
Nanomedicines for Overcoming Cancer Drug Resistance




Abstract
:1. Introduction
2. Nanomedicines against Drug Resistance in Chemotherapy
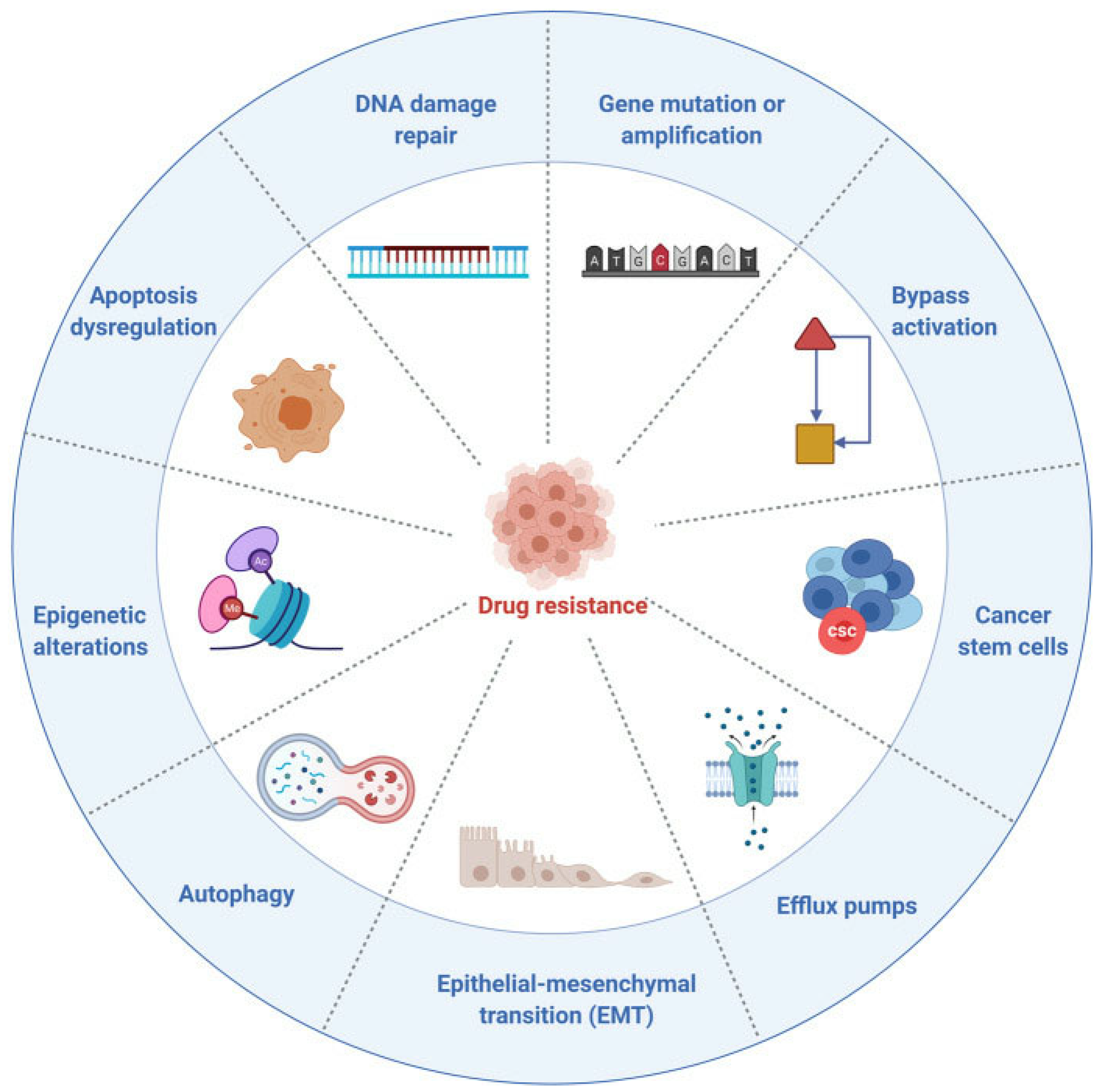
2.1. Mechanisms in Drug Resistance of Chemotherapy
2.2. Nanomedicines to Overcome Chemotherapy Resistance

3. Nanomedicines against Drug Resistance in Targeted Therapy
3.1. Mechanisms in Drug Resistance of Targeted Therapy
3.2. Nanomedicines to Overcome Targeted Therapy Resistance
4. Nanomedicines against Drug Resistance in Immunotherapy
4.1. Mechanisms in Drug Resistance of Immunotherapy
4.2. Nanomedicines to Overcome Immunotherapy Resistance
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Wu, Q.; Yang, Z.; Nie, Y.; Shi, Y.; Fan, D. Multi-drug resistance in cancer chemotherapeutics: Mechanisms and lab approaches. Cancer Lett. 2014, 347, 159–166. [Google Scholar] [CrossRef]
- Cohen, P.; Cross, D.; Jänne, P.A. Kinase drug discovery 20 years after imatinib: Progress and future directions. Nat. Rev. Drug Discov. 2021, 20, 551–569. [Google Scholar] [CrossRef] [PubMed]
- Bashash, D.; Zandi, Z.; Kashani, B.; Pourbagheri-Sigaroodi, A.; Salari, S.; Ghaffari, S.H. Resistance to immunotherapy in human malignancies: Mechanisms, research progresses, challenges, and opportunities. J. Cell. Physiol. 2022, 237, 346–372. [Google Scholar] [CrossRef] [PubMed]
- Gottesman, M.M. Mechanisms of cancer drug resistance. Annu. Rev. Med. 2002, 53, 615–627. [Google Scholar] [CrossRef] [Green Version]
- Asić, K. Dominant mechanisms of primary resistance differ from dominant mechanisms of secondary resistance to targeted therapies. Crit. Rev. Oncol. Hematol. 2016, 97, 178–196. [Google Scholar] [CrossRef]
- Wang, W.; Sun, Y.; Liu, X.; Kumar, S.K.; Jin, F.; Dai, Y. Dual-targeted therapy circumvents non-genetic drug resistance to targeted therapy. Front. Oncol. 2022, 12, 859455. [Google Scholar] [CrossRef] [PubMed]
- Pluchino, K.M.; Hall, M.D.; Goldsborough, A.S.; Callaghan, R.; Gottesman, M.M. Collateral sensitivity as a strategy against cancer multidrug resistance. Drug Resist. Updat. 2012, 15, 98–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikolaou, M.; Pavlopoulou, A.; Georgakilas, A.G.; Kyrodimos, E. The challenge of drug resistance in cancer treatment: A current overview. Clin Exp Metastasis 2018, 35, 309–318. [Google Scholar] [CrossRef]
- Nussinov, R.; Tsai, C.J.; Jang, H. Anticancer drug resistance: An update and perspective. Drug Resist. Updat. 2021, 59, 100796. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Wu, Z.X.; Assaraf, Y.G.; Chen, Z.S.; Wang, L. Overcoming anti-cancer drug resistance via restoration of tumor suppressor gene function. Drug Resist. Updat. 2021, 57, 100770. [Google Scholar] [CrossRef]
- Dallavalle, S.; Dobričić, V.; Lazzarato, L.; Gazzano, E.; Machuqueiro, M.; Pajeva, I.; Tsakovska, I.; Zidar, N.; Fruttero, R. Improvement of conventional anti-cancer drugs as new tools against multidrug resistant tumors. Drug Resist. Updat. 2020, 50, 100682. [Google Scholar] [CrossRef] [PubMed]
- Ravindran Menon, D.; Hammerlindl, H.; Torrano, J.; Schaider, H.; Fujita, M. Epigenetics and metabolism at the crossroads of stress-induced plasticity, stemness and therapeutic resistance in cancer. Theranostics 2020, 10, 6261–6277. [Google Scholar] [CrossRef] [PubMed]
- Barrueto, L.; Caminero, F.; Cash, L.; Makris, C.; Lamichhane, P.; Deshmukh, R.R. Resistance to checkpoint inhibition in cancer immunotherapy. Transl. Oncol. 2020, 13, 100738. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.W.; Barbie, D.A.; Flaherty, K.T. Mechanisms of resistance to immune checkpoint inhibitors. Br. J. Cancer 2018, 118, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Khalaf, K.; Hana, D.; Chou, J.T.; Singh, C.; Mackiewicz, A.; Kaczmarek, M. Aspects of the tumor microenvironment involved in immune resistance and drug resistance. Front. Immunol. 2021, 12, 656364. [Google Scholar] [CrossRef] [PubMed]
- Erin, N.; Grahovac, J.; Brozovic, A.; Efferth, T. Tumor microenvironment and epithelial mesenchymal transition as targets to overcome tumor multidrug resistance. Drug Resist. Updat. 2020, 53, 100715. [Google Scholar] [CrossRef] [PubMed]
- Elgendy, S.M.; Alyammahi, S.K.; Alhamad, D.W.; Abdin, S.M.; Omar, H.A. Ferroptosis: An emerging approach for targeting cancer stem cells and drug resistance. Crit. Rev. Oncol. Hematol. 2020, 155, 103095. [Google Scholar] [CrossRef]
- Li, Y.; Wang, Z.; Ajani, J.A.; Song, S. Drug resistance and cancer stem cells. Cell Commun. Signal. 2021, 19, 19. [Google Scholar] [CrossRef]
- Su, Z.; Dong, S.; Zhao, S.C.; Liu, K.; Tan, Y.; Jiang, X.; Assaraf, Y.G.; Qin, B.; Chen, Z.S.; Zou, C. Novel nanomedicines to overcome cancer multidrug resistance. Drug Resist. Updat. 2021, 58, 100777. [Google Scholar] [CrossRef]
- Martin, J.D.; Cabral, H.; Stylianopoulos, T.; Jain, R.K. Improving cancer immunotherapy using nanomedicines: Progress, opportunities and challenges. Nat. Rev. Clin. Oncol. 2020, 17, 251–266. [Google Scholar] [CrossRef]
- Sharma, M.; Bakshi, A.K.; Mittapelly, N.; Gautam, S.; Marwaha, D.; Rai, N.; Singh, N.; Tiwari, P.; Agarwal, N.; Kumar, A. Recent updates on innovative approaches to overcome drug resistance for better outcomes in cancer. J. Control. Release 2022, 346, 43–70. [Google Scholar] [CrossRef] [PubMed]
- Sanaei, M.J.; Pourbagheri-Sigaroodi, A.; Kaveh, V.; Sheikholeslami, S.A.; Salari, S.; Bashash, D. The application of nano-medicine to overcome the challenges related to immune checkpoint blockades in cancer immunotherapy: Recent advances and opportunities. Crit. Rev. Oncol. Hematol. 2021, 157, 103160. [Google Scholar] [CrossRef]
- Wei, G.; Wang, Y.; Yang, G.; Wang, Y.; Ju, R. Recent progress in nanomedicine for enhanced cancer chemotherapy. Theranostics 2021, 11, 6370–6392. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Zhu, Y.; Wang, W.; Wang, G.; Zhang, S.; Cheng, H. Emerging nano-based strategies against drug resistance in tumor chemotherapy. Front. Bioeng. Biotechnol. 2021, 9, 798882. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Khan, A.R.; Yang, X.; Dong, B.; Ji, J.; Zhai, G. The reversal of chemotherapy-induced multidrug resistance by nanomedicine for cancer therapy. J. Control. Release 2021, 335, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Hong, W.; Ren, W.; Xu, T.; Qian, Z.; He, Z. Recent progress in targeted delivery vectors based on biomimetic nanoparticles. Signal Transduct. Target. Ther. 2021, 6, 225. [Google Scholar] [CrossRef]
- Liu, J.; Song, L.; Liu, S.; Zhao, S.; Jiang, Q.; Ding, B. A tailored DNA nanoplatform for synergistic RNAi-/chemotherapy of multidrug-resistant Tumors. Angew. Chem. Int. Ed. 2018, 57, 15486–15490. [Google Scholar] [CrossRef]
- Yi, S.; Liao, R.; Zhao, W.; Huang, Y.; He, Y. Multifunctional co-transport carriers based on cyclodextrin assembly for cancer synergistic therapy. Theranostics 2022, 12, 2560–2579. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Wang, M.; Wang, H.; Zhou, J.; Chen, J. Multifunctional human serum albumin fusion protein as a docetaxel nanocarrier for chemo-photothermal synergetic therapy of ovarian cancer. ACS Appl. Mater. Interfaces 2022, 14, 19907–19917. [Google Scholar] [CrossRef]
- Li, Z.; Chen, Y.; Yang, Y.; Yu, Y.; Zhang, Y.; Zhu, D.; Yu, X.; Ouyang, X.; Xie, Z.; Zhao, Y.; et al. Recent Advances in nanomaterials-based chemo-photothermal combination therapy for improving cancer treatment. Front. Bioeng. Biotechnol. 2019, 7, 293. [Google Scholar] [CrossRef]
- Zhang, C.; Zhou, X.; Zhang, H.; Han, X.; Li, B.; Yang, R.; Zhou, X. Recent progress of novel nanotechnology challenging the multidrug resistance of cancer. Front. Pharmacol. 2022, 13, 776895. [Google Scholar] [CrossRef] [PubMed]
- Muggia, F.M.; Hainsworth, J.D.; Jeffers, S.; Miller, M.; Groshen, S.; Roman, L.; Uziely, B.; Muderspach, L.; Garcia, A.; Burnett, A.; et al. Phase II study of liposomal doxorubicin in refractory ovarian cancer: Antitumor activity and toxicity modification by liposomal encapsulation. J. Clin. Oncol. 1997, 15, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, E.; Poizot-Martin, I.; Saint-Marc, T.; Spano, J.P.; Cacoub, P. Phase IV study of liposomal daunorubicin (DaunoXome) in AIDS-related Kaposi sarcoma. Am. J. Clin. Oncol. 2002, 25, 57–59. [Google Scholar] [CrossRef] [PubMed]
- Salehi, B.; Selamoglu, Z.; Mileski, K.S.; Pezzani, R.; Redaelli, M.; Cho, W.C.; Kobarfard, F.; Rajabi, S.; Martorell, M.; Kumar, P.; et al. Liposomal cytarabine as cancer therapy: From chemistry to medicine. Biomolecules 2019, 9, 773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berges, R.; Bello, U. Effect of a new leuprorelin formulation on testosterone levels in patients with advanced prostate cancer. Curr. Med. Res. Opin. 2006, 22, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Wang, L.; Xu, H.Q.; Huang, X.E.; Qian, Y.D.; Xiang, J. Clinical comparison between paclitaxel liposome (Lipusu®) and paclitaxel for treatment of patients with metastatic gastric cancer. Asian Pac. J. Cancer Prev. 2013, 14, 2591–2594. [Google Scholar] [CrossRef] [Green Version]
- Fraguas-Sánchez, A.I.; Lozza, I.; Torres-Suárez, A.I. Actively targeted nanomedicines in breast cancer: From pre-clinal investigation to clinic. Cancers 2022, 14, 1198. [Google Scholar] [CrossRef]
- Luo, C.; Wang, Y.; Chen, Q.; Han, X.; Liu, X.; Sun, J.; He, Z. Advances of paclitaxel formulations based on nanosystem delivery technology. Mini. Rev. Med. Chem. 2012, 12, 434–444. [Google Scholar] [CrossRef]
- Douer, D. Efficacy and safety of vincristine sulfate liposome injection in the treatment of adult acute lymphocytic leukemia. Oncologist 2016, 21, 840–847. [Google Scholar] [CrossRef] [Green Version]
- Milano, G.; Innocenti, F.; Minami, H. Liposomal irinotecan (Onivyde): Exemplifying the benefits of nanotherapeutic drugs. Cancer Sci. 2022, 113, 2224–2231. [Google Scholar] [CrossRef]
- Kang, Y.K.; Ryu, M.H.; Park, S.H.; Kim, J.G.; Kim, J.W.; Cho, S.H.; Park, Y.I.; Park, S.R.; Rha, S.Y.; Kang, M.J.; et al. Efficacy and safety findings from DREAM: A phase III study of DHP107 (oral paclitaxel) versus i.v. paclitaxel in patients with advanced gastric cancer after failure of first-line chemotherapy. Ann. Oncol. 2018, 29, 1220–1226. [Google Scholar] [CrossRef] [PubMed]
- Cafaro, A.; Giannini, M.B.; Silimbani, P.; Cangini, D.; Masini, C.; Ghelli Luserna Di Rorà, A.; Simonetti, G.; Martinelli, G.; Cerchione, C. CPX-351 daunorubicin-cytarabine liposome: A novel formulation to treat patients with newly diagnosed secondary acute myeloid leukemia. Minerva Med. 2020, 111, 455–466. [Google Scholar] [CrossRef]
- Bar-Zeev, M.; Livney, Y.D.; Assaraf, Y.G. Targeted nanomedicine for cancer therapeutics: Towards precision medicine overcoming drug resistance. Drug Resist. Updat. 2017, 31, 15–30. [Google Scholar] [CrossRef]
- Lepeltier, E.; Rijo, P.; Rizzolio, F.; Popovtzer, R.; Petrikaite, V.; Assaraf, Y.G.; Passirani, C. Nanomedicine to target multidrug resistant tumors. Drug Resist. Updat. 2020, 52, 100704. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Song, M.; Li, W.; Huang, J.; Yang, G.; Wang, Y. Multifunctional nanoplatforms co-delivering combinatorial dual-drug for eliminating cancer multidrug resistance. Theranostics 2021, 11, 6334–6354. [Google Scholar] [CrossRef]
- Chen, Z.S.; Tiwari, A.K. Multidrug resistance proteins (MRPs/ABCCs) in cancer chemotherapy and genetic diseases. FEBS J. 2011, 278, 3226–3245. [Google Scholar] [CrossRef] [Green Version]
- Amawi, H.; Sim, H.M.; Tiwari, A.K.; Ambudkar, S.V.; Shukla, S. ABC transporter-mediated multidrug-resistant cancer. Adv. Exp. Med. Biol. 2019, 1141, 549–580. [Google Scholar] [CrossRef]
- Muriithi, W.; Macharia, L.W.; Heming, C.P.; Echevarria, J.L.; Nyachieo, A.; Filho, P.N.; Neto, V.M. ABC transporters and the hallmarks of cancer: Roles in cancer aggressiveness beyond multidrug resistance. Cancer Biol. Med. 2020, 17, 253–269. [Google Scholar] [CrossRef]
- Rothem, L.; Ifergan, I.; Kaufman, Y.; Priest, D.G.; Jansen, G.; Assaraf, Y.G. Resistance to multiple novel antifolates is mediated via defective drug transport resulting from clustered mutations in the reduced folate carrier gene in human leukaemia cell lines. Biochem. J. 2002, 367, 741–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosson, G. Reduced folate carrier: Biochemistry and molecular biology of the normal and methotrexate-resistant cell. Br. J. Biomed. Sci. 2003, 60, 117–129. [Google Scholar] [CrossRef]
- Kordus, S.L.; Baughn, A.D. Revitalizing antifolates through understanding mechanisms that govern susceptibility and resistance. Medchemcomm 2019, 10, 880–895. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Bai, L.; Hou, L.; Deng, H.; Luan, S.; Liu, D.; Huang, M.; Zhao, L. Trends in targeting Bcl-2 anti-apoptotic proteins for cancer treatment. Eur. J. Med. Chem. 2022, 232, 114184. [Google Scholar] [CrossRef] [PubMed]
- Cory, S.; Roberts, A.W.; Colman, P.M.; Adams, J.M. Targeting BCL-2-like proteins to kill cancer cells. Trends Cancer 2016, 2, 443–460. [Google Scholar] [CrossRef] [PubMed]
- Sarosiek, K.A.; Letai, A. Directly targeting the mitochondrial pathway of apoptosis for cancer therapy using BH3 mimetics-recent successes, current challenges and future promise. FEBS J. 2016, 283, 3523–3533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.Y.; Guan, Y.D.; Chen, X.S.; Yang, J.M.; Cheng, Y. DNA repair pathways in cancer therapy and resistance. Front. Pharmacol. 2021, 11, 629266. [Google Scholar] [CrossRef] [PubMed]
- Alhmoud, J.F.; Woolley, J.F.; Al Moustafa, A.E.; Malki, M.I. DNA damage/repair management in cancers. Cancers 2020, 12, 1050. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, M.; Kastan, M.B. The DNA damage response: Implications for tumor responses to radiation and chemotherapy. Annu. Rev. Med. 2015, 66, 129–143. [Google Scholar] [CrossRef] [Green Version]
- Dal Bo, M.; De Mattia, E.; Baboci, L.; Mezzalira, S.; Cecchin, E.; Assaraf, Y.G.; Toffoli, G. New insights into the pharmacological, immunological, and CAR-T-cell approaches in the treatment of hepatocellular carcinoma. Drug Resist. Updat. 2020, 51, 100702. [Google Scholar] [CrossRef] [PubMed]
- Holohan, C.; Van Schaeybroeck, S.; Longley, D.B.; Johnston, P.G. Cancer drug resistance: An evolving paradigm. Nat. Rev. Cancer 2013, 13, 714–726. [Google Scholar] [CrossRef] [PubMed]
- Geller, L.T.; Barzily-Rokni, M.; Danino, T.; Jonas, O.H.; Shental, N.; Nejman, D.; Gavert, N.; Zwang, Y.; Cooper, Z.A.; Shee, K.; et al. Potential role of intratumor bacteria in mediating tumor resistance to the chemotherapeutic drug gemcitabine. Science 2017, 357, 1156–1160. [Google Scholar] [CrossRef] [Green Version]
- Dartier, J.; Lemaitre, E.; Chourpa, I.; Goupille, C.; Servais, S.; Chevalier, S.; Mahéo, K.; Dumas, J.F. ATP-dependent activity and mitochondrial localization of drug efflux pumps in doxorubicin-resistant breast cancer cells. Biochim. Biophys. Acta Gen. Subj. 2017, 1861, 1075–1084. [Google Scholar] [CrossRef]
- Ruan, L.; Chen, J.; Du, C.; Lu, H.; Zhang, J.; Cai, X.; Dou, R.; Lin, W.; Chai, Z.; Nie, G.; et al. Mitochondrial temperature-responsive drug delivery reverses drug resistance in lung cancer. Bioact. Mater. 2021, 13, 191–199. [Google Scholar] [CrossRef]
- Cheng, F.; Pan, Q.; Gao, W.; Pu, Y.; Luo, K.; He, B. Reversing chemotherapy resistance by a synergy between lysosomal pH-activated mitochondrial drug delivery and erlotinib-mediated drug efflux inhibition. ACS Appl. Mater. Interfaces 2021, 13, 29257–29268. [Google Scholar] [CrossRef]
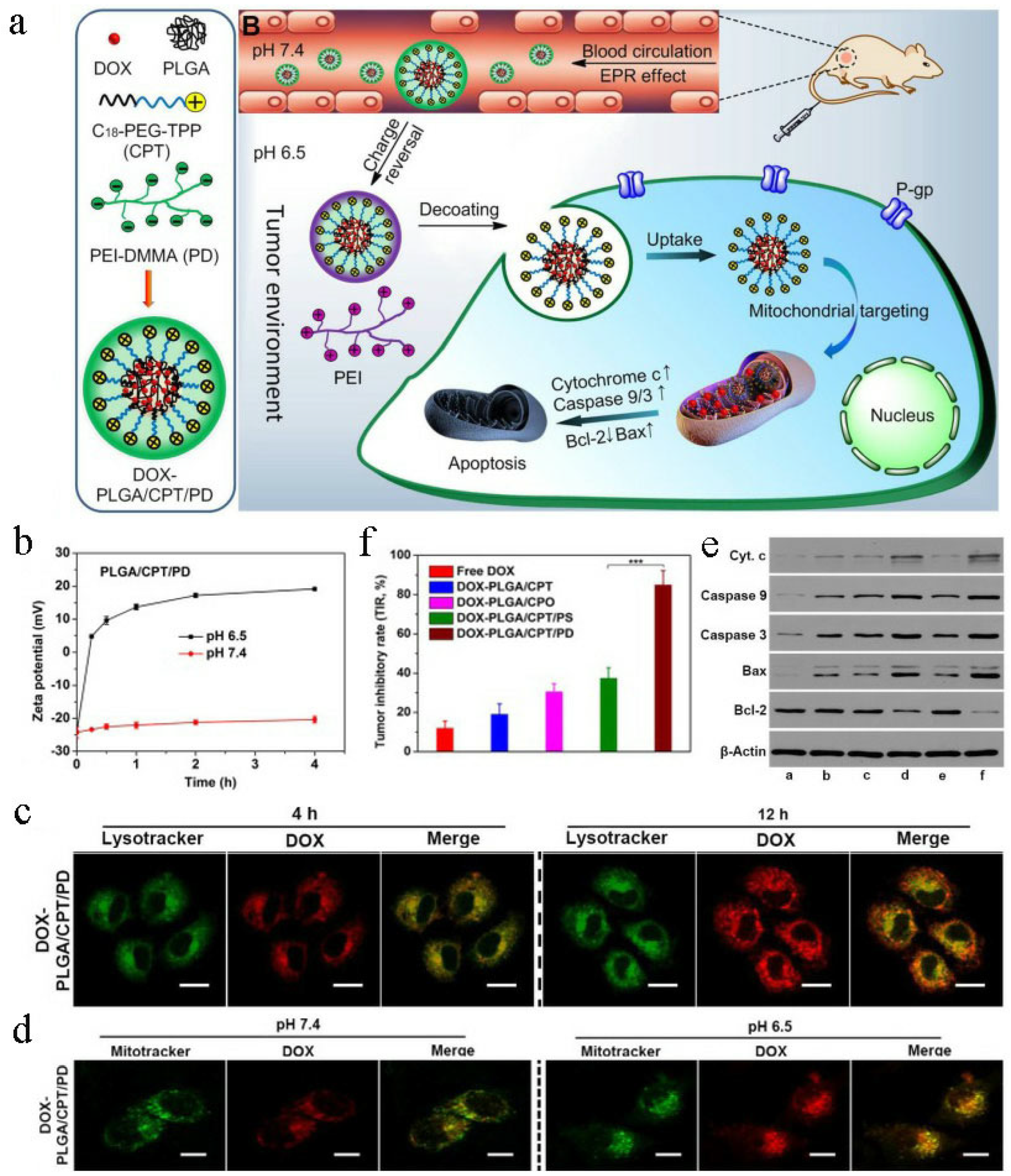
- Zhou, M.; Li, L.; Li, L.; Lin, X.; Wang, F.; Li, Q.; Huang, Y. Overcoming chemotherapy resistance via simultaneous drug-efflux circumvention and mitochondrial targeting. Acta Pharm. Sin. B 2019, 9, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, C.; Chen, J.; Liu, L.; Hu, M.; Li, J.; Bi, H. Trackable mitochondria-targeting nanomicellar loaded with doxorubicin for overcoming drug resistance. ACS Appl. Mater. Interfaces 2017, 9, 25152–25163. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.; Peng, Y.; Qiu, L. Mitochondria-targeted vitamin E succinate delivery for reversal of multidrug resistance. J. Control. Release 2021, 337, 117–131. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.; Sun, Y.; Li, Y.; Ma, X.; Zhang, S.; Yuan, Y.; Kohn, J.; Liu, C.; Qian, J. Synergistic combination of bioactive hydroxyapatite nanoparticles and the chemotherapeutic doxorubicin to overcome tumor multidrug resistance. Small 2021, 17, e2007672. [Google Scholar] [CrossRef] [PubMed]
- Gao, D.; Zhu, Q.; Ruan, J.; Sun, T.; Han, L. Polyplexes by polymerized dequalinium and bifunctional aptamer for mitochondrial targeting drug release to overcome drug resistance. ACS Appl. Bio. Mater. 2020, 3, 5182–5192. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, X.; Zhou, M.; Nan, X.; Chen, X.; Zhang, X. Mitochondrial-targeting lonidamine-doxorubicin nanoparticles for synergistic chemotherapy to conquer drug resistance. ACS Appl. Mater. Interfaces 2017, 9, 43498–43507. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Li, J.M.; Deng, K.; Zhou, W.; Wang, C.X.; Wang, Q.; Li, K.H.; Zhao, H.Y.; Huang, S.W. Tumor acidity activated triphenylphosphonium-based mitochondrial targeting nanocarriers for overcoming drug resistance of cancer therapy. Theranostics 2019, 9, 7033–7050. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Yu, H.; Zhang, L.J.; Wu, B.; Wang, C.X.; Wang, Q.; Deng, K.; Zhuo, R.X.; Huang, S.W. Redox-triggered activation of nanocarriers for mitochondria-targeting cancer chemotherapy. Nanoscale 2017, 9, 17044–17053. [Google Scholar] [CrossRef] [PubMed]
- Xiang, L.; Wang, Y.; Lan, J.; Na, F.; Wu, S.; Gong, Y.; Du, H.; Shao, B.; Xie, G. HIF-1-dependent heme synthesis promotes gemcitabine resistance in human non-small cell lung cancers via enhanced ABCB6 expression. Cell. Mol. Life Sci. 2022, 79, 343. [Google Scholar] [CrossRef] [PubMed]
- Samanta, D.; Gilkes, D.M.; Chaturvedi, P.; Xiang, L.; Semenza, G.L. Hypoxia-inducible factors are required for chemotherapy resistance of breast cancer stem cells. Proc. Natl. Acad. Sci. USA 2014, 111, E5429–E5438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karakashev, S.V.; Reginato, M.J. Progress toward overcoming hypoxia-induced resistance to solid tumor therapy. Cancer Manag. Res. 2015, 7, 253–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghattass, K.; Assah, R.; El-Sabban, M.; Gali-Muhtasib, H. Targeting hypoxia for sensitization of tumors to radio- and chemotherapy. Curr. Cancer Drug Targets 2013, 13, 670–685. [Google Scholar] [CrossRef]
- Albadari, N.; Deng, S.; Li, W. The transcriptional factors HIF-1 and HIF-2 and their novel inhibitors in cancer therapy. Expert Opin. Drug Discov. 2019, 14, 667–682. [Google Scholar] [CrossRef]
- Lu, H.; Samanta, D.; Xiang, L.; Zhang, H.; Hu, H.; Chen, I.; Bullen, J.W.; Semenza, G.L. Chemotherapy triggers HIF-1-dependent glutathione synthesis and copper chelation that induces the breast cancer stem cell phenotype. Proc. Natl. Acad. Sci. USA 2015, 112, E4600–E4609. [Google Scholar] [CrossRef] [Green Version]
- Luo, K.; Guo, W.; Yu, Y.; Xu, S.; Zhou, M.; Xiang, K.; Niu, K.; Zhu, X.; Zhu, G.; An, Z.; et al. Reduction-sensitive platinum (IV)-prodrug nano-sensitizer with an ultra-high drug loading for efficient chemo-radiotherapy of Pt-resistant cervical cancer in vivo. J. Control. Release 2020, 326, 25–37. [Google Scholar] [CrossRef]
- Li, J.; Xi, W.; Li, X.; Sun, H.; Li, Y. Advances in inhibition of protein-protein interactions targeting hypoxia-inducible factor-1 for cancer therapy. Bioorg. Med. Chem. 2019, 27, 1145–1158. [Google Scholar] [CrossRef]
- Wang, X.; Du, Z.W.; Xu, T.M.; Wang, X.J.; Li, W.; Gao, J.L.; Li, J.; Zhu, H. HIF-1α is a rational target for future ovarian cancer therapies. Front. Oncol. 2021, 11, 785111. [Google Scholar] [CrossRef]
- Shirai, Y.; Chow, C.C.T.; Kambe, G.; Suwa, T.; Kobayashi, M.; Takahashi, I.; Harada, H.; Nam, J.M. An overview of the recent development of anticancer agents targeting the HIF-1 transcription factor. Cancers 2021, 13, 2813. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Zhao, G. Small molecules targeting HIF-1α pathway for cancer therapy in recent years. Bioorg. Med. Chem. 2020, 28, 115235. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.; Xiang, X.; Li, S.; Xie, P.; Gong, Q.; Goh, B.C.; Wang, L. Targeting hypoxia-inducible factor-1, for cancer treatment: Recent advances in developing small-molecule inhibitors from natural compounds. Semin. Cancer Biol. 2022, 80, 379–390. [Google Scholar] [CrossRef] [PubMed]
- Montigaud, Y.; Ucakar, B.; Krishnamachary, B.; Bhujwalla, Z.M.; Feron, O.; Préat, V.; Danhier, F.; Gallez, B.; Danhier, P. Optimized acriflavine-loaded lipid nanocapsules as a safe and effective delivery system to treat breast cancer. Int. J. Pharm. 2018, 551, 322–328. [Google Scholar] [CrossRef]
- Weijer, R.; Broekgaarden, M.; Krekorian, M.; Alles, L.K.; van Wijk, A.C.; Mackaaij, C.; Verheij, J.; van der Wal, A.C.; van Gulik, T.M.; Storm, G.; et al. Inhibition of hypoxia inducible factor 1 and topoisomerase with acriflavine sensitizes perihilar cholangiocarcinomas to photodynamic therapy. Oncotarget 2016, 7, 3341–3356. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; He, C.; Liu, X.; Chen, Y.; Zhao, P.; Chen, C.; Yan, R.; Li, M.; Fan, T.; Altine, B.; et al. One-pot synthesis of a microporous organosilica-coated cisplatin nanoplatform for HIF-1-targeted combination cancer therapy. Theranostics 2020, 10, 2918–2929. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Bao, Q.; Chen, Z.; Yao, L.; Ci, Z.; Wei, X.; Wu, Y.; Zhu, J.; Sun, K.; Zhou, G.; et al. Circumventing drug resistance pathways with a nanoparticle-based photodynamic method. Nano Lett. 2021, 21, 9115–9123. [Google Scholar] [CrossRef]
- Li, Y.; Deng, Y.; Tian, X.; Ke, H.; Guo, M.; Zhu, A.; Yang, T.; Guo, Z.; Ge, Z.; Yang, X.; et al. Multipronged design of light-triggered nanoparticles to overcome cisplatin resistance for efficient ablation of resistant tumor. ACS Nano 2015, 9, 9626–9637. [Google Scholar] [CrossRef]
- Yang, G.G.; Pan, Z.Y.; Zhang, D.Y.; Cao, Q.; Ji, L.N.; Mao, Z.W. Precisely assembled nanoparticles against cisplatin resistance via cancer-specific targeting of mitochondria and imaging-guided chemo-photothermal therapy. ACS Appl. Mater. Interfaces 2020, 12, 43444–43455. [Google Scholar] [CrossRef]
- Wang, T.; Wang, D.; Yu, H.; Wang, M.; Liu, J.; Feng, B.; Zhou, F.; Yin, Q.; Zhang, Z.; Huang, Y.; et al. Intracellularly acid-switchable multifunctional micelles for combinational photo/chemotherapy of the drug-resistant tumor. ACS Nano 2016, 10, 3496–3508. [Google Scholar] [CrossRef]
- Souslova, T.; Averill-Bates, D.A. Multidrug-resistant hela cells overexpressing MRP1 exhibit sensitivity to cell killing by hyperthermia: Interactions with etoposide. Int. J Radiat. Oncol. Biol. Phys. 2004, 60, 1538–1551. [Google Scholar] [CrossRef] [PubMed]
- Stein, U.; Jürchott, K.; Walther, W.; Bergmann, S.; Schlag, P.M.; Royer, H.D. Hyperthermia-induced nuclear translocation of transcription factor YB-1 leads to enhanced expression of multidrug resistance-related ABC transporters. J. Biol. Chem. 2001, 276, 28562–28569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nair, J.B.; Joseph, M.M.; Arya, J.S.; Sreedevi, P.; Sujai, P.T.; Maiti, K.K. Elucidating a thermoresponsive multimodal photo-chemotherapeutic nanodelivery vehicle to overcome the barriers of doxorubicin therapy. ACS Appl. Mater. Interfaces 2020, 12, 43365–43379. [Google Scholar] [CrossRef]
- Jiang, D.; Xu, M.; Pei, Y.; Huang, Y.; Chen, Y.; Ma, F.; Lu, H.; Chen, J. Core-matched nanoassemblies for targeted co-delivery of chemotherapy and photosensitizer to treat drug-resistant cancer. Acta Biomater. 2019, 88, 406–421. [Google Scholar] [CrossRef] [PubMed]
- Jiang, D.; Gao, X.; Kang, T.; Feng, X.; Yao, J.; Yang, M.; Jing, Y.; Zhu, Q.; Feng, J.; Chen, J. Actively targeting D-α-tocopheryl polyethylene glycol 1000 succinate-poly(lactic acid) nanoparticles as vesicles for chemo-photodynamic combination therapy of doxorubicin-resistant breast cancer. Nanoscale 2016, 8, 3100–3118. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wang, H.; Chen, Y.; Wang, Y.; Li, H.; Han, H.; Chen, T.; Jin, Q.; Ji, J. pH- and NIR light-responsive polymeric prodrug micelles for hyperthermia-assisted site-specific chemotherapy to reverse drug resistance in cancer treatment. Small 2016, 12, 2731–2740. [Google Scholar] [CrossRef] [PubMed]
- Gaio, E.; Conte, C.; Esposito, D.; Miotto, G.; Quaglia, F.; Moret, F.; Reddi, E. Co-delivery of docetaxel and disulfonate tetraphenyl chlorin in one nanoparticle produces strong synergism between chemo- and photodynamic therapy in drug-sensitive and -resistant cancer cells. Mol. Pharm. 2018, 15, 4599–4611. [Google Scholar] [CrossRef]
- Shi, C.; Huang, H.; Zhou, X.; Zhang, Z.; Ma, H.; Yao, Q.; Shao, K.; Sun, W.; Du, J.; Fan, J.; et al. Reversing multidrug resistance by inducing mitochondrial dysfunction for enhanced chemo-photodynamic therapy in tumor. ACS Appl. Mater. Interfaces 2021, 13, 45259–45268. [Google Scholar] [CrossRef]
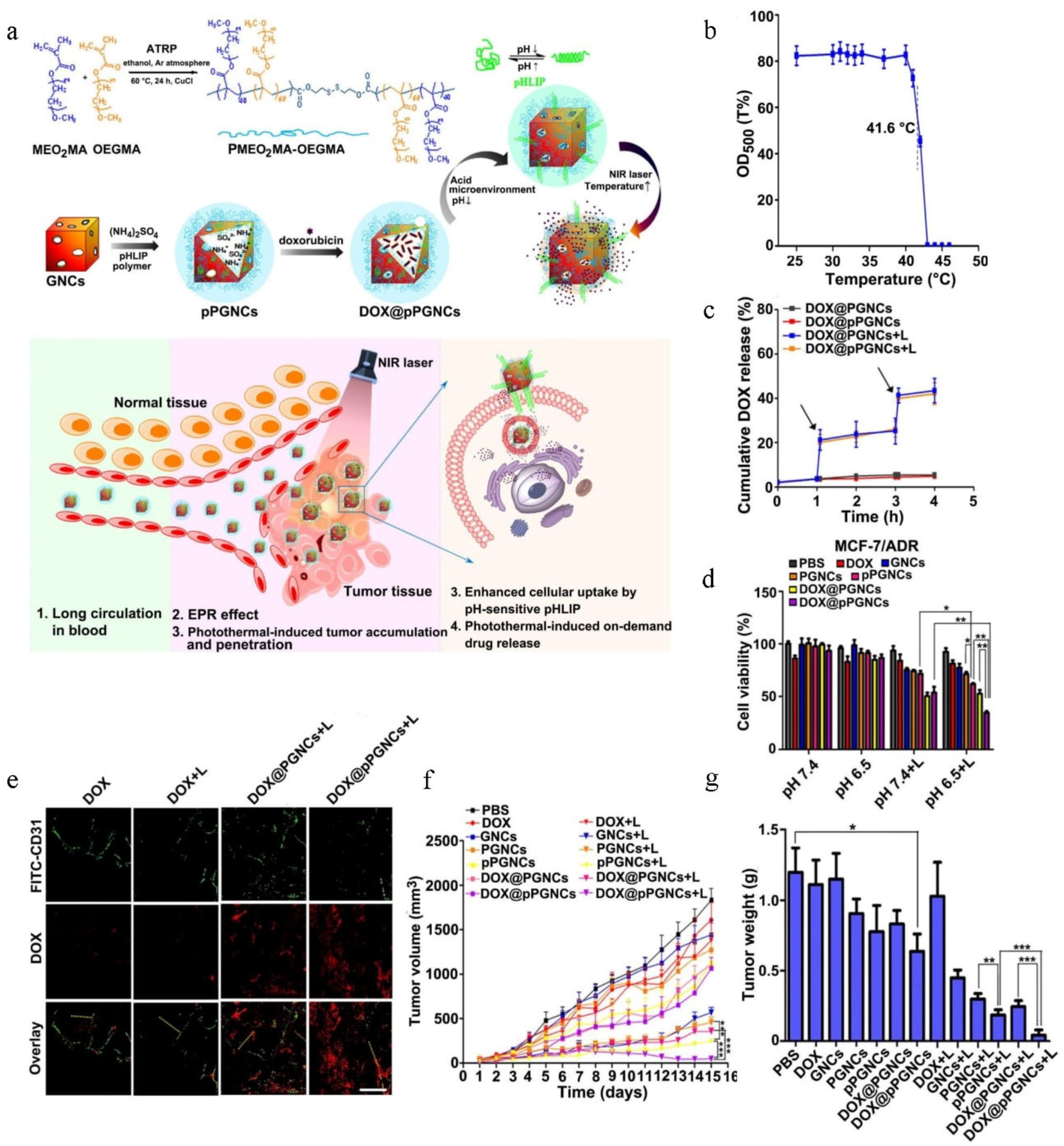
- Huang, W.; Zhao, H.; Wan, J.; Zhou, Y.; Xu, Q.; Zhao, Y.; Yang, X.; Gan, L. pH- and photothermal-driven multistage delivery nanoplatform for overcoming cancer drug resistance. Theranostics 2019, 9, 3825–3839. [Google Scholar] [CrossRef]
- Shi, W.; Zhang, P.; Zou, F.; Zhou, J.; Yin, Z.; Cai, Z.; Ghaleb, H.; Jiang, Y.; Huang, W.; Liu, Y.; et al. Exploration of novel phthalazinone derivatives as potential efflux transporter inhibitors for reversing multidrug resistance and improving the oral absorption of paclitaxel. Eur. J. Med. Chem. 2022, 233, 114231. [Google Scholar] [CrossRef]
- Dong, J.; Qin, Z.; Zhang, W.-D.; Cheng, G.; Yehuda, A.G.; Ashby, C.R., Jr.; Chen, Z.-S.; Cheng, X.-D.; Qin, J.-J. Medicinal chemistry strategies to discover P-glycoprotein inhibitors: An update. Drug Resist. Updat. 2020, 49, 100681. [Google Scholar] [CrossRef] [PubMed]
- Halder, J.; Pradhan, D.; Kar, B.; Ghosh, G.; Rath, G. Nanotherapeutics approaches to overcome P-glycoprotein-mediated multi-drug resistance in cancer. Nanomedicine 2022, 40, 102494. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Xu, H.; Ashby, C.R., Jr.; Assaraf, Y.G.; Chen, Z.S.; Liu, H.M. Chemical molecular-based approach to overcome multidrug resistance in cancer by targeting P-glycoprotein (P-gp). Med. Res. Rev. 2021, 41, 525–555. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Shi, T.; Zhang, L.; Zhu, P.; Deng, M.; Huang, C.; Hu, T.; Jiang, L.; Li, J. Mammalian drug efflux transporters of the ATP binding cassette (ABC) family in multidrug resistance: A review of the past decade. Cancer Lett. 2016, 370, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Rana, M.S.; Ediriweera, M.K.; Rajagopalan, U.; Karunaratne, D.N.; Tennekoon, K.H.; Samarakoon, S.R. A new liposomal nanocarrier for co-delivery of gedunin and p-glycoprotein siRNA to target breast cancer stem cells. Nat. Prod. Res. 2022, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Kara, G.; Calin, G.A.; Ozpolat, B. RNAi-based therapeutics and tumor targeted delivery in cancer. Adv. Drug Deliv. Rev. 2022, 182, 114113. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, N.S.; Tekade, R.K.; Chougule, M.B. Nanocarrier mediated delivery of siRNA/miRNA in combination with chemotherapeutic agents for cancer therapy: Current progress and advances. J. Control. Release 2014, 194, 238–256. [Google Scholar] [CrossRef] [Green Version]
- Tsouris, V.; Joo, M.K.; Kim, S.H.; Kwon, I.C.; Won, Y.Y. Nano carriers that enable co-delivery of chemotherapy and RNAi agents for treatment of drug-resistant cancers. Biotechnol. Adv. 2014, 32, 1037–1050. [Google Scholar] [CrossRef]
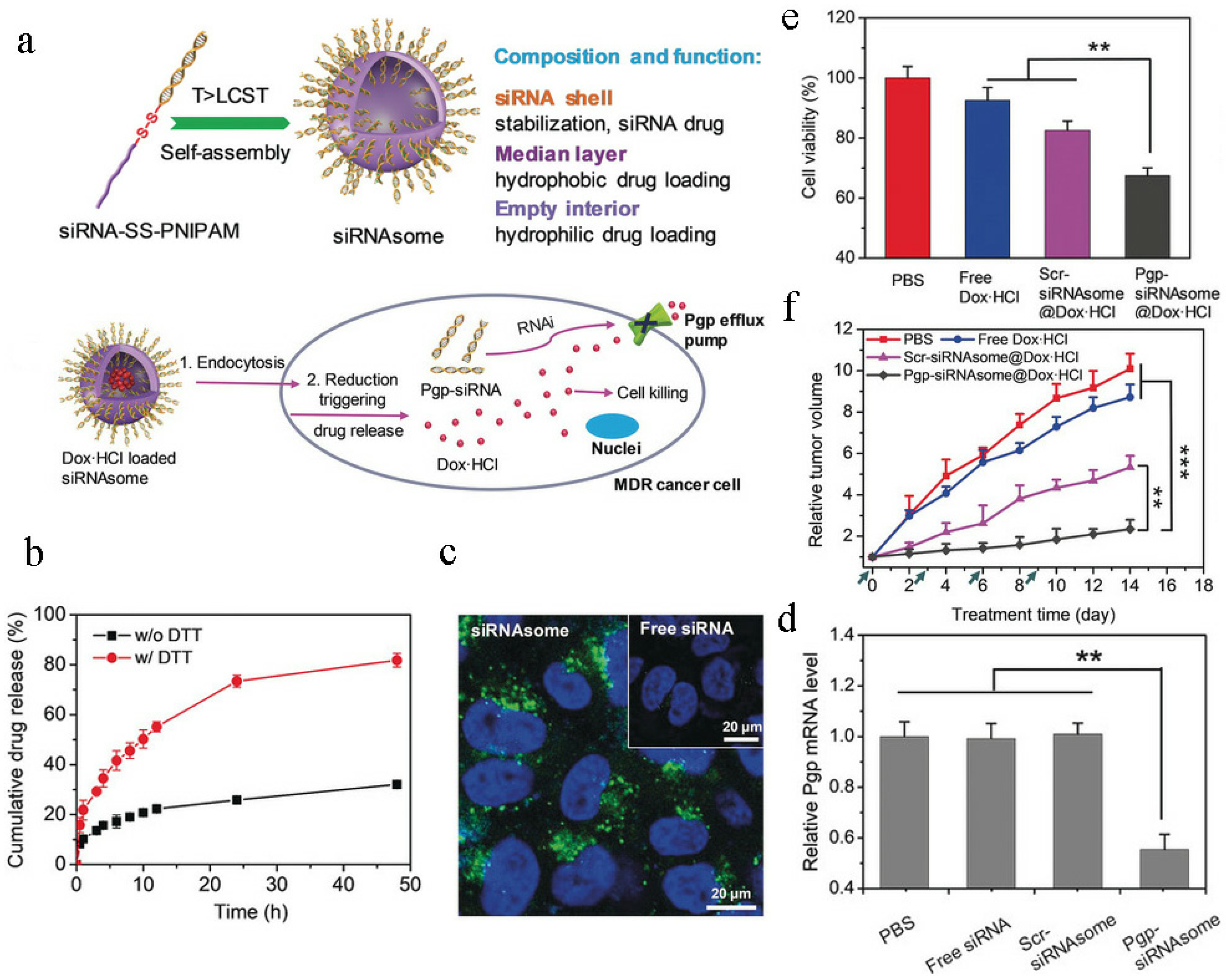
- Zheng, M.; Jiang, T.; Yang, W.; Zou, Y.; Wu, H.; Liu, X.; Zhu, F.; Qian, R.; Ling, D.; McDonald, K.; et al. The siRNAsome: A cation-free and versatile nanostructure for siRNA and drug co-delivery. Angew. Chem. Int. Ed. 2019, 58, 4938–4942. [Google Scholar] [CrossRef]
- Curtin, N.J. DNA repair dysregulation from cancer driver to therapeutic target. Nat. Rev. Cancer 2012, 12, 801–817. [Google Scholar] [CrossRef]
- Yang, C.; Zang, W.; Tang, Z.; Ji, Y.; Xu, R.; Yang, Y.; Luo, A.; Hu, B.; Zhang, Z.; Liu, Z.; et al. A20/TNFAIP3 regulates the DNA damage response and mediates tumor cell resistance to DNA-damaging therapy. Cancer Res. 2018, 78, 1069–1082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stover, E.H.; Konstantinopoulos, P.A.; Matulonis, U.A.; Swisher, E.M. Biomarkers of response and resistance to DNA repair targeted therapies. Clin. Cancer Res. 2016, 22, 5651–5660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadoughi, F.; Mirsafaei, L.; Dana, P.M.; Hallajzadeh, J.; Asemi, Z.; Mansournia, M.A.; Montazer, M.; Hosseinpour, M.; Yousefi, B. The role of DNA damage response in chemo- and radio-resistance of cancer cells: Can DDR inhibitors sole the problem? DNA Repair 2021, 101, 103074. [Google Scholar] [CrossRef] [PubMed]
- Bouwman, P.; Jonkers, J. The effects of deregulated DNA damage signalling on cancer chemotherapy response and resistance. Nat. Rev. Cancer 2012, 12, 587–598. [Google Scholar] [CrossRef]
- Pilié, P.G.; Tang, C.; Mills, G.B.; Yap, T.A. State-of-the-art strategies for targeting the DNA damage response in cancer. Nat. Rev. Clin. Oncol. 2019, 16, 81–104. [Google Scholar] [CrossRef]
- Sharma, M.; Anand, P.; Padwad, Y.S.; Dogra, V.; Acharya, V. DNA damage response proteins synergistically affect the cancer prognosis and resistance. Free. Radic. Biol. Med. 2022, 178, 174–188. [Google Scholar] [CrossRef]
- Li, L.; Kumar, A.K.; Hu, Z.; Guo, Z. Small molecule inhibitors targeting key proteins in the DNA damage response for cancer therapy. Curr. Med. Chem. 2021, 28, 963–985. [Google Scholar] [CrossRef]
- Zhu, Y.; Hu, J.; Hu, Y.; Liu, W. Targeting DNA repair pathways: A novel approach to reduce cancer therapeutic resistance. Cancer Treat. Rev. 2009, 35, 590–596. [Google Scholar] [CrossRef]
- Helleday, T.; Petermann, E.; Lundin, C.; Hodgson, B.; Sharma, R.A. DNA repair pathways as targets for cancer therapy. Nat. Rev. Cancer 2008, 8, 193–204. [Google Scholar] [CrossRef]
- Wang, L.; Yu, Y.; Wei, D.; Zhang, L.; Zhang, X.; Zhang, G.; Ding, D.; Xiao, H.; Zhang, D. A systematic strategy of combinational blow for overcoming cascade drug resistance via NIR-light-triggered hyperthermia. Adv. Mater. 2021, 33, e2100599. [Google Scholar] [CrossRef]
- Tang, Y.; Chen, Y.; Zhang, Z.; Tang, B.; Zhou, Z.; Chen, H. Nanoparticle-based RNAi therapeutics targeting cancer stem cells: Update and prospective. Pharmaceutics 2021, 13, 2116. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Song, X.; Xu, D.; Tiek, D.; Goenka, A.; Wu, B.; Sastry, N.; Hu, B.; Cheng, S.Y. Stem cell programs in cancer initiation, progression, and therapy resistance. Theranostics 2020, 10, 8721–8743. [Google Scholar] [CrossRef] [PubMed]
- Dean, M.; Fojo, T.; Bates, S. Tumor stem cells and drug resistance. Nat. Rev. Cancer 2005, 5, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Phi, L.T.H.; Sari, I.N.; Yang, Y.G.; Lee, S.H.; Jun, N.; Kim, K.S.; Lee, Y.K.; Kwon, H.Y. Cancer stem cells (CSCs) in drug resistance and their therapeutic implications in cancer treatment. Stem Cells Int. 2018, 2018, 5416923. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Mayea, Y.; Mir, C.; Masson, F.; Paciucci, R.; LLeonart, M.E. Insights into new mechanisms and models of cancer stem cell multidrug resistance. Semin. Cancer Biol. 2020, 60, 166–180. [Google Scholar] [CrossRef]
- Shen, S.; Xu, X.; Lin, S.; Zhang, Y.; Liu, H.; Zhang, C.; Mo, R. A nanotherapeutic strategy to overcome chemotherapeutic resistance of cancer stem-like cells. Nat. Nanotechnol. 2021, 16, 104–113. [Google Scholar] [CrossRef]
- Wei, X.; Liu, L.; Guo, X.; Wang, Y.; Zhao, J.; Zhou, S. Light-activated ROS-responsive nanoplatform co-delivering apatinib and doxorubicin for enhanced chemo-photodynamic therapy of multidrug-resistant tumors. ACS Appl. Mater. Interfaces 2018, 10, 17672–17684. [Google Scholar] [CrossRef]
- Byeon, Y.; Lee, J.W.; Choi, W.S.; Won, J.E.; Kim, G.H.; Kim, M.G.; Wi, T.I.; Lee, J.M.; Kang, T.H.; Jung, I.D.; et al. CD44-targeting PLGA nanoparticles incorporating paclitaxel and FAK siRNA overcome chemoresistance in epithelial ovarian cancer. Cancer Res. 2018, 78, 6247–6256. [Google Scholar] [CrossRef] [Green Version]
- Wei, X.; Liu, L.; Li, X.; Wang, Y.; Guo, X.; Zhao, J.; Zhou, S. Selectively targeting tumor-associated macrophages and tumor cells with polymeric micelles for enhanced cancer chemo-immunotherapy. J. Control. Release 2019, 313, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Xing, Y.; Ding, T.; Wang, Z.; Wang, L.; Guan, H.; Tang, J.; Mo, D.; Zhang, J. Temporally controlled photothermal/photodynamic and combined therapy for overcoming multidrug resistance of cancer by polydopamine nanoclustered micelles. ACS Appl. Mater. Interfaces 2019, 11, 13945–13953. [Google Scholar] [CrossRef]
- Baghbani, F.; Moztarzadeh, F. Bypassing multidrug resistant ovarian cancer using ultrasound responsive doxorubicin/curcumin co-deliver alginate nanodroplets. Colloids Surf. B Biointerfaces 2017, 153, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Sun, R.; Liu, X.; Li, G.; Wang, H.; Luo, Y.; Huang, G.; Wang, X.; Zeng, G.; Liu, Z.; Wu, S. Photoactivated H2 nanogenerator for enhanced chemotherapy of bladder cancer. ACS Nano 2020, 14, 8135–8148. [Google Scholar] [CrossRef] [PubMed]
- Younis, M.; Faming, W.; Hongyan, Z.; Mengmeng, T.; Hang, S.; Liudi, Y. Iguratimod encapsulated PLGA-NPs improves therapeutic outcome in glioma, glioma stem-like cells and temozolomide resistant glioma cells. Nanomedicine 2019, 22, 102101. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhang, M.; Jin, H.; Tang, Y.; Wu, A.; Xu, Q.; Huang, Y. Prodrug-like, PEGylated protein toxin trichosanthin for reversal of chemoresistance. Mol. Pharm. 2017, 14, 1429–1438. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Song, F.; Liu, Y.; Tian, J.; Liu, C.; Li, R.; Zhang, Q. A dual pH-sensitive liposomal system with charge-reversal and NO generation for overcoming multidrug resistance in cancer. Nanoscale 2019, 11, 3814–3826. [Google Scholar] [CrossRef]
- Kommineni, N.; Mahira, S.; Domb, A.J.; Khan, W. Cabazitaxel-loaded nanocarriers for cancer therapy with reduced side effects. Pharmaceutics 2019, 11, 141. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Wu, X.; Yang, H.; Li, L.; Ye, Z.; Rao, Y. A nuclear targeted Dox-aptamer loaded liposome delivery platform for the circumvention of drug resistance in breast cancer. Biomed. Pharmacother. 2019, 117, 109072. [Google Scholar] [CrossRef]
- Zhang, L.; Su, H.; Liu, Y.; Pang, N.; Li, J.; Qi, X.R. Enhancing solid tumor therapy with sequential delivery of dexamethasone and docetaxel engineered in a single carrier to overcome stromal resistance to drug delivery. J. Control. Release 2019, 294, 1–16. [Google Scholar] [CrossRef]
- Chen, Y.; Cheng, Y.; Zhao, P.; Zhang, S.; Li, M.; He, C.; Zhang, X.; Yang, T.; Yan, R.; Ye, P.; et al. Co-delivery of doxorubicin and imatinib by pH sensitive cleavable PEGylated nanoliposomes with folate-mediated targeting to overcome multidrug resistance. Int. J. Pharm. 2018, 542, 266–279. [Google Scholar] [CrossRef]
- Zhu, Y.X.; Jia, H.R.; Duan, Q.Y.; Liu, X.; Yang, J.; Liu, Y.; Wu, F.G. Photosensitizer-doped and plasma membrane-responsive liposomes for nuclear drug delivery and multidrug resistance reversal. ACS Appl. Mater. Interfaces 2020, 12, 36882–36894. [Google Scholar] [CrossRef]
- Wang, C.; Guan, W.; Peng, J.; Chen, Y.; Xu, G.; Dou, H. Gene/paclitaxel co-delivering nanocarriers prepared by framework-induced self-assembly for the inhibition of highly drug-resistant tumors. Acta Biomater. 2020, 103, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Jin, H.; Wang, C.; Zhang, Z.; Ruan, H.; Sun, L.; Yang, C.; Li, Y.; Qin, W.; Wang, C. Synergistic cisplatin/doxorubicin combination chemotherapy for multidrug-resistant cancer via polymeric nanogels targeting delivery. ACS Appl. Mater. Interfaces 2017, 9, 9426–9436. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Tung, C.H. Redox-responsive cisplatin nanogels for anticancer drug delivery. Chem. Commun. 2018, 54, 8367–8370. [Google Scholar] [CrossRef]
- Zhang, X.; Chen, X.; Guo, Y.; Jia, H.R.; Jiang, Y.W.; Wu, F.G. Endosome/lysosome-detained supramolecular nanogels as an efflux retarder and autophagy inhibitor for repeated photodynamic therapy of multidrug-resistant cancer. Nanoscale Horiz. 2020, 5, 481–487. [Google Scholar] [CrossRef]
- Sun, L.; Wang, D.; Chen, Y.; Wang, L.; Huang, P.; Li, Y.; Liu, Z.; Yao, H.; Shi, J. Core-shell hierarchical mesostructured silica nanoparticles for gene/chemo-synergetic stepwise therapy of multidrug-resistant cancer. Biomaterials 2017, 133, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Del Valle, A.C.; Yeh, C.K.; Huang, Y.F. Near infrared-activatable platinum-decorated gold nanostars for synergistic photothermal/ferroptotic therapy in combating cancer drug resistance. Adv. Healthc. Mater. 2020, 9, e2000864. [Google Scholar] [CrossRef]
- Wang, Z.; Chang, Z.M.; Shao, D.; Zhang, F.; Chen, F.; Li, L.; Ge, M.F.; Hu, R.; Zheng, X.; Wang, Y.; et al. Janus gold triangle-mesoporous silica nanoplatforms for hypoxia-activated radio-chemo-photothermal therapy of liver cancer. ACS Appl. Mater. Interfaces 2019, 11, 34755–34765. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Jiang, Z.; Xu, W.; Sun, T.; Zhuang, X.; Ding, J.; Chen, X. Spatiotemporally targeted nanomedicine overcomes hypoxia-induced drug resistance of tumor cells after disrupting neovasculature. Nano Lett. 2020, 20, 6191–6198. [Google Scholar] [CrossRef]
- Zhang, H.; Cui, W.; Qu, X.; Wu, H.; Qu, L.; Zhang, X.; Mäkilä, E.; Salonen, J.; Zhu, Y.; Yang, Z.; et al. Photothermal-responsive nanosized hybrid polymersome as versatile therapeutics codelivery nanovehicle for effective tumor suppression. Proc. Natl. Acad. Sci. USA 2019, 116, 7744–7749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, J.; Wang, F.; Wang, S.; Liu, L.; Liu, K.; Ye, Y.; Wang, Z.; Wang, H.; Chen, B.; Jiang, J.; et al. Hyperthermia-triggered on-demand biomimetic nanocarriers for synergetic photothermal and chemotherapy. Adv. Sci. 2020, 7, 1903642. [Google Scholar] [CrossRef] [Green Version]
- Yang, Q.; Xiao, Y.; Yin, Y.; Li, G.; Peng, J. Erythrocyte membrane-camouflaged IR780 and DTX coloading polymeric nanoparticles for imaging-guided cancer photo-chemo combination therapy. Mol. Pharm. 2019, 16, 3208–3220. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lv, F.M.; Wang, D.L.; Du, J.L.; Guo, H.Y.; Chen, H.N.; Zhao, S.J.; Liu, Z.P.; Liu, Y. Synergistic antitumor effects on drug-resistant breast cancer of paclitaxel/lapatinib composite canocrystals. Molecules 2020, 25, 604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; He, D.; Guo, Q.; Zhang, Z.; Ru, D.; Wang, L.; Gong, K.; Liu, F.; Duan, Y.; Li, H. Exosome-liposome hybrid nanoparticle codelivery of TP and miR497 conspicuously overcomes chemoresistant ovarian cancer. J. Nanobiotechnology 2022, 20, 50. [Google Scholar] [CrossRef] [PubMed]
- Russo, E.; Spallarossa, A.; Tasso, B.; Villa, C.; Brullo, C. Nanotechnology of tyrosine kinase inhibitors in cancer therapy: A perspective. Int. J. Mol. Sci. 2021, 22, 6538. [Google Scholar] [CrossRef]
- Liang, X.; Wu, P.; Yang, Q.; Xie, Y.; He, C.; Yin, L.; Yin, Z.; Yue, G.; Zou, Y.; Li, L.; et al. An update of new small-molecule anticancer drugs approved from 2015 to 2020. Eur. J. Med. Chem. 2021, 220, 113473. [Google Scholar] [CrossRef]
- Ferguson, F.M.; Gray, N.S. Kinase inhibitors: The road ahead. Nat. Rev. Drug Discov. 2018, 17, 353–377. [Google Scholar] [CrossRef]
- Attwood, M.M.; Fabbro, D.; Sokolov, A.V.; Knapp, S.; Schiöth, H.B. Trends in kinase drug discovery: Targets, indications and inhibitor design. Nat. Rev. Drug Discov. 2021, 20, 839–861. [Google Scholar] [CrossRef]
- Bergholz, J.S.; Wang, Q.; Kabraji, S.; Zhao, J.J. Integrating immunotherapy and targeted therapy in cancer treatment: Mechanistic insights and clinical implications. Clin. Cancer Res. 2020, 26, 5557–5566. [Google Scholar] [CrossRef]
- Chen, E.Y.; Raghunathan, V.; Prasad, V. An overview of cancer drugs approved by the US food and drug administration based on the surrogate end point of response rate. JAMA Intern. Med. 2019, 179, 915–921. [Google Scholar] [CrossRef]
- Du, J.; Yan, H.; Xu, Z.; Yang, B.; He, Q.; Wang, X.; Luo, P. Cutaneous toxicity of FDA-approved small-molecule kinase inhibitors. Expert Opin. Drug Metab. Toxicol. 2021, 17, 1311–1325. [Google Scholar] [CrossRef]
- Zhong, L.; Li, Y.; Xiong, L.; Wang, W.; Wu, M.; Yuan, T.; Yang, W.; Tian, C.; Miao, Z.; Wang, T.; et al. Small molecules in targeted cancer therapy: Advances, challenges, and future perspectives. Signal Transduct. Target. Ther. 2021, 6, 201. [Google Scholar] [CrossRef] [PubMed]
- Pisa, R.; Kapoor, T.M. Chemical strategies to overcome resistance against targeted anticancer therapeutics. Nat. Chem. Biol. 2020, 16, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Pi, M.; Kuang, H.; Yue, C.; Yang, Q.; Wu, A.; Li, Y.; Assaraf, Y.G.; Yang, D.H.; Wu, S. Targeting metabolism to overcome cancer drug resistance: A promising therapeutic strategy for diffuse large B cell lymphoma. Drug Resist. Updat. 2022, 61, 100822. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Ji, Q.; Li, Q. Resistance to anti-EGFR therapies in metastatic colorectal cancer: Underlying mechanisms and reversal strategies. J. Exp. Clin. Cancer Res. 2021, 40, 328. [Google Scholar] [CrossRef] [PubMed]
- Asao, T.; Takahashi, F.; Takahashi, K. Resistance to molecularly targeted therapy in non-small-cell lung cancer. Respir. Investig. 2019, 57, 20–26. [Google Scholar] [CrossRef]
- Ye, L.; Chen, X.; Zhou, F. EGFR-mutant NSCLC: Emerging novel drugs. Curr. Opin. Oncol. 2021, 33, 87–94. [Google Scholar] [CrossRef]
- Hochart, A.; Leblond, P.; Le Bourhis, X.; Meignan, S.; Tulasne, D. Inhibition du récepteur MET: Un espoir dans la lutte contre les résistances aux thérapies ciblées? [MET receptor inhibition: Hope against resistance to targeted therapies?]. Bull. Cancer. 2017, 104, 157–166. [Google Scholar] [CrossRef]
- Rezayatmand, H.; Razmkhah, M.; Razeghian-Jahromi, I. Drug resistance in cancer therapy: The Pandora’s Box of cancer stem cells. Stem Cell Res. Ther. 2022, 13, 181. [Google Scholar] [CrossRef]
- Adhikari, S.; Bhattacharya, A.; Adhikary, S.; Singh, V.; Gadad, S.S.; Roy, S.; Das, C. The paradigm of drug resistance in cancer: An epigenetic perspective. Biosci. Rep. 2022, 42, BSR20211812. [Google Scholar] [CrossRef]
- Najafi, M.; Farhood, B.; Mortezaee, K. Cancer stem cells (CSCs) in cancer progression and therapy. J. Cell Physiol. 2019, 234, 8381–8395. [Google Scholar] [CrossRef]
- Deng, J.; Shao, J.; Markowitz, J.S.; An, G. ABC transporters in multi-drug resistance and ADME-Tox of small molecule tyrosine kinase inhibitors. Pharm. Res. 2014, 31, 2237–2255. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Ye, J.; Xie, Q.; Liu, B.; Liu, M. Targeting regulated cell death with pharmacological small molecules: An update on autophagy-dependent cell death, ferroptosis, and necroptosis in cancer. J. Med. Chem. 2022, 65, 2989–3001. [Google Scholar] [CrossRef] [PubMed]
- Jones, V.S.; Huang, R.Y.; Chen, L.P.; Chen, Z.S.; Fu, L.; Huang, R.P. Cytokines in cancer drug resistance: Cues to new therapeutic strategies. Biochim. Biophys. Acta 2016, 1865, 255–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skoulidis, F.; Papadimitrakopoulou, V.A. Targeting the gatekeeper: Osimertinib in EGFR T790M mutation-positive non-small cell lung cancer. Clin. Cancer Res. 2017, 23, 618–622. [Google Scholar] [CrossRef] [Green Version]
- Mayor, S. Osimertinib effective in EGFR T790M-positive lung cancer. Lancet Oncol. 2017, 18, e9. [Google Scholar] [CrossRef]
- Carlisle, J.W.; Ramalingam, S.S. Role of osimertinib in the treatment of EGFR-mutation positive non-small-cell lung cancer. Future Oncol. 2019, 15, 805–816. [Google Scholar] [CrossRef]
- Tang, Z.H.; Lu, J.J. Osimertinib resistance in non-small cell lung cancer: Mechanisms and therapeutic strategies. Cancer Lett. 2018, 420, 242–246. [Google Scholar] [CrossRef]
- Lu, X.; Yu, L.; Zhang, Z.; Ren, X.; Smaill, J.B.; Ding, K. Targeting EGFRL858R/T790M and EGFRL858R/T790M/C797S resistance mutations in NSCLC: Current developments in medicinal chemistry. Med. Res. Rev. 2018, 38, 1550–1581. [Google Scholar] [CrossRef]
- Chen, W.; Yu, D.; Sun, S.Y.; Li, F. Nanoparticles for co-delivery of osimertinib and selumetinib to overcome osimertinib-acquired resistance in non-small cell lung cancer. Acta Biomater. 2021, 129, 258–268. [Google Scholar] [CrossRef]
- Lim, S.M.; Yang, S.D.; Lim, S.; Heo, S.G.; Daniel, S.; Markovets, A.; Minoo, R.; Pyo, K.H.; Yun, M.R.; Hong, M.H.; et al. Molecular landscape of osimertinib resistance in patients and patient-derived preclinical models. Ther. Adv. Med. Oncol. 2022, 14, 17588359221079125. [Google Scholar] [CrossRef] [PubMed]
- Chude, C.I.; Amaravadi, R.K. Targeting autophagy in cancer: Update on clinical trials and novel inhibitors. Int. J. Mol. Sci. 2017, 18, 1279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, J.M.M.; Towers, C.G.; Thorburn, A. Targeting autophagy in cancer. Nat. Rev. Cancer 2017, 17, 528–542. [Google Scholar] [CrossRef]
- Ishaq, M.; Ojha, R.; Sharma, A.P.; Singh, S.K. Autophagy in cancer: Recent advances and future directions. Semin. Cancer Biol. 2020, 66, 171–181. [Google Scholar] [CrossRef]
- Tan, Q.; Wang, Z.; Wang, Q.; Wang, Y.; Huang, Z.; Su, N.; Jin, M.; Kuang, L.; Qi, H.; Ni, Z.; et al. A novel FGFR1-binding peptide exhibits anti-tumor effect on lung cancer by inhibiting proliferation and angiogenesis. Int. J. Biol. Sci. 2018, 14, 1389–1398. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Han, L.L.; Du, F.; Liu, X.M.; Li, J.; Wang, H.H.; Song, M.H.; Li, Z.; Li, G.Y. FGFR1 induces acquired resistance against gefitinib by activating AKT/mTOR pathway in NSCLC. Onco Targets Ther. 2019, 12, 9809–9816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farnsworth, D.A.; Chen, Y.T.; de Rappard Yuswack, G.; Lockwood, W.W. Emerging molecular dependencies of mutant EGFR-Driven non-small cell lung cancer. Cells 2021, 10, 3553. [Google Scholar] [CrossRef]
- Vad-Nielsen, J.; Gammelgaard, K.R.; Daugaard, T.F.; Nielsen, A.L. Cause-and-effect relationship between FGFR1 expression and epithelial-mesenchymal transition in EGFR-mutated non-small cell lung cancer cells. Lung Cancer 2019, 132, 132–140. [Google Scholar] [CrossRef]
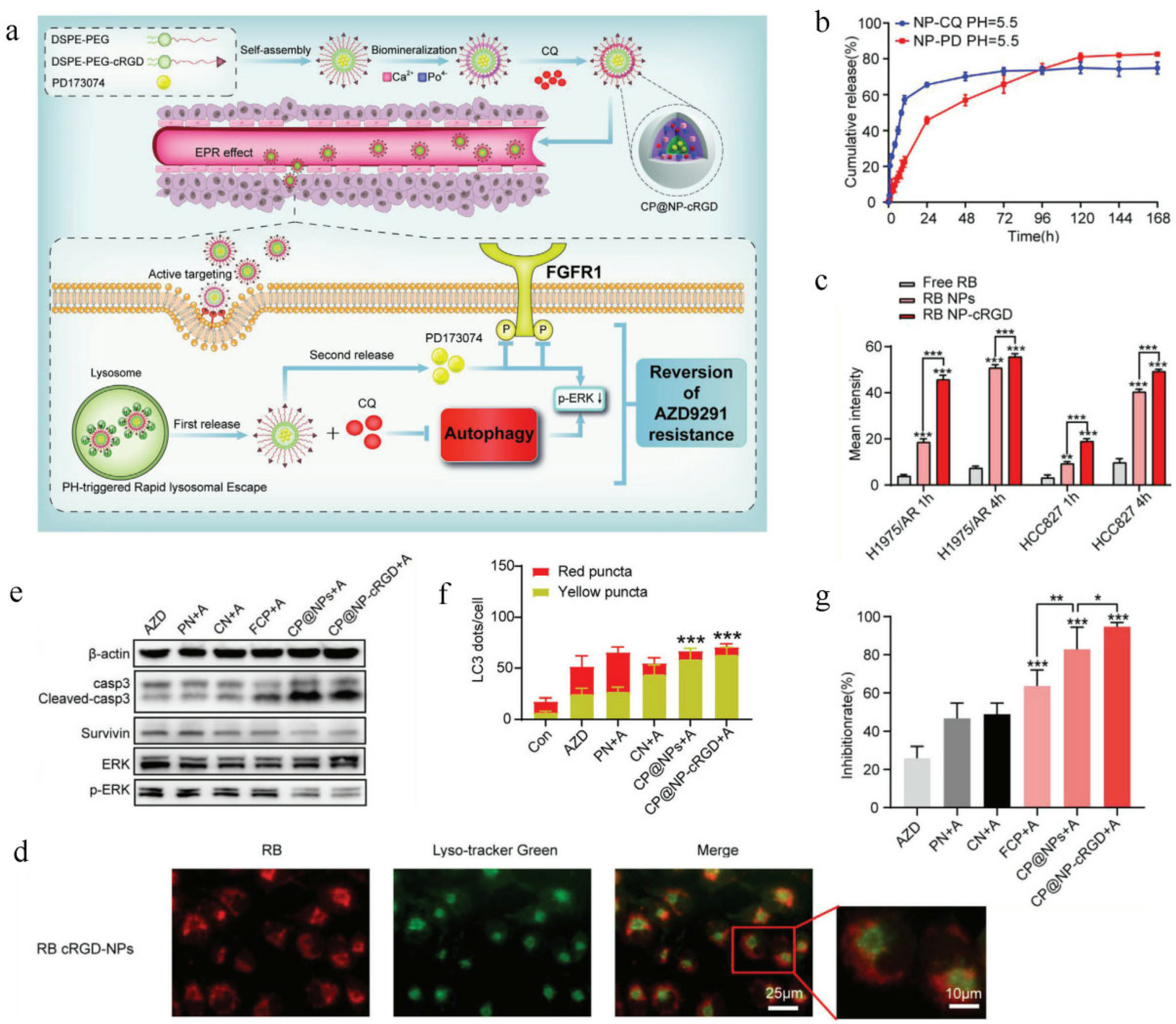
- Gu, Y.; Lai, S.; Dong, Y.; Fu, H.; Song, L.; Chen, T.; Duan, Y.; Zhang, Z. AZD9291 resistance reversal activity of a pH-sensitive nanocarrier dual-loaded with chloroquine and FGFR1 inhibitor in NSCLC. Adv. Sci. 2020, 8, 2002922. [Google Scholar] [CrossRef]
- Feng, Y.; Wang, L.; Wang, T.; Li, Y.; Xun, Q.; Zhang, R.; Liu, L.; Li, L.; Wang, W.; Tian, Y.; et al. Tumor cell-secreted exosomal miR-22-3p inhibits transgelin and induces vascular abnormalization to promote tumor budding. Mol. Ther. 2021, 29, 2151–2166. [Google Scholar] [CrossRef]
- Emami Nejad, A.; Najafgholian, S.; Rostami, A.; Sistani, A.; Shojaeifar, S.; Esparvarinha, M.; Nedaeinia, R.; Haghjooy Javanmard, S.; Taherian, M.; Ahmadlou, M.; et al. The role of hypoxia in the tumor microenvironment and development of cancer stem cell: A novel approach to developing treatment. Cancer Cell Int. 2021, 21, 62. [Google Scholar] [CrossRef]
- Mazumdar, J.; Dondeti, V.; Simon, M.C. Hypoxia-inducible factors in stem cells and cancer. J. Cell Mol. Med. 2009, 13, 4319–4328. [Google Scholar] [CrossRef] [PubMed]
- Jin, Q.; Huang, F.; Xu, X.; He, H.; Zhang, Y. High expression of hypoxia inducible factor 1α related with acquired resistant to EGFR tyrosine kinase inhibitors in NSCLC. Sci. Rep. 2021, 11, 1199. [Google Scholar] [CrossRef] [PubMed]
- Meng, S.; Wang, G.; Lu, Y.; Fan, Z. Functional cooperation between HIF-1α and c-Jun in mediating primary and acquired resistance to gefitinib in NSCLC cells with activating mutation of EGFR. Lung Cancer 2018, 121, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Liu, Y.; Oeck, S.; Zhang, G.J.; Schramm, A.; Glazer, P.M. Hypoxia induces resistance to EGFR inhibitors in lung cancer cells via upregulation of FGFR1 and the MAPK pathway. Cancer Res. 2020, 80, 4655–4667. [Google Scholar] [CrossRef] [PubMed]
- Bera, H.; Abosheasha, M.A.; Ito, Y.; Ueda, M. Hypoxia-responsive pullulan-based nanoparticles as erlotinib carriers. Int. J. Biol. Macromol. 2021, 191, 764–774. [Google Scholar] [CrossRef] [PubMed]
- Bera, H.; Abosheasha, M.A.; Ito, Y.; Ueda, M. Etherified pullulan-polyethylenimine based nanoscaffolds improved chemosensitivity of erlotinib on hypoxic cancer cells. Carbohydr. Polym. 2021, 271, 118441. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Xu, L.; Li, X.; Li, Z.; Wang, J.; Chen, H.; Li, X.; Gao, Y. Co-delivery of gefitinib and hematoporphyrin by aptamer-modified fluorinated dendrimer for hypoxia alleviation and enhanced synergistic chemo-photodynamic therapy of NSCLC. Eur. J. Pharm. Sci. 2021, 167, 106004. [Google Scholar] [CrossRef] [PubMed]
- Guan, Q.; Li, Y.; Zhang, H.; Liu, S.; Ding, Z.; Fan, Z.; Wang, Q.; Wang, Z.; Han, J.; Liu, M.; et al. Laser-responsive multi-functional nanoparticles for efficient combinational chemo-photodynamic therapy against breast cancer. Colloids Surf. B Biointerfaces 2022, 216, 112574. [Google Scholar] [CrossRef] [PubMed]
- Gong, G.; Pan, J.; He, Y.; Shang, J.; Wang, X.; Zhang, Y.; Zhang, G.; Wang, F.; Zhao, G.; Guo, J. Self-assembly of nanomicelles with rationally designed multifunctional building blocks for synergistic chemo-photodynamic therapy. Theranostics 2022, 12, 2028–2040. [Google Scholar] [CrossRef]
- Wang, Y.; Huo, J.; Li, S.; Huang, R.; Fan, D.; Cheng, H.; Wan, B.; Du, Y.; He, H.; Zhang, G. Self-rectifiable and hypoxia-assisted chemo-photodynamic nanoinhibitor for synergistic cancer therapy. ACS Appl. Mater. Interfaces 2022, 14, 10092–10101. [Google Scholar] [CrossRef]
- Yang, Y.; Chen, F.; Xu, N.; Yao, Q.; Wang, R.; Xie, X.; Zhang, F.; He, Y.; Shao, D.; Dong, W.F.; et al. Red-light-triggered self-destructive mesoporous silica nanoparticles for cascade-amplifying chemo-photodynamic therapy favoring antitumor immune responses. Biomaterials 2022, 281, 121368. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Wang, S.; Deng, D.; Xiao, Z.; Dong, Z.; Wang, Z.; Lei, Q.; Gao, S.; Huang, G.; Zhang, E.; et al. Fluorinated chitosan to enhance transmucosal delivery of sonosensitizer-conjugated catalase for sonodynamic bladder cancer treatment post-intravesical instillation. ACS Nano 2020, 14, 1586–1599. [Google Scholar] [CrossRef] [PubMed]
- She, J.; Zhou, X.; Zhang, Y.; Zhang, R.; Li, Q.; Zhu, W.; Meng, Z.; Liu, Z. Thermo-triggered in situ chitosan-based gelation system for repeated and enhanced sonodynamic therapy post a single injection. Adv. Healthc. Mater. 2021, 10, e2001208. [Google Scholar] [CrossRef] [PubMed]
- Yuan, M.; Liang, S.; Zhou, Y.; Xiao, X.; Liu, B.; Yang, C.; Ma, P.; Cheng, Z.; Lin, J. A robust oxygen-carrying hemoglobin-based natural sonosensitizer for sonodynamic cancer therapy. Nano Lett. 2021, 21, 6042–6050. [Google Scholar] [CrossRef] [PubMed]
- Ren, Q.; Yu, N.; Wang, L.; Wen, M.; Geng, P.; Jiang, Q.; Li, M.; Chen, Z. Nanoarchitectonics with metal-organic frameworks and platinum nanozymes with improved oxygen evolution for enhanced sonodynamic/chemo-therapy. J. Colloid Interface Sci. 2022, 614, 147–159. [Google Scholar] [CrossRef]
- Sun, D.; Pang, X.; Cheng, Y.; Ming, J.; Xiang, S.; Zhang, C.; Lv, P.; Chu, C.; Chen, X.; Liu, G.; et al. Ultrasound-switchable nanozyme augments sonodynamic therapy against multidrug-resistant bacterial infection. ACS Nano 2020, 14, 2063–2076. [Google Scholar] [CrossRef]
- Gong, Z.; Dai, Z. Design and challenges of sonodynamic therapy system for cancer theranostics: From equipment to sensitizers. Adv. Sci. 2021, 8, 2002178. [Google Scholar] [CrossRef]
- Dong, C.; Hu, H.; Sun, L.; Chen, Y. Inorganic chemoreactive nanosonosensitzers with unique physiochemical properties and structural features for versatile sonodynamic nanotherapies. Biomed. Mater. 2021, 16, 032006. [Google Scholar] [CrossRef]
- Li, D.; Yang, Y.; Li, D.; Pan, J.; Chu, C.; Liu, G. Organic sonosensitizers for sonodynamic therapy: From small molecules and nanoparticles toward clinical development. Small 2021, 17, e2101976. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Zhang, L.; Wang, J.; Zhu, L.; Li, Z.; Chen, H.; Gao, Y. An intelligent hypoxia-relieving chitosan-based nanoplatform for enhanced targeted chemo-sonodynamic combination therapy on lung cancer. Carbohydr. Polym. 2021, 274, 118655. [Google Scholar] [CrossRef] [PubMed]
- Wood, S.L.; Pernemalm, M.; Crosbie, P.A.; Whetton, A.D. The role of the tumor-microenvironment in lung cancer-metastasis and its relationship to potential therapeutic targets. Cancer Treat. Rev. 2014, 40, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Breindel, J.L.; Haskins, J.W.; Cowell, E.P.; Zhao, M.; Nguyen, D.X.; Stern, D.F. EGF receptor activates MET through MAPK to enhance non-small cell lung carcinoma invasion and brain metastasis. Cancer Res. 2013, 73, 5053–5065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellerino, A.; Bruno, F.; Rudà, R.; Soffietti, R. Systemic therapy for lung cancer brain metastases. Curr. Treat. Options Oncol. 2021, 22, 110. [Google Scholar] [CrossRef] [PubMed]
- Franchino, F.; Rudà, R.; Soffietti, R. Mechanisms and therapy for cancer metastasis to the brain. Front. Oncol. 2018, 8, 161. [Google Scholar] [CrossRef] [Green Version]
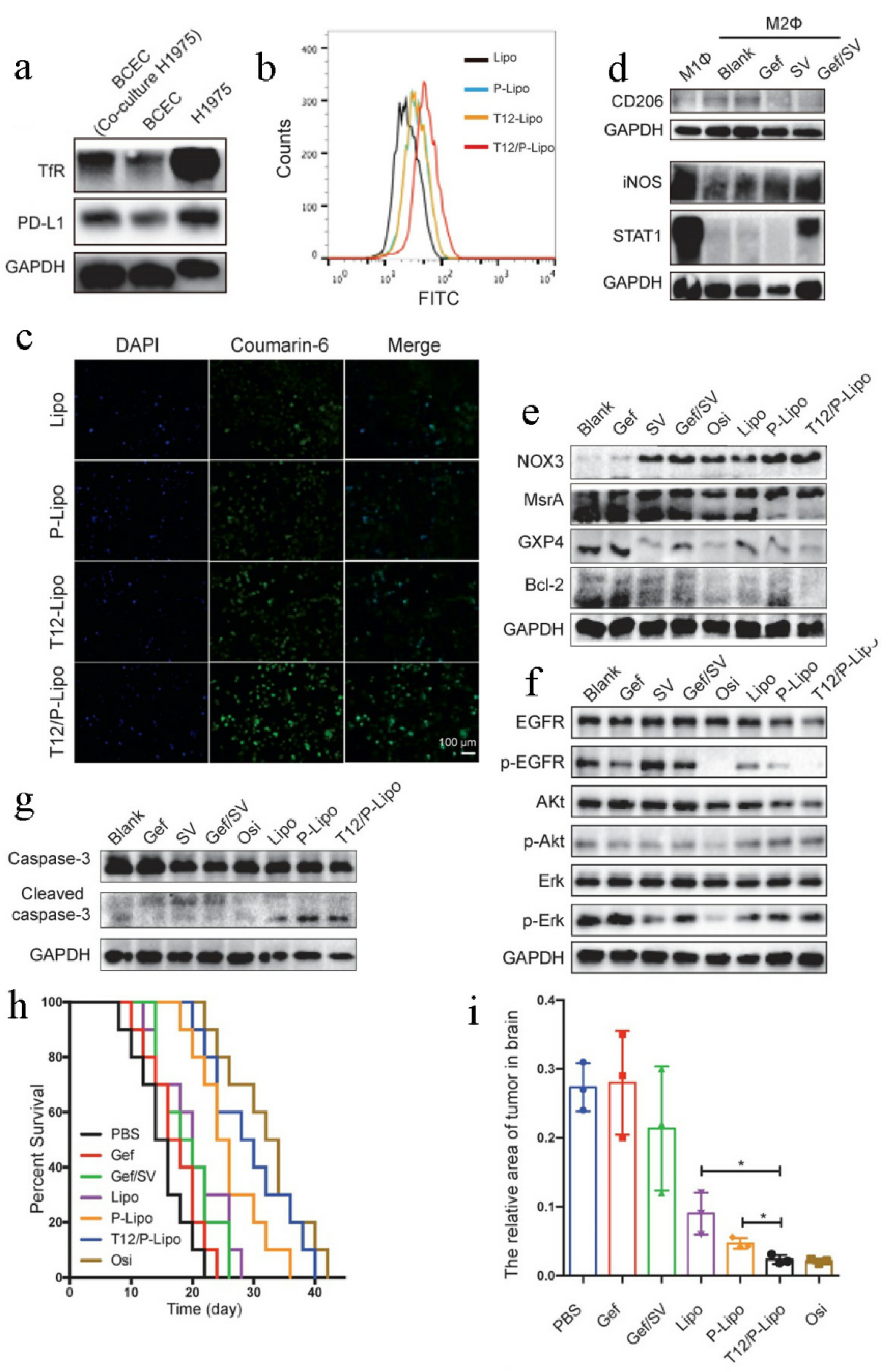
- Yin, W.; Zhao, Y.; Kang, X.; Zhao, P.; Fu, X.; Mo, X.; Wang, Y.; Huang, Y. BBB-penetrating codelivery liposomes treat brain metastasis of non-small cell lung cancer with EGFRT790M mutation. Theranostics 2020, 10, 6122–6135. [Google Scholar] [CrossRef]
- Han, W.; Shi, L.; Ren, L.; Zhou, L.; Li, T.; Qiao, Y.; Wang, H. A nanomedicine approach enables co-delivery of cyclosporin A and gefitinib to potentiate the therapeutic efficacy in drug-resistant lung cancer. Signal Transduct. Target. Ther. 2018, 3, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, D.; Zhang, F.; Wang, J.; He, H.; Duan, S.; Zhu, R.; Chen, C.; Yin, L.; Chen, Y. Biodegradable nanoparticles mediated co-delivery of erlotinib (ELTN) and fedratinib (FDTN) toward the treatment of ELTN-resistant non-small cell lung cancer (NSCLC) via suppression of the JAK2/STAT3 signaling pathway. Front. Pharmacol. 2018, 9, 1214. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Zhang, H.; Zhang, Y.; Lv, T.; Zhang, L.; Li, Z.; Xie, X.; Li, F.; Chen, H.; Jia, L. Erlotinib-guided self-assembled trifunctional click nanotheranostics for distinguishing druggable mutations and synergistic therapy of nonsmall cell lung cancer. Mol. Pharm. 2018, 15, 5146–5161. [Google Scholar] [CrossRef] [PubMed]
- Yin, W.; Yu, X.; Kang, X.; Zhao, Y.; Zhao, P.; Jin, H.; Fu, X.; Wan, Y.; Peng, C.; Huang, Y. Remodeling tumor-associated macrophages and neovascularization overcomes EGFRT790M-associated drug resistance by PD-L1 nanobody-mediated codelivery. Small 2018, 14, e1802372. [Google Scholar] [CrossRef]
- Peng, H.; Chen, B.; Huang, W.; Tang, Y.; Jiang, Y.; Zhang, W.; Huang, Y. Reprogramming tumor-associated macrophages to reverse EGFRT790M resistance by dual-targeting codelivery of gefitinib/vorinostat. Nano Lett. 2017, 17, 7684–7690. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Mei, H.; Gao, Y.; Xie, X.; Nie, H.; Li, T.; Zhang, H.; Jia, L. Co-delivery of oxygen and erlotinib by aptamer-modified liposomal complexes to reverse hypoxia-induced drug resistance in lung cancer. Biomaterials 2017, 145, 56–71. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.B.; Kim, H.R.; Ha, S.J. Immune checkpoint inhibitors in 10 Years: Contribution of basic research and clinical application in cancer immunotherapy. Immune Netw. 2022, 22, e2. [Google Scholar] [CrossRef] [PubMed]
- Seidel, J.A.; Otsuka, A.; Kabashima, K. Anti-PD-1 and anti-CTLA-4 therapies in cancer: Mechanisms of action, efficacy, and limitations. Front. Oncol. 2018, 8, 86. [Google Scholar] [CrossRef] [PubMed]
- Pisibon, C.; Ouertani, A.; Bertolotto, C.; Ballotti, R.; Cheli, Y. Immune checkpoints in cancers: From signaling to the clinic. Cancers 2021, 13, 4573. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Man, S.; Sun, R.; Li, Z.; Wu, Y.; Zuo, D. Recent advances and challenges of immune checkpoint inhibitors in immunotherapy of non-small cell lung cancer. Int. Immunopharmacol. 2020, 85, 106613. [Google Scholar] [CrossRef]
- O’Donnell, J.S.; Teng, M.; Smyth, M.J. Cancer immunoediting and resistance to T cell-based immunotherapy. Nat. Rev. Clin. Oncol. 2019, 16, 151–167. [Google Scholar] [CrossRef]
- Haddad, A.F.; Young, J.S.; Gill, S.; Aghi, M.K. Resistance to immune checkpoint blockade: Mechanisms, counter-acting approaches, and future directions. Semin Cancer Biol. 2022, in press. [Google Scholar] [CrossRef]
- Kalbasi, A.; Ribas, A. Tumour-intrinsic resistance to immune checkpoint blockade. Nat. Rev. Immunol. 2020, 20, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Gondhowiardjo, S.A.; Handoko; Jayalie, V.F.; Apriantoni, R.; Barata, A.R.; Senoaji, F.; Utami, I.; Maubere, F.; Nuryadi, E.; Giselvania, A. Tackling resistance to cancer immunotherapy: What do we know? Molecules 2020, 25, 4096. [Google Scholar] [CrossRef] [PubMed]
- Fares, C.M.; Van Allen, E.M.; Drake, C.G.; Allison, J.P.; Hu-Lieskovan, S. Mechanisms of resistance to immune checkpoint blockade: Why does checkpoint inhibitor immunotherapy not work for all patients? Am. Soc. Clin. Oncol. Educ. Book 2019, 39, 147–164. [Google Scholar] [CrossRef]
- Dianat-Moghadam, H.; Mahari, A.; Salahlou, R.; Khalili, M.; Azizi, M.; Sadeghzadeh, H. Immune evader cancer stem cells direct the perspective approaches to cancer immunotherapy. Stem Cell Res. Ther. 2022, 13, 150. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Jia, Y.; Yu, Y.; Zhang, B.; Xu, F.; Guo, H. Targeting the tumor biophysical microenvironment to reduce resistance to immunotherapy. Adv. Drug Deliv. Rev. 2022, 186, 114319. [Google Scholar] [CrossRef] [PubMed]
- Gide, T.N.; Wilmott, J.S.; Scolyer, R.A.; Long, G.V. Primary and acquired resistance to immune checkpoint inhibitors in metastatic melanoma. Clin. Cancer Res. 2018, 24, 1260–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Draghi, A.; Chamberlain, C.A.; Furness, A.; Donia, M. Acquired resistance to cancer immunotherapy. Semin. Immunopathol. 2019, 41, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Saleh, R.; Elkord, E. Treg-mediated acquired resistance to immune checkpoint inhibitors. Cancer Lett. 2019, 457, 168–179. [Google Scholar] [CrossRef] [PubMed]
- Crispen, P.L.; Kusmartsev, S. Mechanisms of immune evasion in bladder cancer. Cancer Immunol. Immunother. 2020, 69, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Saleh, R.; Elkord, E. Acquired resistance to cancer immunotherapy: Role of tumor-mediated immunosuppression. Semin. Cancer Biol. 2020, 65, 13–27. [Google Scholar] [CrossRef]
- Aspeslagh, S.; Chabanon, R.M.; Champiat, S.; Postel-Vinay, S. Understanding genetic determinants of resistance to immune checkpoint blockers. Semin. Cancer Biol. 2020, 65, 123–139. [Google Scholar] [CrossRef]
- Peng, W.; Chen, J.Q.; Liu, C.; Malu, S.; Creasy, C.; Tetzlaff, M.T.; Xu, C.; McKenzie, J.A.; Zhang, C.; Liang, X.; et al. Loss of PTEN promotes resistance to T cell-mediated immunotherapy. Cancer Discov. 2016, 6, 202–216. [Google Scholar] [CrossRef] [Green Version]
- Cretella, D.; Digiacomo, G.; Giovannetti, E.; Cavazzoni, A. PTEN alterations as a potential mechanism for tumor cell escape from PD-1/PD-L1 inhibition. Cancers 2019, 11, 1318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cetintas, V.B.; Batada, N.N. Is there a causal link between PTEN deficient tumors and immunosuppressive tumor microenvironment? J. Transl. Med. 2020, 18, 45. [Google Scholar] [CrossRef] [Green Version]
- Feng, S.; Cheng, X.; Zhang, L.; Lu, X.; Chaudhary, S.; Teng, R.; Frederickson, C.; Champion, M.M.; Zhao, R.; Cheng, L.; et al. Myeloid-derived suppressor cells inhibit T cell activation through nitrating LCK in mouse cancers. Proc. Natl. Acad. Sci. USA 2018, 115, 10094–10099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, M.D.; Shinde, R.; McGaha, T.L.; Huang, L.; Holmgaard, R.B.; Wolchok, J.D.; Mautino, M.R.; Celis, E.; Sharpe, A.H.; Francisco, L.M.; et al. The PTEN pathway in Tregs is a critical driver of the suppressive tumor microenvironment. Sci. Adv. 2015, 1, e1500845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piro, G.; Carbone, C.; Carbognin, L.; Pilotto, S.; Ciccarese, C.; Iacovelli, R.; Milella, M.; Bria, E.; Tortora, G. Revising PTEN in the era of immunotherapy: New perspectives for an old story. Cancers 2019, 11, 1525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vidotto, T.; Melo, C.M.; Castelli, E.; Koti, M.; Dos Reis, R.B.; Squire, J.A. Emerging role of PTEN loss in evasion of the immune response to tumours. Br. J. Cancer. 2020, 122, 1732–1743. [Google Scholar] [CrossRef]
- Conciatori, F.; Bazzichetto, C.; Falcone, I.; Ciuffreda, L.; Ferretti, G.; Vari, S.; Ferraresi, V.; Cognetti, F.; Milella, M. PTEN function at the interface between cancer and tumor microenvironment: Implications for response to immunotherapy. Int. J. Mol. Sci. 2020, 21, 5337. [Google Scholar] [CrossRef]
- Arico, S.; Petiot, A.; Bauvy, C.; Dubbelhuis, P.F.; Meijer, A.J.; Codogno, P.; Ogier-Denis, E. The tumor suppressor PTEN positively regulates macroautophagy by inhibiting the phosphatidylinositol 3-kinase/protein kinase B pathway. J. Biol. Chem. 2001, 276, 35243–35246. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.X.; Wang, Y.; Ding, J.; Jiang, A.; Wang, J.; Yu, M.; Blake, S.; Liu, S.; Bieberich, C.J.; Farokhzad, O.C.; et al. Reactivation of the tumor suppressor PTEN by mRNA nanoparticles enhances antitumor immunity in preclinical models. Sci. Transl. Med. 2021, 13, eaba9772. [Google Scholar] [CrossRef]
- Qu, F.; Geng, R.; Liu, Y.; Zhu, J. Advanced nanocarrier- and microneedle-based transdermal drug delivery strategies for skin diseases treatment. Theranostics 2022, 12, 3372–3406. [Google Scholar] [CrossRef]
- Alimardani, V.; Abolmaali, S.S.; Tamaddon, A.M.; Ashfaq, M. Recent advances on microneedle arrays-mediated technology in cancer diagnosis and therapy. Drug Deliv. Transl. Res. 2021, 11, 788–816. [Google Scholar] [CrossRef]
- Lee, S.J.; Lee, H.S.; Hwang, Y.H.; Kim, J.J.; Kang, K.Y.; Kim, S.J.; Kim, H.K.; Kim, J.D.; Jeong, D.H.; Paik, M.J.; et al. Enhanced anti-tumor immunotherapy by dissolving microneedle patch loaded ovalbumin. PLoS ONE 2019, 14, e0220382. [Google Scholar] [CrossRef] [Green Version]
- Li, D.; Hu, D.; Xu, H.; Patra, H.K.; Liu, X.; Zhou, Z.; Tang, J.; Slater, N.; Shen, Y. Progress and perspective of microneedle system for anti-cancer drug delivery. Biomaterials 2021, 264, 120410. [Google Scholar] [CrossRef]
- Kulkarni, D.; Damiri, F.; Rojekar, S.; Zehravi, M.; Ramproshad, S.; Dhoke, D.; Musale, S.; Mulani, A.A.; Modak, P.; Paradhi, R.; et al. Recent advancements in microneedle technology for multifaceted biomedical applications. Pharmaceutics 2022, 14, 1097. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Ye, Y.; Hochu, G.M.; Sadeghifar, H.; Gu, Z. Enhanced cancer immunotherapy by microneedle patch-assisted delivery of anti-PD1 antibody. Nano Lett. 2016, 16, 2334–2340. [Google Scholar] [CrossRef] [PubMed]
- Ye, Y.; Wang, J.; Hu, Q.; Hochu, G.M.; Xin, H.; Wang, C.; Gu, Z. Synergistic transcutaneous immunotherapy enhances antitumor immune responses through delivery of checkpoint inhibitors. ACS Nano 2016, 10, 8956–8963. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Lu, C.; Qin, W.; Chen, M.; Quan, G.; Liu, H.; Wang, L.; Bai, X.; Pan, X.; Wu, C. Construction of a core-shell microneedle system to achieve targeted co-delivery of checkpoint inhibitors for melanoma immunotherapy. Acta Biomater. 2020, 104, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Kanugo, A. Recent advances of nanotechnology in the treatment of skin cancer. Curr. Pharm. Biotechnol. 2022. [Google Scholar] [CrossRef]
- Lan, X.; Zhu, W.; Huang, X.; Yu, Y.; Xiao, H.; Jin, L.; Pu, J.J.; Xie, X.; She, J.; Lui, V.W.Y.; et al. Microneedles loaded with anti-PD-1-cisplatin nanoparticles for synergistic cancer immuno-chemotherapy. Nanoscale 2020, 12, 18885–18898. [Google Scholar] [CrossRef]
- Cifaldi, L.; Di Santo, J.; Olive, D. Editorial: Molecular strategies aimed to boost NK cell-based immunotherapy of cancer. Front. Immunol. 2020, 11, 1132. [Google Scholar] [CrossRef]
- Tarannum, M.; Romee, R.; Shapiro, R.M. Innovative strategies to improve the clinical application of NK cell-based immunotherapy. Front. Immunol. 2022, 13, 859177. [Google Scholar] [CrossRef]
- Guillerey, C.; Huntington, N.D.; Smyth, M.J. Targeting natural killer cells in cancer immunotherapy. Nat. Immunol. 2016, 17, 1025–1036. [Google Scholar] [CrossRef] [PubMed]
- Mikelez-Alonso, I.; Magadán, S.; González-Fernández, Á.; Borrego, F. Natural killer (NK) cell-based immunotherapies and the many faces of NK cell memory: A look into how nanoparticles enhance NK cell activity. Adv. Drug Deliv. Rev. 2021, 176, 113860. [Google Scholar] [CrossRef] [PubMed]
- Otegbeye, F.; Ojo, E.; Moreton, S.; Mackowski, N.; Lee, D.A.; de Lima, M.; Wald, D.N. Inhibiting TGF-beta signaling preserves the function of highly activated, in vitro expanded natural killer cells in AML and colon cancer models. PLoS ONE 2018, 13, e0191358. [Google Scholar] [CrossRef] [Green Version]
- Regis, S.; Dondero, A.; Caliendo, F.; Bottino, C.; Castriconi, R. NK cell function regulation by TGF-β-induced epigenetic mechanisms. Front. Immunol. 2020, 11, 311. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.H.; Liao, Y.J.; Chiou, T.J.; Huang, H.T.; Lin, Y.H.; Twu, Y.C. TGF-β regulated leukemia cell susceptibility against NK targeting through the down-regulation of the CD48 expression. Immunobiology 2019, 224, 649–658. [Google Scholar] [CrossRef]
- Shi, L.; Lin, H.; Li, G.; Sun, Y.; Shen, J.; Xu, J.; Lin, C.; Yeh, S.; Cai, X.; Chang, C. Cisplatin enhances NK cells immunotherapy efficacy to suppress HCC progression via altering the androgen receptor (AR)-ULBP2 signals. Cancer Lett. 2016, 373, 45–56. [Google Scholar] [CrossRef] [Green Version]
- Yoo, J.Y.; Jaime-Ramirez, A.C.; Bolyard, C.; Dai, H.; Nallanagulagari, T.; Wojton, J.; Hurwitz, B.S.; Relation, T.; Lee, T.J.; Lotze, M.T.; et al. Bortezomib treatment sensitizes oncolytic HSV-1-treated tumors to NK cell immunotherapy. Clin. Cancer Res. 2016, 22, 5265–5276. [Google Scholar] [CrossRef] [Green Version]
- Padrón, L.J.; Maurer, D.M.; O’Hara, M.H.; O’Reilly, E.M.; Wolff, R.A.; Wainberg, Z.A.; Ko, A.H.; Fisher, G.; Rahma, O.; Lyman, J.P.; et al. Sotigalimab and/or nivolumab with chemotherapy in first-line metastatic pancreatic cancer: Clinical and immunologic analyses from the randomized phase 2 PRINCE trial. Nat. Med. 2022, 28, 1167–1177. [Google Scholar] [CrossRef] [PubMed]
- Avery, J.C.; Hoffmann, P.R. Selenium, selenoproteins, and immunity. Nutrients 2018, 10, 1203. [Google Scholar] [CrossRef] [Green Version]
- Lai, H.; Zeng, D.; Liu, C.; Zhang, Q.; Wang, X.; Chen, T. Selenium-containing ruthenium complex synergizes with natural killer cells to enhance immunotherapy against prostate cancer via activating TRAIL/FasL signaling. Biomaterials 2019, 219, 119377. [Google Scholar] [CrossRef]
- Liu, C.; Lai, H.; Chen, T. Boosting natural killer cell-based cancer immunotherapy with selenocystine/transforming growth factor-beta inhibitor-encapsulated nanoemulsion. ACS Nano 2020, 14, 11067–11082. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Petit, P.F.; Van den Eynde, B.J. Apoptosis of tumor-infiltrating T lymphocytes: A new immune checkpoint mechanism. Cancer Immunol. Immunother. 2019, 68, 835–847. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, Y.; Mittra, A.; Naqash, A.R.; Takebe, N. A review of mechanisms of resistance to immune checkpoint inhibitors and potential strategies for therapy. Cancer Drug Resist. 2020, 3, 252–275. [Google Scholar] [CrossRef] [PubMed]
- Haibe, Y.; El Husseini, Z.; El Sayed, R.; Shamseddine, A. Resisting resistance to immune checkpoint therapy: A systematic review. Int. J. Mol. Sci. 2020, 21, 6176. [Google Scholar] [CrossRef]
- Patel, S.A.; Minn, A.J. Combination cancer therapy with immune checkpoint blockade: Mechanisms and strategies. Immunity 2018, 48, 417–433. [Google Scholar] [CrossRef] [Green Version]
- Larkin, J.; Hodi, F.S.; Wolchok, J.D. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N. Eng. J. Med. 2015, 373, 1270–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Y.; Stephan, M.T.; Gai, S.A.; Abraham, W.; Shearer, A.; Irvine, D.J. In vivo targeting of adoptively transferred T-cells with antibody- and cytokine-conjugated liposomes. J. Control Release 2013, 172, 426–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, D.; Park, C.G.; Hartl, C.A.; Subedi, N.; Cartwright, A.N.; Puerto, R.B.; Zheng, Y.; Maiarana, J.; Freeman, G.J.; Wucherpfennig, K.W.; et al. T cell-targeting nanoparticles focus delivery of immunotherapy to improve antitumor immunity. Nat. Commun. 2017, 8, 1747. [Google Scholar] [CrossRef]
- Manspeaker, M.P.; Thomas, S.N. Lymphatic immunomodulation using engineered drug delivery systems for cancer immunotherapy. Adv. Drug Deliv. Rev. 2020, 160, 19–35. [Google Scholar] [CrossRef]
- Francis, D.M.; Manspeaker, M.P.; Archer, P.A.; Sestito, L.F.; Heiler, A.J.; Schudel, A.; Thomas, S.N. Drug-eluting immune checkpoint blockade antibody-nanoparticle conjugate enhances locoregional and systemic combination cancer immunotherapy through T lymphocyte targeting. Biomaterials 2021, 279, 121184. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Wang, W.; Wu, F.; Zheng, T.; Ashley, J.; Mohammadniaei, M.; Zhang, Q.; Wang, M.; Li, L.; Shen, J.; et al. Biodegradable poly(γ-glutamic acid)@glucose oxidase@carbon dot nanoparticles for simultaneous multimodal imaging and synergetic cancer therapy. Biomaterials 2020, 252, 120106. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Xu, Y.; Ji, W.; Zhou, S.; Li, L.; Qiu, L.; Qian, Z.; Wang, X.; Zhang, H. Biomimetic black phosphorus quantum dots-based photothermal therapy combined with anti-PD-L1 treatment inhibits recurrence and metastasis in triple-negative breast cancer. J. Nanobiotechnology 2021, 19, 181. [Google Scholar] [CrossRef]
- Zhao, P.; Xu, Y.; Ji, W.; Li, L.; Qiu, L.; Zhou, S.; Qian, Z.; Zhang, H. Hybrid membrane nanovaccines combined with immune checkpoint blockade to enhance cancer immunotherapy. Int. J. Nanomed. 2022, 17, 73–89. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Xu, L.; Xu, J.; Zhang, R.; Song, G.; Chao, Y.; Feng, L.; Han, F.; Dong, Z.; Li, B.; et al. Smart nanoreactors for pH-responsive tumor homing, mitochondria-targeting, and enhanced photodynamic-immunotherapy of cancer. Nano Lett. 2018, 18, 2475–2484. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Xu, J.; Liang, C.; Chao, Y.; Jin, Q.; Wang, C.; Chen, M.; Liu, Z. Self-supplied tumor oxygenation through separated liposomal delivery of H2O2 and catalase for enhanced radio-immunotherapy of cancer. Nano Lett. 2018, 18, 6360–6368. [Google Scholar] [CrossRef]
- Chung, C.K.; Fransen, M.F.; van der Maaden, K.; Campos, Y.; García-Couce, J.; Kralisch, D.; Chan, A.; Ossendorp, F.; Cruz, L.J. Thermosensitive hydrogels as sustained drug delivery system for CTLA-4 checkpoint blocking antibodies. J. Control. Release 2020, 323, 1–11. [Google Scholar] [CrossRef]
- Ruan, H.; Hu, Q.; Wen, D.; Chen, Q.; Chen, G.; Lu, Y.; Wang, J.; Cheng, H.; Lu, W.; Gu, Z. A dual-bioresponsive drug-delivery depot for combination of epigenetic modulation and immune checkpoint blockade. Adv. Mater. 2019, 31, e1806957. [Google Scholar] [CrossRef]
- Wang, C.; Wang, J.; Zhang, X.; Yu, S.; Wen, D.; Hu, Q.; Ye, Y.; Bomba, H.; Hu, X.; Liu, Z.; et al. In situ formed reactive oxygen species-responsive scaffold with gemcitabine and checkpoint inhibitor for combination therapy. Sci. Transl. Med. 2018, 10, eaan3682. [Google Scholar] [CrossRef] [Green Version]
- Longmire, M.; Choyke, P.L.; Kobayashi, H. Clearance properties of nano-sized particles and molecules as imaging agents: Considerations and caveats. Nanomedicine 2008, 3, 703–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, K.C.; Wang, Y.; Luehmann, H.P.; Cai, X.; Xing, W.; Pang, B.; Zhao, Y.; Cutler, C.S.; Wang, L.V.; Liu, Y.; et al. Radioactive 198Au-doped nanostructures with different shapes for in vivo analyses of their biodistribution, tumor uptake, and intratumoral distribution. ACS Nano 2014, 8, 4385–4394. [Google Scholar] [CrossRef]
- Decuzzi, P.; Pasqualini, R.; Arap, W.; Ferrari, M. Intravascular delivery of particulate systems: Does geometry really matter? Pharm. Res. 2009, 26, 235–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, K.; Li, Y.; Luo, J.; Lee, J.S.; Xiao, W.; Gonik, A.M.; Agarwal, R.G.; Lam, K.S. The effect of surface charge on in vivo biodistribution of PEG-oligocholic acid based micellar nanoparticles. Biomaterials 2011, 32, 3435–3446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanco, E.; Shen, H.; Ferrari, M. Principles of nanoparticle design for overcoming biological barriers to drug delivery. Nat. Biotechnol. 2015, 33, 941–951. [Google Scholar] [CrossRef] [PubMed]
- Nehoff, H.; Parayath, N.N.; Domanovitch, L.; Taurin, S.; Greish, K. Nanomedicine for drug targeting: Strategies beyond the enhanced permeability and retention effect. Int. J. Nanomed. 2014, 9, 2539–2555. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, P.V.; Hervé-Aubert, K.; Chourpa, I.; Allard-Vannier, E. Active targeting strategy in nanomedicines using anti-EGFR ligands-A promising approach for cancer therapy and diagnosis. Int. J. Pharm. 2021, 609, 121134. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Zhou, Z.; Qiu, N.; Shen, Y. Rational design of cancer nanomedicine: Nanoproperty integration and synchronization. Adv. Mater. 2017, 29, 1606628. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.; Park, C.; Yi, G.; Lee, D.; Koo, H. Active targeting strategies using biological ligands for nanoparticle drug delivery systems. Cancers 2019, 11, 640. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trade Name | Active Ingredient | Nanoformulation | Indications | Approval Date | Clinical Effect | Reference |
|---|---|---|---|---|---|---|
| Doxil® | Doxorubicin | Liposome | Ovarian and breast cancer | 1995 | Fewer and less severe side effects Longer periods of drug circulation in vivo Prolonged interval to progression and progression-free survival time | [32] |
| DaunoXome® | Daunorubicin | Liposome | HIV-related Kaposi’s Sarcoma | 1996 | No obvious cardiotoxicity Longer periods of drug circulation in vivo As effective as the conventional chemotherapy | [33] |
| DepoCyt® | Cytarabine | Liposome | Lymphomatous meningitis | 1999 | Reduced cardiotoxicity Pronounced effectiveness | [34] |
| Eligard® | Leuprolide | Nanosphere | Prostate cancer | 2002 | More sustained testosterone suppression Higher response rates | [35] |
| Lipusu® | Paclitaxel | Liposome | Ovarian cancer and breast cancer | 2003 | Reduced adverse reactions As effective as the paclitaxel | [36] |
| Abraxane® | Paclitaxel | Nanoparticle | Metastatic breast cancer | 2005 | Lower overall toxicity Better anticancer effect | [37] |
| Genexol-PM® | Paclitaxel | Micelle | Breast cancer and Lung cancer | 2007 | Reduced toxicities of paclitaxel Enhanced antitumor efficiency | [38] |
| Marqibo® | Vincristine | Liposome | Acute lymphoid leukemia | 2012 | Reduced neurotoxicity Overall increase in therapeutic index | [39] |
| Onivyde® | Irinotecan | Liposome | Metastatic pancreatic cancer | 2015 | Longer half-life Enhanced anticancer efficiency | [40] |
| Liporaxel® | Paclitaxel | Emulsion | Gastric cancer | 2016 | Reduced neurotoxicity As effective as paclitaxel | [41] |
| Vyxeos® | Daunorubicin and cytarabine | Liposome | Acute myeloid leukemia | 2017 | Prolonged overall survival (OS) and event-free survival (EFS) | [42] |
| Nanoformulation | Name | Particle Size | Payload | Reversal Mechanism of Drug Resistance | Cell Line | Tumor Model | Reference |
|---|---|---|---|---|---|---|---|
| Polymeric micelles | ACP-Dox and Apa micelles | 104 ± 2 nm | DOX and apatinib | Inhibit P-gp activity | MCF-7/ADR cells | MCF-7/ADR tumor-bearing mice | [127] |
| HA-PLGA (PTX and FAK siRNA)-NPs | 232.9 ± 6.9 nm | PTX and FAK siRNA | siRNA-mediated silencing of FAK | HeyA8-MDR and SKOV3-TR cells | Drug-resistant, patient-derived xenograft (PDX) model | [128] | |
| ACP-R837 and PPP-DOX | ~110 nm | R837 and DOX | Synergistic chemo-immunotherapy | 4T1 cells | 4T1 tumor-bearing mice | [129] | |
| NC-DOX | ~122 nm | DOX and IR780 | Combined chemotherapy/PTT/PDT | MCF-7/ADR cells | MCF-7/ADR tumor-bearing mice | [130] | |
| Polymeric nanoparticles | Dox-Cur-NDs | 55.1 ± 3.0 nm | DOX and CUR | Down-regulate the expression of P-gp | A2780 ADR cells | A2780 ADR tumor-bearing mice | [131] |
| [FeFe]TPP/GEM/FCS NPs | 176.0 ± 17.2 nm | Gemcitabine and [FeFe]TPP | Reduce the of function P-gp efflux pump | T24 cells | T24 tumor-bearing mice | [132] | |
| IGU-PLGA-NPs | 199.6 nm | Iguratimod | Facilitate BBB penetration and inhibit GSCs proliferation and stemness | U87 and U251TMZ-R cells | U87 tumor-bearing mice | [133] | |
| Liposomes | rTLM-PEG, PTX liposomes | / | PTX and trichosanthin | Reverse caspase 9 phosphorylation and induce caspase 3-dependent apoptosis | A549/T cells | A549/T tumor-bearing mice | [134] |
| PTX/NO/DMA-L | 146.3 ± 0.82 nm | PTX and DETA NONOate | NO-mediated down-regulation of P-gp | A549/T cells | A549/T tumor-bearing mice | [135] | |
| CBZ liposomes | 108.53 ± 1.5 nm | CBZ | G2/M phase arrest | MCF-7 and MDA-MB-231 cells | Female SD rats | [136] | |
| Lip (Ap-Dox) | 128.6 nm | Ap-Dox complex | Bypass the P-gp-mediated drug efflux | MCF-7/ADR cells | MCF-7/ADR tumor-bearing nude mice | [137] | |
| (DEX and DTX)-Lip | 74.02 ± 0.41 nm | DTX and dexamethasone | Overcome stroma obstacles | Multidrug-resistant KBv cells and 4 T1 cells | Multidrug-resistant KBv and metastatic 4 T1 tumor models | [138] | |
| FPL-DOX/IM | 159 ± 6 nm | DOX and imatinib | Inhibit ABC transporter function | MCF-7/ADR cells | MCF-7/ADR tumor-bearing mice | [139] | |
| PpIX/Dox liposomes | 55.9 ± 20.9 nm | DOX and PpIX | Disrupt the structure of P-gp | MCF-7/ADR cells | MCF-7/ADR tumor-bearing mice | [140] | |
| Nanogels | LNGs-PTX-siRNA | ~100 nm | PTX and MDR1 siRNA | Knockdown MDR1 | DROV cells | DROV tumor-bearing mice | [141] |
| CDDP/DOX-NGs | ~100 nm | CDDP and DOX | Combination chemotherapy | MCF-7/ADR cells | MCF-7/ADR tumor-bearing mice | [142] | |
| HA/Cis/Dox | 45 ± 9.9 nm | DOX | GSH-induced DOX release | A2780cis cells | / | [143] | |
| SiPT75 | 75.5 ± 19.8 nm | TPPS | Elude the drug efflux pumps and retards exocytosis of cells | A549/DDP cells | A549/DDP tumor-bearing mice | [144] | |
| Inorganic nanoparticles | H-MSNs-DOX/siRNA nanoparticles | ~100 nm | P-gp siRNA and DOX | siRNA-mediated silencing of P-gp | MCF-7/ADR cells | MCF-7/ADR tumor-bearing mice | [145] |
| Pt-AuNS | ~85 nm | Pt | GSH depletion and GPX4 inactivation | MCF-7/ADR cells | MCF-7/ADR tumor-bearing mice | [146] | |
| FA-GT-MSNs@TPZ | ~60 nm | TPZ | Synergistic radio-chemo-photothermal therapy | Hypoxic SMMC-7721 cells | SMMC-7721 tumor-bearing mice | [147] | |
| Hybrid nanoparticles | SCA4PNPBTZ | ~150 nm | BTZ and CA4P | Inhibit the overexpression of BCRP/ABCG2 | A549 cells | Human A549 pulmonary adenocarcinoma xenograft model and PDX model of colon cancer | [148] |
| cNPs | 286 ± 79 nm | Afatinib, rapamycin and docetaxel | Synergistic treatment | HER2-positive breast cancer cells, EGFR-positive NSCLC cells and SKBR-3/AR cell lines | HER2-positive breast cancer mouse model | [149] | |
| 4T1-HANG-GNR-DC | 103.1 ± 7.6 nm | CDDP and DOX | Synergistic chemo-photothermal therapy | 4T1 cells | 4T1 tumor-bearing mice | [150] | |
| IR780/DTX-PCEC@RBC | ~150 nm | IR780 and DTX | Combination therapy | MCF-7 cells | MCF-7 tumor-bearing mice | [151] | |
| cNC@PDA-PEG | 170.5 ± 1.4 nm | Paclitaxel/lapatinib | Combination therapy | MCF-7/ADR cells | / | [152] | |
| miR497/TP-HENPs | 125 ± 6 nm | miR497 and triptolide | Synergically suppress mTOR signaling pathway | SKOV3-CDDP cells | SKOV3-CDDP tumor-bearing mice | [153] |
| Nanoformulation | Name | Particle Size | Payload | Reversal Mechanism of Drug Resistance | Cell Line | Tumor Model | Reference |
|---|---|---|---|---|---|---|---|
| Polymeric micelles | CP@NP-cRGD | 123.4 ± 0.4 nm | CQ and PD173074 | Dual FGFR1-autophagy blockade | H1975/AR and HCC827/AR cells | H1975/AR tumor-bearing mice | [188] |
| CsA/Gef-NPs | 37.1 ± 13.1 nm | Cyclosporin A and gefitinib | Cyclosporin A-mediated gefitinib sensitization | PC-9-GR cells | PC-9-GR tumor-bearing mice | [216] | |
| Polymeric nanoparticles | ELTN and FDTN@PEG-PLA | ~120 nm | Fedratinib and Erlotinib | Inhibit the JAK2/STAT3 signaling pathway | Erlotinib-resistant H1650 cells | Erlotinib-resistant H1650 xenograft tumor model | [217] |
| CE7Ns | 234.2 ± 8.5 nm | Cy7 and erlotinib | Synergistic erlotinib-targeted therapy and photodynamic therapy | PC-9 and Erlotinib-resistant H1975 cells | PC-9 tumor-bearing mice | [218] | |
| ERL-loaded CMP-HA-NI-PEI-NBA | 755.77 ± 51.11 nm | Erlotinib | Hypoxia-triggered rapid drug release | Drug-resistant hypoxic HeLa cells | / | [196] | |
| Liposomes | T12/P-Lipo | ~153 nm | Simvastatin and gefitinib | TAM targeting and enhanced BBB penetration | EGFRT790M-mutated H1975 cells | EGFRT790M-mutated H1975 brain metastasis model | [215] |
| P-Lipo | 156 nm | Simvastatin and gefitinib | Neovascularization regulation and M2-macrophage repolarization | EGFRT790M-mutated H1975 cells | EGFRT790M-mutated H1975 tumor-bearing mice | [219] | |
| tLGV | ~180 n | Gefitinib and vorinostat | TAM reprogramming | EGFRT790M-mutated H1975 cells | EGFRT790M-positive H1975 tumor model | [220] | |
| Hybrid nanoparticles | ACLEP | 184.8 ± 5.87 nm | Erlotinib and PFOB | Reverse hypoxia-induced drug resistance | A549 and Erlotinib-resistant H1975 cells | A549 tumor-bearing mice | [221] |
| Nanoformulation | Name | Particle Size | Payload | Reversal Mechanism of Drug Resistance | Cell Line | Tumor Model | Reference |
|---|---|---|---|---|---|---|---|
| Hybrid nanoparticles | mPTEN@NPs | 111.8 ± 15.3 nm | PTEN mRNA | Improve the sensitivity of ICB therapy | B16F10 cells | B16F10 melanoma tumor-bearing mice | [248] |
| PGA@GOx@Mn, Cu-CDs | ~80 nm | Gox and Mn, Cu-CDs | Combined action of starving therapy/PDT/PTT and checkpoint-blockade immunotherapy | 4T1 cells | 4T1 tumor-bearing mice | [281] | |
| BBPQDs | 30 nm | BPQDs | Reprogram the immunosuppressive TME | 4T1 cells | 4T1 tumor-bearing mice | [282] | |
| R837@HM-NPs | 71 ± 4.1 nm | R837 | Reprogram the immunosuppressive TME | 4T1 cells | 4T1 tumor-bearing mice | [283] | |
| CAT@S/Ce6-CTPP/DPEG | ~100 nm | Catalase and Ce6 | Combined action of PDT and immunotherapy | 4T1 cells | 4T1 tumor-bearing mice | [284] | |
| Liposomes | H2O2@Liposome and CAT@Liposome | ~140 nm | H2O2 and Catalase | Radio-immunotherapy | 4T1 cells | 4T1 tumor-bearing mice | [285] |
| Nanoemulsion | SSB NMs | ~130 nm | SeC and TGF-β inhibitor | Improve the sensitivity of cell-based immunotherapy | MDA-MB-231 cells | MDA-MB-231 tumor-bearing mice | [271] |
| Polymeric nanoparticles | ANCs | ~30 nm | ICB mAb and small-molecule immunomodulators | T lymphocyte targeting and combination therapy | B16F10 and 4T1 cells | B16F10 and 4T1 tumor-bearing mice | [280] |
| Nanogels | P407 hydrogel | ~28 nm | Anti-CTLA-4 antibodies | Sustained antibody release | D1DCs and MC-38 cells | CT26 tumor-bearing mice | [286] |
| Zeb-aPD1-NPs-Gel | ~100 nm | Zebularine and anti-PD1 antibody | Controlled drug release and reversal of immunosuppressive TME | B16F10 cells | B16F10 melanoma-bearing mice | [287] | |
| aPDL1-GEM@Gel | / | Gemcitabine and PD-L1 blocking antibody | Combination therapy | B16F10 and 4T1 cells | B16F10 and 4T1 tumor-bearing mice | [288] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, T.; Gong, H.; Xu, J.; Huang, Y.; Wu, F.; He, Z. Nanomedicines for Overcoming Cancer Drug Resistance. Pharmaceutics 2022, 14, 1606. https://doi.org/10.3390/pharmaceutics14081606
Hu T, Gong H, Xu J, Huang Y, Wu F, He Z. Nanomedicines for Overcoming Cancer Drug Resistance. Pharmaceutics. 2022; 14(8):1606. https://doi.org/10.3390/pharmaceutics14081606
Chicago/Turabian StyleHu, Tingting, Hanlin Gong, Jiayue Xu, Yuan Huang, Fengbo Wu, and Zhiyao He. 2022. "Nanomedicines for Overcoming Cancer Drug Resistance" Pharmaceutics 14, no. 8: 1606. https://doi.org/10.3390/pharmaceutics14081606
APA StyleHu, T., Gong, H., Xu, J., Huang, Y., Wu, F., & He, Z. (2022). Nanomedicines for Overcoming Cancer Drug Resistance. Pharmaceutics, 14(8), 1606. https://doi.org/10.3390/pharmaceutics14081606