
The Burden of Hepatitis B, Hepatitis C, and Human Immunodeficiency Viruses in Ovarian Cancer Patients in Nairobi, Kenya

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment of Study Participants
2.2. Blood-Serum Sample Collection
2.3. Laboratory Analysis of HBV, HCV, and HIV
2.4. Data Management
3. Results
3.1. Description of Participants’ Baseline Demographic and Clinical Factors
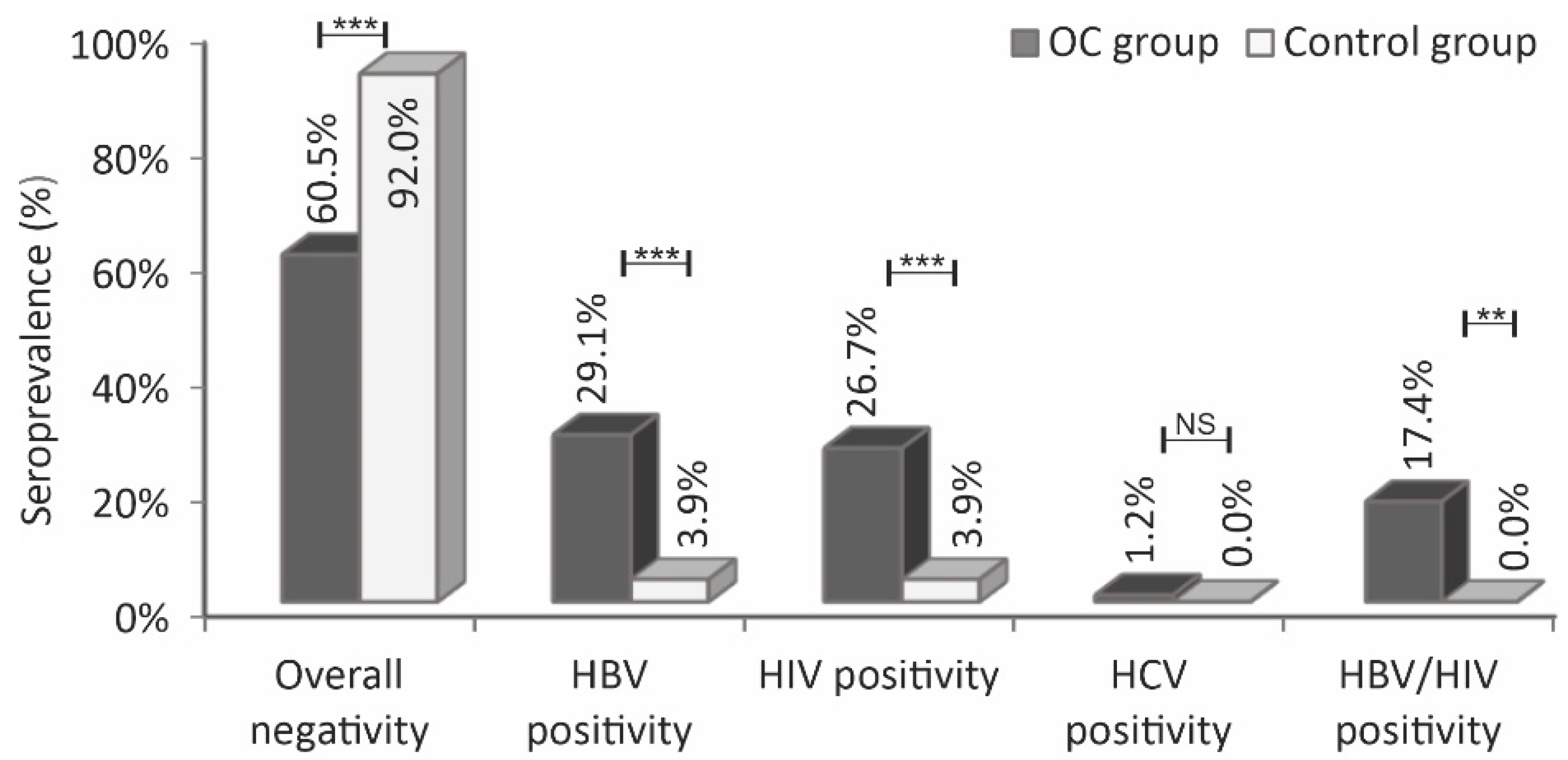
3.2. Comparison of HBV, HCV, HIV, and HBV/HIV Serological Status of the Ovarian Cancer Patients against the Control Subjects
3.3. Association of HBV, HCV, HIV, and HBV/HIV Serological Status of the Participants with Age
3.4. Association of HBV, HCV, HIV, and HBV/HIV Seropositivity Status with the Subjects’ Age Groups (Menopausal Status)
3.5. Association of Ovarian Cancer Patients’ HBV Serological Status with Clinical Factors
3.6. Association of Ovarian Cancer Patients’ HIV Serological Status with Clinical Factors
3.7. Association of Ovarian Cancer Patients’ HBV/HIV Coinfection Status with the Clinical Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Cheserem, E.J.; Kihara, A.-B.; Kosgei, R.J.; Gathara, D.; Gichuhi, S. Ovarian cancer in Kenyatta National Hospital in Kenya: Characteristics and management. Open J. Obstet. Gynecol. 2013, 3, 165–171. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Bryant, C.S.; Chamala, S.; Qazi, A.; Seward, S.; Pal, J.; Steffes, C.P.; Weaver, D.W.; Morris, R.; Malone, J.M.; et al. Ritonavir blocks AKT signaling, activates apoptosis and inhibits migration and invasion in ovarian cancer cells. Mol. Cancer 2009, 8, 26. [Google Scholar] [CrossRef] [Green Version]
- Wanyama, F.M.; Blanchard, V. Glycomic-Based Biomarkers for Ovarian Cancer: Advances and Challenges. Diagnostics 2021, 11, 643. [Google Scholar] [CrossRef]
- Tinelli, A.; Vergara, D.; Martignago, R.; Leo, G.; Malvasi, A.; Tinelli, R.; Marsigliante, S.; Maffia, M.; Lorusso, V. Ovarian cancer biomarkers: A focus on genomic and proteomic findings. Curr. Genom. 2007, 8, 335–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turkoglu, O.; Zeb, A.; Graham, S.; Szyperski, T.; Szender, J.B.; Odunsi, K.; Bahado-Singh, R. Metabolomics of biomarker discovery in ovarian cancer: A systematic review of the current literature. Metab. Off. J. Metab. Soc. 2016, 12, 60. [Google Scholar] [CrossRef] [Green Version]
- Wong, L.; Cheung, T.H.; Yim, S.F.; Lao, T.T. Prevalence and impact of hepatitis B virus infection in ovarian cancer patients in an endemic area-A retrospective cohort study. J. Viral Hepat. 2020, 27, 520–525. [Google Scholar] [CrossRef]
- Levinson, K.L.; Riedel, D.J.; Ojalvo, L.S.; Chan, W.; Angarita, A.M.; Fader, A.N.; Rositch, A.F. Gynecologic cancer in HIV-infected women: Treatment and outcomes in a multi-institutional cohort. AIDS 2018, 32, 171–177. [Google Scholar] [CrossRef]
- de Martel, C.; Georges, D.; Bray, F.; Ferlay, J.; Clifford, G.M. Global burden of cancer attributable to infections in 2018: A worldwide incidence analysis. Lancet Glob. Health 2020, 8, e180–e190. [Google Scholar] [CrossRef] [Green Version]
- Parkin, D.M. The global health burden of infection-associated cancers in the year 2002. Int. J. Cancer 2006, 118, 3030–3044. [Google Scholar] [CrossRef] [Green Version]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [Green Version]
- Ott, J.J.; Stevens, G.A.; Groeger, J.; Wiersma, S.T. Global epidemiology of hepatitis B virus infection: New estimates of age-specific HBsAg seroprevalence and endemicity. Vaccine 2012, 30, 2212–2219. [Google Scholar] [CrossRef] [Green Version]
- Amponsah-Dacosta, E. Hepatitis B virus infection and hepatocellular carcinoma in sub-Saharan Africa: Implications for elimination of viral hepatitis by 2030? World J. Gastroenterol. 2021, 27, 6025–6038. [Google Scholar] [CrossRef]
- Kamiza, A.B.; Su, F.H.; Wang, W.C.; Sung, F.C.; Chang, S.N.; Yeh, C.C. Chronic hepatitis infection is associated with extrahepatic cancer development: A nationwide population-based study in Taiwan. BMC Cancer 2016, 16, 861. [Google Scholar] [CrossRef] [Green Version]
- Mutuma, G.Z.; Mbuchi, M.W.; Zeyhle, E.; Fasana, R.; Okoth, F.A.; Kabanga, J.M.; Kuria, J.; Shiramba, L.; Njenga, M.K.; Osidiana, V. Prevalence of Hepatitis B Virus (HBV) surface antigen and HBVassociated hepatocellular carcinoma in Kenyans of various ages. Afr. J. Health Sci. 2011, 18, 53–61. [Google Scholar]
- Hyams, K.C.; Okoth, F.A.; Tukei, P.M.; Mugambi, M.; Johnson, B.; Morrill, J.C.; Gray, G.C.; Woody, J.N. Epidemiology of hepatitis B in eastern Kenya. J. Med. Virol. 1989, 28, 106–109. [Google Scholar] [CrossRef]
- Bwogi, J.; Braka, F.; Makumbi, I.; Mishra, V.; Bakamutumaho, B.; Nanyunja, M.; Opio, A.; Downing, R.; Biryahwaho, B.; Lewis, R.F. Hepatitis B infection is highly endemic in Uganda: Findings from a national serosurvey. Afr. Health Sci. 2009, 9, 98–108. [Google Scholar] [PubMed]
- Kiire, C.F. The epidemiology and prophylaxis of hepatitis B in sub-Saharan Africa: A view from tropical and subtropical Africa. Gut 1996, 38 (Suppl. 2), S5–S12. [Google Scholar] [CrossRef] [Green Version]
- Tsega, E.; Mengesha, B.; Nordenfelt, E.; Hansson, B.G.; Lindberg, J. Prevalence of hepatitis B virus markers among Ethiopian blood donors: Is HBsAg screening necessary? Trop. Geogr. Med. 1987, 39, 336–340. [Google Scholar]
- Lok, A.S.; McMahon, B.J. Chronic hepatitis B. Hepatology 2001, 34, 1225–1241. [Google Scholar] [CrossRef] [Green Version]
- Pattullo, V. Hepatitis B reactivation in the setting of chemotherapy and immunosuppression-prevention is better than cure. World J. Hepatol. 2015, 7, 954–967. [Google Scholar] [CrossRef] [PubMed]
- Voican, C.; Mir, O.; Loulergue, P.; Dhooge, M.; Brezault, C.; Dréanic, J.; Chaussade, S.; Pol, S.; Coriat, R. Hepatitis B virus reactivation in patients with solid tumors receiving systemic anticancer treatment. Ann. Oncol. 2016, 27, 2172–2183. [Google Scholar] [CrossRef] [PubMed]
- Dunn, G.P.; Bruce, A.T.; Ikeda, H.; Old, L.J.; Schreiber, R.D. Cancer immunoediting: From immunosurveillance to tumor escape. Nat. Immunol. 2002, 3, 991–998. [Google Scholar] [CrossRef]
- Bertoletti, A.; Gehring, A.J. The immune response during hepatitis B virus infection. J. Gen. Virol. 2006, 87, 1439–1449. [Google Scholar] [CrossRef]
- Sureau, C.; Negro, F. The hepatitis delta virus: Replication and pathogenesis. J. Hepatol. 2016, 64 (Suppl. 1), S102–S116. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Hepatitis D. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-d (accessed on 2 June 2022).
- Polish, L.B.; Gallagher, M.; Fields, H.A.; Hadler, S.C. Delta hepatitis: Molecular biology and clinical and epidemiological features. Clin. Microbiol. Rev. 1993, 6, 211–229. [Google Scholar] [CrossRef] [PubMed]
- Kenny-Walsh, E. Clinical outcomes after hepatitis C infection from contaminated anti-D immune globulin. Irish Hepatology Research Group. N. Engl. J. Med. 1999, 340, 1228–1233. [Google Scholar] [CrossRef]
- Refky, B.; Kotb, S.; Fady, T.; Marwan, A.; Abd El-Khalek, D.; Elnahas, W.; Hafez, M.T.; Malik, E.; Soliman, A.A. Impact of liver cirrhosis due to chronic hepatitis C viral infection on the outcome of ovarian cancer: A prospective study. BMC Cancer 2015, 15, 754. [Google Scholar] [CrossRef] [Green Version]
- Muasya, T.; Lore, W.; Yano, K.; Yatsuhashi, H.; Owiti, F.; Fukuda, M.; Tamada, M.; Kulundu, J.; Tukei, J.; Okoth, F. Prevalence of hepatitis C virus and its genotypes among a cohort of drug users in Kenya. East Afr. Med. J. 2008, 85, 318–325. [Google Scholar] [CrossRef] [Green Version]
- Mwangi, J.W. Viral markers in a blood donor population. East Afr. Med. J. 1999, 76, 35–37. [Google Scholar]
- El-Zanaty, F.; Way, A. Egypt demographic and health survey 2008. Egyptian: Ministry of Health. Cairo El-Zanaty Assoc. Macro Int. 2009, FR220, 241–251. [Google Scholar]
- Messina, J.P.; Humphreys, I.; Flaxman, A.; Brown, A.; Cooke, G.S.; Pybus, O.G.; Barnes, E. Global distribution and prevalence of hepatitis C virus genotypes. Hepatology 2015, 61, 77–87. [Google Scholar] [CrossRef] [Green Version]
- Coghill, A.E.; Newcomb, P.A.; Madeleine, M.M.; Richardson, B.A.; Mutyaba, I.; Okuku, F.; Phipps, W.; Wabinga, H.; Orem, J.; Casper, C. Contribution of HIV infection to mortality among cancer patients in Uganda. AIDS 2013, 27, 2933–2942. [Google Scholar] [CrossRef] [Green Version]
- Oliver, N.T.; Chiao, E.Y. Malignancies in women with HIV infection. Curr. Opin. HIV AIDS 2017, 12, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Joint United Programme on HIV/AIDS. 2020 Global AIDS Update; UNAIDS. Available online: https://www.unaids.org/en/resources/documents/2020/global-aids-report (accessed on 2 June 2020).
- World Health Organization. Global HIV & AIDS Statistics—2020 Fact Sheet. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/prevalence-of-hiv-among-adults-aged-15-to-49-(-) (accessed on 3 June 2022).
- Patel, P.; Hanson, D.L.; Sullivan, P.S.; Novak, R.M.; Moorman, A.C.; Tong, T.C.; Holmberg, S.D.; Brooks, J.T. Incidence of types of cancer among HIV-infected persons compared with the general population in the United States, 1992–2003. Ann. Intern. Med. 2008, 148, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Parkin, D.M.; Hämmerl, L.; Ferlay, J.; Kantelhardt, E.J. Cancer in Africa 2018: The role of infections. Int. J. Cancer 2020, 146, 2089–2103. [Google Scholar] [CrossRef]
- Brüning, A.; Burger, P.; Vogel, M.; Rahmeh, M.; Gingelmaiers, A.; Friese, K.; Lenhard, M.; Burges, A. Nelfinavir induces the unfolded protein response in ovarian cancer cells, resulting in ER vacuolization, cell cycle retardation and apoptosis. Cancer Biol. Ther. 2009, 8, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Alter, M.J. Epidemiology of viral hepatitis and HIV co-infection. J. Hepatol. 2006, 44 (Suppl. 1), S6–S9. [Google Scholar] [CrossRef]
- Thio, C.L. Hepatitis B and human immunodeficiency virus coinfection. Hepatology 2009, 49, S138–S145. [Google Scholar] [CrossRef]
- Kerubo, G.; Khamadi, S.; Okoth, V.; Madise, N.; Ezeh, A.; Ziraba, A.; Mwau, M. Hepatitis B, Hepatitis C and HIV-1 Coinfection in Two Informal Urban Settlements in Nairobi, Kenya. PLoS ONE 2015, 10, e0129247. [Google Scholar] [CrossRef] [Green Version]
- Rouet, F.; Chaix, M.L.; Inwoley, A.; Msellati, P.; Viho, I.; Combe, P.; Leroy, V.; Dabis, F.; Rouzioux, C.; ANRS 1236 DITRAME-B&C Study Group. HBV and HCV prevalence and viraemia in HIV-positive and HIV-negative pregnant women in Abidjan, Côte d’Ivoire: The ANRS 1236 study. J. Med. Virol. 2004, 74, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Attia, K.A.; Eholié, S.; Messou, E.; Danel, C.; Polneau, S.; Chenal, H.; Toni, T.; Mbamy, M.; Seyler, C.; Wakasugi, N.; et al. Prevalence and virological profiles of hepatitis B infection in human immunodeficiency virus patients. World J. Hepatol. 2012, 4, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Sagoe, K.W.C.; Agyei, A.A.; Ziga, F.; Lartey, M.; Adiku, T.K.; Seshi, M.; Arens, M.Q.; Mingle, J.A.A. Prevalence and impact of hepatitis B and C virus co-infections in antiretroviral treatment naïve patients with HIV infection at a major treatment center in Ghana. J. Med. Virol. 2012, 84, 6–10. [Google Scholar] [CrossRef]
- Noreh, J.; Sekadde-Kigondu, C.; Karanja, J.G.; Thagana, N.G. Median age at menopause in a rural population of western Kenya. East Afr. Med. J. 1997, 74, 634–638. [Google Scholar]
- Ngaira, J.A.M.; Kimotho, J.; Mirigi, I.; Osman, S. Prevalence, awareness and risk factors associated with Hepatitis B infection among pregnant women attending the antenatal clinic at Mbagathi District Hospital in Nairobi, Kenya. Pan Afr. Med. J. 2016, 24, 315. [Google Scholar] [CrossRef]
- Awole, M.; Gebre-Selassie, S. Seroprevalence of HBsAg and its risk factors amoung pregnant women in Jimma, Southwest Ethiopia. Ethiop. J. Health Dev. 2005, 19, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Day, S.L.; Odem-Davis, K.; Mandaliya, K.N.; Jerome, K.R.; Cook, L.; Masese, L.N.; Scott, J.; Kim, H.N.; Graham, S.M.; McClelland, R.S. Prevalence, clinical and virologic outcomes of hepatitis B virus co-infection in HIV-1 positive Kenyan women on antiretroviral therapy. PLoS ONE 2013, 8, e59346. [Google Scholar]
- Ly, K.N.; Kim, A.A.; Umuro, M.; Drobenuic, J.; Williamson, J.M.; Montgomery, J.M.; Fields, B.S.; Teshale, E.H. Prevalence of Hepatitis B Virus Infection in Kenya, 2007. Am. J. Trop. Med. Hyg. 2016, 95, 348–353. [Google Scholar] [CrossRef] [Green Version]
- Pettigrew, N.M.; Bagshawe, A.F.; Cameron, H.M.; Cameron, C.H.; Dorman, J.M.; MacSween, R.N. Hepatitis B surface antigenaemia in Kenyans with chronic liver disease. Trans. R. Soc. Trop. Med. Hyg. 1976, 70, 462–465. [Google Scholar] [CrossRef]
- Hwang, J.P.; Feld, J.J.; Hammond, S.P.; Wang, S.H.; Alston-Johnson, D.E.; Cryer, D.R.; Hershman, D.L.; Loehrer, A.P.; Sabichi, A.L.; Symington, B.E.; et al. Hepatitis B Virus Screening and Management for Patients With Cancer Prior to Therapy: ASCO Provisional Clinical Opinion Update. J. Clin. Oncol. 2020, 38, 3698–3715. [Google Scholar] [CrossRef]
- Wu, E.S.; Urban, R.R.; Krantz, E.M.; Mugisha, N.M.; Nakisige, C.; Schwartz, S.M.; Gray, H.J.; Casper, C. The association between HIV infection and cervical cancer presentation and survival in Uganda. Gynecol. Oncol. Rep. 2020, 31, 100516. [Google Scholar] [CrossRef] [PubMed]
- McLean, K.; VanDeVen, N.A.; Sorenson, D.R.; Daudi, S.; Liu, J.R. The HIV protease inhibitor saquinavir induces endoplasmic reticulum stress, autophagy, and apoptosis in ovarian cancer cells. Gynecol. Oncol. 2009, 112, 623–630. [Google Scholar] [CrossRef]
- Gills, J.J.; Lopiccolo, J.; Tsurutani, J.; Shoemaker, R.H.; Best, C.J.; Abu-Asab, M.S.; Borojerdi, J.; Warfel, N.A.; Gardner, E.R.; Danish, M.; et al. Nelfinavir, A lead HIV protease inhibitor, is a broad-spectrum, anticancer agent that induces endoplasmic reticulum stress, autophagy, and apoptosis in vitro and in vivo. Clin. Cancer Res. 2007, 13, 5183–5194. [Google Scholar] [CrossRef] [Green Version]
- Subeha, M.R.; Telleria, C.M. The Anti-Cancer Properties of the HIV Protease Inhibitor Nelfinavir. Cancers 2020, 12, 3437. [Google Scholar] [CrossRef] [PubMed]
- Matthews, G.V.; Manzini, P.; Hu, Z.; Khabo, P.; Maja, P.; Matchaba, G.; Sangweni, P.; Metcalf, J.; Pool, N.; Orsega, S. Impact of lamivudine on HIV and hepatitis B virus-related outcomes in HIV/hepatitis B virus individuals in a randomized clinical trial of antiretroviral therapy in southern Africa. AIDS 2011, 25, 1727–1735. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Rapid Advice: Antiretroviral Therapy for HIV Infection in Adults and Adolescents-NOVEMBER 2009. Available online: https://apps.who.int/iris/handle/10665/107280 (accessed on 3 June 2022).


{kind=link}
| Characteristics | OC Group n = 86 | Control Group n = 50 |
|---|---|---|
| Age (years) | ||
| Range | 19–81 | 18–74 |
| Mean ± SD | 50.6 ± 15.6 | 37.9 ± 11.5 |
| Median | 50 | 34.5 |
| Interquartile range | 39–65 | 29–47 |
| Tumor stage % (n) | ||
| FIGO I & II (early stage) | 17.4 (15) | |
| FIGO III & IV (late stage) | 82.6 (71) | |
| Surgical debulking % (n) | ||
| Yes | 44.2 (38) | |
| No | 55.8 (48) | |
| Chemotherapy % (n) | ||
| On chemotherapy | 77.9 (67) | |
| No chemotherapy | 22.1 (19) |
| Infection | OC Group, n = 86 | Control Group, n = 50 | ||||
|---|---|---|---|---|---|---|
| Seropositivity | Seronegativity | p-Value | Seropositivity | Seronegativity | p-Value | |
| HBV | ||||||
| Age range (years) | 19–74 | 20–81 | 0.266 b | 50–59 | 18–74 | 0.026 b |
| Mean ± SD | 52.8 ± 16.1 | 49.7 ± 15.4 | 54.5 ± 6.4 | 37.2 ± 11.2 | ||
| Median | 52 | 49 | 54.5 | 34 | ||
| Interquartile range | 41–68 | 38–61 | - | 28–46 | ||
| HIV | ||||||
| Age range (years) | 28–73 | 19–81 | 0.575 b | 42–47 | 18–74 | 0.320 b |
| Mean ± SD | 51.9 ± 12.9 | 50.1 ± 16.5 | 44.5 ± 3.5 | 37.6 ± 11.6 | ||
| Median | 49 | 51 | 44.5 | 34 | ||
| Interquartile range | 45–60 | 38–65 | - | 28–46 | ||
| HCV | ||||||
| Age range (years) | 38 | 19–81 | 0.442 b | - | 18–74 | |
| Mean ± SD | 38 | 50.7 ± 15.6 | - | 37.9 ± 11.5 | ||
| Median | - | 50.7 | - | 34.5 | ||
| Interquartile range | - | 39–65 | - | 29–47 | ||
| HBV/HIV | ||||||
| Age range (years) | 19–74 | 20–81 | 0.153 b | - | 18–74 | |
| Mean ± SD | 55 ± 13.7 | 46 ± 15.8 | - | 37.9 ± 11.5 | ||
| Median | 55 | 49 | - | 34.5 | ||
| Interquartile range | 48–69 | 38–63 | - | 29–47 | ||
| Sero-Status % (n) | OC Group, n = 86 | Control Group, n = 50 | ||||||
|---|---|---|---|---|---|---|---|---|
| 18–48 Years | >49 Years | OR (95% CI) | p-Value | 18–48 Years | >49 Years | OR (95% CI) | p-Value | |
| HBV | ||||||||
| Seropositivity | 36 (9) | 64 (16) | 1.611 (0.618–4.203) | 0.327 c | 50 (1) | 50 (1) | 5.000 (0.282–88.527) | 0.230 d |
| Seronegativity | 47.5 (29) | 52.5 (32) | 83.3 (40) | 16.7 (8) | ||||
| HIV | ||||||||
| Seropositivity | 39.1(9) | 60.9 (14) | 0.754 (0.285–1.994) | 0.568 c | 100 (2) | 0 (0) | 1.051 (0.981–1.127) | 0.496 d |
| Seronegativity | 46 (29) | 54 (34) | 81.3 (39) | 18.8 (9) | ||||
| HCV | ||||||||
| Seropositivity | 100 (1) | 0 (0) | 1.027 (0.975–1.082) | 0.258 d | - | - | - | - |
| Seronegativity | 43.5 (37) | 56.5 (48) | 82 (41) | 18 (9) | - | |||
| HBV/HIV | ||||||||
| Seropositivity | 26.7 (4) | 73.3 (11) | 2.527 (0.735–8.693) | 0.134 d | - | - | - | - |
| Seronegativity | 47.9 (34) | 52.1 (37) | 82 (41) | 18 (9) | - | |||
| Clinical Factors | HBV Seropositive 29.1% (25) | HBV Seronegative 70.9% (61) | OR (95% CI) | p-Value |
|---|---|---|---|---|
| Tumor stage % (n) | 1.155 (0.330–4.042) | 1.000 c | ||
| Late stage | 24.4 (21) | 58.1 (50) | ||
| Early stage | 4.7 (4) | 12.8 (11) | ||
| Surgical debulking % (n) | 1.243 (0.488–3.163) | 0.648 c | ||
| Done | 14 (12) | 30.2 (26) | ||
| Not done | 15.1 (13) | 40.7 (35) | ||
| Chemotherapy % (n) | 0.858 (0.284–2.586) | 0.785 c | ||
| No chemo | 7 (6) | 15.1 (13) | ||
| On chemo | 22.1 (19) | 55.8 (48) |
| Clinical Factors | HIV Seropositive 26.7% (23) | HIV Seronegative 73.3% (63) | OR (95% CI) | p-Value |
|---|---|---|---|---|
| Tumor stage % (n) | 2.730 (0.566–13.168) | 0.335 d | ||
| Late stage | 24.4 (21) | 58.1 (50) | ||
| Early stage | 2.3 (2) | 15.1 (13) | ||
| Surgical debulking % (n) | 1.222 (0.469–3.187) | 0.681 c | ||
| Yes | 12.8 (11) | 31.4 (27) | ||
| No | 14 (12) | 41.9 (36) | ||
| Chemotherapy % (n) | 0.858 (0.242–2.242) | 0.590 c | ||
| No chemo | 7 (6) | 15.1 (13) | ||
| On chemo | 19.8 (17) | 58.1 (50) |
| Clinical Factors | HBV/HIV Seropositive 17.4 (15) | HBV/HIV Seronegative 82.6 (71) | OR (95% CI) | p-Value |
|---|---|---|---|---|
| Tumor stage % (n) | 1.457 (0.292–7.257) | 1.000 d | ||
| Late stage | 15.1 (13) | 67.4 (58) | ||
| Early stage | 2.3 (2) | 15.1 (13) | ||
| Surgical debulking % (n) | 1.562 (0.510–4.779) | 0.432 c | ||
| Yes | 9.3 (8) | 34.9 (30) | ||
| No | 8.1 (7) | 47.7 (41) | ||
| Chemotherapy % (n) | 1.279 (0.491–3.329) | 0.733 d | ||
| No chemo | 4.7 (4) | 17.4 (15) | ||
| On chemo | 12.8 (11) | 65.1 (56) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wanyama, F.M.; Tauber, R.; Mokomba, A.; Nyongesa, C.; Blanchard, V. The Burden of Hepatitis B, Hepatitis C, and Human Immunodeficiency Viruses in Ovarian Cancer Patients in Nairobi, Kenya. Infect. Dis. Rep. 2022, 14, 433-445. https://doi.org/10.3390/idr14030047
Wanyama FM, Tauber R, Mokomba A, Nyongesa C, Blanchard V. The Burden of Hepatitis B, Hepatitis C, and Human Immunodeficiency Viruses in Ovarian Cancer Patients in Nairobi, Kenya. Infectious Disease Reports. 2022; 14(3):433-445. https://doi.org/10.3390/idr14030047
Chicago/Turabian StyleWanyama, Francis Mugeni, Rudolf Tauber, Alfred Mokomba, Catherine Nyongesa, and Véronique Blanchard. 2022. "The Burden of Hepatitis B, Hepatitis C, and Human Immunodeficiency Viruses in Ovarian Cancer Patients in Nairobi, Kenya" Infectious Disease Reports 14, no. 3: 433-445. https://doi.org/10.3390/idr14030047
APA StyleWanyama, F. M., Tauber, R., Mokomba, A., Nyongesa, C., & Blanchard, V. (2022). The Burden of Hepatitis B, Hepatitis C, and Human Immunodeficiency Viruses in Ovarian Cancer Patients in Nairobi, Kenya. Infectious Disease Reports, 14(3), 433-445. https://doi.org/10.3390/idr14030047