
The Efficacy, the Treatment Response and the Aquaretic Effects of a Three-Year Tolvaptan Regimen in Polycystic Kidney Disease Patients



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Clinical and Laboratory Assessment
2.3. Statistical Analysis
3. Results
3.1. The Tolvaptan Effectiveness on Kidney Volume, Renal Function and Renal Prognosis
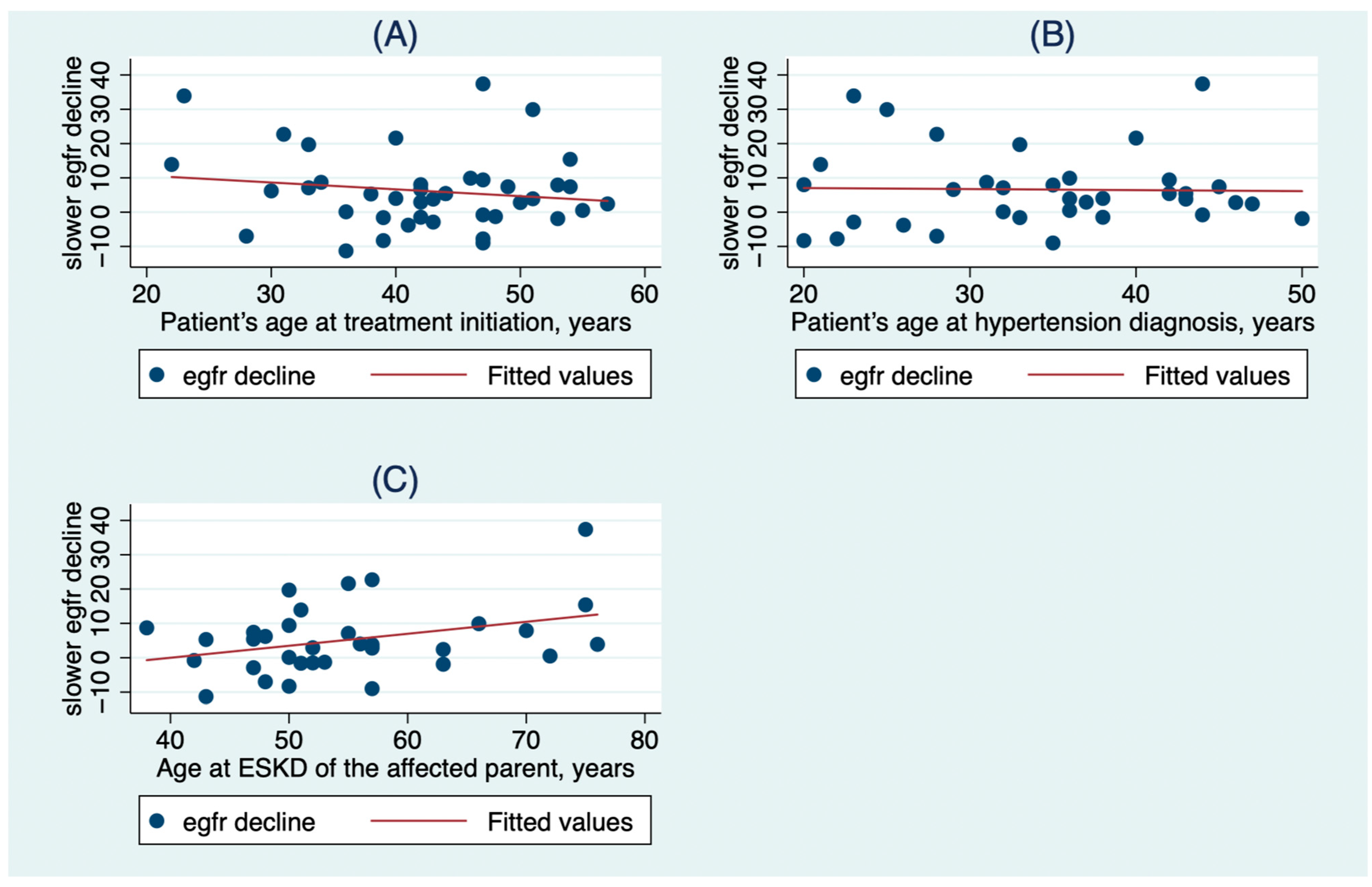
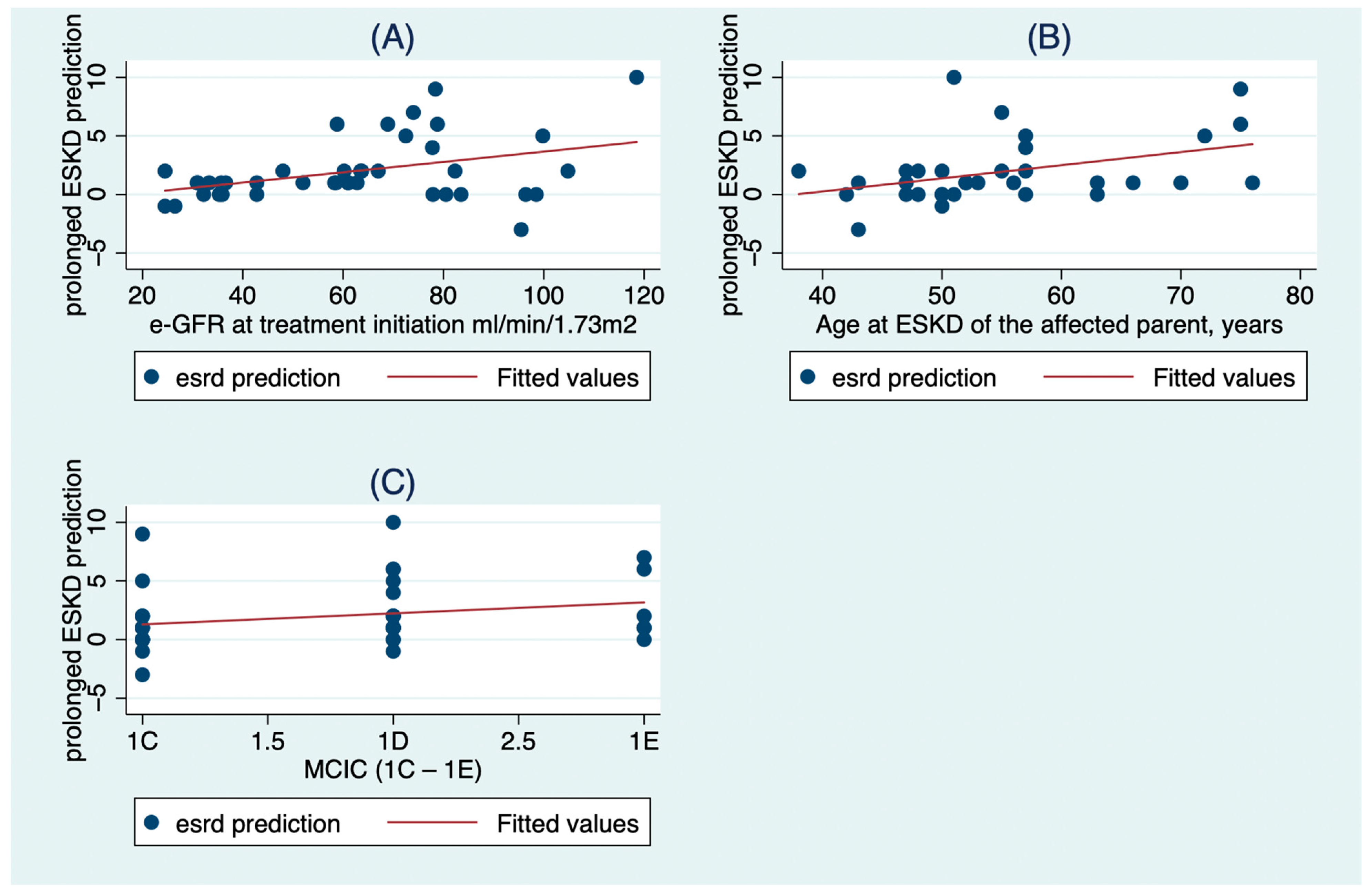
3.2. The Factors That Influenced the Response to Treatment
3.3. The Aquaretic Adverse Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lanktree, M.B.; Haghighi, A.; Guiard, E.; Iliuta, I.; Song, X.; Harris, P.C.; Patterson, D.; Pei, Y. Prevalence Estimates of Polycyxtic Kidney and Liver Disease by Population Sequencing. J. Am. Soc. Nephrol. 2018, 29, 2593–2600. [Google Scholar] [CrossRef] [PubMed]
- Torres, V.E.; Chapman, A.B.; Devuyst, O.; Gansevoort, R.T.; Grantham, J.J.; Higashihara, E.; Perrone, R.D.; Krasa, H.B.; Ouyang, J.; Czerwiec, F.S. Tolvaptan in patients with autosomal dominant polycystic kidney disease. New Engl. J. Med. 2012, 367, 2407–2418. [Google Scholar] [CrossRef] [PubMed]
- Torres, V.E.; Chapman, A.B.; Devuyst, O.; Gansevoort, R.T.; Perrone, R.D.; Koch, G.; Ouyang, J.; McQuade, R.D.; Blais, J.D.; Czerwiec, F.S.; et al. Tolvaptan in Later-Stage Autosomal Dominant Polycystic Kidney Disease. N. Engl. J. Med. 2017, 377, 1930–1942. [Google Scholar] [CrossRef] [PubMed]
- Chebib, F.T.; Perrone, R.D.; Chapman, A.B.; Dahl, N.K.; Harris, P.C.; Mrug, M.; Mustafa, R.A.; Rastogi, A.; Watnick, T.; Yu, A.S.L.; et al. A Practical Guide for Treatment of Rapidly Progressive ADPKD with Tolvaptan. J. Am. Soc. Nephrol. JASN. 2018, 29, 2458–2470. [Google Scholar] [CrossRef] [PubMed]
- Irazabal, M.V.; Rangel, L.J.; Bergstralh, E.J.; Osborn, S.L.; Harmon, A.J.; Sundsbak, J.L.; Bae, K.T.; Chapman, A.B.; Grantham, J.J.; Mrug, M.; et al. Imaging classification of autosomal dominant polycystic kidney disease: A simple model for selecting patients for clinical trials. J. Am. Soc. Nephrol. JASN 2015, 26, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Torres, V.E.; Higashihara, E.; Devuyst, O.; Chapman, A.B.; Gansevoort, R.T.; Grantham, J.J.; Perrone, R.D.; Ouyang, J.; Blais, J.D.; Czerwiec, F.S. Effect of Tolvaptan in Autosomal Dominant Polycystic Kidney Disease by CKD Stage: Results from the TEMPO 3:4 Trial. Clin. J. Am. Soc. Nephrol. CJASN 2016, 11, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Grantham, J.J.; Torres, V.E.; Chapman, A.B.; Guay-Woodford, L.M.; Bae, K.T.; King, B.F.; Wetzel, L.H.; Baumgarten, D.A.; Kenney, P.J.; Harris, P.C.; et al. Volume Progression in Polycystic Kidney Disease. New Engl. J. Med. 2006, 354, 2122–2130. [Google Scholar] [CrossRef] [PubMed]
- Torres, V.E.; Chapman, A.B.; Devuyst, O.; Gansevoort, R.T.; Perrone, R.D.; Dandurand, A.; Ouyang, J.; Czerwiec, F.S.; Blais, J.D.; TEMPO 4:4 Trial Investigators. Multicenter, open-label, extension trial to evaluate the long-term efficacy and safety of early versus delayed treatment with tolvaptan in autosomal dominant polycystic kidney disease: The TEMPO 4:4 Trial. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Ren. Assoc. 2017, 32, 1262. [Google Scholar] [CrossRef] [PubMed]
- Gregory, A.V.; Chebib, F.T.; Poudyal, B.; Holmes, H.L.; Yu, A.S.L.; Landsittel, D.P.; Bae, K.T.; Chapman, A.B.; Frederic, R.O.; Mrug, M.; et al. Utility of new image-derived biomarkers for autosomal dominant polycystic kidney disease prognosis using automated instance cyst segmentation. Kidney Int. 2023, 104, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Schrier, R.W.; Abebe, K.Z.; Perrone, R.D.; Torres, V.E.; Braun, W.E.; Steinman, T.I.; Winklhofer, F.T.; Brosnahan, G.; Czarnecki, P.G.; Hogan, M.C.; et al. Blood pressure in early autosomal dominant polycystic kidney disease. New Engl. J. Med. 2014, 371, 2255–2266. [Google Scholar] [CrossRef] [PubMed]
- Torres, V.E.; Abebe, K.Z.; Chapman, A.B.; Schrier, R.W.; Braun, W.E.; Steinman, T.I.; Winklhofer, F.T.; Brosnahan, G.; Czarnecki, P.G.; Hogan, M.C.; et al. Angiotensin blockade in late autosomal dominant polycystic kidney disease. New Engl. J. Med. 2014, 371, 2267–2276. [Google Scholar] [CrossRef] [PubMed]
- Irazabal, M.V.; Abebe, K.Z.; Bae, K.T.; Perrone, R.D.; Chapman, A.B.; Schrier, R.W.; Yu, A.S.; Braun, W.E.; Steinman, T.I.; Harris, P.C.; et al. Prognostic enrichment design in clinical trials for autosomal dominant polycystic kidney disease: The HALT-PKD clinical trial. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Ren. Assoc. 2017, 32, 1857–1865. [Google Scholar] [CrossRef] [PubMed]
- Barua, M.; Cil, O.; Paterson, A.D.; Wang, K.; He, N.; Dicks, E.; Parfrey, P.; Pei, Y. Family history of renal disease severity predicts the mutated gene in ADPKD. J. Am. Soc. Nephrol. JASN 2009, 20, 1833–1838. [Google Scholar] [CrossRef] [PubMed]
- Baboolal, K.; Ravine, D.; Daniels, J.; Williams, N.; Holmans, P.; Coles, G.A.; Williams, J.D. Association of the angiotensin I converting enzyme gene deletion polymorphism with early onset of ESRF in PKD1 adult polycystic kidney disease. Kidney Int. 1997, 52, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Sussman, C.R.; Wang, X.; Chebib, F.T.; Torres, V.E. Modulation of polycystic kidney disease by G-protein coupled receptors and cyclic AMP signaling. Cell. Signal. 2020, 72, 109649. [Google Scholar] [CrossRef] [PubMed]
- Chebib, F.T.; Torres, V.E. Autosomal Dominant Polycystic Kidney Disease: Core Curriculum 2016. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2016, 67, 792–810. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.J.; Kwon, T.H. Molecular mechanisms regulating aquaporin-2 in kidney collecting duct. Am. J. Physiology. Ren. Physiol. 2016, 311, F1318–F1328. [Google Scholar] [CrossRef] [PubMed]
- Zittema, D.; Boertien, W.E.; van Beek, A.P.; Dullaart, R.P.; Franssen, C.F.; de Jong, P.E.; Meijer, E.; Gansevoort, R.T. Vasopressin, copeptin, and renal concentrating capacity in patients with autosomal dominant polycystic kidney disease without renal impairment. Clin. J. Am. Soc. Nephrol. CJASN 2012, 7, 906–913. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total | Male | Female | p-Value | |
|---|---|---|---|---|
| Patients, n (%) | 41 (100%) | 23 (56%) | 18 (44%) | |
| Age, years, mean (SD) | 42.5 (8.6) | 40.7 (8.6) | 44.7 (8.2) | 0.14 |
| Age at ADPKD diagnosis, years, mean (SD) | 24 (9.4) | 21.5 (8) | 27.7 (10.3) | 0.04 |
| Presence of HTN, n (%) | 39 (100%) | 21 (54%) | 18 (46%) | 0.2 |
| Age at HTN diagnosis, years, mean (SD) | 34 (8.5) | 31.5 (8) | 38 (8) | 0.02 |
| Age at ESKD of the affected parent, years, mean (SD) | 55 (20) | 54 (9) | 57 (11) | 0.4 |
| MCIC 1C, n (%) | 17 (41%) | 9 (39%) | 8 (44%) | 0.84 |
| MCIC 1D, n (%) | 18 (44%) | 11 (48%) | 7 (39%) | |
| MCIC 1E, n (%) | 6 (15%) | 3 (13%) | 3 (17%) | |
| CKD stage 1, n (%) | 6 (15%) | 5 (22%) | 1 (6%) | 0.47 |
| CKD stage 2, n (%) | 17 (42%) | 7 (30%) | 10 (55%) | |
| CKD stage 3a, n (%) | 5 (12%) | 3 (13%) | 2 (11%) | |
| CKD stage 3b, n (%) | 10 (24%) | 6 (26%) | 4 (22%) | |
| CKD stage 4, n (%) | 3 (7%) | 2 (9%) | 1 (6%) | |
| TKV (mL), median (IQR) | 1703 (1531) | 1933 (3370) | 1599 (1298) | 0.85 |
| e-GFR, mL/min/1.73 m2, mean (SD) | 61.8 (24.6) | 63.4 (28.4) | 59.9 (19.4) | 0.65 |
| ESKD prediction, years, mean (SD) | 13 (7) | 13.7 (8) | 12.3 (5.5) | 0.52 |
| Expected without Treatment at 3 Years | Measured After 3 Years of Tolvaptan Treatment | p-Value | |
|---|---|---|---|
| TKV (mL), median (IQR) Mean (SD) | 2180 (1091) 2717 (1839) | 2250 (1357) 2773 (2087) | 0.48 |
| e-GFR (mL/min/1.73 m2), mean (SD) | 51.1 (25.2)1 | 57.3 (30) | <0.001 |
| e-GFR (mL/min/1.73 m2), mean (SD) | 48.8 (27.4)2 | 57.3 (30) | <0.001 |
| ESKD prediction (years), mean (SD) | 10 (7) | 12 (8) | <0.001 |
| β-Coefficient | Std. Err. | p > |t| | [95% Conf. Interval] | |
|---|---|---|---|---|
| Patient’s age at treatment initiation, years | −0.9 | 0.29 | 0.006 | [−1.52, −0.29] |
| Patient’s age at hypertension diagnosis, years | 0.88 | 0.3 | 0.008 | [0.25, 1.52] |
| Age at ESKD of the affected parent, years | 0.57 | 0.2 | 0.008 | [0.16, 0.98] |
| β-Coefficient | Std. Err. | p > |t| | [95% Conf. Interval] | |
|---|---|---|---|---|
| e-GFR at treatment initiation mL/min/1.73 m2 | 0.06 | 0.017 | 0.001 | [0.03, 0.1] |
| Age at ESKD of the affected parent, years | 0.13 | 0.05 | 0.013 | [0.03, 0.23] |
| MCIC (1C—1E) | 1.93 | 0.7 | 0.013 | [0.46, 3.39] |
| Prior to Tolvaptan Initiation | During Tolvaptan Treatment (18 Consecutive Measurements) | |
|---|---|---|
| 24 h urine volume, mL, mean (SD) | 3167 (1217) | 5403 (1900) |
| Urine osmolality, mOsm/kg, mean (SD) | 354 (200) | 198 (91) |
| β-Coefficient | Std. Error | p > |z| | [95% Conf. Interval] | |
|---|---|---|---|---|
| e-GFR, mL/min/1.73 m2–Urine volume (mL) | 0.00002 | 0.0002 | 0.9 | [−0.0004, 0.0004] |
| serum sodium, mEq/L–Urine volume (mL) | 0.0001 | 0.0001 | 0.15 | [−0.00003, 0.0003] |
| serum potassium, mEq/L–Urine volume (mL) | 0.0001 | 0.0001 | 0.4 | [−0.0002, 0.0004] |
| serum calcium, mg/dL–Urine volume (mL) | −6.89 × 10–6 | 0.00002 | 0.65 | [−0.00004, 0.00002] |
| serum phosphorus, mg/dL–Urine volume (mL) | 0.00002 | 0.00002 | 0.4 | [−0.00003, 0.0001] |
| serum uric acid, mg/dL–Urine volume (mL) | 0.00006 | 0.00004 | 0.16 | [−0.000022, 0.0001] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gkika, V.; Louka, M.; Tsagkatakis, M.; Tsirpanlis, G. The Efficacy, the Treatment Response and the Aquaretic Effects of a Three-Year Tolvaptan Regimen in Polycystic Kidney Disease Patients. Clin. Pract. 2023, 13, 1035-1042. https://doi.org/10.3390/clinpract13050092
Gkika V, Louka M, Tsagkatakis M, Tsirpanlis G. The Efficacy, the Treatment Response and the Aquaretic Effects of a Three-Year Tolvaptan Regimen in Polycystic Kidney Disease Patients. Clinics and Practice. 2023; 13(5):1035-1042. https://doi.org/10.3390/clinpract13050092
Chicago/Turabian StyleGkika, Vasiliki, Michaela Louka, Mihail Tsagkatakis, and George Tsirpanlis. 2023. "The Efficacy, the Treatment Response and the Aquaretic Effects of a Three-Year Tolvaptan Regimen in Polycystic Kidney Disease Patients" Clinics and Practice 13, no. 5: 1035-1042. https://doi.org/10.3390/clinpract13050092
APA StyleGkika, V., Louka, M., Tsagkatakis, M., & Tsirpanlis, G. (2023). The Efficacy, the Treatment Response and the Aquaretic Effects of a Three-Year Tolvaptan Regimen in Polycystic Kidney Disease Patients. Clinics and Practice, 13(5), 1035-1042. https://doi.org/10.3390/clinpract13050092