skin cancer: How to enhance drug penetration? J. Photochem. Photobiol. B 2019, 197, 111544. [Google Scholar] [CrossRef] [PubMed]
- Yazdanyar, S.; Zarchi, K.; Jemec, G.B.E. Pain during topical photodynamic therapy—Comparing methyl aminolevulinate (Metvix ®) to aminolaevulinic acid (Ameluz ®); an intra-individual clinical study. Photodiagnosis. Photodyn. Ther. 2017, 20, 6–9. [Google Scholar] [CrossRef] [PubMed]
- National Center for Biotechnology Information. PubChem Compound Summary for CID 24737828, Aminolevulinic Acid Phosphate. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Aminolevulinic-acid-phosphate (accessed on 6 August 2021).
- Al-Saber, F.; Aldosari, W.; Alselaiti, M.; Khalfan, H.; Kaladari, A.; Khan, G.; Harb, G.; Rehani, R.; Kudo, S.; Koda, A.; et al. The safety and tolerability of 5-aminolevulinic acid phosphate with sodium ferrous citrate in patients with type 2 diabetes mellitus in Bahrain. J. Diabetes Res. 2016, 2016, 8294805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higashikawa, F.; Kanno, K.; Ogata, A.; Sugiyama, M. Reduction of fatigue and anger-hostility by the oral administration of 5-aminolevulinic acid phosphate: A randomized, double-blind, placebo-controlled, parallel study. Sci. Rep. 2020, 10, 16004. [Google Scholar] [CrossRef]
- Tarstedt, M.; Gillstedt, M.; Wennberg Larkö, A.M.; Paoli, J. Aminolevulinic acid and methyl aminolevulinate equally effective in topical photodynamic therapy for non-melanoma skin cancers. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 420–423. [Google Scholar] [CrossRef]
- Ezzedine, K.; Painchault, C.; Brignone, M. Systematic literature review and network meta-analysis of the efficacy and acceptability of interventions in Actinic Keratoses. Acta Derm.-Venereol. 2021, 101, adv00358. [Google Scholar] [CrossRef]
- Moloney, F.J.; Collins, P. Randomized, double-blind, prospective study to compare topical 5-aminolaevulinic acid methylester with topical 5-aminolaevulinic acid photodynamic therapy for extensive scalp actinic keratosis. Br. J. Dermatol. 2007, 157, 87–91. [Google Scholar] [CrossRef]
- Fu, C.; Kuang, B.H.; Qin, L.; Zeng, X.Y.; Wang, B.C. Efficacy and safety of photodynamic therapy with amino-5-laevulinate nanoemulsion versus methyl-5-aminolaevulinate for actinic keratosis: A meta-analysis. Photodiagnosis. Photodyn. Ther. 2019, 27, 408–414. [Google Scholar] [CrossRef]
- Patel, G.; Armstrong, A.W.; Eisen, D.B. Efficacy of photodynamic therapy vs other interventions in randomized clinical trials for the treatment of actinic keratoses: A systematic review and meta-analysis. JAMA Dermatol. 2014, 150, 1281–1288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, D.Y.; Kim, K.H.; Song, K.H. Comparative study of photodynamic therapy with topical methyl aminolevulinate versus 5-aminolevulinic acid for facial actinic keratosis with long-term follow-up. Ann. Dermatol. 2014, 26, 321–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Räsänen, J.; Neittaanmäki, N.; Ylitalo, L.; Hagman, J.; Rissanen, P.; Ylianttila, L.; Salmivuori, M.; Snellman, E.; Grönroos, M. DL-PDT for AK: Multicentre trial comparing BF-200 ALA with MAL. Br. J. Dermatol. 2019, 181, e37. [Google Scholar] [CrossRef] [Green Version]
- Menezes, P.F.; Requena, M.B.; Bagnato, V.S. Optimization of photodynamic therapy using negative pressure. Photomed. Laser. Surg. 2014, 32, 296–301. [Google Scholar] [CrossRef] [Green Version]
- Blanco, K.C.; Moriyama, L.T.; Inada, N.M.; Sálvio, A.G.; Menezes, P.F.C.; Leite, E.J.S.; Kurachi, C.; Bagnato, V.S. Fluorescence guided PDT for optimization of the outcome of skin cancer treatment. Front. Phys. 2015, 3, 30. [Google Scholar] [CrossRef] [Green Version]
- Foged, C.; Philipsen, P.A.; Wulf, H.C.; Haedersdal, M.; Togsverd-Bo, K. Skin surface protoporphyrin IX fluorescence is associated with epidermal but not dermal fluorescence intensities. Photodiagnosis. Photodyn. Ther. 2020, 30, 101681. [Google Scholar] [CrossRef] [PubMed]
- Godin, B.; Touitou, E. Transdermal skin delivery: Predictions for humans from in vivo, ex vivo and animal models. Adv. Drug Deliv. Rev. 2007, 59, 1152–1161. [Google Scholar] [CrossRef]
- Rodriguez, L.; de Bruijn, H.S.; Di Venosa, G.; Mamone, L.; Robinson, D.J.; Juarranz, A.; Batlle, A.; Casas, A. Porphyrin synthesis from aminolevulinic acid esters in endothelial cells and its role in photodynamic therapy. J. Photochem. Photobiol. B 2009, 96, 249–254. [Google Scholar] [CrossRef]
- Takahashi, O.; Kirikoshi, R.; Manabe, N. Racemization of serine residues catalyzed by dihydrogen phosphate ion: A computational study. Catalysts 2017, 7, 363. [Google Scholar] [CrossRef] [Green Version]
- Dyakin, V.V.; Wisniewski, T.M.; Lajtha, A. Racemization in post-translational modifications relevance to protein aging, aggregation and neurodegeneration: Tip of the iceberg. Symmetry 2021, 13, 455. [Google Scholar] [CrossRef]
- Borgia, F.; Giuffrida, R.; Caradonna, E.; Vaccaro, M.; Guarneri, F.; Cannavò, S.P. Early and late onset side effects of photodynamic therapy. Biomedicines 2018, 6, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warren, C.B.; Karai, L.J.; Vidimos, A.; Maytin, E.V. Pain associated with aminolevulinic acid-photodynamic therapy of skin disease. J. Am. Acad. Dermatol. 2009, 61, 1033–1043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serra-Guillén, C.; Nagore, E.; Bancalari, E.; Kindem, S.; Sanmartín, O.; Llombart, B.; Requena, C.; Serra-Guillén, I.; Calomarde, L.; Diago, A.; et al. A randomized intraindividual comparative study of methyl-5-aminolaevulinate vs. 5-aminolaevulinic acid nanoemulsion (BF-200 ALA) in photodynamic therapy for actinic keratosis of the face and scalp. Br. J. Dermatol. 2018, 179, 1410–1411. [Google Scholar] [CrossRef] [PubMed]
- Räsänen, J.E.; Neittaanmäki, N.; Ylitalo, L.; Hagman, J.; Rissanen, P.; Ylianttila, L.; Salmivuori, M.; Snellman, E.; Grönroos, M. 5-aminolaevulinic acid nanoemulsion is more effective than methyl-5-aminolaevulinate in daylight photodynamic therapy for actinic keratosis: A nonsponsored randomized double-blind multicentre trial. Br. J. Dermatol. 2019, 181, 265–274. [Google Scholar] [CrossRef]
- Szeimies, R.M.; Calzavara-Pinton, P. A randomized, double-blind trial comparing 5-aminolaevulinic acid nanoemulsion with methyl 5-aminolaevulinate in daylight photodynamic therapy for actinic keratosis. Br. J. Dermatol. 2019, 181, 223–224. [Google Scholar] [CrossRef]
- Lee, P.K.; Kloser, A. Current methods for photodynamic therapy in the US: Comparison of MAL/PDT and ALA/PDT. J. Drugs Dermatol. 2013, 12, 925–930. [Google Scholar]
- Dirschka, T.; Radny, P.; Dominicus, R.; Mensing, H.; Brüning, H.; Jenne, L.; Karl, L.; Sebastian, M.; Oster-Schmidt, C.; Klövekorn, W.; et al. AK-CT002 Study Group. Photodynamic therapy with BF-200 ALA for the treatment of actinic keratosis: Results of a multicentre, randomized, observer-blind phase III study in comparison with a registered methyl-5-aminolaevulinate cream and placebo. Br. J. Dermatol. 2012, 166, 137–146. [Google Scholar] [CrossRef]
- Dirschka, T.; Ekanayake-Bohlig, S.; Dominicus, R.; Aschoff, R.; Herrera-Ceballos, E.; Botella-Estrada, R.; Hunfeld, A.; Kremser, M.; Schmitz, B.; Lübbert, H.; et al. A randomized, intraindividual, non-inferiority, Phase III study comparing daylight photodynamic therapy with BF-200 ALA gel and MAL cream for the treatment of actinic keratosis. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 288–297. [Google Scholar] [CrossRef]
- Olsen, E.A.; Abernethy, M.L.; Kulp-Shorten, C.; Callen, J.P.; Glazer, S.D.; Huntley, A.; McCray, M.; Monroe, A.B.; Tschen, E.; Wolf, J.E., Jr. A double-blind, vehicle-controlled study evaluating masoprocol cream in the treatment of actinic keratoses on the head and neck. J. Am. Acad. Dermatol. 1991, 24, 738–743. [Google Scholar] [CrossRef]
- Ibbotson, S.H.; Valentine, R.; Hearn, R. Is the pain of topical photodynamic therapy with methyl aminolevulinate any different from that with 5-aminolaevulinic acid? Photodermatol. Photoimmunol. Photomed. 2012, 28, 272–273. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade | Definition |
|---|---|
| Poor | extensive occurrence of scarring, atrophy, or induration |
| Fair | slight to moderate occurrence of scarring, atrophy, or induration |
| Good | no scarring, atrophy, or induration, moderate redness or increase in pigmentation compared with adjacent skin |
| Excellent | no scarring, atrophy, or induration, slight or no redness or change in pigmentation compared with adjacent skin |
| Variable | Category | Parameter | Estimate |
|---|---|---|---|
| Age | years | Min-max | 60–84 |
| Sex | male | n (%) | 21 (95%) |
| female | 1 (5%) | ||
| Localizations of lesions | face | n (%) | 4 (18%) |
| scalp | 18 (82%) | ||
| Thickness grade, according to Olsen et al. [14] | I grade (thin) | n (%) | 9 (24%) |
| II grade (moderately thick) | 18 (49%) | ||
| III grade (thick) | 10 (27%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartosińska, J.; Szczepanik-Kułak, P.; Raczkiewicz, D.; Niewiedzioł, M.; Gerkowicz, A.; Kowalczuk, D.; Kwaśny, M.; Krasowska, D. Topical Photodynamic Therapy with Different Forms of 5-Aminolevulinic Acid in the Treatment of Actinic Keratosis. Pharmaceutics 2022, 14, 346. https://doi.org/10.3390/pharmaceutics14020346
Bartosińska J, Szczepanik-Kułak P, Raczkiewicz D, Niewiedzioł M, Gerkowicz A, Kowalczuk D, Kwaśny M, Krasowska D. Topical Photodynamic Therapy with Different Forms of 5-Aminolevulinic Acid in the Treatment of Actinic Keratosis. Pharmaceutics. 2022; 14(2):346. https://doi.org/10.3390/pharmaceutics14020346
Chicago/Turabian StyleBartosińska, Joanna, Paulina Szczepanik-Kułak, Dorota Raczkiewicz, Marta Niewiedzioł, Agnieszka Gerkowicz, Dorota Kowalczuk, Mirosław Kwaśny, and Dorota Krasowska. 2022. "Topical Photodynamic Therapy with Different Forms of 5-Aminolevulinic Acid in the Treatment of Actinic Keratosis" Pharmaceutics 14, no. 2: 346. https://doi.org/10.3390/pharmaceutics14020346
APA StyleBartosińska, J., Szczepanik-Kułak, P., Raczkiewicz, D., Niewiedzioł, M., Gerkowicz, A., Kowalczuk, D., Kwaśny, M., & Krasowska, D. (2022). Topical Photodynamic Therapy with Different Forms of 5-Aminolevulinic Acid in the Treatment of Actinic Keratosis. Pharmaceutics, 14(2), 346. https://doi.org/10.3390/pharmaceutics14020346