
The “Light Knife” for Gastric Cancer: Photodynamic Therapy


Abstract
:1. Introduction
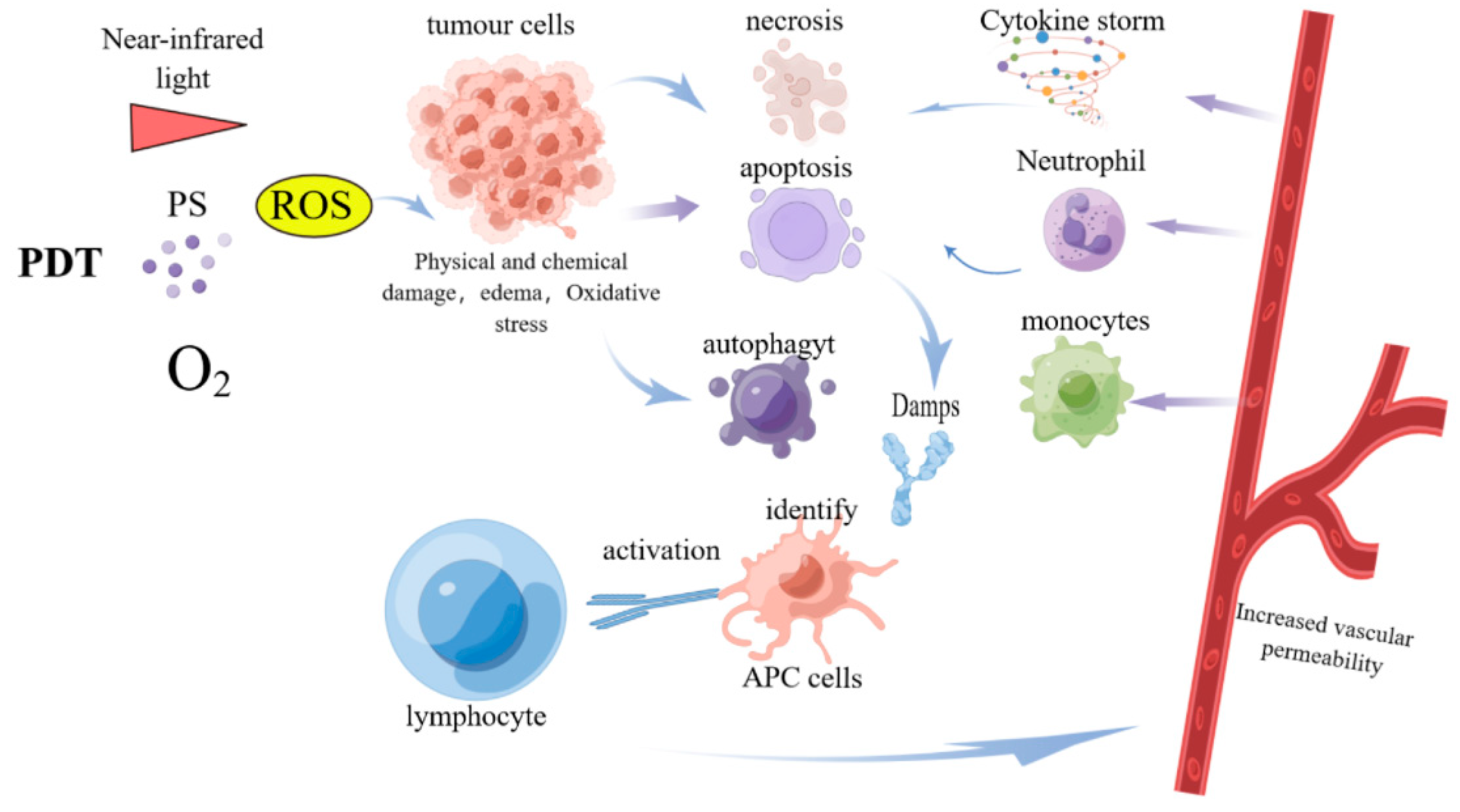
2. New Mechanisms of PDT Anti-Tumor Therapy
3. Application of New PSs in GC
3.1. Comparison of PS in the Treatment of GC
3.2. The Effect of Using New PSs in PDT for GC
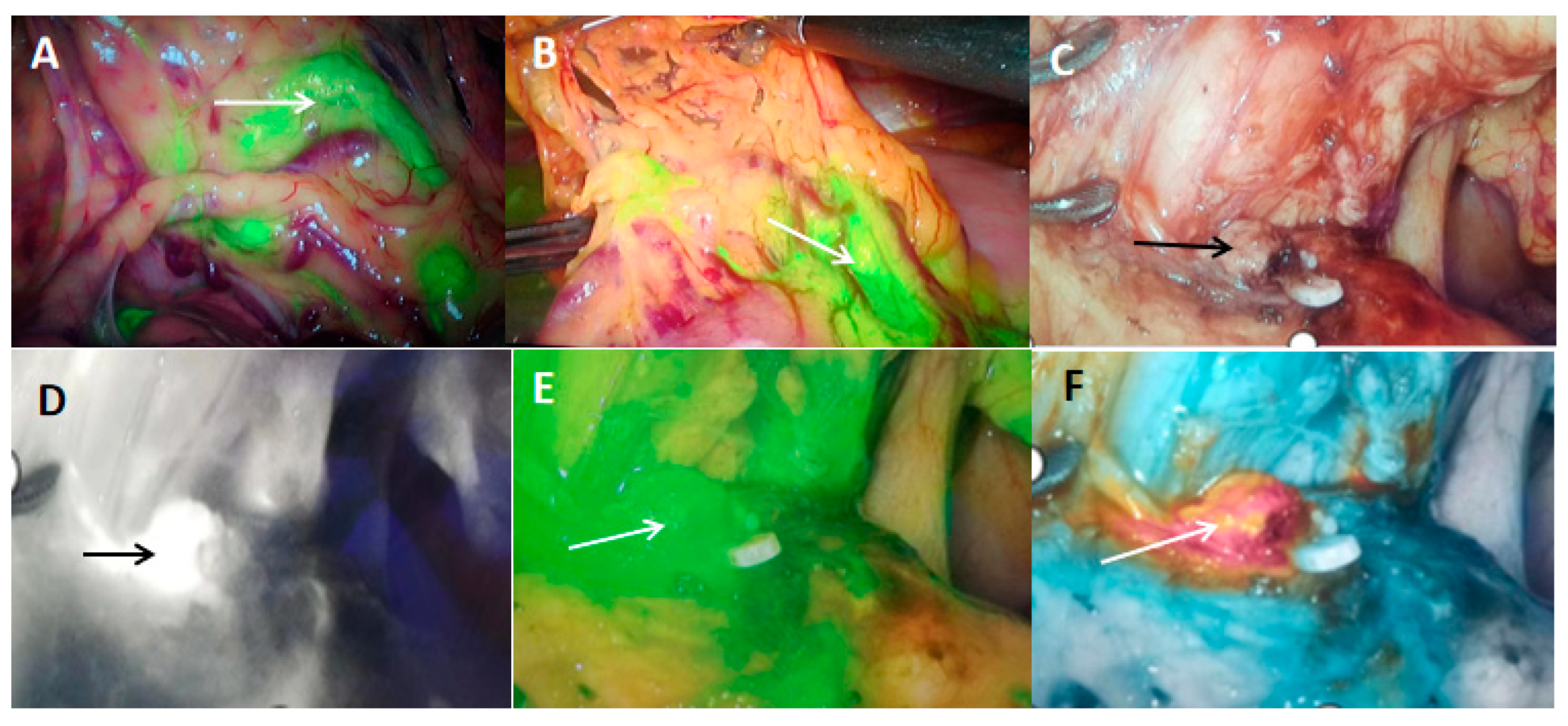
4. Diagnostic Role of Photodynamics in GC
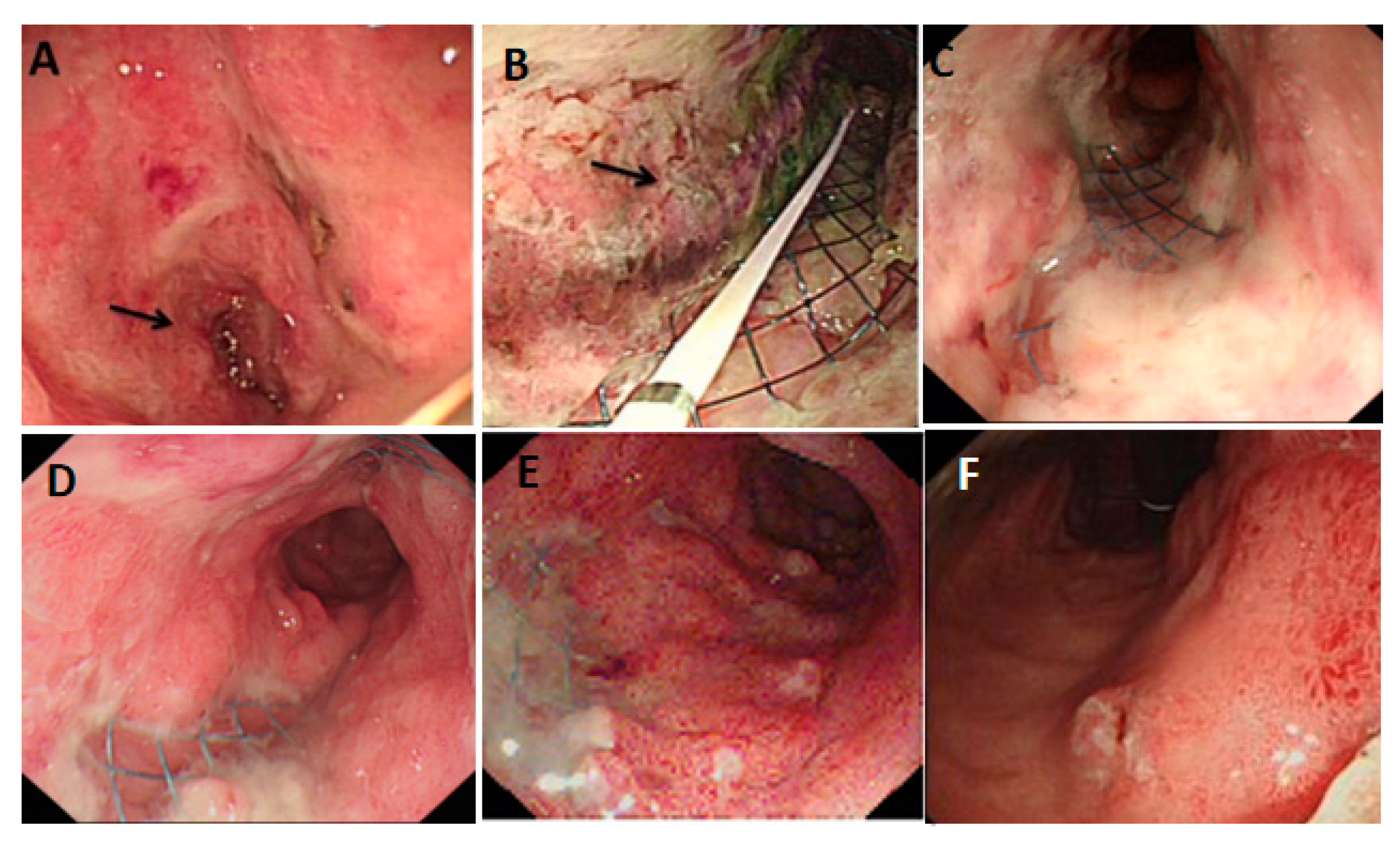
5. Effects of PDT on GC
5.1. PDT for Early Gastric Cancer (EGC)
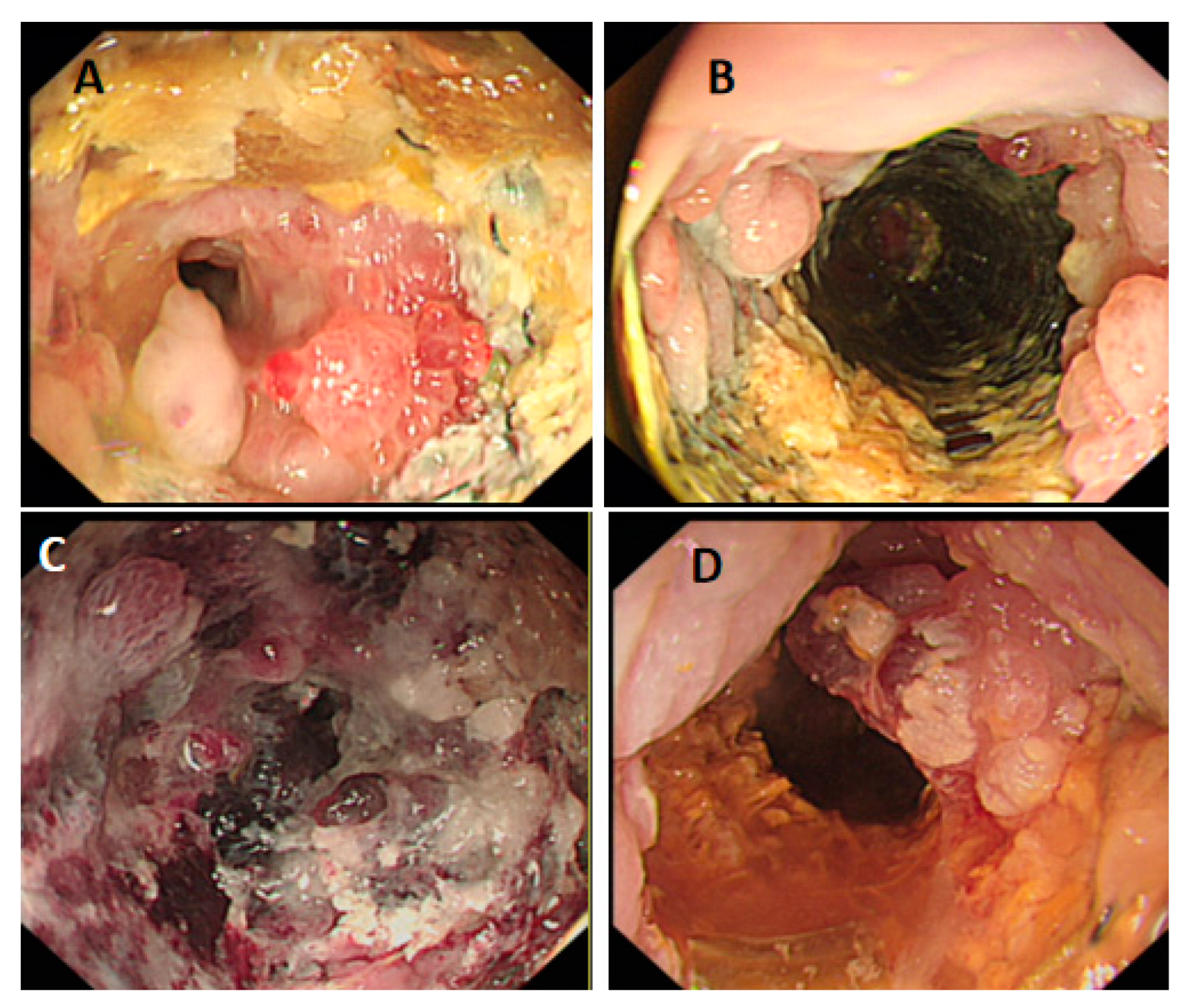
5.2. PDT for the Treatment of Locally Advanced and Peritoneal Metastatic GC
6. Combined Treatment of PDT
6.1. Combined Use of PDT and Chemotherapy Drugs
6.2. Combined Use of PDT and Targeted Drugs
6.3. PDT Combined with Immunotherapy
6.4. Combined Use of PDT and Hyperthermia
7. Conclusions and Outlook
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. International Agency for Research on Cancer. GLOBOCAN 2020: Stomach Cancer Fact Sheet; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Digklia, A.; Wagner, A.D. Advanced gastric cancer: Current treatment landscape and future perspectives. World J. Gastroenterol. 2016, 22, 2403–2414. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef] [PubMed]
- Wilke, H.; Muro, K.; Van Cutsem, E.; Oh, S.C.; Bodoky, G.; Shimada, Y.; Hironaka, S.; Sugimoto, N.; Lipatov, O.; Kim, T.Y.; et al. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): A double-blind, randomised phase 3 trial. Lancet Oncol. 2014, 15, 1224–1235. [Google Scholar] [CrossRef] [PubMed]
- Dank, M.; Zaluski, J.; Barone, C.; Valvere, V.; Yalcin, S.; Peschel, C.; Wenczl, M.; Goker, E.; Cisar, L.; Wang, K.; et al. Randomized phase III study comparing irinotecan combined with 5-fluorouracil and folinic acid to cisplatin combined with 5-fluorouracil in chemotherapy naive patients with advanced adenocarcinoma of the stomach or esophagogastric junction. Ann. Oncol. 2008, 19, 1450–1457. [Google Scholar] [CrossRef] [PubMed]
- Al-Batran, S.E.; Hartmann, J.T.; Probst, S.; Schmalenberg, H.; Hollerbach, S.; Hofheinz, R.; Rethwisch, V.; Seipelt, G.; Homann, N.; Wilhelm, G.; et al. Phase III trial in metastatic gastroesophageal adenocarcinoma with fluorouracil, leucovorin plus either oxaliplatin or cisplatin: A study of the Arbeitsgemeinschaft Internistische Onkologie. J. Clin. Oncol. 2008, 26, 1435–1442. [Google Scholar] [CrossRef]
- Xu, R.H.; Zhang, Y.; Pan, H.; Feng, J.; Zhang, T.; Liu, T.; Qin, Y.; Qin, S.; Yin, X.; Liu, B.; et al. Efficacy and safety of weekly paclitaxel with or without ramucirumab as second-line therapy for the treatment of advanced gastric or gastroesophageal junction adenocarcinoma (RAINBOW-Asia): A randomised, multicentre, double-blind, phase 3 trial. Lancet Gastroenterol. Hepatol. 2021, 6, 1015–1024. [Google Scholar] [CrossRef]
- Bartley, A.N.; Washington, M.K.; Ismaila, N.; Ajani, J.A. HER2 Testing and Clinical Decision Making in Gastroesophageal Adenocarcinoma: Guideline Summary From the College of American Pathologists, American Society for Clinical Pathology, and American Society of Clinical Oncology. J. Oncol. Pract. 2017, 13, 53–57. [Google Scholar] [CrossRef]
- Kono, K.; Nakajima, S.; Mimura, K. Current status of immune checkpoint inhibitors for gastric cancer. Gastric Cancer 2020, 23, 565–578. [Google Scholar] [CrossRef]
- Polónia, A.; Pinto, R.; Cameselle-Teijeiro, J.F.; Schmitt, F.C.; Paredes, J. Prognostic value of stromal tumour infiltrating lymphocytes and programmed cell death-ligand 1 expression in breast cancer. J. Clin. Pathol. 2017, 70, 860–867. [Google Scholar] [CrossRef]
- Kawazoe, A.; Kuwata, T.; Kuboki, Y.; Shitara, K.; Nagatsuma, A.K.; Aizawa, M.; Yoshino, T.; Doi, T.; Ohtsu, A.; Ochiai, A. Clinicopathological features of programmed death ligand 1 expression with tumor-infiltrating lymphocyte, mismatch repair, and Epstein-Barr virus status in a large cohort of gastric cancer patients. Gastric Cancer 2017, 20, 407–415. [Google Scholar] [CrossRef]
- Shitara, K.; Van Cutsem, E.; Bang, Y.J.; Fuchs, C.; Wyrwicz, L.; Lee, K.W.; Kudaba, I.; Garrido, M.; Chung, H.C.; Lee, J.; et al. Efficacy and Safety of Pembrolizumab or Pembrolizumab Plus Chemotherapy vs Chemotherapy Alone for Patients with First-line, Advanced Gastric Cancer: The KEYNOTE-062 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1571–1580. [Google Scholar] [CrossRef]
- Davar, D.; Dzutsev, A.K.; McCulloch, J.A.; Rodrigues, R.R.; Chauvin, J.M.; Morrison, R.M.; Deblasio, R.N.; Menna, C.; Ding, Q.; Pagliano, O.; et al. Fecal microbiota transplant overcomes resistance to anti-PD-1 therapy in melanoma patients. Science 2021, 371, 595–602. [Google Scholar] [CrossRef]
- Zhao, S.; Ren, S.; Jiang, T.; Zhu, B.; Li, X.; Zhao, C.; Jia, Y.; Shi, J.; Zhang, L.; Liu, X.; et al. Low-Dose Apatinib Optimizes Tumor Microenvironment and Potentiates Antitumor Effect of PD-1/PD-L1 Blockade in Lung Cancer. Cancer Immunol. Res. 2019, 7, 630–643. [Google Scholar] [CrossRef]
- Lee, C.H.; Shah, A.Y.; Rasco, D.; Rao, A.; Taylor, M.H.; Di Simone, C.; Hsieh, J.J.; Pinto, A.; Shaffer, D.R.; Girones Sarrio, R.; et al. Lenvatinib plus pembrolizumab in patients with either treatment-naive or previously treated metastatic renal cell carcinoma (Study 111/KEYNOTE-146): A phase 1b/2 study. Lancet Oncol. 2021, 22, 946–958. [Google Scholar] [CrossRef]
- Wang, C.; Liu, Y.; Dong, L.; Li, X.; Yang, Q.; Brock, M.V.; Mei, Q.; Liu, J.; Chen, M.; Shi, F.; et al. Efficacy of Decitabine plus Anti-PD-1 Camrelizumab in Patients with Hodgkin Lymphoma Who Progressed or Relapsed after PD-1 Blockade Monotherapy. Clin. Cancer Res. 2021, 27, 2782–2791. [Google Scholar] [CrossRef]
- González, C.A.; Megraud, F.; Buissonniere, A.; Lujan Barroso, L.; Agudo, A.; Duell, E.J.; Boutron-Ruault, M.C.; Clavel-Chapelon, F.; Palli, D.; Krogh, V.; et al. Helicobacter pylori infection assessed by ELISA and by immunoblot and noncardia gastric cancer risk in a prospective study: The Eurgast-EPIC project. Ann. Oncol. 2012, 23, 1320–1324. [Google Scholar] [CrossRef]
- Plummer, M.; Franceschi, S.; Vignat, J.; Forman, D.; de Martel, C. Global burden of gastric cancer attributable to Helicobacter pylori. Int J. Cancer 2015, 136, 487–490. [Google Scholar] [CrossRef]
- Li, W.Q.; Zhang, J.Y.; Ma, J.L.; Li, Z.X.; Zhang, L.; Zhang, Y.; Guo, Y.; Zhou, T.; Li, J.Y.; Shen, L.; et al. Effects of Helicobacter pylori treatment and vitamin and garlic supplementation on gastric cancer incidence and mortality: Follow-up of a randomized intervention trial. BMJ 2019, 366, l5016. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Ma, R.; Yan, L.; Chen, X.; Zhu, G. Combined chemotherapy and photodynamic therapy using a nanohybrid based on layered double hydroxides to conquer cisplatin resistance. Chem. Commun. (Camb.) 2015, 51, 11587–11590. [Google Scholar] [CrossRef]
- He, C.; Liu, D.; Lin, W. Self-assembled core-shell nanoparticles for combined chemotherapy and photodynamic therapy of resistant head and neck cancers. ACS Nano 2015, 9, 991–1003. [Google Scholar] [CrossRef]
- Korbelik, M. PDT-associated host response and its role in the therapy outcome. Lasers Surg. Med. 2006, 38, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Alzeibak, R.; Mishchenko, T.A.; Shilyagina, N.Y.; Balalaeva, I.V.; Vedunova, M.V.; Krysko, D.V. Targeting immunogenic cancer cell death by photodynamic therapy: Past, present and future. J. Immunother. Cancer 2021, 9, e001926. [Google Scholar] [CrossRef] [PubMed]
- Castano, A.P.; Mroz, P.; Hamblin, M.R. Photodynamic therapy and anti-tumour immunity. Nat. Rev. Cancer 2006, 6, 535–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, C.W.; Li, J.; Pu, K. Recent Progresses in Phototherapy-Synergized Cancer Immunotherapy. Adv. Funct. Mater. 2018, 28, 1804688. [Google Scholar] [CrossRef]
- Lucky, S.S.; Idris, N.M.; Huang, K.; Kim, J.; Li, Z.; Thong, P.S.; Xu, R.; Soo, K.C.; Zhang, Y. In vivo Biocompatibility, Biodistribution and Therapeutic Efficiency of Titania Coated Upconversion Nanoparticles for Photodynamic Therapy of Solid Oral Cancers. Theranostics 2016, 6, 1844–1865. [Google Scholar] [CrossRef]
- Zhao, C.Y.; Cheng, R.; Yang, Z.; Tian, Z.M. Nanotechnology for Cancer Therapy Based on Chemotherapy. Molecules 2018, 23, 826. [Google Scholar] [CrossRef] [Green Version]
- Im, B.N.; Shin, H.; Lim, B.; Lee, J.; Kim, K.S.; Park, J.M.; Na, K. Helicobacter pylori-targeting multiligand photosensitizer for effective antibacterial endoscopic photodynamic therapy. Biomaterials 2021, 271, 120745. [Google Scholar] [CrossRef]
- Lee, D.J.; Juvekar, V.; Lee, H.W.; Kim, E.S.; Noh, C.K.; Shin, S.J.; Kim, H.M. Cancer-Targeted Azo Dye for Two-Photon Photodynamic Therapy in Human Colon Tissue. Anal. Chem. 2021, 93, 16821–16827. [Google Scholar] [CrossRef]
- Kwiatkowski, S.; Knap, B.; Przystupski, D.; Saczko, J.; Kędzierska, E.; Knap-Czop, K.; Kotlińska, J.; Michel, O.; Kotowski, K.; Kulbacka, J. Photodynamic therapy–mechanisms, photosensitizers and combinations. Biomed. Pharmacother. 2018, 106, 1098–1107. [Google Scholar] [CrossRef]
- Dysart, J.S.; Patterson, M.S. Characterization of Photofrin photobleaching for singlet oxygen dose estimation during photodynamic therapy of MLL cells in vitro. Phys. Med. Biol. 2005, 50, 2597–2616. [Google Scholar] [CrossRef]
- Moan, J.; Berg, K.; Kvam, E.; Western, A.; Malik, Z.; Ruck, A.; Schneckenburger, H. Intracellular localization of photosensitizers. Ciba Found. Symp. 1989, 146, 95–107; discussion 107–111. [Google Scholar]
- Luo, Y.; Kessel, D. Initiation of apoptosis versus necrosis by photodynamic therapy with chloroaluminum phthalocyanine. Photochem. Photobiol. 1997, 66, 479–483. [Google Scholar] [CrossRef]
- Kessel, D.; Castelli, M.; Reiners, J.J. Ruthenium red-mediated suppression of Bcl-2 loss and Ca(2+) release initiated by photodamage to the endoplasmic reticulum: Scavenging of reactive oxygen species. Cell Death Differ. 2005, 12, 502–511. [Google Scholar] [CrossRef]
- Weyergang, A.; Berg, K.; Kaalhus, O.; Peng, Q.; Selbo, P.K. Photodynamic therapy targets the mTOR signaling network in vitro and in vivo. Mol. Pharm. 2009, 6, 255–264. [Google Scholar] [CrossRef]
- Inguscio, V.; Panzarini, E.; Dini, L. Autophagy Contributes to the Death/Survival Balance in Cancer PhotoDynamic Therapy. Cells 2012, 1, 464–491. [Google Scholar] [CrossRef]
- Tan, Y.K.; Liu, K.J.; Zou, H.; Yao, H.L.; Jin, J.Y.; Zhang, C.Y.; Li, Q.Z.; Xiong, L.; Lei, S.L.; Chen, W. Inhibitory Effect and Molecular Mechanism of the New Phorphyrin-Based HCE6 Photosensitizer on the Activity of MKN45 Human Gastric Cancer Cells. J. Biomed. Nanotechnol. 2019, 15, 1345–1353. [Google Scholar] [CrossRef]
- Ding, J.; Kang, X.; Feng, M.; Tan, J.; Feng, Q.; Wang, X.; Wang, J.; Liu, J.; Li, Z.; Guan, W.; et al. A novel active mitochondrion-selective fluorescent probe for the NIR fluorescence imaging and targeted photodynamic therapy of gastric cancer. Biomater. Sci. 2022, 10, 4756–4763. [Google Scholar] [CrossRef]
- Shui, S.; Zhao, Z.; Wang, H.; Conrad, M.; Liu, G. Non-enzymatic lipid peroxidation initiated by photodynamic therapy drives a distinct ferroptosis-like cell death pathway. Redox Biol. 2021, 45, 102056. [Google Scholar] [CrossRef]
- Valančiūtė, A.; Mathieson, L.; O’Connor, R.A.; Scott, J.I.; Vendrell, M.; Dorward, D.A.; Akram, A.R.; Dhaliwal, K. Phototherapeutic Induction of Immunogenic Cell Death and CD8+ T Cell-Granzyme B Mediated Cytolysis in Human Lung Cancer Cells and Organoids. Cancers 2022, 14, 4119. [Google Scholar] [CrossRef]
- Sweeney, E.E.; Cano-Mejia, J.; Fernandes, R. Photothermal Therapy Generates a Thermal Window of Immunogenic Cell Death in Neuroblastoma. Small 2018, 14, e1800678. [Google Scholar] [CrossRef]
- Krysko, D.V.; Garg, A.D.; Kaczmarek, A.; Krysko, O.; Agostinis, P.; Vandenabeele, P. Immunogenic cell death and DAMPs in cancer therapy. Nat. Rev. Cancer 2012, 12, 860–875. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.D.; Galluzzi, L.; Apetoh, L.; Baert, T.; Birge, R.B.; Bravo-San Pedro, J.M.; Breckpot, K.; Brough, D.; Chaurio, R.; Cirone, M.; et al. Molecular and Translational Classifications of DAMPs in Immunogenic Cell Death. Front. Immunol. 2015, 6, 588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galluzzi, L.; Vitale, I.; Warren, S.; Adjemian, S.; Agostinis, P.; Martinez, A.B.; Chan, T.A.; Coukos, G.; Demaria, S.; Deutsch, E.; et al. Consensus guidelines for the definition, detection and interpretation of immunogenic cell death. J. Immunother. Cancer 2020, 8, e000337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garg, A.D.; Nowis, D.; Golab, J.; Agostinis, P. Photodynamic therapy: Illuminating the road from cell death towards anti-tumour immunity. Apoptosis 2010, 15, 1050–1071. [Google Scholar] [CrossRef] [PubMed]
- Turubanova, V.D.; Balalaeva, I.V.; Mishchenko, T.A.; Catanzaro, E.; Alzeibak, R.; Peskova, N.N.; Efimova, I.; Bachert, C.; Mitroshina, E.V.; Krysko, O.; et al. Immunogenic cell death induced by a new photodynamic therapy based on photosens and photodithazine. J. Immunother. Cancer 2019, 7, 350. [Google Scholar] [CrossRef]
- Kessel, D.; Reiners, J.J., Jr. Effects of Combined Lysosomal and Mitochondrial Photodamage in a Non-small-Cell Lung Cancer Cell Line: The Role of Paraptosis. Photochem. Photobiol. 2017, 93, 1502–1508. [Google Scholar] [CrossRef]
- Wachowska, M.; Muchowicz, A.; Demkow, U. Immunological aspects of antitumor photodynamic therapy outcome. Cent. Eur. J. Immunol. 2015, 40, 481–485. [Google Scholar] [CrossRef] [Green Version]
- Agostinis, P.; Berg, K.; Cengel, K.A.; Foster, T.H.; Girotti, A.W.; Gollnick, S.O.; Hahn, S.M.; Hamblin, M.R.; Juzeniene, A.; Kessel, D.; et al. Photodynamic therapy of cancer: An update. CA Cancer J. Clin. 2011, 61, 250–281. [Google Scholar] [CrossRef]
- Loh, C.S.; Bedwell, J.; MacRobert, A.J.; Krasner, N.; Phillips, D.; Bown, S.G. Photodynamic therapy of the normal rat stomach: A comparative study between di-sulphonated aluminium phthalocyanine and 5-aminolaevulinic acid. Br. J. Cancer 1992, 66, 452–462. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.L.; Wei, J.; Cheng, L.W.; Zhang, Q.; Yan, P.; Wang, G. 5-aminolevulinic acid-mediated photodynamic effects on the proliferation and apoptosis of gastric cancer cell MKN-45. Cancer Res. Clin 2016, 5, 221–225. [Google Scholar]
- Rabenstein, T.; May, A.; Gossner, L.; Manner, H.; Pech, O.; Günter, E.; Huijmans, J.; Vieth, M.; Stolte, M.; Ell, C. Invisible gastric carcinoma detected by random biopsy: Long-term results after photodynamic therapy. Endoscopy 2008, 40, 899–904. [Google Scholar] [CrossRef]
- Oinuma, T.; Nakamura, T.; Nishiwaki, Y. Report on the National Survey of Photodynamic Therapy (PDT) for Gastric Cancer in Japan (a secondary publication). Laser Ther. 2016, 25, 87–98. [Google Scholar] [CrossRef]
- Namiki, Y.; Namiki, T.; Date, M.; Yanagihara, K.; Yashiro, M.; Takahashi, H. Enhanced photodynamic antitumor effect on gastric cancer by a novel photosensitive stealth liposome. Pharmacol. Res. 2004, 50, 65–76. [Google Scholar] [CrossRef]
- Chen, J.; Mao, L.; Liu, S.; Liang, Y.; Wang, S.; Wang, Y.; Zhao, Q.; Zhang, X.; Che, Y.; Gao, L.; et al. Effects of a novel porphyrin-based photosensitizer on sensitive and multidrug-resistant human gastric cancer cell lines. J. Photochem. Photobiol. B 2015, 151, 186–193. [Google Scholar] [CrossRef]
- Korsak, B.; Almeida, G.M.; Rocha, S.; Pereira, C.; Mendes, N.; Osório, H.; Pereira, P.M.R.; Rodrigues, J.M.M.; Schneider, R.J.; Sarmento, B.; et al. Porphyrin modified trastuzumab improves efficacy of HER2 targeted photodynamic therapy of gastric cancer. Int. J. Cancer 2017, 141, 1478–1489. [Google Scholar] [CrossRef] [Green Version]
- Igarashi, A.; Konno, H.; Tanaka, T.; Nakamura, S.; Sadzuka, Y.; Hirano, T.; Fujise, Y. Liposomal photofrin enhances therapeutic efficacy of photodynamic therapy against the human gastric cancer. Toxicol. Lett. 2003, 145, 133–141. [Google Scholar] [CrossRef] [Green Version]
- Kishi, K.; Yano, M.; Inoue, M.; Miyashiro, I.; Motoori, M.; Tanaka, K.; Goto, K.; Eguchi, H.; Noura, S.; Yamada, T.; et al. Talaporfin-mediated photodynamic therapy for peritoneal metastasis of gastric cancer in an in vivo mouse model: Drug distribution and efficacy studies. Int. J. Oncol. 2010, 36, 313–320. [Google Scholar] [CrossRef] [Green Version]
- Kato, H.; Kito, T.; Furuse, K.; Sakai, E.; Ito, K.; Mimura, S.; Okusima, N.; Naito, K.; Suzuki, S. Photodynamic therapy in the early treatment of cancer. Gan To Kagaku Ryoho 1990, 17, 1833–1838. [Google Scholar]
- Kato, H.; Horai, T.; Furuse, K.; Fukuoka, M.; Suzuki, S.; Hiki, Y.; Ito, Y.; Mimura, S.; Tenjin, Y.; Hisazumi, H.; et al. Photodynamic therapy for cancers: A clinical trial of porfimer sodium in Japan. Jpn. J. Cancer Res. 1993, 84, 1209–1214. [Google Scholar] [CrossRef]
- Mimura, S.; Ito, Y.; Nagayo, T.; Ichii, M.; Kato, H.; Sakai, H.; Goto, K.; Noguchi, Y.; Tanimura, H.; Nagai, Y.; et al. Cooperative clinical trial of photodynamic therapy with photofrin II and excimer dye laser for early gastric cancer. Lasers Surg. Med. 1996, 19, 168–172. [Google Scholar] [CrossRef]
- Iyer, A.K.; Greish, K.; Seki, T.; Okazaki, S.; Fang, J.; Takeshita, K.; Maeda, H. Polymeric micelles of zinc protoporphyrin for tumor targeted delivery based on EPR effect and singlet oxygen generation. J. Drug Target. 2007, 15, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Hamblin, M.R.; Newman, E.L. On the mechanism of the tumour-localising effect in photodynamic therapy. J. Photochem. Photobiol. B 1994, 23, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Teng, Y.; Fu, Y.; Zhang, C. Chlorins e6 loaded silica nanoparticles coated with gastric cancer cell membrane for tumor specific photodynamic therapy of gastric cancer. Int. J. Nanomed. 2019, 14, 5061–5071. [Google Scholar] [CrossRef] [PubMed]
- Pan, S.; Pei, L.; Zhang, A.; Zhang, Y.; Zhang, C.; Huang, M.; Huang, Z.; Liu, B.; Wang, L.; Ma, L.; et al. Passion fruit-like exosome-PMA/Au-BSA@Ce6 nanovehicles for real-time fluorescence imaging and enhanced targeted photodynamic therapy with deep penetration and superior retention behavior in tumor. Biomaterials 2020, 230, 119606. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Karashima, T.; Kamada, M.; Shuin, T.; Kurabayashi, A.; Furihata, M.; Fujita, H.; Utsumi, K.; Sasaki, J. Regulation of 5-aminolevulinic acid-mediated protoporphyrin IX accumulation in human urothelial carcinomas. Pathobiology 2009, 76, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Namikawa, T.; Yatabe, T.; Inoue, K.; Shuin, T.; Hanazaki, K. Clinical applications of 5-aminolevulinic acid-mediated fluorescence for gastric cancer. World J. Gastroenterol. 2015, 21, 8769–8775. [Google Scholar] [CrossRef]
- Namikawa, T.; Inoue, K.; Uemura, S.; Shiga, M.; Maeda, H.; Kitagawa, H.; Fukuhara, H.; Kobayashi, M.; Shuin, T.; Hanazaki, K. Photodynamic diagnosis using 5-aminolevulinic acid during gastrectomy for gastric cancer. J. Surg. Oncol. 2014, 109, 213–217. [Google Scholar] [CrossRef]
- Tsujimoto, H.; Morimoto, Y.; Takahata, R.; Nomura, S.; Yoshida, K.; Horiguchi, H.; Hiraki, S.; Ono, S.; Miyazaki, H.; Saito, D.; et al. Photodynamic therapy using nanoparticle loaded with indocyanine green for experimental peritoneal dissemination of gastric cancer. Cancer Sci. 2014, 105, 1626–1630. [Google Scholar] [CrossRef]
- Liu, F.F. Photodynamic therapy for early esophageal and gastric cancer. Chin. J. Laser Med. 2005, 14, 1. [Google Scholar]
- Yu, X.H.; Wang, Q.T.; Zhang, F.X.; Sun, Y.B.; Zhao, L. Correlation between clinical efficacy and histopathological classification and grading of advanced gastric cancer treated with laser photodynamic therapy. Chin. Oncol. Clin. Rehabil. 2008, 15, 201–203. [Google Scholar]
- Song, D.X. Short-term and long-term efficacy of photodynamic therapy in 148 cases of upper digestive tract cancer. Chin. J. Laser Med. 2008, 17, 23–27. [Google Scholar]
- Xu, S.; Bulin, A.L.; Hurbin, A.; Elleaume, H.; Coll, J.L.; Broekgaarden, M. Photodynamic Diagnosis and Therapy for Peritoneal Carcinomatosis: Emerging Perspectives. Cancers 2020, 12, 2491. [Google Scholar] [CrossRef]
- Xin, J.; Wang, S.; Zhang, L.; Xin, B.; He, Y.; Wang, J.; Wang, S.; Shen, L.; Zhang, Z.; Yao, C. Comparison of the synergistic anticancer activity of AlPcS4 photodynamic therapy in combination with different low-dose chemotherapeutic agents on gastric cancer cells. Oncol. Rep. 2018, 40, 165–178. [Google Scholar] [CrossRef]
- Long, W.; Zhang, L.; Wang, Y.; Xie, H.; Wang, L.; Yu, H. Research Progress and Prospects of Autophagy in the Mechanism of Multidrug Resistance in Tumors. J. Oncol. 2022, 2022, 7032614. [Google Scholar] [CrossRef]
- Zhao, R.; Ning, X.; Wang, M.; Yu, A.; Wang, Y. A multifunctional nano-delivery system enhances the chemo-co-phototherapy of tumor multidrug resistance via mitochondrial-targeting and inhibiting P-glycoprotein-mediated efflux. J. Mater. Chem. B 2021, 9, 9174–9182. [Google Scholar] [CrossRef]
- Wang, B.; Wang, Y.; Zhang, T.; Gao, L.; Xiang, L.; Maswikiti, E.P.; Wang, N.; Yu, Y.; Ma, C.; Ma, H.; et al. Photodynamic therapy combined with bimetallic stent in the treatment of gastric cancer with malignant duodenobiliary obstruction: A case report and literature review. Transl. Cancer Res. 2022, 11, 2425–2432. [Google Scholar] [CrossRef]
- Shirasu, N.; Yamada, H.; Shibaguchi, H.; Kuroki, M.; Kuroki, M. Potent and specific antitumor effect of CEA-targeted photoimmunotherapy. Int. J. Cancer 2014, 135, 2697–2710. [Google Scholar] [CrossRef]
- Ma, C.H.; Ma, H.H.; Deng, X.B.; Yu, R.; Song, K.W.; Wei, K.K.; Wang, C.J.; Li, H.X.; Chen, H. Photodynamic Therapy in Combination with Chemotherapy, Targeted, and Immunotherapy As a Successful Therapeutic Approach for Advanced Gastric Adenocarcinoma: A Case Report and Literature Review. Photobiomodul. Photomed. Laser Surg. 2022, 40, 308–314. [Google Scholar] [CrossRef]
- Krosl, G.; Korbelik, M.; Dougherty, G.J. Induction of immune cell infiltration into murine SCCVII tumour by photofrin-based photodynamic therapy. Br. J. Cancer 1995, 71, 549–555. [Google Scholar] [CrossRef] [Green Version]
- Sun, J.; Cecic, I.; Parkins, C.S.; Korbelik, M. Neutrophils as inflammatory and immune effectors in photodynamic therapy-treated mouse SCCVII tumours. Photochem. Photobiol. Sci. 2002, 1, 690–695. [Google Scholar] [CrossRef]
- Gollnick, S.O.; Evans, S.S.; Baumann, H.; Owczarczak, B.; Maier, P.; Vaughan, L.; Wang, W.C.; Unger, E.; Henderson, B.W. Role of cytokines in photodynamic therapy-induced local and systemic inflammation. Br. J. Cancer 2003, 88, 1772–1779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gollnick, S.O.; Vaughan, L.; Henderson, B.W. Generation of effective antitumor vaccines using photodynamic therapy. Cancer Res. 2002, 62, 1604–1608. [Google Scholar] [PubMed]
- Korbelik, M.; Sun, J. Photodynamic therapy-generated vaccine for cancer therapy. Cancer Immunol. Immunother. 2006, 55, 900–909. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Ma, W.; Li, Y. Generation of effective vaccines against liver cancer by using photodynamic therapy. Lasers Med. Sci. 2009, 24, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Gollnick, S.O.; Brackett, C.M. Enhancement of anti-tumor immunity by photodynamic therapy. Immunol. Res. 2010, 46, 216–226. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Hady, E.S.; Martin-Hirsch, P.; Duggan-Keen, M.; Stern, P.L.; Moore, J.V.; Corbitt, G.; Kitchener, H.C.; Hampson, I.N. Immunological and viral factors associated with the response of vulval intraepithelial neoplasia to photodynamic therapy. Cancer Res. 2001, 61, 192–196. [Google Scholar]
- Nagareddy, R.; Thomas, R.G.; Jeong, Y.Y. Stimuli-Responsive Polymeric Nanomaterials for the Delivery of Immunotherapy Moieties: Antigens, Adjuvants and Agonists. Int. J. Mol. Sci. 2021, 22, 12510. [Google Scholar] [CrossRef]
- Tan, K.; Li, R.; Huang, X.; Liu, Q. Outer Membrane Vesicles: Current Status and Future Direction of These Novel Vaccine Adjuvants. Front. Microbiol. 2018, 9, 783. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Xu, L.; Wang, C.; Yang, R.; Zhuang, Q.; Han, X.; Dong, Z.; Zhu, W.; Peng, R.; Liu, Z. Near-Infrared-Triggered Photodynamic Therapy with Multitasking Upconversion Nanoparticles in Combination with Checkpoint Blockade for Immunotherapy of Colorectal Cancer. ACS Nano 2017, 11, 4463–4474. [Google Scholar] [CrossRef]
- Zheng, X.; Xing, D.; Zhou, F.; Wu, B.; Chen, W.R. Indocyanine green-containing nanostructure as near infrared dual-functional targeting probes for optical imaging and photothermal therapy. Mol. Pharm. 2011, 8, 447–456. [Google Scholar] [CrossRef]
- Zheng, X.; Zhou, F.; Wu, B.; Chen, W.R.; Xing, D. Enhanced tumor treatment using biofunctional indocyanine green-containing nanostructure by intratumoral or intravenous injection. Mol. Pharm. 2012, 9, 514–522. [Google Scholar] [CrossRef] [Green Version]
- Yanai, H.; Kuroiwa, Y.; Shimizu, N.; Matsubara, Y.; Okamoto, T.; Hirano, A.; Nakamura, Y.; Okita, K.; Sekine, T. The pilot experience of immunotherapy-combined photodynamic therapy for advanced gastric cancer in elderly patients. Int. J. Gastrointest. Cancer 2002, 32, 139–142. [Google Scholar] [CrossRef]
- Kurokawa, H.; Ito, H.; Terasaki, M.; Matsui, H. Hyperthermia enhances photodynamic therapy by regulation of HCP1 and ABCG2 expressions via high level ROS generation. Sci. Rep. 2019, 9, 1638. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mechanism | Mode of Action | References |
|---|---|---|
| Necrosis | Substantial membrane photodamage | Ref. [33] |
| Apoptosis | Mediated Bcl-2 loss and promoted the release of Ca (2+) from the endoplasmic reticulum | Ref. [34] |
| Autophagy | Targets the mTOR signaling network | Refs. [35,36] |
| Pyroptosis | Photodynamics induced pyroptosis through ROS-NLRP3-CASP1-GSDMD pathway | Ref. [38] |
| Ferroptosis | Non-enzymatic lipid peroxidation | Ref. [39] |
| Author | Photosensitizer | Year | Activation Wavelength | Cell Line | Efficacy |
|---|---|---|---|---|---|
| Tan YK [37] | HCE6 | 2019 | 660 nm | MKN45 | Completely kill the cell |
| Namiki Y [54] | PSSL | 2003 | 300–750 nm | MKN-45, MKN-74 NUGC4, HSC-43 | The cell killing rate of PSSL was 53 times higher than that of CE6-NA photosensitizer |
| Chen J [55] | DTP | 2015 | 650 nm | MGC803 MGC803/PA | Eradicate gastric cancer cells whether or not they express MDR |
| Wang X [51] | 5-ALA | 2016 | 375–400 nm | MKN-45 | Significantly inhibit proliferation and promote apoptosis |
| Korsak B [56] | Trast:Porph | 2017 | - | Her2-Positive cells | Higher selectivity and cytotoxicity than trastuzumab |
| Author | Photosensitizer | Year | Activation Wavelength | Cell Line | Modeling Animal | Efficacy |
|---|---|---|---|---|---|---|
| Igarashi A [57] | 1 LPF | 2003 | 630 nm | MT-2 | BALB/c nude mice | Enhanced selective aggregation of photosensitizers in tumor tissue |
| Kishi K [58] | Talaporfin | 2010 | 664 nm | MKN-45 | BALB/c nude mice | Possibly effective in patients with advanced GC and metastatic peritoneal nodules |
| Namiki Y [54] | PSSL | 2003 | 300–750 nm | MKN-45 MKN-74 NUGC4 HSC-43 | BALB/c nude mice | Stronger photodynamic effect than CE6-NA |
| Author | Photosensitizer | Year | Activation Wavelength | Tumor Types | Number of Patients | Efficacy |
|---|---|---|---|---|---|---|
| Kato H [59] | Photofrin II(DHE) | 1833 | 630 nm | Early GC | 120 | CR77% |
| Kato H [60] | Photofrin | 1993 | 630 nm | Superficial cancer | 58 | CR83% |
| Mimura S [61] | Photofrin II | 1996 | 630 nm | Early GC | 27 | CR88% |
| Rabenstein [52] | ALA | 2008 | 635 nm | Early GC | 22 | CR68% |
| Oinuma T [53] | Photofrin, Talaporfin, ALA, HPD | 2016 | Early GC | 57 | CR74% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.; Ewetse, M.P.; Ma, C.; Pu, W.; Xu, B.; He, P.; Wang, Y.; Zhu, J.; Chen, H. The “Light Knife” for Gastric Cancer: Photodynamic Therapy. Pharmaceutics 2023, 15, 101. https://doi.org/10.3390/pharmaceutics15010101
Wang H, Ewetse MP, Ma C, Pu W, Xu B, He P, Wang Y, Zhu J, Chen H. The “Light Knife” for Gastric Cancer: Photodynamic Therapy. Pharmaceutics. 2023; 15(1):101. https://doi.org/10.3390/pharmaceutics15010101
Chicago/Turabian StyleWang, Haiyun, Maswikiti Paul Ewetse, Chenhui Ma, Weigao Pu, Bo Xu, Puyi He, Yunpeng Wang, Jingyu Zhu, and Hao Chen. 2023. "The “Light Knife” for Gastric Cancer: Photodynamic Therapy" Pharmaceutics 15, no. 1: 101. https://doi.org/10.3390/pharmaceutics15010101
APA StyleWang, H., Ewetse, M. P., Ma, C., Pu, W., Xu, B., He, P., Wang, Y., Zhu, J., & Chen, H. (2023). The “Light Knife” for Gastric Cancer: Photodynamic Therapy. Pharmaceutics, 15(1), 101. https://doi.org/10.3390/pharmaceutics15010101