
Off-Label Prescribing in Pediatric Population—Literature Review for 2012–2022



Abstract
:1. Introduction
2. The Need for Pediatric Drugs
2.1. Features of the Children
2.2. Drug Formulations for Children
2.3. Dosing in Children
2.4. Conducting Clinical Research with Children
3. Legislative and Ethical Measures for Off-Label Restriction
4. Methods
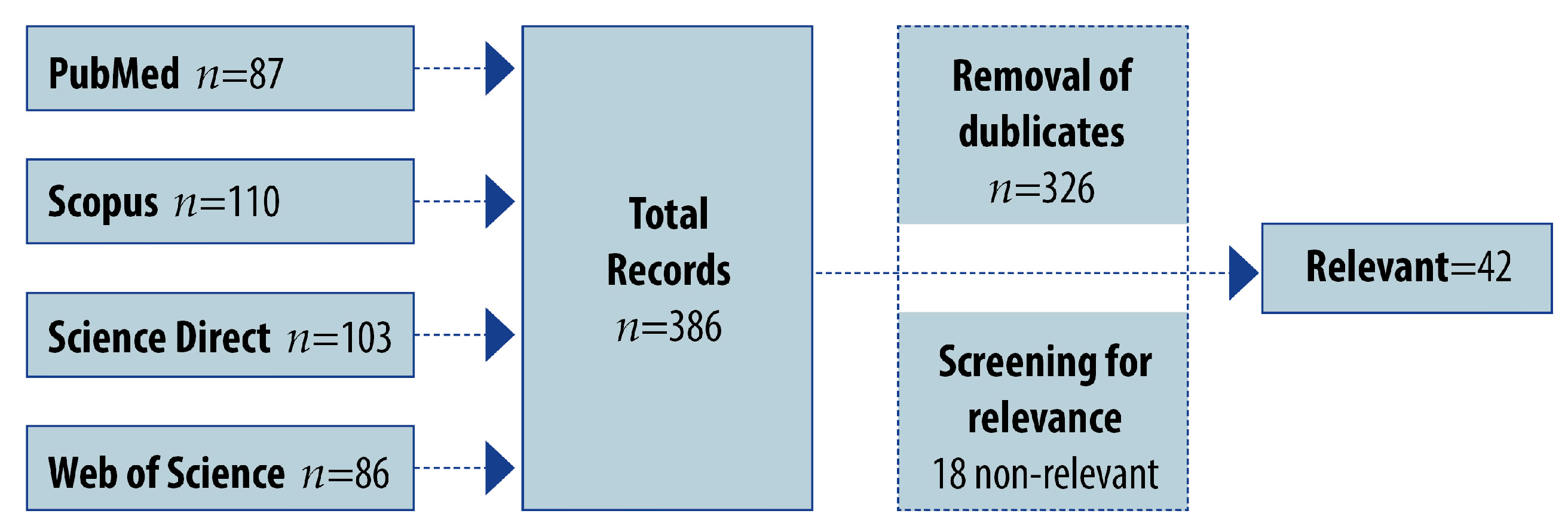
4.1. Search Strategy for the Prevalence of Off-Label Use
4.2. Inclusion and Exclusion Criteria
5. Results
5.1. Overall Prevalence of Off-Label Drug Prescribing in Pediatrics
5.2. Prevalence of Off-Label Drug Prescribing in Neonates
5.3. Prevalence of Off-Label Drug Prescribing by Drug Groups
6. Discussion
7. Conclusions
7.1. Achievements
7.2. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rusz, C.-M.; Ősz, B.-E.; Jîtcă, G.; Miklos, A.; Bătrînu, M.-G.; Imre, S. Off-Label Medication: From a Simple Concept to Complex Practical Aspects. Int. J. Environ. Res. Public Health 2021, 18, 10447. [Google Scholar] [CrossRef]
- Wu, H.; Wu, G. Strategy to address innovative off-label medication use in China: Grading management. Eur. J. Clin. Pharmacol. 2014, 70, 1271–1273. [Google Scholar] [CrossRef]
- Kaley, V.R.; Aregullin, E.O.; Samuel, B.P.; Vettukattil, J.J. Trends in the off-label use of β-blockers in pediatric patients. Pediatr. Int. 2019, 61, 1071–1080. [Google Scholar] [CrossRef]
- Aronson, J.K.; Ferner, R.E. Unlicensed and off-label uses of medicines: Definitions and clarification of terminology. Br. J. Clin. Pharmacol. 2017, 83, 2615–2625. [Google Scholar] [CrossRef]
- Oni, L.; Hawcutt, D.; Turner, M.; Beresford, M.; McWilliam, S.; Barton, C.; Park, B.; Murray, P.; Wilm, B.; Copple, I.; et al. Optimising the use of medicines to reduce acute kidney injury in children and babies. Pharmacol. Ther. 2017, 174, 55–62. [Google Scholar] [CrossRef]
- Allen, H.C.; Garbe, M.C.; Lees, J.; Aziz, N.; Chaaban, H.; Miller, J.L.; Johnson, P.; DeLeon, S. Off-Label Medication use in Children, More Common than We Think: A Systematic Review of the Literature. J. Okla. State Med. Assoc. 2018, 111, 776–783. [Google Scholar]
- Zhang, L.L.; Li, Y.P.; Linan, Z.; Iang, Y.; Hu, D.; Liu, Y.; Lv, J. Evidence-based evaluation on off-label drug use policies in 15 countries. Chin. J. Evid.-Based Med. 2012, 12, 426–435. [Google Scholar]
- Nardini, C. The ethics of clinical trials. Ecancermedicalscience 2014, 8, 387. [Google Scholar] [CrossRef]
- Seale, J.P. Off-label prescribing. Med. J. Aust. 2014, 200, 65. [Google Scholar] [CrossRef]
- Khan, D.; Kirby, D.; Bryson, S.; Shah, M.; Mohammed, A.R. Paediatric specific dosage forms: Patient and formulation considerations. Int. J. Pharm. 2022, 616, 121501. [Google Scholar] [CrossRef]
- Lenk, C. Off-label drug use in paediatrics: A world-wide problem. Curr. Drug Targets 2012, 13, 878–884. [Google Scholar] [CrossRef]
- McCune, S.; Portman, R.J. Accelerating Pediatric Drug Development: A 2022 Special Issue of Therapeutic Innovation & Regulatory Science. Ther. Innov. Regul. Sci. 2022, 56, 869–872. [Google Scholar] [CrossRef]
- Klassen, T.P.; Hartling, L.; Craig, J.C.; Offringa, M. Children Are Not Just Small Adults: The Urgent Need for High-Quality Trial Evidence in Children. PLOS Med. 2008, 5, e172. [Google Scholar] [CrossRef]
- Martinez-Castaldi, C.; Silverstein, M.; Bauchner, H. Child Versus Adult Research: The Gap in High-Quality Study Design. Pediatrics 2008, 122, 52–57. [Google Scholar] [CrossRef]
- Allegaert, K.; Anker, J.v.D. Neonates are not just little children and need more finesse in dosing of antibiotics. Acta Clin. Belg. 2019, 74, 157–163. [Google Scholar] [CrossRef]
- Batchelor, H.K.; Marriott, J.F. Paediatric pharmacokinetics: Key considerations. Br. J. Clin. Pharmacol. 2015, 79, 395–404. [Google Scholar] [CrossRef]
- Ku, L.C.; Smith, P.B. Dosing in neonates: Special considerations in physiology and trial design. Pediatr. Res. 2015, 77, 2–9. [Google Scholar] [CrossRef]
- Mulugeta, Y.; Barrett, J.S.; Nelson, R.; Eshete, A.T.; Mushtaq, A.; Yao, L.; Glasgow, N.; Mulberg, A.E.; Gonzalez, D.; Green, D.; et al. Exposure Matching for Extrapolation of Efficacy in Pediatric Drug Development. J. Clin. Pharmacol. 2016, 56, 1326–1334. [Google Scholar] [CrossRef]
- Jimenez, R.; Smith, A.; Carleton, B. New Ways of Detecting ADRs in Neonates and Children. Curr. Pharm. Des. 2015, 21, 5643–5649. [Google Scholar] [CrossRef]
- Stephenson, T. How children’s responses to drugs differ from adults. Br. J. Clin. Pharmacol. 2005, 59, 670–673. [Google Scholar] [CrossRef]
- Raymond, A.S.; Brasseur, D. Development of medicines for children in Europe: Ethical implications. Paediatr. Respir. Rev. 2005, 6, 45–51. [Google Scholar] [CrossRef]
- O’Hara, K. Paediatric pharmacokinetics and drug doses. Aust. Prescr. 2016, 39, 208–210. [Google Scholar] [CrossRef]
- Milne, C.-P.; Bruss, J.B. The economics of pediatric formulation development for off-patent drugs. Clin. Ther. 2008, 30, 2133–2145. [Google Scholar] [CrossRef]
- Ogbonna, J.D.N.; Cunha, E.; Attama, A.A.; Ofokansi, K.C.; Ferreira, H.; Pinto, S.; Gomes, J.; Marx, M.G.; Peres, A.M.; Lobo, J.M.S.; et al. Overcoming Challenges in Pediatric Formulation with a Patient-Centric Design Approach: A Proof-of-Concept Study on the Design of an Oral Solution of a Bitter Drug. Pharmaceuticals 2022, 15, 1331. [Google Scholar] [CrossRef]
- Nunn, T.; Williams, J. Formulation of medicines for children. Br. J. Clin. Pharmacol. 2005, 59, 674–676. [Google Scholar] [CrossRef]
- Duncan, J.C.; Bracken, L.E.; Nunn, A.J.; Peak, M.; Turner, M.A. Development and evaluation of an assessment of the age-appropriateness/inappropriateness of formulations used in children. Int. J. Clin. Pharm. 2022, 44, 1394–1405. [Google Scholar] [CrossRef]
- Batchelor, H.K.; Marriott, J.F. Formulations for children: Problems and solutions. Br. J. Clin. Pharmacol. 2015, 79, 405–418. [Google Scholar] [CrossRef]
- Ranmal, S.R.; Cram, A.; Tuleu, C. Age-appropriate and acceptable paediatric dosage forms: Insights into end-user perceptions, preferences and practices from the Children’s Acceptability of Oral Formulations (CALF) Study. Int. J. Pharm. 2016, 514, 296–307. [Google Scholar] [CrossRef]
- Souza, A.; Santos, D.; Fonseca, S.; Medeiros, M.; Batista, L.; Turner, M.; Coelho, H. Toxic excipients in medications for neonates in Brazil. Eur. J. Pediatr. 2014, 173, 935–945. [Google Scholar] [CrossRef]
- Fabiano, V.; Mameli, C.; Zuccotti, G.V. Paediatric pharmacology: Remember the excipients. Pharmacol. Res. 2011, 63, 362–365. [Google Scholar] [CrossRef]
- Saito, J.; Agrawal, A.; Patravale, V.; Pandya, A.; Orubu, S.; Zhao, M.; Andrews, G.P.; Petit-Turcotte, C.; Landry, H.; Croker, A.; et al. The Current States, Challenges, Ongoing Efforts, and Future Perspectives of Pharmaceutical Excipients in Pediatric Patients in Each Country and Region. Children 2022, 9, 453. [Google Scholar] [CrossRef]
- Alessandrini, E.; Brako, F.; Scarpa, M.; Lupo, M.; Bonifazi, D.; Pignataro, V.; Cavallo, M.; Cullufe, O.; Enache, C.; Nafria, B.; et al. Children’s Preferences for Oral Dosage Forms and Their Involvement in Formulation Research via EPTRI (European Paediatric Translational Research Infrastructure). Pharmaceutics 2021, 13, 730. [Google Scholar] [CrossRef]
- Li, J.; Li, C.; Zhang, H.; Gao, X.; Wang, T.; Wang, Z.; Zheng, A. Preparation of Azithromycin Amorphous Solid Dispersion by Hot-Melt Extrusion: An Advantageous Technology with Taste Masking and Solubilization Effects. Polymers 2022, 14, 495. [Google Scholar] [CrossRef]
- Huynh, D.T.M.; Hai, H.T.; Hau, N.M.; Lan, H.K.; Vinh, T.P.; De Tran, V.; Pham, D.T. Preparations and characterizations of effervescent granules containing azithromycin solid dispersion for children and elder: Solubility enhancement, taste-masking, and digestive acidic protection. Heliyon 2023, 9, e16592. [Google Scholar] [CrossRef]
- Cornilă, A.; Iurian, S.; Tomuță, I.; Porfire, A. Orally Dispersible Dosage Forms for Paediatric Use: Current Knowledge and Development of Nanostructure-Based Formulations. Pharmaceutics 2022, 14, 1621. [Google Scholar] [CrossRef]
- Van Riet-Nales, D.A.; Kozarewicz, P.; Aylward, B.; de Vries, R.; Egberts, T.C.G.; Rademaker, C.M.A.; Schobben, A.F.A.M. Paediatric Drug Development and Formulation Design—A European Perspective. AAPS Pharmscitech. 2017, 18, 241–249. [Google Scholar] [CrossRef]
- Baguley, D.; Lim, E.; Bevan, A.; Pallet, A.; Faust, S.N. Prescribing for children—Taste and palatability affect adherence to antibiotics: A review. Arch. Dis. Child. 2012, 97, 293–297. [Google Scholar] [CrossRef]
- Yuliani, S.H.; Putri, D.C.A.; Virginia, D.M.; Gani, M.R.; Riswanto, F.D.O. Prevalence, Risk, and Challenges of Extemporaneous Preparation for Pediatric Patients in Developing Nations: A Review. Pharmaceutics 2023, 15, 840. [Google Scholar] [CrossRef]
- MacArthur, R.B.; Ashworth, L.D.; Zhan, K.; Parrish, R.H., 2nd. How Compounding Pharmacies Fill Critical Gaps in Pediatric Drug Development Processes: Suggested Regulatory Changes to Meet Future Challenges. Children 2022, 9, 1885. [Google Scholar] [CrossRef]
- Mennella, J.A.; Spector, A.C.; Reed, D.R.; Coldwell, S.E. The bad taste of medicines: Overview of basic research on bitter taste. Clin. Ther. 2013, 35, 1225–1246. [Google Scholar] [CrossRef]
- Smith, L.; Leggett, C.; Borg, C. Administration of medicines to children: A practical guide. Aust. Prescr. 2022, 45, 188–192. [Google Scholar] [CrossRef]
- Vieira, I.; Sousa, J.J.; Vitorino, C. Paediatric Medicines—Regulatory Drivers, Restraints, Opportunities and Challenges. J. Pharm. Sci. 2021, 110, 1545–1556. [Google Scholar] [CrossRef]
- Kearns, G.L.; Abdel-Rahman, S.M.; Alander, S.W.; Blowey, D.L.; Leeder, J.S.; Kauffman, R.E. Developmental Pharmacology—Drug Disposition, Action, and Therapy in Infants and Children. N. Engl. J. Med. 2003, 349, 1157–1167. [Google Scholar] [CrossRef]
- Rahimzadeh, V.; Wolfert, S.; Buenger, V.; Campbell, C.; French, R.; Ludwinski, D.; Weinstein, A.; Barrett, C. A systematic literature review to identify ethical, legal, and social responsibilities of nonprofit organizations when funding clinical trials in pediatric cancer. Pediatr. Blood Cancer 2022, 69, e29854. [Google Scholar] [CrossRef]
- Shaniv, D.; Bolisetty, S.; Young, T.E.; Mangum, B.; Ainsworth, S.; Elbers, L.; Schultz, P.; Cucchi, M.; de Wildt, S.N.; van der Zanden, T.M.; et al. Neonatal Drug Formularies—A Global Scope. Children 2023, 10, 848. [Google Scholar] [CrossRef]
- Suwa, M.; Miyake, S.; Urushihara, H. Comparison of Regulations and Status of Promoting Drug Development and Authorization of Pediatric Indications among Japan, the United States and the United Kingdom. Rinsho yakuri/Jpn. J. Clin. Pharmacol. Ther. 2022, 53, 225–234. [Google Scholar] [CrossRef]
- Le, J.; Bradley, J.S. Optimizing Antibiotic Drug Therapy in Pediatrics: Current State and Future Needs. J. Clin. Pharmacol. 2018, 58 (Suppl. 10), S108–S122. [Google Scholar] [CrossRef]
- Mahmood, I. A comparison of different methods for the first-in-pediatric dose selection. J. Clin. Translat. Res. 2022, 8, 369–381. [Google Scholar]
- Gaeta, F.; Conti, V.; Pepe, A.; Vajro, P.; Filippelli, A.; Mandato, C. Drug dosing in children with obesity: A narrative updated review. Ital. J. Pediatr. 2022, 48, 168. [Google Scholar] [CrossRef]
- van den Anker, J.; Reed, M.D.; Allegaert, K.; Kearns, G.L. Developmental Changes in Pharmacokinetics and Pharmacodynamics. J. Clin. Pharmacol. 2018, 58 (Suppl. 10), S10–S25. [Google Scholar] [CrossRef]
- Anderson, B.J.; Holford, N.H.G. Understanding dosing: Children are small adults, neonates are immature children. Arch. Dis. Child. 2013, 98, 737–744. [Google Scholar] [CrossRef]
- Roy, H.; Bertoldi, C.; Farrell, C.; Rousseau, E. Prescribing drugs to overweight and obese children: Balancing efficacy and safety. Paediatr. Child Health 2021, 26, e236–e239. [Google Scholar] [CrossRef]
- Kendrick, J.G.; Carr, R.R.; Ensom, M.H. Pediatric Obesity: Pharmacokinetics and Implications for Drug Dosing. Clin. Ther. 2015, 37, 1897–1923. [Google Scholar] [CrossRef]
- Joseph, P.D.; Craig, J.C.; Caldwell, P.H. Clinical trials in children. Br. J. Clin. Pharmacol. 2015, 79, 357–369. [Google Scholar] [CrossRef]
- Pawar, G.; Wu, F.; Zhao, L.; Fang, L.; Burckart, G.J.; Feng, K.; Mousa, Y.M.; Naumann, F.; Batchelor, H.K. Development of a Pediatric Relative Bioavailability/Bioequivalence Database and Identification of Putative Risk Factors Associated with Evaluation of Pediatric Oral Products. AAPS J. 2021, 23, 57. [Google Scholar] [CrossRef]
- Matsui, K.; Ibuki, T.; Tashiro, S.; Nakamura, H.; Study Group on Regulatory Science for Early Clinical Application of Pediatric Pharmaceuticals. Principles of ethical consideration required for clinical research involving children. Pediatr. Int. 2021, 63, 248–259. [Google Scholar] [CrossRef]
- Krishna, S.; Fuloria, M. Ethical Considerations in Neonatal Research. NeoReviews 2022, 23, e151–e158. [Google Scholar] [CrossRef]
- Declaration of Helsinki. Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects (accessed on 30 July 2023).
- The Belmont Report: Ethical Principles and Guidelines for the Protection of Human Subject of Research. Available online: https://www.hhs.gov/ohrp/sites/default/files/the-belmont-report-508c_FINAL.pdf (accessed on 24 August 2023).
- Guideline for Good Clinical Practice E6(R2). Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-guideline-good-clinical-practice-e6r2-step-5_en.pdf (accessed on 25 August 2023).
- ICH Topic E11. Clinical Investigation of Medicinal Products in the Paediatric Population. CPMP/ICH/2711/99. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/e-11-clinical-investigation-medicinal-products-paediatric-population-step-5_en.pdf (accessed on 5 August 2023).
- Directive 2001/20/EC of the European Parliament and the Council on the Approximation of the Laws, Regulations and Administrative Provisions of the Member States Relating to Implementation of Good Clinical Practice-GCP-in the Conduct of Clinical Trials on Medicinal Products for Human Use. Available online: https://health.ec.europa.eu/system/files/2016-11/dir_2001_20_en_0.pdf (accessed on 12 August 2023).
- Code for Federal Regulations (CFR), Title 45, Part 46, Subpart D. Additional Protections for Children Involved as Subjects in Research. Available online: https://www.ecfr.gov/current/title-45/subtitle-A/subchapter-A/part-46/subpart-D (accessed on 15 August 2023).
- NHI Policy and Guidelines on the Inclusion of Children as Participants in Research Involving Human Subjects. March 1998. Available online: https://grants.nih.gov/grants/guide/notice-files/not98-024.html (accessed on 15 August 2023).
- Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans—TCPS 2. 2022. Available online: https://ethics.gc.ca/eng/documents/tcps2-2022-en.pdf (accessed on 21 August 2023).
- Thompson, G.; Barker, C.I.; Folgori, L.; Bielicki, J.A.; Bradley, J.S.; Lutsar, I.; Sharland, M. Global shortage of neonatal and paediatric antibiotic trials: Rapid review. BMJ Open 2017, 7, e016293. [Google Scholar] [CrossRef]
- The World Bank. Population Ages 0–14 (% of Total Population). Available online: https://data.worldbank.org/indicator/SP.POP.0014.TO.ZS (accessed on 25 August 2023).
- van der Zanden, T.M.; Smeets, N.J.; de Hoop-Sommen, M.; Schwerzel, M.F.; Huang, H.J.; Barten, L.J.; van der Heijden, J.E.; Freriksen, J.J.; Horstink, A.A.; Holsappel, I.H.; et al. Off-Label, but on-Evidence? A Review of the Level of Evidence for Pediatric Pharmacotherapy. Clin. Pharmacol. Ther. 2022, 112, 1243–1253. [Google Scholar] [CrossRef]
- Fung, A.; Yue, X.; Wigle, P.R.; Guo, J.J. Off-label medication use in rare pediatric diseases in the United States. Intractable Rare Dis. Res. 2021, 10, 238–245. [Google Scholar] [CrossRef]
- Lagler, F.B.; Hirschfeld, S.; Kindblom, J.M. Challenges in clinical trials for children and young people. Arch. Dis. Child. 2021, 106, 321–325. [Google Scholar] [CrossRef]
- Tsukamoto, K.; Carroll, K.A.; Onishi, T.; Matsumaru, N.; Brasseur, D.; Nakamura, H. Improvement of Pediatric Drug Development: Regulatory and Practical Frameworks. Clin. Ther. 2016, 38, 574–581. [Google Scholar] [CrossRef]
- Song, L.; Jia, Y.; Ran, S.; Li, B.; Xu, J.; Huo, B.; Yin, N.; Ai, M.; Liu, Y. Current situation of pediatric clinical trials in China: Focus on trials for drug marketing application and administrative approval. BMC Pediatr. 2022, 22, 144. [Google Scholar] [CrossRef]
- Siapkara, A.; Fracasso, C.; Egger, G.F.; Rizzari, C.; Trasorras, C.S.; Athanasiou, D.; Turner, M.A.; Working Group Membership. Recommendations by the European Network of Paediatric Research at the European Medicines Agency (Enpr-EMA) Working Group on preparedness of clinical trials about paediatric medicines process. Arch. Dis. Child. 2021, 106, 1149–1154. [Google Scholar] [CrossRef]
- Subramanian, D.; Cruz, C.V.; Garcia-Bournissen, F. Systematic Review of Early Phase Pediatric Clinical Pharmacology Trials. J. Pediatr. Pharmacol. Ther. 2022, 27, 609–617. [Google Scholar] [CrossRef]
- Moore-Hepburn, C.; Rieder, M. Paediatric pharmacotherapy and drug regulation: Moving past the therapeutic orphan. Br. J. Clin. Pharmacol. 2022, 88, 4250–4257. [Google Scholar] [CrossRef]
- Guidi, B.; Parziale, A.; Nocco, L.; Maiese, A.; La Russa, R.; Di Paolo, M.; Turillazzi, E. Regulating pediatric off-label uses of medicines in the EU and USA: Challenges and potential solutions: Comparative regulation framework of off label prescriptions in pediatrics: A review. Int. J. Clin. Pharm. 2021, 44, 264–269. [Google Scholar] [CrossRef]
- Carvalho, M.L. Challenges on off label medicine use. Rev. Paul. Pediatr. 2016, 34, 1–2. [Google Scholar] [CrossRef]
- Regulation (EC) No. 1901/2006 of the European Parliament and of the Council of 12 December 2006 on Medicinal Products for Paediatric Use. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32006R1901 (accessed on 15 August 2023).
- European Commission, Directorate-General for Health and Food Safety; Marjolein, W.; Hoebert, J.; Vertvloet, M.; Puigmarti, C.M.; Damen, N.; Marchange, S.; Langedijk, J.; Lisman, J.; van Dijk, L. Study on Off-Label Use of Medicinal Products in the European Union. 2019. Available online: https://data.europa.eu/doi/10.2875/464022 (accessed on 27 August 2023).
- Tomasi, P.A.; Egger, G.F.; Pallidis, C.; Saint-Raymond, A. Enabling Development of Paediatric Medicines in Europe: 10 Years of the EU Paediatric Regulation. Pediatr. Drugs 2017, 19, 505–513. [Google Scholar] [CrossRef]
- Pediatric Research Equity Act of 2003. Public Law, 108–155, 2003. Available online: https://www.govinfo.gov/content/pkg/PLAW-108publ155/pdf/PLAW-108publ155.pdf (accessed on 12 August 2023).
- Best Pharmaceuticals for Children Act. Public Law, 107–109, 2002. Available online: https://www.congress.gov/107/plaws/publ109/PLAW-107publ109.pdf (accessed on 25 August 2023).
- Neville, K.A.; Frattarelli, D.A.; Galinkin, J.L.; Green, T.P.; Johnson, T.D.; Paul, I.M.; Anker, J.N.V.D.; American Academy of Pediatrics Committee on Drugs. Off-Label Use of Drugs in Children. Pediatrics 2014, 133, 563–567. [Google Scholar] [CrossRef]
- de Wildt, S.N.; Foeldvari, I.; Siapkara, A.; Lepola, P.; Kriström, B.; Ruggieri, L.; Eichler, I.; Egger, G.F. Off-label is not always off-evidence: Authorising paediatric indications for old medicines. Lancet Child Adolesc. Health 2023, 7, 371–372. [Google Scholar] [CrossRef]
- General Medical Council. Good Practice in Prescribing and Managing Medicines and Devices. General Medical Council (5 April 2021). 2021. Available online: https://www.gmc-uk.org/-/media/documents/prescribing-guidance-updated-english-20210405_pdf-85260533.pdf (accessed on 28 August 2023).
- Meng, M.; Zhou, Q.; Lei, W.; Tian, M.; Wang, P.; Liu, Y.; Sun, Y.; Chen, Y.; Li, Q. Recommendations on Off-Label Drug Use in Pediatric Guidelines. Front. Pharmacol. 2022, 13, 892574. [Google Scholar] [CrossRef]
- Balan, S.; Hassali, M.A.; Mak, V.S.L. Awareness, knowledge and views of off-label prescribing in children: A systematic review. Br. J. Clin. Pharmacol. 2015, 80, 1269–1280. [Google Scholar] [CrossRef]
- Tsujii, N.; Saito, T.; Izumoto, Y.; Usami, M.; Okada, T.; Negoro, H.; Iida, J. Experiences with Patient Refusal of Off-Label Prescribing of Psychotropic Medications to Children and Adolescents in Japan. J. Child Adolesc. Psychopharmacol. 2016, 26, 642–645. [Google Scholar] [CrossRef]
- Carnovale, C.; Conti, V.; Perrone, V.; Antoniazzi, S.; Pozzi, M.; Merlino, L.; Venegoni, M.; Clementi, E.; Radice, S. Paediatric drug use with focus on off-label prescriptions in Lombardy and implications for therapeutic approaches. Eur. J. Pediatr. 2013, 172, 1679–1685. [Google Scholar] [CrossRef]
- Kieran, E.A.; O’Callaghan, N.; O’Donnell, C. Unlicensed and off-label drug use in an Irish neonatal intensive care unit: A prospective cohort study. Acta Paediatr. 2014, 103, e139–e142. [Google Scholar] [CrossRef]
- Moulis, F.; Durrieu, G.; Lapeyre-Mestre, M. Off-label and unlicensed drug use in children population. Therapies 2018, 73, 135–149. [Google Scholar] [CrossRef]
- Gore, R.; Chugh, P.K.; Tripathi, C.D.; Lhamo, Y.; Gautam, S. Pediatric Off-Label and Unlicensed Drug Use and Its Implications. Curr. Clin. Pharmacol. 2017, 12, 18–25. [Google Scholar] [CrossRef]
- Magalhães, J.; Rodrigues, A.T.; Roque, F.; Figueiras, A.; Falcão, A.; Herdeiro, M.T. Use of off-label and unlicenced drugs in hospitalised paediatric patients: A systematic review. Eur. J. Clin. Pharmacol. 2015, 71, 1–13. [Google Scholar] [CrossRef]
- Balan, S.; Hassali, M.; Mak, V. Non-regulatory related factors leading to off-label prescribing in children: A concept map. Res. Soc. Adm. Pharm. 2017, 13, 1219–1221. [Google Scholar] [CrossRef]
- Knopf, H.; Wolf, I.-K.; Sarganas, G.; Zhuang, W.; Rascher, W.; Neubert, A. Off-label medicine use in children and adolescents: Results of a population-based study in Germany. BMC Public Health 2013, 13, 631. [Google Scholar] [CrossRef]
- Ribeiro, M.; Jorge, A.; Macedo, A.F. Off-label drug prescribing in a Portuguese Paediatric Emergency Unit. Int. J. Clin. Pharm. 2012, 35, 30–36. [Google Scholar] [CrossRef]
- Langerová, P.; Vrtal, J.; Urbánek, K. Incidence of unlicensed and off-label prescription in children. Ital. J. Pediatr. 2014, 40, 12. [Google Scholar] [CrossRef]
- Bhadiyadara, S.N.; Rana, D.A.; Malhotra, S.D.; Patel, V.J. Off-label and Unlicensed Drug Use in Paediatric Outpatient Department—A Prospective Study at a Tertiary Care Teaching Hospital. J. Young Pharm. 2015, 7, 164. [Google Scholar] [CrossRef]
- Oshikoya, K.A.; Oreagba, I.A.; Godman, B.; Fadare, J.; Orubu, S.; Massele, A.; Senbanjo, I.O. Off-label prescribing for children with chronic diseases in Nigeria; findings and implications. Expert Opin. Drug Saf. 2017, 16, 981–988. [Google Scholar] [CrossRef]
- Lindell-Osuagwu, L.; Hakkarainen, M.; Sepponen, K.; Vainio, K.; Naaranlahti, T.; Kokki, H. Prescribing for off-label use and unauthorized medicines in three paediatric wards in Finland, the status before and after the European Union Paediatric Regulation. J. Clin. Pharm. Ther. 2014, 39, 144–153. [Google Scholar] [CrossRef]
- Teigen, A.; Wang, S.; Truong, B.T.; Bjerknes, K. Off-label and unlicensed medicines to hospitalised children in Norway. J. Pharm. Pharmacol. 2017, 69, 432–438. [Google Scholar] [CrossRef]
- Kimland, E.; Nydert, P.; Odlind, V.; Böttiger, Y.; Lindemalm, S. Paediatric drug use with focus on off-label prescriptions at Swedish hospitals—A nationwide study. Acta Paediatr. 2012, 101, 772–778. [Google Scholar] [CrossRef]
- Palčevski, G.; Skočibušić, N.; Vlahović-Palčevski, V. Unlicensed and off-label drug use in hospitalized children in Croatia: A cross-sectional survey. Eur. J. Clin. Pharmacol. 2012, 68, 1073–1077. [Google Scholar] [CrossRef]
- Slažneva, J.; Kovács, L.; Kuželová, M. Off-label drug use among hospitalized children: Identifying extent and nature. Eur. Pharm. J. 2012, 59, 48–54. [Google Scholar] [CrossRef]
- Maltz, L.A.; Klugman, D.; Spaeder, M.C.; Wessel, D.L. Off-Label Drug Use in a Single-Center Pediatric Cardiac Intensive Care Unit. World J. Pediatr. Congenit. Heart Surg. 2013, 4, 262–266. [Google Scholar] [CrossRef]
- Corny, J.; Bailey, B.; Lebel, D.; Bussières, J.-F. Unlicensed and off-label drug use in paediatrics in a mother-child tertiary care hospital. Paediatr. Child Health 2016, 21, 83–87. [Google Scholar] [CrossRef]
- Czarniak, P.; Bint, L.; Favié, L.; Parsons, R.; Hughes, J.; Sunderland, B. Clinical Setting Influences Off-Label and Unlicensed Prescribing in a Paediatric Teaching Hospital. PLoS ONE 2015, 10, e0120630. [Google Scholar] [CrossRef]
- Taylor, D.M.; Joffe, P.; Taylor, S.E.; Jones, A.; Cheek, J.A.; Craig, S.S.; Graudins, A.; Dhir, R.; Krieser, D.; Babl, F.E. Off-label and unlicenced medicine administration to paediatric emergency department patients. Emerg. Med. Australas. 2015, 27, 440–446. [Google Scholar] [CrossRef]
- Landwehr, C.; Richardson, J.; Bint, L.; Parsons, R.; Sunderland, B.; Czarniak, P. Cross-sectional survey of off-label and unlicensed prescribing for inpatients at a paediatric teaching hospital in Western Australia. PLoS ONE 2019, 14, e0210237. [Google Scholar] [CrossRef]
- Lee, J.L.; Redzuan, A.M.; Shah, N.M. Unlicensed and off-label use of medicines in children admitted to the intensive care units of a hospital in Malaysia. Int. J. Clin. Pharm. 2013, 35, 1025–1029. [Google Scholar] [CrossRef]
- Tukayo, B.L.A.; Sunderland, B.; Parsons, R.; Czarniak, P. High prevalence of off-label and unlicensed paediatric prescribing in a hospital in Indonesia during the period Aug.—Oct. 2014. PLoS ONE 2020, 15, e0227687. [Google Scholar] [CrossRef]
- Mohamad, N.F.; Ali, A.M.; Shah, N.M. Respiratory drugs prescribed off-label among children in the outpatient clinics of a hospital in Malaysia. Int. J. Clin. Pharm. 2014, 37, 127–132. [Google Scholar] [CrossRef]
- Jobanputra, N.; Save, S.U.; Bavdekar, S.B. Off-label and unlicensed drug use in children admitted to Pediatric Intensive Care Units (PICU). Int. J. Risk Saf. Med. 2015, 27, 113–121. [Google Scholar] [CrossRef]
- Ballard, C.D.; Peterson, G.M.; Thompson, A.J.; Beggs, S.A. Off-label use of medicines in paediatric inpatients at an Australian teaching hospital. J. Paediatr. Child Health 2013, 49, 38–42. [Google Scholar] [CrossRef]
- Ellul, I.C.; Grech, V. Off-label and unlicensed paediatric prescribing in a community setting: A prospective longitudinal cohort study in Malta. Paediatr. Int. Child Health 2014, 34, 12–18. [Google Scholar] [CrossRef]
- Abdulah, R.; Khairinisa, M.A.; Pratiwi, A.A.; Barliana, M.I.; Pradipta, I.S.; Halimah, E.; Diantini, A.; Lestari, K. Off-label paediatric drug use in an Indonesian community setting. J. Clin. Pharm. Ther. 2015, 40, 409–412. [Google Scholar] [CrossRef]
- Dornelles, A.D.; Calegari, L.H.; de Souza, L.; Ebone, P.; Tonelli, T.S.; Carvalho, C.G. The Unlicensed and Off-label Prescription of Medications in General Paediatric Ward: An Observational Study. Curr. Pediatr. Rev. 2019, 15, 62–66. [Google Scholar] [CrossRef]
- Conroy, S.; Choonara, I.; Impicciatore, P.; Mohn, A.; Arnell, H.; Rane, A.; Knoeppel, C.; Seyberth, H.; Pandolfini, C.; Raffaelli, M.P.; et al. Survey of unlicensed and off label drug use in paediatric wards in European countries. European Network for Drug Investigation in Children. BMJ 2000, 320, 79–82. [Google Scholar] [CrossRef]
- Schaffer, A.L.; Bruno, C.; Buckley, N.A.; Cairns, R.; Litchfield, M.; Paget, S.; Zoega, H.; Nassar, N.; Pearson, S. Prescribed medicine use and extent of off-label use according to age in a nationwide sample of Australian children. Paediatr. Périnat. Epidemiol. 2022, 36, 726–737. [Google Scholar] [CrossRef]
- Luedtke, K.E.; Buck, M.L. Evaluation of Off-label Prescribing at a Children’s Rehabilitation Center. J. Pediatr. Pharmacol. Ther. 2014, 19, 296–301. [Google Scholar] [CrossRef]
- Gonçalves, M.G.; Heineck, I. Frequency of prescriptions of off-label drugs and drugs not approved for pediatric use in primary health care in a southern municipality of Brazil. Rev. Paul Pediatr. 2016, 34, 11–17. [Google Scholar] [CrossRef]
- Dos Santos, L.; Heineck, I. Drug utilization study in pediatric prescriptions of a university hospital in southern brazil: Off-label, unlicensed and high-alert medications. Farm. Hosp. 2012, 36, 180–186. [Google Scholar] [CrossRef]
- Pereira Gomes, V.; Melo da Silva, K.; Oliveira Chagas, S.; dos Santos Magalhães, I.R. Off-label and unlicensed utilization of drugs in a Brazilian pediatric hospital. Farm. Hosp. 2015, 39, 176–180. [Google Scholar] [CrossRef]
- Aamir, M.; Khan, J.A.; Shakeel, F.; Asim, S.M. Unlicensed and off-label use of drugs in pediatric surgical units at tertiary care hospitals of Pakistan. Int. J. Clin. Pharm. 2017, 39, 860–866. [Google Scholar] [CrossRef]
- Saito, J.; Nadatani, N.; Setoguchi, M.; Nakao, M.; Kimura, H.; Sameshima, M.; Kobayashi, K.; Matsumoto, H.; Yoshikawa, N.; Yokoyama, T.; et al. Potentially harmful excipients in neonatal medications: A multicenter nationwide observational study in Japan. J. Pharm. Health Care Sci. 2021, 7, 23. [Google Scholar] [CrossRef]
- Flint, R.B.; van Beek, F.; Andriessen, P.; Zimmermann, L.J.; Liem, K.D.; Reiss, I.K.; de Groot, R.; Tibboel, D.; Burger, D.M.; Simons, S.H.; et al. Large differences in neonatal drug use between NICUs are common practice: Time for consensus? Br. J. Clin. Pharmacol. 2018, 84, 1313–1323. [Google Scholar] [CrossRef]
- Alonso, A.S.; Avila-Alvarez, A.; Eiriz, M.C.; Roca, C.M.; Gómez, P.Y.; López, A.C.; Trisac, J.L.F.; Díaz, S.P. Use of off-label drugs in neonatal intensive care. Anal. Pediatr. 2019, 91, 237–243. [Google Scholar] [CrossRef]
- Schweigertova, J.; Durisova, A.; Dolnikova, D.; Ondriasova, E.; Balazova, M.; Slezakova, V.; Kuzelova, M. Off-label and unlicensed use of medicinal products in the neonatal setting in the Slovak Republic. Pediatr. Int. 2016, 58, 126–131. [Google Scholar] [CrossRef]
- Silva, J.; Flor-De-Lima, F.; Soares, H.; Guimarães, H. Off-Label and Unlicensed Drug Use in Neonatology: Reality in a Portuguese University Hospital. Acta Med. Portug. 2015, 28, 297–306. [Google Scholar] [CrossRef]
- Riou, S.; Plaisant, F.; Boulch, D.M.; Kassai, B.; Claris, O.; Nguyen, K.-A. Unlicensed and off-label drug use: A prospective study in French NICU. Acta Paediatr. 2015, 104, e228–e231. [Google Scholar] [CrossRef]
- Cuzzolin, L.; Agostino, R. Off-label and unlicensed drug treatments in Neonatal Intensive Care Units: An Italian multicentre study. Eur. J. Clin. Pharmacol. 2016, 72, 117–123. [Google Scholar] [CrossRef]
- Carvalho, C.G.; Ribeiro, M.R.; Bonilha, M.M.; Fernandes, M., Jr.; Procianoy, R.S.; Silveira, R.C. Use of off-label and unlicensed drugs in the neonatal intensive care unit and its association with severity scores. J. Pediatr. 2012, 88, 465–470. [Google Scholar] [CrossRef]
- Costa, H.T.M.d.L.; Costa, T.X.; Martins, R.R.; Oliveira, A.G. Use of off-label and unlicensed medicines in neonatal intensive care. PLoS ONE 2018, 13, e0204427. [Google Scholar] [CrossRef]
- Vieira, V.C.; Costa, R.S.; Lima, R.C.G.; Queiroz, D.B.; de Medeiros, D.S. Prescription of off-label and unlicensed drugs for preterm infants in a neonatal intensive care unit. Rev. Brasil. Ter. Intens. 2021, 33, 266–275. [Google Scholar] [CrossRef]
- Jain, S.; Saini, S.S.; Chawla, D.; Kumar, P.; Dhir, S. Off-label use of drugs in neonatal intensive care units. Indian Pediatr. 2014, 51, 644–646. [Google Scholar] [CrossRef]
- Chauthankar, S.A.; Marathe, P.A.; Potey, A.V.; Nanavati, R.N. Drug utilization in neonatal intensive care unit of a tertiary-care hospital in Mumbai, India. Indian Pediatr. 2017, 54, 931–934. [Google Scholar] [CrossRef]
- Aamir, M.; Khan, J.A.; Shakeel, F.; Shareef, R.; Shah, N. Drug utilization in neonatal setting of Pakistan: Focus on unlicensed and off label drug prescribing. BMC Pediatr. 2018, 18, 242. [Google Scholar] [CrossRef]
- Nir-Neuman, H.; Abu-Kishk, I.; Toledano, M.; Heyman, E.; Ziv-Baran, T.; Berkovitch, M. Unlicensed and Off-Label Medication Use in Pediatric and Neonatal Intensive Care Units: No Change Over a Decade. Adv. Ther. 2018, 35, 1122–1132. [Google Scholar] [CrossRef]
- Lindell-Osuagwu, L.; Korhonen, M.J.; Saano, S.; Helin-Tanninen, M.; Naaranlahti, T.; Kokki, H. Off-label and unlicensed drug prescribing in three paediatric wards in Finland and review of the international literature. J. Clin. Pharm. Ther. 2009, 34, 277–287. [Google Scholar] [CrossRef]
- Belayneh, A.; Abatneh, E.; Abebe, D.; Getachew, M.; Kebede, B.; Dessie, B. Off-label medication use in pediatrics and associated factors at public hospitals in east Gojjam zone, Ethiopia. SAGE Open Med. 2022, 10, 20503121221096534. [Google Scholar] [CrossRef]
- Czaja, A.S.; Reiter, P.D.; Schultz, M.L.; Valuck, R.J. Patterns of Off-Label Prescribing in the Pediatric Intensive Care Unit and Prioritizing Future Research. J. Pediatr. Pharmacol. Ther. 2015, 20, 186–196. [Google Scholar] [CrossRef]
- Blanco-Reina, E.; Medina-Claros, A.; Vega-Jiménez, M.; Ocaña-Riola, R.; Márquez-Romero, E.; Ruiz-Extremera, Á. Drug utilization pattern in children and off-label use of medicines in a pediatric intensive care unit. Med. Intensiv. 2015, 40, 1–8. [Google Scholar] [CrossRef]
- Arocas Casañ, V.; Cabezuelo Escribano, B.; Garrido-Corro, B.; De la Cruz Murie, P.; Blázquez Álvarez, M.J.; De la Rubia Nieto, M.A. Off-label and unlicensed drug use in a Spanish Neonatal Intensive Care Unit. Farm. Hosp. 2017, 41, 371–381. [Google Scholar] [CrossRef]
- Oishi, K.; Inage, E.; Kojima, M.; Yamada, H.; Tanaka, Y.; Yoneyama, T.; Yamazaki, S.; Honjo, A.; Baba, Y.; Kudo, T.; et al. Evidence of off-label inhalation therapy on pediatric asthma practice in Japan. Pediatr. Int. 2023, 65, e15595. [Google Scholar] [CrossRef]
- Smeets, N.J.L.; Raaijmakers, L.P.M.; van der Zanden, T.M.; Male, C.; de Wildt, S.N. Guiding future paediatric drug studies based on existing pharmacokinetic and efficacy data: Cardiovascular drugs as a proof of concept. Br. J. Clin. Pharmacol. 2023, 89, 2888–2901. [Google Scholar] [CrossRef]
- Zodidi, M. Off Label and Unlicensed Drug Use in Neonatal Wards (Excluding Neonatal ICU) at Tygerberg Children’s Hospital (TBH). Master’s Thesis, (MMed)-Stellenbosch University, Stellenbosch, South Africa, December 2019. Available online: http://hdl.handle.net/10019.1/106987 (accessed on 20 August 2023).
- Balan, S.; Hassali, M.A.A.; Mak, V.S.L. Two decades of off-label prescribing in children: A literature review. World J. Pediatr. 2018, 14, 528–540. [Google Scholar] [CrossRef]
- Le Jeunne, C.; Billon, N.; Dandon, A.; Berdaï, D.; Adgibi, Y.; Bergmann, J.-F.; Bordet, R.; Carpentier, A.; Cohn, E.; Courcier, S.; et al. Off-label Prescriptions: How to Identify Them, Frame Them, Announce Them and Monitor Them in Practice? Therapies 2013, 68, 233–239. [Google Scholar] [CrossRef]
- Schrier, L.; Hadjipanayis, A.; Stiris, T.; Ross-Russell, R.I.; Valiulis, A.; Turner, M.A.; Zhao, W.; De Cock, P.; De Wildt, S.N.; Allegaert, K.; et al. Off-label use of medicines in neonates, infants, children, and adolescents: A joint policy statement by the European Academy of Paediatrics and the European society for Developmental Perinatal and Pediatric Pharmacology. Eur. J. Pediatr. 2020, 179, 839–847. [Google Scholar] [CrossRef]
- van der Zanden, T.M.; Mooij, M.G.; Vet, N.J.; Neubert, A.; Rascher, W.; Lagler, F.B.; Male, C.; Grytli, H.; Halvorsen, T.; de Hoog, M.; et al. Benefit-Risk Assessment of Off-Label Drug Use in Children: The Bravo Framework. Clin. Pharmacol. Ther. 2021, 110, 952–965. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Kalra, A.; Goindi, S. Issues Impacting Therapeutic Outcomes in Pediatric Patients: An Overview. Curr. Pediatr. Rev. 2014, 10, 184–193. [Google Scholar] [CrossRef]
- Ivanovska, V.; Rademaker, C.M.; van Dijk, L.; Mantel-Teeuwisse, A.K. Pediatric Drug Formulations: A Review of Challenges and Progress. Pediatrics 2014, 134, 361–372. [Google Scholar] [CrossRef]
- Richey, R.H.; Hughes, C.; Craig, J.V.; Shah, U.U.; Ford, J.L.; Barker, C.E.; Peak, M.; Nunn, A.J.; Turner, M.A. A systematic review of the use of dosage form manipulation to obtain required doses to inform use of manipulation in paediatric practice. Int. J. Pharm. 2017, 518, 155–166. [Google Scholar] [CrossRef]
- Greenberg, R.G.; McCune, S.; Attar, S.; Hovinga, C.; Stewart, B.; Lacaze-Masmonteil, T. Pediatric Clinical Research Networks: Role in Accelerating Development of Therapeutics in Children. Ther. Innov. Regul. Sci. 2022, 56, 934–947. [Google Scholar] [CrossRef]
- Green, D.J.; Zineh, I.; Burckart, G.J. Pediatric Drug Development: Outlook for Science-Based Innovation. Clin. Pharmacol. Ther. 2018, 103, 376–378. [Google Scholar] [CrossRef]
- Samuels, S.; Park, K.; Bhatt-Mehta, V.; Sun, H.; Mulugeta, Y.; Yao, L.; Green, D.J.; Burckart, G.J. Pediatric Efficacy Extrapolation in Drug Development Submitted to the US Food and Drug Administration 2015–2020. J. Clin. Pharmacol. 2023, 63, 307–313. [Google Scholar] [CrossRef]
- Dunn, A.; Jung, D.; Bollinger, L.L.; Krams, M.; Smith, B.P.; Gobburu, J.V.S. Accelerating the Availability of Medications to Pediatric Patients by Optimizing the Use of Extrapolation of Efficacy. Ther. Innov. Regul. Sci. 2022, 56, 873–882. [Google Scholar] [CrossRef]
- Ward, R.M.; Benjamin, D.K.; Davis, J.M.; Gorman, R.L.; Kauffman, R.; Kearns, G.L.; Murphy, M.D.; Sherwin, C.M. The Need for Pediatric Drug Development. J. Pediatr. 2018, 192, 13–21. [Google Scholar] [CrossRef]
- State of Paediatric Medicines in the EU. Available online: https://health.ec.europa.eu/system/files/2017-11/2017_childrensmedicines_report_en_0.pdf (accessed on 28 August 2023).
- Boosting the Development of Medicines for Children. Closing Report of the European Medicines Agency and European Commission (DG Health and Food Safety) Action Plan on Paediatrics. EMA/635567/2022. Available online: https://www.ema.europa.eu/en/documents/report/boosting-development-medicines-children-closing-report-european-medicines-agency-european-commission_en.pdf (accessed on 26 August 2023).
- Bellis, J.R.; Kirkham, J.J.; Nunn, A.J.; Pirmohamed, M. Adverse drug reactions and off-label and unlicensed medicines in children: A prospective cohort study of unplanned admissions to a paediatric hospital. Br. J. Clin. Pharmacol. 2014, 77, 545–553. [Google Scholar] [CrossRef]
- Saiyed, M.M.; Lalwani, T.; Rana, D. Is off-label use a risk factor for adverse drug reactions in pediatric patients? A prospective study in an Indian tertiary care hospital. Int. J. Risk Saf. Med. 2015, 27, 45–53. [Google Scholar] [CrossRef]
- Kaguelidou, F.; Ouèdraogo, M.; Treluyer, J.-M.; Le Jeunne, C.; Annereau, M.; Blanc, P.; Bureau, S.; Ducassou, S.; Fiquet, B.; Flamein, F.; et al. Paediatric drug development and evaluation: Existing challenges and recommendations. Therapie 2023, 78, 105–114. [Google Scholar] [CrossRef]
- Yamashiro, Y.; Martin, J.; Gazarian, M.; Kling, S.; Nakamura, H.; Matsui, A.; Cucchiara, S.; Aloi, M.; Wynn, E.L.; Mulberg, A.E. Drug Development: The use of unlicensed/off-label medicines in pediatrics. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 506–510. [Google Scholar] [CrossRef]
- Costa, H.T.M.L.; Florencio, A.P.; Bezerra, P.K.D.V.; Cavalcanti, J.E.C.; Costa, T.X.; Fernandes, F.E.M.; Martins, R.R. Comparative assessment of off-label and unlicensed drug prescription in neonatal intensive care: FDA versus Brazilian guidelines. An. Pediatr. 2021, 94, 153–160. [Google Scholar] [CrossRef]


{kind=link}
| Country | % Off-Label Prescriptions (Total Prescriptions) | Type of Study (Number of Patients and Age) | Studied Period |
|---|---|---|---|
| Italy [89] | 3.3% (4,027,119) | Retrospective (n = 1,708,755 non-clinical setting; 0–18 years) | 12 months (January–December 2011) |
| Finland [100] | 71% (1054) | Retrospective (n = 123; inpatients; 0–18 years) | 0.5 months (April–May 2011) |
| Norway [101] | 44% (930) | Prospective cross-sectional (n = 400 inpatients; 0–17 years) | 6 months (September–October 2013 and (September–December 2014) |
| Sweden [102] | 41% (11 294) | Prospective (n = 2947 inpatients; 0–18 years) | 4 days (2 days in May and 2 days in October 2008) |
| Portugal [96] | 28.1% (724) | Retrospective descriptive (n = 700 outpatient; 0–18 years) | 12 months (January–October 2010) |
| Croatia [103] | 19.7% (1643) | Prospective (n = 531 inpatients; 0–18 years) | 12 months (May 2010–April 2011) |
| Slovakia [104] | 15.7% (267) | Prospective (n = 68 inpatients; 2–18 years) | 1 month (February–March 2011) |
| USA [105] | 36% (1090) | Retrospective cohort (n = 82 inpatients; 0–18 years) | 3 months (June 2008–August 2008) |
| Canada [106] | 38.2% (2145) | Retrospective cross-sectional (n = 308 inpatients; 0–18 years) | A day (5 March 2014) |
| Australia [107] | 25.7% (2654) | Retrospective (n = 699 ED *, in- and outpatients; 0–18 years) | 24 months (January–December 2008) |
| Australia [108] | 30.5% (6786) | Retrospective observational (n = 3343 ED patients; 0–17 years) | 12 months (July 2011–June 2012) |
| Australia [109] | 53.9% (1160) | Retrospective cross-sectional study (n = 190 inpatients; 0–18 years) | 1 month (June 2013) |
| Malaysia [110] | 34.1% (1295) | Prospective (n = 194 inpatients; 28 days–18 years) | 3 months (April–June 2012) |
| Indonesia [111] | 71.5% (1961) | Retrospective cross-sectional (n = 200 inpatients; 1 month–18 years) | 3 months (August–October 2014) |
| Malaysia [112] | 35.6% (508) | Prospective (n = 220 outpatients; 1 month–17 years) | 6 months (July 2011–December 2011) |
| Nigeria [99] | 7.7% (1746) | Retrospective descriptive (n = 477 inpatients; 0–16 years) | 12 months (January–October 2015) |
| Country | % Off-Label Prescriptions (Total Prescriptions) | Type of Study (Number of Patients and Age) | Studied Period |
|---|---|---|---|
| Czech Republic [97] | 9.02% (8559) | Prospective observational (n = 4282 outpatients; 0–15 years) | 6 months (January–June 2012) |
| Slovakia [104] | 21% (206) | Prospective (n = 49 inpatients; 0–6 years) | 1 month (February–March 2011) |
| USA [120] | 57% (240) | Prospective observational (n = 40 inpatients; 3 weeks–15 years) | 4.5 months (November 2011–April 2012) |
| Brazil [121] | 31.7% (731) | Retrospective cross-sectional (n = 705 outpatients; 0–12 years) | 5 months (August–December 2012 |
| Brazil [122] | 39% (342) | Prospective cross-sectional (n = 342 inpatients; 0–14 years) | 3 months (November 2007–January 2008) |
| Brazil [123] | 77.8% (1158) | Prospective (n = 320 inpatients; 2–14 years) | 6 months (September 2012–February 2013 |
| Brazil [117] | 45% (1328) | Prospective observational (n = 157 inpatients; 1 month–12 years) | A week period Phase 1 (August 2014) Phase 2 (January 2015) |
| Australia [114] | 31.8% (887) | Retrospective (n = 300 inpatients; 0–12 years) Group 1—150 consecutive patients Group 2—150 consecutive patients | 2 months Group 1 (1 July 2009–5 August 2009). Group 2 (1 January 2010–22 February 2010) |
| India [113] | 41.25% (1789) | Prospective observational (n = 482 PICU patients; 1 month–12 years) | 12 months (April 2012–March 2013) |
| India [98] | 10.1% (405) | Prospective cross-sectional (n = 170 outpatients; 15 days–12 years) | 2 months (July 2012–August 2012) |
| Indonesia [116] | 18.6% (4936) | Retrospective population-based (n = 4936 outpatients; 0–5 years) | 12 months (January–December 2012) |
| Pakistan [124] | 48.6% (3168) | Prospective, observational (n = 895 inpatients; 1 month–15 years) | 12 months (March 2014–February 2015) |
| Malta [115] | 51.7% (209) | Prospective (n = 209 outpatients; 0–14 years) | A month period Phase 1 (September 2006) Phase 2 (January 2007) |
| Country | % Off-Label Prescriptions (Total Prescriptions) | Type of Study (Number of Patients and Age) | Studied Period |
|---|---|---|---|
| Spain [127] | 22.5% (564) | A Prospective, observational study (n = 84 NICU * patients) | 6 months (April–September 2018) |
| Slovakia [128] | 43% (962) | Prospective cross-sectional (n = 202 NICU patients) | 6 months (April–September 2012) |
| Portugal [129] | 52.7% (1011) | Retrospective cross-sectional study (n = 218 NICU patients) | 6 months (January–June 2013) |
| France [130] | 59.5% (8891) | Prospective, observational (n = 910 NICU patients) | 12 months (January–December 2012) |
| Italy [131] | 59% (720) | Prospective (n = 220 NICU patients) | 1-day survey (May–July 2014) |
| Ireland [90] | 94% (900) | Prospective (n = 110 NICU patients) | 2 months (February–March 2012) |
| Brazil [132] | 27.7% (318) | Observational cohort study (n = 61 NICU patients) | 1.5 months (July–August 2011) |
| Brazil [133] | 49.3% (3935) | Prospective cohort study (n = 220 NICU patients) | 12 months (August 2015–July 2016) |
| Brazil [134] | 79.0% (16,143) | A nonconcurrent, hospital-based cohort study (n = 592 NICU preterm patients) | 24 months (January 2016–December 2017) |
| India [135] | 50% (568) | Prospective (n = 156 NICU patients) | 3 months (June–August 2009) |
| India [136] | 12.3% (2642) | Prospective descriptive (n = 460 NICU patients) | 9 months (July 2014–March 2015) |
| Pakistan [137] | 52.14% (3448) | Prospective, observational (n = 1300 inpatients) | 12 months (May 2014–April 2015) |
| Israel [138] | 64.8% (1064) | Prospective (n = 134 NICU patients) | 2 months (December 2015–January 2016) |
| Reason for Off-Label Determination | Prevalence of the Reason (%) | Reference |
|---|---|---|
| Dosage | 25.7–40–52–61.29 | [129,136,137,138] |
| Indication | 13.68–36 | [137,138] |
| Frequency | 32 | [138] |
| Age | 10.79–15–44.8 | [130,137,138] |
| Route of administration | 14 | [138] |
| Combined (more than one reason) | 0.11–8.12–15 | [136,137,138] |
| Contraindication | 13.8 | [128] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petkova, V.; Georgieva, D.; Dimitrov, M.; Nikolova, I. Off-Label Prescribing in Pediatric Population—Literature Review for 2012–2022. Pharmaceutics 2023, 15, 2652. https://doi.org/10.3390/pharmaceutics15122652
Petkova V, Georgieva D, Dimitrov M, Nikolova I. Off-Label Prescribing in Pediatric Population—Literature Review for 2012–2022. Pharmaceutics. 2023; 15(12):2652. https://doi.org/10.3390/pharmaceutics15122652
Chicago/Turabian StylePetkova, Valentina, Dilyana Georgieva, Milen Dimitrov, and Irina Nikolova. 2023. "Off-Label Prescribing in Pediatric Population—Literature Review for 2012–2022" Pharmaceutics 15, no. 12: 2652. https://doi.org/10.3390/pharmaceutics15122652
APA StylePetkova, V., Georgieva, D., Dimitrov, M., & Nikolova, I. (2023). Off-Label Prescribing in Pediatric Population—Literature Review for 2012–2022. Pharmaceutics, 15(12), 2652. https://doi.org/10.3390/pharmaceutics15122652