
Pleural Fluid-to-Blood BNP Ratio May Contribute to Prognosis in Malignant Pleural Mesothelioma

 , ,
, ,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
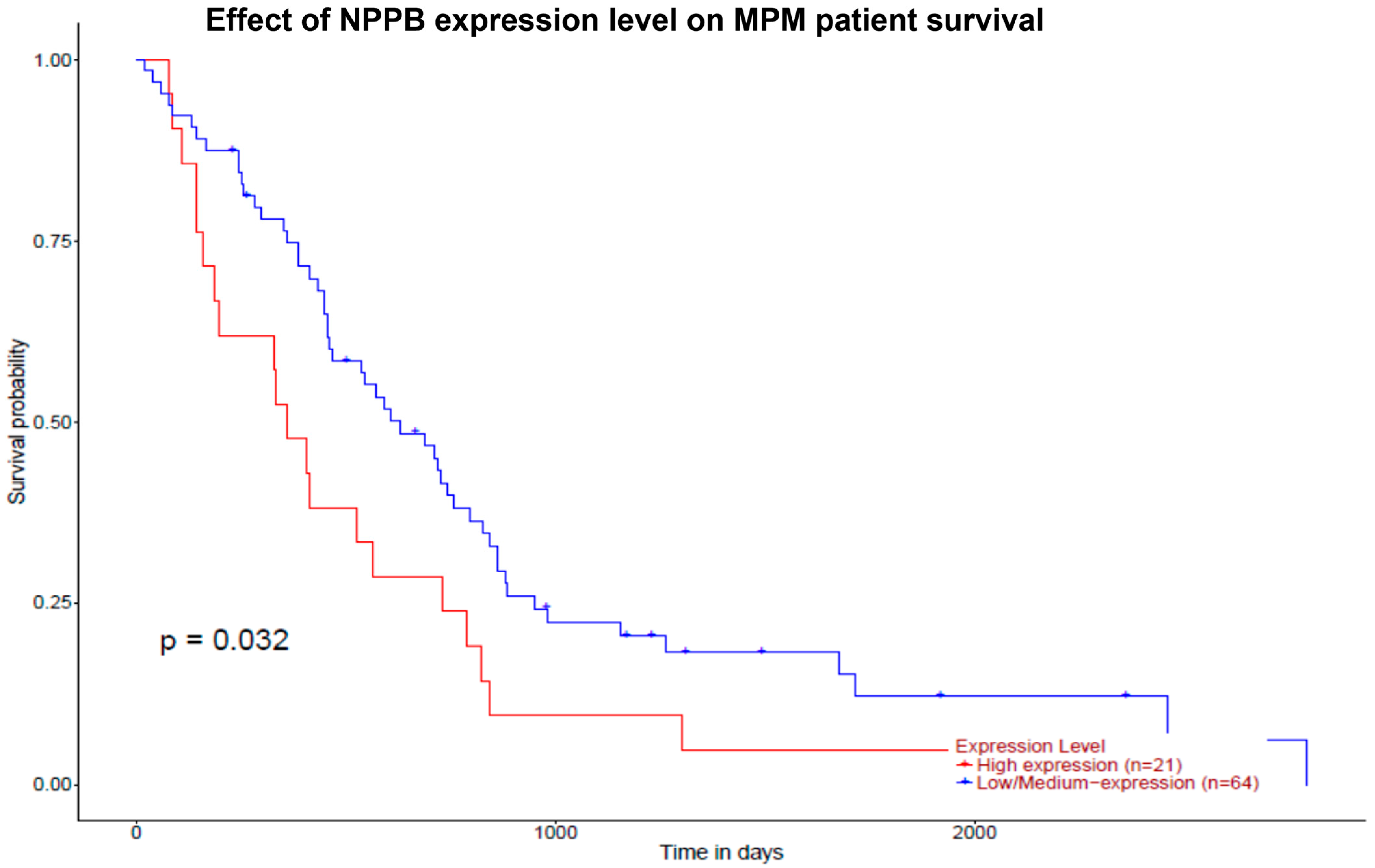
2.1. Evaluation of Prognostic Significance of NPPB Gene Expression in MPM
2.2. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zakynthinos, E.; Kiropoulos, T.; Gourgoulianis, K.; Filippatos, G. Diagnostic and prognostic impact of brain natriuretic peptide in cardiac and noncardiac diseases. Heart Lung J. Crit. Care 2008, 37, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Porcel, J.M.; Martínez-Alonso, M.; Cao, G.; Bielsa, S.; Sopena, A.; Esquerda, A. Biomarkers of heart failure in pleural fluid. Chest 2009, 136, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Papanikolaou, J.; Makris, D.; Mpaka, M.; Palli, E.; Zygoulis, P.; Zakynthinos, E. New insights into the mechanisms involved in B-type natriuretic peptide elevation and its prognostic value in septic patients. Crit. Care 2014, 18, R94. [Google Scholar] [CrossRef] [PubMed]
- Robier, C.; Neubauer, M.; Binter, G.; Raggam, R.B. Extensive elevation of BNP but not NT-ProBNP in a patient with advanced urothelial carcinoma in absence of cardiac failure and volume overload. Clin. Chem. Lab. Med. 2014, 52, e99–e101. [Google Scholar] [CrossRef] [PubMed]
- Burjonroppa, S.C.; Tong, A.T.; Xiao, L.C.; Johnson, M.M.; Yusuf, S.W.; Lenihan, D.J. Cancer patients with markedly elevated B-type natriuretic peptide may not have volume overload. Am. J. Clin. Oncol. 2007, 30, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Andreu, A.; Guglin, M. Exaggerated NT-proBNP production in patients with hematologic malignancies: A case series. Congest. Heart Fail. 2012, 18, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Lafaras, C.; Mandala, E.; Saratzis, A.; Platogiannis, D.; Barbetakis, N.; Papoti, S.; Christopoulou, M.; Ilonidis, G.; Bischiniotis, T. Pro-brain natriuretic peptide is a sensitive marker for detecting cardiac metastases in patients with non-small cell lung cancer. Onkologie 2009, 32, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Tsolaki, V.; Zarogiannis, S.; Zygoulis, P.; Kalomenidis, I.; Jagirdar, R.; Makris, D.; Daniil, Z.; Magkouta, S.; Triantafyllou, I.; Papanikolaou, J.; et al. Malignant mesothelioma cells secrete natriuretic peptides: Data and diagnostic clinical implications. Respirology 2020, 25, 1060–1065. [Google Scholar] [CrossRef]
- Porcel, J.M. Natriuretic peptides in pleural effusions: Beyond a diagnosis of heart failure. Respirology 2020, 25, 1021–1022. [Google Scholar] [CrossRef]
- Røe, O.D.; Stella, G.M. Malignant pleural mesothelioma: History, controversy and future of a manmade epidemic. Eur. Respir. Rev. 2015, 24, 115–131. [Google Scholar] [CrossRef]
- Ringgaard Petersen, T.; Panou, V.; Meristoudis, C.; Weinreich, U.M.; Røe, O.D. Clinical prognostic factors in pleural mesothelioma: Best supportive care and anti-tumor treatments in a real-life setting. Acta Oncol. 2021, 60, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Gogou, E.; Kerenidi, T.; Chamos, V.; Zintzaras, E.; Gourgoulianis, K.I. Mesothelioma mortality in Greece from 1983 to 2003. Int. J. Clin. Pract. 2009, 63, 944–948. [Google Scholar] [CrossRef]
- Krug, L.M.; Pass, H.I.; Rusch, V.W.; Kindler, H.L.; Sugarbaker, D.J.; Rosenzweig, K.E.; Flores, R.; Friedberg, J.S.; Pisters, K.; Monberg, M.; et al. Multicenter phase II trial of neoadjuvant pemetrexed plus cisplatin followed by extrapleural pneumonectomy and radiation for malignant pleural mesothelioma. J. Clin. Oncol. 2009, 27, 3007–3013. [Google Scholar] [CrossRef] [PubMed]
- Fennell, D.A.; Parmar, A.; Shamash, J.; Evans, M.T.; Sheaff, M.T.; Sylvester, R.; Dhaliwal, K.; Gower, N.; Steele, J.; Rudd, R. Statistical validation of the EORTC prognostic model for malignant pleural mesothelioma based on three consecutive phase II trials. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 184–189. [Google Scholar] [CrossRef]
- Ghanim, B.; Hoda, M.A.; Winter, M.P.; Klikovits, T.; Alimohammadi, A.; Hegedus, B.; Dome, B.; Grusch, M.; Arns, M.; Schenk, P.; et al. Pretreatment serum C-reactive protein levels predict benefit from multimodality treatment including radical surgery in malignant pleural mesothelioma: A retrospective multicenter analysis. Ann. Surg. 2012, 256, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, M.; Takeuchi, J.; Takuwa, T.; Kuroda, A.; Nakamura, A.; Nakamichi, T.; Matsumoto, S.; Kondo, N.; Nakano, T.; Morimoto, T.; et al. Pleural thickness after neoadjuvant chemotherapy is a prognostic factor in malignant pleural mesothelioma. J. Thorac. Cardiovasc. Surg. 2019, 157, 404–413. [Google Scholar] [CrossRef] [PubMed]
- de Perrot, M.; Dong, Z.; Bradbury, P.; Patsios, D.; Keshavjee, S.; Leighl, N.B.; Hope, A.; Feld, R.; Cho, J. Impact of tumour thickness on survival after radical radiation and surgery in malignant pleural mesothelioma. Eur. Respir. J. 2017, 49, 1601428. [Google Scholar] [CrossRef] [PubMed]
- Nowak, A.K.; Chansky, K.; Rice, D.C.; Pass, H.I.; Kindler, H.L.; Shemanski, L.; Billé, A.; Rintoul, R.C.; Batirel, H.F.; Thomas, C.F.; et al. The IASLC Mesothelioma Staging Project: Proposals for Revisions of the T Descriptors in the Forthcoming Eighth Edition of the TNM Classification for Pleural Mesothelioma. J. Thorac. Oncol. 2016, 11, 2089–2099. [Google Scholar] [CrossRef]
- Nakamura, S.; Ito, T.; Chen-Yoshikawa, T.F. ASO Author Reflections: Pleural Thickness in Patients with Malignant Pleural Mesothelioma. Ann. Surg. Oncol. 2023, 30, 1584–1585. [Google Scholar] [CrossRef]
- Steele, J.P.; Klabatsa, A.; Fennell, D.A.; Palläska, A.; Sheaff, M.T.; Evans, M.T.; Shamash, J.; Rudd, R.M. Prognostic factors in mesothelioma. Lung Cancer 2005, 49 (Suppl. S1), S49–S52. [Google Scholar] [CrossRef]
- Guzmán-Casta, J.; Carrasco-CaraChards, S.; Guzmán-Huesca, J.; Sánchez-Ríos, C.P.; Riera-Sala, R.; Martínez-Herrera, J.F.; Peña-Mirabal, E.S.; Bonilla-Molina, D.; Alatorre-Alexander, J.A.; Martínez-Barrera, L.M.; et al. Prognostic factors for progression-free and overall survival in malignant pleural mesothelioma. Thorac. Cancer 2021, 12, 1014–1022. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Appleton, C.P.; Gillebert, T.C.; Marino, P.N.; Oh, J.K.; Smiseth, O.A.; Waggoner, A.D.; Flachskampf, F.A.; Pellikka, P.A.; Evangelista, A. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J. Am. Soc. Echocardiogr. 2009, 22, 107–133. [Google Scholar] [CrossRef] [PubMed]
- ECOG ACRIN Cancer Research Group. ECOG Performance Status; ECOG ACRIN Cancer Research Group: Boston, MA, USA, 2017. [Google Scholar]
- Dick, I.M.; Lee, Y.C.G.; Cheah, H.M.; Miranda, A.; Robinson, B.W.S.; Creaney, J. Profile of soluble factors in pleural effusions predict prognosis in mesothelioma. Cancer Biomark. 2022, 33, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Goswami, C.P.; Nakshatri, H. PROGgeneV2: Enhancements on the existing database. BMC Cancer 2014, 14, 970. [Google Scholar] [CrossRef] [PubMed]
- Marinho, F.C.; Vargas, F.S.; Fabri, J., Jr.; Acencio, M.M.; Genofre, E.H.; Antonangelo, L.; Sales, R.K.; Teixeira, L.R. Clinical usefulness of B-type natriuretic peptide in the diagnosis of pleural effusions due to heart failure. Respirology 2011, 16, 495–499. [Google Scholar] [CrossRef] [PubMed]
- Man, J.; Barnett, P.; Christoffels, V.M. Structure and function of the Nppa-Nppb cluster locus during heart development and disease. Cell Mol. Life Sci. 2018, 75, 1435–1444. [Google Scholar] [CrossRef] [PubMed]
- Taioli, E.; Wolf, A.S.; Camacho-Rivera, M.; Flores, R.M. Women with malignant pleural mesothelioma have a threefold better survival rate than men. Ann. Thorac. Surg. 2014, 98, 1020–1024. [Google Scholar] [CrossRef]
- Wang, T.J.; Larson, M.G.; Levy, D.; Benjamin, E.J.; Leip, E.P.; Omland, T.; Wolf, P.A.; Vasan, R.S. Plasma natriuretic peptide levels and the risk of cardiovascular events and death. N. Engl. J. Med. 2004, 350, 655–663. [Google Scholar] [CrossRef]
- Januzzi, J.L.; Morss, A.; Tung, R.; Pino, R.; Fifer, M.A.; Thompson, B.T.; Lee-Lewandrowski, E. Natriuretic peptide testing for the evaluation of critically ill patients with shock in the intensive care unit: A prospective cohort study. Crit. Care 2006, 10, R37. [Google Scholar] [CrossRef]
- Calderone, A.; Bel-Hadj, S.; Drapeau, J.; El-Helou, V.; Gosselin, H.; Clement, R.; Villeneuve, L. Scar myofibroblasts of the infarcted rat heart express natriuretic peptides. J. Cell. Physiol. 2006, 207, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Tamura, N.; Chusho, H.; Nakao, K. Brain natriuretic peptide appears to act locally as an antifibrotic factor in the heart. Can. J. Physiol. Pharmacol. 2001, 79, 723–729. [Google Scholar] [CrossRef]
- Mezzasoma, L.; Antognelli, C.; Talesa, V.N. A Novel Role for Brain Natriuretic Peptide: Inhibition of IL-1β Secretion via Downregulation of NF-kB/Erk 1/2 and NALP3/ASC/Caspase-1 Activation in Human THP-1 Monocyte. Mediat. Inflamm. 2017, 2017, 5858315. [Google Scholar] [CrossRef] [PubMed]
- Ohsaki, Y.; Gross, A.J.; Le, P.T.; Oie, H.; Johnson, B.E. Human small cell lung cancer cells produce brain natriuretic peptide. Oncology 1999, 56, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Shojaee, S.; Singh, I.; Solsky, I.; Nana-Sinkam, P. Malignant Pleural Effusion at Presentation in Patients with Small-Cell Lung Cancer. Respiration 2019, 98, 198–202. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, S.P.; Davis, M.; Baxter, G.F. Autocrine and paracrine actions of natriuretic peptides in the heart. Pharmacol. Ther. 2004, 101, 113–129. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Chápuli, R.; Pérez-Pomares, J.M.; Macías, D.; García-Garrido, L.; Carmona, R.; González, M. Differentiation of hemangioblasts from embryonic mesothelial cells? A model on the origin of the vertebrate cardiovascular system. Differ. Res. Biol. Divers. 1999, 64, 133–141. [Google Scholar] [CrossRef]
- Batra, H.; Antony, V.B. Pleural mesothelial cells in pleural and lung diseases. J. Thorac. Dis. 2015, 7, 964–980. [Google Scholar] [CrossRef]
- Leeflang, M.M.; Moons, K.G.; Reitsma, J.B.; Zwinderman, A.H. Bias in sensitivity and specificity caused by data-driven selection of optimal cutoff values: Mechanisms, magnitude, and solutions. Clin. Chem. 2008, 54, 729–737. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Malignant Mesothelioma Effusions (MME) (n = 19) | |
|---|---|
| Age | 67 (61, 80) |
| Sex (male) | 15 (78.9%) |
| Smoking habits/current smokers | 17 (89.5%)/16/17 (94%) |
| Smoking habits (pys) | 45 (0, 100) |
| BMI (kg/m2) | 25.5 (22.4, 34) |
| Arterial hypertension | 8 (42%) |
| Diabetes mellitus | 4 (21%) |
| Asbestos exposure | |
| Definite/confirmed | 10 (52.6%) |
| Possible | 5 (26.3%) |
| Unknown | 4 (21%) |
| TNM | 3 (3, 4) |
| Pleural thickness (max) (cm) | 3 (1.2, 4.5) |
| Performance status | 2 (1, 3) |
| White blood cells (blood) (/μL) | 8900 (5600, 12,900) |
| CRP (mg/dL) | 3.2 (1.2, 4.3) |
| Albumin (serum) (mg/dL) | 3.8 (3.2, 4.3) |
| Serum creatinine (mg/dL) | 1.19 (1.04, 1.4) |
| White blood cells (pleural fluid) (/μL) | 2890 (100, 13,000) |
| Lymphocytes | 70% (56, 80%) |
| Neutrophils | 5% (0, 24%) |
| Mesothelial cells | 20% (10, 35%) |
| Pleural fluid BNP (pg/mL) | 457 (5, 5000) |
| Whole blood BNP (pg/mL) | 73 (8, 268) |
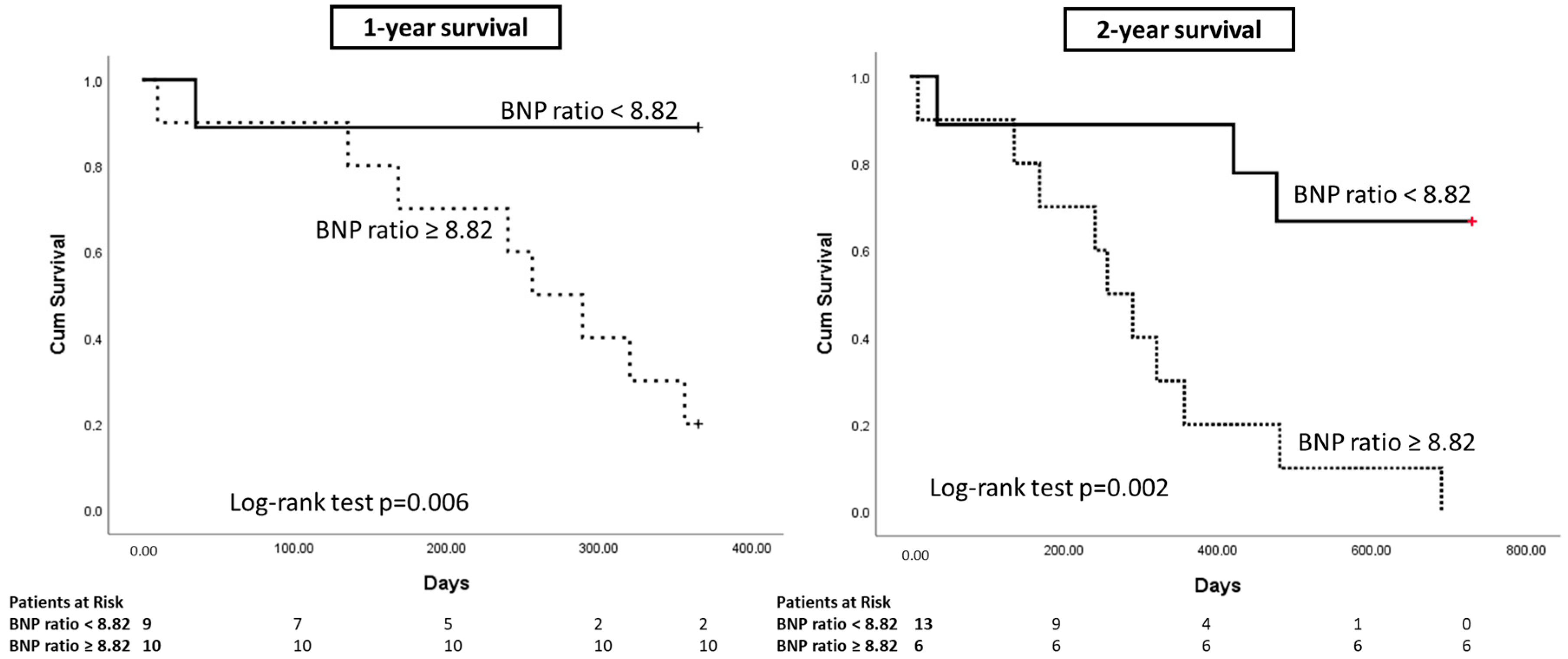
| BNP ratio | 8.82 (0.3, 150.24) |
| Pleural fluid LDH (IU/mL) | 429 (100, 1150) |
| Serum LDH (IU/mL) | 231 (127, 2245) |
| LDH ratio | 1.7 (0.2, 4.7) |
| Pleural fluid protein (mg/dL) | 4.3 (2.9, 5.2) |
| Blood protein (mg/dL) | 6.9 (6.1, 7.8) |
| Protein ratio | 0.63 (0.48, 0.79) |
| 1-Year Survival | 2-Year Survival | |||
|---|---|---|---|---|
| Survivors (n = 10) | Non-Survivors (n = 9) | Survivors (n = 6) | Non-Survivors (n = 13) | |
| Age | 66.5 (61, 78) | 68 (62, 80) | 65.5 (61, 70) | 68 (62, 80) |
| Sex (male) | 7 (70%) | 8 (88.9%) | 5 (83.3%) | 10 (76.9%) |
| Smoking habits/current smokers | 9/10 (90%) 9/9 (100%) | 8/9 (88.9%) 7/8 (87.5%) | 5/6 (83.3%) 5/5 (100%) | 12/13 (92.3%) 12/12 (100%) |
| Smoking habits (pys) | 45 (0, 50) | 30 (0, 100) | 46.5 (0, 50) | 40 (0, 100) |
| BMI (k/m2) | 25.9 (22.4, 34) | 25.3 (23, 27.4) | 25.6 (22.4, 34) | 25.5 (23, 32) |
| Arterial hypertension | 5 (50%) | 3 (33.33%) | 2 (33.4%) | 6 (46.2%) |
| Diabetes mellitus | 3 (30%) | 1 (11%) | 2 (33.4%) | 2 (15.4%) |
| Asbestos exposure | ||||
| Definite/confirmed | 4 (40%) | 6 (66.67%) | 3 (50%) | 7 (53.8%) |
| Possible | 3 (30%) | 2 (22.2%) | 1 (16.7%) | 4 (30.8%) |
| Unknown | 3 (30%) | 1 (11.1%) | 2 (33.3%) | 2 (15.4%) |
| TNM | 3 (3, 4) | 3 (3, 3) | 3 (3, 4) | 3 (3, 4) |
| Pleural thickness (max) (cm) | 2.8 (1.5, 4.3) | 3.4 (1.2, 4.5) | 3.1 (1.8, 4.3) | 3 (1.2, 4.5) |
| Performance status | 1 (1, 2) | 2 (1, 3) | 1 (1, 2) | 2 (1, 3) |
| White blood cells (blood) (/μL) | 8680 (5600, 10,200) | 9870 (6700, 12,900) | 7339.5 (5600, 95,670) * | 9379 (6700, 12,900) |
| CRP (mg/dL) | 3.2 (1.2, 4.3) | 3.3 (2.8, 3.8) | 2.6 (1.2, 4) | 3.4 (2.8, 4.3) |
| Albumin (serum) (mg/dL) | 3.7 (3.2, 4.3) | 3.8 (2.8, 3.8) | 3.8 (3.2, 4.3) | 3.7 (3.4, 4.2) |
| White blood cells (pleural fluid) (/μL) | 2329 (100, 9400) | 2980 (800, 13,000) | 2329 (100, 9400) | 2980 (200, 13,000) |
| Lymphocytes | 78% (60, 80%) * | 65% (56, 72%) | 70% (60, 80%) | 70% (56, 80%) |
| Neutrophils | 7.5% (2, 24%) | 5% (0, 10%) | 15% (4, 24%) * | 4% (0, 10%) |
| Mesothelial cells | 16.5% (10, 20%) # | 30% (20, 35%) | 15% (15, 20%) * | 28% (10, 35%) |
| Pleural fluid BNP (pg/mL) | 413 (5, 5000) | 1016 (210, 5000) | 379.5 (5, 567) * | 699 (210, 5000) |
| Serum BNP (pg/mL) | 108.5 (16, 203) | 26.5 (8, 268) | 86 (16, 110) | 58 (8, 268) |
| BNP ratio | 3.49 (0.3, 26) * | 28.75 (4.05, 150.24) | 3.49 (0.3, 7.76) * | 22.8 (2.42, 150.24) |
| Pleural fluid LDH (IU/mL) | 404 (100, 1134) | 459 (182, 1150) | 418 (100, 489) | 445 (114, 1150) |
| Serum LDH (IU/mL) | 219 (127, 2245) | 245 (151, 380) | 173 (155, 207) | 245 (127, 2245) |
| LDH ratio | 1.6 (0.2, 3.9) | 1.87 (0.8, 4.7) | 2.4 (0.5, 3.2) | 1.35 (0.2, 4.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsolaki, V.; Zakynthinos, G.E.; Zarogiannis, S.; Zygoulis, P.; Kalomenidis, I.; Jagirdar, R.; Triantafyllou, I.; Gourgoulianis, K.I.; Makris, D.; Zakynthinos, E. Pleural Fluid-to-Blood BNP Ratio May Contribute to Prognosis in Malignant Pleural Mesothelioma. Clin. Pract. 2023, 13, 1111-1122. https://doi.org/10.3390/clinpract13050099
Tsolaki V, Zakynthinos GE, Zarogiannis S, Zygoulis P, Kalomenidis I, Jagirdar R, Triantafyllou I, Gourgoulianis KI, Makris D, Zakynthinos E. Pleural Fluid-to-Blood BNP Ratio May Contribute to Prognosis in Malignant Pleural Mesothelioma. Clinics and Practice. 2023; 13(5):1111-1122. https://doi.org/10.3390/clinpract13050099
Chicago/Turabian StyleTsolaki, Vasiliki, George E. Zakynthinos, Sotirios Zarogiannis, Paris Zygoulis, Ioannis Kalomenidis, Rajesh Jagirdar, Ioannis Triantafyllou, Konstantinos I. Gourgoulianis, Demosthenes Makris, and Epaminondas Zakynthinos. 2023. "Pleural Fluid-to-Blood BNP Ratio May Contribute to Prognosis in Malignant Pleural Mesothelioma" Clinics and Practice 13, no. 5: 1111-1122. https://doi.org/10.3390/clinpract13050099
APA StyleTsolaki, V., Zakynthinos, G. E., Zarogiannis, S., Zygoulis, P., Kalomenidis, I., Jagirdar, R., Triantafyllou, I., Gourgoulianis, K. I., Makris, D., & Zakynthinos, E. (2023). Pleural Fluid-to-Blood BNP Ratio May Contribute to Prognosis in Malignant Pleural Mesothelioma. Clinics and Practice, 13(5), 1111-1122. https://doi.org/10.3390/clinpract13050099