
An Insight on the Possible Association between Inflammatory Bowel Disease and Biologic Therapy with IL-17 Inhibitors in Psoriasis Patients


 , ,
, ,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
3. Influence of Biologic Therapy on the Course of Inflammatory Bowel Disease
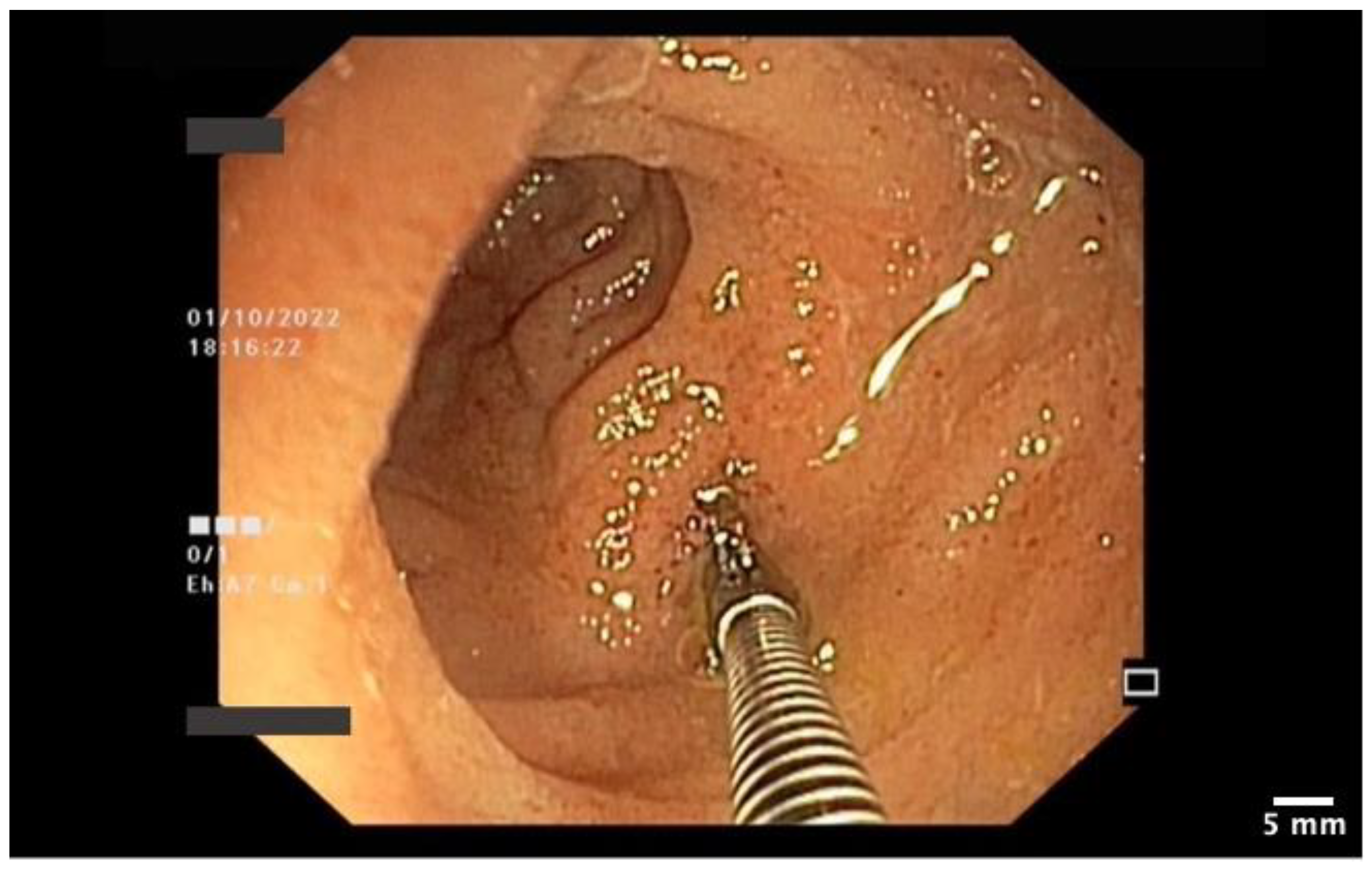
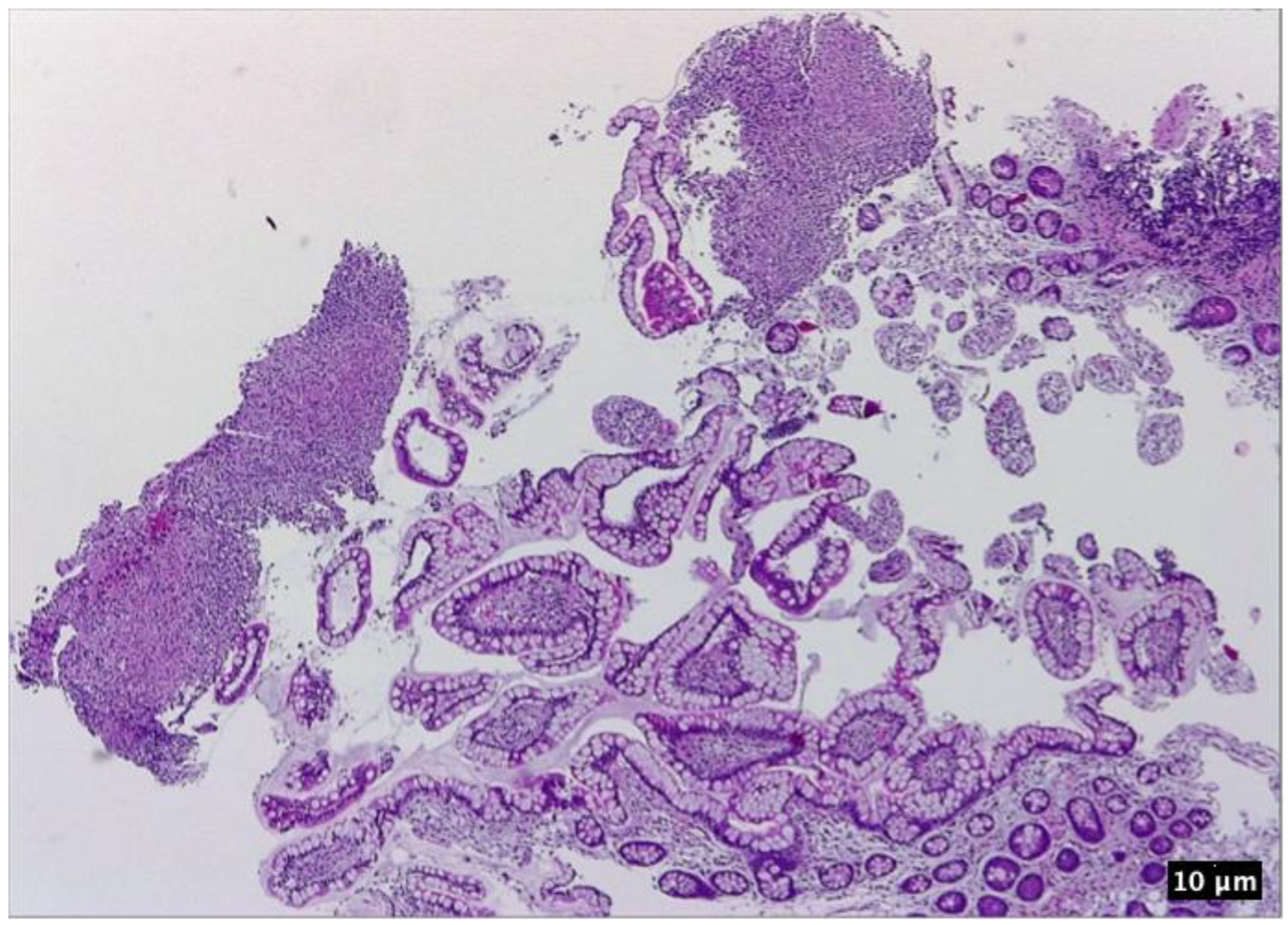
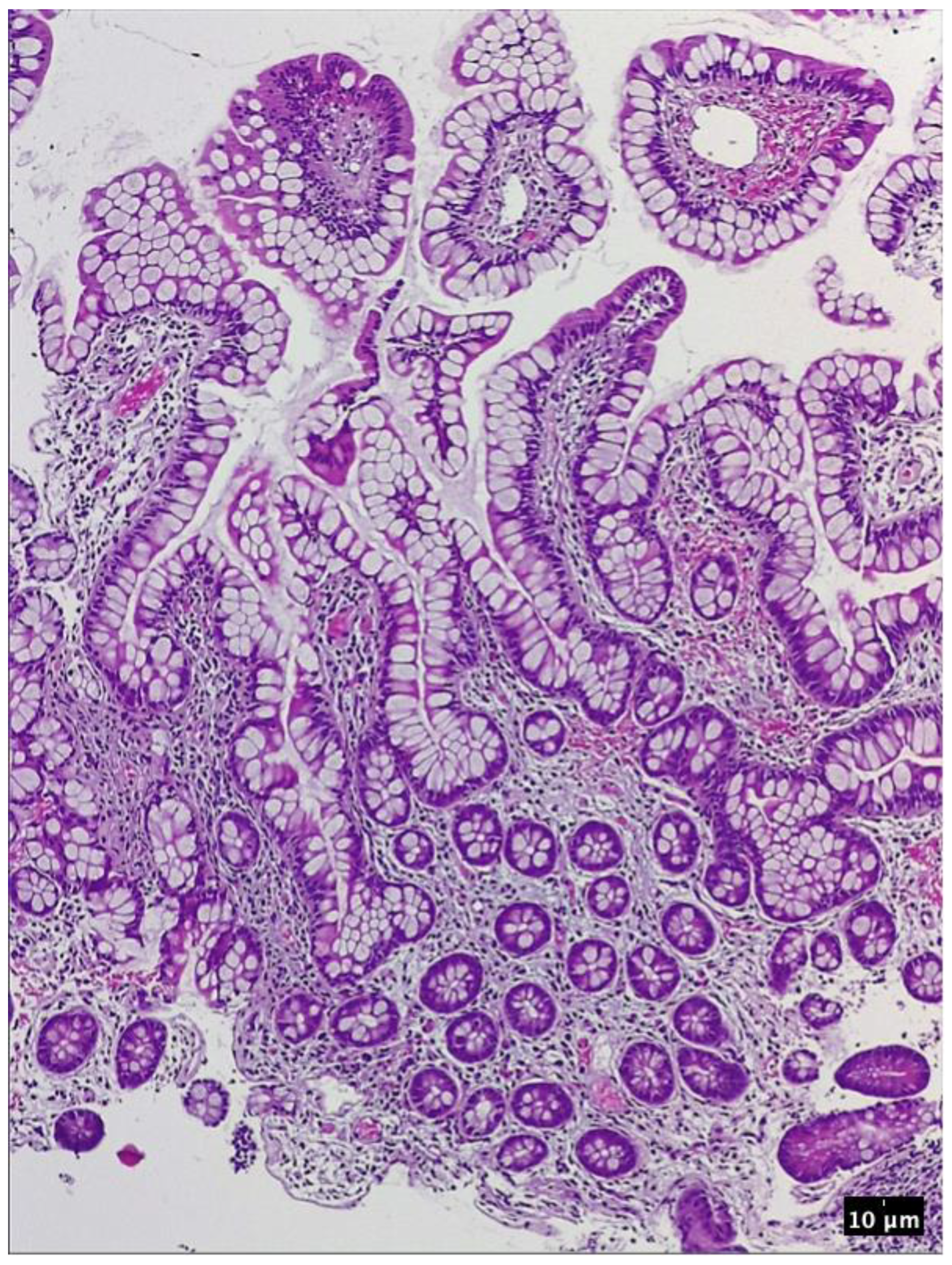
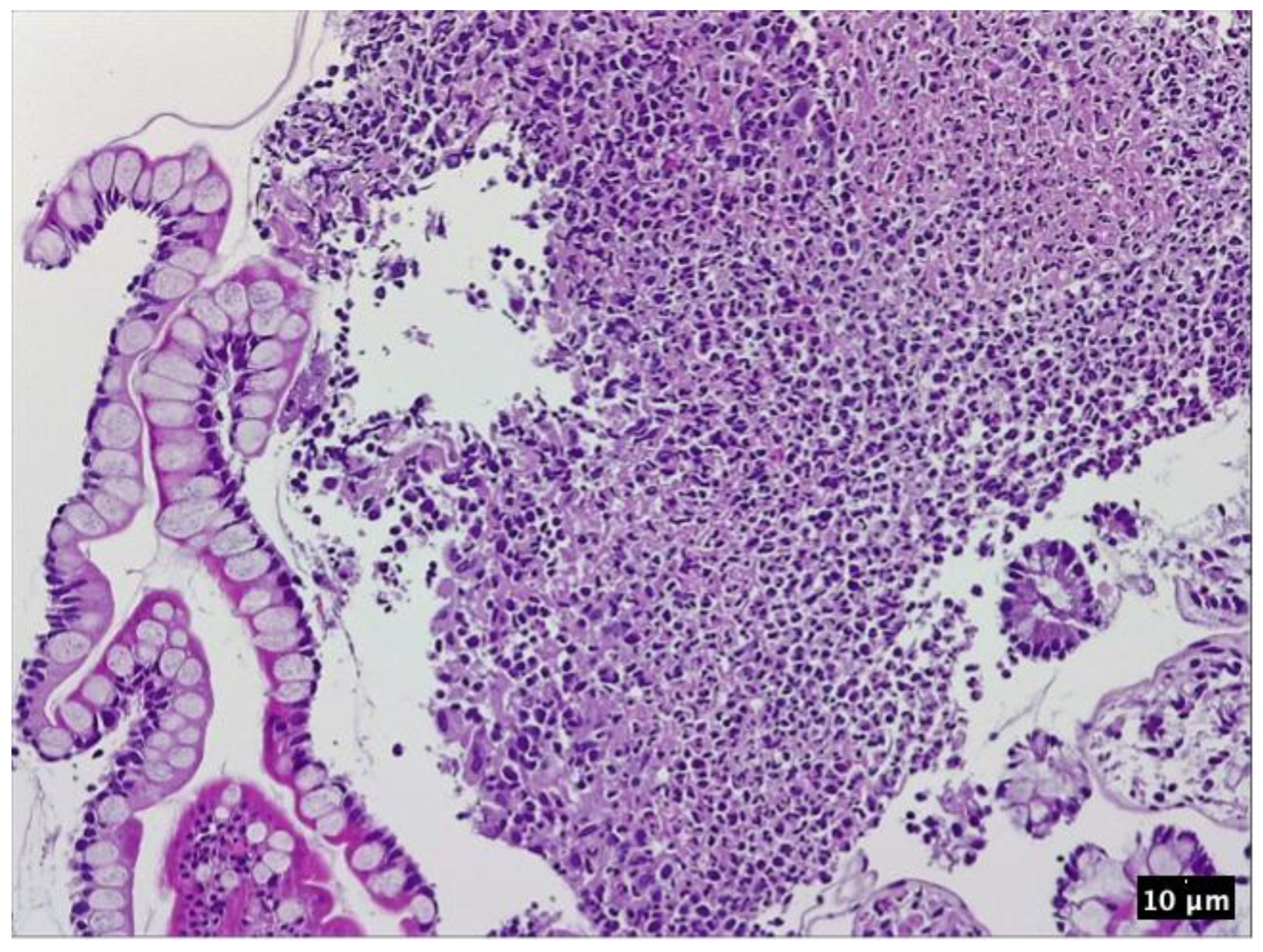
4. Case Presentation
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HLA | Human leukocyte antigen |
| DNA | Dezoxyribonulceic acid |
| TNF-alpha | Tumor necrosis factor-alpha |
| IL | Interleukin |
| VEGF | Vascular endothelial growth factor |
| PDE4 | Phosphodiesterase 4 |
| CD | Crohn’s disease |
| UC | Ulcerative colitis |
| IBD | Inflammatory bowel disease |
| OR | Odds ratio |
| GHAS | Global histology activity scores |
| mcg | microgram |
| HE | Hematoxilin and eosin |
| ANCA | Anti-neutrophil cytoplasmic antibodies |
References
- Boehncke, W.H.; Schön, M.P. Psoriasis. Lancet 2015, 386, 983–994. [Google Scholar] [CrossRef]
- Mahil, S.K.; Capon, F.; Barker, J.N. Update on psoriasis immunopathogenesis and targeted immunotherapy. Semin. Immunopathol. 2016, 38, 11–27. [Google Scholar] [CrossRef] [PubMed]
- Capon, F.; Munro, M.; Barker, J.; Trembath, R. Searching for the major histocompatibility complex psoriasis susceptibility gene. J. Investig. Dermatol. 2002, 118, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Gilliet, M.; Lande, R. Antimicrobial peptides and self-DNA in autoimmune skin inflammation. Curr. Opin. Immunol. 2008, 20, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Lande, R.; Botti, E.; Jandus, C.; Dojcinovic, D.; Fanelli, G.; Conrad, C.; Chamilos, G.; Feldmeyer, L.; Marinari, B.; Chon, S.; et al. The antimicrobial peptide LL37 is a T-cell autoantigen in psoriasis. Nat. Commun. 2014, 5, 5621. [Google Scholar] [CrossRef] [PubMed]
- Bergboer, J.G.M.; Zeeuwen, P.; Schalkwijk, J. Genetics of psoriasis: Evidence for epistatic interaction between skin barrier abnormalities and immune deviation. J. Investig. Dermatol. 2012, 132, 2320–2331. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.; Chang, S.H.; Martinez, G.J.; Yang, X.O.; Nurieva, R.; Kang, H.S.; Ma, L.; Watowich, S.S.; Jetten, A.M.; Tian, Q.; et al. Critical regulation of early Th17 cell differentiation by interleukin-1 signaling. Immunity 2009, 30, 576–587. [Google Scholar] [CrossRef]
- Xia, Y.P.; Li, B.; Hylton, D.; Detmar, M.; Yancopoulos, G.D.; Rudge, J.S. Transgenic delivery of VEGF to mouse skin leads to an inflammatory condition resembling human psoriasis. Blood 2003, 102, 161–168. [Google Scholar] [CrossRef]
- Zaba, L.C.; Cardinale, I.; Gilleaudeau, P.; Sullivan-Whalen, M.; Suárez-Fariñas, M.; Fuentes-Duculan, J.; Novitskaya, I.; Khatcherian, A.; Bluth, M.J.; Lowes, M.A.; et al. Amelioration of epidermal hyperplasia by TNF inhibition is associated with reduced Th17 responses. J. Exp. Med. 2007, 204, 3183–3194. [Google Scholar] [CrossRef]
- Nestle, F.O.; Conrad, C.; Tun-Kyi, A.; Homey, B.; Gombert, M.; Boyman, O.; Burg, G.; Liu, Y.J.; Gilliet, M. Plasmacytoid predendritic cells initiate psoriasis through interferon-alpha production. J. Exp. Med. 2005, 202, 135–143. [Google Scholar] [CrossRef]
- Terui, T.; Ozawa, M.; Tagami, H. Role of neutrophils in induction of acute inflammation in T-cell-mediated immune dermatosis, psoriasis: A neutrophil-associated inflammation-boosting loop. Exp. Dermatol. 2000, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Reich, K.; Papp, K.A.; Matheson, R.T.; Tu, J.H.; Bissonnette, R.; Bourcier, M.; Gratton, D.; Kunynetz, R.A.; Poulin, Y.; Rosoph, L.A.; et al. Evidence that a neutrophil-keratinocyte crosstalk is an early target of IL-17A inhibition in psoriasis. Exp. Dermatol. 2015, 24, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Bos, J.D.; Hulsebosch, H.J.; Krieg, S.R.; Bakker, P.M.; Cormane, R.H. Immunocompetent cells in psoriasis. In situ immunophenotyping by monoclonal antibodies. Arch. Dermatol. Res. 1983, 275, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Kagami, S.; Rizzo, H.L.; Lee, J.J.; Koguchi, Y.; Blauvelt, A. Circulating Th17, Th22, and Th1 cells are increased in psoriasis. J. Investig. Dermatol. 2010, 130, 1373–1383. [Google Scholar] [CrossRef] [PubMed]
- Capon, F.; Di Meglio, P.; Szaub, J.; Prescott, N.J.; Dunster, C.; Baumber, L.; Timms, K.; Gutin, A.; Abkevic, V.; Burden, A.D.; et al. Sequence variants in the genes for the interleukin-23 receptor (IL23R) and its ligand (IL12B) confer protection against psoriasis. Hum. Genet. 2007, 122, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Zaba, L.C.; Fuentes-Duculan, J.; Eungdamrong, N.J.; Johnson-Huang, L.M.; Nograles, K.E.; White, T.R.; Pierson, K.C.; Lentini, T.; Suárez-Fariñas, M.; Lowes, M.A.; et al. Identification of TNF-related apoptosis-inducing ligand and other molecules that distinguish inflammatory from resident dendritic cells in patients with psoriasis. J. Allergy Clin. Immunol. 2010, 125, 1261–1268.e9. [Google Scholar] [CrossRef] [PubMed]
- Johnson-Huang, L.M.; Suárez-Fariñas, M.; Pierson, K.C.; Fuentes-Duculan, J.; Cueto, I.; Lentini, T.; Sullivan-Whalen, M.; Gilleaudeau, P.; Krueger, J.G.; Haider, A.S.; et al. A single intradermal injection of IFN-γ induces an inflammatory state in both non-lesional psoriatic and healthy skin. J. Investig. Dermatol. 2012, 132, 1177–1187. [Google Scholar] [CrossRef]
- Madonna, S.; Scarponi, C.; Sestito, R.; Pallotta, S.; Cavani, A.; Albanesi, C. The IFN-gamma-dependent suppressor of cytokine signaling 1 promoter activity is positively regulated by IFN regulatory factor-1 and Sp1 but repressed by growth factor independence-1b and Krüppel-like factor-4, and it is dysregulated in psoriatic keratinocytes. J. Immunol. 2010, 185, 2467–2481. [Google Scholar] [CrossRef]
- Nair, R.P.; Duffin, K.C.; Helms, C.; Ding, J.; Stuart, P.E.; Goldgar, D.; Gudjonsson, J.E.; Li, Y.; Tejasvi, T.; Feng, B.J.; et al. Genome-wide scan reveals association of psoriasis with IL-23 and NF-kappaB pathways. Nat. Genet. 2009, 41, 199–204. [Google Scholar] [CrossRef]
- Gandhi, M.; Alwawi, E.; Gordon, K.B. Anti-p40 antibodies ustekinumab and briakinumab: Blockade of interleukin-12 and interleukin-23 in the treatment of psoriasis. Semin. Cutan. Med. Surg. 2010, 29, 48–52. [Google Scholar] [CrossRef]
- Gaffen, S.L.; Kramer, J.M.; Yu, J.J.; Shen, F. The IL-17 cytokine family. Vitam. Horm. 2006, 74, 255–282. [Google Scholar] [CrossRef]
- Krueger, J.G.; Fretzin, S.; Suárez-Fariñas, M.; Haslett, P.A.; Phipps, K.M.; Cameron, G.S.; McColm, J.; Katcherian, A.; Cueto, I.; White, T.; et al. IL-17A is essential for cell activation and inflammatory gene circuits in subjects with psoriasis. J. Allergy Clin. Immunol. 2012, 130, 145–154.e9. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.C.; Tan, X.Y.; Luxenberg, D.P.; Karim, R.; Dunussi-Joannopoulos, K.; Collins, M.; Fouser, L.A. Interleukin (IL)-22 and IL-17 are coexpressed by Th17 cells and cooperatively enhance expression of antimicrobial peptides. J. Exp. Med. 2006, 203, 2271–2279. [Google Scholar] [CrossRef] [PubMed]
- Goodman, W.A.; Levine, A.D.; Massari, J.V.; Sugiyama, H.; McCormick, T.S.; Cooper, K.D. IL-6 signaling in psoriasis prevents immune suppression by regulatory T cells. J. Immunol. 2009, 183, 3170–3176. [Google Scholar] [CrossRef] [PubMed]
- Chiricozzi, A.; Guttman-Yassky, E.; Suárez-Fariñas, M.; Nograles, K.E.; Tian, S.; Cardinale, I.; Chimenti, S.; Krueger, J.G. Integrative responses to IL-17 and TNF-α in human keratinocytes account for key inflammatory pathogenic circuits in psoriasis. J. Investig. Dermatol. 2011, 131, 677–687. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Chen, Y.; Yu, Q.; Shi, Y. Biologic and Small-Molecule Therapies for Moderate-to-Severe Psoriasis: Focus on Psoriasis Comorbidities. BioDrugs 2023, 37, 35–55. [Google Scholar] [CrossRef] [PubMed]
- Ion, A.; Dorobanțu, A.M.; Popa, L.G.; Mihai, M.M.; Orzan, O.A. Risks of Biologic Therapy and the Importance of Multidisciplinary Approach for an Accurate Management of Patients with Moderate-Severe Psoriasis and Concomitant Diseases. Biology 2022, 11, 808. [Google Scholar] [CrossRef]
- Fu, Y.; Lee, C.H.; Chi, C.C. Association of Psoriasis with Inflammatory Bowel Disease: A Systematic Review and Meta-analysis. JAMA Dermatol. 2018, 154, 1417–1423. [Google Scholar] [CrossRef]
- Alinaghi, F.; Tekin, H.G.; Burisch, J.; Wu, J.J.; Thyssen, J.P.; Egeberg, A. Global Prevalence and Bidirectional Association Between Psoriasis and Inflammatory Bowel Disease-A Systematic Review and Meta-analysis. J. Crohn’s Colitis 2020, 14, 351–360. [Google Scholar] [CrossRef]
- Feagan, B.G.; Panaccione, R.; Sandborn, W.J.; D’Haens, G.R.; Schreiber, S.; Rutgeerts, P.J.; Loftus, E.V., Jr.; Lomax, K.G.; Yu, A.P.; Wu, E.Q.; et al. Effects of adalimumab therapy on incidence of hospitalization and surgery in Crohn’s disease: Results from the CHARM study. Gastroenterology 2008, 135, 1493–1499. [Google Scholar] [CrossRef]
- Watanabe, M.; Hibi, T.; Mostafa, N.M.; Chao, J.; Arora, V.; Camez, A.; Petersson, J.; Thakkar, R. Long-term safety and efficacy of adalimumab in Japanese patients with moderate to severe Crohn’s disease. J. Crohn’s Colitis 2014, 8, 1407–1416. [Google Scholar] [CrossRef] [PubMed]
- Lichtiger, S.; Binion, D.G.; Wolf, D.C.; Present, D.H.; Bensimon, A.G.; Wu, E.; Yu, A.P.; Cardoso, A.T.; Chao, J.; Mulani, P.M.; et al. The CHOICE trial: Adalimumab demonstrates safety, fistula healing, improved quality of life and increased work productivity in patients with Crohn’s disease who failed prior infliximab therapy. Aliment. Pharmacol. Ther. 2010, 32, 1228–1239. [Google Scholar] [CrossRef] [PubMed]
- Feagan, B.G.; Sandborn, W.J.; Gasink, C.; Jacobstein, D.; Lang, Y.; Friedman, J.R.; Blank, M.A.; Johanns, J.; Gao, L.L.; Miao, Y.; et al. Ustekinumab as Induction and Maintenance Therapy for Crohn’s Disease. N. Engl. J. Med. 2016, 375, 1946–1960. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Friedman, J.R.; Chan, D.; Pollack, P.; Yang, F.; Jacobstein, D.; Brodmerkel, C.; Gasink, C.; Feagan, B.G.; Sandborn, W.J.; et al. Effects of Ustekinumab on Histologic Disease Activity in Patients with Crohn’s Disease. Gastroenterology 2019, 157, 1019–1031.e7. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, Z.; Venkata, K.; Zhang, N.; Malik, T.A. Comparative Effectiveness of Ustekinumab Versus Adalimumab in Induction of Clinical Response and Remission in Crohn’s Disease: Experience of a Real-World Cohort at a Tertiary Care Inflammatory Bowel Disease Referral Center. Gastroenterol. Res. 2019, 12, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Korzenik, J.; Larsen, M.D.; Nielsen, J.; Kjeldsen, J.; Nørgård, B.M. Increased risk of developing Crohn’s disease or ulcerative colitis in 17 018 patients while under treatment with anti-TNFα agents, particularly etanercept, for autoimmune diseases other than inflammatory bowel disease. Aliment. Pharmacol. Ther. 2019, 50, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, K.; Rogers, S. Development of Crohn disease in a patient on etanercept for psoriasis. Br. J. Dermatol. 2007, 157, 396. [Google Scholar] [CrossRef]
- Tichy, M.; Hercogova, J. Manifestation of Crohn’s disease in a young woman during the course of treatment for severe form of chronic plaque psoriasis with etanercept. Dermatol. Ther. 2014, 27, 211–214. [Google Scholar] [CrossRef]
- Gordon, K.B.; Blauvelt, A.; Papp, K.A.; Langley, R.G.; Luger, T.; Ohtsuki, M.; Reich, K.; Amato, D.; Ball, S.G.; Braun, D.K.; et al. Phase 3 Trials of Ixekizumab in Moderate-to-Severe Plaque Psoriasis. N. Engl. J. Med. 2016, 375, 345–356. [Google Scholar] [CrossRef]
- Reich, K.; Leonardi, C.; Langley, R.G.; Warren, R.B.; Bachelez, H.; Romiti, R.; Ohtsuki, M.; Xu, W.; Acharya, N.; Solotkin, K.; et al. Inflammatory bowel disease among patients with psoriasis treated with ixekizumab: A presentation of adjudicated data from an integrated database of 7 randomized controlled and uncontrolled trials. J. Am. Acad. Dermatol. 2017, 76, 441–448.e2. [Google Scholar] [CrossRef]
- Schreiber, S.; Colombel, J.F.; Feagan, B.G.; Reich, K.; Deodhar, A.A.; McInnes, I.B.; Porter, B.; Das Gupta, A.; Pricop, L.; Fox, T. Incidence rates of inflammatory bowel disease in patients with psoriasis, psoriatic arthritis and ankylosing spondylitis treated with secukinumab: A retrospective analysis of pooled data from 21 clinical trials. Ann. Rheum. Dis. 2019, 78, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Feagan, B.G.; Sandborn, W.J.; D’Haens, G.; Panés, J.; Kaser, A.; Ferrante, M.; Louis, E.; Franchimont, D.; Dewit, O.; Seidler, U.; et al. Induction therapy with the selective interleukin-23 inhibitor risankizumab in patients with moderate-to-severe Crohn’s disease: A randomised, double-blind, placebo-controlled phase 2 study. Lancet 2017, 389, 1699–1709. [Google Scholar] [CrossRef] [PubMed]
- Feagan, B.G.; Panés, J.; Ferrante, M.; Kaser, A.; D’Haens, G.R.; Sandborn, W.J.; Louis, E.; Neurath, M.F.; Franchimont, D.; Dewit, O.; et al. Risankizumab in patients with moderate to severe Crohn’s disease: An open-label extension study. Lancet Gastroenterol. Hepatol. 2018, 3, 671–680. [Google Scholar] [CrossRef] [PubMed]
- Sandborn, W.J.; D’Haens, G.R.; Reinisch, W.; Panés, J.; Chan, D.; Gonzalez, S.; Weisel, K.; Germinaro, M.; Frustaci, M.E.; Yang, Z.; et al. Guselkumab for the Treatment of Crohn’s Disease: Induction Results from the Phase 2 GALAXI-1 Study. Gastroenterology 2022, 162, 1650–1664.e8. [Google Scholar] [CrossRef] [PubMed]
- Grossberg, L.B. A Case Report of Successful Treatment of Crohn’s Disease and Psoriasis with Guselkumab. Inflamm. Bowel Dis. 2019, 25, e84. [Google Scholar] [CrossRef] [PubMed]
- Berman, H.S.; Villa, N.M.; Shi, V.Y.; Hsiao, J.L. Guselkumab in the treatment of concomitant hidradenitis suppurativa, psoriasis, and Crohn’s disease. J. Dermatolog. Treat. 2021, 32, 261–263. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, M.; Panaccione, R.; Baert, F.; Bossuyt, P.; Colombel, J.F.; Danese, S.; Dubinsky, M.; Feagan, B.G.; Hisamatsu, T.; Lim, A.; et al. Risankizumab as maintenance therapy for moderately to severely active Crohn’s disease: Results from the multicentre, randomised, double-blind, placebo-controlled, withdrawal phase 3 FORTIFY maintenance trial. Lancet 2022, 399, 2031–2046. [Google Scholar] [CrossRef]
- Sands, B.E.; Han, C.; Gasink, C.; Jacobstein, D.; Szapary, P.; Gao, L.L.; Lang, Y.; Targan, S.; Sandborn, W.J.; Feagan, B.G. The Effects of Ustekinumab on Health-related Quality of Life in Patients with Moderate to Severe Crohn’s Disease. J. Crohn’s Colitis 2018, 12, 883–895. [Google Scholar] [CrossRef]
- Yiu, Z.Z.N.; Becher, G.; Kirby, B.; Laws, P.; Reynolds, N.J.; Smith, C.H.; Warren, R.B.; Griffiths, C.E.M. Drug Survival Associated with Effectiveness and Safety of Treatment with Guselkumab, Ixekizumab, Secukinumab, Ustekinumab, and Adalimumab in Patients with Psoriasis. JAMA Dermatol. 2022, 158, 1131–1141. [Google Scholar] [CrossRef]
- Smith, M.K.; Pai, J.; Panaccione, R.; Beck, P.; Ferraz, J.G.; Jijon, H. Crohn’s-like disease in a patient exposed to anti-Interleukin-17 blockade (Ixekizumab) for the treatment of chronic plaque psoriasis: A case report. BMC Gastroenterol. 2019, 19, 162. [Google Scholar] [CrossRef]
- Fitzpatrick, L.R. Novel Pharmacological Approaches for Inflammatory Bowel Disease: Targeting Key Intracellular Pathways and the IL-23/IL-17 Axis. Int. J. Inflam. 2012, 2012, 389404. [Google Scholar] [CrossRef] [PubMed]
- Baeten, D.L.; Kuchroo, V.K. How Cytokine networks fuel inflammation: Interleukin-17 and a tale of two autoimmune diseases. Nat. Med. 2013, 19, 824–825. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, W.B.; McInnes, I.B. Th17 cells and IL-17 a—Focus on immunopathogenesis and immunotherapeutics. Semin. Arthritis. Rheum. 2013, 43, 158–170. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, J.R.; Zhang, Y.; Brown, W.A.; Smith, C.L.; Byrne, F.R.; Fiorino, M.; Stevens, E.; Bigler, J.; Davis, J.A.; Rottman, J.B.; et al. Differential Roles for Interleukin-23 and Interleukin-17 in Intestinal Immunoregulation. Immunity 2015, 43, 739–750. [Google Scholar] [CrossRef]
- Yang, X.O.; Chang, S.H.; Park, H.; Nurieva, R.; Shah, B.; Acero, L.; Wang, Y.H.; Schluns, K.S.; Broaddus, R.R.; Zhu, Z.; et al. Regulation of inflammatory responses by IL-17F. J. Exp. Med. 2008, 205, 1063–1075. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, W., Jr.; Kamanaka, M.; Booth, C.J.; Town, T.; Nakae, S.; Iwakura, Y.; Kolls, J.K.; Flavell, R.A. A protective function for interleukin 17A in T cell-mediated intestinal inflammation. Nat. Immunol. 2009, 10, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Deng, Z.; Wang, S.; Wu, C.; Wang, C. IL-17 inhibitor-associated inflammatory bowel disease: A study based on literature and database analysis. Front. Pharmacol. 2023, 14, 1124628. [Google Scholar] [CrossRef]
- Hueber, W.; Sands, B.E.; Lewitzky, S.; Vandemeulebroecke, M.; Reinisch, W.; Higgins, P.D.; Wehkamp, J.; Feagan, B.G.; Yao, M.D.; Karczewski, M.; et al. Secukinumab, a human anti-IL-17A monoclonal antibody, for moderate to severe Crohn’s disease: Unexpected results of a randomised, double-blind placebo-controlled trial. Gut 2012, 61, 1693–1700. [Google Scholar] [CrossRef]
- Wang, J.; Bhatia, A.; Krugliak Cleveland, N.; Gupta, N.; Dalal, S.; Rubin, D.T.; Sakuraba, A. Rapid Onset of Inflammatory Bowel Disease after Receiving Secukinumab Infusion. ACG Case Rep. J. 2018, 5, e56. [Google Scholar] [CrossRef]
- Philipose, J.; Ahmed, M.; Idiculla, P.S.; Mulrooney, S.M.; Gumaste, V.V. Severe de novo Ulcerative Colitis following Ixekizumab Therapy. Case Rep. Gastroenterol. 2018, 12, 617–621. [Google Scholar] [CrossRef]
- Haidari, W.; Al-Naqshabandi, S.; Ahn, C.S.; Bloomfeld, R.S.; Feldman, S.R. Asymptomatic Crohn’s disease identified in a patient being treated with secukinumab: A case report. SAGE Open Med. Case Rep. 2019, 7, 2050313x19893580. [Google Scholar] [CrossRef] [PubMed]
- Achufusi, T.G.; Harnee, P.S.; Rawlins, S. A Rare Case of New-Onset Ulcerative Colitis following Initiation of Secukinumab. Case Rep. Med. 2019, 2019, 2975631. [Google Scholar] [CrossRef] [PubMed]
- Merino Gallego, E.; Gómez Torres, K.; Martínez Amate, E. Debut Of Inflammatory Bowel Disease Associated To Ixekizumab In Patient with Moderate, Difficult -To-Manage Psoriasis. Gastroenterol. Hepatol. 2020, 43, 622–623. [Google Scholar] [CrossRef] [PubMed]
- Nazarian, A.; Grin, A.; Wijeratne, D.T. Ixekizumab Associated New-Onset Inflammatory Bowel Disease. ACG Case Rep. J. 2020, 7, e00316. [Google Scholar] [CrossRef] [PubMed]
- Marin, M.; Alzueta, N.; Pío, M.; Gascón, A.; Castresana, M. Ulcerative colitis induced by ixekizumab: A case report. Eur. J. Hosp. Pharm. 2021, 28, 50–52. [Google Scholar] [CrossRef] [PubMed]
- Mu, X.; Fardy, J.; Reid, S.; Trahey, J. Severe drug-associated colitis with Crohn’s features in setting of ixekizumab therapy for chronic plaque psoriasis. BMC Gastroenterol. 2021, 21, 361. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Systemic Treatment (Biologic Therapy Class and Novel Small-Molecule Inhibitor) | Drug | Chemical Structure | Mechanism of Action |
|---|---|---|---|
| IL-17 inhibitors | Ixekizumab | Humanized immunoglobulin G4 monoclonal antibody | Binding to interleukin 17 (IL-17A) and blocking its proinflammatory effects. |
| Secukinumab | Human IgG1 monoclonal antibody | ||
| IL-23 inhibitors | Guselkumab | Recombined human monoclonal antibody | Selective binding and blocking the p19 alpha subunit of IL-23. |
| Risankizumab | Humanized IgG monoclonal antibody | ||
| Tildrakizumab | Recombined human monoclonal antibody | ||
| IL-12/23 inhibitors | Ustekinumab | Human monoclonal antibody | Binds to the p40 subunit common to IL-12 and IL-23, thus preventing their interaction with the IL-12 receptor β1 subunit of the IL-12 and IL-23 receptor complexes. |
| TNF-alpha inhibitors | Adalimumab | Human monoclonal antibody | Binds with specificity to tumor necrosis factor-alpha (TNF-alpha) and inhibits its interaction with cell receptors. |
| Infliximab | Chimeric monoclonal antibody | ||
| Etanercept | Fusion protein produced by recombinant DNA | ||
| Certolizumab pegol | PEGylated, humanized, antigen-binding fragment of an anti-TNF monoclonal antibody | ||
| Small-molecule inhibitor | Apremilast | Polyaromatic molecule, a small-molecule inhibitor of the enzyme phosphodiesterase 4 (PDE4) | It selectively targets and inhibits the activity of small molecules. |
| Comorbidity | Recommended Therapeutic Option |
|---|---|
| Psoriatic arthritis | TNF-α inhibitors, ixekizumab, secukinumab, guselkumab, risankizumab |
| Congestive heart failure | IL-17 and IL-23 inhibitors |
| Metabolic syndrome | IL-17 inhibitors, ustekinumab, IL-23 inhibitors, apremilast |
| Depression | IL-23 inhibitors |
| Malignancy | IL-17 inhibitors, IL-23 inhibitors, apremilast |
| Inflammatory bowel disease | TNF-alpha inhibitors (adalimumab, infliximab, certolizumab pegol), ustekinumab, IL-23 inhibitors |
| Reference | Age and Gender | Type of IL-17 Inhibitor | Duration of Biologic Therapy | Personal or Family History | Gastroenterologic Diagnosis | Management |
|---|---|---|---|---|---|---|
| Wang J et al., 2018 [59] | 41-year-old female | Secukinumab | One week | Family history of CD and UC | Moderately active colitis | Corticosteroid therapy Infliximab Methotrexate |
| Philipose J et al., 2018 [60] | 31-year-old male | Ixekizumab | Three months | Smoking history | Steroid-refractory UC with a superimposed Cytomegalovirus infection | Infliximab Antiviral therapy |
| Haidari W et al., 2019 [61] | 65-year-old male | Secukinumab | A year and a half | Psoriatic arthritis | Asymptomatic CD | Switch to Guselkumab |
| Smith MK et al., 2019 [50] | 42-year-old male | Ixekizumab | Twelve weeks | None | Crohn’s-like colitis | Glucocorticoids Ustekinumab |
| Achufusi TG et al., 2019 [62] | 39-year-old male | Secukinumab | Six months | None | Unspecified colitis | Infliximab and glucocorticoids Apremilast |
| Merino Gallego E et al., 2020 [63] | 42-year-old-male | Ixekizumab | Two weeks | None | CD | Corticosteroid therapy |
| Nazarian A et al., 2020 [64] | 48-year-old female | Ixekizumab | Twelve weeks | Smoking history Psoriatic arthritis | CD | Corticosteroid therapy Adalimumab |
| Marin M et al., 2021 [65] | 76-year-old female | Ixekizumab | Twenty weeks | None | Unspecified colitis | Corticosteroid therapy Guselkumab |
| Mu X et al., 2021 [66] | 45-year-old male | Ixekizumab | Nine months | None | CD | Corticosteroid therapy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orzan, O.A.; Țieranu, C.G.; Olteanu, A.O.; Dorobanțu, A.M.; Cojocaru, A.; Mihai, M.M.; Popa, L.G.; Gheorghiu, A.M.; Giurcăneanu, C.; Ion, A. An Insight on the Possible Association between Inflammatory Bowel Disease and Biologic Therapy with IL-17 Inhibitors in Psoriasis Patients. Pharmaceutics 2023, 15, 2171. https://doi.org/10.3390/pharmaceutics15082171
Orzan OA, Țieranu CG, Olteanu AO, Dorobanțu AM, Cojocaru A, Mihai MM, Popa LG, Gheorghiu AM, Giurcăneanu C, Ion A. An Insight on the Possible Association between Inflammatory Bowel Disease and Biologic Therapy with IL-17 Inhibitors in Psoriasis Patients. Pharmaceutics. 2023; 15(8):2171. https://doi.org/10.3390/pharmaceutics15082171
Chicago/Turabian StyleOrzan, Olguța Anca, Cristian George Țieranu, Andrei Ovidiu Olteanu, Alexandra Maria Dorobanțu, Anca Cojocaru, Mara Mădălina Mihai, Liliana Gabriela Popa, Ana Maria Gheorghiu, Călin Giurcăneanu, and Ana Ion. 2023. "An Insight on the Possible Association between Inflammatory Bowel Disease and Biologic Therapy with IL-17 Inhibitors in Psoriasis Patients" Pharmaceutics 15, no. 8: 2171. https://doi.org/10.3390/pharmaceutics15082171
APA StyleOrzan, O. A., Țieranu, C. G., Olteanu, A. O., Dorobanțu, A. M., Cojocaru, A., Mihai, M. M., Popa, L. G., Gheorghiu, A. M., Giurcăneanu, C., & Ion, A. (2023). An Insight on the Possible Association between Inflammatory Bowel Disease and Biologic Therapy with IL-17 Inhibitors in Psoriasis Patients. Pharmaceutics, 15(8), 2171. https://doi.org/10.3390/pharmaceutics15082171