
COVID-19 and the Endocrine System: A Review of the Current Information and Misinformation

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
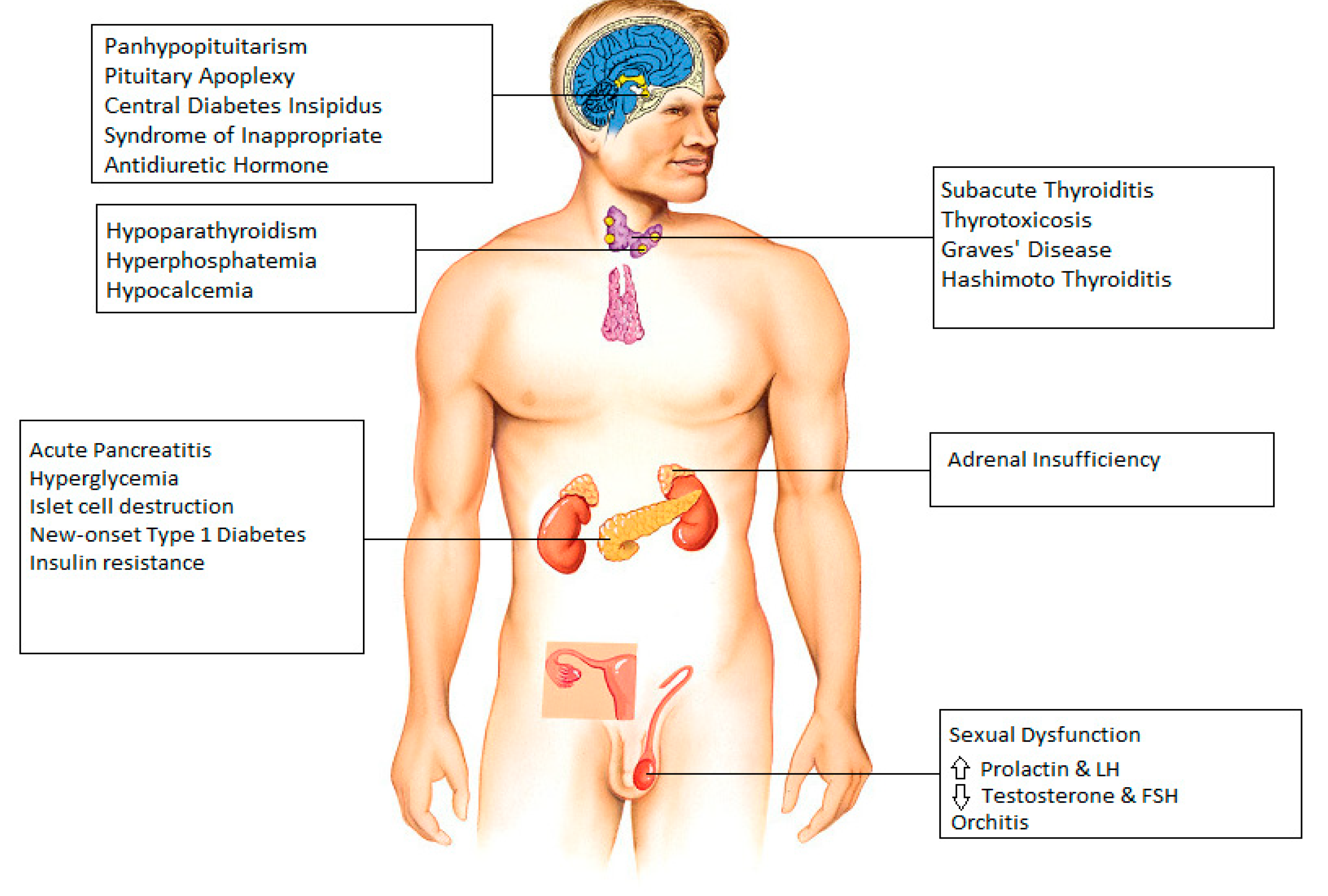
2.1. COVID-19 and Endocrine System
2.2. Hypothalamus and Pituitary
2.3. Thyroid
2.4. Parathyroid
2.5. Pancreas
2.6. Adrenal Gland
2.7. Gonads
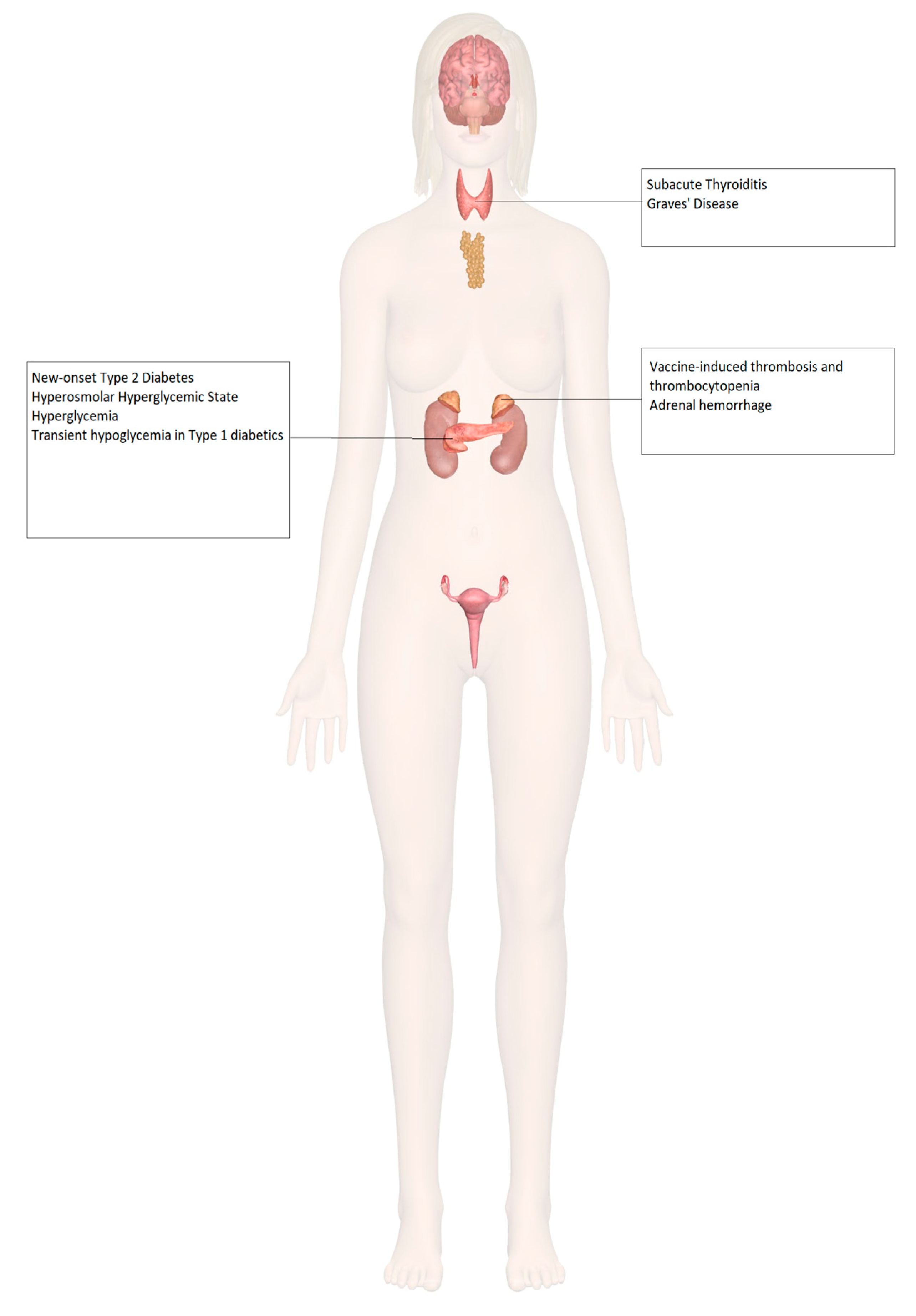
2.8. Endocrinopathies and COVID-19 Vaccines
2.9. Adrenal Insufficiency
2.10. Diabetes Mellitus
2.11. Thyroid Disorders
2.12. Hypogonadism and Infertility
2.13. Osteoporosis
2.14. Misinformation: COVID-19 Vaccine and Endocrine System

{kind=link}
{kind=link}
| Author (Country, Year) | System Involved | Age and Sex of the Patient | Type of Vaccine | Onset of Symptom | Presenting Symptoms | Final Diagnosis | Complications | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Taylor et al. (Wales, 2021) [71] | Adrenal | 38, Male | Astra Zeneca | 8 days after Dose 1 | Severe abdominal pain Vomiting | Vaccine–Induced Thrombosis and Thrombocytopenia with Bilateral Adrenal Hemorrhage | Dural venous sinus thrombosis | Intravenous Immunoglobulin, Hydrocortisone, Argatroban Plasma exchange | Improved platelet count after plasma exchange |
| Boyle et al. (United Kingdom, 2021) [72] | Adrenal | 55, Female | Astra Zeneca | 8 days after Dose 1 | Left iliac fossa pain Vomiting | Left Adrenal Hemorrhage | Thrombo-embolism in both lungs, left basilic vein, and left renal vein | Hydrocortisone Apixaban | Positive response to therapy, conservatively managed further |
| Abu-Rumaileh et al. (Jordan, 2021) [78] | Diabetes | 58, Male | Pfizer/BioNTech | 21 days after Dose 1 (2 days after Dose 2) | Nocturia Polyuria Polydipsia Altered mental status Weight loss | Hyperosmolar Hyperglycemic State | IV Fluids Insulin drip Glargine 50 units daily plus 10 units pre-meal insulin | Insulin tapered and stopped in 4 weeks Metformin continued with good glycemic control | |
| Mishra et al. (India, 2021) [79] | Diabetes | 58, Female | Covishield | 1 day | None Hypertension and tachycardia None | Exacerbation of hyperglycemia in pre-existing Type 2 Diabetes Mellitus | None | Increased dose of Metformin in patient 1 No interventions in patients 2 and 3 | Return to previous blood glucose levels in 1 month, 3 days and 15 days, respectively |
| 64, Male | |||||||||
| 1 day | |||||||||
| 65, Male | 6 days | ||||||||
| Heald et al. (United Kingdom, 2021) [80] | Diabetes | 20 patients Median age 53 (range 26–70), 11 Females, 9 Males | Pfizer/BioNTech [8] Astra Zeneca [12] | 7 days | None | Transient hypoglycemia in Type 1Diabetes Mellitus patients | None | No intervention | Return to previous glucose levels in further 7 days |
| Irlemi et al. (Turkey, 2021) [81] | Thyroid | 35, Female | CoronaVac | 4 days after Dose 2 4 days after Dose 1 7 days after Dose 2 | Anterior neck pain Fever Palpitations Weight loss Fatigue | Subacute Thyroiditis (secondary to ASIA syndrome) | Recurrent myalgia and neck pain in patient 2 | Methylprednisolone 16 mg once daily propranolol 25 mg twice daily No intervention in patient 3 | Complete resolution of symptoms |
| 34, Female | |||||||||
| 37, Female | |||||||||
| Franquemont et al. (USA, 2021) [82] | Thyroid | 42, Female | Pfizer/BioNTech | 5 days after Dose 1 | Sore throat Palpitation Tachycardia | Subacute Thyroiditis | None | Prednisone 40mg daily and Propranolol 20mg as needed | Rapid improvement of symptoms after therapy |
| Oyibo (United Kingdom, 2021) [83] | Thyroid | 55, Female | Astra Zeneca | 21 days after Dose 1 | Neck pain Swelling Headache Sore throat Myalgia Palpitation | Subacute Thyroiditis | None | Levothyroxine 50 mg daily Propranolol | Resolution of symptoms after therapy |
| Sahin et al. (Turkey, 2021) [84] | Thyroid | 67, Male | Subacute Thyroiditis | ||||||
| Vera-Lastra et al. (Mexico, 2021) [86] | Thyroid | 3 days | Grave’s disease |
| Author | Study Design | Criteria | Patient Population | Conclusion | Limitations |
|---|---|---|---|---|---|
| Gonzalez et al. [88]. | Single-center prospective study | Inclusion: Men aged 18–50, no underlying fertility issues. | 45 male participants. | No significant decrease in sperm parameters after 2 doses of COVID-19 vaccination. |
|
| Exclusion: COVID-19 symptoms or positive results within the last 90 days. | |||||
| Lifshitz et al. [89]. | Prospective cohort study | Inclusion: Men < 45 years old, fertile men were considered to be those who had previously successfully impregnated their partners without the use of artificial reproductive technology. | 75 male participants. | Semen parameters found to be within normal parameters after COVID-19 vaccination. |
|
| Exclusion: Previously diagnosed with SARS-CoV-2 infection, taking medications known to be detrimental to semen parameters. | |||||
| Lipkind et al. [93] | Retrospective cohort study | Inclusion: Single-gestation pregnancies. | 46,079 participants. | COVID-19 vaccination during pregnancy was not significantly associated with increased risk for preterm birth overall or SGA at birth |
|
| Exclusion: Age < 16 or >49 years, multiple gestations, no documented care in the health system, implausible gestational age, pregnancy start date outside the prespecified periods. | |||||
| Blakeway et al. [94]. | Retrospective cohort study | Inclusion: Pregnant women with known vaccination status, complete maternal and fetal outcome data. | 1328 Participants. | Similar pregnancy outcomes seen in vaccinated and unvaccinated participants. |
|
| Exclusion: Complicated pregnancies with genetic syndromes, fully vaccinated before getting pregnant. |
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zou, X.; Chen, K.; Zou, J.; Han, P.; Hao, J.; Han, Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front. Med. 2020, 14, 185–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazartigues, E.; Qadir, M.M.F.; Mauvais-Jarvis, F. Endocrine Significance of SARS-CoV-2′s Reliance on ACE2. Endocrinology 2020, 161, bqaa108. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Kruger, N.; Herrler, T.; Erichsen, S.; Pöhlmann, S. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef] [PubMed]
- Brosnahan, S.B.; Jonkman, A.H.; Kugler, M.C.; Munger, J.S.; Kaufman, D.A. COVID-19 and Respiratory System Disorders: Current Knowledge, Future Clinical and Translational Research Questions. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 2586–2597. [Google Scholar] [CrossRef] [PubMed]
- Chigr, F.; Merzouki, M.; Najimi, M. Autonomic Brain Centers and Pathophysiology of COVID-19. ACS Chem. Neurosci. 2020, 11, 1520–1522. [Google Scholar] [CrossRef] [PubMed]
- Poyiadji, N.; Shahin, G.; Noujaim, D.; Stone, M.; Patel, S.; Griffith, B. COVID-19-associated Acute Hemorrhagic Necrotizing Encephalopathy: Imaging Features. Radiology 2020, 296, E119–E120. [Google Scholar] [CrossRef] [Green Version]
- Zhou, L.; Zhang, M.; Wang, J.; Gao, J. Sars-Cov-2: Underestimated damage to nervous system. Travel Med. Infect Dis. 2020, 36, 101642. [Google Scholar] [CrossRef] [PubMed]
- Kaya, M.G.; Ertürk, C.; Güven, M. Pituitary Insufficiency Diagnosed After Coronavirus Disease-19: A Case Report. Erciyes Med. J. 2021, 44, 3. [Google Scholar] [CrossRef]
- Martinez-Perez, R.; Kortz, M.W.; Carroll, B.W.; Duran, D.; Neill, J.S.; Luzardo, G.D.; Zachariah, M.A. Coronavirus Disease 2019 and Pituitary Apoplexy: A Single-Center Case Series and Review of the Literature. World Neurosurg. 2021, 152, e678–e687. [Google Scholar] [CrossRef]
- Zhang, X.; Cai, H.; Hu, J.; Lian, J.; Gu, J.; Zhang, S.; Yang, Y. Epidemiological, clinical characteristics of cases of SARS-CoV-2 infection with abnormal imaging findings. Int. J. Infect. Dis. 2020, 94, 81–87. [Google Scholar] [CrossRef]
- Sheikh, A.B.; Javed, N.; Sheikh, A.A.E.; Upadhyay, S.; Shekhar, R. Diabetes Insipidus and Concomitant Myocarditis: A Late Sequelae of COVID-19 Infection. J. Investig. Med. High Impact Case Rep. 2021, 9, 2324709621999954. [Google Scholar] [CrossRef]
- Ho, K.S.; Narasimhan, B.; Kumar, A.; Flynn, E.; Salonia, J.; El-Hachem, K.; Mathew, J.P. Syndrome of inappropriate antidiuretic hormone as the initial presentation of COVID-19: A novel case report. Nefrol. Engl. Ed. 2021, 41, 219–220. [Google Scholar]
- Yousaf, Z.; Al-Shokri, S.D.; Al-Soub, H.; Mohamed, M.F.H. COVID-19-associated SIADH: A clue in the times of pandemic! Am. J. Physiol.-Endocrinol. Metab. 2020, 318, E882–E885. [Google Scholar] [CrossRef] [PubMed]
- Li, M.Y.; Li, L.; Zhang, Y.; Wang, X.S. Expression of the SARS-CoV-2 cell receptor gene ACE2 in a wide variety of human tissues. Infect. Dis. Poverty 2020, 9, 45. [Google Scholar] [CrossRef]
- Rotondi, M.; Coperchini, F.; Ricci, G.; Denegri, M.; Croce, L.; Ngnitejeu, S.T.; Chiovato, L. Detection of SARS-COV-2 receptor ACE-2 mRNA in thyroid cells: A clue for COVID-19-related subacute thyroiditis. J. Endocrinol. Investig. 2021, 44, 1085–1090. [Google Scholar] [CrossRef]
- Brancatella, A.; Ricci, D.; Viola, N.; Sgro, D.; Santini, F.; Latrofa, F. Subacute Thyroiditis After Sars-COV-2 Infection. J. Clin. Endocrinol. Metab. 2020, 105, 2367–2370. [Google Scholar] [CrossRef] [PubMed]
- Brancatella, A.; Ricci, D.; Cappellani, D.; Viola, N.; Sgro, D.; Santini, F.; Latrofa, F. Is Subacute Thyroiditis an Underestimated Manifestation of SARS-CoV-2 Infection? Insights from a Case Series. J. Clin. Endocrinol. Metab. 2020, 105, e3742–e3746. [Google Scholar] [CrossRef]
- Chakraborty, U.; Ghosh, S.; Chandra, A.; Ray, A.K. Subacute thyroiditis as a presenting manifestation of COVID-19: A report of an exceedingly rare clinical entity. BMJ Case Rep. CP 2020, 13, e239953. [Google Scholar] [CrossRef]
- Lania, A.; Sandri, M.T.; Cellini, M.; Mirani, M.; Lavezzi, E.; Mazziotti, G. Thyrotoxicosis in patients with COVID-19: The THYRCOV study. Eur. J. Endocrinol. 2020, 183, 381–387. [Google Scholar] [CrossRef]
- Mateu-Salat, M.; Urgell, E.; Chico, A. SARS-COV-2 as a trigger for autoimmune disease: Report of two cases of Graves’ disease after COVID-19. J. Endocrinol. Investig. 2020, 43, 1527–1528. [Google Scholar] [CrossRef]
- Muller, I.; Cannavaro, D.; Dazzi, D.; Covelli, D.; Mantovani, G.; Muscatello, A.; Ferrante, E.; Orsi, E.; Resi, V.; Longari, V.; et al. SARS-CoV-2-related atypical thyroiditis. Lancet Diabetes Endocrinol. 2020, 8, 739–741. [Google Scholar] [CrossRef]
- Dixit, N.M.; Truong, K.P.; Rabadia, S.V.; Li, D.; Srivastava, P.K.; Mosaferi, T.; Calfon Press, M.A.; Donangelo, I.; Kelesidis, T. Sudden Cardiac Arrest in a Patient with Myxedema Coma and COVID-19. J. Endocr. Soc. 2020, 4, bvaa130. [Google Scholar] [CrossRef]
- Tee, L.Y.; Harjanto, S.; Rosario, B.H. COVID-19 complicated by Hashimoto’s thyroiditis. Singap. Med. J. 2021, 62, 265. [Google Scholar] [CrossRef] [PubMed]
- Trimboli, P.; Camponovo, C.; Scappaticcio, L.; Bellastella, G.; Piccardo, A.; Rotondi, M. Thyroid sequelae of COVID-19: A systematic review of reviews. Rev. Endocr. Metab. Disord. 2021, 22, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Cippa, P.E.; Cugnata, F.; Ferrari, P.; Brombin, C.; Ruinelli, L.; Bianchi, G.; Beria, N.; Schulz, L.; Bernasconi, E.; Merlani, P.; et al. A data-driven approach to identify risk profiles and protective drugs in COVID-19. Proc. Natl. Acad. Sci. USA 2021, 118, e2016877118. [Google Scholar] [CrossRef]
- Scappaticcio, L.; Pitoia, F.; Esposito, K.; Piccardo, A.; Trimboli, P. Impact of COVID-19 on the thyroid gland: An update. Rev. Endocr. Metab. Disord. 2020, 22, 803–815. [Google Scholar] [CrossRef]
- Ding, Y.; He, L.; Zhang, Q.; Huang, Z.; Che, X.; Hou, J.; Hou, J.; Wang, H.; Shen, H.; Qiu, L.; et al. Organ distribution of severe acute respiratory syndrome (SARS) associated coronavirus (SARS-CoV) in SARS patients: Implications for pathogenesis and virus transmission pathways. J. Pathol. 2004, 203, 622–630. [Google Scholar] [CrossRef]
- He, L.; Ding, Y.; Zhang, Q.; Che, X.; He, Y.; Shen, H.; Wang, H.; Li, Z.; Zhao, L.; Geng, J.; et al. Expression of elevated levels of pro-inflammatory cytokines in SARS-CoV-infected ACE2+ cells in SARS patients: Relation to the acute lung injury and pathogenesis of SARS. J. Pathol. 2006, 210, 288–297. [Google Scholar] [CrossRef]
- Elkattawy, S.; Alyacoub, R.; Ayad, S.; Pandya, M.; Eckman, A. A Novel Case of Hypoparathyroidism Secondary to SARS-CoV-2 Infection. Cureus 2020, 12, e10097. [Google Scholar] [CrossRef]
- Liu, J.; Han, P.; Wu, J.; Gong, J.; Tian, D. Prevalence and predictive value of hypocalcemia in severe COVID-19 patients. J. Infect. Public Health 2020, 13, 1224–1228. [Google Scholar] [CrossRef]
- Liu, F.; Long, X.; Zhang, B.; Zhang, W.; Chen, X.; Zhang, Z. ACE2 Expression in Pancreas May Cause Pancreatic Damage After SARS-CoV-2 Infection. Clin. Gastroenterol. Hepatol. 2020, 18, 2128–2130.e2. [Google Scholar] [CrossRef]
- de Sa, T.C.; Soares, C.; Rocha, M. Acute pancreatitis and COVID-19: A literature review. World, J. Gastrointest. Surg. 2021, 13, 574–584. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A. Hyperglycemia and COVID-19: What was known and what is really new? Diabetes Res. Clin. Pract. 2020, 167, 108383. [Google Scholar] [CrossRef] [PubMed]
- Saand, A.R.; Flores, M.; Kewan, T.; Alqaisi, S.; Alwakeel, M.; Griffiths, L.; Wang, X.; Han, X.; Burton, R.; Al-Jaghbeer, M.J.; et al. Does inpatient hyperglycemia predict a worse outcome in COVID-19 intensive care unit patients? J. Diabetes 2021, 13, 253–260. [Google Scholar] [CrossRef]
- Brufsky, A. Hyperglycemia, hydroxychloroquine, and the COVID-19 pandemic. J. Med. Virol. 2020, 92, 770–775. [Google Scholar] [CrossRef] [Green Version]
- Gianchandani, R.; Esfandiari, N.H.; Ang, L.; Iyengar, J.; Knotts, S.; Choksi, P.; Pop-Busui, R. Managing Hyperglycemia in the COVID-19 Inflammatory Storm. Diabetes 2020, 69, 2048–2053. [Google Scholar] [CrossRef]
- Mao, Y.; Xu, B.; Guan, W.; Xu, D.; Li, F.; Ren, R.; Zhu, X.; Gao, Y.; Jiang, L. The Adrenal Cortex, an Underestimated Site of SARS-CoV-2 Infection. Front. Endocrinol. 2020, 11, 593179. [Google Scholar] [CrossRef] [PubMed]
- Heidarpour, M.; Vakhshoori, M.; Abbasi, S.; Shafie, D.; Rezaei, N. Adrenal insufficiency in coronavirus disease 2019: A case report. J. Med. Case. Rep. 2020, 14, 134. [Google Scholar] [CrossRef]
- Hashim, M.; Athar, S.; Gaba, W.H. New onset adrenal insufficiency in a patient with COVID-19. BMJ Case Rep. CP 2021, 14, e237690. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, A.B.; Javaid, M.A.; Sheikh, A.A.E.; Shekhar, R. Central adrenal insufficiency and diabetes insipidus as potential endocrine manifestations of COVID-19 infection: A case report. Pan Afr. Med. J. 2021, 38, 222. [Google Scholar] [PubMed]
- Pal, R. COVID-19, hypothalamo-pituitary-adrenal axis and clinical implications. Endocrine 2020, 68, 251–252. [Google Scholar] [CrossRef]
- Massarotti, C.; Garolla, A.; Maccarini, E.; Scaruffi, P.; Stigliani, S.; Anserini, P.; Foresta, C. SARS-CoV-2 in the semen: Where does it come from? Andrology 2021, 9, 39–41. [Google Scholar] [CrossRef] [PubMed]
- Selek, A.; Guclu, M.; Bolu, S.E. COVID-19 pandemic: What about the gonads? Hormones Athens 2021, 20, 259–268. [Google Scholar] [CrossRef]
- Dutta, S.; Sengupta, P. SARS-CoV-2 and Male Infertility: Possible Multifaceted Pathology. Reprod. Sci. 2021, 28, 23–26. [Google Scholar] [CrossRef]
- Bhasin, S.; Brito, J.P.; Cunningham, G.R.; Hayes, F.J.; Hodis, H.N.; Matsumoto, A.M.; Snyder, P.J.; Swerdloff, R.S.; Wu, F.C.; Yialamas, M.A. Testosterone Therapy in Men with Hypogonadism: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2018, 103, 1715–1744. [Google Scholar] [CrossRef] [Green Version]
- Seymen, C.M. The other side of COVID-19 pandemic: Effects on male fertility. J. Med. Virol. 2021, 93, 1396–1402. [Google Scholar] [CrossRef]
- Mannur, S.; Jabeen, T.; Khader, M.A.; Rao, L.S.S. Post-COVID-19 Associated Decline in Long-Term Male Fertility and Embryo Quality during Assisted Reproductive Technology. QJM 2021, 114, 328–330. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Bridwell, R.E.; Merrill, D.R.; Griffith, S.A.; Wray, J.; Oliver, J.J. A coronavirus disease 2019 (COVID-19) patient with bilateral orchitis. Am. J. Emerg. Med. 2021, 42, 260.e3–260.e5. [Google Scholar] [CrossRef] [PubMed]
- Segars, J.; Katler, Q.; McQueen, D.B.; Kotlyar, A.; Glenn, T.; Knight, Z.; Feinberg, E.C.; Taylor, H.S.; Toner, J.P.; Kawwass, J.F.L. Prior and novel coronaviruses, Coronavirus Disease 2019 (COVID-19), and human reproduction: What is known? Fertil. Steril. 2020, 113, 1140–1149. [Google Scholar] [CrossRef]
- Stanley, K.E.; Thomas, E.; Leaver, M.; Wells, D. Coronavirus disease-19 and fertility: Viral host entry protein expression in male and female reproductive tissues. Fertil. Steril. 2020, 114, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Luger, A.; Giustina, A.; Peeters, R. European Society of Endocrinology (ESE)’s Statement Concerning COVID 19 Vaccination: ‘Follow the Same Recommendations for Patients with Stable Endocrine Disorders as for the General Population’; European Society of Endocrinology: Bristol, UK, 2021. [Google Scholar]
- Puig-Domingo, M.; Marazuela, M.; Yildiz, B.O.; Giustina, A. COVID-19 and endocrine and metabolic diseases. An updated statement from the European Society of Endocrinology. Endocrine 2021, 72, 301–316. [Google Scholar] [CrossRef] [PubMed]
- Katznelson, L.; Gadelha, M. Glucocorticoid use in patients with adrenal insufficiency following administration of the COVID-19 vaccine: A pituitary society statement. Pituitary 2021, 24, 143–145. [Google Scholar] [CrossRef] [PubMed]
- Fauci, A.S.; Dale, D.C. The effect of in vivo hydrocortisone on subpopulations of human lymphocytes. J. Clin. Investig. 1974, 53, 240–246. [Google Scholar] [CrossRef]
- Fauci, A.S.; Pratt, K.R.; Whalen, G. Activation of human B lymphocytes. IV. Regulatory effects of corticosteroids on the triggering signal in the plaque-forming cell response of human peripheral blood B lymphocytes to polyclonal activation. J. Immunol. 1977, 119, 598–603. [Google Scholar] [PubMed]
- Yasir, M.; Goyal, A.; Bansal, P.; Sonthalia, S. Corticosteroid Adverse Effects; StatPearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- Inoue, S.; Shibata, Y.; Takabatake, N.; Igarashi, A.; Abe, S.; Kubota, I. Influence of corticosteroid therapy on the serum antibody response to influenza vaccine in elderly patients with chronic pulmonary diseases. EXCLI J. 2013, 12, 760–765. [Google Scholar] [PubMed]
- Fischer, L.; Gerstel, P.F.; Poncet, A.; Siegrist, C.A.; Laffitte, E.; Gabay, C.; Seebach, J.D.; Ribi, C. Pneumococcal polysaccharide vaccination in adults undergoing immunosuppressive treatment for inflammatory diseases—A longitudinal study. Arthritis Res. Ther. 2015, 17, 151. [Google Scholar] [CrossRef] [Green Version]
- Yildiz, N.; Sever, L.; Kasapcopur, O.; Cullu, F.; Arisoy, N.; Caliskan, S. Hepatitis B virus vaccination in children with steroid sensitive nephrotic syndrome: Immunogenicity and safety? Vaccine 2013, 31, 3309–3312. [Google Scholar] [CrossRef]
- Taylor, P.; Allen, L.; Shrikrishnapalasuriyar, N.; Stechman, M.; Rees, A. Vaccine-induced thrombosis and thrombocytopenia with bilateral adrenal haemorrhage. Clin. Endocrinol. 2021. [CrossRef]
- Boyle, L.D.; Morganstein, D.L.; Mitra, I.; Nogueira, E.F. A rare case of multiple thrombi and left adrenal haemorrhage following COVID-19 vaccination. Endocr. Abstr. 2021, 74, NCC4. [Google Scholar] [CrossRef]
- Lampasona, V.; Secchi, M.; Scavini, M.; Bazzigaluppi, E.; Brigatti, C.; Marzinotto, I.; Davalli, A.; Caretto, A.; Laurenzi, A.; Martinenghi, S.; et al. Antibody response to multiple antigens of SARS-CoV-2 in patients with diabetes: An observational cohort study. Diabetologia 2020, 63, 2548–2558. [Google Scholar] [CrossRef]
- Frasca, D.; Diaz, A.; Romero, M.; Mendez, N.V.; Landin, A.M.; Ryan, J.G.; Blomberg, B.B. Young and elderly patients with type 2 diabetes have optimal B cell responses to the seasonal influenza vaccine. Vaccine 2013, 31, 3603–3610. [Google Scholar] [CrossRef] [Green Version]
- Li Volti, S.; Caruso-Nicoletti, M.; Biazzo, F.; Sciacca, A.; Mandara, G.; Mancuso, M.; Mollica, F. Hyporesponsiveness to intradermal administration of hepatitis B vaccine in insulin dependent diabetes mellitus. Arch. Dis. Child. 1998, 78, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Looijmans-Van den Akker, I.; Verheij, T.J.; Buskens, E.; Nichol, K.L.; Rutten, G.E.; Hak, E. Clinical effectiveness of first and repeat influenza vaccination in adult and elderly diabetic patients. Diabetes Care 2006, 29, 1771–1776. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.A.; Poland, G.A. Use of influenza and pneumococcal vaccines in people with diabetes. Diabetes Care 2000, 23, 95–108. [Google Scholar] [CrossRef] [Green Version]
- Abu-Rumaileh, M.A.; Gharaibeh, A.M.; Gharaibeh, N.E. COVID-19 Vaccine and Hyperosmolar Hyperglycemic State. Cureus 2021, 13, e14125. [Google Scholar] [CrossRef] [PubMed]
- Mishra, A.; Ghosh, A.; Dutta, K.; Tyagi, K.; Misra, A. Exacerbation of hyperglycemia in patients with type 2 diabetes after vaccination for COVID19: Report of three cases. Diabetes Metab. Syndr. 2021, 15, 102151. [Google Scholar] [CrossRef]
- Heald, A.; Rea, R.; Horne, L.; Metters, A.; Steele, T.; Leivesley, K.; Whyte, M.B.; Stedman, M.; Ollier, W. Analysis of continuous glucose tracking data in people with Type 1 Diabetes (T1DM) after COVID-19 Vaccination reveals unexpected link between immune and metabolic response, augmented by adjunctive oral medication. Int. J. Clin. Pract. 2021, 75, e14714. [Google Scholar] [CrossRef] [PubMed]
- Iremli, B.G.; Sendur, S.N.; Unluturk, U. Three Cases of Subacute Thyroiditis Following SARS-CoV-2 Vaccine: Post-vaccination ASIA Syndrome. J. Clin. Endocrinol. Metab. 2021, 106, 2600–2605. [Google Scholar] [CrossRef]
- Franquemont, S.; Galvez, J. Subacute Thyroiditis After mRNA Vaccine for Covid-19. J. Endocr. Soc. 2021, 5, A956–A957. [Google Scholar] [CrossRef]
- Oyibo, S.O. Subacute Thyroiditis After Receiving the Adenovirus-Vectored Vaccine for Coronavirus Disease (COVID-19). Cureus 2021, 13, e16045. [Google Scholar] [CrossRef] [PubMed]
- Sahin Tekin, M.; Saylisoy, S.; Yorulmaz, G. Subacute thyroiditis following COVID-19 vaccination in a 67-year-old male patient: A case report. Hum. Vaccines Immunother. 2021, 17, 4090–4092. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; Sharif, K.; Shoenfeld, Y. The ASIA syndrome: Basic concepts. Mediterr. J. Rheumatol. 2017, 28, 64–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vera-Lastra, O.; Ordinola Navarro, A.; Cruz Domiguez, M.P.; Medina, G.; Sanchez Valadez, T.I.; Jara, L.J. Two Cases of Graves’ Disease Following SARS-CoV-2 Vaccination: An Autoimmune/Inflammatory Syndrome Induced by Adjuvants. Thyroid 2021, 31, 1436–1439. [Google Scholar] [CrossRef]
- Acheampong, D.O.; Barffour, I.K.; Boye, A.; Aninagyei, E.; Ocansey, S.; Morna, M.T. Male predisposition to severe COVID-19: Review of evidence and potential therapeutic prospects. Biomed. Pharmacother. 2020, 131, 110748. [Google Scholar] [CrossRef]
- Shimabukuro, T.T.; Cole, M.; Su, J.R. Reports of Anaphylaxis After Receipt of mRNA COVID-19 Vaccines in the US-December 14, 2020-January 18, 2021. JAMA 2021, 325, 1101–1102. [Google Scholar] [CrossRef]
- Fischinger, S.; Boudreau, C.M.; Butler, A.L.; Streeck, H.; Alter, G. Sex differences in vaccine-induced humoral immunity. Semin. Immunopathol. 2019, 41, 239–249. [Google Scholar] [CrossRef] [Green Version]
- Ruggieri, A.; Anticoli, S.; D’Ambrosio, A.; Giordani, L.; Viora, M. The influence of sex and gender on immunity, infection and vaccination. Ann. Dell’istituto Super. Sanita 2016, 52, 198–204. [Google Scholar]
- Trigunaite, A.; Dimo, J.; Jorgensen, T.N. Suppressive effects of androgens on the immune system. Cell. Immunol. 2015, 294, 87–94. [Google Scholar] [CrossRef]
- Tsourdi, E.; Yu, E.W.; Jan de Beur, S.M.; Drake, M.T. Vaccination for Coronavirus Disease 2019 (COVID-19) and Relationship to Osteoporosis Care: Current Evidence and Suggested Approaches. J. Bone Miner. Res. 2021, 36, 1042–1047. [Google Scholar] [CrossRef] [PubMed]
- Roozenbeek, J.; Schneider, C.R.; Dryhurst, S.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; Van Der Bles, A.M.; Van Der Linden, S. Susceptibility to misinformation about COVID-19 around the world. R. Soc. Open Sci. 2020, 7, 201199. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Sajjadi, N.B.; Nowlin, W.; Nowlin, R.; Wenger, D.; Beal, J.M.; Vassar, M.; Hartwell, M. United States internet searches for “infertility” following COVID-19 vaccine misinformation. J. Osteopath. Med. 2021, 121, 583–587. [Google Scholar] [CrossRef] [PubMed]
- Berry, S.D.; Johnson, K.S.; Myles, L.; Herndon, L.; Montoya, A.; Fashaw, S.; Gifford, D. Lessons learned from frontline skilled nursing facility staff regarding COVID-19 vaccine hesitancy. J. Am. Geriatr. Soc. 2021, 69, 1140–1146. [Google Scholar] [CrossRef]
- Gonzalez, D.C.; Nassau, D.E.; Khodamoradi, K.; Ibrahim, E.; Blachman-Braun, R.; Ory, J.; Ramasamy, R. Sperm Parameters Before and After COVID-19 mRNA Vaccination. JAMA 2021, 326, 273–274. [Google Scholar] [CrossRef]
- Lifshitz, D.; Haas, J.; Lebovitz, O.; Raviv, G.; Orvieto, R.; Aizer, A. Does mRNA SARS-CoV-2 vaccine detrimentally affect male fertility, as reflected by semen analysis? Reprod. Biomed. Online 2022, 44, 145–149. [Google Scholar] [CrossRef]
- Available online: https://www.deseret.com/u-s-world/2021/2/13/22278041/pregnant-women-covid-19-vaccine-dr-anthony-fauci (accessed on 30 November 2021).
- Gray, K.J.; Bordt, E.A.; Atyeo, C.; Deriso, E.; Akinwunmi, B.; Young, N.; Baez, A.M.; Shook, L.L.; Cvrk, D.; James, K.; et al. COVID-19 vaccine response in pregnant and lactating women: A cohort study. Am. J. Obstet. Gynecol. 2021, 225, 303-e1. [Google Scholar]
- Wang, C.L.; Liu, Y.Y.; Wu, C.H.; Wang, C.Y.; Wang, C.H.; Long, C.Y. Impact of COVID-19 on Pregnancy. Int. J. Med. Sci. 2021, 18, 763–767. [Google Scholar] [CrossRef]
- Lipkind, H.S.; Vazquez-Benitez, G.; DeSilva, M.; Vesco, K.K.; Ackerman-Banks, C.; Zhu, J.; Boyce, T.G.; Daley, M.F.; Fuller, C.C.; Getahun, D.; et al. Receipt of COVID-19 Vaccine During Pregnancy and Preterm or Small-for-Gestational-Age at Birth—Eight Integrated Health Care Organizations, United States, December 15, 2020–July 22, 2021. Morb. Mortal. Wkly. Rep. 2022, 71, 26–30. [Google Scholar] [CrossRef]
- Blakeway, H.; Prasad, S.; Kalafat, E.; Heath, P.T.; Ladhani, S.N.; Le Doare, K.; Magee, L.A.; O’Brien, P.; Rezvani, A.; von Dadelszen, P.; et al. COVID-19 vaccination during pregnancy: Coverage and safety. Am. J. Obstet. Gynecol. 2022, 226, 236.e1–236.e14. [Google Scholar] [CrossRef]
- Zambrano, L.D.; Ellington, S.; Strid, P.; Galang, R.R.; Oduyebo, T.; Tong, V.T.; Woodworth, K.R.; Nahabedian, J.F., III; Azziz-Baumgartner, E.; Gilboa, S.M.; et al. CDC COVID-19 Response Pregnancy and Infant Linked Outcomes Team. Update: Characteristics of symptomatic women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status—United States, January 22–October 3, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1641–1647. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mirza, S.A.; Sheikh, A.A.E.; Barbera, M.; Ijaz, Z.; Javaid, M.A.; Shekhar, R.; Pal, S.; Sheikh, A.B. COVID-19 and the Endocrine System: A Review of the Current Information and Misinformation. Infect. Dis. Rep. 2022, 14, 184-197. https://doi.org/10.3390/idr14020023
Mirza SA, Sheikh AAE, Barbera M, Ijaz Z, Javaid MA, Shekhar R, Pal S, Sheikh AB. COVID-19 and the Endocrine System: A Review of the Current Information and Misinformation. Infectious Disease Reports. 2022; 14(2):184-197. https://doi.org/10.3390/idr14020023
Chicago/Turabian StyleMirza, Samir Ahmed, Abdul Ahad Ehsan Sheikh, Michaela Barbera, Zainab Ijaz, Muhammad Ali Javaid, Rahul Shekhar, Suman Pal, and Abu Baker Sheikh. 2022. "COVID-19 and the Endocrine System: A Review of the Current Information and Misinformation" Infectious Disease Reports 14, no. 2: 184-197. https://doi.org/10.3390/idr14020023
APA StyleMirza, S. A., Sheikh, A. A. E., Barbera, M., Ijaz, Z., Javaid, M. A., Shekhar, R., Pal, S., & Sheikh, A. B. (2022). COVID-19 and the Endocrine System: A Review of the Current Information and Misinformation. Infectious Disease Reports, 14(2), 184-197. https://doi.org/10.3390/idr14020023