
Novel Treatments for Age-Related Macular Degeneration: A Review of Clinical Advances in Sustained Drug Delivery Systems


 ,
,
Abstract
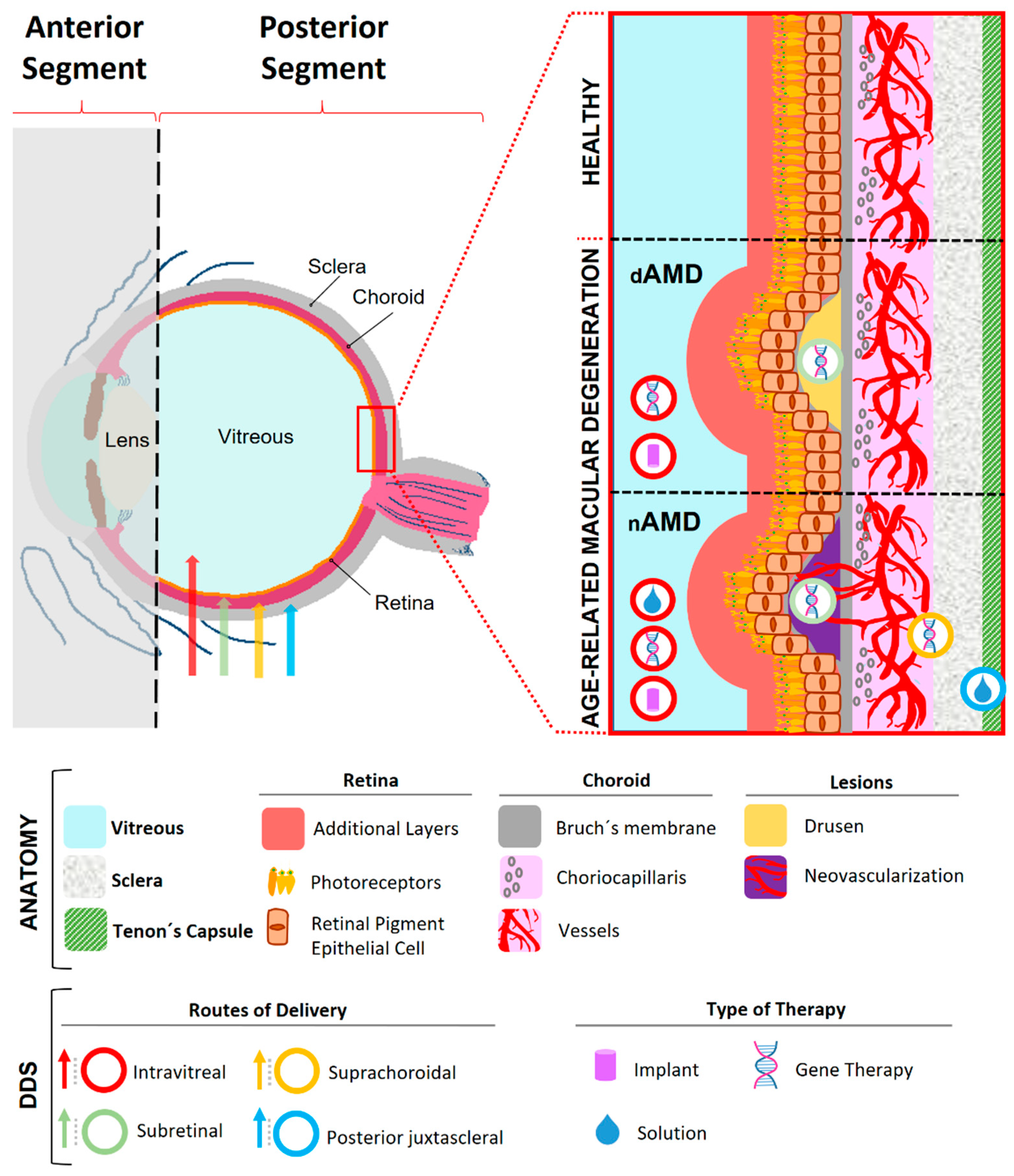
:1. Pathogenesis
2. Routes and Barriers for Drug Delivery in AMD
3. Current Treatment Options in AMD
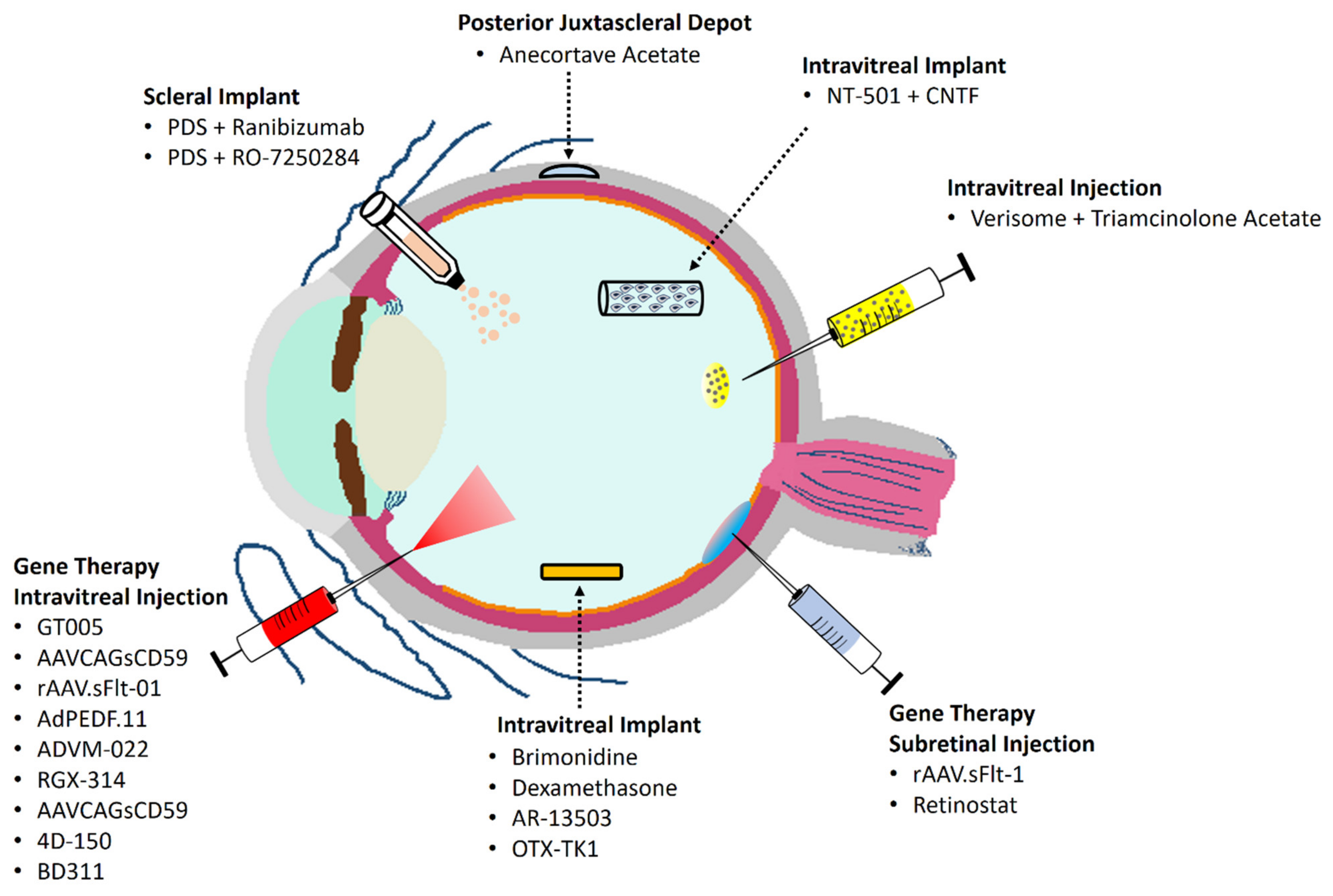
4. Emerging Sustained Drug Delivery Systems in AMD
4.1. Dry Age-Related Macular Disease
4.1.1. Brimonidine Drug Delivery System
4.1.2. NT-501 Implant
4.1.3. Ongoing Clinical Trials
4.2. Neovascular Age-Related Macular Disease
4.2.1. Ranibizumab Port Delivery System
4.2.2. Gene Therapy
4.2.3. Corticosteroid Implants
- A.
- Anecortave acetate
- B.
- Triamcinolone acetate
- C.
- Dexamethasone
4.2.4. Ongoing Clinical Trials
5. Conclusions
6. Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.; Klein, R.; Cheng, C.Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef] [Green Version]
- Pennington, K.L.; DeAngelis, M.M. Epidemiology of age-related macular degeneration (AMD): Associations with cardiovascular disease phenotypes and lipid factors. Eye Vis. 2016, 3, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Word Report on Vision. Available online: https://apps.who.int/iris/rest/bitstreams/1257940/retrieve (accessed on 16 February 2022).
- Hadziahmetovic, M.; Malek, G. Age-Related Macular Degeneration Revisited: From Pathology and Cellular Stress to Potential Therapies. Front. Cell Dev. Biol. 2020, 8, 612812. [Google Scholar] [CrossRef] [PubMed]
- Ferris, F.L., 3rd. Senile macular degeneration: Review of epidemiologic features. Am. J. Epidemiol. 1983, 118, 132–151. [Google Scholar] [CrossRef]
- Ferris, F.L., 3rd; Fine, S.L.; Hyman, L. Age-related macular degeneration and blindness due to neovascular maculopathy. Arch. Ophthalmol. 1984, 102, 1640–1642. [Google Scholar] [CrossRef]
- Holz, F.G.; Strauss, E.C.; Schmitz-Valckenberg, S.; van Lookeren Campagne, M. Geographic atrophy: Clinical features and potential therapeutic approaches. Ophthalmology 2014, 121, 1079–1091. [Google Scholar] [CrossRef]
- Fleckenstein, M.; Mitchell, P.; Freund, K.B.; Sadda, S.; Holz, F.G.; Brittain, C.; Henry, E.C.; Ferrara, D. The Progression of Geographic Atrophy Secondary to Age-Related Macular Degeneration. Ophthalmology 2018, 125, 369–390. [Google Scholar] [CrossRef]
- Gass, J.D.; Agarwal, A.; Lavina, A.M.; Tawansy, K.A. Focal inner retinal hemorrhages in patients with drusen: An early sign of occult choroidal neovascularization and chorioretinal anastomosis. Retina 2003, 23, 741–751. [Google Scholar] [CrossRef]
- Spanish Eyes Epidemiological Study Group. Prevalence of age-related macular degeneration in Spain. Br. J. Ophthalmol. 2011, 95, 931–936. [Google Scholar] [CrossRef]
- Holz, F.G.; Schmitz-Valckenberg, S.; Fleckenstein, M. Recent developments in the treatment of age-related macular degeneration. J. Clin. Investig. 2014, 124, 1430–1438. [Google Scholar] [CrossRef] [Green Version]
- Schmidt-Erfurth, U.; Chong, V.; Loewenstein, A.; Larsen, M.; Souied, E.; Schlingemann, R.; Eldem, B.; Mones, J.; Richard, G.; Bandello, F.; et al. Guidelines for the management of neovascular age-related macular degeneration by the European Society of Retina Specialists (EURETINA). Br. J. Ophthalmol. 2014, 98, 1144–1167. [Google Scholar] [CrossRef]
- Bourla, D.H.; Young, T.A. Age-related macular degeneration: A practical approach to a challenging disease. J. Am. Geriatr. Soc. 2006, 54, 1130–1135. [Google Scholar] [CrossRef]
- Pauleikhoff, D. neovascular age-related macular degeneration: Natural History and Treatment Outcomes. Retina 2005, 25, 1065–1084. [Google Scholar] [CrossRef]
- Damian, J.; Pastor, R.; Armada, F.; Arias, L. Epidemiology of age-related macular degeneration. Situation in Spain. Aten. Primaria 2006, 38, 51–57. [Google Scholar] [CrossRef]
- Holekamp, N.M. Review of neovascular age-related macular degeneration treatment options. Am. J. Manag. Care 2019, 25, S172–S181. [Google Scholar]
- Cholkar, K.; Dasari, R.S.; Pal, D.; Mitra, A.K. Eye: Anatomy, physiology and barriers to drug delivery. Ocul. Transp. Recept. 2013, 1–36. [Google Scholar] [CrossRef]
- Del Amo, E.M.; Rimpela, A.K.; Heikkinen, E.; Kari, O.K.; Ramsay, E.; Lajunen, T.; Schmitt, M.; Pelkonen, L.; Bhattacharya, M.; Richardson, D.; et al. Pharmacokinetic aspects of retinal drug delivery. Prog. Retin. Eye Res. 2017, 57, 134–185. [Google Scholar] [CrossRef]
- Maurice, D.M.; Polgar, J. Diffusion across the sclera. Exp. Eye Res. 1977, 25, 577–582. [Google Scholar] [CrossRef]
- Cheruvu, N.P.; Kompella, U.B. Bovine and porcine transscleral solute transport: Influence of lipophilicity and the Choroid-Bruch’s layer. Investig. Ophthalmol. Vis. Sci. 2006, 47, 4513–4522. [Google Scholar] [CrossRef]
- Pitkanen, L.; Ranta, V.P.; Moilanen, H.; Urtti, A. Permeability of retinal pigment epithelium: Effects of permeant molecular weight and lipophilicity. Investig. Ophthalmol. Vis. Sci. 2005, 46, 641–646. [Google Scholar] [CrossRef] [Green Version]
- Tornquist, P.; Alm, A.; Bill, A. Permeability of ocular vessels and transport across the blood-retinal-barrier. Eye 1990, 4 Pt 2, 303–309. [Google Scholar] [CrossRef]
- Crowell, S.R.; Wang, K.; Famili, A.; Shatz, W.; Loyet, K.M.; Chang, V.; Liu, Y.; Prabhu, S.; Kamath, A.V.; Kelley, R.F. Influence of Charge, Hydrophobicity, and Size on Vitreous Pharmacokinetics of Large Molecules. Transl. Vis. Sci. Technol. 2019, 8, 1. [Google Scholar] [CrossRef] [Green Version]
- Kang-Mieler, J.J.; Osswald, C.R.; Mieler, W.F. Advances in ocular drug delivery: Emphasis on the posterior segment. Expert Opin. Drug. Deliv. 2014, 11, 1647–1660. [Google Scholar] [CrossRef]
- Maloney, M.H.; Payne, S.R.; Herrin, J.; Sangaralingham, L.R.; Shah, N.D.; Barkmeier, A.J. Risk of Systemic Adverse Events after Intravitreal Bevacizumab, Ranibizumab, and Aflibercept in Routine Clinical Practice. Ophthalmology 2021, 128, 417–424. [Google Scholar] [CrossRef]
- Waite, D.; Wang, Y.; Jones, D.; Stitt, A.; Raj Singh, T.R. Posterior drug delivery via periocular route: Challenges and opportunities. Ther. Deliv. 2017, 8, 685–699. [Google Scholar] [CrossRef] [Green Version]
- Ghate, D.; Brooks, W.; McCarey, B.E.; Edelhauser, H.F. Pharmacokinetics of intraocular drug delivery by periocular injections using ocular fluorophotometry. Invest. Ophthalmol. Vis. Sci. 2007, 48, 2230–2237. [Google Scholar] [CrossRef]
- Grassmann, F.; Fleckenstein, M.; Chew, E.Y.; Strunz, T.; Schmitz-Valckenberg, S.; Gobel, A.P.; Klein, M.L.; Ratnapriya, R.; Swaroop, A.; Holz, F.G.; et al. Clinical and genetic factors associated with progression of geographic atrophy lesions in age-related macular degeneration. PLoS ONE 2015, 10, e0126636. [Google Scholar] [CrossRef]
- Holan, V.; Hermankova, B.; Kossl, J. Perspectives of Stem Cell-Based Therapy for Age-Related Retinal Degenerative Diseases. Cell Transpl. 2017, 26, 1538–1541. [Google Scholar] [CrossRef] [Green Version]
- Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch. Ophthalmol. 2001, 119, 1417–1436. [Google Scholar] [CrossRef] [Green Version]
- Agron, E.; Mares, J.; Clemons, T.E.; Swaroop, A.; Chew, E.Y.; Keenan, T.D.L.; AREDS and AREDS2 Research Groups. Dietary Nutrient Intake and Progression to Late Age-Related Macular Degeneration in the Age-Related Eye Disease Studies 1 and 2. Ophthalmology 2021, 128, 425–442. [Google Scholar] [CrossRef]
- Chew, E.Y.; Clemons, T.E.; Agron, E.; Sperduto, R.D.; Sangiovanni, J.P.; Kurinij, N.; Davis, M.D.; Age-Related Eye Disease Study Research, G. Long-term effects of vitamins C and E, beta-carotene, and zinc on age-related macular degeneration: AREDS report no. 35. Ophthalmology 2013, 120, 1604–1611.e1604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omenn, G.S.; Goodman, G.E.; Thornquist, M.D.; Balmes, J.; Cullen, M.R.; Glass, A.; Keogh, J.P.; Meyskens, F.L.; Valanis, B.; Williams, J.H.; et al. Effects of a combination of beta carotene and vitamin A on lung cancer and cardiovascular disease. N. Engl. J. Med. 1996, 334, 1150–1155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Age-Related Eye Disease Study 2 Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: The Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA 2013, 309, 2005–2015. [Google Scholar] [CrossRef] [PubMed]
- Vavvas, D.G.; Small, K.W.; Awh, C.C.; Zanke, B.W.; Tibshirani, R.J.; Kustra, R. CFH and ARMS2 genetic risk determines progression to neovascular age-related macular degeneration after antioxidant and zinc supplementation. Proc. Natl. Acad. Sci. USA 2018, 115, E696–E704. [Google Scholar] [CrossRef] [Green Version]
- Seddon, J.M.; Silver, R.E.; Rosner, B. Response to AREDS supplements according to genetic factors: Survival analysis approach using the eye as the unit of analysis. Br. J. Ophthalmol. 2016, 100, 1731–1737. [Google Scholar] [CrossRef]
- Rauch, R.; Weingessel, B.; Maca, S.M.; Vecsei-Marlovits, P.V. Time to first treatment: The significance of early treatment of exudative age-related macular degeneration. Retina 2012, 32, 1260–1264. [Google Scholar] [CrossRef]
- Lim, J.H.; Wickremasinghe, S.S.; Xie, J.; Chauhan, D.S.; Baird, P.N.; Robman, L.D.; Hageman, G.; Guymer, R.H. Delay to treatment and visual outcomes in patients treated with anti-vascular endothelial growth factor for age-related macular degeneration. Am. J. Ophthalmol. 2012, 153, 678–686.e2. [Google Scholar] [CrossRef] [Green Version]
- Arias, L.; Armada, F.; Donate, J.; Garcia-Arumi, J.; Giralt, J.; Pazos, B.; Pinero, A.; Martinez, F.; Mondejar, J.J.; Ortega, I.; et al. Delay in treating age-related macular degeneration in Spain is associated with progressive vision loss. Eye 2009, 23, 326–333. [Google Scholar] [CrossRef]
- Tuuminen, R.; Uusitalo-Jarvinen, H.; Aaltonen, V.; Hautala, N.; Kaipiainen, S.; Laitamaki, N.; Ollila, M.; Rantanen, J.; Valimaki, S.; Sipila, R.; et al. The Finnish national guideline for diagnosis, treatment and follow-up of patients with wet age-related macular degeneration. Acta Ophthalmol. 2017, 95, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Bakri, S.J.; Thorne, J.E.; Ho, A.C.; Ehlers, J.P.; Schoenberger, S.D.; Yeh, S.; Kim, S.J. Safety and Efficacy of Anti-Vascular Endothelial Growth Factor Therapies for Neovascular Age-Related Macular Degeneration: A Report by the American Academy of Ophthalmology. Ophthalmology 2019, 126, 55–63. [Google Scholar] [CrossRef] [Green Version]
- Peden, M.C.; Suner, I.J.; Hammer, M.E.; Grizzard, W.S. Long-term outcomes in eyes receiving fixed-interval dosing of anti-vascular endothelial growth factor agents for wet age-related macular degeneration. Ophthalmology 2015, 122, 803–808. [Google Scholar] [CrossRef]
- Kuppermann, B.D.; Patel, S.S.; Boyer, D.S.; Augustin, A.J.; Freeman, W.R.; Kerr, K.J.; Guo, Q.; Schneider, S.; Lopez, F.J. Phase 2 Study of the Safety and Efficacy of Brimonidine Drug Delivery System (Brimo Dds) Generation 1 in Patients with Geographic Atrophy Secondary to Age-Related Macular Degeneration. Retina 2021, 41, 144–155. [Google Scholar] [CrossRef]
- Clinical Trial. A Safety and Efficacy Study of Brimonidine Intravitreal Implant in Geographic Atrophy Secondary to Age-related Macular Degeneration (BEACON), Identifier NCT02087085. Available online: https://clinicaltrials.gov/ct2/show/NCT02087085 (accessed on 8 March 2022).
- LaVail, M.M.; Yasumura, D.; Matthes, M.T.; Lau-Villacorta, C.; Unoki, K.; Sung, C.H.; Steinberg, R.H. Protection of mouse photoreceptors by survival factors in retinal degenerations. Investig. Ophthalmol. Vis. Sci. 1998, 39, 592–602. [Google Scholar]
- Cayouette, M.; Gravel, C. Adenovirus-mediated gene transfer of ciliary neurotrophic factor can prevent photoreceptor degeneration in the retinal degeneration (rd) mouse. Hum. Gene Ther. 1997, 8, 423–430. [Google Scholar] [CrossRef]
- LaVail, M.M.; Unoki, K.; Yasumura, D.; Matthes, M.T.; Yancopoulos, G.D.; Steinberg, R.H. Multiple growth factors, cytokines, and neurotrophins rescue photoreceptors from the damaging effects of constant light. Proc. Natl. Acad. Sci. USA 1992, 89, 11249–11253. [Google Scholar] [CrossRef] [Green Version]
- Stahl, N.; Yancopoulos, G.D. The tripartite CNTF receptor complex: Activation and signaling involves components shared with other cytokines. J. Neurobiol. 1994, 25, 1454–1466. [Google Scholar] [CrossRef]
- Tao, W. Application of encapsulated cell technology for retinal degenerative diseases. Expert Opin. Biol. Ther. 2006, 6, 717–726. [Google Scholar] [CrossRef]
- Zhang, K.; Hopkins, J.J.; Heier, J.S.; Birch, D.G.; Halperin, L.S.; Albini, T.A.; Brown, D.M.; Jaffe, G.J.; Tao, W.; Williams, G.A. Ciliary neurotrophic factor delivered by encapsulated cell intraocular implants for treatment of geographic atrophy in age-related macular degeneration. Proc. Natl. Acad. Sci. USA 2011, 108, 6241–6245. [Google Scholar] [CrossRef] [Green Version]
- Kauper, K.; McGovern, C.; Sherman, S.; Heatherton, P.; Rapoza, R.; Stabila, P.; Dean, B.; Lee, A.; Borges, S.; Bouchard, B.; et al. Two-year intraocular delivery of ciliary neurotrophic factor by encapsulated cell technology implants in patients with chronic retinal degenerative diseases. Investig. Ophthalmol. Vis. Sci. 2012, 53, 7484–7491. [Google Scholar] [CrossRef]
- Clinical Trial. FocuS: First in Human Study to Evaluate the Safety and Efficacy of GT005 Administered in Subjects with Dry AMD, Identifier: NCT03846193. Available online: https://clinicaltrials.gov/ct2/show/NCT03846193 (accessed on 22 March 2022).
- Clinical Trial. Treatment of Advanced Dry Age Related Macular Degeneration with AAVCAGsCD59, Identifier: NCT03144999. Available online: https://clinicaltrials.gov/ct2/show/NCT03144999. (accessed on 22 March 2022).
- Campochiaro, P.A.; Marcus, D.M.; Awh, C.C.; Regillo, C.; Adamis, A.P.; Bantseev, V.; Chiang, Y.; Ehrlich, J.S.; Erickson, S.; Hanley, W.D.; et al. The Port Delivery System with Ranibizumab for Neovascular Age-Related Macular Degeneration: Results from the Randomized Phase 2 Ladder Clinical Trial. Ophthalmology 2019, 126, 1141–1154. [Google Scholar] [CrossRef] [Green Version]
- Rubio, R.G. Long-acting anti-VEGF delivery. Retina Today 2014, 78–80. [Google Scholar]
- Khanani, A.M.; Callanan, D.; Dreyer, R.; Chen, S.; Howard, J.G.; Hopkins, J.J.; Lin, C.Y.; Lorenz-Candlin, M.; Makadia, S.; Patel, S.; et al. End-of-Study Results for the Ladder Phase 2 Trial of the Port Delivery System with Ranibizumab for Neovascular Age-Related Macular Degeneration. Ophthalmol. Retina 2021, 5, 775–787. [Google Scholar] [CrossRef]
- Holekamp, N.M.; Campochiaro, P.A.; Chang, M.A.; Miller, D.; Pieramici, D.; Adamis, A.P.; Brittain, C.; Evans, E.; Kaufman, D.; Maass, K.F.; et al. Archway Randomized Phase 3 Trial of the Port Delivery System with Ranibizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology 2022, 129, 295–307. [Google Scholar] [CrossRef]
- Clinical Trial. Extension Study for the Port Delivery System with Ranibizumab (Portal), Identifier NCT03683251. Available online: https://clinicaltrials.gov/ct2/show/NCT03683251 (accessed on 8 March 2022).
- Clinical Trial. A Study of the Efficacy, Safety, and Pharmacokinetics of A 36-Week Refill Regimen for the Port Delivery System with Ranibizumab in Patients with Neovascular Age-Related Macular Degeneration (Velodrome), Identifier NCT04657289. Available online: https://clinicaltrials.gov/ct2/show/NCT04657289 (accessed on 8 March 2022).
- Clinical Trial. A Study Of The Effectiveness And Safety Of A 36-Week Refill Regimen For The Port Delivery System with Ranibizumab Vs Aflibercept Treat & Extend In Subjects with Neovascular Age-Related Macular Degeneration (Diagrid). Identifier NCT05126966. Available online: https://www.clinicaltrials.gov/ct2/show/NCT05126966 (accessed on 8 March 2022).
- Clinical Trial. A Study Of The Response to Treatment After Transition to The Port Delivery System with Ranibizumab [Susvimo (Ranibizumab Injection)] In Patients with Neovascular Age-Related Macular Degeneration Previously Treated with Intravitreal Agents Other Than Ranibizumab (Belvedere). Identifier NTC04853251. Available online: https://clinicaltrials.gov/ct2/show/NCT04853251 (accessed on 8 March 2022).
- Clinical Trial. Study of RO7250284 in Participants with Neovascular Age-Related Macular Degeneration, Identifier NCT04567303. Available online: https://clinicaltrials.gov/ct2/show/NCT04567303 (accessed on 8 March 2022).
- Rakoczy, E.P.; Lai, C.M.; Magno, A.L.; Wikstrom, M.E.; French, M.A.; Pierce, C.M.; Schwartz, S.D.; Blumenkranz, M.S.; Chalberg, T.W.; Degli-Esposti, M.A.; et al. Gene therapy with recombinant adeno-associated vectors for neovascular age-related macular degeneration: 1 year follow-up of a phase 1 randomised clinical trial. Lancet 2015, 386, 2395–2403. [Google Scholar] [CrossRef] [Green Version]
- Constable, I.J.; Pierce, C.M.; Lai, C.M.; Magno, A.L.; Degli-Esposti, M.A.; French, M.A.; McAllister, I.L.; Butler, S.; Barone, S.B.; Schwartz, S.D.; et al. Phase 2a Randomized Clinical Trial: Safety and Post Hoc Analysis of Subretinal rAAV.sFLT-1 for Wet Age-related Macular Degeneration. eBioMedicine 2016, 14, 168–175. [Google Scholar] [CrossRef] [Green Version]
- Constable, I.J.; Blumenkranz, M.S.; Schwartz, S.D.; Barone, S.; Lai, C.M.; Rakoczy, E.P. Gene Therapy for Age-Related Macular Degeneration. Asia-Pac. J. Ophthalmol. 2016, 5, 300–303. [Google Scholar] [CrossRef]
- Constable, I.J.; Lai, C.M.; Magno, A.L.; French, M.A.; Barone, S.B.; Schwartz, S.D.; Blumenkranz, M.S.; Degli-Esposti, M.A.; Rakoczy, E.P. Gene Therapy in Neovascular Age-related Macular Degeneration: Three-Year Follow-up of a Phase 1 Randomized Dose Escalation Trial. Am. J. Ophthalmol. 2017, 177, 150–158. [Google Scholar] [CrossRef]
- Rakoczy, E.P.; Magno, A.L.; Lai, C.M.; Pierce, C.M.; Degli-Esposti, M.A.; Blumenkranz, M.S.; Constable, I.J. Three-Year Follow-Up of Phase 1 and 2a rAAV.sFLT-1 Subretinal Gene Therapy Trials for Exudative Age-Related Macular Degeneration. Am. J. Ophthalmol. 2019, 204, 113–123. [Google Scholar] [CrossRef]
- Heier, J.S.; Kherani, S.; Desai, S.; Dugel, P.; Kaushal, S.; Cheng, S.H.; Delacono, C.; Purvis, A.; Richards, S.; Le-Halpere, A.; et al. Intravitreous injection of AAV2-sFLT01 in patients with advanced neovascular age-related macular degeneration: A phase 1, open-label trial. Lancet 2017, 390, 50–61. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Lauer, A.K.; Sohn, E.H.; Mir, T.A.; Naylor, S.; Anderton, M.C.; Kelleher, M.; Harrop, R.; Ellis, S.; Mitrophanous, K.A. Lentiviral Vector Gene Transfer of Endostatin/Angiostatin for Macular Degeneration (GEM) Study. Hum. Gene Ther. 2017, 28, 99–111. [Google Scholar] [CrossRef]
- Clinical Trial. A Follow-up Study to Evaluate the Safety of RetinoStat® in Patients with Age-Related Macular Degeneration, Identifier: NCT01678872. Available online: https://clinicaltrials.gov/ct2/show/NCT01678872 (accessed on 22 March 2022).
- Campochiaro, P.A.; Nguyen, Q.D.; Shah, S.M.; Klein, M.L.; Holz, E.; Frank, R.N.; Saperstein, D.A.; Gupta, A.; Stout, J.T.; Macko, J.; et al. Adenoviral vector-delivered pigment epithelium-derived factor for neovascular age-related macular degeneration: Results of a phase I clinical trial. Hum. Gene Ther. 2006, 17, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.F. AL-3789: A novel ophthalmic angiostatic steroid. Expert Opin. Investig. Drugs 1997, 6, 1867–1877. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, D.J.; Goldberg, M.F.; Hudson, H.; Jerdan, J.A.; Krueger, S.; Luna, S.; Robertson, S.M.; Russell, S.; Singerman, L.; Slakter, J.S.; et al. Anecortave acetate as monotherapy for the treatment of subfoveal lesions in patients with exudative age-related macular degeneration (AMD): Interim (month 6) analysis of clinical safety and efficacy. Retina 2003, 23, 14–23. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, D.J.; Goldberg, M.F.; Hudson, H.; Jerdan, J.A.; Krueger, D.S.; Luna, S.P.; Robertson, S.M.; Russell, S.; Singerman, L.; Slakter, J.S.; et al. Anecortave acetate as monotherapy for treatment of subfoveal neovascularization in age-related macular degeneration: Twelve-month clinical outcomes. Ophthalmology 2003, 110, 2372–2383; discuss in 2384–2385. [Google Scholar] [CrossRef]
- Schmidt-Erfurth, U.; Michels, S.; Michels, R.; Aue, A. Anecortave acetate for the treatment of subfoveal choroidal neovascularization secondary to age-related macular degeneration. Eur. J. Ophthalmol. 2005, 15, 482–485. [Google Scholar] [CrossRef]
- Augustin, A.J.; D’Amico, D.J.; Mieler, W.F.; Schneebaum, C.; Beasley, C. Safety of posterior juxtascleral depot administration of the angiostatic cortisene anecortave acetate for treatment of subfoveal choroidal neovascularization in patients with age-related macular degeneration. Graefes Arch. Clin. Exp. Ophthalmol. 2005, 243, 9–12. [Google Scholar] [CrossRef]
- Slakter, J.S.; Bochow, T.W.; D’Amico, D.J.; Marks, B.; Jerdan, J.; Sullivan, E.K.; Robertson, S.M.; Slakter, J.S.; Sullins, G.; Zilliox, P.; et al. Anecortave acetate (15 milligrams) versus photodynamic therapy for treatment of subfoveal neovascularization in age-related macular degeneration. Ophthalmology 2006, 113, 3–13. [Google Scholar] [CrossRef]
- Lim, J.I.; Niec, M.; Wong, V. One year results of a phase 1 study of the safety and tolerability of combination therapy using sustained release intravitreal triamcinolone acetonide and ranibizumab for subfoveal neovascular AMD. Br. J. Ophthalmol. 2015, 99, 618–623. [Google Scholar] [CrossRef] [Green Version]
- Kuppermann, B.D.; Goldstein, M.; Maturi, R.K.; Pollack, A.; Singer, M.; Tufail, A.; Weinberger, D.; Li, X.Y.; Liu, C.C.; Lou, J.; et al. Dexamethasone Intravitreal Implant as Adjunctive Therapy to Ranibizumab in Neovascular Age-Related Macular Degeneration: A Multicenter Randomized Controlled Trial. Ophthalmologica 2015, 234, 40–54. [Google Scholar] [CrossRef] [Green Version]
- Rezar-Dreindl, S.; Eibenberger, K.; Buehl, W.; Georgopoulos, M.; Weigert, G.; Krall, C.; Dunavoelgyi, R.; Schmidt-Erfurth, U.; Sacu, S. Role of Additional Dexamethasone for the Management of Persistent or Recurrent Neovascular Age-Related Macular Degeneration under Ranibizumab Treatment. Retina 2017, 37, 962–970. [Google Scholar] [CrossRef]
- Rezar-Dreindl, S.; Sacu, S.; Eibenberger, K.; Pollreisz, A.; Buhl, W.; Georgopoulos, M.; Krall, C.; Weigert, G.; Schmidt-Erfurth, U. The Intraocular Cytokine Profile and Therapeutic Response in Persistent Neovascular Age-Related Macular Degeneration. Investig. Ophthalmol. Vis. Sci. 2016, 57, 4144–4150. [Google Scholar] [CrossRef] [Green Version]
- Chaudhary, V.; Barbosa, J.; Lam, W.C.; Mak, M.; Mavrikakis, E.; Mohaghegh, P.S. Ozurdex in age-related macular degeneration as adjunct to ranibizumab (The OARA Study). Can. J. Ophthalmol. 2016, 51, 302–305. [Google Scholar] [CrossRef]
- Clinical Trial. A Study Assessing AR-13503 Implant in Subjects with nAMD or DME. Identifier: NCT03835884. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03835884 (accessed on 8 April 2022).
- Clinical Trial. Study Evaluating the Treatment of OTX-TKI for Subjects with Neovascular Age-related Macular Degeneration. Identifier: NTC04989699. Available online: https://clinicaltrials.gov/ct2/show/NCT04989699 (accessed on 8 April 2022).



{kind=link}
{kind=link}
| Name | Synthesized Products | Vector | Phase | Route of Delivery | Sponsor | Trial Registration Number |
|---|---|---|---|---|---|---|
| ADVM-22 | Aflibercept | AAV.7m8 | I | Intravitreal | Adverum Biotechnologies, Inc. (Redwood City, CA, USA). | NCT03748784 |
| Extension | Intravitreal | Adverum Biotechnologies, Inc. | NCT04645212 | |||
| RGX-314 | Anti-VEGF Fab | AAV8 | I/IIa | Subretinal | Regenxbio Inc. (Rockville, MD, USA). | NCT03066258 |
| II | Subretinal | Regenxbio Inc. | NCT04832724 | |||
| IIb/III | Subretinal | Regenxbio Inc. | NCT04704921 | |||
| Extension | Subretinal | Regenxbio Inc. | NCT03999801 | |||
| II | Suprachoroidal | Regenxbio Inc. | NCT04514653 | |||
| Extension | Suprachoroidal | Regenxbio Inc. | NCT05210803 | |||
| AAVCAGsCD59 | CD59s | AAV2 | I | Intravitreal | Janseen Research & Development, LLC (Raritan, NJ, USA) | NCT03585556 |
| 4D-150 | VEGF-C miRNA + aflibercept | AAV | I/II | Intravitreal | 4D Molecular Therapeutics (Emeryville, CA, USA) | NCT05197270 |
| BD311 | Anti-VEGF-A | IDL | I | Suprachoroidal | Shanghai BDgene Co., Ltd. (Shangai, China). | NCT05099094 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez-Gómez, Y.; Alba-Molina, D.; Blanco-Blanco, M.; Pérez-Fajardo, L.; Reyes-Ortega, F.; Ortega-Llamas, L.; Villalba-González, M.; Fernández-Choquet de Isla, I.; Pugliese, F.; Stoikow, I.; et al. Novel Treatments for Age-Related Macular Degeneration: A Review of Clinical Advances in Sustained Drug Delivery Systems. Pharmaceutics 2022, 14, 1473. https://doi.org/10.3390/pharmaceutics14071473
Jiménez-Gómez Y, Alba-Molina D, Blanco-Blanco M, Pérez-Fajardo L, Reyes-Ortega F, Ortega-Llamas L, Villalba-González M, Fernández-Choquet de Isla I, Pugliese F, Stoikow I, et al. Novel Treatments for Age-Related Macular Degeneration: A Review of Clinical Advances in Sustained Drug Delivery Systems. Pharmaceutics. 2022; 14(7):1473. https://doi.org/10.3390/pharmaceutics14071473
Chicago/Turabian StyleJiménez-Gómez, Yolanda, David Alba-Molina, Mario Blanco-Blanco, Lorena Pérez-Fajardo, Felisa Reyes-Ortega, Laura Ortega-Llamas, Marta Villalba-González, Ignacio Fernández-Choquet de Isla, Francisco Pugliese, Indira Stoikow, and et al. 2022. "Novel Treatments for Age-Related Macular Degeneration: A Review of Clinical Advances in Sustained Drug Delivery Systems" Pharmaceutics 14, no. 7: 1473. https://doi.org/10.3390/pharmaceutics14071473
APA StyleJiménez-Gómez, Y., Alba-Molina, D., Blanco-Blanco, M., Pérez-Fajardo, L., Reyes-Ortega, F., Ortega-Llamas, L., Villalba-González, M., Fernández-Choquet de Isla, I., Pugliese, F., Stoikow, I., & González-Andrades, M. (2022). Novel Treatments for Age-Related Macular Degeneration: A Review of Clinical Advances in Sustained Drug Delivery Systems. Pharmaceutics, 14(7), 1473. https://doi.org/10.3390/pharmaceutics14071473