1. Introduction
Half of the world’s population lacks access to essential health services [
1]. There is a shortage of 7.2 million skilled health professionals worldwide, projected to increase to 12.9 million by 2035 based on population growth models [
2]. Financial hardship affects approximately 2 billion people, with 1 billion experiencing catastrophic out-of-pocket health spending (Sustainable Development Goal indicator 3.8.2) and 344 million slipping into extreme poverty due to healthcare costs [
3]. These statistics highlight the challenges of two major indicators of Universal Health Coverage (UHC): health service coverage and health expenditures. Many developing countries, including Bangladesh, struggle to achieve UHC, similar to neighboring countries. In South Asia, all eight countries are developing, and the region’s population stands at about 1.88 billion, making it the most densely populated area globally and representing a quarter of the world’s population [
4]. According to the Sustainable Development Report, the progress toward UHC in these nations is as follows as of 2019: Maldives—69%; Sri Lanka—67%; Bhutan—62%; India—61%; Nepal—53%; Bangladesh—51%; Pakistan—45%; and Afghanistan—37% [
5]. Bangladesh has achieved 51% of its UHC goal in the past 20 years. Achieving the remaining 49% within the next 11 years will be challenging without significant changes in policy and resource support.
Bangladesh faces multiple challenges.
Table 1 shows the total HRH in South Asian countries. The standard threshold for medical doctors is 10 per 10,000 population, with only Maldives, Pakistan, and Sri Lanka meeting this target [
6]. For nursing and midwifery personnel, the threshold is 40, but only Maldives has achieved this target, with most countries falling far below [
7]. The WHO recommends a dentist-to-population ratio of 1.33:10,000 for developing countries [
8]. Regarding pharmacists, while no WHO standard was found, a survey across 89 countries showed a population density of 6 pharmacists per 10,000 people. Only India and Maldives in South Asia have reached this common density [
9]. There is no WHO standard for the number of community health workers (CHWs), but they play a crucial role where resources are limited. CHWs have the potential to extend healthcare to remote and marginalized communities, addressing unmet health needs and improving access to services and health system performance [
10].
In terms of financial hardship, the out-of-pocket expenditure in Bangladesh is 74% (2020), with a Gross Domestic Product (GDP) per capita of only USD 2233 during the same period. For comparison, as a developed country, Japan’s out-of-pocket expenditure is 12.57% (2020), and its GDP per capita is USD 41,683.09 [
11,
12]. According to the WHO, the recommended out-of-pocket expenditure threshold is 10% [
13]. Bangladesh’s out-of-pocket expenditure is more than seven times higher than this standard threshold.
Various service models exist to provide healthcare services in Bangladesh, and they are making progress. However, they have limitations in overcoming the aforementioned challenges toward achieving Universal Health Coverage (UHC). Governmental organizations are facing challenges, such as a shortage of resources, corruption, and bureaucratic complexities, in addressing UHC challenges. Private healthcare services are excessively priced, creating an imbalance compared to income ratios [
14]. Additionally, private healthcare facilities primarily focus on urban areas and are not accessible to all. Non-governmental organizations (NGOs) also contribute to the healthcare sector to address UHC challenges, but their project-based and donor-oriented activities are not sustainable enough to serve as a long-term solution on a wide scale. As the challenges remain with the existing service models, there is a need to explore new approaches to enhance the healthcare scenario and accelerate UHC activities.
In a developing country like Bangladesh, increasing the necessary healthcare workforce, increasing 0 insurance coverage to 100% coverage, and making changes in other relevant policies within a short time are quite difficult. But one positive aspect is Bangladesh’s progress in building digital infrastructure. Leveraging advanced digital health mechanisms can potentially help to enhance this progress. Digital health significantly contributes to advancing Universal Health Coverage (UHC) by enhancing accessibility through telemedicine, mobile apps, and electronic health records. Continuous health monitoring empowers individuals to take proactive measures, reducing the risk of severe health issues. Data analytics in digital records facilitates informed decision-making and efficient resource allocation, improving healthcare efficiency. Moreover, it is cost-effective, aiding in reducing healthcare costs [
15,
16,
17,
18].
Developing countries are actively embracing digital health, as seen in the Global Digital Health Monitor (GDHM), and utilizing the WHO/ITU eHealth Strategy Toolkit.
Table 2 illustrates the progress in South Asian countries, emphasizing the need for continued efforts to achieve targets [
19].
To assist in overcoming the challenges of UHC in Bangladesh and to address the limitations of current service delivery approaches, this study aims to achieve the following outcomes:
Introduce the Micro Healthcare Entrepreneurship (MHE) concept as a new bottom-up service delivery approach to overcome the limitations of existing mechanisms toward achieving UHC.
Understand the prospects of the MHE concept among the existing community-based service providers.
List the challenges associated with MHE implementation by the existing service providers.
The proposed Micro Healthcare Entrepreneurship (MHE) concept combines digital health, community-based entrepreneurs/resources, and a social business fund. The success of digital healthcare technology and social business funds has been proven in different settings, but how these components will work together to create community-based health entrepreneurs is not yet known. The research hypothesis suggests that community healthcare service providers in Bangladesh might be interested in adopting the MHE concept over the existing approaches in their community.
The rest of this paper is organized as follows:
Section 2 introduces the MHE concept,
Section 3 describes the method and results,
Section 4 discusses the potential impacts and limitations, and
Section 5 concludes the report with a description of future works.
2. Micro Healthcare Entrepreneurship (MHE) Concept
In response to the challenges mentioned in the previous section, this study proposes the MHE concept to facilitate UHC in developing countries with low-resource settings. MHE refers to a community-based microenterprise equipped with digital health technologies and local human resources aimed at delivering affordable primary healthcare services to the doorsteps of unreached communities.
The MHE concept was inspired by the Grameen model. Local resources are given top priority, and the beneficiaries themselves are the main driving force. The Grameen model proved successful in increasing access to finance, connectivity, and electricity and solving various social problems. The MHE concept follows the Grameen model to increase access to healthcare. The Grameen Bank model is globally recognized as the “grassroots” of microfinance models and received the 2006 Nobel Peace Prize along with the founder Muhammad Yunus [
20].
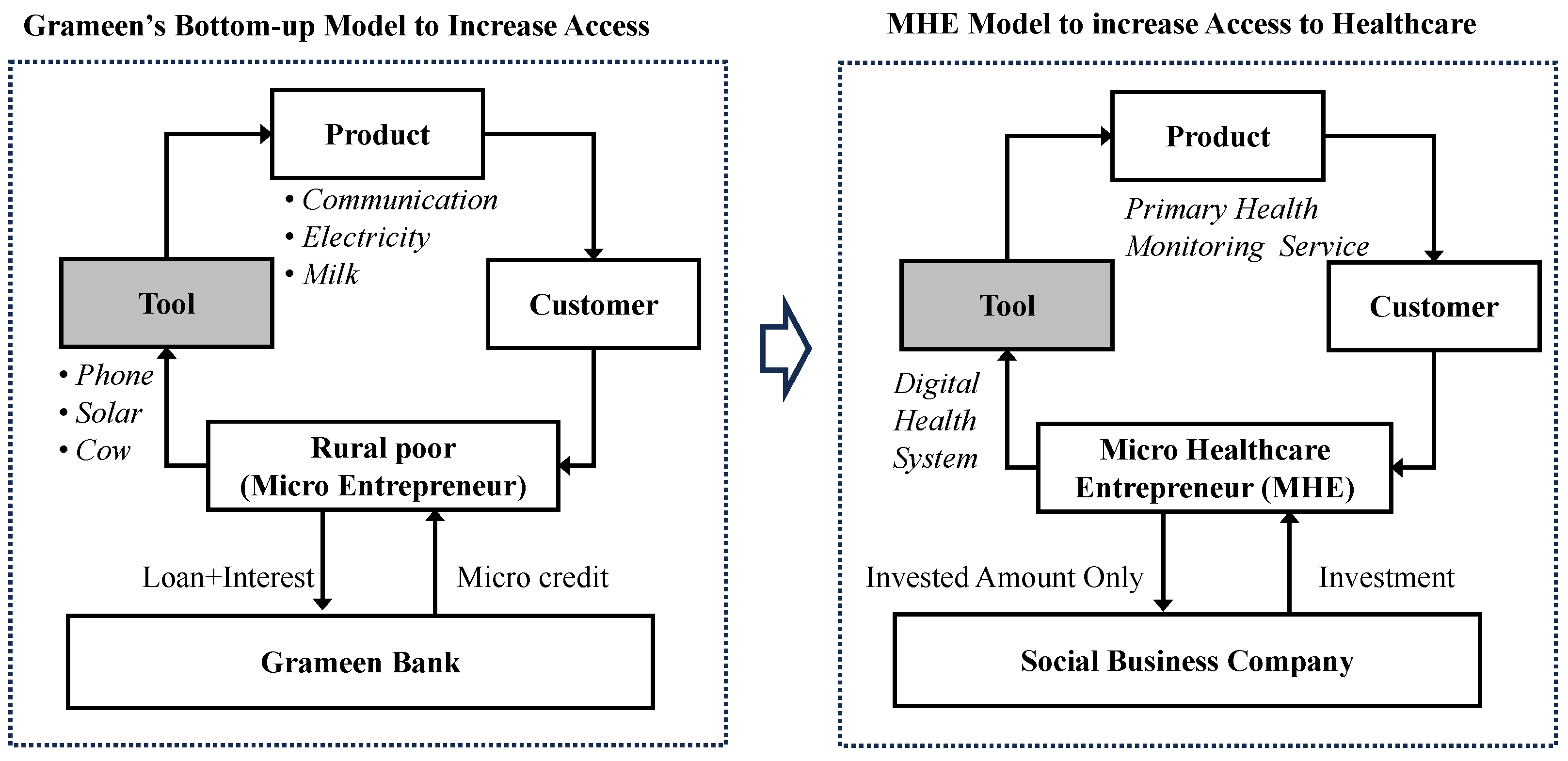
Figure 1 illustrates the basic structure of the Grameen model. The Grameen Bank generated funds and provided them to poor, rural women, who purchased phones as tools to use for business. Their product was phone call services when mobile phones were not widely available, and other community members were their customers. After making a profit, the women entrepreneurs returned the money to the Grameen Bank with interest. Following this Grameen model, approximately 10 million beneficiaries in Bangladesh improved their lives by just replacing products/services, such as solar panels, yogurt, cows, etc.
The proposed MHE model adopts the same architecture. Rather than receiving a loan from a microfinance institute, the MHE receives investments from social business companies in a non-loss, non-dividend manner. The social business company becomes their financial partner and provides mentorship about the business.
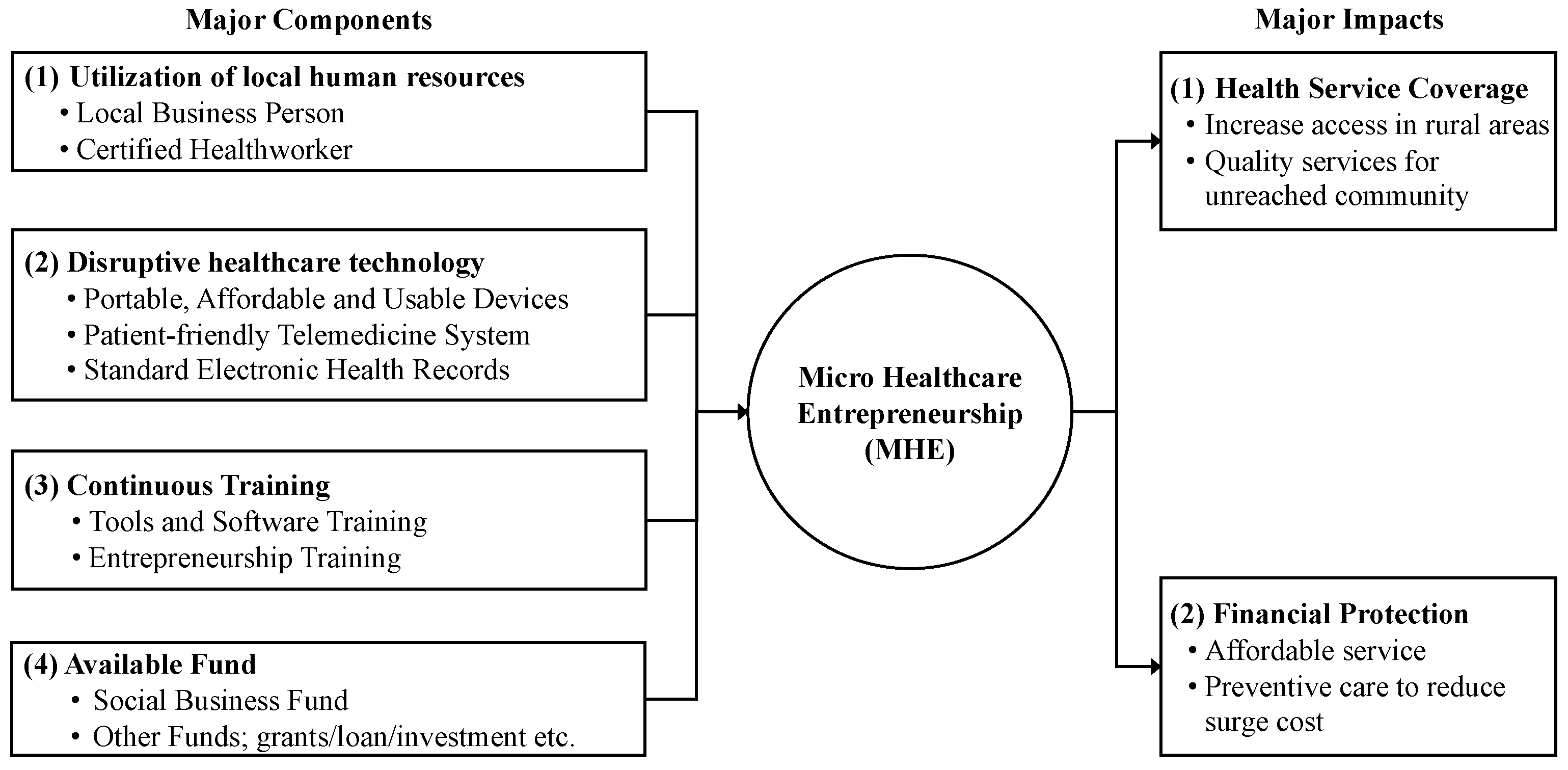
MHE has four major components: (1) local human resources; (2) portable, affordable, and usable technology; (3) continuous training; and (4) available funds. The study assumes that this proposed concept can assist in accelerating UHC progress. The current service providers in developing countries like Bangladesh have limitations in overcoming the UHC challenge.
Table 3 summarizes the limitations of the current service providers in Bangladesh and compares them to the proposed concept. Health entrepreneurs are very keen to engage with other entrepreneurs and innovators not only when it comes to putting new healthcare technology to use but also when it comes to engaging with the most vulnerable groups in the community [
21].
Figure 2 illustrates the basic concept of the MHE. The key components are explained below.
2.1. Utilization of Local Human Resources
Local human resources are the primary component of MHE. Their role is to operate the business in the community to provide primary healthcare services. There are two kinds of human resources:
Existing Health-Related Business Person: Pharmacies and village doctors are influential figures in providing community-level primary healthcare services. According to the Directorate General of Drug Administration (DGDA) in Bangladesh, there are 172,282 retail allopathic, Unani, Ayurvedic, and homeopathic and biochemical pharmacies [
22]. Surprisingly, 60% of the population (as of 2022), primarily residing in rural areas, consider the pharmacy their first point of medical consultation. Urban dwellers also prefer pharmacies as their initial point of contact. In a study of 302 customers from 76 pharmacies, Chowdhury et al. found that 90% of customers seek services from the pharmacy as their first point of care, citing reasons such as “Ease of access to pharmacies (86%)”, “Lower cost (46%)”, “Availability of medicine (33%)”, “Knowing the medicine seller (20%)”, and “Convenient hours of operation (19%)” [
23]. According to Mahmood et al., in a study conducted in rural areas of Bangladesh covering 7600 households, 67% of patients depended on village doctors as their first point of contact for healthcare services [
24]. These pharmacy owners and village doctors play multiple roles—acting as consultants, medicine sellers, and operators. They can be trained to become Mobile Health Entrepreneurs (MHEs). Additionally, individuals already involved in healthcare businesses or those interested in healthcare services and willing to take on the challenge of becoming healthcare entrepreneurs can also assume this role. Their responsibilities include assigning certified health workers, providing healthcare services to the community, and maintaining relationships with funding organizations, technology providers, and doctors.
Certified Health Worker: Identifying certified health workers involves checking the respective country’s government requirements, which can vary in duration, ranging from six months or more. The role of a health worker will be to perform health screening, connect online doctors, and print and explain prescriptions to patients.
2.2. Disruptive Healthcare Technology
The MHE concept utilizes advanced digital health technologies, emphasizing portable medical devices or IoMT (Internet of Medical Things), a patient-friendly telemedicine system, and a standard electronic health record system.
Portable, Affordable, and Usable Devices: Recently, medical and communication devices have started becoming portable, accurate, and affordable. These devices enable quick diagnosis, simple maintenance, and seamless data retrieval from digital systems. For instance, the Portable Health Clinic [
25] is equipped with medical sensors for primary health screenings, capturing around 14 vital signs. These devices must be government-certified and undergo quality measurement testing [
26]. Devices from several Asian and African countries were collected and tested at Kyushu University Hospital. Devices that passed our laboratory test are included in our list of recommended devices.
Patient-friendly Telemedicine System: Patients in rural areas often face challenges accessing healthcare due to a shortage of local healthcare professionals. To address this issue, the proposed model connects patients with doctors registered as telemedicine practitioners in the system. Telemedicine can significantly improve healthcare provision in remote areas for both emergency and non-emergency care [
27]. Utilizing telemedicine technology, these doctors can remotely review patients’ medical histories and reports and engage in real-time discussions with them via video and audio systems. Following the consultation, the doctor can promptly issue an online prescription and provide detailed explanations to the patient. The prescription is then printed by the Micro Healthcare Entrepreneurship (MHE) initiative and explained in the local language to ensure clarity and understanding.
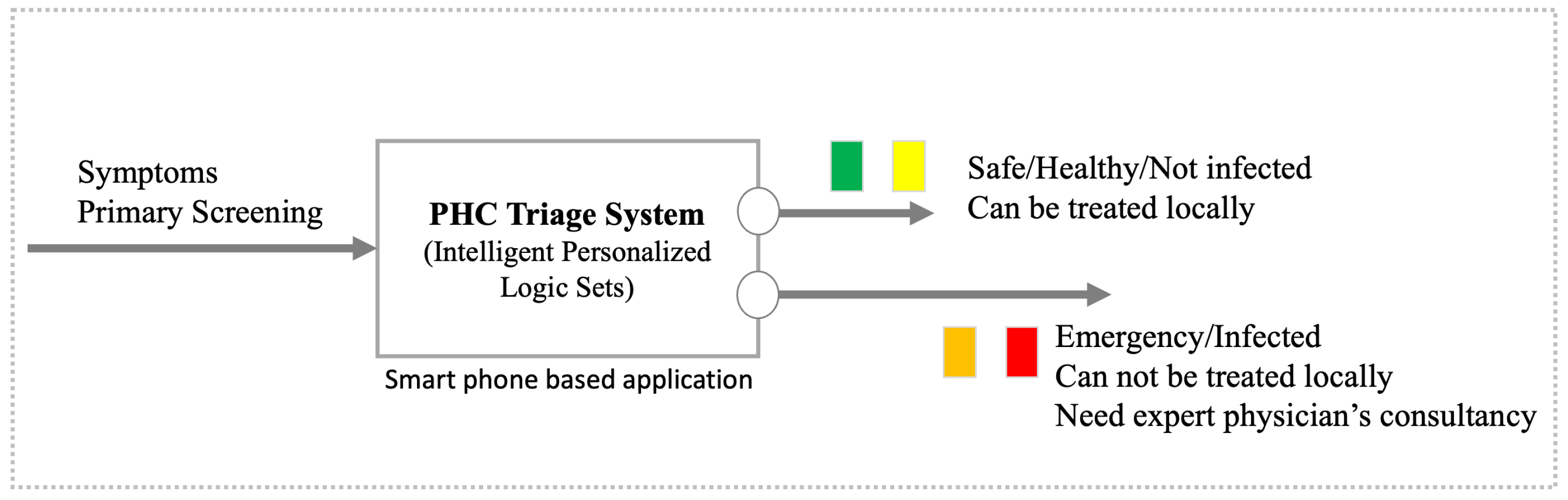
Concept of Triage: A triage logic has been developed to categorize patients according to their health status. Patients are classified into four categories: green (healthy), yellow (cautious), orange (affected), and red (risky). Only patients marked as orange or red require consultation with a doctor, while those in the green and yellow categories can be attended to by local healthcare workers. This approach helps alleviate the burden on telemedicine doctors, ensuring that their expertise is utilized where it is most needed.
Electronic Health Records: A patient’s electronic health records (EHRs) will be securely managed in the cloud, enabling secure and efficient access by authorized healthcare professionals. Our lab has developed several innovative technologies to detect and prevent medical errors, as well as to suggest potential non-communicable disease (NCD) risks for proactive patient care. This comprehensive approach can save time, reduce costs, minimize medical errors, and significantly enhance the productivity and quality of healthcare delivery [
28]. Without strong internet access, rural residents face significant barriers to access to quality healthcare services.
2.3. Continuous Training
The rapid evolution of information and communication technology (ICT), consumer behavior, and the demand for digital services necessitates continuous training on technological updates, relevant technologies, and entrepreneurial knowledge to ensure the sustainability of MHE.
Tools and Software Training: Due to frequent software updates (at least annually) and device refreshes (approximately every three years), continuous training for staff is crucial. Online training can be an efficient and cost-effective solution to address these ongoing learning needs.
Entrepreneurship Training: Entrepreneurial orientation (EO) has been shown to have a significant positive influence on social innovativeness [
29]. Entrepreneurship training is included as another sub-component of the MHE model, equipping individuals with the skills and knowledge to navigate the nuances of healthcare entrepreneurship. Recognizing the sensitivity of the healthcare field, this training incorporates real-world experiences from operating businesses in rural areas and integrates patient feedback to ensure its relevance and effectiveness.
2.4. Available Funds
Entrepreneurs can use a social business fund or other startup funds to establish and run the business smoothly.
Social Business Fund: Social business is a new term coined by Professor Muhammad Yunus, the founder of Grameen Bank and a 2006 Nobel Laureate. It is dedicated to supporting startup or existing entrepreneurs with interest-free, collateral-free, dividend-free, and stock-free funds. Entrepreneurs are required to repay the actual investment after a specified period with the 20% share transfer fee. This is to cover the cost associated with the services provided by the investor and make it easy for Nobin Udyokta (Young Entrepreneur), NU, to buy the shares at face value [
30]. The program has already provided social business funds to 150,000 entrepreneurs (as of September 2023) in Bangladesh. Social business funds were also created in other Asian and African countries, including Yemen and Kosovo.
Other Funds: Other than the social business fund, entrepreneurs can also manage funds from other sources, such as bank loans, personal loans, venture capital, grants, etc. Each funding source has different characteristics. It should be determined which one will be easier to obtain, has flexible conditions, and poses less risk to the entrepreneurs.
These components represent the foundational elements of the MHE model. However, it is important to acknowledge that these components may evolve in the future due to changing service needs, technological advancements, or other requirements. For instance, the integration of innovative solutions such as digital twins and blockchain has the potential to revolutionize the operations of MHEs. Digital twin technology enables MHEs to generate virtual replicas of medical assets, facilitating optimal resource allocation and enhancing service delivery. Similarly, blockchain technology can revolutionize data management within MHEs, ensuring the secure and transparent handling of patient information while streamlining administrative processes. Embracing these advancements holds promise for significantly enhancing the efficiency and effectiveness of MHEs in delivering healthcare services to underserved communities in developing countries.
3. Methods and Results
To validate the four major components of the MHE model, experiments, training sessions, and workshops were conducted in diverse resource settings. This allowed for testing the model’s efficacy in various real-world contexts.
3.1. Experiment to Validate Technology
The Portable Health Clinic system was tested in 32 different locations in Bangladesh by trained healthcare workers.
Figure 3 illustrates the triage concept, which classifies patients into four different categories for NCDs, demonstrated during a random checkup.
Table 4 presents the PHC screening data in Bangladesh, revealing that 61% of people are diagnosed as healthy, while the remaining 39% are unhealthy and do not require consultations with doctors. This helps reduce costs for patients and alleviates the cognitive load of doctors by reducing the number of consultations.
3.2. Training and Workshops to Check the Acceptability of MHE Concept
Local human resources targeted as potential entrepreneurs were invited to workshops in three phases to introduce the concept, outline their roles, and obtain their feedback after training. All three workshops were held on Grameen premises, Dhaka, Bangladesh, from July 2022 to January 2023, each lasting for two full days. The workshops covered various modules, including hands-on training with the Portable Health Clinic digital health system and an introduction to the MHE concept. Fundamental entrepreneurial sessions were also delivered to prepare participants for health entrepreneurship. The workshop design, methodology, and content remained consistent across all three sessions.
The target group comprised community-based health service providers and individuals aspiring to work as Micro Healthcare Entrepreneurs in the community health sector in Bangladesh. Participants from different regions of Bangladesh attended the in-person workshops. Across the three workshops, a total of 60 participants were selected from 1087 applicants. The selection process involved two screening stages to assess eligibility criteria, including age, gender, location, availability to attend the workshop, healthcare certification or involvement, business engagement, and entrepreneurial interest, among other considerations.
Both qualitative and quantitative methods were employed to obtain feedback from workshop attendees. Qualitative surveys included online interviews, open-ended survey questions, and focus group discussions. Content analysis was utilized for the data analysis of qualitative surveys. Quantitative surveys included closed-ended questions such as multiple choice, yes/no, and rating scales. Descriptive statistics were used for the data analysis of quantitative surveys.
To evaluate the implementation prospects and challenges of the MHE concept, responses were collected from 60 individuals engaged in community-based health services in various rural and urban locations in Bangladesh. Responses were collected through the organization of three workshops in different phases. Following the workshops, an online survey form with several questions was utilized to gather their feedback, and the key questions and answers are detailed in
Table 5.
3.3. A Comparison of Funding Sources to Make MHE a Sustainable Enterprise
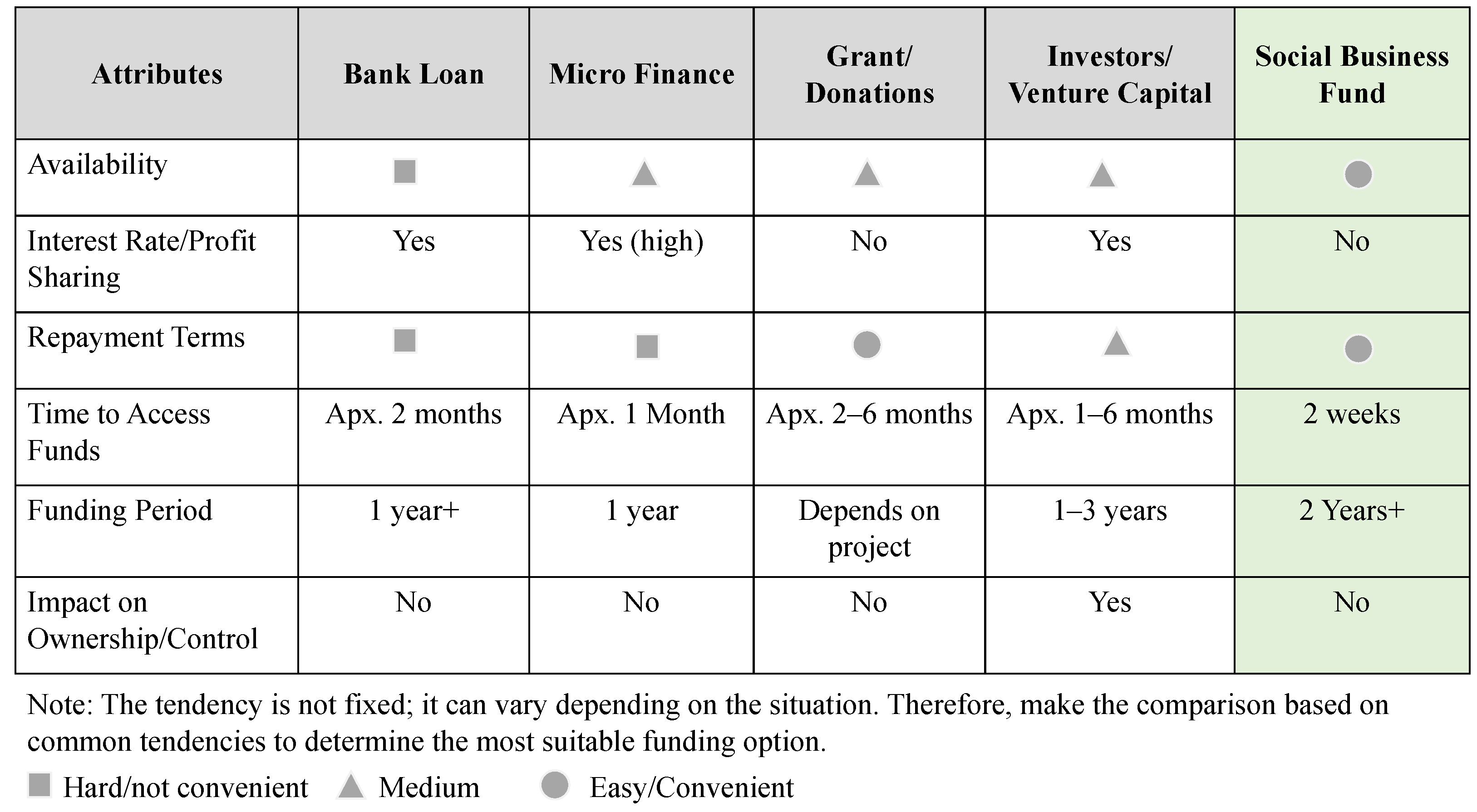
As MHE is a business aimed at sustainability and ensuring low-cost services, the investment funds in MHE should meet certain criteria to make entrepreneurs feel that their funding sources are flexible, less risky, and do not create excessive financial burdens. During the workshop, participants were asked about their preferred funding sources as startup capital. In their feedback during open group discussions, they mentioned specific attributes, which are listed in
Figure 4. Using these attributes, a comparative analysis was conducted between the social business fund and other available funding sources in their community. The features of all funding sources were collected through an analysis of the available literature and the service packages of those organizations. It appears that the social business fund is more suitable than other funding sources. If the financial burden is reduced, then the capital cost is lower, and the flexible conditions to get funded for expansions of their business can help them make it a sustainable enterprise.
3.4. Prospects and Challenges
This section explains the prospects and challenges of MHE, considering feedback from community-level health service providers during their participation in workshops.
3.4.1. Prospects
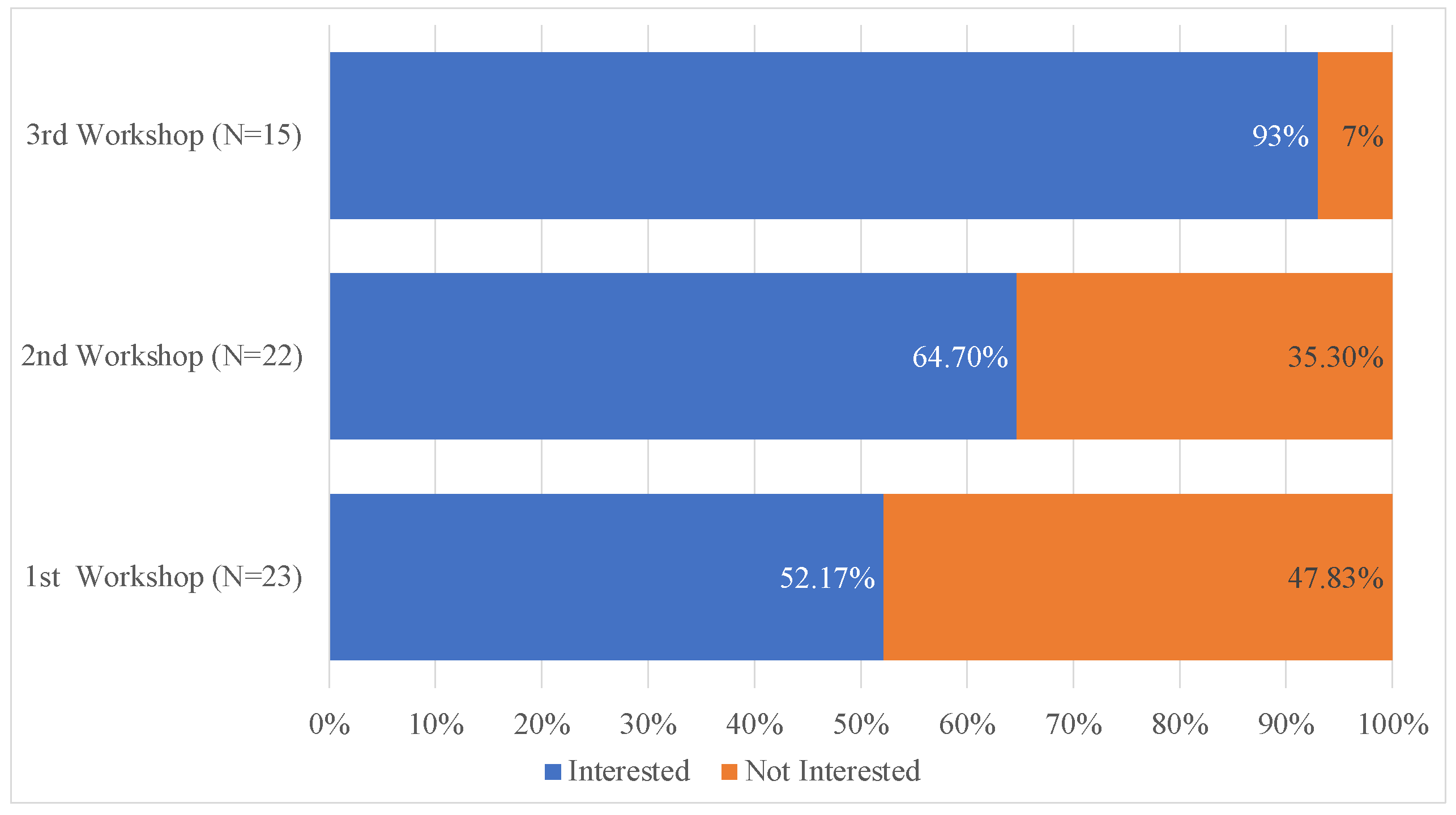
To comprehend the prospects of MHE, following the explanation of its concept and components, efforts were made to gauge the level of interest among community health service providers through workshops, as stated in
Figure 5. The figure indicates that in the first workshop, 52.17% showed interest; in the second workshop, it increased to 64.70%; and in the third workshop, interest in engaging in MHE surged to 93%. The first workshop was open to all, including students and potential business persons in both rural and urban areas. The second and third workshops were redesigned based on feedback from the first workshop. Rural pharmacy owners were given priority in the third workshop.
Table 5 demonstrates that the target group favored the MHE concept due to its utilization of digital health technology, affordability, and ease of operation. Community health workers expressed interest in implementing this concept at the community level, but they also expect continuous support in business development and sustainability, funding for business expansions, and a reduction in the price of digital health systems. Regarding startup funding, although they have the opportunity to access social business funds and other funding sources, they are prepared to provide approximately 30-50% of the total initial investment themselves.
3.4.2. Challenges
To understand the challenges for the future implementation of MHE, workshop participants were surveyed, revealing several obstacles that could be addressed during implementation:
(a) Quality Issues with Portable Medical Devices: Digital health systems like portable medical devices are key components of MHE. Various devices available in the market are currently utilized by service providers in Bangladesh’s digital health practice. However, concerns persist regarding the quality of these devices. To address these challenges, all available devices in the Bangladeshi market were tested in the lab at Kyushu University Hospital in Japan, and only devices passing these tests are approved for use within the integrated Portable Health Clinic system of the MHE concept [
26].
(b) Data Collection Challenges: Concerns were expressed regarding data collection. Usually, in Bangladesh, patients fail to maintain records of their medical history, most of them relying solely on paper-based documents, while others directly consult with doctors without documentation. This poses a challenge in collecting comprehensive medical histories. Furthermore, in remote areas with weak or no internet connectivity, the data collection process can face obstacles. In the MHE concept, emphasis is placed on adopting technology like the Smart Health Gantt Chart (SHGC) system. This system can collect, store, and analyze various forms of data—paper-based, audio conversations, digital records, etc. Additionally, healthcare workers can capture photos of previous documents and upload them to the system later when internet connectivity is available.
(c) Data Privacy and Security: Concerns about data privacy and security were shared by the workshop attendees, who worried about potential liabilities. To address this, the MHE proposes a collaboration with a registered digital health company in each specific country. This company would possess the necessary permissions and arrangements for data security and privacy. MHE entrepreneurs would operate under a partnership with this registered company, alleviating their liability concerns. The primary digital health service provider will ensure compliance with local and international regulations governing data privacy and security.
(d) Collaboration with Stakeholders: In Bangladesh’s rural healthcare landscape, village doctors, pharmacies, and smaller clinics play crucial roles. Recognizing their influence, the MHE initiative focuses on integrating these stakeholders, particularly pharmacists and village doctors, into its framework. This formalized integration aims to minimize potential disruptions and leverage existing trust within the community. Additionally, MHE collaborates with government and NGO clinics, offering support and addressing their lack of digital tools and patient data management capabilities. This partnership creates a win–win situation, allowing MHEs to contribute while benefiting from the established infrastructure of these clinics. Finally, MHE complements larger private hospitals by focusing on primary care while seamlessly referring complex cases for specialized treatment, fostering a collaborative and comprehensive healthcare ecosystem.
(e) Cost of Digital Health System: Participants expressed concerns about the expenses involved in acquiring and implementing the digital health system. However, scaling up the implementation could potentially reduce costs.
(f) Rapid Changes in Technology: Participants highlighted the challenge of keeping up with fast-paced technological advancements. Continuous research, development, and collaboration with digital health companies like Portable Health Clinic could address this issue.
(g) Lack of Public Awareness: Participants expressed concerns about the lack of public awareness regarding the importance of primary healthcare services. Regular community education events are essential to addressing this issue.
(h) Government Policy Issues: Participants highlighted challenges related to government policies, emphasizing the need for clear and supportive policies. The government’s efforts to adopt digital health policies and create an ecosystem for digital health entrepreneurs are promising. Collaborative work with the government and adherence to designed business models aligned with policies could enhance safety and effectiveness.
4. Discussion
The proposed MHE model focuses on community resources with the integration of digital health. Existing service delivery approaches, including government health service providers, suffer from both a shortage of human resources for health and an inequitable distribution of human resources [
31]. Private services are expensive and sometimes add unnecessary costs, while also being urban-focused [
14,
32]. NGO-led development initiatives are not sustainable [
33].
By examining previous successes in digital health systems, such as the Portable Health Clinic system and its pilot projects in ten developing countries, serving over 50,000 people, it can be seen that a digital health system has the potential to address healthcare accessibility and contribute to the progress of Universal Health Coverage (UHC) within low-resource settings In MHE, pressure on human resources is reduced by triaging patients at the root. Service fees are affordable and accessible to all types of communities, which helps overcome the limitations of private care. MHE is a self-dependent business model, so it is not like an NGO and does not depend on funding. The components of MHE, such as digital health and social business funds, have been utilized in many cases, with success proven in various research studies [
34]. This is also explained in the Methods and Results Section. This study also focused on understanding the prospects and challenges of the MHE model based on the feedback of local human resources.
Table 3 shows the existing challenges of UHC in South Asian countries and Bangladesh and also provides a comparison of existing service delivery approaches.
4.1. Potential Impact of MHE on UHC
(a) Reducing Out-of-Pocket Expenditures: Bangladesh faces a substantial burden of out-of-pocket healthcare expenses, accounting for 72.99% (2021) [
35]. MHE can help reduce these costs by implementing primary health screenings, early disease detection, and preventive care, ultimately lowering out-of-pocket expenses. While several health insurance organizations offer packages for corporate executive employees, rural individuals often lack coverage. Grameen Kalyan provides health insurance services with a focus on Grameen Bank members.
(b) Overcoming the Shortage of Human Resources for Health (HRH): The country grapples with a significant shortage of healthcare resources, including doctors, nurses, and other medical staff. Utilizing digital triage software within the Portable Health Clinic digital health system has shown a remarkable 69% reduction in doctors’ time, enabling better resource allocation and increased access to healthcare services [
36].
(c) Collaboration with Existing Stakeholders: Inefficiencies in functional resources, particularly the underutilization of community clinics, pose a significant challenge. Collaborating between MHEs and government-run community clinics can substantially enhance their functionality, optimizing healthcare service delivery across Bangladesh.
(d) Establishment of an Interoperable Health Information System: The effectiveness of healthcare is hindered by the absence or inefficiency of individual health data management systems. MHE’s involvement in managing individual health data, collaborating in electronic health record (EHR) systems, and providing a summarized view of life-long medical history through visualization can efficiently address this issue.
(e) Efficient Utilization of Resources: The disproportionate distribution of healthcare professionals between rural and urban areas highlights the need for improved access to quality healthcare. Leveraging digital health solutions and community-based entrepreneurship under MHE initiatives aims to bridge this gap, ensuring equitable healthcare access across diverse regions.
(f) Increasing Awareness of Primary Healthcare: The absence of compulsory health checkups contributes to a lack of awareness about preventive healthcare. One of the major objectives of MHEs is to establish healthcare services in academia, industries, and other community groups, promoting regular annual health checkups to raise awareness and prioritize preventive care measures.
4.2. Limitations
The proposed Micro Health Entrepreneurship (MHE) model is a conceptual framework inspired by the established Grameen model. While each of the four components of the model has been tested separately, the complete implementation of the entire model is still pending. Nonetheless, to better grasp the potential and challenges associated with implementation, the concept was introduced to community health service providers, who serve as the primary drivers for field-level implementation.
The challenges highlighted by local community healthcare providers, particularly about government policy issues, remain a forward-looking task. The potential impacts are listed, but they have not been measured yet.
5. Conclusions
Developing countries are currently facing significant challenges in achieving Universal Health Coverage (UHC) by 2030 using existing resources and approaches. This study proposes a bottom-up approach called Micro Healthcare Entrepreneurship (MHE) as a promising concept to advance UHC. The components of the MHE model are described and have been individually tested in various settings in Bangladesh, demonstrating their effectiveness.
To assess the integrated performance of the model, feedback was collected from local healthcare providers through in-person workshops. During these workshops, the MHE concept was explained, and primary health screening services were demonstrated. Participants’ willingness to engage in MHE was measured, and the challenges they identified were documented. While most expressed interest in MHE involvement, they also noted significant challenges, albeit manageable ones.
Future research could focus on implementing the model at the field level and evaluating its impact, with adjustments made as necessary. It is anticipated that the MHE concept will play a crucial role in improving healthcare accessibility and affordability, thereby contributing to the achievement of Universal Health Coverage in developing countries.


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}