
Blockchain Technology and Artificial Intelligence Based Decentralized Access Control Model to Enable Secure Interoperability for Healthcare

 , , , ,
, , , ,  ,
,  and
and
Abstract
:1. Introduction
Motivation, Objective, and Contributions
- Various issues in the healthcare industry are explored and the benefits of integrating blockchain technology in the healthcare industry are discussed.
- A blockchain-supported, decentralized access control solution is proposed and implemented. Moreover, it can be tailored for implementation on other blockchain frameworks.
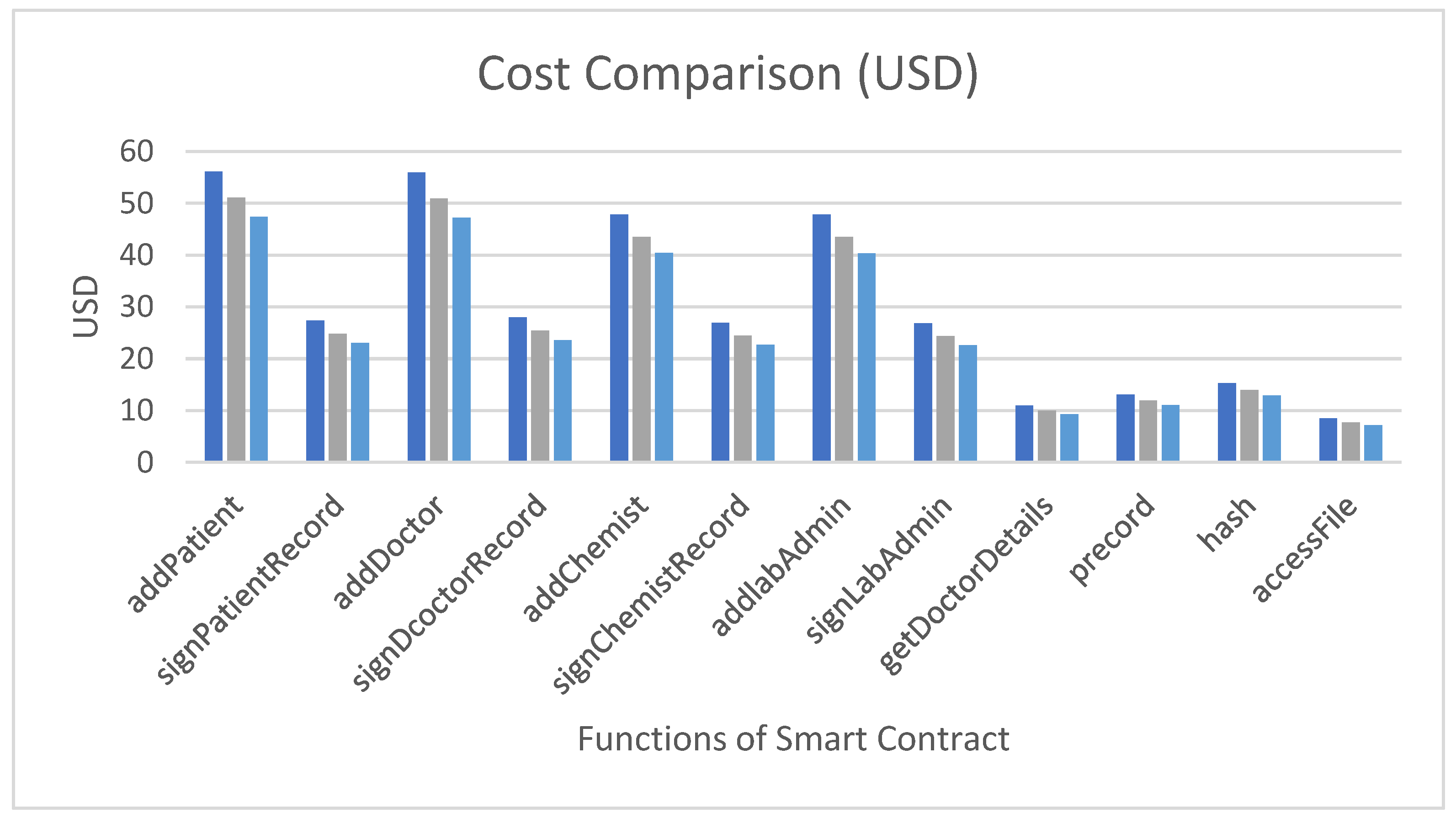
- The execution costs of various functions of smart contracts with slow, standard, and fast executions are compared.
- The proof-of-authority consensus procedure is employed in the proposed paradigm. A few selected nodes will function as validators that will have the authority to validate the transactions. Because only preselected validator nodes will validate the transaction, the time necessary to create a block is predictable and smaller than the time required to generate a block using the proof-of-work process.
2. Literature Study
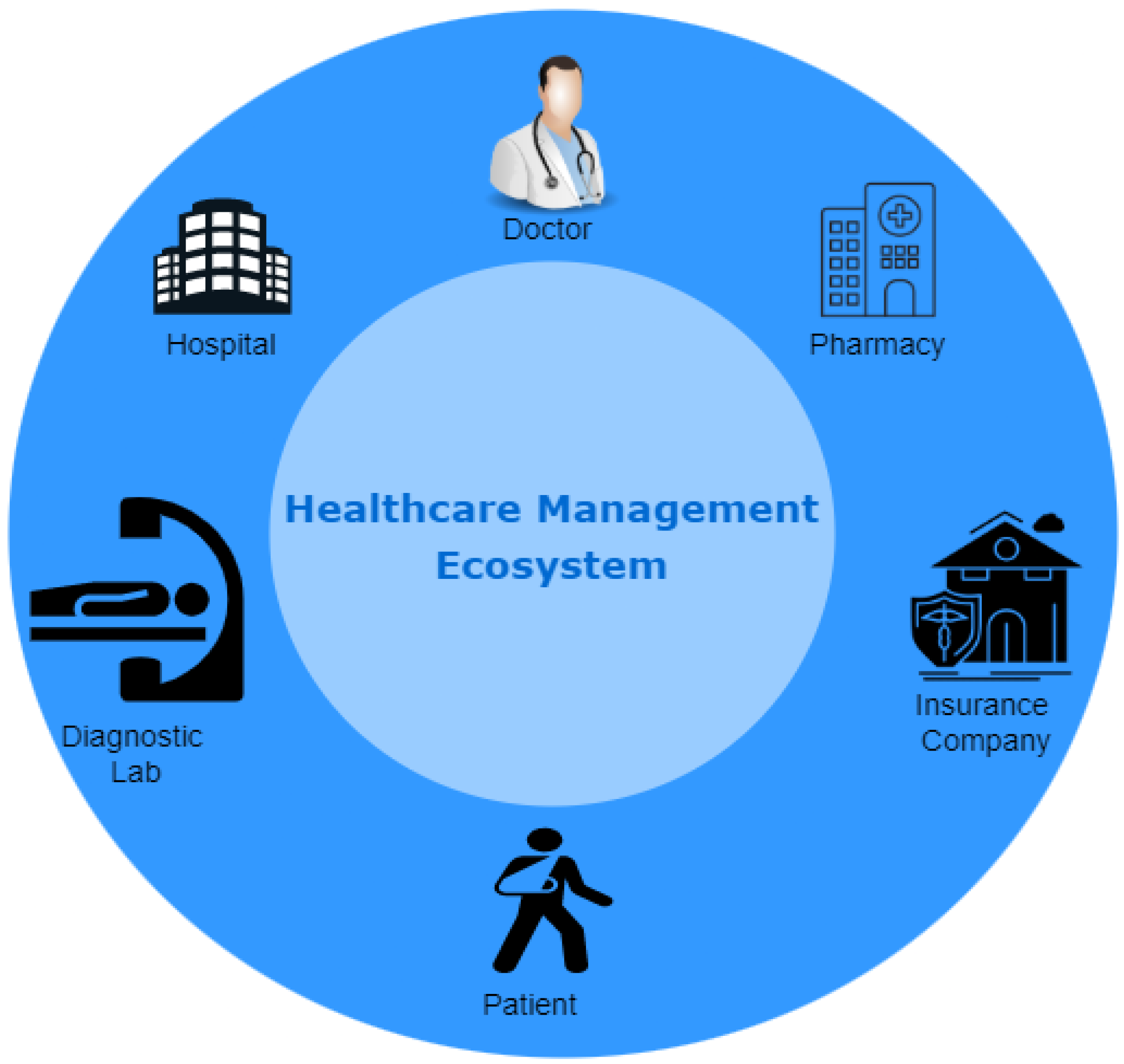
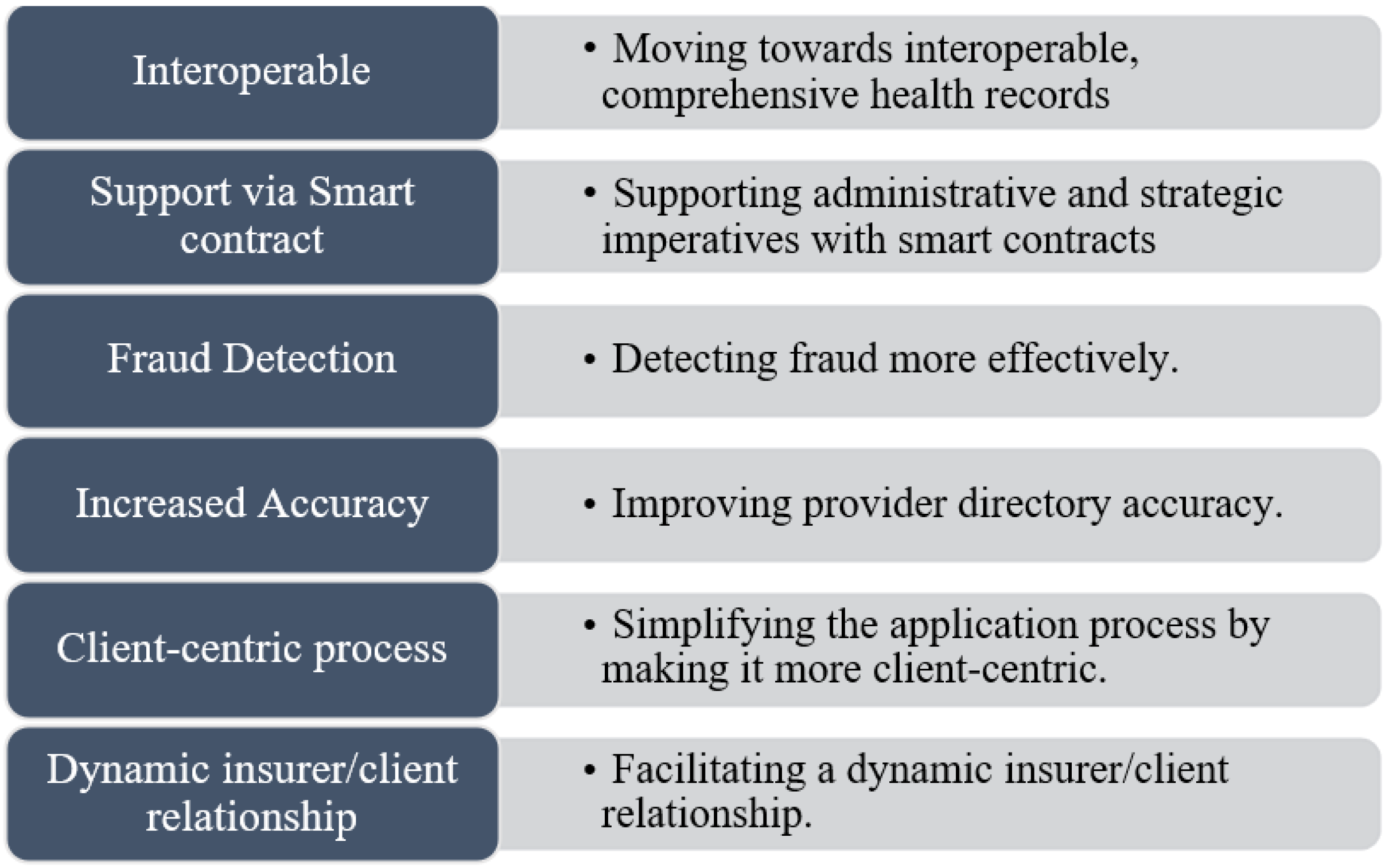
3. Benefits of Employing Blockchain Technology for Healthcare
- Towards complete and interoperable health records
- 2.
- Smart contracts for better coordination
- 3.
- More successfully detecting fraud
- 4.
- Improving the correctness of the provider directory
- 5.
- More client-centric to simplify it
- 6.
- Assisting in the development of a dynamic insurer–client relationship
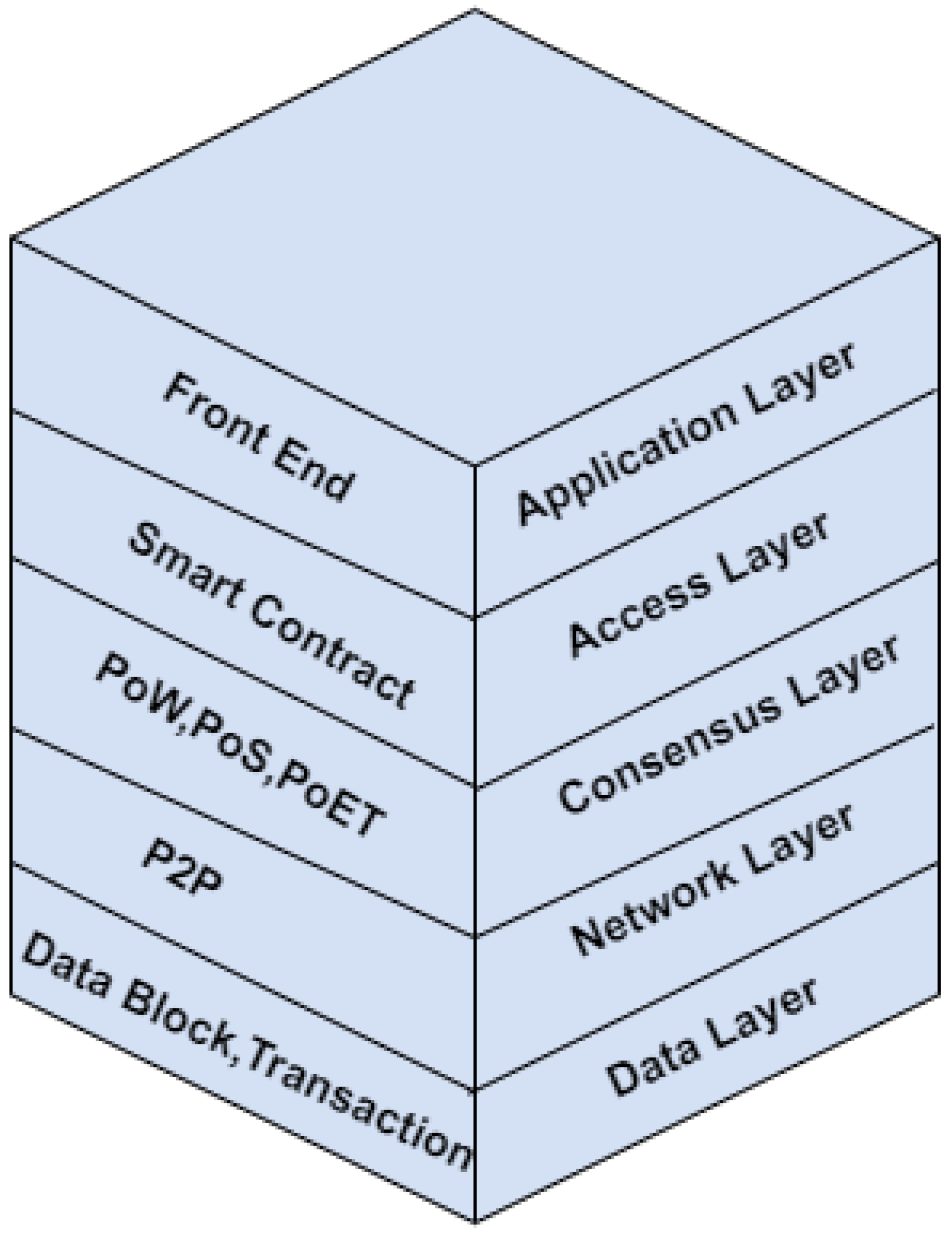
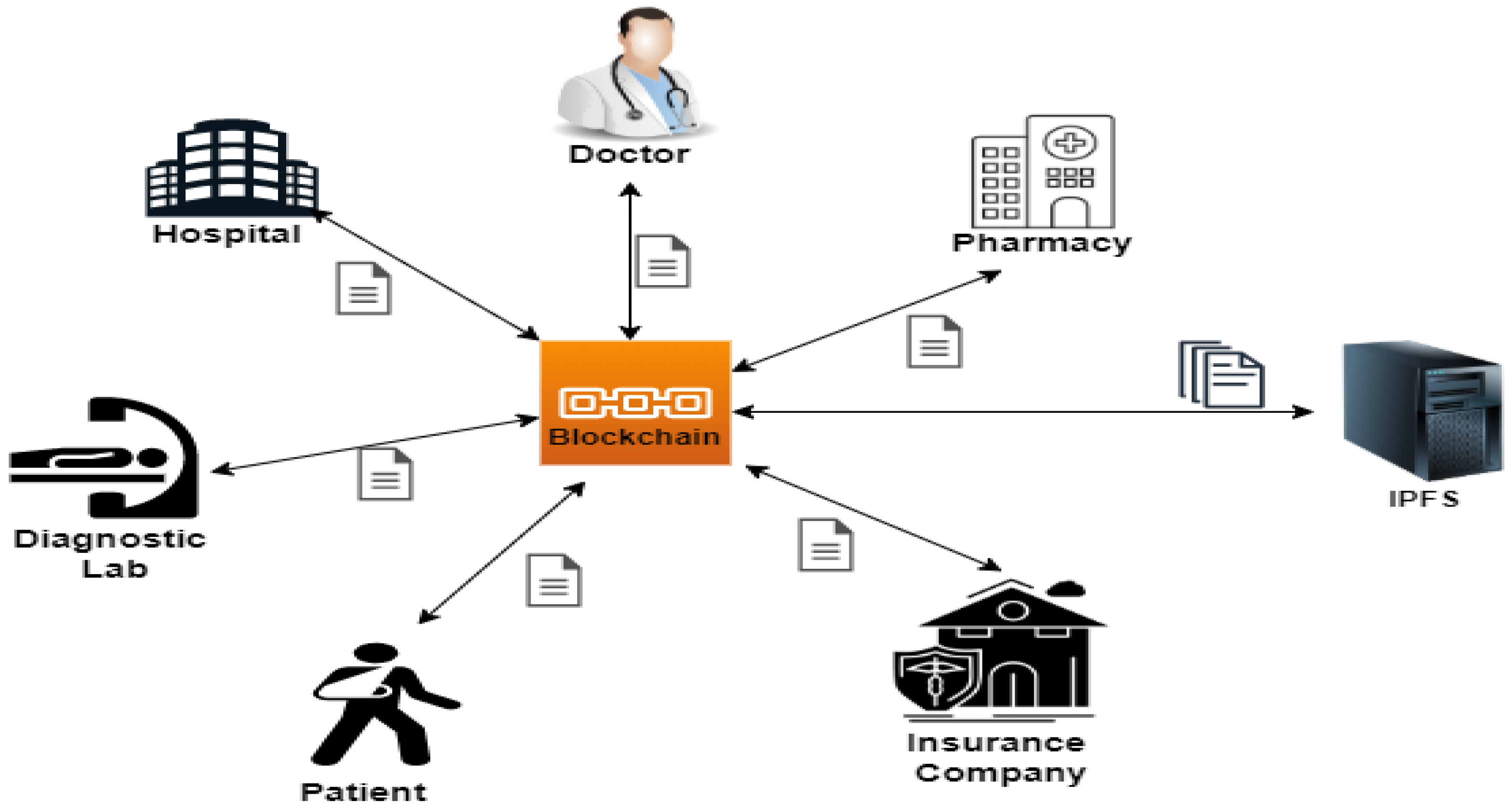
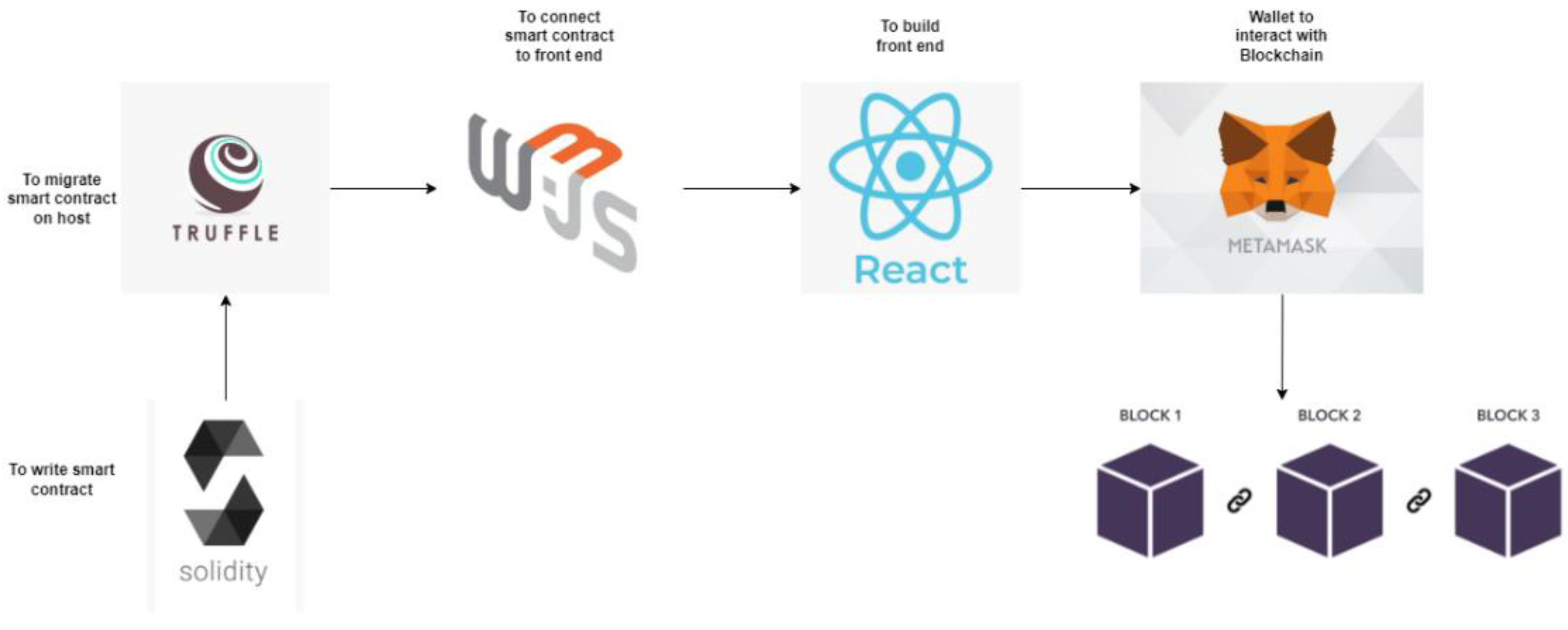
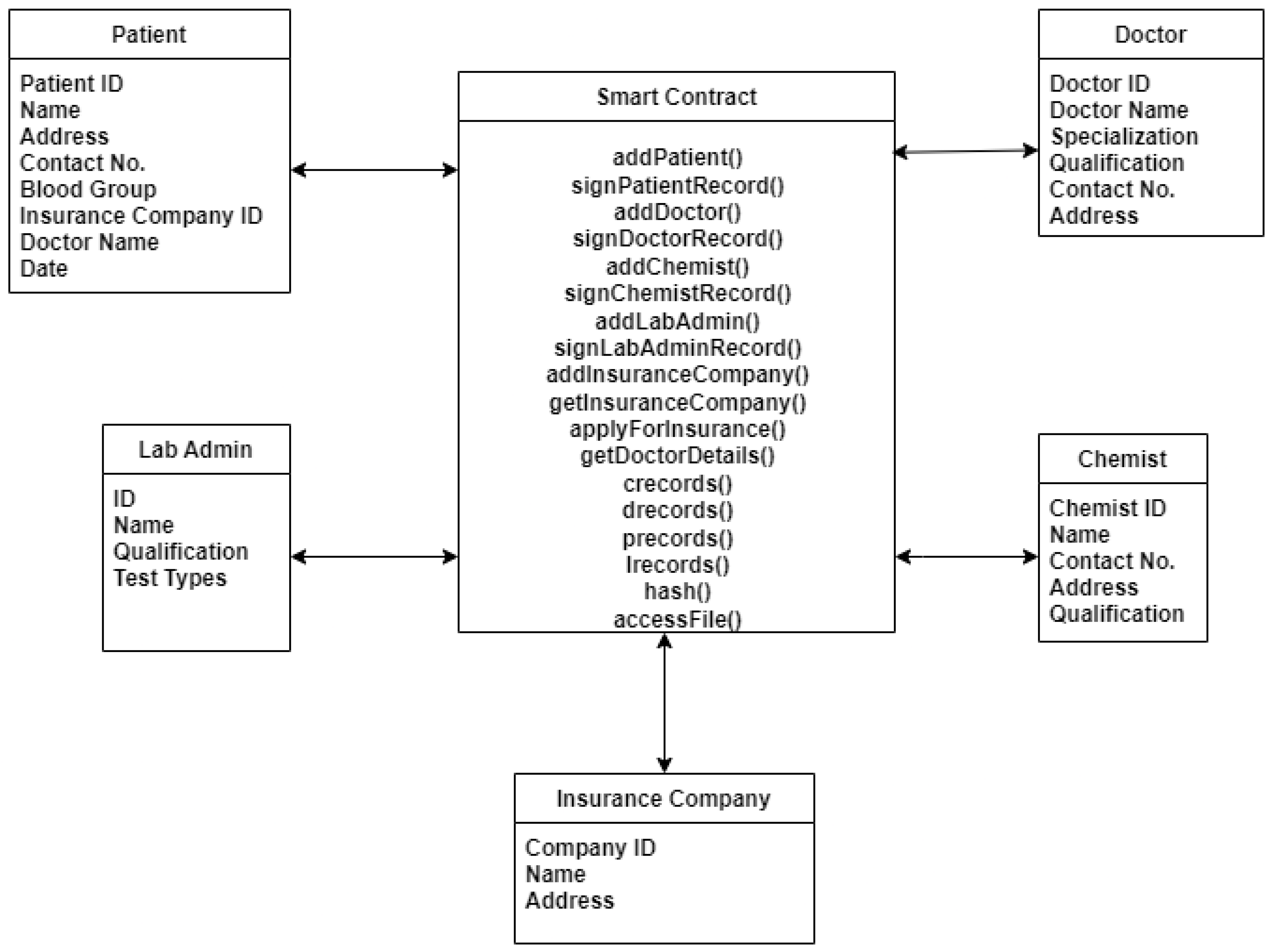
4. Proposed Architecture
5. Proposed Methodology
5.1. Registration
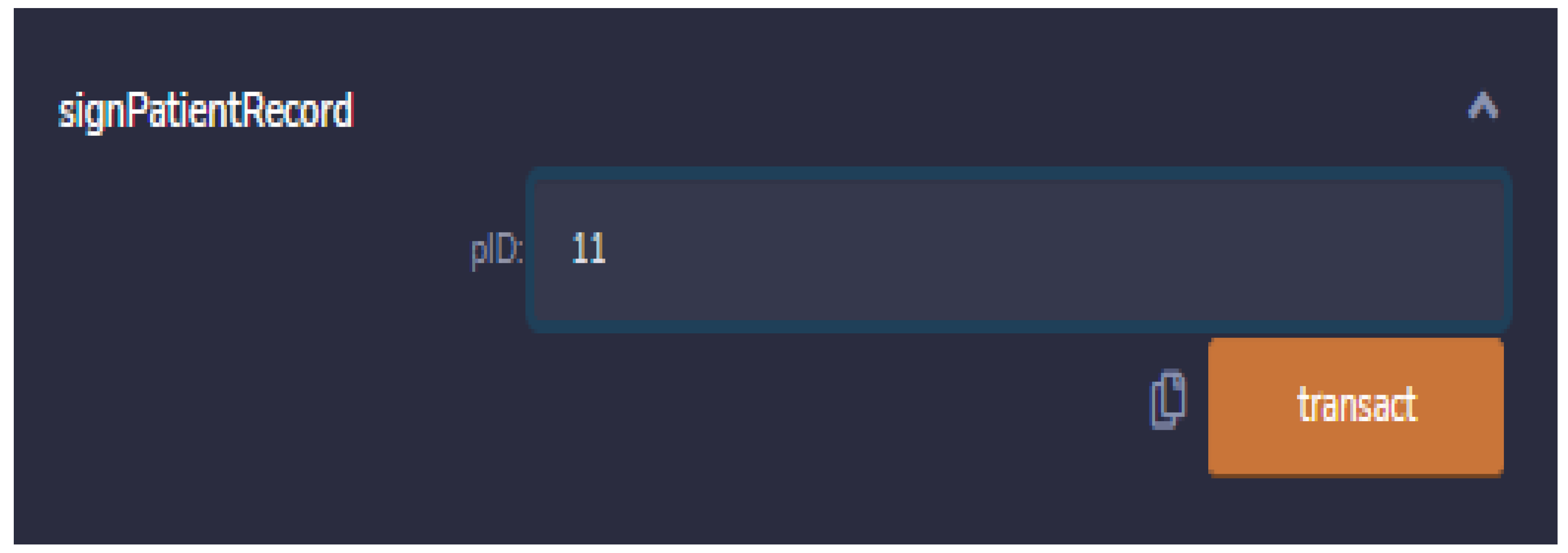
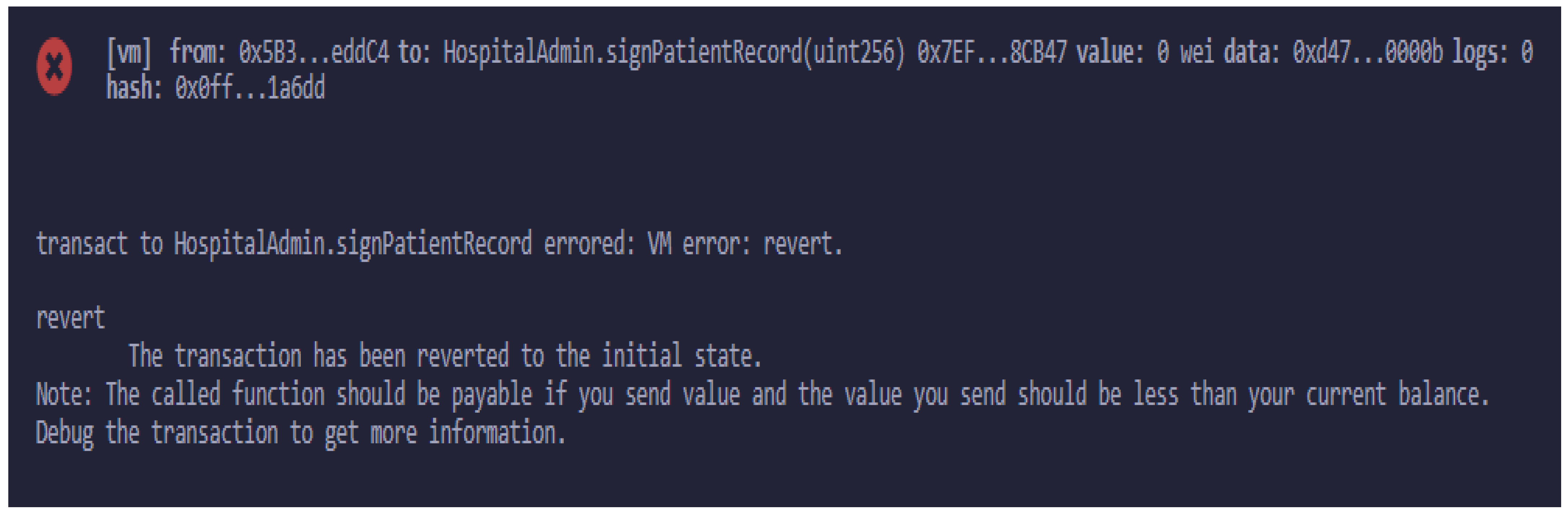
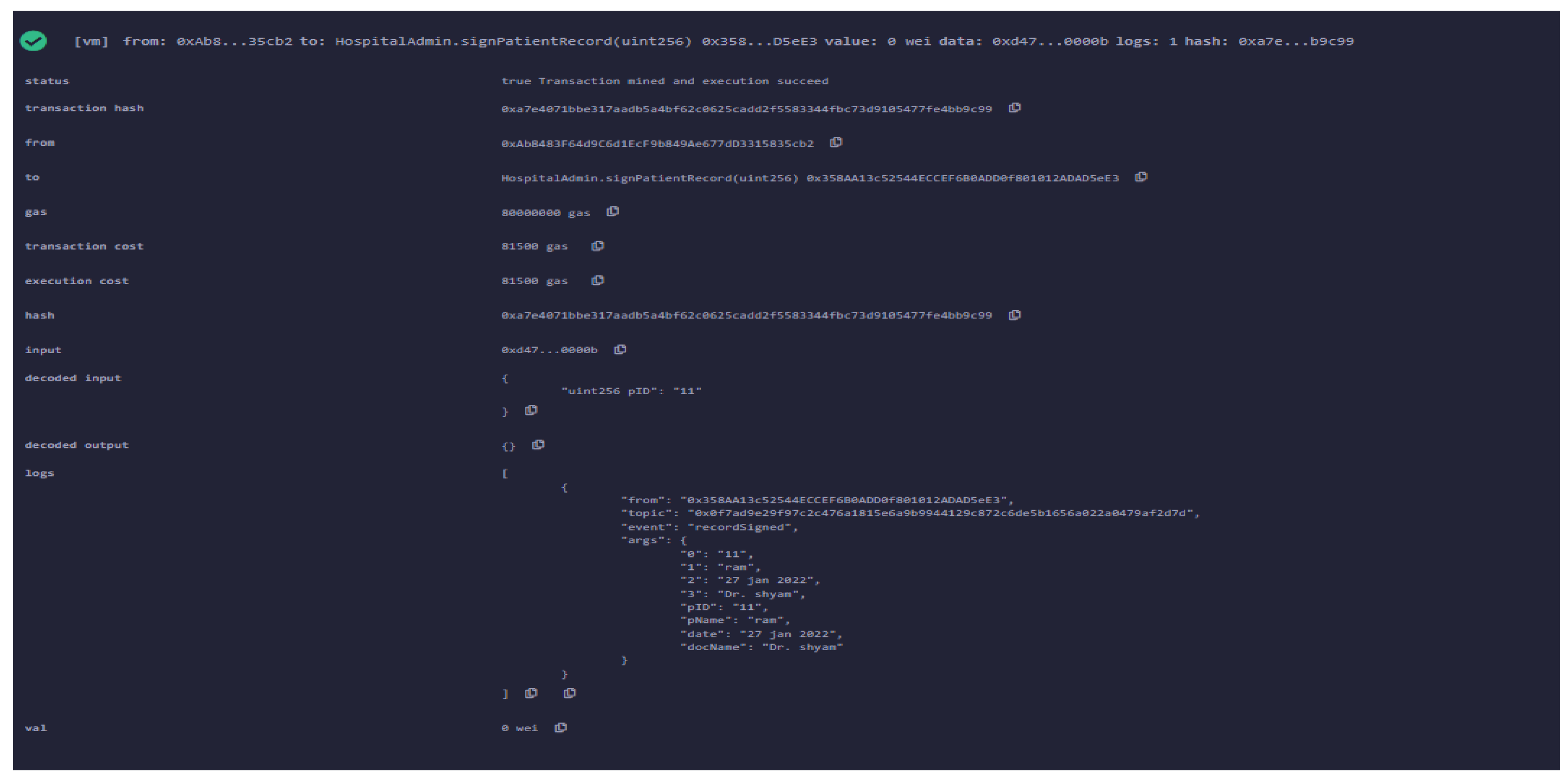
5.2. Treatment
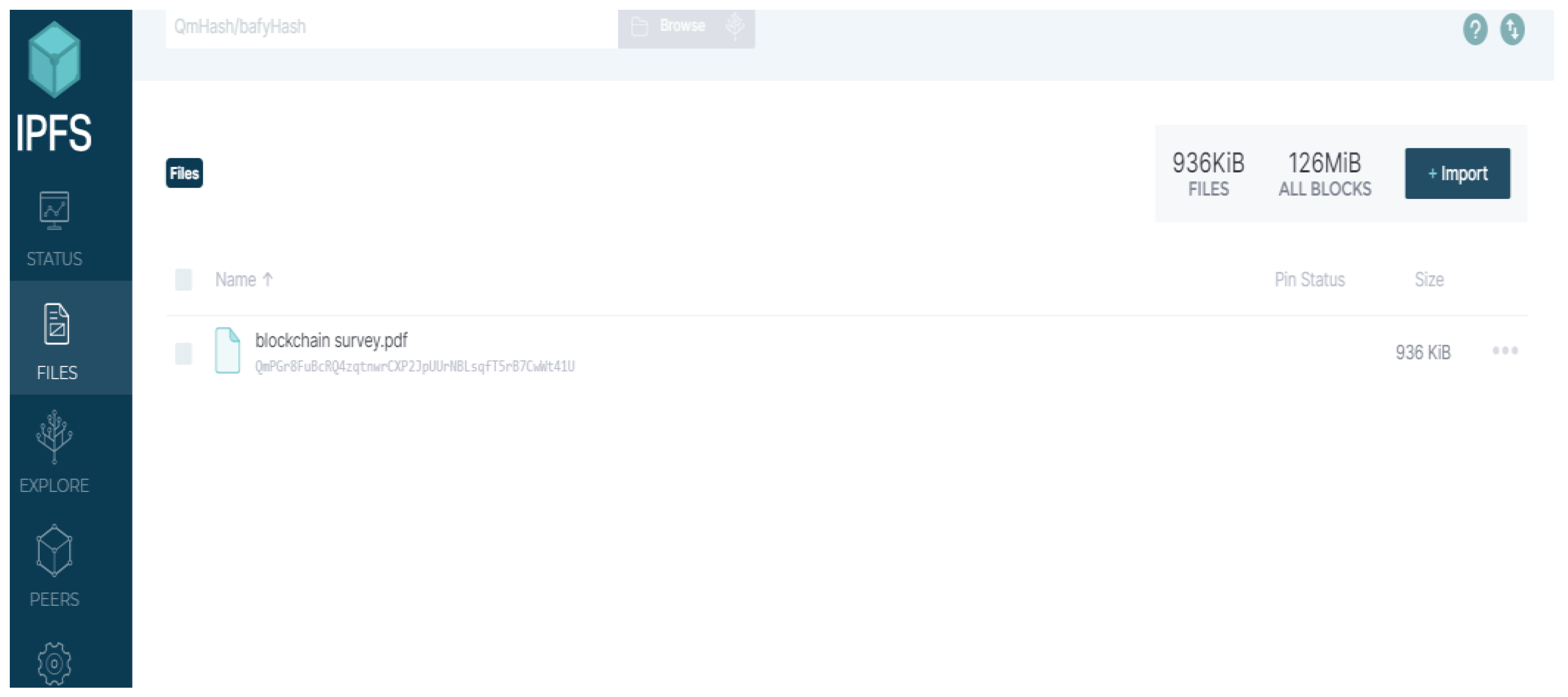
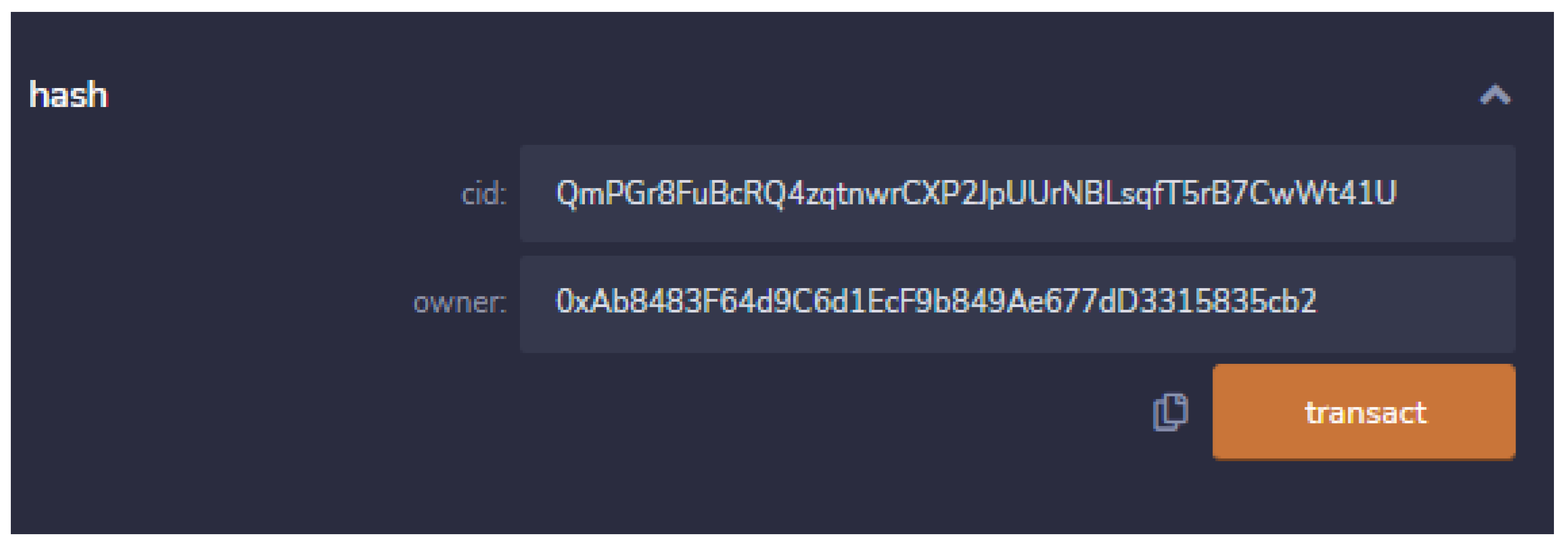
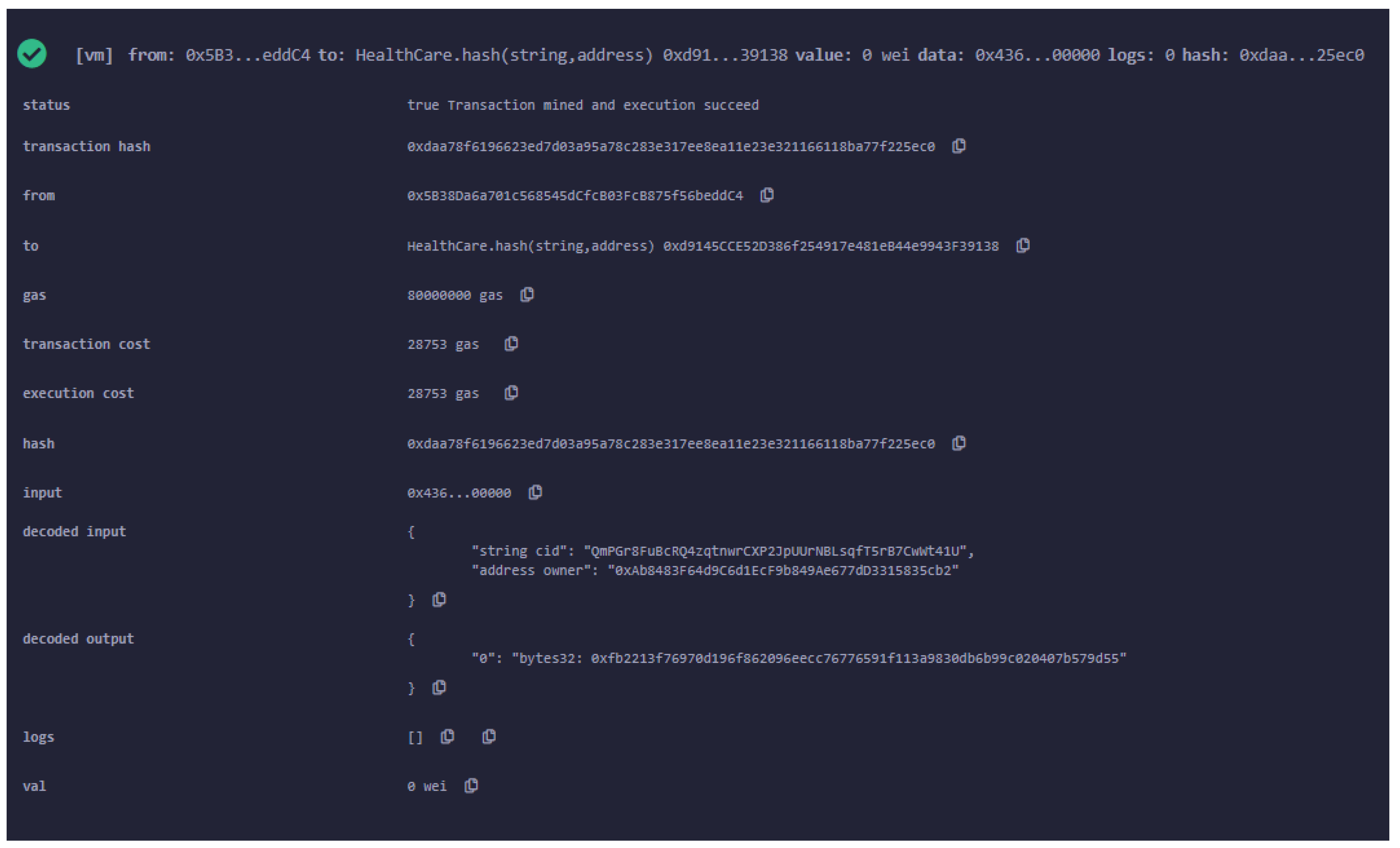
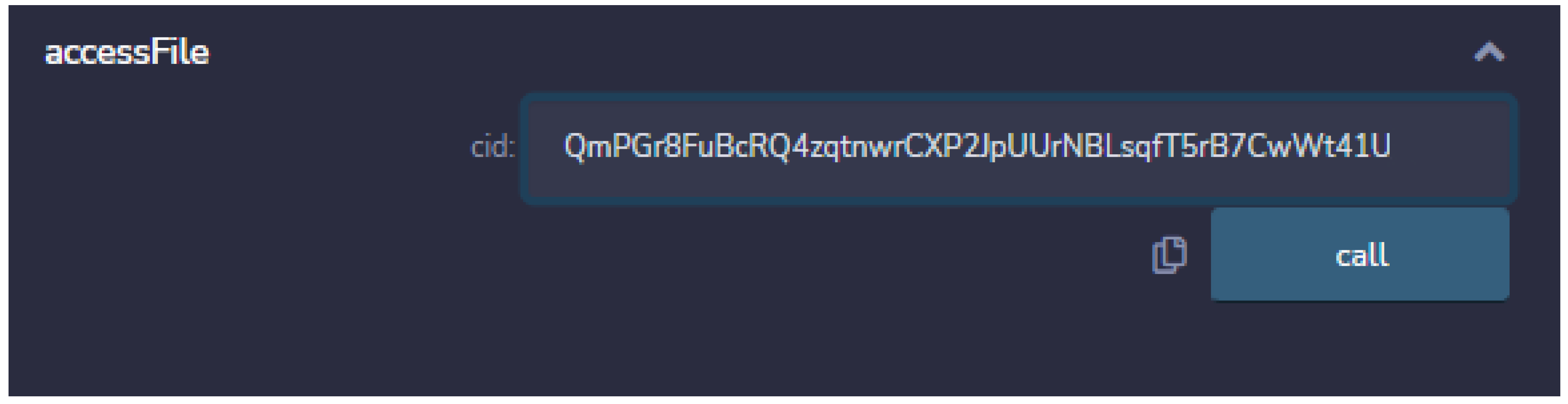
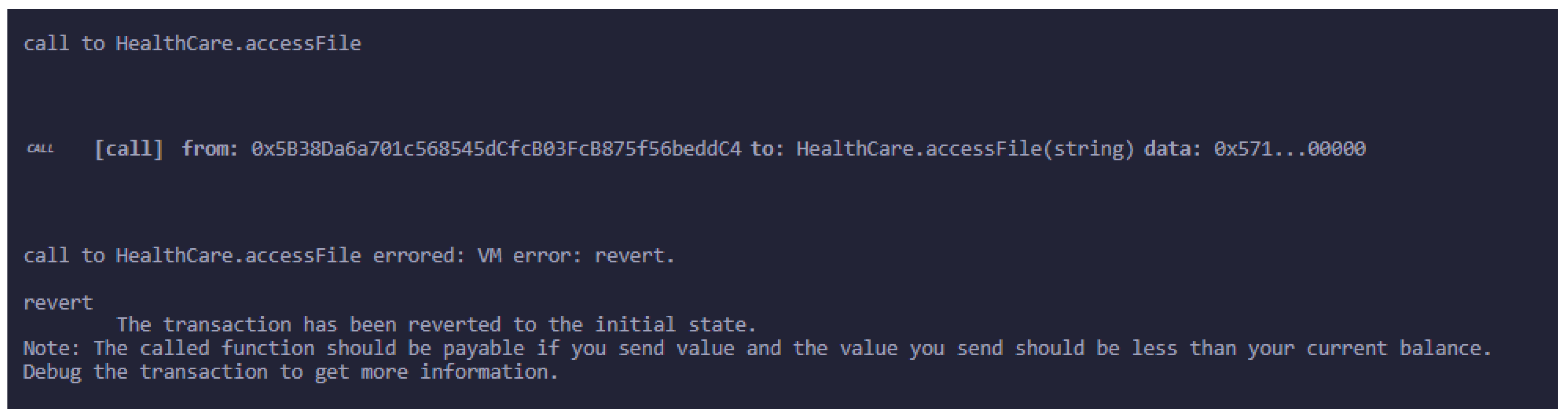
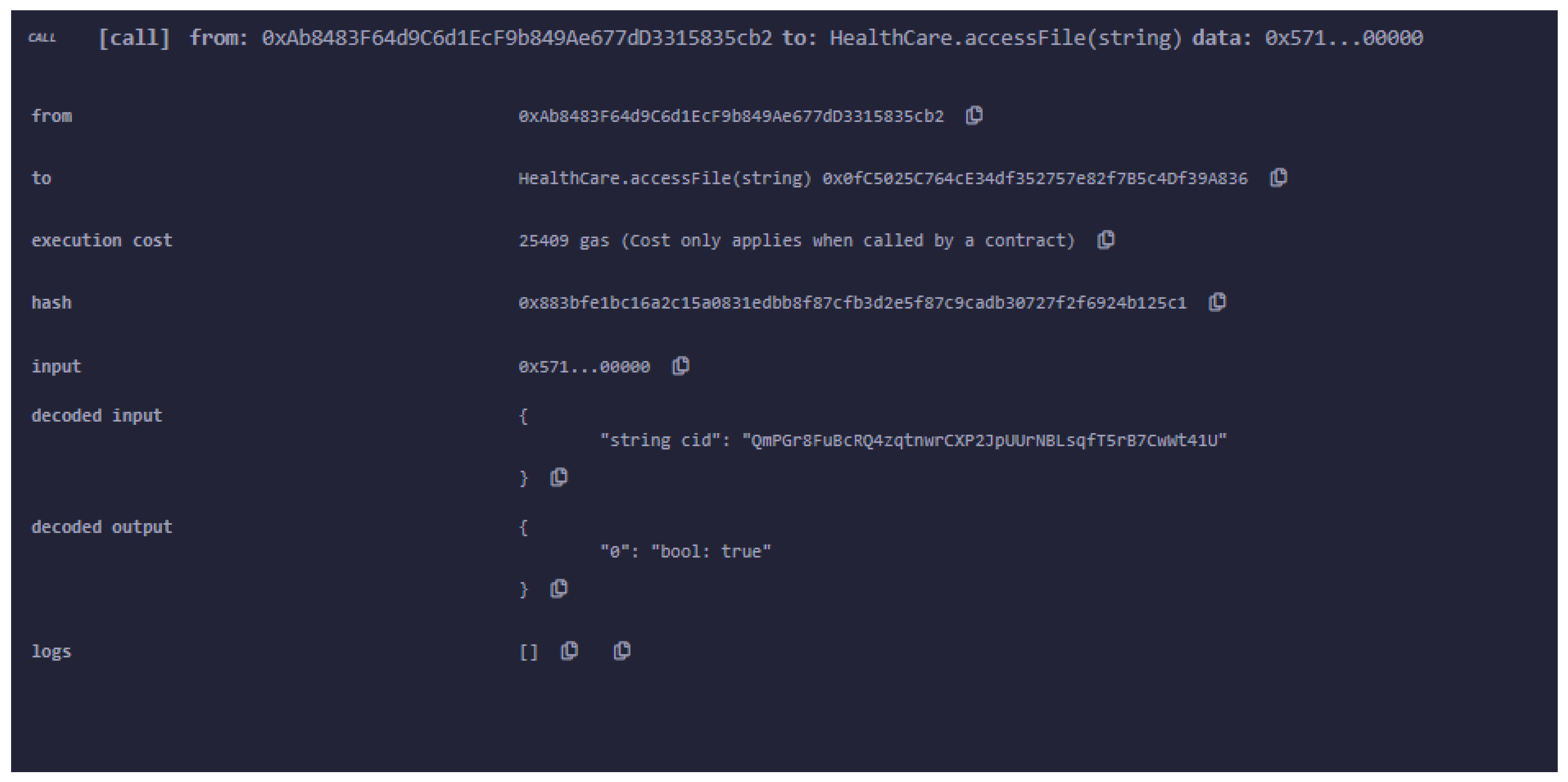
5.3. Document Upload on IPFS and Association with the Owner
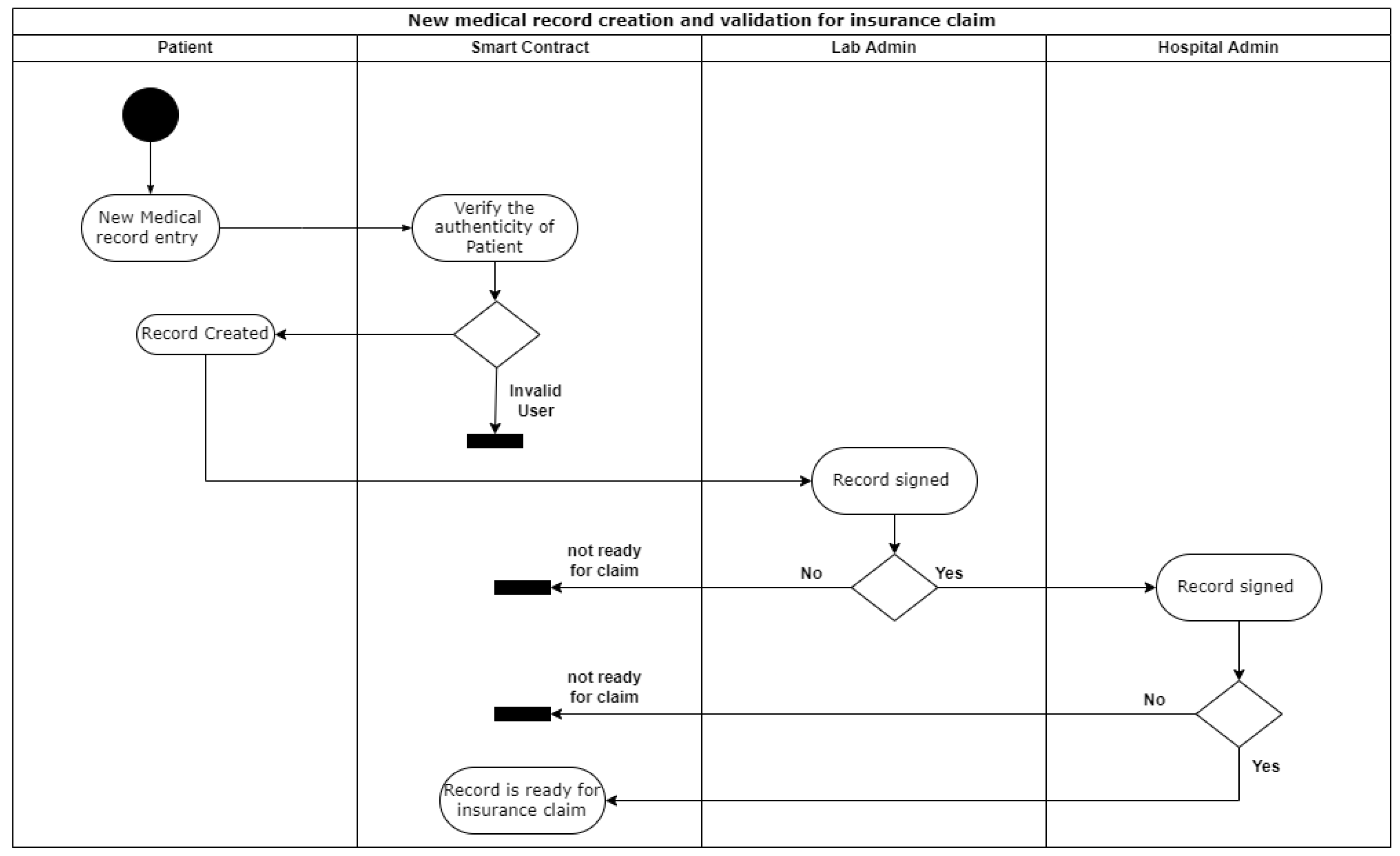
5.4. Insurance Claim
| Algorithm 1: Add New Entity |
|
| Algorithm 2: Approval of New Medical Record for Insurance Claim |
|
6. Result and Analysis
7. Research Implications
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zheng, Z.; Xie, S.; Dai, H.N.; Chen, X.; Wang, H. Blockchain challenges and opportunities: A survey. Int. J. Web Grid Serv. 2018, 14, 352–375. [Google Scholar] [CrossRef]
- Hyla, T.; Peja´s, J. Long-term verification of signatures based on a blockchain. Comput. Electr. Eng. 2020, 81, 106523. [Google Scholar] [CrossRef]
- Kumar, G.; Saha, R.; Rai, M.K.; Thomas, R.; Kim, T.H. Proof-of-work consensus approach in blockchain technology for cloud and fog computing using maximization-factorization statistics. IEEE Internet Cings J. 2019, 6, 6835–6842. [Google Scholar] [CrossRef]
- Thomason, J.; Ahmad, M.; Bronder, P.; Hoyt, E.; Pocock, S.; Bouteloupe, J.; Donaghy, K.; Huysman, D.; Willenberg, T.; Joakim, B.; et al. Blockchain—Powering and empowering the poor in developing countries. In Transforming Climate Finance and Green Investment with Blockchains; Academic Press: Cambridge, MA, USA, 2018. [Google Scholar]
- Clauson, K.A.; Breeden, E.A.; Davidson, C.; Mackey, T.K. Leveraging blockchain technology to enhance supply chain management in healthcare: An exploration of challenges and opportunities in the health supply chain. Blockchain Healthc. Today 2018, 1, 1–12. [Google Scholar] [CrossRef]
- Sylim, P.; Liu, F.; Marcelo, A.; Fontelo, P. Blockchain technology for detecting falsified and substandard drugs in distribution: Pharmaceutical supply chain intervention. JMIR Res. Protoc. 2018, 7, e10163. [Google Scholar] [CrossRef]
- Dagher, G.G.; Mohler, J.; Milojkovic, M.; Marella, P.B. Ancile: Privacy-preserving framework for access control and interoperability of electronic health records using blockchain technology. Sustain. Cities Soc. 2018, 39, 283–297. [Google Scholar] [CrossRef]
- Hathaliya, J.J.; Tanwar, S.; Tyagi, S.; Kumar, N. Securing electronics healthcare records in healthcare 4.0: A biometricbased approach. Comput. Electr. Eng. 2019, 76, 398–410. [Google Scholar] [CrossRef]
- Azzi, R.; Chamoun, R.K.; Sokhn, M. The power of a blockchain-based supply chain. Comput. Ind. Eng. 2019, 135, 582–592. [Google Scholar] [CrossRef]
- Bhutta, M.N.M.; Bhattia, S.; Alojail, M.A.; Nisar, K.; Cao, Y.; Chaudhry, S.A.; Sun, Z. Towards Secure IoT-Based Payments by Extension of Payment Card Industry Data Security Standard (PCI DSS). Wirel. Commun. Mob. Comput. 2022, 2022, 10. [Google Scholar] [CrossRef]
- Kumar, A.; Sharma, S.; Singh, A.; Alwadain, A.; Choi, B.J.; Manual-Brenosa, J.; Goyal, N. Revolutionary Strategies Analysis and Proposed System for Future Infrastructure in Internet of Things. Sustainability 2021, 14, 71. [Google Scholar] [CrossRef]
- Francisco, K.; Swanson, D. The Supply chain has no clothes: Technology adoption of blockchain for supply chain transparency. Logistics 2018, 2, 2. [Google Scholar] [CrossRef] [Green Version]
- Verhoeven, P.; Sinn, F.; Herden, T. Examples from blockchain implementations in logistics and supply chain management: Exploring the mindful use of a new technology. Logistics 2018, 2, 20. [Google Scholar] [CrossRef] [Green Version]
- Figorilli, S.; Antonucci, F.; Costa, C. A Blockchain Implementation Prototype for the Electronic Open Source Traceability of Wood along the Whole Supply Chain. Sensors 2018, 18, 3133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemieux, V.L. Trusting records: Is Blockchain technology the answer? Rec. Manag. J. 2016, 26, 110–139. [Google Scholar] [CrossRef]
- Weber, I.; Xu, X.; Riveret, R.; Governatori, G.; Ponomarev, A.; Mendling, J. Untrusted business process monitoring and execution using blockchain. In Proceedings of the International Conference on Business Process Management, Rome, Italy, 6–10 September 2016; Springer: Cham, Switzerland, 2016. [Google Scholar]
- Waseem, Q.; Alshamrani, S.S.; Nisar, K.; Wan Din, W.I.S.; Alghamdi, A.S. Future Technology: Software-Defined Network (SDN) Forensic. Symmetry 2021, 13, 767. [Google Scholar] [CrossRef]
- Daisuke, I.; Kashiyama, M.; Ueno, T. Tamper-resistant mobile health using blockchain technology. JMIR Mhealth Uhealth 2017, 5, e111. [Google Scholar]
- Vazirani, A.A.; O’Donoghue, O.; Brindley, D.; Meinert, E. Implementing Blockchains for Efficient Health Care: Systematic Review. J. Med. Internet Res. 2019, 21, e12439. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, Z.; Khan, A.S.; Nisar, K.; Haider, I.; Hassan, R.; Haque, M.; Tarmizi, S.; Rodrigues, J. Anomaly Detection Using Deep Neural Network for IoT Architecture. Appl. Sci. 2021, 11, 7050. [Google Scholar] [CrossRef]
- Sabir, Z.; Ibrahim, A.A.A.; Raja, M.A.Z.; Nisar, K.; Umar, M.; Rodrigues, J.J.P.C.; Mahmoud, S.R. Soft Computing Paradigms to Find the Numerical Solutions of a Nonlinear Influenza Disease Model. Appl. Sci. 2021, 11, 8549. [Google Scholar] [CrossRef]
- Shen, B.; Guo, J.; Yang, Y. MedChain: Efficient Healthcare Data Sharing via Blockchain. Appl. Sci. 2019, 9, 1207. [Google Scholar] [CrossRef] [Green Version]
- Haque, M.R.; Tan, S.C.; Yusoff, Z.; Nisar, K.; Lee, C.K.; Kaspin, R.; Shankar Chowdhry, B.; Buyya, R.; Prasad Majumder, S.; Gupta, M.; et al. Automated controller placement for software-defined networks to resist DDoS attack. Comput. Mater. Contin. 2021, 68, 3147–3165. [Google Scholar] [CrossRef]
- Litchfield, A.T.; Khan, A. A Review of Issues in Healthcare Information Management Systems and Blockchain Solutions. In Proceedings of the CONF-IRM, International Conference on Information Resources Management, CONF-IRM 2019, Auckland, New Zealand, 27–29 May 2019. [Google Scholar]
- Wei, L.L.Y.; Ibrahim, A.A.A.; Nisar, K.; Ismail, Z.I.A.; Welch, I. Survey on Geographic Visual Display Techniques in Epidemiology: Taxonomy and Characterization. J. Ind. Inf. Integr. 2020, 18, 1–14. [Google Scholar] [CrossRef]
- Zhang, P.; Schmidt, D.C.; White, J.; Lenz, G. Blockchain Technology Use Cases in Healthcare. In Advances in Computers; Elsevier: Amsterdam, The Netherlands, 2018; Volume 111, pp. 1–41. [Google Scholar]
- Sodhro, A.H.; Al-Rakhami, M.S.; Wang, L.; Magsi, H.; Zahid, N.; Pirbhulal, S.; Nisar, K.; Ahmad, A. Decentralized Energy Efficient Model for Data Transmission in IoT-based Healthcare System. In Proceedings of the 2021 IEEE 93rd Vehicular Technology Conference (VTC2021-Spring), Helsinki, Finland, 25–28 April 2021; pp. 1–5. [Google Scholar] [CrossRef]
- Shuja, J.; Ahmad, R.W.; Gani, A.; Ahmed, A.I.A.; Siddiqa, A.; Nisar, K.; Khan, S.U.; Zomaya, A.Y. Greening emerging IT technologies: Techniques and practices. J. Internet Serv. Appl. (JISA) 2017, 89, 1–11. [Google Scholar] [CrossRef]
- Lee, S.H.; Yang, C.S. Fingernail analysis management system using microscopy sensor and blockchain technology. Int. J. Distrib. Sens. Netw. 2018, 14, 1550147718767044. [Google Scholar] [CrossRef] [Green Version]
- Agbo, C.C.; Mahmoud, Q.H.; Eklund, J.M. Blockchain technology in healthcare: A systematic review. Healthcare 2019, 7, 56. [Google Scholar] [CrossRef] [Green Version]
- Haider, I.; Khan, K.B.; Haider, M.A.; Saeed, A.; Nisar, K. Automated Robotic System for Assistance of Isolated Patients of Coronavirus (COVID-19). In Proceedings of the 2020 IEEE 23rd International Multitopic Conference (INMIC), Bahawalpur, Pakistan, 5–7 November 2020; pp. 1–6. [Google Scholar] [CrossRef]
- Haider, I.; Mehdi, M.A.; Amin, A.; Nisar, K. A Hand Gesture Recognition based Communication System for Mute people. In Proceedings of the 2020 IEEE 23rd International Multitopic Conference (INMIC), Bahawalpur, Pakistan, 5–7 November 2020; pp. 1–6. [Google Scholar] [CrossRef]
- Kumar, T.; Ramani, V.; Ahmad, I.; Braeken, A.; Harjula, E.; Ylianttila, M. Blockchain Utilization in Healthcare: Key Requirements and Challenges. In Proceedings of the 2018 IEEE 20th International Conference on e-Health Networking, Applications and Services (Healthcom), Ostrava, Czech Republic, 17–20 September 2018. [Google Scholar]
- Genestier, P.; Zouarhi, S.; Limeux, P.; Excoer, D.; Prola, A.; Sandon, S.; Temerson, J.M. Blockchain for consent management in the ehealth environment: A nugget for privacy and security challenges. J. Int. Soc. Telemed. Ehealth 2017, 5, GKR-e24. [Google Scholar]
- Chowdhry, B.S.; Shah, A.A.; Harris, N.; Hussain, T.; Nisar, K. Development of a Smart Instrumentation for Analyzing Railway Track Health Monitoring Using Forced Vibration. In Proceedings of the 2020 IEEE 14th International Conference on Application of Information and Communication Technologies (AICT), Tashkent, Uzbekistan, 7–9 November 2020; pp. 1–5. [Google Scholar] [CrossRef]
- Boulos, M.N.K.; Wilson, J.T.; Clauson, K.A. Geospatial blockchain: Promises, challenges, and scenarios in health and healthcare. Int. J. Health Geogr. 2018, 17, 25. [Google Scholar] [CrossRef]
- Khatoon, A. A Blockchain-Based Smart Contract System for Healthcare Management. Electronics 2020, 9, 94. [Google Scholar] [CrossRef] [Green Version]
- Thomas, J. Medical records and issues in negligence. Indian J. Urol. 2009, 25, 384–388. [Google Scholar] [CrossRef]
- Thenmozhi, M.; Dhanalakshmi, R.; Geetha, S.; Valli, R. Implementing blockchain technologies for health insurance claim processing in hospitals. In Proceedings of the 2020 IEEE 23rd International Multitopic Conference (INMIC), Bahawalpur, Pakistan, 5–7 November 2020. [Google Scholar]
- Pandit, M.; Gupta, D.; Anand, D.; Goyal, N.; Aljahdali, H.M.; Mansilla, A.O.; Kumar, A. Towards Design and Feasibility Analysis of DePaaS: AI Based Global Unified Software Defect Prediction Framework. Appl. Sci. 2022, 12, 493. [Google Scholar] [CrossRef]
- Nisar, K.; Ibrahim, A.A.A.; Wu, L.; Adamov, A.; Deen, M.J. Smart home for elderly living using Wireless Sensor Networks and an Android application. In Proceedings of the 2016 10th IEEE International Conference on Application of Information and Communication Technologies AICT2016, Azerbaijan, Baku, 12–14 October 2016; pp. 1–8. [Google Scholar] [CrossRef]
- Rana, S.K.; Rana, S.K. Blockchain based business model for digital assets management in trust less collaborative environment. J. Crit. Rev. 2020, 7, 738–750. [Google Scholar]
- Lilhore, U.K.; Imoize, A.L.; Lee, C.-C.; Simaiya, S.; Pani, S.K.; Goyal, N.; Kumar, A.; Li, C.-T. Enhanced Convolutional Neural Network Model for Cassava Leaf Disease Identification and Classification. Mathematics 2022, 10, 580. [Google Scholar] [CrossRef]
- Jamil, F.; Qayyum, F.; Alhelaly, S.; Javed, F.; Muthanna, A. Intelligent Microservice Based on Blockchain for Healthcare Applications. Comput. Mater. Contin. 2021, 69, 2513–2530. [Google Scholar] [CrossRef]
- Kumar, A.; Sharma, S. IFTTT rely based a semantic web approach to simplifying trigger-action programming for end-user application with IoT applications. In Semantic IoT: Theory and Applications; Springer: Cham, Switzerland, 2021; pp. 385–397. [Google Scholar]
- Khezr, S.; Moniruzzaman, M.; Yassine, A.; Benlamri, R. Blockchain technology in healthcare: A comprehensive review and directions for future research. Appl. Sci. 2019, 9, 1736. [Google Scholar] [CrossRef] [Green Version]
- Rana, A.K.; Sharma, S. Industry 4.0 manufacturing based on IoT, cloud computing, and big data: Manufacturing purpose scenario. In Advances in Communication and Computational Technology; Springer: Singapore, 2021; pp. 1109–1119. [Google Scholar]
- Ratta, P.; Kaur, A.; Sharma, S.; Shabaz, M.; Dhiman, G. Application of Blockchain and Internet of Things in Healthcare and medical sector: Application, challenges and future prespectives. J. Food Qual. 2021, 2021, 1–20. [Google Scholar] [CrossRef]
- Rana, A.K.; Sharma, S. Enhanced energy-efficient heterogeneous routing protocols in WSNs for IoT application. IJEAT 2019, 9, 4418–4425. [Google Scholar] [CrossRef]
- Hasselgren, A.; Rensaa, J.A.H.; Kralevska, K.; Gligoroski, D.; Faxvaag, A. Blockchain for Increased Trust in Virtual Health Care Proof-of-Concept Study. J. Med. Internet Res. 2021, 23, 1–15. [Google Scholar] [CrossRef]
- Sarkar, N.I.; Kuang, A.X.M.; Nisar, K.; Amphawan, A. Performance Studies of Integrated Network Scenarios in a Hospital Environment. Int. J. Inf. Commun. Technol. Hum. Dev. (IJICTHD) 2014, 6, 35–68. [Google Scholar] [CrossRef] [Green Version]
- Rana, A.K.; Sharma, S. Contiki Cooja Security Solution (CCSS) with IPv6 routing protocol for low-power and lossy networks (RPL) in Internet of Things applications. In Mobile Radio Communications and 5G Networks; Springer: Singapore, 2021; pp. 251–259. [Google Scholar]
- Rana, S.K.; Kim, H.C.; Pani, S.K.; Rana, S.K.; Joo, M.I.; Rana, A.K.; Aich, S. Blockchain-Based Model to Improve the Performance of the Next-Generation Digital Supply Chain. Sustainability 2021, 13, 10008. [Google Scholar] [CrossRef]
- Kumar, A.; Sharma, S.; Goyal, N.; Singh, A.; Cheng, X.; Singh, P. Secure and energy-efficient smart building architecture with emerging technology IoT. Comput. Commun. 2021, 176, 207–217. [Google Scholar] [CrossRef]
- Nisar, N.; Hasbullah, H. The Effect of Panoramic View of a Digital Map on User Satisfaction. In Proceedings of the International Symposium on Information Technology 2008 (ITSim2008), KLCC, Kuala Lumpur, Malaysia, 26–28 August 2008; pp. 1–4. [Google Scholar] [CrossRef]
- Hasbullah, H.; Nisar, K.; Said, A. The effect of echo on voice quality in VoIP network. In Proceedings of the International Association for Science and Technology Development (IASTED) Calgary, AB, Canada; Advances in Computer Science and Engineering (ACSE): Phuket, Thailand, 2009; pp. 95–100, ISBN 978-088986790-1. [Google Scholar]
- Nisar, N.; Said, A.M.; Hasbullah, H. Enhanced Performance of IPv6 Packet Transmission over VoIP Network. In Proceedings of the 2nd IEEE International Conference on Computer Science and Information Technology, Beijing, China, 11 August 2009; pp. 500–504. [Google Scholar] [CrossRef]
- Nisar, K.; Said, A.M.; Hasbullah, H. Enhanced performance of WLANs packet transmission over VoIP Network. In Proceedings of the 2010 IEEE 24th International Conference on Advanced Information Networking and Applications, Workshops, (AINA 2010), Perth, Australia, 20–23 April 2010; pp. 485–490. [Google Scholar] [CrossRef]
- Jimson, E.R.; Nisar, K.; bin Ahmad Hijazi, M.H. Bandwidth Management using Software Defined Network and Comparison of the Throughput Performance with Traditional Network. In Proceedings of the International Conference on Computer and Drone Applications (ICONDA) 2017, Kuching, Malaysia, 9–11 November 2017; pp. 71–76. [Google Scholar] [CrossRef]
- Nisar, K.; Lawal, I.A.; Abualsaud, K.; El-Fouly, T.M. A New WDM Application Response Time in WLAN Network and Fixed WiMAX using Distributed. In Proceedings of the 11th ACS/IEEE International Conference on Computer Systems and Applications (AICCSA’ 2014), Doha, Qatar, 10–13 November 2014; pp. 781–787. [Google Scholar] [CrossRef]
- Nisar, K.; Said, A.M.; Hasbullah, H. Enhanced Performance of Packet Transmission Using System Model Over VoIP Network. In Proceedings of the International Symposium on Information Technology 2010 (ITSim 2010), KLCC, Kuala Lumpur, Malaysia, 15 June 2010; pp. 1005–1008. [Google Scholar] [CrossRef]
- Sattar, F.; Hussain, M.; Nisar, K. A secure architecture for open source VoIP solutions. In Proceedings of the IEEE International Conference on Information and Communication Technologies (ICICT), Karachi, Pakistan, 23–24 July 2011; pp. 1–6. [Google Scholar]
- Rana, A.; Chakraborty, C.; Sharma, S.; Dhawan, S.; Pani, S.K.; Ashraf, I. Internet of Medical Things-Based Secure and Energy-Efficient Framework for Health Care. Big Data 2021, 10, 18–33. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.; Sharma, M.; Das, R.P.; Muduli, K.; Raut, R.; Narkhede, B.E.; Shee, H.; Misra, A. Assessing Effectiveness of Humanitarian Activities against COVID-19 Disruption: The Role of Blockchain-Enabled Digital Humanitarian Network. Sustainability 2022, 14, 1904. [Google Scholar] [CrossRef]
- Swain, S.; Peter, O.; Adimuthu, R.; Muduli, K. Blockchain technology for limiting the impact of pandemic. In Computational Modelling and Data Analysis in COVID-19 Research; CRC Press: Boca Raton, FL, USA, 2021; pp. 165–186. [Google Scholar]




























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gas Price in ETH = 0.000000122, ETH Price (USD) = 2740 | ||||
|---|---|---|---|---|
| Sr.No. | Function | Gas Consumed (GWEI) | Cost for Fast Execution (ETH) | Cost for Fast Execution (USD) |
| 1 | addPatient | 167,933 | 0.020487826 | 56.13664324 |
| 2 | addDoctor | 167,368 | 0.020418896 | 55.94777504 |
| 3 | addChemist | 143,061 | 0.017453442 | 47.82243108 |
| 4 | addlabAdmin | 143,023 | 0.017448806 | 47.80972844 |
| 5 | signPatientRecord | 81,699 | 0.009967278 | 27.31034172 |
| 6 | signDcoctorRecord | 83,693 | 0.010210546 | 27.97689604 |
| 7 | signChemistRecord | 80,596 | 0.009832712 | 26.94163088 |
| 8 | signLabAdmin | 80,332 | 0.009800504 | 26.85338096 |
| 9 | getDoctorDetails | 32,941 | 0.004018802 | 11.01151748 |
| 10 | precord | 39,277 | 0.004791794 | 13.12951556 |
| 11 | hash | 45,872 | 0.005596384 | 15.33409216 |
| 12 | accessFile | 25,434 | 0.003102948 | 8.50207752 |
| Gas Price in ETH = 0.000000115, ETH Price (USD) = 2740 | ||||
|---|---|---|---|---|
| Sr.No. | Function | Gas Consumed (GWEI) | Cost for Standard Execution (ETH) | Cost for Standard Execution (USD) |
| 1 | addPatient | 167,933 | 0.019312295 | 52.9156883 |
| 2 | addDoctor | 167,368 | 0.01924732 | 52.7376568 |
| 3 | addChemist | 143,061 | 0.016452015 | 45.0785211 |
| 4 | addlabAdmin | 143,023 | 0.016447645 | 45.0665473 |
| 5 | signPatientRecord | 81,699 | 0.009395385 | 25.7433549 |
| 6 | signDcoctorRecord | 83,693 | 0.009624695 | 26.3716643 |
| 7 | signChemistRecord | 80,596 | 0.00926854 | 25.3957996 |
| 8 | signLabAdmin | 80,332 | 0.00923818 | 25.3126132 |
| 9 | getDoctorDetails | 32,941 | 0.003788215 | 10.3797091 |
| 10 | precord | 39,277 | 0.004516855 | 12.3761827 |
| 11 | hash | 45,872 | 0.00527528 | 14.4542672 |
| 12 | accessFile | 25,434 | 0.00292491 | 8.0142534 |
| Gas Price in ETH = 0.000000109, ETH Price (USD) = 2740 | ||||
|---|---|---|---|---|
| Sr.No. | Function | Gas Consumed (GWEI) | Cost for Slow Execution (ETH) | Cost for Slow Execution (USD) |
| 1 | addPatient | 167,933 | 0.018304697 | 50.15486978 |
| 2 | addDoctor | 167,368 | 0.018243112 | 49.98612688 |
| 3 | addChemist | 143,061 | 0.015593649 | 42.72659826 |
| 4 | addlabAdmin | 143,023 | 0.015589507 | 42.71524918 |
| 5 | signPatientRecord | 81,699 | 0.008905191 | 24.40022334 |
| 6 | signDcoctorRecord | 83,693 | 0.009122537 | 24.99575138 |
| 7 | signChemistRecord | 80,596 | 0.008784964 | 24.07080136 |
| 8 | signLabAdmin | 80,332 | 0.008756188 | 23.99195512 |
| 9 | getDoctorDetails | 32,941 | 0.003590569 | 9.83815906 |
| 10 | precord | 39,277 | 0.004281193 | 11.73046882 |
| 11 | hash | 45,872 | 0.005000048 | 13.70013152 |
| 12 | accessFile | 25,434 | 0.002772306 | 7.59611844 |
| Attributes | Proposed Approach | Existing Approache [15,42] |
|---|---|---|
| Transaction execution | Fast | Slow |
| Chances of 51% attack | Low | High |
| Energy Consumption | Low | High |
| Processing power requirement | Low | High |
| Validators | Fixed | Public |
| Consensus | PoA | PoW |
| Scalability | High | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rana, S.K.; Rana, S.K.; Nisar, K.; Ag Ibrahim, A.A.; Rana, A.K.; Goyal, N.; Chawla, P. Blockchain Technology and Artificial Intelligence Based Decentralized Access Control Model to Enable Secure Interoperability for Healthcare. Sustainability 2022, 14, 9471. https://doi.org/10.3390/su14159471
Rana SK, Rana SK, Nisar K, Ag Ibrahim AA, Rana AK, Goyal N, Chawla P. Blockchain Technology and Artificial Intelligence Based Decentralized Access Control Model to Enable Secure Interoperability for Healthcare. Sustainability. 2022; 14(15):9471. https://doi.org/10.3390/su14159471
Chicago/Turabian StyleRana, Sumit Kumar, Sanjeev Kumar Rana, Kashif Nisar, Ag Asri Ag Ibrahim, Arun Kumar Rana, Nitin Goyal, and Paras Chawla. 2022. "Blockchain Technology and Artificial Intelligence Based Decentralized Access Control Model to Enable Secure Interoperability for Healthcare" Sustainability 14, no. 15: 9471. https://doi.org/10.3390/su14159471
APA StyleRana, S. K., Rana, S. K., Nisar, K., Ag Ibrahim, A. A., Rana, A. K., Goyal, N., & Chawla, P. (2022). Blockchain Technology and Artificial Intelligence Based Decentralized Access Control Model to Enable Secure Interoperability for Healthcare. Sustainability, 14(15), 9471. https://doi.org/10.3390/su14159471