
Diagnosis of Herpes Simplex Virus: Laboratory and Point-of-Care Techniques


Abstract
:1. Introduction
2. Detection of HSV in Lesions
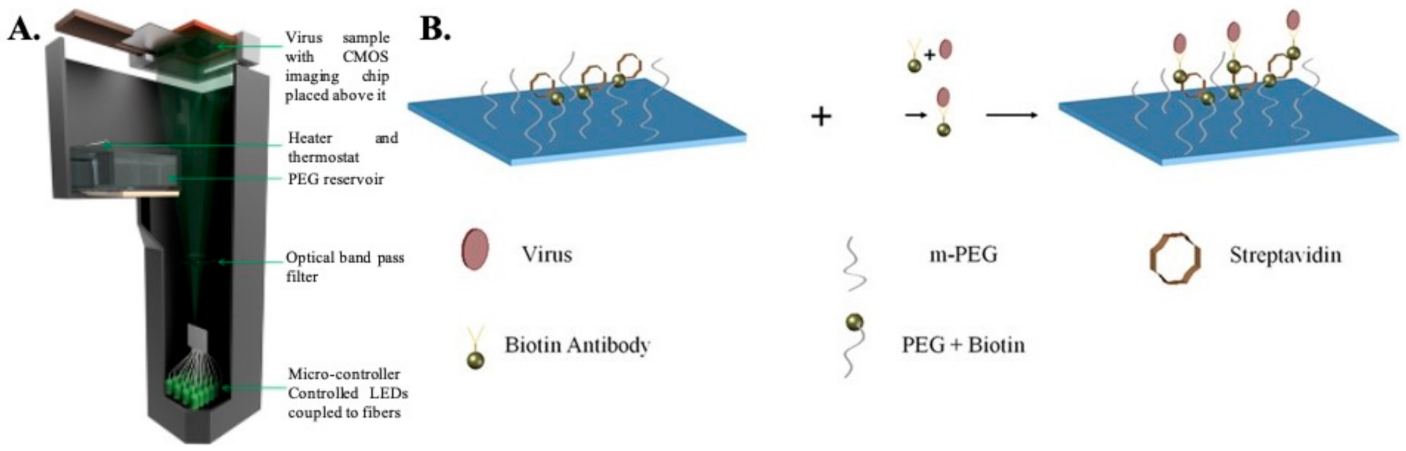
2.1. Microscopy and Imaging
2.2. Detecting Viral Glycoproteins
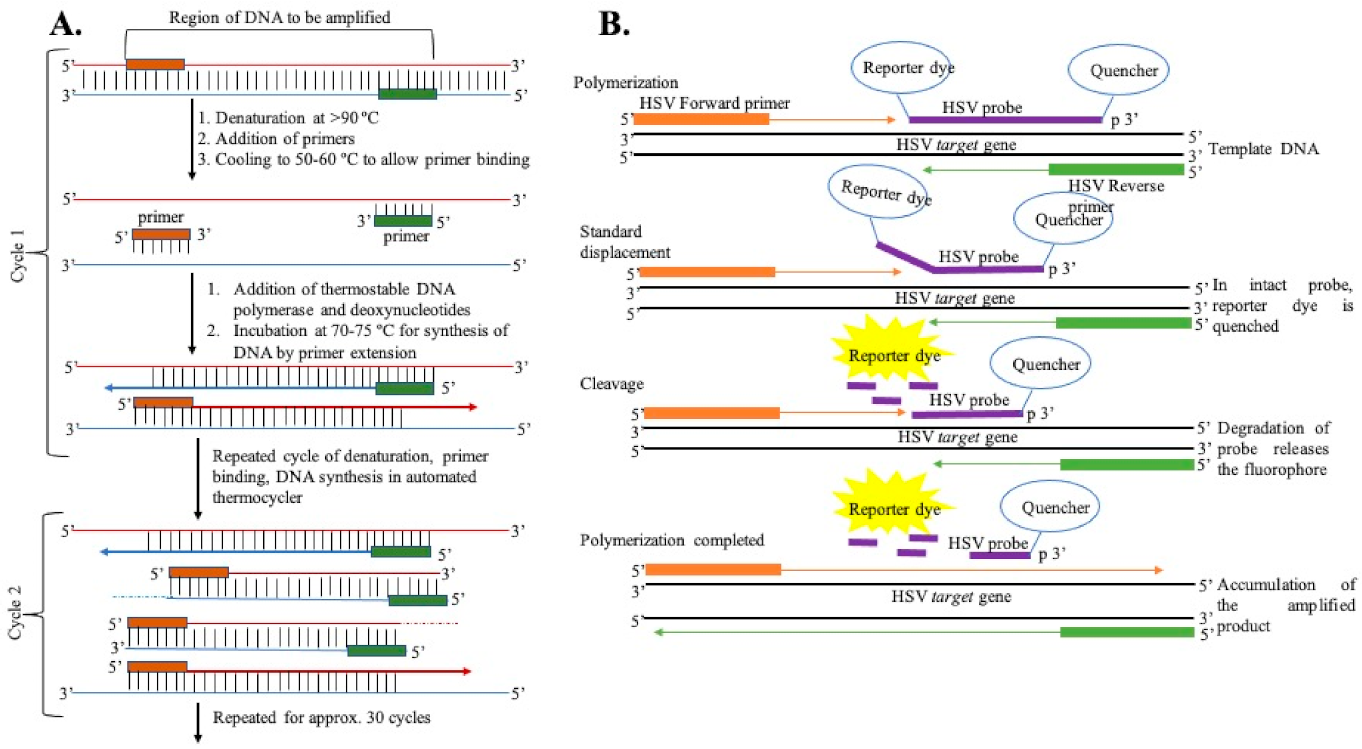
2.3. Detecting Viral Genetic Material
3. Detection of Viral Antibodies in Blood (Serological Assays)
3.1. Passive Agglutination or Hemagglutination Assay
3.2. Western Blot Assay
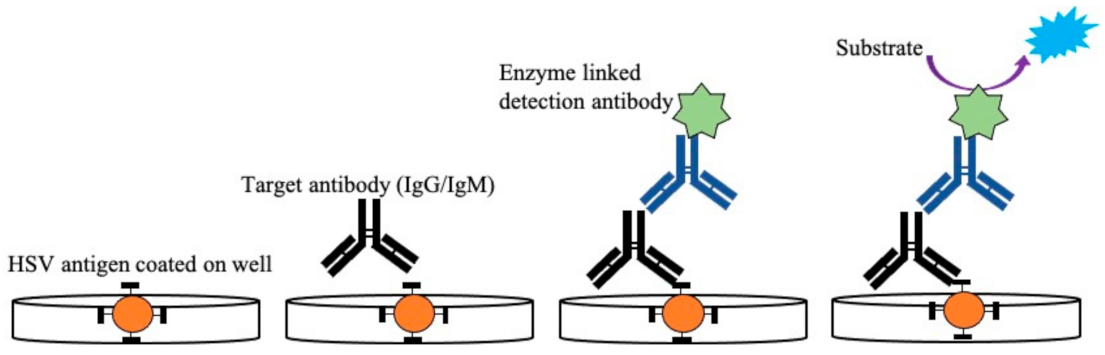
3.3. Enzyme-Linked Immunosorbent Assay (ELISA)
3.4. Fluorescence Immunoassay
3.5. Multiplexed Flow Immunoassay
3.6. Luciferase Immunoprecipitation Assay
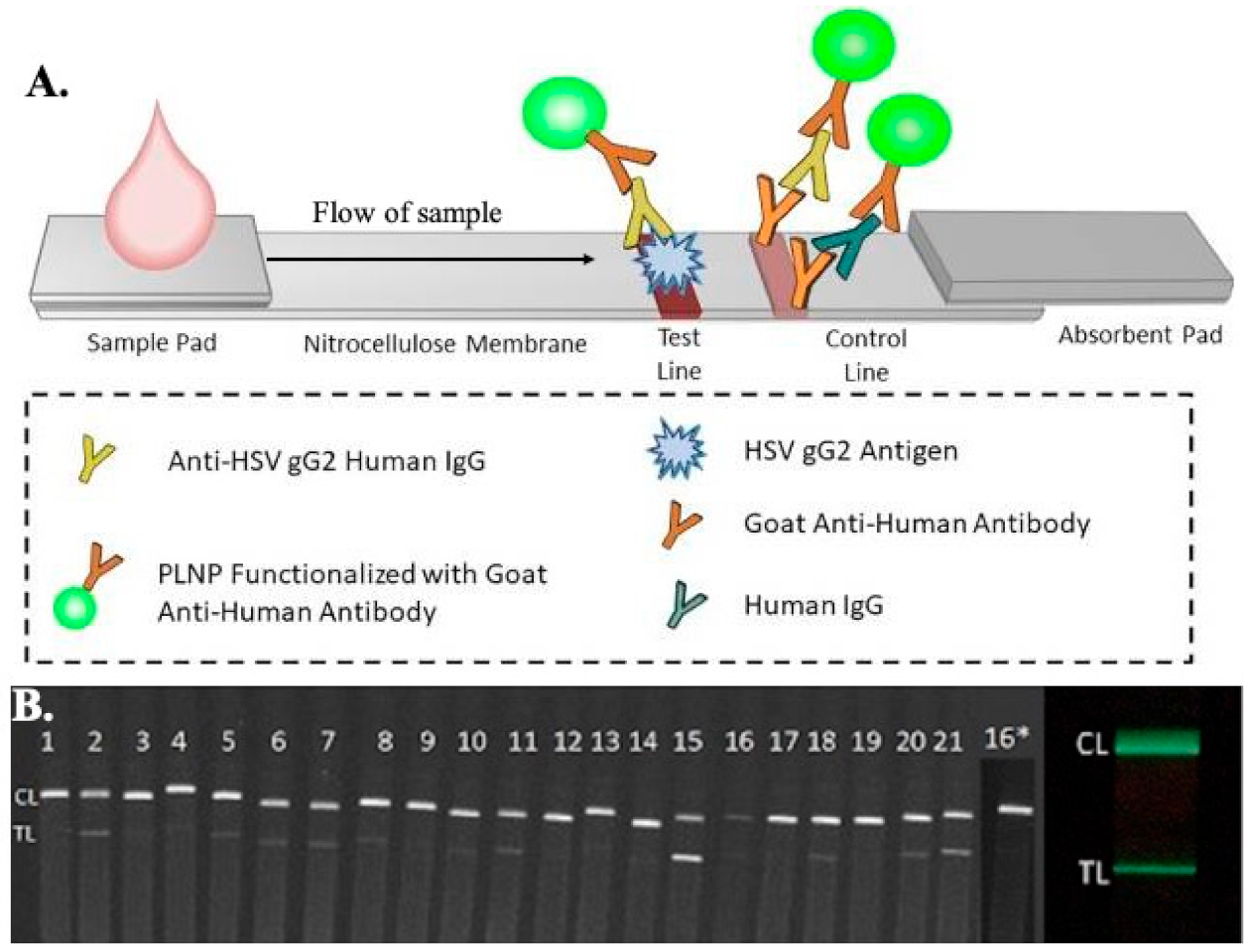
3.7. Microfluidic-Based Point-of-Care Devices
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johnston, C.; Corey, L. Current Concepts for Genital Herpes Simplex Virus Infection: Diagnostics and Pathogenesis of Genital Tract Shedding. Clin. Microbiol. Rev. 2016, 29, 149–161. [Google Scholar] [CrossRef] [Green Version]
- Whitley, R.; Baines, J. Clinical management of herpes simplex virus infections: Past, present, and future. F1000Research 2018, 7. F1000 Faculty Rev-1726. [Google Scholar] [CrossRef] [Green Version]
- Crimi, S.; Fiorillo, L.; Bianchi, A.; D’Amico, C.; Amoroso, G.; Gorassini, F.; Mastroieni, R.; Marino, S.; Scoglio, C.; Catalano, F.; et al. Herpes Virus, Oral Clinical Signs and QoL: Systematic Review of Recent Data. Viruses 2019, 11, 463. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Zhang, Y.; Li, Q. Characteristics of herpes simplex virus infection and pathogenesis suggest a strategy for vaccine development. Rev. Med. Virol. 2019, 29, e2054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arvin, A.; Campadelli-Fiume, G.; Mocarski, E.; Moore, P.S.; Roizman, B.; Whitley, R.; Yamanishi, K. Human Herpesviruses: Biology, Therapy, and Immunoprophylaxis; Cambridge University Press: Cambridge, UK, 2007. [Google Scholar]
- Weiss, H. Epidemiology of herpes simplex virus type 2 infection in the developing world. Herpes 2004, 11 (Suppl. 1), 24A–35A. [Google Scholar]
- Gaydos, C.; Hardick, J. Point of care diagnostics for sexually transmitted infections: Perspectives and advances. Expert Rev. Anti. Infect. Ther. 2014, 12, 657–672. [Google Scholar] [CrossRef] [Green Version]
- James, C.; Harfouche, M.; Welton, N.J.; Turner, K.M.E.; Abu-Raddad, L.J.; Gottlieb, S.L.; Looker, K.J. Herpes simplex virus: Global infection prevalence and incidence estimates, 2016. Bull. World Health Organ. 2020, 98, 315–329. [Google Scholar] [CrossRef] [PubMed]
- Looker, K.J.; Welton, N.J.; Sabin, K.M.; Dalal, S.; Vickerman, P.; Turner, K.M.E.; Boily, M.C.; Gottlieb, S.L. Global and regional estimates of the contribution of herpes simplex virus type 2 infection to HIV incidence: A population attributable fraction analysis using published epidemiological data. Lancet Infect. Dis. 2020, 20, 240–249. [Google Scholar] [CrossRef] [Green Version]
- Smith, G. Herpesvirus transport to the nervous system and back again. Annu. Rev. Microbiol. 2012, 66, 153–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, G.A.; Gross, S.P.; Enquist, L.W. Herpesviruses use bidirectional fast-axonal transport to spread in sensory neurons. Proc. Natl. Acad. Sci. USA 2001, 98, 3466–3470. [Google Scholar] [CrossRef] [Green Version]
- Chew, T.; Taylor, K.E.; Mossman, K.L. Innate and adaptive immune responses to herpes simplex virus. Viruses 2009, 1, 979–1002. [Google Scholar] [CrossRef] [Green Version]
- Ike, A.C.; Onu, C.J.; Ononugbo, C.M.; Reward, E.E.; Muo, S.O. Immune Response to Herpes Simplex Virus Infection and Vaccine Development. Vaccines 2020, 8, 302. [Google Scholar] [CrossRef]
- Nash, A.A.; Cambouropoulos, P. The immune response to herpes simplex virus. Semin. Virol. 1993, 4, 181–186. [Google Scholar] [CrossRef]
- Suazo, P.A.; Tognarelli, E.I.; Kalergis, A.M.; González, P.A. Herpes simplex virus 2 infection: Molecular association with HIV and novel microbicides to prevent disease. Med. Microbiol. Immunol. 2015, 204, 161–176. [Google Scholar] [CrossRef] [PubMed]
- Aoki, F.Y. Management of genital herpes in HIV-infected patients. Herpes 2001, 8, 41–45. [Google Scholar] [PubMed]
- Cherpes, T.L.; Matthews, D.B.; Maryak, S.A. Neonatal herpes simplex virus infection. Clin. Obstet. Gynecol. 2012, 55, 938–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimberlin, D.W. Neonatal herpes simplex infection. Clin. Microbiol. Rev. 2004, 17, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayoub, H.H.; Chemaitelly, H.; Abu-Raddad, L.J. Epidemiological Impact of Novel Preventive and Therapeutic HSV-2 Vaccination in the United States: Mathematical Modeling Analyses. Vaccines 2020, 8, 366. [Google Scholar] [CrossRef]
- Razonable, R.R. Antiviral drugs for viruses other than human immunodeficiency virus. Mayo Clin. Proc. 2011, 86, 1009–1026. [Google Scholar] [CrossRef] [Green Version]
- Munday, P.E.; Vuddamalay, J.; Slomka, M.J.; Brown, D.W. Role of type specific herpes simplex virus serology in the diagnosis and management of genital herpes. Sex. Transm. Infect. 1998, 74, 175–178. [Google Scholar] [CrossRef] [Green Version]
- Kozel, T.R.; Burnham-Marusich, A.R. Point-of-Care Testing for Infectious Diseases: Past, Present, and Future. J. Clin. Microbiol. 2017, 55, 2313–2320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Philip, S.S.; Ahrens, K.; Shayevich, C.; de la Roca, R.; Williams, M.; Wilson, D.; Bernstein, K.; Klausner, J.D. Evaluation of a New Point-of-Care Serologic Assay for Herpes Simplex Virus Type 2 Infection. Clin. Infect. Dis. 2008, 47, e79–e82. [Google Scholar] [CrossRef] [Green Version]
- Laderman, E.I.; Whitworth, E.; Dumaual, E.; Jones, M.; Hudak, A.; Hogrefe, W.; Carney, J.; Groen, J. Rapid, sensitive, and specific lateral-flow immunochromatographic point-of-care device for detection of herpes simplex virus type 2-specific immunoglobulin G antibodies in serum and whole blood. Clin. Vaccine Immunol. 2008, 15, 159–163. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Preiksaitis, J.; Ferenczy, A.; Romanowski, B. The laboratory diagnosis of herpes simplex virus infections. Can. J. Infect. Dis. Med. Microbiol. 2005, 16, 92–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, N.W.; Buchan, B.W.; Ledeboer, N.A. Light microscopy, culture, molecular, and serologic methods for detection of herpes simplex virus. J. Clin. Microbiol. 2014, 52, 2–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, H.H.; Mühlbauer, G.; Rinner, B.; Stelzl, E.; Berger, A.; Dörr, H.-W.; Santner, B.; Marth, E.; Rabenau, H. Detection of Herpes Simplex Virus DNA by Real-Time PCR. J. Clin. Microbiol. 2000, 38, 2638–2642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaneko, H.; Iida, T.; Aoki, K.; Ohno, S.; Suzutani, T. Sensitive and rapid detection of herpes simplex virus and varicella-zoster virus DNA by loop-mediated isothermal amplification. J. Clin. Microbiol. 2005, 43, 3290–3296. [Google Scholar] [CrossRef] [Green Version]
- Katz, D.; Hilliard, J.K.; Mirkovic, R.R.; Word, R.A. ELISA for detection of IgG and IgM antibodies to HSV-1 and HSV-2 in human sera. J. Virol. Methods 1986, 14, 43–55. [Google Scholar] [CrossRef]
- Ashley, R.L.; Militoni, J.; Lee, F.; Nahmias, A.; Corey, L. Comparison of Western blot (immunoblot) and glycoprotein G-specific immunodot enzyme assay for detecting antibodies to herpes simplex virus types 1 and 2 in human sera. J. Clin. Microbiol. 1988, 26, 662–667. [Google Scholar] [CrossRef] [Green Version]
- Pouletty, P.; Chomel, J.J.; Thouvenot, D.; Catalan, F.; Rabillon, V.; Kadouche, J. Detection of herpes simplex virus in direct specimens by immunofluorescence assay using a monoclonal antibody. J. Clin. Microbiol. 1987, 25, 958–959. [Google Scholar] [CrossRef] [Green Version]
- Olivo, P.D. Detection of herpes simplex virus by measurement of luciferase activity in an infected-cell lysate. J. Virol. Methods 1994, 47, 117–128. [Google Scholar] [CrossRef]
- LeGoff, J.; Péré, H.; Bélec, L. Diagnosis of genital herpes simplex virus infection in the clinical laboratory. Virol. J. 2014, 11, 83. [Google Scholar] [CrossRef]
- Morgan, C.; Rose, H.M.; Mednis, B. Electron microscopy of herpes simplex virus. I. Entry. J. Virol. 1968, 2, 507–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Folkers, E.; Vreeswijk, J.; Oranje, A.P.; Wagenaar, F.; Duivenvoorden, J.N. Improved detection of HSV by electron microscopy in clinical specimens using ultracentrifugation and colloidal gold immunoelectron microscopy: Comparison with viral culture and cytodiagnosis. J. Virol. Methods 1991, 34, 273–289. [Google Scholar] [CrossRef]
- Ray, A.; Daloglu, M.U.; Ho, J.; Torres, A.; Mcleod, E.; Ozcan, A. Computational sensing of herpes simplex virus using a cost-effective on-chip microscope. Sci. Rep. 2017, 7, 4856. [Google Scholar] [CrossRef] [PubMed]
- Koenig, M.; Reynolds, K.S.; Aldous, W.; Hickman, M. Comparison of Light-Cycler PCR, enzyme immunoassay, and tissue culture for detection of herpes simplex virus. Diagn. Microbiol. Infect. Dis. 2001, 40, 107–110. [Google Scholar] [CrossRef]
- Slinger, R.; Amrud, K.; Sant, N.; Ramotar, K.; Desjardins, M. A comparison of the Quidel Solana HSV 1 + 2/VZV Assay, the Focus Diagnostics Simplexa HSV 1 & 2 Direct Assay and the Luminex Aries HSV 1&2 Assay for detection of herpes simplex virus 1 and 2 from swab specimens. J. Clin. Virol. 2019, 113, 35–38. [Google Scholar] [CrossRef]
- Al-Shobaili, H.; Hassanein, K.M.; Mostafa, M.S.; Al Duways, A.S. Evaluation of the HerpeSelect Express rapid test in the detection of herpes simplex virus type 2 antibodies in patients with genital ulcer disease. J. Clin. Lab. Anal. 2015, 29, 43–46. [Google Scholar] [CrossRef]
- Kim, H.-J.; Tong, Y.; Tang, W.; Quimson, L.; Cope, V.A.; Pan, X.; Motre, A.; Kong, R.; Hong, J.; Kohn, D.; et al. A rapid and simple isothermal nucleic acid amplification test for detection of herpes simplex virus types 1 and 2. J. Clin. Virol. 2011, 50, 26–30. [Google Scholar] [CrossRef] [Green Version]
- Morrow, R.A.; Friedrich, D.; Meier, A.; Corey, L. Use of “biokit HSV-2 Rapid Assay” to improve the positive predictive value of Focus HerpeSelect HSV-2 ELISA. BMC Infect. Dis. 2005, 5, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daaboul, G.G.; Freedman, D.S.; Scherr, S.M.; Carter, E.; Rosca, A.; Bernstein, D.; Mire, C.E.; Agans, K.N.; Hoenen, T.; Geisbert, T.W.; et al. Enhanced light microscopy visualization of virus particles from Zika virus to filamentous ebolaviruses. PLoS ONE 2017, 12, e0179728. [Google Scholar] [CrossRef]
- Solomon, A.R.; Rasmussen, J.E.; Varani, J.; Pierson, C.L. The Tzanck smear in the diagnosis of cutaneous herpes simplex. JAMA 1984, 251, 633–635. [Google Scholar] [CrossRef]
- Kelly, B.; Shimoni, T. Reintroducing the Tzanck Smear. Am. J. Clin. Dermatol. 2009, 10, 141–152. [Google Scholar] [CrossRef]
- Eksomtramage, T.; Aiempanakit, K. Recurrent extragenital herpes simplex type 2 occurring in a distal location of the same dermatome. IDCases 2020, 21, e00783. [Google Scholar] [CrossRef] [PubMed]
- Nahass, G.T.; Mandel, M.J.; Cook, S.; Fan, W.; Leonardi, C.L. Detection of herpes simplex and varicella-zoster infection from cutaneous lesions in different clinical stages with the polymerase chain reaction. J. Am. Acad. Dermatol. 1995, 32, 730–733. [Google Scholar] [CrossRef]
- Nahass, G.T.; Goldstein, B.A.; Zhu, W.Y.; Serfling, U.; Penneys, N.S.; Leonardi, C.L. Comparison of Tzanck smear, viral culture, and DNA diagnostic methods in detection of herpes simplex and varicella-zoster infection. JAMA 1992, 268, 2541–2544. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Aoyama, Y. Detection of multinucleated giant cells in differentiated keratinocytes with herpes simplex virus and varicella zoster virus infections by modified Tzanck smear method. J. Dermatol. 2021, 48, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.S.; Landry, M.L.; Balkovic, E.S.; Hsiung, G.D. Impact of cell culture sensitivity and virus concentration on rapid detection of herpes simplex virus by cytopathic effects and immunoperoxidase staining. J. Clin. Microbiol. 1987, 25, 1401–1405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jerome, K.R.; Morrow, R.A. Herpes Simplex Virus. In Manual of Clinical Microbiology; Wiley: New York, NY, USA, 2015. [Google Scholar]
- Moore, D.F. Comparison of human fibroblast cells and primary rabbit kidney cells for isolation of herpes simplex virus. J. Clin. Microbiol. 1984, 19, 548–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witte, R.; Andriasyan, V.; Georgi, F.; Yakimovich, A.; Greber, U.F. Concepts in Light Microscopy of Viruses. Viruses 2018, 10, 202. [Google Scholar] [CrossRef] [Green Version]
- Marie, D.; Brussaard, C.P.D.; Thyrhaug, R.; Bratbak, G.; Vaulot, D. Enumeration of marine viruses in culture and natural samples by flow cytometry. Appl. Environ. Microbiol. 1999, 65, 45–52. [Google Scholar] [CrossRef] [Green Version]
- Parveen, N.; Borrenberghs, D.; Rocha, S.; Hendrix, J. Single Viruses on the Fluorescence Microscope: Imaging Molecular Mobility, Interactions and Structure Sheds New Light on Viral Replication. Viruses 2018, 10, 250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, A.B.; Mazelier, M.; Léger, P.; Lozach, P.-Y. Deciphering Virus Entry with Fluorescently Labeled Viral Particles BT—Influenza Virus: Methods and Protocols. In Influenza Virus; Yamauchi, Y., Ed.; Springer: New York, NY, USA, 2018; pp. 159–183. ISBN 9781493986781. [Google Scholar]
- Nikolic, D.; Kohn, D.; Yen-Lieberman, B.; Procop, G.W. Detection of Herpes Simplex Virus and Varicella-Zoster Virus by Traditional and Multiplex Molecular Methods. Am. J. Clin. Pathol. 2019, 151, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.L.; Brandt, K.; Horsman, G.B. Comparison of Chemicon SimulFluor Direct Fluorescent Antibody Staining with Cell Culture and Shell Vial Direct Immunoperoxidase Staining for Detection of Herpes Simplex Virus and with Cytospin Direct Immunofluorescence Staining for Detection of Varicella-Zoster Virus. Clin. Diagn. Lab. Immunol. 2001, 8, 909–912. [Google Scholar] [CrossRef] [Green Version]
- Lafferty, W.E.; Krofft, S.; Remington, M.; Giddings, R.; Winter, C.; Cent, A.; Corey, L. Diagnosis of herpes simplex virus by direct immunofluorescence and viral isolation from samples of external genital lesions in a high-prevalence population. J. Clin. Microbiol. 1987, 25, 323–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, F.; Day, S.; Lu, X.; Tang, Y.-W. Laboratory diagnosis of HSV and varicella zoster virus infections. Future Virol. 2014, 9, 721–731. [Google Scholar] [CrossRef]
- Patwardhan, V.; Bhalla, P.; Rawat, D.; Garg, V.K.; Sardana, K.; Sethi, S. A Comparative Analysis of Polymerase Chain Reaction and Direct Fluorescent Antibody Test for Diagnosis of Genital Herpes. J. Lab. Physicians 2017, 9, 53–56. [Google Scholar] [CrossRef]
- Muller, W.J.; Zheng, X. Laboratory Diagnosis of Neonatal Herpes Simplex Virus Infections. J. Clin. Microbiol. 2019, 57, e01460-18. [Google Scholar] [CrossRef] [Green Version]
- Caviness, A.C.; Oelze, L.L.; Saz, U.E.; Greer, J.M.; Demmler-Harrison, G.J. Direct immunofluorescence assay compared to cell culture for the diagnosis of mucocutaneous herpes simplex virus infections in children. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2010, 49, 58–60. [Google Scholar] [CrossRef]
- Miller, S.E.; Levenson, R.M.; Aldridge, C.; Hester, S.; Kenan, D.J.; Howell, D.N. Identification of focal viral infections by confocal microscopy for subsequent ultrastructural analysis. Ultrastruct. Pathol. 1997, 21, 183–193. [Google Scholar] [CrossRef]
- Müller, R.T.; Pourmirzaie, R.; Pavan-Langston, D.; Cavalcanti, B.M.; Aggarwal, S.; Colón, C.; Jamali, A.; Cruzat, A.; Hamrah, P. In Vivo Confocal Microscopy Demonstrates Bilateral Loss of Endothelial Cells in Unilateral Herpes Simplex Keratitis. Investig. Ophthalmol. Vis. Sci. 2015, 56, 4899–4906. [Google Scholar] [CrossRef] [PubMed]
- Hillenaar, T.; Wubbels, R.; Weenen, C.; Remeijer, L. Endothelial Involvement in Herpes Simplex Virus Keratitis: An in vivo Confocal Microscopy Study. Investig. Ophthalmol. Vis. Sci. 2008, 49, 2808. [Google Scholar] [CrossRef]
- Cinotti, E.; Perrot, J.L.; Labeille, B.; Campolmi, N.; Thuret, G.; Naigeon, N.; Bourlet, T.; Pillet, S.; Cambazard, F. First identification of the herpes simplex virus by skin-dedicated ex vivo fluorescence confocal microscopy during herpetic skin infections. Clin. Exp. Dermatol. 2015, 40, 421–425. [Google Scholar] [CrossRef]
- Howell, D.N.; Miller, S.E. Identification of viral infection by confocal microscopy. Methods Enzymol. 1999, 307, 573–591. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Li, Y.; Yang, Y.; Wang, J.; Zhu, C.; Tang, S.; Pang, C.; Tang, W.; Cai, Q.; Li, Z.; et al. The Detection and Characterization of Herpes Simplex Virus Type 1 in Confirmed Measles Cases. Sci. Rep. 2019, 9, 12785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Debarbieux, S.; Depaepe, L.; Poulalhon, N.; Dalle, S.; Balme, B.; Thomas, L. Reflectance confocal microscopy characteristics of eight cases of pustular eruptions and histopathological correlations. Ski. Res. Technol. 2013, 19, e444–e452. [Google Scholar] [CrossRef] [PubMed]
- Levine, A.; Markowitz, O. Introduction to reflectance confocal microscopy and its use in clinical practice. JAAD Case Rep. 2018, 4, 1014–1023. [Google Scholar] [CrossRef] [Green Version]
- Folkers, E.; Vreeswijk, J.; Oranje, A.P.; Duivenvoorden, J.N. Rapid diagnosis in varicella and herpes zoster: Re-evaluation of direct smear (Tzanck test) and electron microscopy including colloidal gold immuno-electron microscopy in comparison with virus isolation. Br. J. Dermatol. 1989, 121, 287–296. [Google Scholar] [CrossRef]
- Goldsmith, C.S.; Miller, S.E. Modern Uses of Electron Microscopy for Detection of Viruses. Clin. Microbiol. Rev. 2009, 22, 552–563. [Google Scholar] [CrossRef] [Green Version]
- Vreeswijk, J.; Folkers, E.; Wagenaar, F.; Kapsenberg, J.G. The use of colloidal gold immunoelectron microscopy to diagnose varicella-zoster virus (VZV) infections by rapid discrimination between VZV, HSV-1 and HSV-2. J. Virol. Methods 1988, 22, 255–271. [Google Scholar] [CrossRef]
- Greenbaum, A.; Luo, W.; Su, T.-W.; Göröcs, Z.; Xue, L.; Isikman, S.O.; Coskun, A.F.; Mudanyali, O.; Ozcan, A. Imaging without lenses: Achievements and remaining challenges of wide-field on-chip microscopy. Nat. Methods 2012, 9, 889–895. [Google Scholar] [CrossRef]
- Zhang, Y.; Ouyang, M.; Ray, A.; Liu, T.; Kong, J.; Bai, B.; Kim, D.; Guziak, A.; Luo, Y.; Feizi, A.; et al. Computational cytometer based on magnetically modulated coherent imaging and deep learning. Light Sci. Appl. 2019, 8, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daloglu, M.U.; Ray, A.; Collazo, M.J.; Brown, C.; Tseng, D.; Chocarro-Ruiz, B.; Lechuga, L.M.; Cascio, D.; Ozcan, A. Low-cost and portable UV holographic microscope for high-contrast protein crystal imaging. APL Photonics 2019, 4, 30804. [Google Scholar] [CrossRef] [Green Version]
- Daloglu, M.U.; Ray, A.; Gorocs, Z.; Xiong, M.; Malik, R.; Bitan, G.; McLeod, E.; Ozcan, A. Computational On-Chip Imaging of Nanoparticles and Biomolecules using Ultraviolet Light. Sci. Rep. 2017, 7, 44157. [Google Scholar] [CrossRef] [Green Version]
- Ray, A.; Li, S.; Segura, T.; Ozcan, A. High-Throughput Quantification of Nanoparticle Degradation Using Computational Microscopy and Its Application to Drug Delivery Nanocapsules. ACS Photonics 2017, 4, 1216–1224. [Google Scholar] [CrossRef]
- Ozcan, A.; McLeod, E. Lensless Imaging and Sensing. Annu. Rev. Biomed. Eng. 2016, 18, 77–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLeod, E.; Ozcan, A. Unconventional methods of imaging: Computational microscopy and compact implementations. Rep. Prog. Phys. 2016, 79, 76001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ray, A.; Khalid, M.A.; Demčenko, A.; Daloglu, M.; Tseng, D.; Reboud, J.; Cooper, J.M.; Ozcan, A. Holographic detection of nanoparticles using acoustically actuated nanolenses. Nat. Commun. 2020, 11, 171. [Google Scholar] [CrossRef]
- Wu, Y.; Ray, A.; Wei, Q.; Feizi, A.; Tong, X.; Chen, E.; Luo, Y.; Ozcan, A. Deep Learning Enables High-Throughput Analysis of Particle-Aggregation-Based Biosensors Imaged Using Holography. ACS Photonics 2019, 6, 294–301. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Ray, A.; Wei, Q.; Feizi, A.; Tong, X.; Chen, E.; Luo, Y.; Ozcan, A. Particle-Aggregation Based Virus Sensor Using Deep Learning and Lensless Digital Holography. In Proceedings of the Conference on Lasers and Electro-Optics, San Jose, CA, USA, 9–14 May 2019; p. ATu4K.3. [Google Scholar]
- Storch, G.A.; Reed, C.A.; Dalu, Z.A. Evaluation of a latex agglutination test for herpes simplex virus. J. Clin. Microbiol. 1988, 26, 787–788. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.F.; Pepose, J.S. Sandwich enzyme immunoassay and latex agglutination test for herpes simplex virus keratitis. J. Clin. Microbiol. 1990, 28, 785–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smalley, D.L.; Dunn, C.E. Evaluation of a new latex agglutination method for detection of antibody to Mycoplasma pneumoniae. Lab. Med. 1990, 21, 661–662. [Google Scholar] [CrossRef] [Green Version]
- Kowalski, R.P.; Gordon, Y.J. Evaluation of Immunologlic Tests for the Detection of Ocular Herpes Simplex Virus. Ophthalmology 1989, 96, 1583–1586. [Google Scholar] [CrossRef]
- Carter, M.; Shieh, J.C. Chapter 14—Biochemical Assays and Intracellular Signaling. In Guide to Research Techniques in Neuroscience; Carter, M., Shieh, J.C., Eds.; Academic Press: New York, NY, USA, 2010; pp. 297–329. ISBN 9780123748492. [Google Scholar]
- López Roa, P.; Alonso, R.; de Egea, V.; Usubillaga, R.; Muñoz, P.; Bouza, E. PCR for detection of herpes simplex virus in cerebrospinal fluid: Alternative acceptance criteria for diagnostic workup. J. Clin. Microbiol. 2013, 51, 2880–2883. [Google Scholar] [CrossRef] [Green Version]
- Gardella, C.; Huang, M.-L.; Wald, A.; Magaret, A.; Selke, S.; Morrow, R.; Corey, L. Rapid polymerase chain reaction assay to detect herpes simplex virus in the genital tract of women in labor. Obstet. Gynecol. 2010, 115, 1209–1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wald, A.; Huang, M.-L.; Carrell, D.; Selke, S.; Corey, L. Polymerase Chain Reaction for Detection of Herpes Simplex Virus (HSV) DNA on Mucosal Surfaces: Comparison with HSV Isolation in Cell Culture. J. Infect. Dis. 2003, 188, 1345–1351. [Google Scholar] [CrossRef]
- Scoular, A.; Gillespie, G.; Carman, W.F. Polymerase chain reaction for diagnosis of genital herpes in a genitourinary medicine clinic. Sex. Transm. Infect. 2002, 78, 21–25. [Google Scholar] [CrossRef] [Green Version]
- Kimura, H.; Futamura, M.; Kito, H.; Ando, T.; Goto, M.; Kuzushima, K.; Shibata, M.; Morishima, T. Detection of Viral DNA in Neonatal Herpes Simplex Virus Infections: Frequent and Prolonged Presence in Serum and Cerebrospinal Fluid. J. Infect. Dis. 1991, 164, 289–293. [Google Scholar] [CrossRef]
- Malm, G.; Forsgren, M. Neonatal herpes simplex virus infections: HSV DNA in cerebrospinal fluid and serum. Arch. Dis. Child. Fetal Neonatal Ed. 1999, 81, F24–F29. [Google Scholar] [CrossRef] [Green Version]
- Golden, W.C. Polymerase chain reaction in neonatal HSV encephalitis: An assay to count on? J. Perinatol. 2009, 29, 259–261. [Google Scholar] [CrossRef] [Green Version]
- Kimberlin, D.W.; Lakeman, F.D.; Arvin, A.M.; Prober, C.G.; Corey, L.; Powell, D.A.; Burchett, S.K.; Jacobs, R.F.; Starr, S.E.; Whitley, R.J. Application of the polymerase chain reaction to the diagnosis and management of neonatal herpes simplex virus disease. J. Infect. Dis. 1996, 174, 1162–1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strick, L.B.; Wald, A. Diagnostics for Herpes Simplex Virus. Mol. Diagn. Ther. 2006, 10, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Espy, M.J.; Uhl, J.R.; Sloan, L.M.; Buckwalter, S.P.; Jones, M.F.; Vetter, E.A.; Yao, J.D.C.; Wengenack, N.L.; Rosenblatt, J.E.; Cockerill, F.R., 3rd; et al. Real-time PCR in clinical microbiology: Applications for routine laboratory testing. Clin. Microbiol. Rev. 2006, 19, 165–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deepak, S.; Kottapalli, K.; Rakwal, R.; Oros, G.; Rangappa, K.; Iwahashi, H.; Masuo, Y.; Agrawal, G. Real-Time PCR: Revolutionizing Detection and Expression Analysis of Genes. Curr. Genom. 2007, 8, 234–251. [Google Scholar] [CrossRef]
- Schremser, V.; Antoniewicz, L.; Tschachler, E.; Geusau, A. Polymerase chain reaction for the diagnosis of herpesvirus infections in dermatology. Wien. Klin. Wochenschr. 2020, 132, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Pandori, M.W.; Lei, J.; Wong, E.H.; Klausner, J.; Liska, S. Real-Time PCR for detection of herpes simplex virus without nucleic acid extraction. BMC Infect. Dis. 2006, 6, 104. [Google Scholar] [CrossRef] [Green Version]
- Van, T.T.; Mongkolrattanothai, K.; Arevalo, M.; Lustestica, M.; Dien Bard, J. Impact of a Rapid Herpes Simplex Virus PCR Assay on Duration of Acyclovir Therapy. J. Clin. Microbiol. 2017, 55, 1557–1565. [Google Scholar] [CrossRef] [Green Version]
- Tang, Y.W.; Mitchell, P.S.; Espy, M.J.; Smith, T.F.; Persing, D.H. Molecular diagnosis of herpes simplex virus infections in the central nervous system. J. Clin. Microbiol. 1999, 37, 2127–2136. [Google Scholar] [CrossRef] [Green Version]
- Mejías, A.; Bustos, R.; Ardura, M.I.; Ramírez, C.; Sánchez, P.J. Persistence of herpes simplex virus DNA in cerebrospinal fluid of neonates with herpes simplex virus encephalitis. J. Perinatol. 2009, 29, 290–296. [Google Scholar] [CrossRef] [Green Version]
- Druce, J.; Catton, M.; Chibo, D.; Minerds, K.; Tyssen, D.; Kostecki, R.; Maskill, B.; Leong-Shaw, W.; Gerrard, M.; Birch, C. Utility of a multiplex PCR assay for detecting herpesvirus DNA in clinical samples. J. Clin. Microbiol. 2002, 40, 1728–1732. [Google Scholar] [CrossRef] [Green Version]
- Marshall, D.S.; Linfert, D.R.; Draghi, A.; McCarter, Y.S.; Tsongalis, G.J. Identification of Herpes Simplex Virus Genital Infection: Comparison of a Multiplex PCR Assay and Traditional Viral Isolation Techniques. Mod. Pathol. 2001, 14, 152–156. [Google Scholar] [CrossRef]
- Yap, T.; Khor, S.; Kim, J.S.; Kim, J.; Kim, S.Y.; Kern, J.S.; Martyres, R.; Varigos, G.; Chan, H.T.; McCullough, M.J.; et al. Intraoral human herpes viruses detectable by PCR in majority of patients. Oral Dis. 2021, 27, 378–387. [Google Scholar] [CrossRef]
- Dominguez, S.R.; Pretty, K.; Hengartner, R.; Robinson, C.C. Comparison of Herpes Simplex Virus PCR with Culture for Virus Detection in Multisource Surface Swab Specimens from Neonates. J. Clin. Microbiol. 2018, 56, e00632-18. [Google Scholar] [CrossRef] [Green Version]
- Espy, M.J.; Uhl, J.R.; Mitchell, P.S.; Thorvilson, J.N.; Svien, K.A.; Wold, A.D.; Smith, T.F. Diagnosis of Herpes Simplex Virus Infections in the Clinical Laboratory by LightCycler PCR. J. Clin. Microbiol. 2000, 38, 795–799. [Google Scholar] [CrossRef] [Green Version]
- Notomi, T.; Okayama, H.; Masubuchi, H.; Yonekawa, T.; Watanabe, K.; Amino, N.; Hase, T. Loop-mediated isothermal amplification of DNA. Nucleic Acids Res. 2000, 28, E63. [Google Scholar] [CrossRef] [Green Version]
- Smirnova, D.I.; Petrusha, O.A.; Gracheva, A.V.; Volynskaya, E.A.; Zverev, V.V.; Faizuloev, E.B. Rapid diagnostics of genital herpes by loop-mediated isothermal amplification method with fluorescent detection. J. Microbiol. Epidemiol. Immunobiol. 2019, 40–46. [Google Scholar] [CrossRef]
- Pourhossein, B.; Soleimanjahi, H.; Behzadian, F.; Khansarinejad, B. Loop-Mediated Isothermal Amplification (LAMP) for the Rapid Diagnosis of Herpes Simplex Virus Type 1 (HSV-1). Iran. J. Virol. 2011, 5, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Enomoto, Y.; Yoshikawa, T.; Ihira, M.; Akimoto, S.; Miyake, F.; Usui, C.; Suga, S.; Suzuki, K.; Kawana, T.; Nishiyama, Y.; et al. Rapid Diagnosis of Herpes Simplex Virus Infection by a Loop-Mediated Isothermal Amplification Method. J. Clin. Microbiol. 2005, 43, 951–955. [Google Scholar] [CrossRef] [Green Version]
- Reddy, A.K.; Balne, P.K.; Reddy, R.K.; Mathai, A.; Kaur, I. Loop-mediated isothermal amplification assay for the diagnosis of retinitis caused by herpes simplex virus-1. Clin. Microbiol. Infect. 2011, 17, 210–213. [Google Scholar] [CrossRef] [Green Version]
- Gadkar, V.J.; Goldfarb, D.M.; Gantt, S.; Tilley, P.A.G. Real-time Detection and Monitoring of Loop Mediated Amplification (LAMP) Reaction Using Self-quenching and De-quenching Fluorogenic Probes. Sci. Rep. 2018, 8, 5548. [Google Scholar] [CrossRef] [Green Version]
- Kinoshita, H.; Nakamichi, K.; Lim, C.-K.; Takayama-Ito, M.; Wang, L.; Iizuka, I.; Kurane, I.; Saijo, M. A loop-mediated isothermal amplification assay for the detection and quantification of JC polyomavirus in cerebrospinal fluid: A diagnostic and clinical management tool and technique for progressive multifocal leukoencephalopathy. Virol. J. 2018, 15, 136. [Google Scholar] [CrossRef]
- Becherer, L.; Borst, N.; Bakheit, M.; Frischmann, S.; Zengerle, R.; von Stetten, F. Loop-mediated isothermal amplification (LAMP)—Review and classification of methods for sequence-specific detection. Anal. Methods 2020, 12, 717–746. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, T.; Yagami, A.; Suzuki, K.; Ihira, M.; Yoshikawa, T.; Matsunaga, K. Clinical utility of loop-mediated isothermal amplification assay for the diagnosis of common alpha herpesvirus skin infections. J. Dermatol. 2013, 40, 1033–1037. [Google Scholar] [CrossRef] [PubMed]
- Rolando, J.C.; Jue, E.; Barlow, J.T.; Ismagilov, R.F. Real-time kinetics and high-resolution melt curves in single-molecule digital LAMP to differentiate and study specific and non-specific amplification. Nucleic Acids Res. 2020, 48, e42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barreda-García, S.; Miranda-Castro, R.; de-los-Santos-Álvarez, N.; Miranda-Ordieres, A.J.; Lobo-Castañón, M.J. Helicase-dependent isothermal amplification: A novel tool in the development of molecular-based analytical systems for rapid pathogen detection. Anal. Bioanal. Chem. 2018, 410, 679–693. [Google Scholar] [CrossRef] [PubMed]
- Teo, J.W.P.; Chiang, D.; Jureen, R.; Lin, R.T.P. Clinical evaluation of a helicase-dependant amplification (HDA)–based commercial assay for the simultaneous detection of HSV-1 and HSV-2. Diagn. Microbiol. Infect. Dis. 2015, 83, 261–262. [Google Scholar] [CrossRef]
- Lemieux, B.; Li, Y.; Kong, H.; Tang, Y.-W. Near instrument-free, simple molecular device for rapid detection of herpes simplex viruses. Expert Rev. Mol. Diagn. 2012, 12, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Miller, N.S.; Yen-Lieberman, B.; Poulter, M.D.; Tang, Y.-W.; Granato, P.A. Comparative clinical evaluation of the IsoAmp® HSV Assay with ELVIS® HSV culture/ID/typing test system for the detection of herpes simplex virus in genital and oral lesions. J. Clin. Virol. 2012, 54, 355–358. [Google Scholar] [CrossRef] [Green Version]
- Granato, P.A.; Alkins, B.R.; Yen-Lieberman, B.; Greene, W.H.; Connolly, J.; Buchan, B.W.; Ledeboer, N.A. Comparative Evaluation of AmpliVue HSV 1 + 2 Assay with ELVIS Culture for Detecting Herpes Simplex Virus 1 (HSV-1) and HSV-2 in Clinical Specimens. J. Clin. Microbiol. 2015, 53, 3922–3925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowalski, R.P.; Karenchak, L.M.; Dhaliwal, D.K.; Mammen, A. AmpliVue Is a Practical and Timely Test for the Detection of HSV From Keratitis Specimens. Eye Contact Lens 2018, 44, S244–S248. [Google Scholar] [CrossRef] [PubMed]
- Tong, Y.; McCarthy, K.; Kong, H.; Lemieux, B. Development and comparison of a rapid isothermal nucleic acid amplification test for typing of herpes simplex virus types 1 and 2 on a portable fluorescence detector. J. Mol. Diagn. 2012, 14, 569–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jevšnik, M.; Lusa, L.; Uršič, T.; Glinšek Biškup, U.; Petrovec, M. Detection of herpes simplex and varicella-zoster virus from skin lesions: Comparison of RT-PCR and isothermal amplification for rapid identification. Diagn. Microbiol. Infect. Dis. 2020, 97, 115015. [Google Scholar] [CrossRef]
- Kino, Y.; Minamishima, Y. Passive Hemagglutination Assays for the Detection of Antibodies to Herpes Viruses. Microbiol. Immunol. 1993, 37, 365–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trybala, E.; Bergström, T.; Olofsson, S.; Svennerholm, B.; Jeansson, S. An evaluation of a hemagglutination-inhibition test for the detection of antibodies to herpes simplex virus type 1. Clin. Diagn. Virol. 1995, 3, 191–201. [Google Scholar] [CrossRef]
- Zweerink, H.J.; Corey, L. Virus-specific antibodies in sera from patients with genital herpes simplex virus infection. Infect. Immun. 1982, 37, 413–421. [Google Scholar] [CrossRef] [Green Version]
- García-Cisneros, S.; Sánchez-Alemán, M.Á.; Conde-Glez, C.J.; Lara-Zaragoza, S.J.; Herrera-Ortiz, A.; Plett-Torres, T.; Olamendi-Portugal, M. Performance of ELISA and Western blot to detect antibodies against HSV-2 using dried blood spots. J. Infect. Public Health 2019, 12, 224–228. [Google Scholar] [CrossRef]
- Martins, T.B.; Welch, R.J.; Hill, H.R.; Litwin, C.M. Comparison of a multiplexed herpes simplex virus type-specific immunoglobulin G serology assay to immunoblot, Western blot, and enzyme-linked immunosorbent assays. Clin. Vaccine Immunol. 2009, 16, 55–60. [Google Scholar] [CrossRef] [Green Version]
- Golden, M.R.; Ashley-Morrow, R.; Swenson, P.; Hogrefe, W.R.; Handsfield, H.H.; Wald, A. Herpes simplex virus type 2 (HSV-2) Western blot confirmatory testing among men testing positive for HSV-2 using the focus enzyme-linked immunosorbent assay in a sexually transmitted disease clinic. Sex. Transm. Dis. 2005, 32, 771–777. [Google Scholar] [CrossRef]
- Cowan, F.M. Testing for type-specific antibody to herpes simplex virus—Implications for clinical practice. J. Antimicrob. Chemother. 2000, 45, 9–13. [Google Scholar] [CrossRef] [Green Version]
- de Ory, F.; Guisasola, M.E.; Balfagón, P.; Sanz, J.C. Comparison of commercial methods of immunoblot, ELISA, and chemiluminescent immunoassay for detecting type-specific herpes simplex viruses-1 and -2 IgG. J. Clin. Lab. Anal. 2018, 32, e22203. [Google Scholar] [CrossRef]
- Reddy, S.M.; Balakrishnan, P.; Uma, S.; Thyagarajan, S.P.; Solomon, S. Performance of two commercial enzyme-linked immunosorbent assay kits using recombinant glycoprotein G2 antigen for detection of herpes simplex virus type 2 specific antibodies. Clin. Diagn. Lab. Immunol. 2005, 12, 359–360. [Google Scholar] [CrossRef] [Green Version]
- Kimmel, N.; Friedman, M.G.; Sarov, I. Enzyme-linked immunosorbent assay (ELISA) for detection of herpes simplex virus-specific IgM antibodies. J. Virol. Methods 1982, 4, 219–227. [Google Scholar] [CrossRef]
- Clayton, A.L.; Roberts, C.; Godley, M.; Best, J.M.; Chantler, S.M. Herpes simplex virus detection by ELISA: Effect of enzyme amplification, nature of lesion sampled and specimen treatment. J. Med. Virol. 1986, 20, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Hogrefe, W.; Su, X.; Song, J.; Ashley, R.; Kong, L. Detection of Herpes Simplex Virus Type 2-Specific Immunoglobulin G Antibodies in African Sera by Using Recombinant gG2, Western Blotting, and gG2 Inhibition. J. Clin. Microbiol. 2002, 40, 3635–3640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashido, M.; Lee, F.K.; Inouye, S.; Kawana, T. Detection of herpes simplex virus type-specific antibodies by an enzyme-linked immunosorbent assay based on glycoprotein G. J. Med. Virol. 1997, 53, 319–323. [Google Scholar] [CrossRef]
- Mark, H.D.; Nanda, J.P.; Roberts, J.; Rompalo, A.; Melendez, J.H.; Zenilman, J. Performance of focus ELISA tests for HSV-1 and HSV-2 antibodies among university students with no history of genital herpes. Sex. Transm. Dis. 2007, 34, 681–685. [Google Scholar] [CrossRef] [Green Version]
- Ashley, R.L. Sorting out the new HSV type specific antibody tests. Sex. Transm. Infect. 2001, 77, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Görander, S.; Svennerholm, B.; Liljeqvist, J.-Å. Secreted Portion of Glycoprotein G of Herpes Simplex Virus Type 2 Is a Novel Antigen for Type-Discriminating Serology. J. Clin. Microbiol. 2003, 41, 3681–3686. [Google Scholar] [CrossRef] [Green Version]
- Wald, A.; Ashley-Morrow, R. Serological Testing for Herpes Simplex Virus (HSV)–1 and HSV-2 Infection. Clin. Infect. Dis. 2002, 35, S173–S182. [Google Scholar] [CrossRef]
- Ho, D.W.T.; Field, P.R.; Sjögren-Jansson, E.; Jeansson, S.; Cunningham, A.L. Indirect ELISA for the detection of HSV-2 specific IgG and IgM antibodies with glycoprotein G (gG-2). J. Virol. Methods 1992, 36, 249–264. [Google Scholar] [CrossRef]
- Aldisi, R.S.; Elsidiq, M.S.; Dargham, S.R.; Sahara, A.S.; Al-Absi, E.S.; Nofal, M.Y.; Mohammed, L.I.; Abu-Raddad, L.J.; Nasrallah, G.K. Performance evaluation of four type-specific commercial assays for detection of herpes simplex virus type 1 antibodies in a Middle East and North Africa population. J. Clin. Virol. 2018, 103, 1–7. [Google Scholar] [CrossRef] [PubMed]
- van Dyck, E.; Buvé, A.; Weiss, H.A.; Glynn, J.R.; Brown, D.W.G.; De Deken, B.; Parry, J.; Hayes, R.J. Performance of commercially available enzyme immunoassays for detection of antibodies against herpes simplex virus type 2 in African populations. J. Clin. Microbiol. 2004, 42, 2961–2965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, Q.-N.; Zhou, J.-W.; Liu, T.-C.; Lin, G.-F.; Dong, Z.-N.; Chen, Z.-H.; Chen, J.-J.; Wu, Y.-S. Development of a time-resolved fluorescence immunoassay for herpes simplex virus type 1 and type 2 IgG antibodies. Luminescence 2015, 30, 649–654. [Google Scholar] [CrossRef] [PubMed]
- Brenner, N.; Mentzer, A.J.; Butt, J.; Michel, A.; Prager, K.; Brozy, J.; Weißbrich, B.; Aiello, A.E.; Meier, H.C.S.; Breuer, J.; et al. Validation of Multiplex Serology detecting human herpesviruses 1-5. PLoS ONE 2018, 13, e0209379. [Google Scholar] [CrossRef] [PubMed]
- Binnicker, M.J.; Jespersen, D.J.; Harring, J.A. Evaluation of three multiplex flow immunoassays compared to an enzyme immunoassay for the detection and differentiation of IgG class antibodies to herpes simplex virus types 1 and 2. Clin. Vaccine Immunol. 2010, 17, 253–257. [Google Scholar] [CrossRef] [Green Version]
- Burbelo, P.D.; Hoshino, Y.; Leahy, H.; Krogmann, T.; Hornung, R.L.; Iadarola, M.J.; Cohen, J.I. Serological diagnosis of human herpes simplex virus type 1 and 2 infections by luciferase immunoprecipitation system assay. Clin. Vaccine Immunol. 2009, 16, 366–371. [Google Scholar] [CrossRef] [Green Version]
- Burbelo, P.D.; Ching, K.H.; Klimavicz, C.M.; Iadarola, M.J. Antibody profiling by Luciferase Immunoprecipitation Systems (LIPS). J. Vis. Exp. 2009, 32, 1549. [Google Scholar] [CrossRef] [Green Version]
- Burbelo, P.D.; Ching, K.H.; Bren, K.E.; Iadarola, M.J. Searching for biomarkers: Humoral response profiling with luciferase immunoprecipitation systems. Expert Rev. Proteom. 2011, 8, 309–316. [Google Scholar] [CrossRef] [Green Version]
- Zubair, A.; Burbelo, P.D.; Vincent, L.G.; Iadarola, M.J.; Smith, P.D.; Morgan, N.Y. Microfluidic LIPS for serum antibody detection: Demonstration of a rapid test for HSV-2 infection. Biomed. Microdevices 2011, 13, 1053–1062. [Google Scholar] [CrossRef] [Green Version]
- Burbelo, P.D.; Gunti, S.; Keller, J.M.; Morse, C.G.; Deeks, S.G.; Lionakis, M.S.; Kapoor, A.; Li, Q.; Cohen, J.I.; Notkins, A.L.; et al. Ultrarapid Measurement of Diagnostic Antibodies by Magnetic Capture of Immune Complexes. Sci. Rep. 2017, 7, 3818. [Google Scholar] [CrossRef] [Green Version]
- Nath, P.; Kabir, A.; Khoubafarin Doust, S.; Kreais, Z.J.; Ray, A. Detection of Bacterial and Viral Pathogens Using Photonic Point-of-Care Devices. Diagnostics 2020, 10, 841. [Google Scholar] [CrossRef]
- Bissonnette, L.; Bergeron, M.G. Portable devices and mobile instruments for infectious diseases point-of-care testing. Expert Rev. Mol. Diagn. 2017, 17, 471–494. [Google Scholar] [CrossRef]
- Pandey, C.M.; Augustine, S.; Kumar, S.; Kumar, S.; Nara, S.; Srivastava, S.; Malhotra, B.D. Microfluidics Based Point-of-Care Diagnostics. Biotechnol. J. 2018, 13, 1700047. [Google Scholar] [CrossRef] [PubMed]
- Mejía-Salazar, J.R.; Rodrigues Cruz, K.; Materón Vásques, E.M.; Novais de Oliveira, O., Jr. Microfluidic Point-of-Care Devices: New Trends and Future Prospects for eHealth Diagnostics. Sensors 2020, 20, 1951. [Google Scholar] [CrossRef] [Green Version]
- Arshavsky-Graham, S.; Segal, E. Lab-on-a-Chip Devices for Point-of-Care Medical Diagnostics; Springer: Berlin/Heidelberg, Germany, 2020; pp. 1–19. [Google Scholar]
- Sachdeva, S.; Davis, R.W.; Saha, A.K. Microfluidic Point-of-Care Testing: Commercial Landscape and Future Directions. Front. Bioeng. Biotechnol. 2021, 8, 1537. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.M.; Balhoff, J.B.; Landwehr, G.M.; Rahman, S.M.; Vaithiyanathan, M.; Melvin, A.T. Microfluidic and Paper-Based Devices for Disease Detection and Diagnostic Research. Int. J. Mol. Sci. 2018, 19, 2731. [Google Scholar] [CrossRef] [Green Version]
- Garg, N.; Boyle, D.; Randall, A.; Teng, A.; Pablo, J.; Liang, X.; Camerini, D.; Lee, A.P. Rapid immunodiagnostics of multiple viral infections in an acoustic microstreaming device with serum and saliva samples. Lab Chip 2019, 19, 1524–1533. [Google Scholar] [CrossRef] [PubMed]
- Qiu, X.; Zhang, J.; Li, Y.; Zhang, C.; Wang, D.; Zhu, W.; Li, F.; Ge, S.; Xia, N.; Qian, S. A bead-based microfluidic system for joint detection in TORCH screening at point-of-care testing. Microsyst. Technol. 2018, 24, 2007–2015. [Google Scholar] [CrossRef]
- Li, X.; Zhang, Q.; Hou, P.; Chen, M.; Hui, W.; Vermorken, A.; Luo, Z.; Li, H.; Li, Q.; Cui, Y. Gold magnetic nanoparticle conjugate-based lateral flow assay for the detection of IgM class antibodies related to TORCH infections. Int. J. Mol. Med. 2015, 36, 1319–1326. [Google Scholar] [CrossRef]
- Shevlin, E.; Morrow, R.A. Comparative performance of the Uni-GoldTM HSV-2 Rapid: A point-of-care HSV-2 diagnostic test in unselected sera from a reference laboratory. J. Clin. Virol. 2014, 61, 378–381. [Google Scholar] [CrossRef] [Green Version]
- Goux, H.J.; Raja, B.; Kourentzi, K.; Trabuco, J.R.C.; Vu, B.V.; Paterson, A.S.; Kirkpatrick, A.; Townsend, B.; Lee, M.; Truong, V.T.T.; et al. Evaluation of a nanophosphor lateral-flow assay for self-testing for herpes simplex virus type 2 seropositivity. PLoS ONE 2019, 14, e0225365. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Techniques | Sensitivity/LOD | Specificity | Time of Assay | Reference |
|---|---|---|---|---|
| Detection using viral lesions | ||||
| Tzanck smear | 84% | - | - | [26] |
| Viral culture | 100% | - | 5–14 days | [26] |
| Direct fluorescence assay | 61% | 90–100% | 60–90 min | [62] |
| Immunoelectron microscopy | 96% | - | - | [71] |
| Digital holographic microscopy (DHM) | ~160 copies/test | - | 3 h | [36] |
| Microparticle aggregation assay using DHM | ~25 copies/test | - | - | [81] |
| Agglutination assay | ||||
| Latex agglutination assay | 100% | 89% | 3 h | [84] |
| Polymerase chain reaction | >4 h | |||
| qPCR | 15 cp/PCR (HSV-1); 8cp/PCR(HSV-2) | - | [107] | |
| RT-PCR | 100% | 100% | [108] | |
| LightCycler PCR | - | 100% | [109] | |
| Loop-mediated isothermal amplification | 10 copies/tube | - | 75 min | [28] |
| Helicase-dependent amplification | 1.5 h | |||
| IsoAMP® HSV (Biohelix Corp. Beverly, MA, USA) | 97.10% | 93.40% | [40] | |
| AmpliVue HSV 1+2 (Quidel, San diego, CA, USA) | 99.20% | 99.70% | [121] | |
| IsoGlow HSV typing assay | 100% | 98–100% | [126] | |
| Solana HSV1+2/VZV, Quidel, San diego, CA, USA) | 97.7–100% (HSV-1); 92.7–99.1% (HSV-2) | 96.3–98.4% (HSV-1); 94.5–97.3% (HSV-2) | [127] | |
| Detection of antibodies in blood | ||||
| Hemagglutination assay | 97% | 84% | 3 h | [129] |
| Western blot assay | ||||
| Anti-HSV-1/HSV-2-gG2 Euroline-WB, Euroimmun®, Lubeck, Germany | 98% | 65.4–100% | >3 h | [131] |
| Enzyme-linked immunosorbent assay | 2h | |||
| using whole antigen | ||||
| Diamex Immunosimplicity HSV | 100% (HSV-1 and HSV-2) | 71% (HSV-1); 61% (HSV-2) | [26] | |
| HSV-1 or-2 IgG (Inverness) | 98% (HSV-1); 95% (HSV-2) | 68%(HSV-1); 85% (HSV-2) | [26] | |
| HSV-1 or-2 IgG enzyme immunoassay (Zeus Scientific, Raritan, NJ) | 92% (HSV-1); 98% (HSV-2) | 72% (HSV-1); 79% (HSV-2) | [26] | |
| gG-based ELISA | ||||
| HerpeSelect 1 or 2 (Focus Diagnostics, Cypress, CA, USA) | 98% (HSV-1); 100% (HSV-2) | 94.1% (HSV-1); 97.1% (HSV-2) | [26] | |
| Kalon HSV-2 ELISA (Kalon Biological, Guildford, UK) | 100% (HSV-2) | 100% (HSV-2) | [26] | |
| biokitHSV-2 | 99.10% | 93.2–98.7% | [26] | |
| Fluorescence immunoassay | 0.568 AU/mL | - | - | [148] |
| Multiplexed flow immunoassays | 4 h for 180 samples | |||
| AtheNA Multi-Lyte (Zeus Scientific, Raritan,NJ) | 99.2%(HSV-1); 97.4% (HSV-2) | 90.2% (HSV-1); 85.5%(HSV-2) | [150] | |
| BioPlex 2200 (BioRad Laboratories, Hercules, CA) | 99.2% (HSV-1); 98.3% (HSV-2) | 96.2% (HSV-1); 97.4% (HSV-2) | [150] | |
| Plexus HerpeSelect (Focus Diagnostic, Cypress, CA) | 96.5% (HSV-1); 93.2% (HSV-2) | 98.8% (HSV-1); 98.4% (HSV-2) | [150] | |
| Luciferase immunoprecipitation assay | 92% (HSV-1); 100% (HSV-2) | 96% (HSV-2); 100% (HSV-2) | <2.5 h | [151] |
| Microfluidic based POC device | - | |||
| Uni-GoldTM (Trinity Biotech, Bray, Ireland) | 94% | 99% | 15 min | [166] |
| LFIA | 100% | 97.30% | [24] | |
| Nanophosphor-LFIA | 96.70% | 100% | [167] | |
| MicroLIPS | 100% | 100% | <10 min | [154] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nath, P.; Kabir, M.A.; Doust, S.K.; Ray, A. Diagnosis of Herpes Simplex Virus: Laboratory and Point-of-Care Techniques. Infect. Dis. Rep. 2021, 13, 518-539. https://doi.org/10.3390/idr13020049
Nath P, Kabir MA, Doust SK, Ray A. Diagnosis of Herpes Simplex Virus: Laboratory and Point-of-Care Techniques. Infectious Disease Reports. 2021; 13(2):518-539. https://doi.org/10.3390/idr13020049
Chicago/Turabian StyleNath, Peuli, Md Alamgir Kabir, Somaiyeh Khoubafarin Doust, and Aniruddha Ray. 2021. "Diagnosis of Herpes Simplex Virus: Laboratory and Point-of-Care Techniques" Infectious Disease Reports 13, no. 2: 518-539. https://doi.org/10.3390/idr13020049
APA StyleNath, P., Kabir, M. A., Doust, S. K., & Ray, A. (2021). Diagnosis of Herpes Simplex Virus: Laboratory and Point-of-Care Techniques. Infectious Disease Reports, 13(2), 518-539. https://doi.org/10.3390/idr13020049