4. Discussion
In situ gels are in solution form during application. Depending on the environment’s temperature, pH, or ion balance conditions, they become gel in the application area. Thus, the residence time in the target tissue is increased. The bioavailability of drugs applied topically to the eye is low due to ocular barriers. In situ gelling systems are often preferred to increase bioavailability. The dilution of the drug, which gels after it is applied to the eye, with the tear film slows down, and the elimination effect of nasolacrimal drainage is reduced. Thus, the contact time and bioavailability of drugs with ocular tissues are increased. In this study, we developed thermosensitive in situ gels of PSC-loaded TPGS micelles that we had previously developed and optimized. While designing our formulas, we determined Poloxamer 407 and Poloxamer 188 as the main gelling agents.
Although Poloxamer 407 is a thermosensitive copolymer with the rheological properties expected from a gel, it does not have good mucoadhesive properties. For this reason, it may lose its gelling ability as soon as it is diluted with tear film after application [
42]. To prevent this situation, the rate of poloxamer 407 used in the formulation can be increased. However, when used at 20–30% (
w/
w) ratios, the T
sol/gel value is below room temperature. This is also another undesirable situation. In this combined use, either poloxamer 188, which is thermosensitive itself, or mucoadhesive polymers such as different derivatives of methylcellulose and Carbopols are preferred. We tried both options in our pre-formulation studies.
Poloxamer 188 is used at a rate of ≥20% (
w/
w), the T
sol/gel value rises above 40 °C and cannot exhibit the rheological properties expected from a gel [
10]. For this reason, it is common practice in many studies to use Poloxamer 407 in combination with poloxamer 188 at appropriate rates to bring the T
sol/gel value to the physiological range. We determined the rates of poloxamer 407 and 188 used in our study as 15–20% (
w/
v). Since our polymer usage ratio is determined as weight/volume, the T
sol/gel temperature values of formulations are compatible with previous studies using poloxamer 407 and 188 at similar rates [
43]. Although the T
sol/gel value of an in situ gel to be applied ocular may differ in some sources, it is expected to be in the range of 30–35 °C. In our studies, the formulation containing a single 20% (
w/
v) poloxamer 407 gave results in this range.
In combining different mucoadhesive polymers with Poloxamer 407, another pillar of pre-formulation studies, we used different types of HPMC (50M, 60M, and 75HD100), MC, NaCMC, and Carbopol 980. It was observed that the formulations using 75HD100 HPMC, MC, NaCMC, and Carbopol 980 did not become gel at temperatures exceeding 75 °C, and/or did not have a clear appearance. The absence of gelation is thought to be due to the high T
sol/gel temperatures of the auxiliary gelling agents used [
44,
45]. Although Carbopol 980 is a pH-sensitive gelling agent, it is used in combination with Poloxamer 407 due to its excellent mucoadhesive properties. Thus, with the synergistic effect combining from both polymers, an in situ gel that is both thermosensitive and pH-sensitive is obtained. However, gelation was not observed at the physiological temperatures and pHs at the rates used. By increasing the Poloxamer 407 ratio, we could adjust the T
sol/gel temperature to the desired ranges. However, the fact that the obtained formulation was not clear was also a significant problem. Conversely, since the acidic nature of Carbopol can stimulate ocular tissues, we also avoided increasing the formulation rate [
42]. For these reasons, we also eliminated Carbopol 980 in pre-formulation studies. Perhaps the most critical finding of the pre-formulation studies was that, despite the high T
sol/gel value, we observed that HPMC (50M and 60M) formulations that gelled when used with an appropriate amount of Poloxamer 407 precipitated during scale-up. We think that this situation is also caused by NaCl. The collapse, which cannot be seen clearly when studied at small scales, can be easily observed at large scales.
We conducted studies to evaluate the effect of Poloxamer 188 in combination with mucoadhesive polymers. The results obtained in these studies with Poloxamer 188, which was used at similar rates with Poloxamer 407, were not different from those obtained with Poloxamer 407. We did not expect any gelation when using only Poloxamer 188 with a higher Tsol/gel temperature than Poloxamer 407 in formulations. However, the fact that the formulations using 75HD100 HPMC, MC, NaCMC, and Carbopol 980 did not have a clear appearance, or the precipitation in the formulations containing 50M and 60M HPMC after scale-up showed that these problems were caused by other polymers, not Poloxamers.
According to the results obtained in the pre-formulation studies, we performed further studies with formulations in the IS1-IS15 range where Poloxamer 407 and Poloxamer 188 were used alone or in combination. All formulations in the range between IS1 and IS15 had a clear appearance, and drug content was found to be ≥90%.
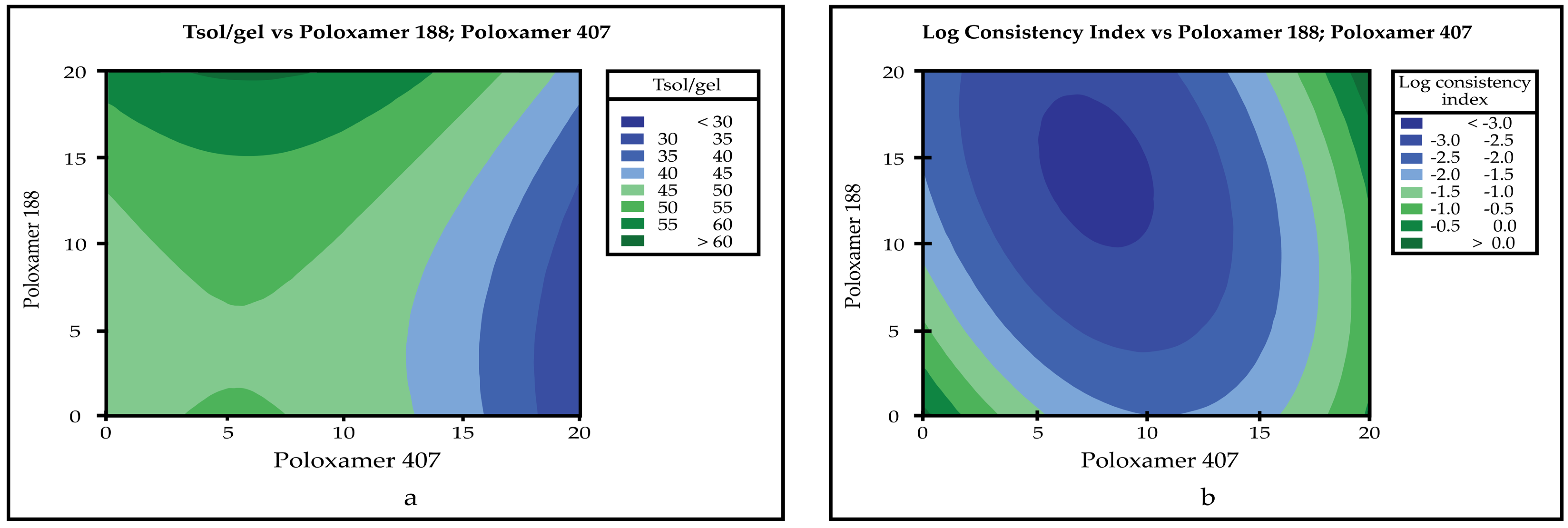
One of the critical parameters for in situ gelling systems is the gelling temperature of the formulation. It is expected that the developed formulation will transition from solution to gel form at physiological temperatures. The expected optimum T
sol/gel temperature value for in situ gels to be applied ocular is between 30–35 °C [
10]. The T
sol/gel value of all formulations developed in the IS1–IS15 range was determined. In the studies, it was seen that IS2, IS3, and IS13 showed gelation in the ocular physiological temperature range. T
sol/gel values of IS2, IS3, and IS13 were found to be 35.75, 30.36, and 35.51 °C, respectively. The data obtained are compatible with previous studies [
10,
29]. It was observed that the T
sol/gel value decreased as the Poloxamer 407 ratio in the formulations increased. In formulations containing single Poloxamer 188, gelation was not observed at physiological temperatures because the T
sol/gel value of Poloxamer 188 was high. In addition, the T
sol/gel value increased as the Poloxamer 188 ratio in the formulations increased. The changes in T
sol/gel value of formulations in the IS7-IS15 range, in which Poloxamer 407 and 188 were used in combination, were determined in parallel with the ratios of Poloxamer 407 and 188.
In situ gels are designed to switch from solution form to gel after application to the eye and increase contact time with ocular tissues. However, after application, they are eroded by tears and blinking action. For this reason, how long the formulations can maintain their integrity in the physiological environment is an important parameter that needs to be examined. Gelling capacity determination is an in vitro study performed with STF at ocular temperatures, mimicking the ocular environment. Thus, it gives preliminary information about the ability of the drug to preserve its integrity in ocular tissues. The gelation moment and complete dissolution of formulation added into STF are followed in the experiment. As soon as the formulation is completely dissolved, the experiment is terminated. In some studies, even if the formation of the gel is followed, it is recorded when the gel is completely dissolved [
27]. In some studies, grouping is made according to the rate of gel formation and dissolution time [
8]. Both gel formation rate and dissolution time are effective parameters in QbD studies. For this reason, we preferred the grouping method that examines both parameters. The studies determined that the gelling capacity was affected by the amount of both Poloxamer types used in the formulations. As the T
sol/gel temperature decreased as the amount of Poloxamer 407 increased, instant gelation was observed in the formulations we dropped into the STF in the gelling capacity studies. However, these gels formed quickly dissolved. This is due to the low gelling capacity of Poloxamer 407 when used alone less than 25% (
w/
w), as stated in the literature, and its rapid dilution with STF [
32,
42]. Since the T
sol/gel temperature was above the physiological temperature in formulations containing Poloxamer 188 alone, no gel formation was observed in the determination of gelation capacity. Similar results were obtained with T
sol/gel temperature in formulations where Poloxamer 407 and 188 were used in combination. IS13 with a T
sol/gel value of 35.51 °C gelled immediately as it was added to the STF. Another important point is that IS13 retained its gel structure for several hours, unlike IS2 and IS3. This result is compatible with the knowledge that the gelation capacity can be increased by using Poloxamer 407 in combination with Poloxamer 188, as stated in the literature [
42].
For any formulation to be applied topically, its viscosity is significant. A drug with a low viscosity can flow before it becomes gel as it is applied, or it can be quickly eliminated with the tear film. Conversely, a drug with a high viscosity cannot be applied to the eye comfortably because it is not fluid [
29]. It is important to produce a formulation with optimum viscosity to increase bioavailability in an organ with a small volume and high turnover, such as the eye. Conversely, the viscosity value of an in situ gel alone is not sufficient data to speculate about the behavior of that gel in vivo. Because viscosity studies are carried out at high speed, deformation occurs in the structure of the formulation. However, once the in situ gel is applied and spread over the eye surface, the mechanically affected parameter is the blink rate. For this reason, oscillation measurements with a low oscillation angle should be made to understand better the performance of an in situ gel in in vivo [
46]. In the light of this information, the rheological properties of in situ gels were examined in detail in this study. The rheology properties of all formulations in the IS1–IS15 range were examined at the ocular temperature, 35 °C. In rheological examinations, it was determined that all formulations showed the Herschel–Bulkley flow characteristic, which is a non-Newtonian flow type.
Hysteresis areas were calculated in thixotropy analyses. The hysteresis area usually reveals the reversibility of the formations’ response to shear, showing two different profiles: thixotropic (positive hysteresis area) or rheopectic (negative hysteresis area) [
47,
48]. When any stress is applied, a decrease in viscosity is observed in systems that show thixotropy behavior, while an increase in viscosity is observed in systems that show rheopectic behavior. After the shear stress is removed in both models, the system slowly returns to its original structures. Rheopexy is more common in colloidal dispersions. The analyses made determined that other formulations except for IS3, IS4, IS5, and IS6 showed rheopectic behavior. However, there is no significant difference between these behavioral models. Since in situ gels are defined as viscous colloidal systems [
49], these findings are compatible with the literature [
28].
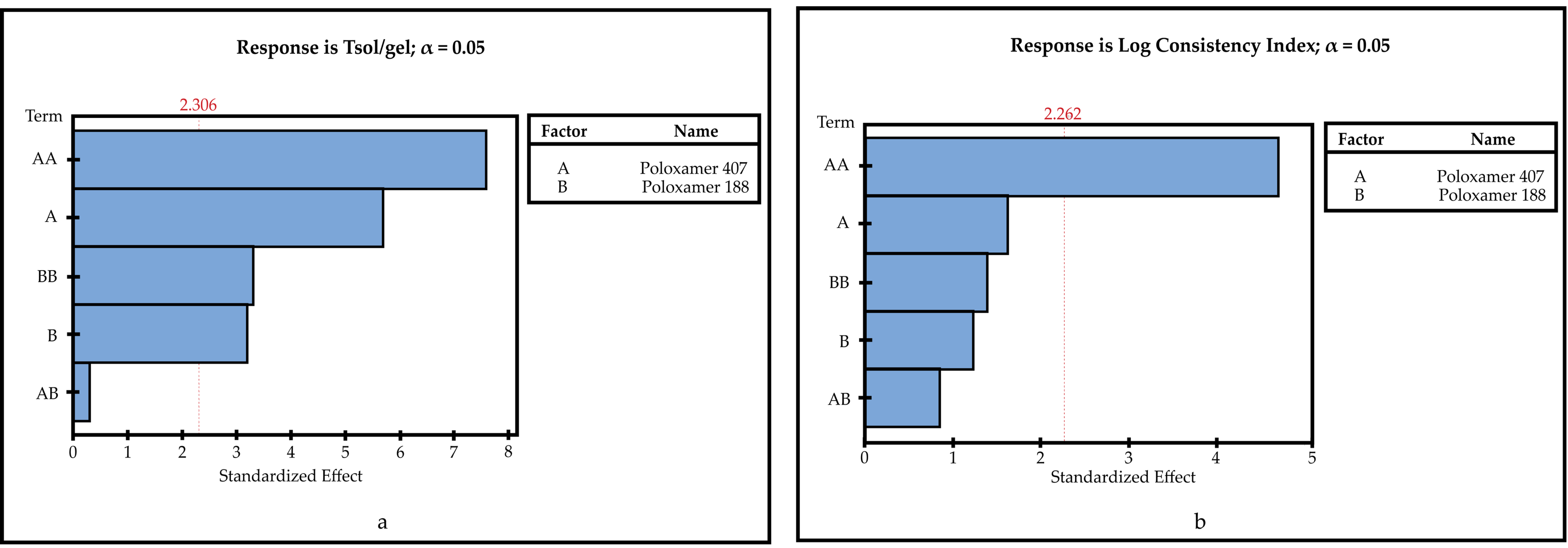
Minitab 18 evaluated the relation between CMAs and CQAs and gave the model summaries. The R2 value demonstrates how the model fits the experimental data, and if the value is close to 100%, the better the model. The adjusted R2 value is the number of terms used in the model considered, and the predicted R2 is an estimation of predicted response values of models are how well [
50]. Except for T
sol/gel temperature R2, the predicted R2 values were weak or moderate (gelling capacity 0.00%, drug content 26.60%, and log consistency index 51.60%). However, obtained R2 values of CQAs were moderate or strong 97.75% for T
sol/gel temperature, 85.88% for log consistency index, 74.81% for drug content, and 53.74% for gelling capacity. These results show that the models obtained are even more successful than the predictions.
Another analysis to understand whether the model is meaningful is the
p value. Models with a
p value less than 0.05 are significant [
51]. In this study, all models except gelling capacity (
p value is 0.159) were found to be significant (
p values< 0.05).
Pareto charts describe the statistical significance of the effects of CMAs on CQAs [
52]. When Pareto charts are examined, it is seen that the effect of both Poloxamer types on Tsol/gel and drug content are significant. The impact of Poloxamer 407 on the log consistency index is significant. However, Poloxamer 407 and Poloxamer 188 have no significant effect on gelling capacity.
Characterization studies of the optimized in situ gelling systems (IS-OPT), which we developed using Poloxamer 407 (20%
w/
v) and Poloxamer 188 (0.404%
w/
v) at the rates determined as a result of the QbD study, were performed. It was observed that IS-OPT was completely clear. The formulation was found to have a drug content of 90.97% and a gelling capacity of “++”. This result is consistent with the gelling capacity of the formulations developed for the QbD study and previous studies. An increase in gelling capacity was observed when poloxamer 407 was used in combination with an appropriate amount of Poloxamer 188 [
42]. T
sol/gel value was calculated as 31.56 °C. Considering that IS-OPT will dilute to a certain amount with tear film when applied to the eye, the T
sol/gel value was found to be 33.91 °C in the analyses made by diluting the formulation in situ gel:STF (50:7). The T
sol/gel temperature of IS-OPT, both undiluted and diluted with STF, shows that this formulation will gel at ocular temperatures when applied.
Rheological studies of the optimized formula were carried out not only at 35 °C, but also at 5 and 25 °C. Thus, an idea of the rheological properties of IS-OPT under different storage conditions was obtained. Conversely, since the rheological behaviors may vary with temperature, the optimized formula was evaluated in all aspects. In the rheology examinations, it was determined that IS-OPT showed Herschel-Bulkley flow at all temperatures (5, 25, and 35 °C), thixotropic at 5 °C, and rheopectic at 25 and 35 °C.
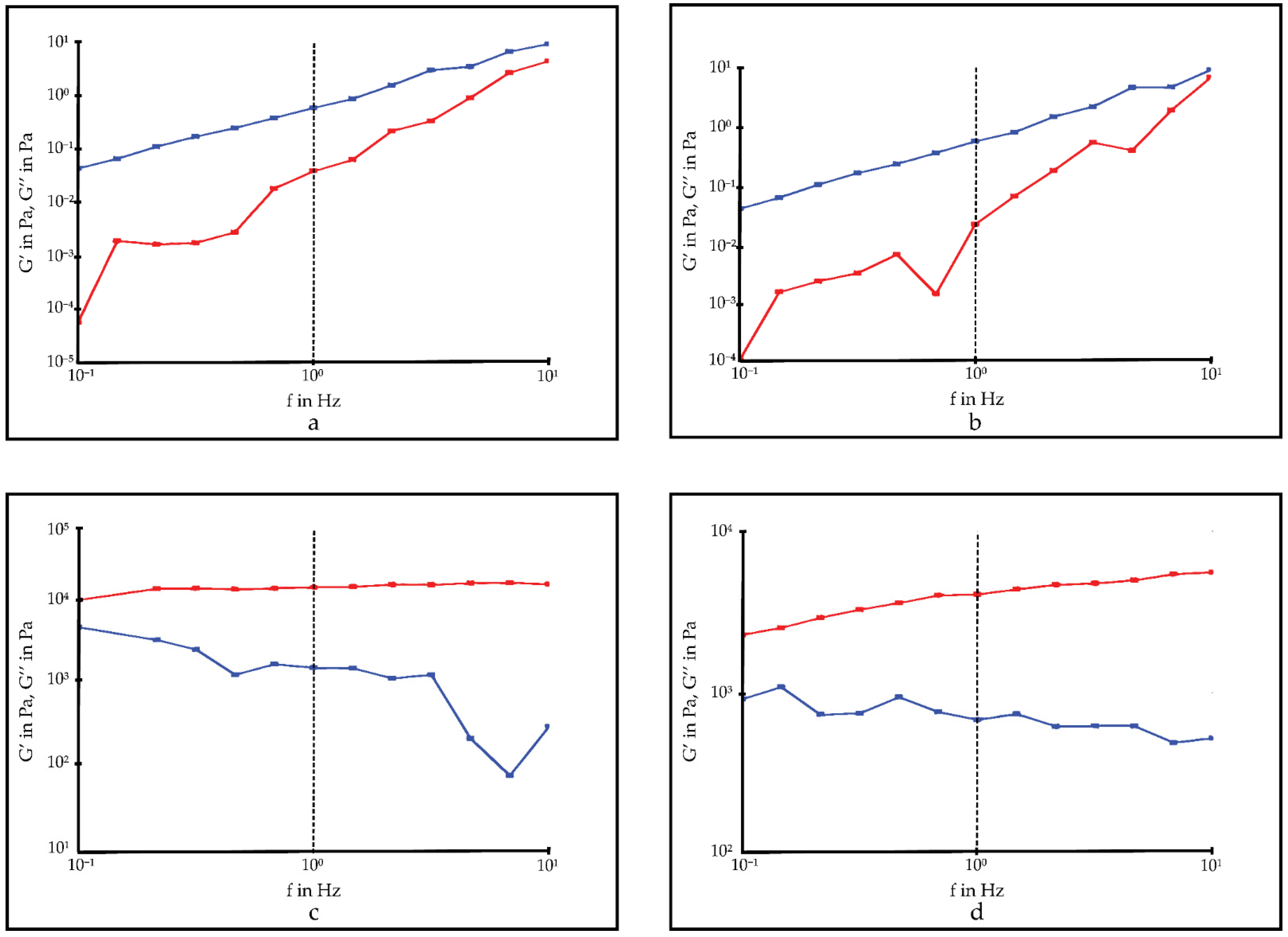
Oscillation studies are used to determine the viscoelastic properties of the drugs. It allows for determining the behavior of semisolid dosage forms in the physiological condition after administration by mimicking the physiological environment with the low shear used during analysis. The viscoelastic property affects the ease of application of a drug and its retention time in the application area. If the dose loss is minimized due to an easy administration and the contact time with the target tissue is increased, bioavailability is also observed. For this reason, it is desired that ocular drugs to be applied topically should show certain viscoelastic properties. Examining the viscoelastic property is an important R&D step in selecting the most suitable formulation for clinical use among the new ocular drugs developed [
9,
28]. Frequency sweep analyses showed G″ ˃ G′ at 5 and 25 °C. These results confirm that IS-OPT was viscoelastic. When the temperature is increased to 35 °C, a rapid increase in the G’ value is observed. This shows that a solid gel structure is formed in the formulation independent of the oscillation frequency. Estimating that IS-OPT will dilute with tear film after it is applied to the eye, oscillation studies were also performed by diluting the formulation in situ gel:STF (50:7) at 35 °C. After dilution with STF, IS-OPT was observed to form a solid gel at 35 °C. However, before dilution, as the oscillation frequency increased, the G′ value, which rose above 10
4, remained below 10
4 after dilution.
Texture profile analyses are used in the pharmaceutical field to determine the mechanical properties of dosage forms. It is used primarily for semi-solid drugs to determine parameters such as ease of removal from the package and ability of topical application and to improve the dosage form, depending on these parameters. Conversely, these mechanical properties can be directly related to in vivo sensory parameters [
53]. Thus, it is possible to obtain information about the effect of the removal the drug from the package and application comfort in terms of patient compliance, the ability of the drug to spread on the tissue surface, and its effect on elimination and bioavailability.
Hardness, one of the mechanical properties determined during TPA, indicates the force required to deform the gels. This parameter expresses the applicability of the gel to the target tissue [
54]. In some studies, it has been stated that hardness can also give an idea about the retention time of the formulation in the application area [
53,
55]. For a gel to be easily applied, it must have a low hardness value. The hardness value of IS-OPT was found to be low at all three temperatures (0.06 ± 0.00, 0.08 ± 0.00, and 0.16 ± 0.10 N for 5, 25, and 35 °C, respectively). The hardness values obtained at 5 and 25 °C gave preliminary information that the optimized formula can be easily applied to the eye. However, the situation is different at physiological temperatures. Since the formulation will become gel form after application at 35 °C, it is expected that the hardness value will increase. Thus, the drug is expected to remain undiluted and resist nasolacrimal drainage [
9]. When the results are examined, it is seen that the hardness value increased at 35 °C. Based on all the results, we can expect that IS-OPT can be easily applied to the eye and will gel after application and will be eliminated more slowly than solution-type preparations.
Compressibility, which defines the work required to compress the product over a given distance, refers to the ease with which the gel is removed from the package and spread at the site of application. The compressibility value should be low such that the gel can be removed from the container and spread easily over the mucosal epithelium [
54]. Although the compressibility value of IS-OPT increased with temperature, it was found to be low for all three temperatures (0.26 ± 0.03, 0.39 ± 0.06, and 1.58 ± 0.15 N.mm for 5, 25, and 35 °C, respectively). Compressibility is a parallel value with hardness. For this reason, it is expected to be low at 5 and 25 °C where the hardness is low. However, since the formulation will turn into gel form at 35 °C, its compressibility is expected to increase. Although the compressibility value of IS-OPT increased with temperature, it was also found to be low for 5 and 25 °C. These findings are consistent with previous studies [
28].
Adhesiveness is defined as the work required to overcome the attractive forces that occur between the surface of the sample and the surface of the probe during analysis. It represents the adhesion of semi-solid drugs that will occur in vivo conditions to the tissue surface as in vitro conditions. It is thought that with the high adhesiveness value, more drugs will adhere to the tissue surface and will have a longer retention time [
54]. In the results, it is seen that the adhesiveness value of IS-OPT increased with temperature (0.10 ± 0.00, 0.20 ± 0.00, and 1.17 ± 0.46 N.mm for 5, 25, and 35 °C, respectively). This shows that the ocular residence time will be long after the in situ gel is applied.
The last parameter measured in TPA, cohesion, represents the restructuring of the gel after application. Cohesion affects the drug’s performance at the application site, and it is expected that more gel will fully recover structurally after application with the higher cohesion value [
54]. The cohesion value of IS-OPT increased with temperature (0.57 ± 0.12, 0.73 ± 0.04, and 1.10 ± 0.31 for 5, 25, and 35 °C, respectively). The increase in cohesion value with increasing temperature indicates high restructuring of the optimized in situ gel. According to these results, the performance of IS-OPT in the ocular tissue is expected to be good.
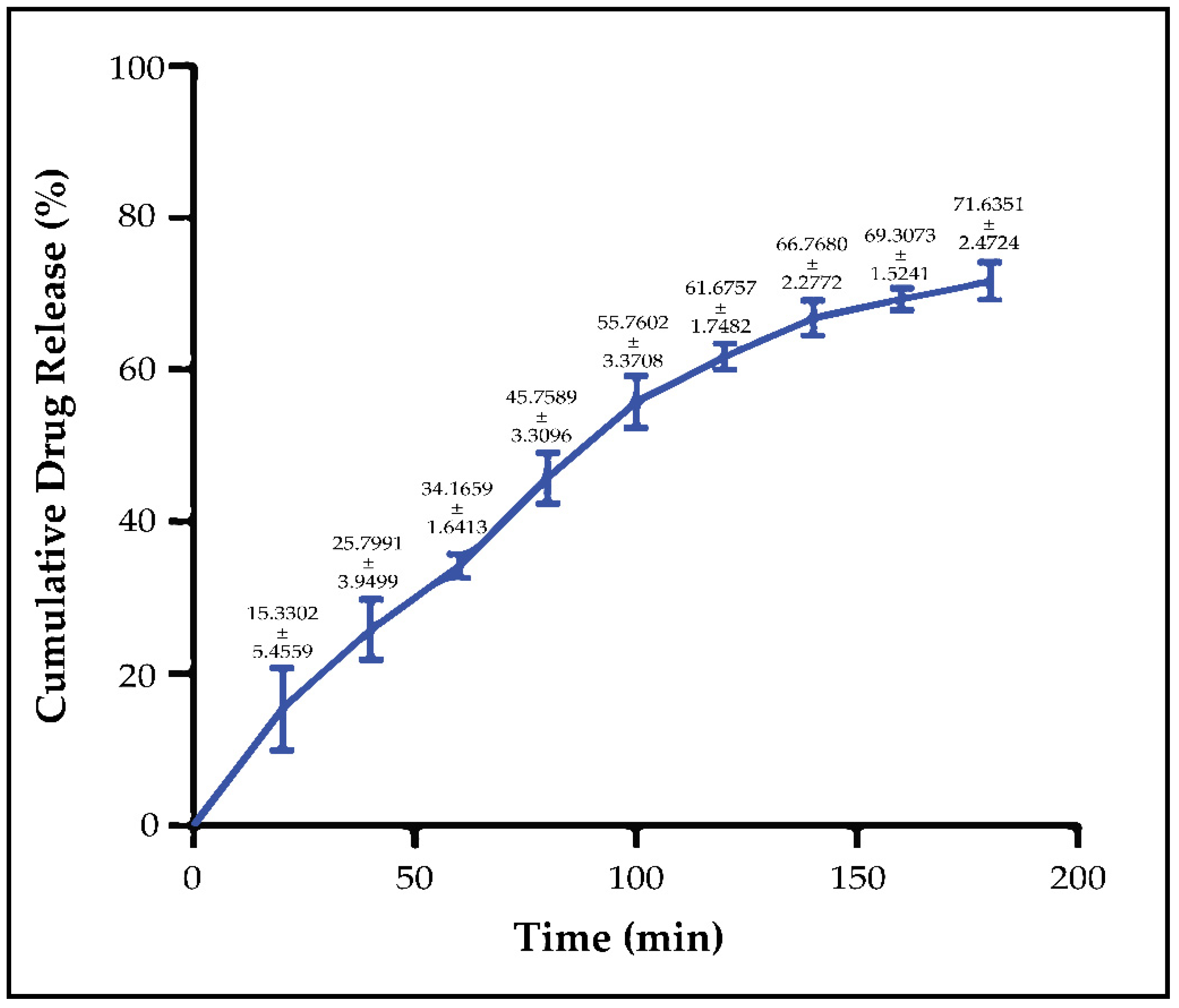
In our previous in vitro release studies, we compared diluted Noxafil
® oral suspension with optimized micellar formulation. In our study with Franz diffusion cells, it was seen that there was a dramatic difference between the release profiles of NM-51 and Noxafil due to increasing the aqueous solubility of PSC via micelles [
15]. It was seen in rheology and texture analyses that IS-OPT had high hardness at physiological temperatures and formed a solid gel structure. In addition, considering the ocular tear turnover rate, performing in vitro drug release studies on Franz diffusion cells would not be a correct approach, and we worked with a membraneless model [
35,
36]. We aimed to mimic tear turnover during the study by completely removing the receptor phase and replacing it with a fresh receptor phase at certain time intervals. It was determined that IS-OPT had a cumulative drug release of 71.6352% at the end of the 3rd hour, and the release was in compliance with zero-order kinetics [
41]. In situ gels are developed to slow the elimination of topically applied drugs and to increase the drug’s contact time with the ocular tissues. Rheology and texture analyses showed that IS-OPT can contact ocular tissues for a long time, as we aimed. According to the release result, the optimized in situ gel will successfully release the PSC in its content during contact with the ocular tissues and reach the therapeutic dose range.
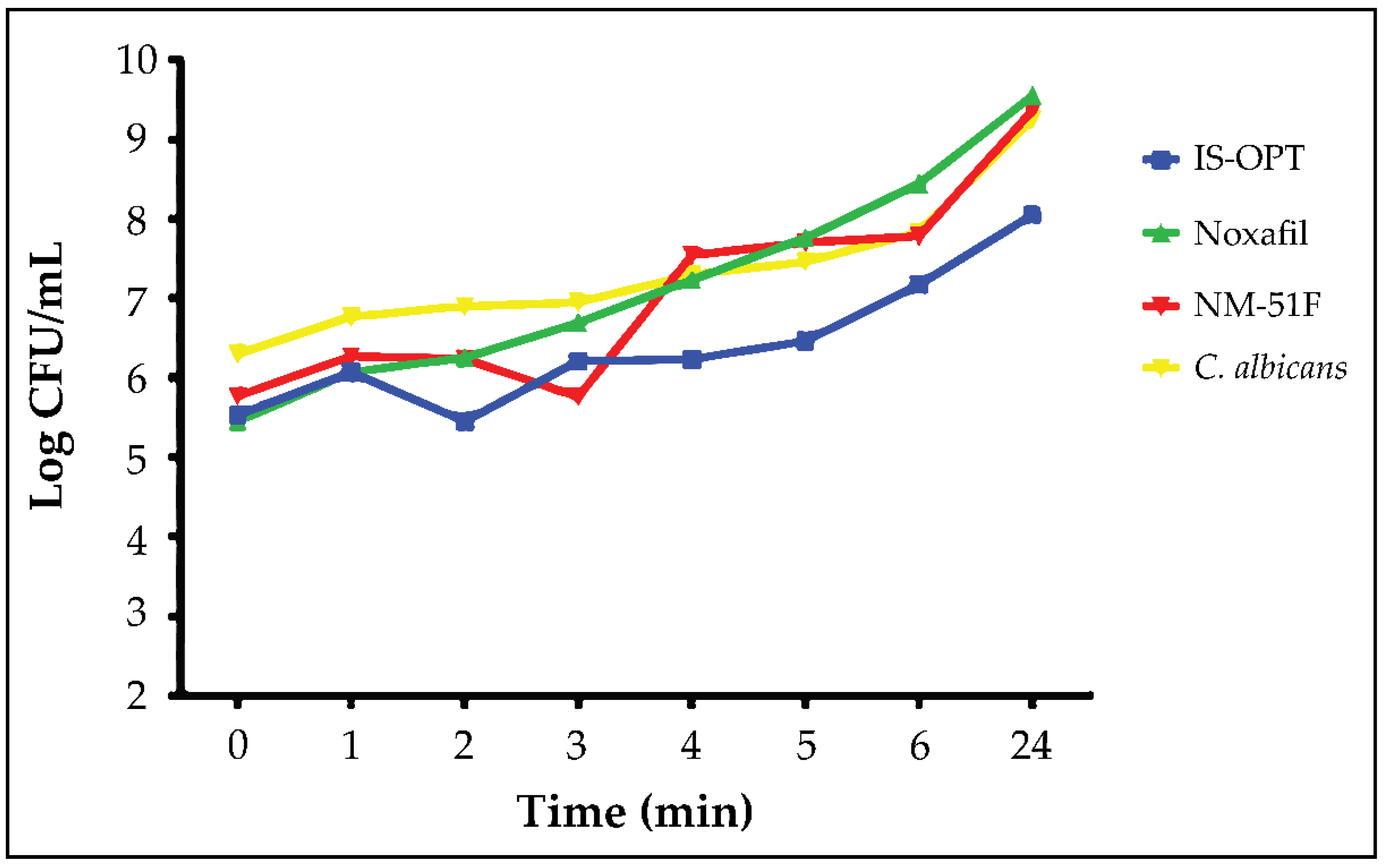
It was determined that all three samples applied in time-kill assay studies showed anti-fungal activity. At the end of the 24th hour, the log of C. albicans surviving in the IS-OPT’s plate was lower than the diluted Noxafil® oral suspension and micelles. When the obtained results were compared with the one-way ANOVA method, it was seen that there was a significant difference between the samples (p = 0.0019).
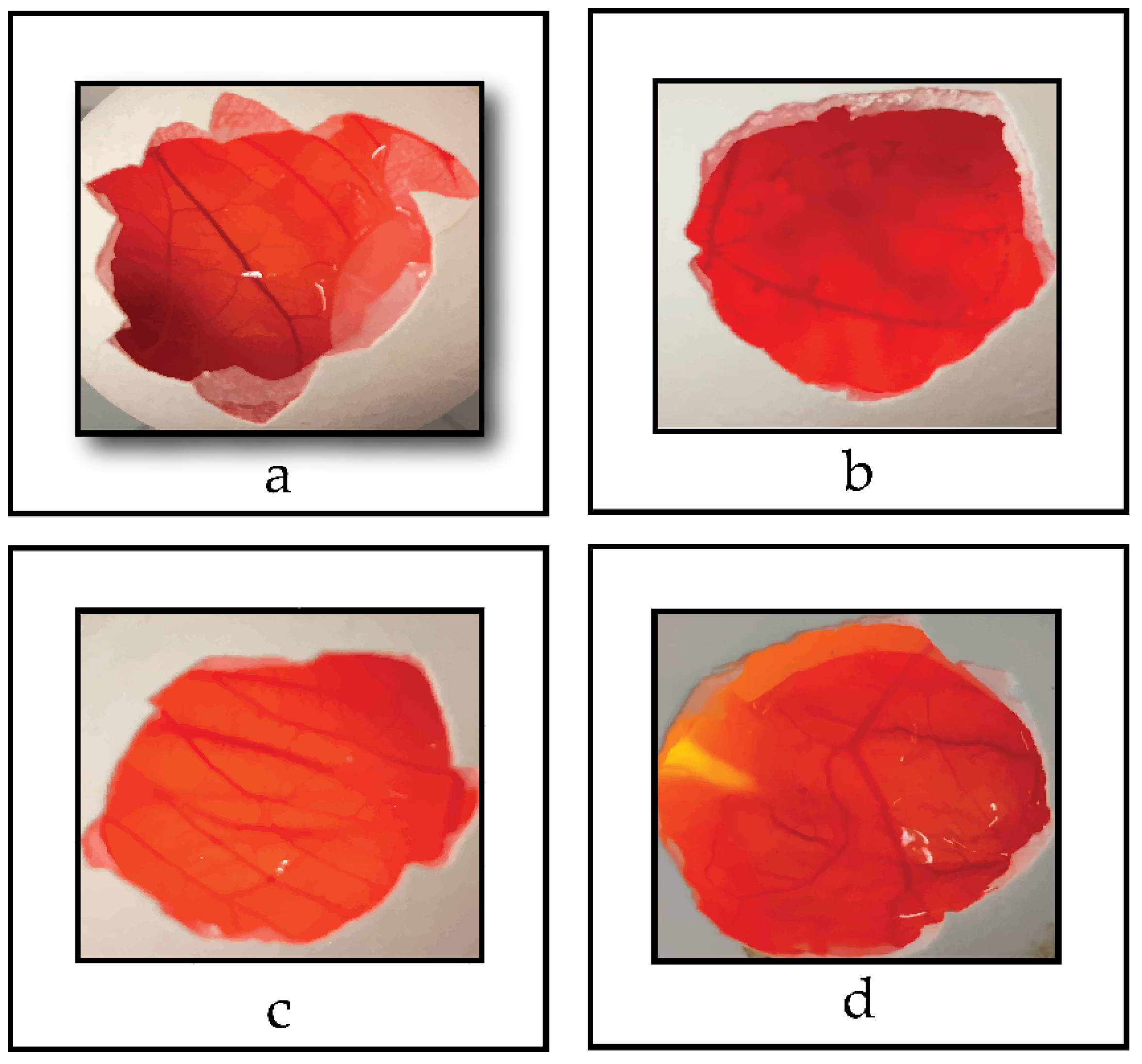
In toxicity studies performed with the HET-CAM method of IS-OPT, no signs of lysis, hemorrhage or coagulation were found in the chorioallantoic membranes at the end of 300 s after applying. This shows us that the ocular application of the optimized in situ gel is safe. In our previous HET-CAM analysis, we compared the micellar formulation and diluted Noxafil
® oral suspension. In studies, Noxafil
® was found to be slightly toxic with a score of 1.5 [
16]. These obtained data question the safety of Noxafil
®, which is used off-label in the treatment of severe ocular fungal infections in the clinic. For this reason, an ocular dosage form containing PSC as an alternative to Noxafil
® is needed in the clinic. Micelles and micellar-based in situ gelling system, which we have optimized in our studies, can be an important alternative.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}