
Ledderhose’s Disease: An Up-to-Date Review of a Rare Non-Malignant Disorder

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
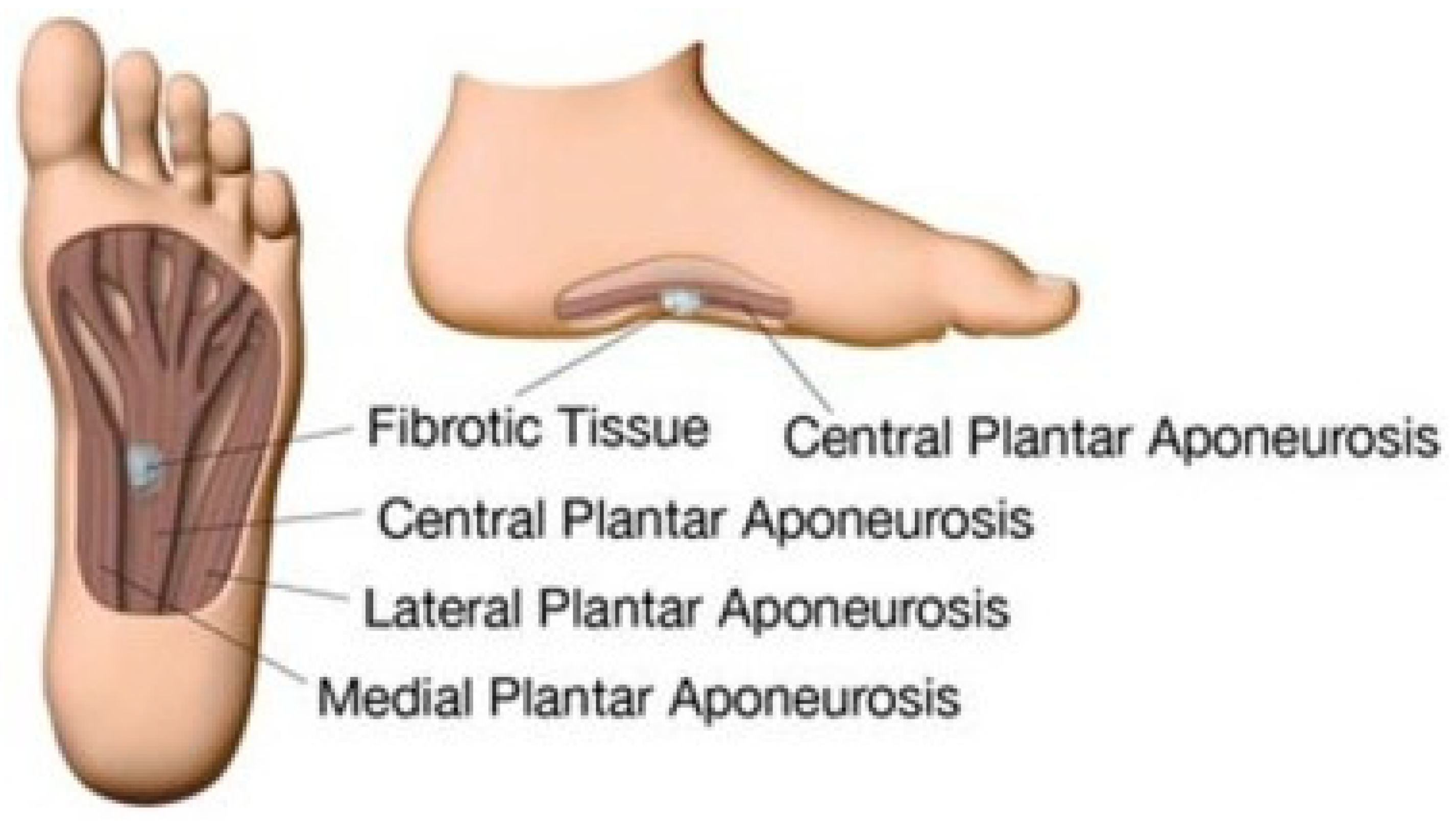
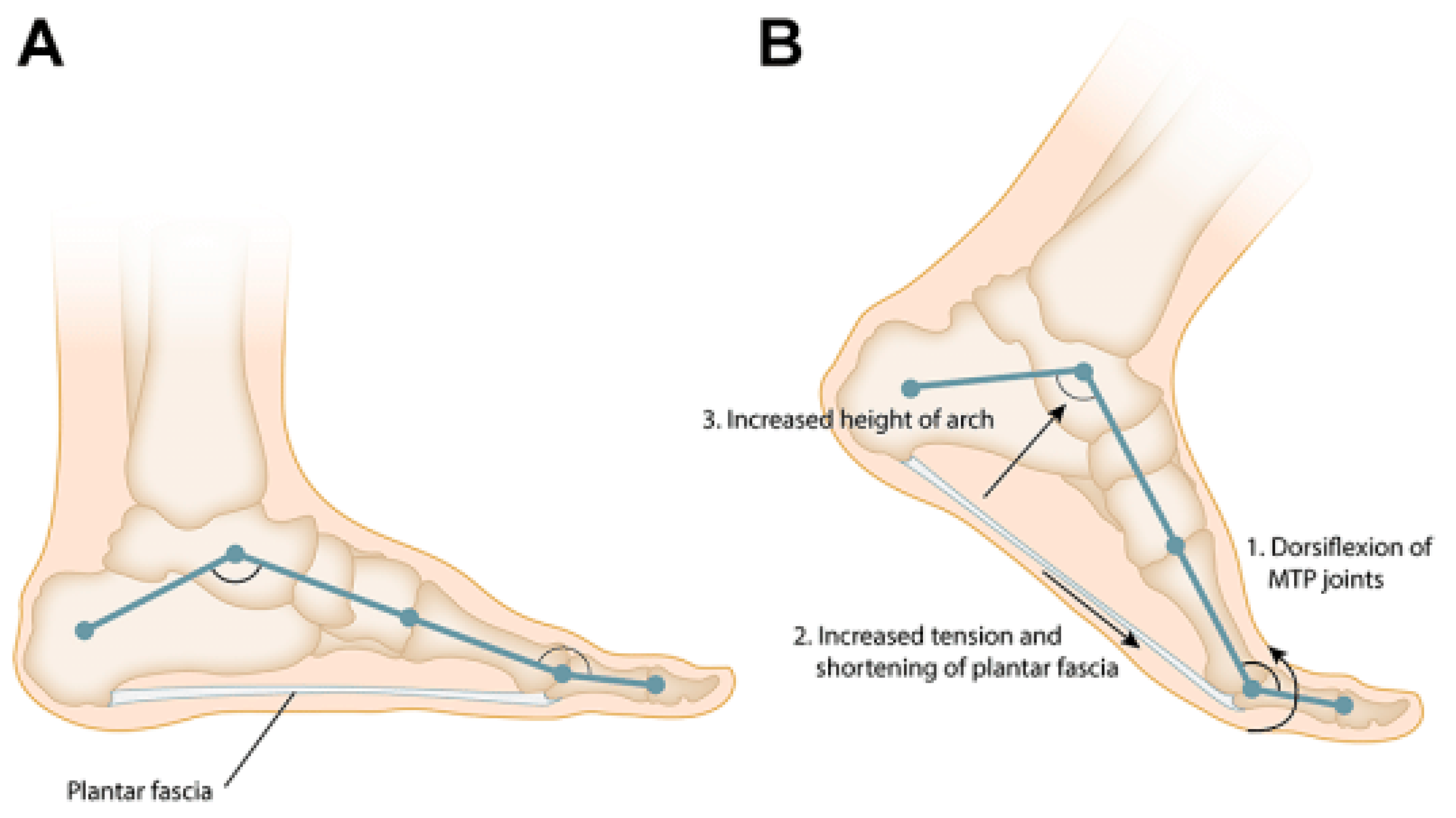
2. Anatomy and Biomechanics of the Plantar Fascia
3. Histology
4. Epidemiology
5. Clinical Presentation
- Grade 1:
- focal lesion with only a small area affected and no skin/muscle involved;
- Grade 2:
- multiple areas which can extend distally/proximally, without any involvement of the skin/muscle;
- Grade 3:
- multiple areas that can extend distally/proximally, with the involvement of skin and/or muscle;
- Grade 4:
- multiple areas that can extend distally/proximally, with the involvement of skin and muscle.
5.1. Imaging
5.2. Differential Diagnosis
6. Non-Operative Management
6.1. Steroid Injections
6.2. Verapamil
6.3. Imatinib
6.4. Radiotherapy
6.5. Extracorporeal Shock Wave Therapy
6.6. Tamoxifen
6.7. Sorafenib
6.8. Mitomycin C
6.9. Collagenase
7. Operative Management
7.1. Endoscopic Subtotal Fasciectomy of the Foot
7.2. Complications after the Surgery
7.3. Recurrence Rate after Excision
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Espert, M.; Anderson, M.R.; Baumhauer, J.F. Current Concepts Review: Plantar Fibromatosis. Foot Ankle Int. 2018, 39, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Goldblum, J.R.; Weiss, A.L.; Folpe, S.W. Benign Fibroblastic/Myofibroblastic Proliferations, Including Superficial Fibromatoses. In Enzinger and Weiss’s Soft Tissue Tumors; Elsevier Health Sciences: Amsterdam, The Netherlands, 2019; pp. 260–263. [Google Scholar]
- Motolese, A.; Mola, F.; Cherubino, M.; Giaccone, M.; Pellegatta, I.; Valdatta, L. Squamous Cell Carcinoma and Ledderhose Disease: A Case Report. Int. J. Low. Extrem. Wounds 2013, 12, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Fausto de Souza, D.; Micaelo, L.; Cuzzi, T.; Ramos-E-Silva, M. Ledderhose Disease: An Unusual Presentation. J. Clin. Aesthetic Dermatol. 2010, 3, 45–47. [Google Scholar]
- Draghi, F.; Gitto, S.; Bortolotto, C.; Draghi, A.G.; Ori Belometti, G. Imaging of Plantar Fascia Disorders: Findings on Plain Radiography, Ultrasound and Magnetic Resonance Imaging. Insights Imaging 2016, 8, 69–78. [Google Scholar] [CrossRef]
- de Haan, A.; Hijmans, J.M.; van der Vegt, A.E.; van der Laan, H.P.; van Nes, J.G.H.; Werker, P.M.N.; Langendijk, J.A.; Steenbakkers, R.J.H.M. Effect of Painful Ledderhose Disease on Dynamic Plantar Foot Pressure Distribution during Walking: A Case-Control Study. Foot Edinb. Scotl. 2023, 56, 101990. [Google Scholar] [CrossRef]
- Jeswani, T.; Morlese, J.; McNally, E.G. Getting to the Heel of the Problem: Plantar Fascia Lesions. Clin. Radiol. 2009, 64, 931–939. [Google Scholar] [CrossRef]
- Rosenbaum, A.J.; DiPreta, J.A.; Misener, D. Plantar Heel Pain. Med. Clin. N. Am. 2014, 98, 339–352. [Google Scholar] [CrossRef]
- Latt, L.D.; Jaffe, D.E.; Tang, Y. Evaluation and Treatment of Chronic Plantar Fasciitis. Foot Ankle Orthop. 2020, 5, 1–11. [Google Scholar] [CrossRef]
- Farsetti, P.; Tudisco, C.; Caterini, R.; Bellocci, M. Ledderhose’s Disease: Case Study with Histologic and Ultrastructural Analysis. Ital. J. Orthop. Traumatol. 1992, 18, 129–133. [Google Scholar]
- Evans, H.L. Multinucleated Giant Cells in Plantar Fibromatosis. Am. J. Surg. Pathol. 2002, 26, 244–248. [Google Scholar] [CrossRef]
- Haun, D.W.; Cho, J.C.S.; Kettner, N.W. Symptomatic Plantar Fibroma with a Unique Sonographic Appearance. J. Clin. Ultrasound JCU 2012, 40, 112–114. [Google Scholar] [CrossRef]
- Adib, O.; Noizet, E.; Croue, A.; Aubé, C. Ledderhose’s Disease: Radiologic/Pathologic Correlation of Superficial Plantar Fibromatosis. Diagn. Interv. Imaging 2014, 95, 893–896. [Google Scholar] [CrossRef] [PubMed]
- Goldblum, J.R.; Fletcher, J.A. Superficial Fibromatoses. In Pathology and Genetics of Tumours of Soft Tissue and Bone; IARC Press: Lyon, France, 2002; Volume 4, pp. 81–82. [Google Scholar]
- Fetsch, J.F.; Laskin, W.B.; Miettinen, M. Palmar-Plantar Fibromatosis in Children and Preadolescents: A Clinicopathologic Study of 56 Cases with Newly Recognized Demographics and Extended Follow-up Information. Am. J. Surg. Pathol. 2005, 29, 1095–1105. [Google Scholar] [CrossRef] [PubMed]
- Godette, G.A.; O’Sullivan, M.; Menelaus, M.B. Plantar Fibromatosis of the Heel in Children: A Report of 14 Cases. J. Pediatr. Orthop. 1997, 17, 16–17. [Google Scholar] [CrossRef] [PubMed]
- Veith, N.T.; Tschernig, T.; Histing, T.; Madry, H. Plantar Fibromatosis—Topical Review. Foot Ankle Int. 2013, 34, 1742–1746. [Google Scholar] [CrossRef] [PubMed]
- de Bree, E.; Zoetmulder, F.A.N.; Keus, R.B.; Peterse, H.L.; van Coevorden, F. Incidence and Treatment of Recurrent Plantar Fibromatosis by Surgery and Postoperative Radiotherapy. Am. J. Surg. 2004, 187, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Pickren, J.W.; Smith, A.G.; Stevenson, T.W.; Stout, A.P. Fibromatosis of the Plantar Fascia. Cancer 1951, 4, 846–856. [Google Scholar] [CrossRef]
- Allen, R.A.; Woolner, L.B.; Ghormley, R.K. Soft-Tissue Tumors of the Sole; with Special Reference to Plantar Fibromatosis. J. Bone Jt. Surg. Am. 1955, 37, 14–26. [Google Scholar] [CrossRef]
- Banerjee, S.; Muhammad, M.S.; Nath, C.; Pal, D. Plantar Fibromatosis: A Case Report. Foot Ankle Online J. 2009, 2, 3. [Google Scholar] [CrossRef]
- Carpenter, B.; Motley, T. McGlamry Comprehensive Textbook of Foot and Ankle Surgery; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011; pp. 710–716. ISBN 978-0-7817-6580-0. [Google Scholar]
- Trybus, M.; Bednarek, M.; Budzyński, P.; Gniadek, M.; Lorkowski, J. Concomitance of Ledderhose’s disease with Dupuytren’s contracture. Own experience. Przegl. Lek. 2012, 69, 663–666. [Google Scholar]
- Adegun, O.K.; Abdelghani, A.; Fortune, F. Oral Manifestation of Plantar–Palmar Fibromatosis. BMJ Case Rep. 2014, 2014, bcr2014204962. [Google Scholar] [CrossRef] [PubMed]
- Amer, A.O.; Jarl, G.M.; Hermansson, L.N. The Effect of Insoles on Foot Pain and Daily Activities. Prosthet. Orthot. Int. 2014, 38, 474–480. [Google Scholar] [CrossRef] [PubMed]
- Wafai, L.; Zayegh, A.; Woulfe, J.; Aziz, S.M.; Begg, R. Identification of Foot Pathologies Based on Plantar Pressure Asymmetry. Sensors 2015, 15, 20392–20408. [Google Scholar] [CrossRef]
- Arts, M.L.J.; Bus, S.A. Twelve Steps per Foot Are Recommended for Valid and Reliable In-Shoe Plantar Pressure Data in Neuropathic Diabetic Patients Wearing Custom Made Footwear. Clin. Biomech. 2011, 26, 880–884. [Google Scholar] [CrossRef] [PubMed]
- Couderc, M.; Kemeny, J.-L.; Lhoste, A.; Soubrier, M.; Dubost, J.-J. Active Plantar Fibromatosis Occurring under Anti-TNFα Therapy for Spondyloarthritis. Joint Bone Spine 2017, 84, 371–372. [Google Scholar] [CrossRef] [PubMed]
- Vandersleyen, V.; Grosber, M.; Wilgenhof, S.; De Kock, J.; Neyns, B.; Gutermuth, J. Vemurafenib-Associated Dupuytren- and Ledderhose Palmoplantar Fibromatosis in Metastatic Melanoma Patients. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1133–1135. [Google Scholar] [CrossRef]
- Sammarco, G.J.; Mangone, P.G. Classification and Treatment of Plantar Fibromatosis. Foot Ankle Int. 2000, 21, 563–569. [Google Scholar] [CrossRef]
- Griffith, J.F.; Wong, T.Y.Y.; Wong, S.M.; Wong, M.W.N.; Metreweli, C. Sonography of Plantar Fibromatosis. AJR Am. J. Roentgenol. 2002, 179, 1167–1172. [Google Scholar] [CrossRef]
- Omor, Y.; Dhaene, B.; Grijseels, S.; Alard, S. Ledderhose Disease: Clinical, Radiological (Ultrasound and MRI), and Anatomopathological Findings. Case Rep. Orthop. 2015, 2015, 741461. [Google Scholar] [CrossRef]
- Cohen, B.E.; Murthy, N.S.; McKenzie, G.A. Ultrasonography of Plantar Fibromatosis: Updated Case Series, Review of the Literature, and a Novel Descriptive Appearance Termed the “Comb Sign”. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2018, 37, 2725–2731. [Google Scholar] [CrossRef]
- McNally, E.G.; Shetty, S. Plantar Fascia: Imaging Diagnosis and Guided Treatment. Semin. Musculoskelet. Radiol. 2010, 14, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Morrison, W.B.; Schweitzer, M.E.; Wapner, K.L.; Lackman, R.D. Plantar Fibromatosis: A Benign Aggressive Neoplasm with a Characteristic Appearance on MR Images. Radiology 1994, 193, 841–845. [Google Scholar] [CrossRef] [PubMed]
- English, C.; Coughlan, R.; Carey, J.; Bergin, D. Plantar and Palmar Fibromatosis: Characteristic Imaging Features and Role of MRI in Clinical Management. Rheumatology 2012, 51, 1134–1136. [Google Scholar] [CrossRef] [PubMed]
- Teo, F.; Shah, M.T.B.M.; Wong, B.S.S. Clinics in diagnostic imaging. Singapore Med. J. 2019, 60, 230–235. [Google Scholar] [CrossRef]
- Miceli, A.J.; Junkins-Hopkins, J.M.; Polley, D.C.; Elston, D.M. Multiple Nodules on the Sole of the Foot. Indian Dermatol. Online J. 2015, 6, 422–424. [Google Scholar] [CrossRef]
- Flanagan, G.; Burt, N.; Reilly, I.N. Intralesional Fenestration and Corticosteroid Injection for Symptomatic Ledderhose Disease of the Foot: Two Case Reports. SAGE Open Med. Case Rep. 2021, 9, 2050313X211011813. [Google Scholar] [CrossRef]
- Spilken, T. Cryotherapy and Other Therapeutical Options for Plantar Fibromatosis. In Dupuytren’s Disease and Related Hyperproliferative Disorders; Springer: Berlin/Heidelberg, Germany, 2012; pp. 401–407. ISBN 978-3-642-22696-0. [Google Scholar]
- Meek, R.M.D.; McLellan, S.; Reilly, J.; Crossan, J.F. The Effect of Steroids on Dupuytren’s Disease: Role of Programmed Cell Death. J. Hand Surg. Edinb. Scotl. 2002, 27, 270–273. [Google Scholar] [CrossRef]
- Ketchum, L.D.; Smith, J.; Robinson, D.W.; Masters, F.W. The Treatment of Hypertrophic Scar, Keloid and Scar Contracture by Triamcinolone Acetonide. Plast. Reconstr. Surg. 1966, 38, 209–218. [Google Scholar] [CrossRef]
- Pentland, A.P.; Anderson, T.F. Plantar Fibromatosis Responds to Intralesional Steroids. J. Am. Acad. Dermatol. 1985, 12, 212–214. [Google Scholar] [CrossRef]
- Carroll, P.; Henshaw, R.M.; Garwood, C.; Raspovic, K.; Kumar, D. Plantar Fibromatosis: Pathophysiology, Surgical and Nonsurgical Therapies: An Evidence-Based Review. Foot Ankle Spec. 2018, 11, 168–176. [Google Scholar] [CrossRef]
- Young, J.R.; Sternbach, S.; Willinger, M.; Hutchinson, I.D.; Rosenbaum, A.J. The Etiology, Evaluation, and Management of Plantar Fibromatosis. Orthop. Res. Rev. 2019, 11, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Dufresne, A.; Penel, N.; Salas, S.; Le Cesne, A.; Perol, D.; Bui, B.; Brain, E.; Ray-Coquard, I.; Jimenez, M.; Blay, J. Updated Outcome with Long-Term Follow-up of Imatinib for the Treatment of Progressive or Recurrent Aggressive Fibromatosis (Desmoid Tumor): A FNCLCC/ French Sarcoma Group Phase II Trial. J. Clin. Oncol. 2009, 27, 10518. [Google Scholar] [CrossRef]
- Jansen, J.T.M.; Broerse, J.J.; Zoetelief, J.; Klein, C.; Seegenschmiedt, H.M. Estimation of the Carcinogenic Risk of Radiotherapy of Benign Diseases from Shoulder to Heel. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2005, 76, 270–277. [Google Scholar] [CrossRef]
- Schuster, J.; Saraiya, S.; Tennyson, N.; Nedelka, M.; Mukhopadhyay, N.; Weiss, E. Patient-Reported Outcomes after Electron Radiation Treatment for Early-Stage Palmar and Plantar Fibromatosis. Pract. Radiat. Oncol. 2015, 5, e651–e658. [Google Scholar] [CrossRef] [PubMed]
- de Haan, A.; van Nes, J.G.H.; Werker, P.M.N.; Langendijk, J.A.; Steenbakkers, R.J.H.M. Radiotherapy for Patients with Ledderhose Disease: Long-Term Effects, Side Effects and Patient-Rated Outcome. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2022, 168, 83–88. [Google Scholar] [CrossRef]
- Chu, C.-N.; Hu, K.-C.; Wu, R.S.-C.; Bau, D.-T. Radiation-Irritated Skin and Hyperpigmentation May Impact the Quality of Life of Breast Cancer Patients after Whole Breast Radiotherapy. BMC Cancer 2021, 21, 330. [Google Scholar] [CrossRef] [PubMed]
- Aqil, A.; Siddiqui, M.R.S.; Solan, M.; Redfern, D.J.; Gulati, V.; Cobb, J.P. Extracorporeal Shock Wave Therapy Is Effective in Treating Chronic Plantar Fasciitis: A Meta-Analysis of RCTs. Clin. Orthop. 2013, 471, 3645–3652. [Google Scholar] [CrossRef]
- Lou, J.; Wang, S.; Liu, S.; Xing, G. Effectiveness of Extracorporeal Shock Wave Therapy Without Local Anesthesia in Patients With Recalcitrant Plantar Fasciitis: A Meta-Analysis of Randomized Controlled Trials. Am. J. Phys. Med. Rehabil. 2017, 96, 529–534. [Google Scholar] [CrossRef]
- Schmitz, C.; Császár, N.B.; Rompe, J.-D.; Chaves, H.; Furia, J.P. Treatment of Chronic Plantar Fasciopathy with Extracorporeal Shock Waves (Review). J. Orthop. Surg. 2013, 8, 31. [Google Scholar] [CrossRef]
- Wang, C.-J. Extracorporeal Shockwave Therapy in Musculoskeletal Disorders. J. Orthop. Surg. 2012, 7, 11. [Google Scholar] [CrossRef]
- Capogrosso, P.; Frey, A.; Jensen, C.F.S.; Rastrelli, G.; Russo, G.I.; Torremade, J.; Albersen, M.; Gruenwald, I.; Reisman, Y.; Corona, G. Low-Intensity Shock Wave Therapy in Sexual Medicine-Clinical Recommendations from the European Society of Sexual Medicine (ESSM). J. Sex. Med. 2019, 16, 1490–1505. [Google Scholar] [CrossRef] [PubMed]
- Abdulsalam, A.J.; Shehab, D.; Elhady, A.A.; Abraham, M. High-Energy Focused Extracorporeal Shockwave Therapy Relieved Pain in Dupuytren’s Disease: A Series of Seven Hands. Eur. J. Phys. Rehabil. Med. 2019, 55, 862–864. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, A.; Imbimbo, C.; Longo, N.; Fusco, F.; Verze, P.; Mangiapia, F.; Creta, M.; Mirone, V. A First Prospective, Randomized, Double-Blind, Placebo-Controlled Clinical Trial Evaluating Extracorporeal Shock Wave Therapy for the Treatment of Peyronie’s Disease. Eur. Urol. 2009, 56, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Frizziero, A.; Barazzuol, M.; Vittadini, F.; Bellon, G.; Masiero, S.; Meneghini, A. Plantar Fascial Fibromatosis: Two Cases Treated With Low-Energy Focused Shock Waves. J. Clin. Rheumatol. Pract. Rep. Rheum. Musculoskelet. Dis. 2017, 23, 63–65. [Google Scholar] [CrossRef] [PubMed]
- Knobloch, K.; Vogt, P.M. High-Energy Focussed Extracorporeal Shockwave Therapy Reduces Pain in Plantar Fibromatosis (Ledderhose’s Disease). BMC Res. Notes 2012, 5, 542. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.T.; Yoon, K.J.; Park, C.-H.; Choi, J.H.; Park, H.-J.; Park, Y.S.; Lee, Y.-T. Follow-up of Clinical and Sonographic Features after Extracorporeal Shock Wave Therapy in Painful Plantar Fibromatosis. PLoS ONE 2020, 15, e0237447. [Google Scholar] [CrossRef]
- Reilly, J.M.; Bluman, E.; Tenforde, A.S. Effect of Shockwave Treatment for Management of Upper and Lower Extremity Musculoskeletal Conditions: A Narrative Review. PM&R 2018, 10, 1385–1403. [Google Scholar] [CrossRef]
- Ogden, J.A.; Alvarez, R.G.; Levitt, R.; Marlow, M. Shock Wave Therapy (Orthotripsy) in Musculoskeletal Disorders. Clin. Orthop. 2001, 387, 22–40. [Google Scholar] [CrossRef]
- Frairia, R.; Berta, L. Biological Effects of Extracorporeal Shock Waves on Fibroblasts. A Review. Muscles Ligaments Tendons J. 2011, 1, 138–147. [Google Scholar]
- Okano, J.; Arakawa, A.; Ogino, S.; Suzuki, Y. Bilateral Plantar Fibromatosis Complicated by Dupuytren’s Contracture. J. Surg. Case Rep. 2020, 2020, rjz402. [Google Scholar] [CrossRef]
- Schoenfeld, J.D.; Agaram, N.P.; Lefkowitz, R.A.; Kelly, C.M.; Healey, J.H.; Gounder, M.M. Sorafenib in Dupuytren and Ledderhose Disease. Oncologist 2022, 27, e294–e296. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.A. Antifibrosis Agents and Glaucoma Surgery. Investig. Ophthalmol. Vis. Sci. 1994, 35, 3789–3791. [Google Scholar]
- Sanders, K.W.; Gage-White, L.; Stucker, F.J. Topical Mitomycin C in the Prevention of Keloid Scar Recurrence. Arch. Facial Plast. Surg. 2005, 7, 172–175. [Google Scholar] [CrossRef] [PubMed]
- Shields, C.L.; Naseripour, M.; Shields, J.A. Topical Mitomycin C for Extensive, Recurrent Conjunctival-Corneal Squamous Cell Carcinoma. Am. J. Ophthalmol. 2002, 133, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Echechipía, S.; Alvarez, M.J.; García, B.E.; Olaguíbel, J.M.; Rodriguez, A.; Lizaso, M.T.; Acero, S.; Tabar, A.I. Generalized Dermatitis Due to Mitomycin C Patch Test. Contact Dermat. 1995, 33, 432. [Google Scholar] [CrossRef]
- Cumurcu, T.; Sener, S.; Cavdar, M. Periocular Allergic Contact Dermatitis Following Topical Mitomycin C Eye Drop Application. Cutan. Ocul. Toxicol. 2011, 30, 239–240. [Google Scholar] [CrossRef]
- Palmer, S.S. Mitomycin as Adjunct Chemotherapy with Trabeculectomy. Ophthalmology 1991, 98, 317–321. [Google Scholar] [CrossRef]
- Rahbar, R.; Shapshay, S.M.; Healy, G.B. Mitomycin: Effects on Laryngeal and Tracheal Stenosis, Benefits, and Complications. Ann. Otol. Rhinol. Laryngol. 2001, 110, 1–6. [Google Scholar] [CrossRef]
- Ingrams, D.R.; Volk, M.S.; Biesman, B.S.; Pankratov, M.M.; Shapshay, S.M. Sinus Surgery: Does Mitomycin C Reduce Stenosis? Laryngoscope 1998, 108, 883–886. [Google Scholar] [CrossRef]
- Amer, K.M.; Mohamed, S.; Amer, R.; Chaudhry, A.; Winters, B.; Abraham, J.A. Effect of Mitomycin C on Recurrence of Plantar Fibromas. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2018, 36, 2554–2561. [Google Scholar] [CrossRef]
- De Vitis, R.; Passiatore, M.; Perna, A.; Starnoni, M.; Taccardo, G. Unusual Intranodular Collagenase Injection: A Case of Bilateral Ledderhose Disease. Plast. Reconstr. Surg. Glob. Open 2020, 8, e2754. [Google Scholar] [CrossRef] [PubMed]
- Hammoudeh, Z.S. Collagenase Clostridium Histolyticum Injection for Plantar Fibromatosis (Ledderhose Disease). Plast. Reconstr. Surg. 2014, 134, 497e–499e. [Google Scholar] [CrossRef] [PubMed]
- Denkler, K.A.; Vaughn, C.J.; Dolan, E.L.; Hansen, S.L. Evidence-Based Medicine: Options for Dupuytren’s Contracture: Incise, Excise, and Dissolve. Plast. Reconstr. Surg. 2017, 139, 240e–255e. [Google Scholar] [CrossRef] [PubMed]
- Beckmann, J.; Kalteis, T.; Baer, W.; Grifka, J.; Lerch, K. Plantar fibromatosis: Therapy by total plantarfasciectomy. Zentralbl. Chir. 2004, 129, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Chen, Q.; Shen, H.; Shen, X.; Wu, S. Fibroma of Tendon Sheath in Planta. SpringerPlus 2016, 5, 575. [Google Scholar] [CrossRef]
- van der Veer, W.M.; Hamburg, S.M.; de Gast, A.; Niessen, F.B. Recurrence of Plantar Fibromatosis after Plantar Fasciectomy: Single-Center Long-Term Results. Plast. Reconstr. Surg. 2008, 122, 486–491. [Google Scholar] [CrossRef]
- Dürr, H.R.; Krödel, A.; Trouillier, H.; Lienemann, A.; Refior, H.J. Fibromatosis of the Plantar Fascia: Diagnosis and Indications For Surgical Treatment. Foot Ankle Int. 1999, 20, 13–17. [Google Scholar] [CrossRef]
- Aluisio, F.V.; Mair, S.D.; Hall, R.L. Plantar Fibromatosis: Treatment of Primary and Recurrent Lesions and Factors Associated with Recurrence. Foot Ankle Int. 1996, 17, 672–678. [Google Scholar] [CrossRef]
- Wapner, K.L.; Ververeli, P.A.; Moore, J.H.; Hecht, P.J.; Becker, C.E.; Lackman, R.D. Plantar Fibromatosis: A Review of Primary and Recurrent Surgical Treatment. Foot Ankle Int. 1995, 16, 548–551. [Google Scholar] [CrossRef]
- Pontious, J.; Flanigan, K.P.; Hillstrom, H.J. Role of the Plantar Fascia in Digital Stabilization. A Case Report. J. Am. Podiatr. Med. Assoc. 1996, 86, 43–47. [Google Scholar] [CrossRef]
- Kan, H.J.; Hovius, S.E.R. Long-Term Follow-up of Flaps for Extensive Dupuytren’s and Ledderhose Disease in One Family. J. Plast. Reconstr. Aesthetic Surg. JPRAS 2012, 65, 1741–1745. [Google Scholar] [CrossRef] [PubMed]
- Neagu, T.P.; Tiglis, M.; Popescu, A. Clinical, histological and therapeutic modern approach of Ledderhose disease. Rom. J. Morphol. Embryol. 2018, 59, 691–697. [Google Scholar] [PubMed]
- Lui, T.H. Endoscopic Subtotal Fasciectomy of the Foot. Arthrosc. Tech. 2016, 5, e1387–e1393. [Google Scholar] [CrossRef] [PubMed]
- Fuiano, M.; Mosca, M.; Caravelli, S.; Massimi, S.; Benedetti, M.G.; Di Caprio, F.; Mosca, S.; Zaffagnini, S. Current Concepts about Treatment Options of Plantar Fibromatosis: A Systematic Review of the Literature. Foot Ankle Surg. 2019, 25, 559–564. [Google Scholar] [CrossRef]
- Strzelczyk, A.; Vogt, H.; Hamer, H.M.; Krämer, G. Continuous Phenobarbital Treatment Leads to Recurrent Plantar Fibromatosis. Epilepsia 2008, 49, 1965–1968. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomac, A.; Ion, A.P.; Opriș, D.R.; Arbănași, E.M.; Ciucanu, C.C.; Bandici, B.C.; Coșarcă, C.M.; Covalcic, D.C.; Mureșan, A.V. Ledderhose’s Disease: An Up-to-Date Review of a Rare Non-Malignant Disorder. Clin. Pract. 2023, 13, 1182-1195. https://doi.org/10.3390/clinpract13050106
Tomac A, Ion AP, Opriș DR, Arbănași EM, Ciucanu CC, Bandici BC, Coșarcă CM, Covalcic DC, Mureșan AV. Ledderhose’s Disease: An Up-to-Date Review of a Rare Non-Malignant Disorder. Clinics and Practice. 2023; 13(5):1182-1195. https://doi.org/10.3390/clinpract13050106
Chicago/Turabian StyleTomac, Alexandru, Alexandru Petru Ion, Diana Roxana Opriș, Eliza Mihaela Arbănași, Claudiu Constantin Ciucanu, Bogdan Corneliu Bandici, Cătălin Mircea Coșarcă, Diana Carina Covalcic, and Adrian Vasile Mureșan. 2023. "Ledderhose’s Disease: An Up-to-Date Review of a Rare Non-Malignant Disorder" Clinics and Practice 13, no. 5: 1182-1195. https://doi.org/10.3390/clinpract13050106
APA StyleTomac, A., Ion, A. P., Opriș, D. R., Arbănași, E. M., Ciucanu, C. C., Bandici, B. C., Coșarcă, C. M., Covalcic, D. C., & Mureșan, A. V. (2023). Ledderhose’s Disease: An Up-to-Date Review of a Rare Non-Malignant Disorder. Clinics and Practice, 13(5), 1182-1195. https://doi.org/10.3390/clinpract13050106