
First Molecular Identification of Three Clinical Isolates of Fungi Causing Mucormycosis in Honduras

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
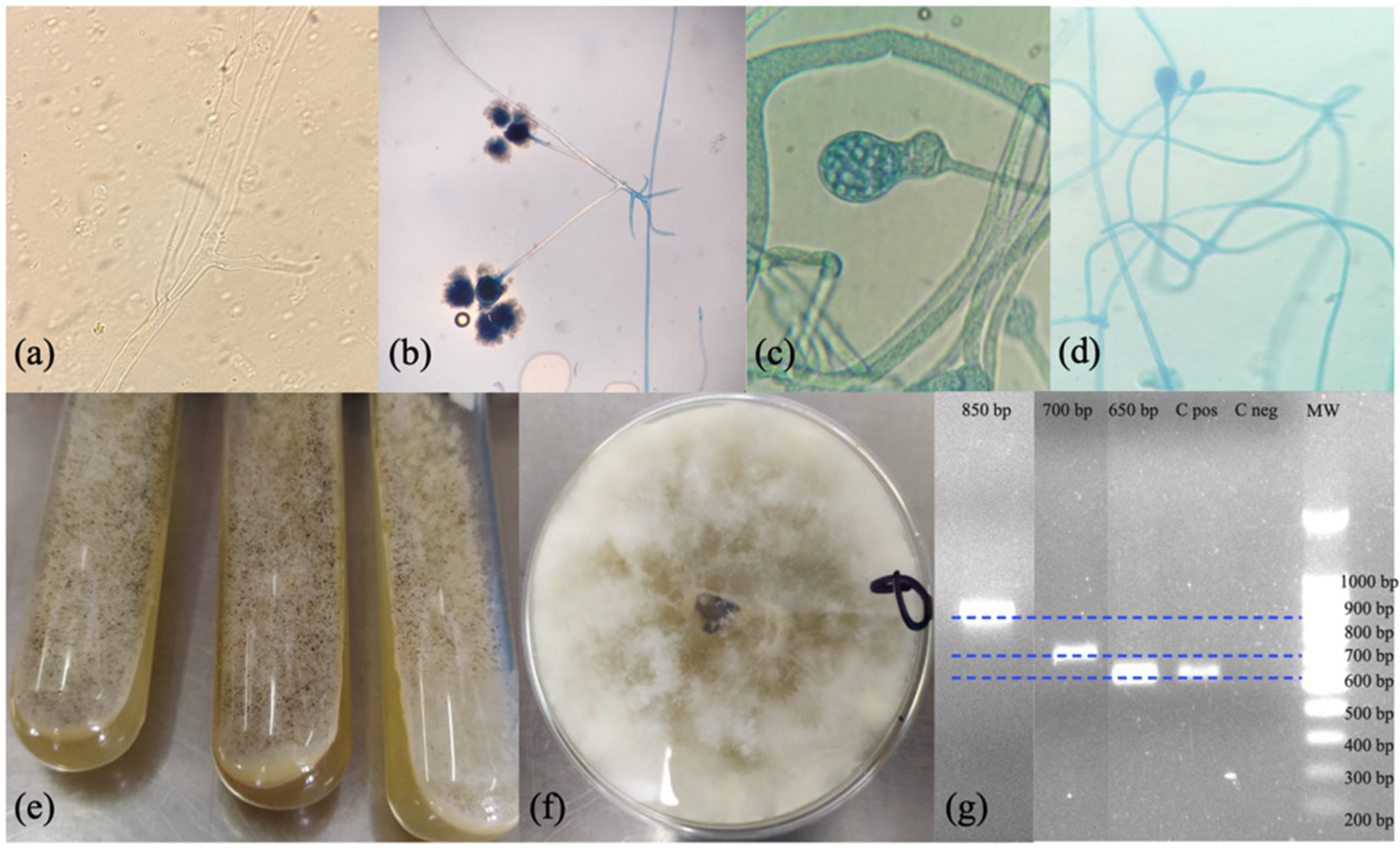
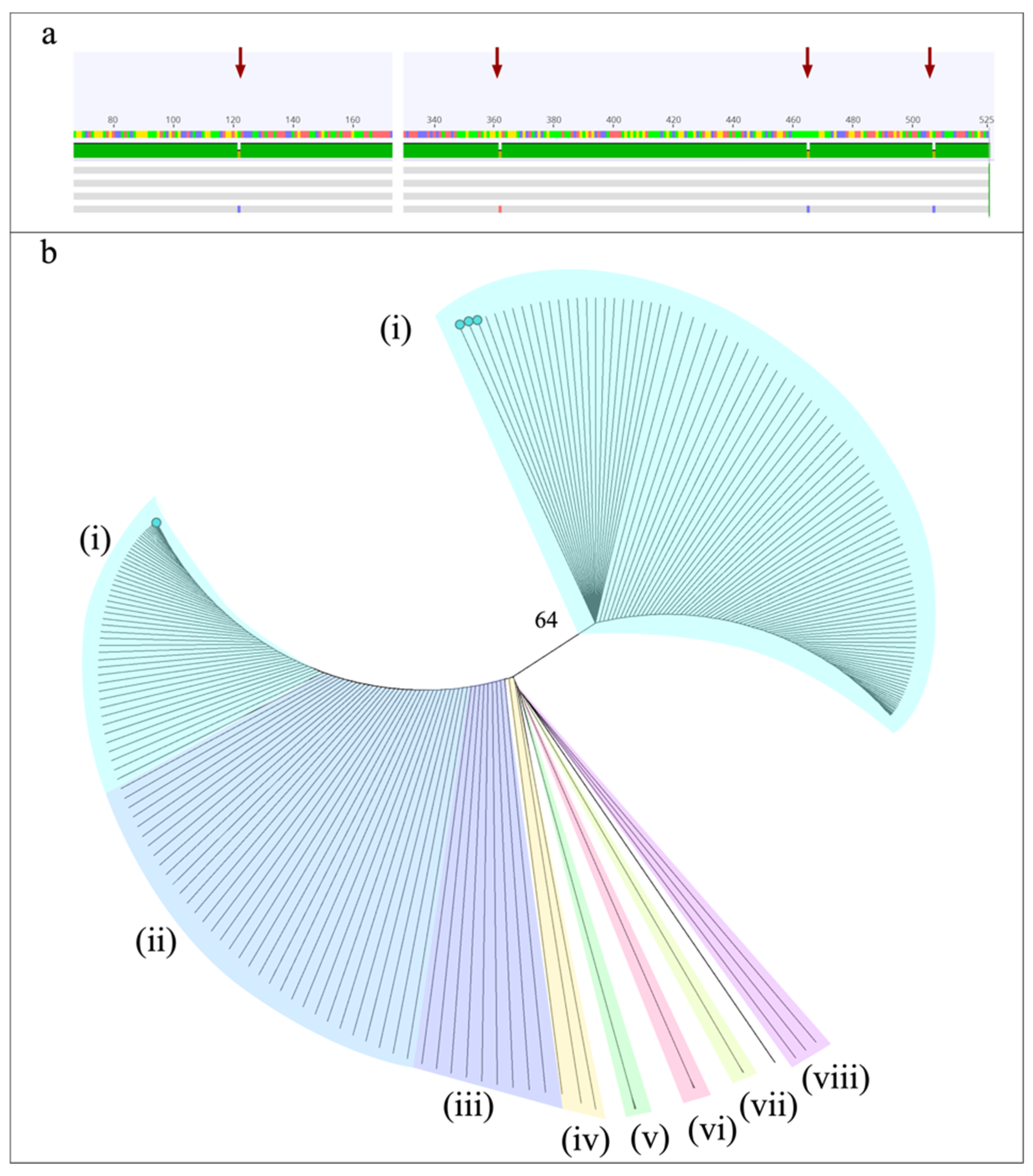
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Skiada, A.; Lass-Floerl, C.; Klimko, N.; Ibrahim, A.; Roilides, E.; Petrikkos, G. Challenges in the diagnosis and treatment of mucormycosis. Med. Mycol. 2018, 56, 93–101. [Google Scholar] [CrossRef] [Green Version]
- Laderas, J.C.P.; Moreno, A.P.; Salido, C.P.; Arista, J.C.R.; Sicilia, M.J.L. Disseminated mucormycosis in immunocompetent patients: A disease that also exists. Rev. Iberoam. Micol. 2015, 32, 63–70. [Google Scholar] [CrossRef]
- Prakash, H.; Chakrabarti, A. Global Epidemiology of Mucormycosis. J. Fungi 2019, 5, 26. [Google Scholar] [CrossRef] [Green Version]
- Prakash, H.; Chakrabarti, A. Epidemiology of Mucormycosis in India. Microorganisms 2021, 9, 523. [Google Scholar] [CrossRef]
- Divakar, P. Fungal Taxa Responsible for Mucormycosis/“Black Fungus” among COVID-19 Patients in India. J. Fungi 2021, 7, 641. [Google Scholar] [CrossRef]
- Walther, G.; Wagner, L.; Kurzai, O. Updates on the Taxonomy of Mucorales with an Emphasis on Clinically Important Taxa. J. Fungi 2019, 5, 106. [Google Scholar] [CrossRef] [Green Version]
- Baskar, H.C.; Chandran, A.; Reddy, C.S.; Singh, S. Rhino-orbital mucormycosis in a COVID-19 patient. BMJ Case Rep. 2021, 14, e244232. [Google Scholar] [CrossRef]
- Prakash, H.; Skiada, A.; Paul, R.; Chakrabarti, A.; Rudramurthy, S. Connecting the Dots: Interplay of Pathogenic Mechanisms between COVID-19 Disease and Mucormycosis. J. Fungi 2021, 7, 616. [Google Scholar] [CrossRef]
- Revannavar, S.M.; Supriya, P.S.; Samaga, L.; Vineeth, V. COVID-19 triggering mucormycosis in a susceptible patient: A new phenomenon in the developing world? BMJ Case Rep. 2021, 14, e241663. [Google Scholar] [CrossRef]
- Rao, V.U.; Arakeri, G.; Madikeri, G.; Shah, A.; Oeppen, R.S.; Brennan, P.A. COVID-19 associated mucormycosis (CAM) in India: A formidable challenge. Br. J. Oral Maxillofac. Surg. 2021, 59, 1095–1098. [Google Scholar] [CrossRef]
- Singh, A.K.; Singh, R.; Joshi, S.R.; Misra, A. Mucormycosis in COVID-19: A systematic review of cases reported worldwide and in India. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102146. [Google Scholar] [CrossRef]
- Guzman-Castro, S.; Chora-Hernandez, L.D.; Trujillo-Alonso, G.; Calvo-Villalobos, I.; Sanchez-Rangel, A.; Ferrer-Alpuin, E.; Ruiz-Jimenez, M.; Corzo-Leon, D.E. COVID-19-associated mucormycosis, diabetes and steroid therapy: Experience in a single centre in Western Mexico. Mycoses 2022, 65, 65–70. [Google Scholar] [CrossRef]
- Meregildo-Rodriguez, E.D.; Espino-Saavedra, W.G. Pediatric rhino-orbital mucormycosis. First peruvian case in times of the COVID-19 pandemic. Rev. Peru. Med. Exp. Salud Publica 2021, 38, 472–473. [Google Scholar] [CrossRef]
- Palou, E.Y.; Ramos, M.A.; Cherenfant, E.; Duarte, A.; Fuentes-Barahona, I.C.; Zambrano, L.I.; Munoz-Lara, F.; Montoya-Ramirez, S.A.; Cardona-Ortiz, A.F.; Valle-Reconco, J.A.; et al. COVID-19 Associated Rhino-Orbital Mucormycosis Complicated by Gangrenous and Bone Necrosis-A Case Report from Honduras. Vaccines 2021, 9, 826. [Google Scholar] [CrossRef]
- Mejia-Santos, H.; Montoya, S.; Chacon-Fuentes, R.; Zielinski-Gutierrez, E.; Lopez, B.; Ning, M.F.; Farach, N.; Garcia-Coto, F.; Rodriguez-Araujo, D.S.; Rosales-Pavon, K.; et al. Notes from the Field: Mucormycosis Cases During the COVID-19 Pandemic-Honduras, May-September 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1747–1749. [Google Scholar] [CrossRef]
- Cornely, O.A.; Alastruey-Izquierdo, A.; Arenz, D.; Chen, S.C.A.; Dannaoui, E.; Hochhegger, B.; Hoenigl, M.; Jensen, H.E.; Lagrou, K.; Lewis, R.E.; et al. Global guideline for the diagnosis and management of mucormycosis: An initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect. Dis. 2019, 19, e405–e421. [Google Scholar] [CrossRef]
- Skiada, A.; Pavleas, I.; Drogari-Apiranthitou, M. Epidemiology and Diagnosis of Mucormycosis: An Update. J. Fungi 2020, 6, 265. [Google Scholar] [CrossRef]
- Schwarz, P.; Bretagne, S.; Gantier, J.C.; Garcia-Hermoso, D.; Lortholary, O.; Dromer, F.; Dannaoui, E. Molecular identification of zygomycetes from culture and experimentally infected tissues. J. Clin. Microbiol. 2006, 44, 340–349. [Google Scholar] [CrossRef] [Green Version]
- Marty, F.M.; Ostrosky-Zeichner, L.; Cornely, O.A.; Mullane, K.M.; Perfect, J.R.; Thompson, G.R.; Alangaden, G.J.; Brown, J.M.; Fredricks, D.N.; Heinz, W.J.; et al. Isavuconazole treatment for mucormycosis: A single-arm open-label trial and case-control analysis. Lancet Infect. Dis. 2016, 16, 828–837. [Google Scholar] [CrossRef]
- Macedo, D.; Leonardelli, F.; Dudiuk, C.; Theill, L.; Cabeza, M.S.; Gamarra, S.; Garcia-Effron, G. Molecular Confirmation of the Linkage between the Rhizopus oryzae CYP51A Gene Coding Region and Its Intrinsic Voriconazole and Fluconazole Resistance. Antimicrob. Agents Chemother. 2018, 62, e00224-18. [Google Scholar] [CrossRef] [Green Version]
- Caramalho, R.; Tyndall, J.D.A.; Monk, B.C.; Larentis, T.; Lass-Florl, C.; Lackner, M. Intrinsic short-tailed azole resistance in mucormycetes is due to an evolutionary conserved aminoacid substitution of the lanosterol 14alpha-demethylase. Sci. Rep. 2017, 7, 15898. [Google Scholar] [CrossRef]
- Dannaoui, E. Antifungal resistance in mucorales. Int. J. Antimicrob. Agents 2017, 50, 617–621. [Google Scholar] [CrossRef]
- Macedo, D.; Leonardelli, F.; Cabeza, M.S.; Gamarra, S.; Garcia-Effron, G. The natural occurring Y129F polymorphism in Rhizopus oryzae (R. arrhizus) Cyp51Ap accounts for its intrinsic voriconazole resistance. Med. Mycol. 2021, 59, 1202–1209. [Google Scholar] [CrossRef]
- De Pauw, B.; Walsh, T.J.; Donnelly, J.P.; Stevens, D.A.; Edwards, J.E.; Calandra, T.; Pappas, P.G.; Maertens, J.; Lortholary, O.; Kauffman, C.A.; et al. Revised Definitions of Invasive Fungal Disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin. Infect. Dis. 2008, 46, 1813–1821. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Montes, K.; Ortiz, B.; Galindo, C.; Figueroa, I.; Braham, S.; Fontecha, G. Identification of Candida Species from Clinical Samples in a Honduran Tertiary Hospital. Pathogens 2019, 8, 237. [Google Scholar] [CrossRef] [Green Version]
- Schoch, C.L.; Seifert, K.A.; Huhndorf, S.; Robert, V.; Spouge, J.L.; Levesque, C.A.; White, M.M. Nuclear ribosomal internal transcribed spacer (ITS) region as a universal DNA barcode marker for Fungi. Proc. Natl. Acad. Sci. USA 2012, 109, 6241–6246. [Google Scholar] [CrossRef] [Green Version]
- Dannaoui, E. Molecular tools for identification of Zygomycetes and the diagnosis of zygomycosis. Clin. Microbiol. Infect. 2009, 15, 66–70. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, T.T.T.; Jeon, Y.J.; Mun, H.Y.; Goh, J.; Chung, N.; Lee, H.B. Isolation and Characterization of Four Unrecorded Mucor Species in Korea. Mycobiology 2019, 48, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Walther, G.; Pawlowska, J.; Alastruey-Izquierdo, A.; Wrzosek, M.; Rodriguez-Tudela, J.L.; Dolatabadi, S.; Chakrabarti, A.; de Hoog, G.S. DNA barcoding in Mucorales: An inventory of biodiversity. Persoonia 2013, 30, 11–47. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Walther, G.; Van Diepeningen, A.D.; Gerrits Van Den Ende, A.H.; Li, R.Y.; Moussa, T.A.; Almaghrabi, O.A.; De Hoog, G.S. DNA barcoding of clinically relevant Cunninghamella species. Med. Mycol. 2015, 53, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A.; Sharma, A.; Chakrabarti, A. The emergence of post-COVID-19 mucormycosis in India: Can we prevent it? Indian J. Ophthalmol. 2021, 69, 1645–1647. [Google Scholar] [CrossRef]
- Jeong, W.; Keighley, C.; Wolfe, R.; Lee, W.L.; Slavin, M.A.; Kong, D.C.M.; Chen, S.C.-A. The epidemiology and clinical manifestations of mucormycosis: A systematic review and meta-analysis of case reports. Clin. Microbiol. Infect. 2019, 25, 26–34. [Google Scholar] [CrossRef] [Green Version]
- Organización Panamericana de la Salud. Alerta Epidemiológica Mucormicosis Asociada a la COVID-19. Available online: https://iris.paho.org/bitstream/handle/10665.2/54284/EpiUpdate11June2021_spa.pdf?sequence=2&isAllowed=y (accessed on 13 January 2022).
- Kermani, W.; Bouttay, R.; Belcadhi, M.; Zaghouani, H.; Ben Ali, M.; Abdelkefi, M. ENT mucormycosis. Report of 4 cases. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2016, 133, 83–86. [Google Scholar] [CrossRef]
- Al-Tarrah, K.; Abdelaty, M.; Behbahani, A.; Mokaddas, E.; Soliman, H.; Albader, A. Cutaneous mucormycosis postcosmetic surgery. Medicine 2016, 95, e4185. [Google Scholar] [CrossRef]
- Bonifaz, A.; Stchigel, A.M.; Guarro, J.; Guevara, E.; Pintos, L.; Sanchis, M.; Cano-Lira, J.F. Primary Cutaneous Mucormycosis Produced by the New Species Apophysomyces mexicanus. J. Clin. Microbiol. 2014, 52, 4428–4431. [Google Scholar] [CrossRef] [Green Version]
- Fanfair, R.N.; Benedict, K.; Bos, J.; Bennett, S.D.; Lo, Y.-C.; Adebanjo, T.; Etienne, K.; Deak, E.; Derado, G.; Shieh, W.-J.; et al. Necrotizing Cutaneous Mucormycosis after a Tornado in Joplin, Missouri, in 2011. N. Engl. J. Med. 2012, 367, 2214–2225. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Herrera, E.; Frias-De-Leon, M.G.; Julian-Castrejon, A.; Cruz-Benitez, L.; Xicohtencatl-Cortes, J.; Hernandez-Castro, R. Rhino-orbital mucormycosis due to Apophysomyces ossiformis in a patient with diabetes mellitus: A case report. BMC Infect. Dis. 2020, 20, 614. [Google Scholar] [CrossRef]
- Alvarez, E.; Stchigel, A.M.; Cano, J.; Sutton, D.A.; Fothergill, A.W.; Chander, J.; Salas, V.; Rinaldi, M.G.; Guarro, J. Molecular phylogenetic diversity of the emerging mucoralean fungus Apophysomyces: Proposal of three new species. Rev. Iberoam. Micol. 2010, 27, 80–89. [Google Scholar] [CrossRef]
- Instituto Nacional del Diabético. ¿Sabías que en Honduras hay 1 Millón de Diabéticos? Available online: https://inadi.gob.hn/sitio/sabias-que-en-honduras-hay-1-millon-de-diabeticos/ (accessed on 13 January 2022).
- OPS Honduras. IV Congreso Nacional de Diabetes. Available online: https://www3.paho.org/hon/index.php?option=com_content&view=article&id=1753:iv-congreso-nacional-de-diabetes&Itemid=260 (accessed on 13 January 2022).
- Despacho de Comunicaciones y Estrategia Presidencial. Resumen de casos en Honduras: COVID19. Available online: http://covid19honduras.org (accessed on 13 January 2022).



{kind=link}
{kind=link}
| Code | Case | Origin | Species ID# | Query Cover | Per. Identity | GenBank Accession Numbers Assigned |
|---|---|---|---|---|---|---|
| IHSS-1 | PM | Clinical sample | Rhizopus oryzae | 100% | 100% | MZ711229 |
| IHSS-3 | PM | Culture | Rhizopus oryzae | 100% | 100% | MZ711233 |
| MCR-1 | ROCM | Culture | Rhizopus delemar/R. oryzae | 100% | 100% | MZ711235 |
| P10 | CM | Culture | Apophysomyces ossiformis | 100% | 100% | OL604794 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortiz, B.; Laínez-Arteaga, I.; Galindo-Morales, C.; Acevedo-Almendárez, L.; Aguilar, K.; Valladares, D.; López, M.; Fontecha, G. First Molecular Identification of Three Clinical Isolates of Fungi Causing Mucormycosis in Honduras. Infect. Dis. Rep. 2022, 14, 258-265. https://doi.org/10.3390/idr14020031
Ortiz B, Laínez-Arteaga I, Galindo-Morales C, Acevedo-Almendárez L, Aguilar K, Valladares D, López M, Fontecha G. First Molecular Identification of Three Clinical Isolates of Fungi Causing Mucormycosis in Honduras. Infectious Disease Reports. 2022; 14(2):258-265. https://doi.org/10.3390/idr14020031
Chicago/Turabian StyleOrtiz, Bryan, Isis Laínez-Arteaga, Celeste Galindo-Morales, Lilia Acevedo-Almendárez, Kateryn Aguilar, Diana Valladares, Miriam López, and Gustavo Fontecha. 2022. "First Molecular Identification of Three Clinical Isolates of Fungi Causing Mucormycosis in Honduras" Infectious Disease Reports 14, no. 2: 258-265. https://doi.org/10.3390/idr14020031
APA StyleOrtiz, B., Laínez-Arteaga, I., Galindo-Morales, C., Acevedo-Almendárez, L., Aguilar, K., Valladares, D., López, M., & Fontecha, G. (2022). First Molecular Identification of Three Clinical Isolates of Fungi Causing Mucormycosis in Honduras. Infectious Disease Reports, 14(2), 258-265. https://doi.org/10.3390/idr14020031