Trimethylamine-N-oxide (TMAO) as Novel Potential Biomarker of Early Predictors of Metabolic Syndrome

 ,
,  ,
,  ,
,  ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
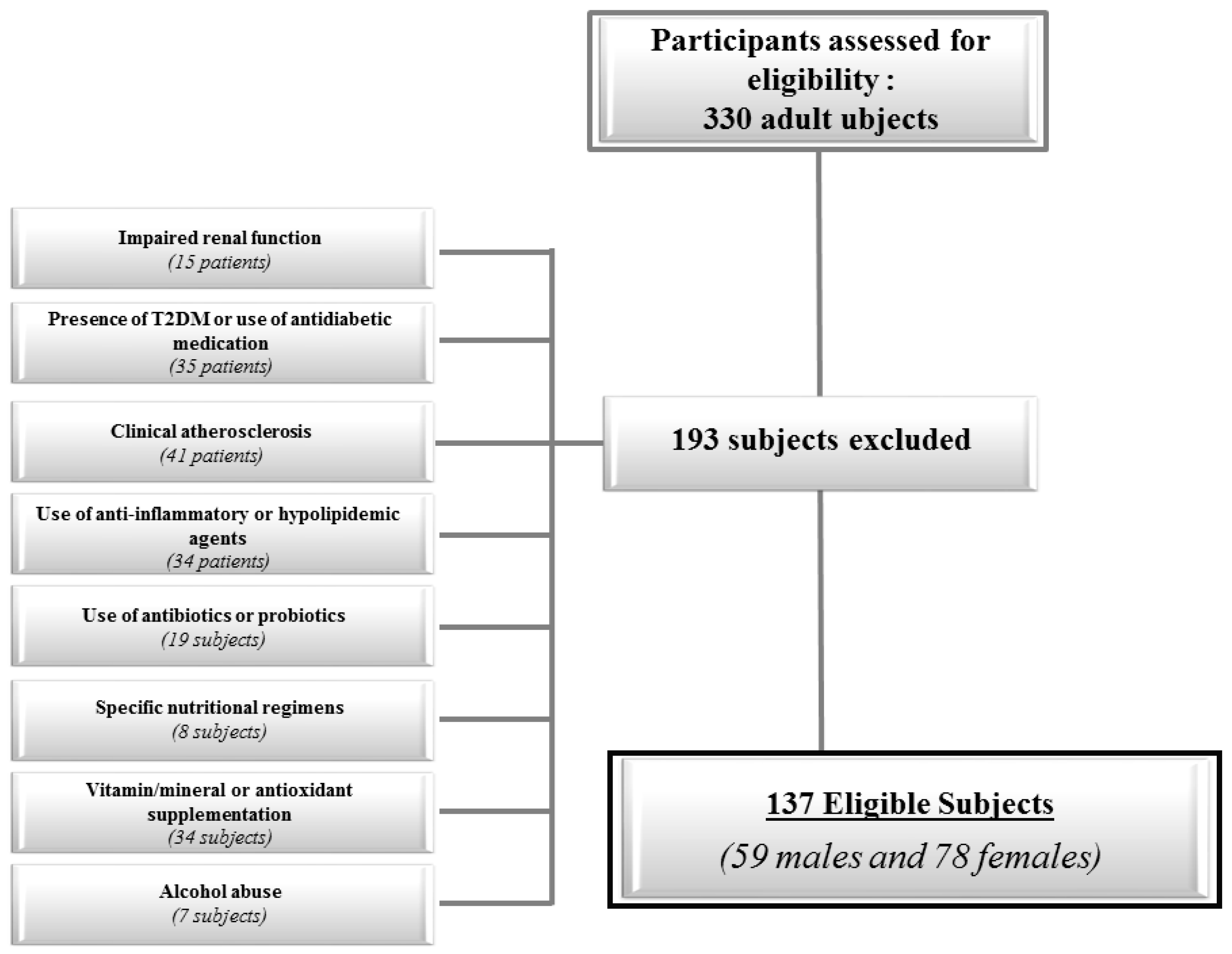
2.2. Population Study
- Impaired renal function (normal values: estimated glomerular filtration rate ≥ 90 mL/min/1.73 m2 calculated by chronic kidney disease epidemiology collaboration equation; CKD EPI) (15 patients)
- Presence of T2DM (defined by criteria of the American Diabetes Association as follows: basal plasma glucose level ≥ 126 mg/dL on two occasions, or glycated hemoglobin (HbA1c) ≥ 6.5% (≥48 mmol/mol) on two occasions, or both at the same time (35 patients). Participants on antidiabetic medication were considered to have T2DM [26].
- Clinical atherosclerosis (coronary artery disease, peripheral vascular disease, CVD) (41 patients)
- Current therapy with anti-inflammatory drugs, statins and other hypolipidemic agents (34 patients);
- User of antibiotics or probiotics within 2 months of recruitment (19 subjects);
- Specific nutritional regimens, including vegan or vegetarian diets (eight subjects);
- Vitamin/mineral or antioxidant supplementation (34 subjects);
- Alcohol abuse according to the Diagnostic and Statistical Manual of Mental Disorders (DSM)-V diagnostic criteria (eleven subjects);
2.3. Lifestyle Habits
2.4. Anthropometric Measurements and Blood Pressure
2.5. Determination of Circulating Levels of TMAO
2.6. Assay Methods
2.7. Cardio-Metabolic Indices
2.8. Criteria to Define MetS
2.9. Dietary Assessment
2.10. Statistical Analysis
3. Results
Correlation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| TMAO | Trimethylamine-N-oxide |
| TMA | Trimethylamine |
| FMO3 | Flavin-monooxygenase-3 |
| T2DM | Type 2 Diabetes Mellitus |
| CVD | Cardiovascular diseases |
| MetS | Metabolic Syndrome |
| HDL | High-density Lipoprotein |
| HoMA-IR | Homeostatic Model Assessment of Insulin Resistance |
| BMI | body mass index |
| VAI | Visceral Adiposity Index |
| FLI | Fatty Liver Index |
| NAFLD | Non-alcoholic Fatty Liver Disease |
| WC | Waist Circumference |
| TG | Triglycerides |
| SBP | Systolic Blood Pressure |
| DBP | Diastolic Blood Pressure |
| ALT | Alanine Transaminase |
| AST | Aspartate Aminotransferase |
| γGT | γ-Glutamyltransferase |
| LDL | Low-Density Lipoprotein |
| SD | Standard Deviation |
| OR | Odds Ratio |
| IC | Interval Confidence |
| ROC | Receiver Operator Characteristic |
| AUC | Area Under Curve. |
References
- Wang, Z.; Klipfel, E.; Bennett, B.J.; Koeth, R.; Levison, B.S.; Dugar, B.; Feldstein, A.E.; Britt, E.B.; Fu, X.; Chung, Y.M.; et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 2011, 472, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiattarella, G.G.; Sannino, A.; Toscano, E.; Giugliano, G.; Gargiulo, G.; Franzone, A.; Trimarco, B.; Esposito, G.; Perrino, C. Gut microbe-generated metabolite trimethylamine-N-oxide as cardiovascular risk biomarker: A systematic review and dose-response meta-analysis. Eur. Heart J. 2017, 38, 2948–2956. [Google Scholar] [CrossRef] [PubMed]
- Kanitsoraphan, C.; Rattanawong, P.; Charoensri, S.; Senthong, V. Trimethylamine N-Oxide and Risk of Cardiovascular Disease and Mortality. Curr. Nutr. Rep. 2018. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Annunziata, G.; Muscogiuri, G.; Ludisio, D.; Di Somma, C.; Maisto, M.; Tenore, G.C.; Colao, A.; Savastano, S. Trimethylamine N-oxide (TMAO), Mediterranean Diet and Nutrition in Healthy, Normal-weight Subjects: Is It Also A Matter Of Gender? Nutrition 2018, in press. [Google Scholar] [CrossRef]
- Zeisel, S.H.; Wishnok, J.S.; Blusztajn, J.K. Formation of methylamines from ingested choline and lecithin. J. Pharmacol. Exp. Ther. 1983, 225, 320–324. [Google Scholar]
- Koeth, R.A.; Wang, Z.; Levison, B.S.; Buffa, J.A.; Org, E.; Sheehy, B.T.; Britt, E.B.; Fu, X.; Wu, Y.; Li, L.; et al. Intestinal microbiota metabolism of L-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat. Med. 2013, 19, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.H.; Hazen, S.L. The contributory role of gut microbiota in cardiovascular disease. J. Clin. Investig. 2014, 124, 4204–4211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ufnal, M.; Zadlo, A.; Ostaszewski, R. TMAO: A small molecule of great expectations. Nutrition 2015, 31, 1317–1323. [Google Scholar] [CrossRef] [PubMed]
- Lent-Schochet, D.; Silva, R.; McLaughlin, M.; Huet, B.; Jialal, I. Changes to trimethylamine-N-oxide and its precursors in nascent metabolic syndrome. Horm. Mol. Biol. Clin. Investig. 2018, 35. [Google Scholar] [CrossRef]
- Zhu, W.; Gregory, J.C.; Org, E.; Buffa, J.A.; Gupta, N.; Wang, Z.; Li, L.; Fu, X.; Wu, Y.; Mehrabian, M.; et al. Gut Microbial Metabolite TMAO Enhances Platelet Hyperreactivity and Thrombosis Risk. Cell 2016, 165, 111–124. [Google Scholar] [CrossRef]
- Schugar, R.C.; Shih, D.M.; Warrier, M.; Helsley, R.N.; Burrows, A.; Ferguson, D.; Brown, A.L.; Gromovsky, A.D.; Heine, M.; Chatterjee, A.; et al. The TMAO-Producing Enzyme Flavin-Containing Monooxygenase 3 Regulates Obesity and the Beiging of White Adipose Tissue. Cell Rep. 2017, 19, 2451–2461. [Google Scholar] [CrossRef] [PubMed]
- Randrianarisoa, E.; Lehn-Stefan, A.; Wang, X.; Hoene, M.; Peter, A.; Heinzmann, S.S.; Zhao, X.; Königsrainer, I.; Königsrainer, A.; Balletshofer, B.; et al. Relationship of Serum Trimethylamine N-Oxide (TMAO) Levels with early Atherosclerosis in Humans. Sci. Rep. 2016, 6, 26745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.M.; Liu, Y.; Zhou, R.F.; Chen, X.L.; Wang, C.; Tan, X.Y.; Wang, L.J.; Zheng, R.D.; Zhang, H.W.; Ling, W.H.; et al. Associations of gut-flora-dependent metabolite trimethylamine-N-oxide, betaine and choline with non-alcoholic fatty liver disease in adults. Sci. Rep. 2016, 6, 19076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchesini, G.; Brizi, M.; Bianchi, G.; Tomassetti, S.; Bugianesi, E.; Lenzi, M.; McCullough, A.J.; Natale, S.; Forlani, G.; Melchionda, N. Nonalcoholic fatty liver disease: A feature of the metabolic syndrome. Diabetes 2001, 50, 1844–1850. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. National Heart, Lung, and Blood Institute. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo, C.; Williams, K.; Hunt, K.J.; Haffner, S.M. The National Cholesterol Education Program–Adult Treatment Panel III, International Diabetes Federation, and World Health Organization definitions of the metabolic syndrome as predictors of incident cardiovascular disease and diabetes. Diabetes Care 2007, 30, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Jialal, I.; Devaraj, S.; Adams-Huet, B.; Chen, X.; Kaur, H. Increased cellular and circulating biomarkers of oxidative stress in nascent metabolic syndrome. J. Clin. Endocrinol. Metab. 2012, 97, E1844–E1850. [Google Scholar] [CrossRef]
- Ntzouvani, A.; Nomikos, T.; Panagiotakos, D.; Fragopoulou, E.; Pitsavos, C.; McCann, A.; Ueland, P.M.; Antonopoulou, S. Amino acid profile and metabolic syndrome in a male Mediterranean population: A cross-sectional study. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 1021–1030. [Google Scholar] [CrossRef]
- Mueller, D.M.; Allenspach, M.; Othman, A.; Saely, C.H.; Muendlein, A.; Vonbank, A.; Drexel, H.; von Eckardstein, A. Plasma levels of trimethylamine-N-oxide are confounded by impaired kidney function and poor metabolic control. Atherosclerosis 2015, 243, 638–644. [Google Scholar] [CrossRef]
- Amato, M.C.; Giordano, C.; Galia, M.; Criscimanna, A.; Vitabile, S.; Midiri, M.; Galluzzo, A.; AlkaMeSy Study Group. Visceral Adiposity Index: A reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care 2010, 33, 920–922. [Google Scholar] [CrossRef] [Green Version]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.C.; Giordano, C. Visceral adiposity index: An indicator of adipose tissue dysfunction. Int. J. Endocrinol. 2014, 2014, 730827. [Google Scholar] [CrossRef] [PubMed]
- Klisic, A.; Isakovic, A.; Kocic, G.; Kavaric, N.; Jovanovic, M.; Zvrko, E.; Skerovic, V.; Ninic, A. Relationship between Oxidative Stress, Inflammation and Dyslipidemia with Fatty Liver Index in Patients with Type 2 Diabetes Mellitus. Exp. Clin. Endocrinol. Diabetes 2018, 126, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Rogulj, D.; Konjevoda, P.; Milić, M.; Mladinić, M.; Domijan, A.M. Fatty liver index as an indicator of metabolic syndrome. Clin. Biochem. 2012, 45, 68–71. [Google Scholar] [CrossRef] [PubMed]
- Yadav, D.; Choi, E.; Ahn, S.V.; Koh, S.B.; Sung, K.C.; Kim, J.Y.; Huh, J.H. Fatty liver index as a simple predictor of incident diabetes from the KoGES-ARIRANG study. Medicine 2016, 95, E4447. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Standards of Medical Care in Diabetes-2017: Summary of Revisions. Diabetes Care 2017, 40, S4–S5. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Waist Circumference and Waist-Hip Ratio. Report of WHO Expert Consultation, Geneva. 8–11 December 2008. Available online: http://apps.who.int/iris/bitstream/10665/44583/1/9789241501491_eng.pdf (accessed on 10 November 2018).
- National Center for Health Statistics. Anthropometry Procedures Manual—National Health and Nutrition Examination Survey (NHANES). Available online: http://www.cdc.gov/nchs/data/nhanes/nhanes_11_12/Anthropometry_Procedures_Manual.pdf (accessed on 10 November 2018).
- Wang, Z.; Levison, B.S.; Hazen, J.E.; Donahue, L.; Li, X.M.; Hazen, S.L. Measurement of trimethylamine-N-oxide by stable isotope dilution liquid chromatography tandem mass spectrometry. Anal. Biochem. 2014, 455, 35–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beale, R.; Airs, R. Quantification of glycine betaine, choline and trimethylamine N-oxide in seawater particulates: Minimisation of seawater associated ion suppression. Anal. Chim. Acta. 2016, 938, 114–122. [Google Scholar] [CrossRef] [Green Version]
- Yu, W.; Xu, C.; Li, G.; Hong, W.; Zhou, Z.; Xiao, C.; Zhao, Y.; Cai, Y.; Huang, M.; Jin, J. Simultaneous determination of trimethylamine N-oxide, choline, betaine by UPLC-MS/MS in human plasma: An application in acute stroke patients. J. Pharm. Biomed. Anal. 2018, 152, 179–187. [Google Scholar] [CrossRef]
- Savastano, S.; Barbato, A.; Di Somma, C.; Guida, B.; Pizza, G.; Barrea, L.; Avallone, S.; Schiano di Cola, M.; Strazzullo, P.; Colao, A. Beyond waist circumference in an adult male population of Southern Italy: Is there any role for subscapular skinfold thickness in the relationship between insulin-like growth factor-I system and metabolic parameters? J. Endocrinol. Investig. 2012, 35, 925–929. [Google Scholar] [CrossRef]
- Savastano, S.; Di Somma, C.; Colao, A.; Barrea, L.; Orio, F.; Finelli, C.; Pasanisi, F.; Contaldo, F.; Tarantino, G. Preliminary data on the relationship between circulating levels of Sirtuin 4, anthropometric and metabolic parameters in obese subjects according to growth hormone/insulin-like growth factor-1 status. Growth Horm. IGF Res. 2015, 25, 28–33. [Google Scholar] [CrossRef] [Green Version]
- Barrea, L.; Tarantino, G.; Di Somma, C.; Muscogiuri, G.; Macchia, P.E.; Falco, A.; Colao, A.; Savastano, S. Adherence to the Mediterranean Diet and Circulating Levels of Sirtuin 4 in Obese Patients: A Novel Association. Oxid. Med. Cell Longev. 2017, 2017, 6101254. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Di Somma, C.; Macchia, P.E.; Falco, A.; Savanelli, M.C.; Orio, F.; Colao, A.; Savastano, S. Influence of nutrition on somatotropic axis: Milk consumption in adult individuals with moderate-severe obesity. Clin. Nutr. 2017, 36, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Macchia, P.E.; Tarantino, G.; Di Somma, C.; Pane, E.; Balato, N.; Napolitano, M.; Colao, A.; Savastano, S. Nutrition: A key environmental dietary factor in clinical severity and cardio-metabolic risk in psoriatic male patients evaluated by 7-day food-frequency questionnaire. J. Transl. Med. 2015, 13, 303. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Amato, M.C.; Giordano, C.; Pitrone, M.; Galluzzo, A. Cut-off points of the visceral adiposity index (VAI) identifying a visceral adipose dysfunction associated with cardiometabolic risk in a Caucasian Sicilian population. Lipids Health Dis. 2011, 10, 183. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]
- Barrea, L.; Muscogiuri, G.; Di Somma, C.; Annunziata, G.; Megna, M.; Falco, A.; Balato, A.; Colao, A.; Savastano, S. Coffee consumption, metabolic syndrome and clinical severity of psoriasis: Good or bad stuff? Arch. Toxicol. 2018, 92, 1831–1845. [Google Scholar] [CrossRef]
- Turconi, G.; Guarcello, M.; Berzolari, F.G.; Carolei, A.; Bazzano, R.; Roggi, C. An evaluation of a colour food photography atlas as a tool for quantifying food portion size in epidemiological dietary surveys. Eur. J. Clin. Nutr. 2005, 59, 923–931. [Google Scholar] [CrossRef] [Green Version]
- Lentjes, M.A.; McTaggart, A.; Mulligan, A.A.; Powell, N.A.; Parry-Smith, D.; Luben, R.N.; Bhaniani, A.; Welch, A.A.; Khaw, K.T. Dietary intake measurement using 7 d diet diaries in British men and women in the European Prospective Investigation into Cancer-Norfolk study: A focus on methodological issues. Br. J. Nutr. 2014, 111, 516–526. [Google Scholar] [CrossRef]
- Yang, K.C.; Hung, H.F.; Lu, C.W.; Chang, H.H.; Lee, L.T.; Huang, K.C. Association of Non-alcoholic Fatty Liver Disease with Metabolic Syndrome Independently of Central Obesity and Insulin Resistance. Sci. Rep. 2016, 6, 27034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumas, M.E.; Barton, R.H.; Toye, A.; Cloarec, O.; Blancher, C.; Rothwell, A.; Fearnside, J.; Tatoud, R.; Blanc, V.; Lindon, J.C.; et al. Metabolic profiling reveals a contribution of gut microbiota to fatty liver phenotype in insulin-resistant mice. Proc. Natl. Acad. Sci. USA 2006, 103, 12511–12516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miao, J.; Ling, A.V.; Manthena, P.V.; Gearing, M.E.; Graham, M.J.; Crooke, R.M.; Croce, K.J.; Esquejo, R.M.; Clish, C.B.; Torrecilla, E.; et al. Flavin-containing monooxygenase 3 as a potential player in diabetes-associated atherosclerosis. Nat. Commun. 2015, 6, 6498. [Google Scholar] [CrossRef] [Green Version]
- Gao, X.; Liu, X.; Xu, J.; Xue, C.; Xue, Y.; Wang, Y. Dietary trimethylamine N-oxide exacerbates impaired glucose tolerance in mice fed a high fat diet. J. Biosci. Bioeng. 2014, 118, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Noga, A.A.; Vance, D.E. A gender-specific role for phosphatidylethanolamine N-methyltransferase-derived phosphatidylcholine in the regulation of plasma high density and very low density lipoproteins in mice. J. Biol. Chem. 2003, 278, 21851–21859. [Google Scholar] [CrossRef] [PubMed]
- Kühn, T.; Rohrmann, S.; Sookthai, D.; Johnson, T.; Katzke, V.; Kaaks, R.; von Eckardstein, A.; Müller, D. Intra-individual variation of plasma trimethylamine-N-oxide (TMAO), betaine and choline over 1 year. Clin. Chem. Lab. Med. 2017, 55, 261–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krüger, R.; Merz, B.; Rist, M.J.; Ferrario, P.G.; Bub, A.; Kulling, S.E.; Watzl, B. Associations of current diet with plasma and urine TMAO in the KarMeN study: Direct and indirect contributions. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef]
- Rohrmann, S.; Linseisen, J.; Allenspach, M.; von Eckardstein, A.; Müller, D. Plasma Concentrations of Trimethylamine-N-oxide Are Directly Associated with Dairy Food Consumption and Low-Grade Inflammation in a German Adult Population. J. Nutr. 2016, 146, 283–289. [Google Scholar] [CrossRef]
- Zhernakova, A.; Kurilshikov, A.; Bonder, M.J.; Tigchelaar, E.F.; Schirmer, M.; Vatanen, T.; Mujagic, Z.; Vila, A.V.; Falony, G.; Vieira-Silva, S.; et al. Population-based metagenomics analysis reveals markers for gut microbiome composition and diversity. Science 2016, 352, 565–569. [Google Scholar] [CrossRef] [Green Version]
- Cho, C.E.; Caudill, M.A. Trimethylamine-N-Oxide: Friend, Foe, or Simply Caught in the Cross-Fire? Trends Endocrinol. Metab. 2017, 28, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Senthong, V.; Li, X.S.; Hudec, T.; Coughlin, J.; Wu, Y.; Levison, B.; Wang, Z.; Hazen, S.L.; Tang, W.H. Plasma Trimethylamine N-Oxide, a Gut Microbe-Generated Phosphatidylcholine Metabolite, Is Associated With Atherosclerotic Burden. J. Am. Coll. Cardiol. 2016, 67, 2620–2628. [Google Scholar] [CrossRef]
- Tang, W.H.; Wang, Z.; Fan, Y.; Levison, B.; Hazen, J.E.; Donahue, L.M.; Wu, Y.; Hazen, S.L. Prognostic value of elevated levels of intestinal microbe-generated metabolite trimethylamine-N-oxide in patients with heart failure: Refining the gut hypothesis. J. Am. Coll. Cardiol. 2014, 64, 1908–1914. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Tang, W.H.; Buffa, J.A.; Fu, X.; Britt, E.B.; Koeth, R.A.; Levison, B.S.; Fan, Y.; Wu, Y.; Hazen, S.L. Prognostic value of choline and betaine depends on intestinal microbiota-generated metabolite trimethylamine-N-oxide. Eur. Heart J. 2014, 35, 904–910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silaghi, C.A.; Silaghi, H.; Colosi, H.A.; Craciun, A.E.; Farcas, A.; Cosma, D.T.; Hancu, N.; Pais, R.; Georgescu, C.E. Prevalence and predictors of non-alcoholic fatty liver disease as defined by the fatty liver index in a type 2 diabetes population. Clujul. Med. 2016, 89, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Fedchuk, L.; Nascimbeni, F.; Pais, R.; Charlotte, F.; Housset, C.; Ratziu, V.; LIDO Study Group. Performance and limitations of steatosis biomarkers in patients with nonalcoholic fatty liver disease. Aliment Pharmacol. Ther. 2014, 40, 1209–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Parameters | Normal Weight n = 34; 24.8% | Over Weight n = 29; 21.2% | Grade I Obesity n = 21; 15.3% | Grade II Obesity n = 15; 10.9% | Grade III Obesity n = 38; 27.7% | p-value |
|---|---|---|---|---|---|---|
| Lifestyle Habits | ||||||
| Age (years) | 35.71 ± 8.48 | 38.14 ± 7.58 | 38.24 ± 5.89 | 35.80 ± 8.20 | 35.00 ± 6.82 | 0.292 |
| Smoking (yes) | 16, 47.1% | 19, 65.5% | 4, 19.0% | 2, 13.3% | 22, 10.5% | χ2 = 19.21, p < 0.001 |
| Physical activity (yes) | 22, 64.7% | 11, 37.9% | 3, 14.3% | 5, 33.3% | 4, 10.5% | χ2 = 27.85, p < 0.001 |
| Anthropometric measurement | ||||||
| BMI (kg/m2) | 23.01 ± 1.49 | 27.32 ± 1.43 | 32.41 ± 1.37 | 37.48 ± 1.56 | 46.99 ± 5.16 | <0.001 |
| WC (cm) | 85.12 ± 10.13 | 94.30 ± 12.38 | 109.65 ± 8.14 | 118.81 ± 13.40 | 139.47 ± 15.15 | <0.001 |
| Blood pressure | ||||||
| SBP (mmHg) | 115.44 ± 8.01 | 121.21 ± 10.90 | 129.52 ± 10.83 | 131.00 ± 16.38 | 133.68 ± 11.79 | <0.001 |
| DBP (mmHg) | 71.33 ± 6.07 | 75.68 ± 7.41 | 81.67 ± 6.77 | 86.33 ± 11.25 | 89.61 ± 9.25 | <0.001 |
| Metabolic profile | ||||||
| Circulating levels of TMAO (µM) | 3.62 ± 2.37 | 8.23 ± 0.67 | 9.03 ± 0.97 | 9.89 ± 0.85 | 11.53 ± 0.96 | <0.001 |
| Fasting Glucose (mg/dL) | 83.65 ± 10.25 | 93.17 ± 13.10 | 96.47 ± 12.11 | 97.73 ± 11.00 | 121.87 ± 10.91 | <0.001 |
| Insulin (µU/mL) | 2.66 ± 1.23 | 7.01 ± 5.35 | 10.69 ± 5.83 | 14.85 ± 9.65 | 31.29 ± 8.87 | <0.001 |
| Total cholesterol (mg/dL) | 146.8 ± 20.28 | 176.69 ± 29.17 | 170.76 ± 20.85 | 206.87 ± 39.57 | 221.37 ± 33.58 | <0.001 |
| HDL cholesterol (mg/dL) | 57.59 ± 7.53 | 50.21 ± 8.19 | 41.95 ± 13.28 | 39.60 ± 10.60 | 37.05 ± 9.42 | <0.001 |
| LDL cholesterol (mg/dL) | 69.92 ± 23.15 | 101.43 ± 30.05 | 103.37 ± 16.67 | 134.49 ± 41.49 | 150.17 ± 38.54 | <0.001 |
| Triglycerides (mg/dL) | 96.71 ± 26.96 | 125.24 ± 28.30 | 155.52 ± 65.23 | 163.87 ± 33.78 | 170.74 ± 70.88 | <0.001 |
| ALT (U/L) | 23.26 ± 6.87 | 24.89 ± 9.06 | 38.14 ± 12.16 | 40.73 ± 17.87 | 41.39 ± 22.49 | <0.001 |
| AST (U/L) | 20.44 ± 5.57 | 26.58 ± 6.67 | 36.83 ± 18.25 | 39.07 ± 14.10 | 41.00 ± 20.12 | <0.001 |
| γGT (U/L) | 25.64 ± 6.62 | 26.52 ± 12.48 | 42.42 ± 19.71 | 44.47 ± 19.65 | 49.53 ± 27.20 | <0.001 |
| Cardio-metabolic indices | ||||||
| HoMA-IR | 0.55 ± 0.28 | 1.49 ± 0.96 | 2.51 ± 1.32 | 3.55 ± 2.31 | 9.52 ± 3.13 | <0.001 |
| VAI | 1.28 ± 0.54 | 2.09 ± 1.27 | 3.42 ± 2.91 | 3.55 ± 1.97 | 3.77 ± 2.18 | <0.001 |
| FLI | 19.89 ± 12.37 | 43.70 ± 21.36 | 79.39 ± 10.26 | 90.98 ± 6.97 | 98.36 ± 2.30 | <0.001 |
| Metabolic Syndrome | ||||||
| MetS (number parameter) | 0.18 ± 0.52 | 1.24 ± 1.02 | 2.33 ± 1.06 | 2.67 ± 1.40 | 3.68 ± 1.07 | <0.001 |
| MetS (presence) | 0, 0 | 4, 13.8% | 9, 42.9% | 9, 60% | 31, 81.6% | χ2 = 61.53, p < 0.001 |
| Nutritional parameters | ||||||
| Total energy intake (kcal) | 2084.79 ± 304.05 | 2249.14 ± 433.86 | 2423.33 ± 211.27 | 2658.67 ± 244.80 | 2966.45 ± 365.69 | <0.001 |
| Parameters | Circulating Levels of TMAO (µM) | p-value | ||
|---|---|---|---|---|
| Gender | Males (n 59) | 9.11 ± 3.09 | 0.015 | |
| Females (n 78) | 7.70 ± 3.28 | |||
| Smoking | Yes (n 68) | 9.38 ± 2.63 | <0.001 | |
| No (n 69) | 7.24 ± 3.49 | |||
| Physical activity | Yes (n 58) | 6.41 ± 3.52 | <0.001 | |
| No (n 79) | 9.69 ± 2.21 | |||
| HoMA-IR | > cut-off (n 64) | 10.53 ± 1.62 | <0.001 | |
| < cut-off (n 73) | 6.36 ± 3.01 | |||
| VAI | > cut-off (n 60) | 10.08 ± 2.13 | <0.001 | |
| < cut-off (n 77) | 6.92 ± 3.33 | |||
| FLI | > cut-off (n 82) | 10.24 ± 1.56 | <0.001 | |
| < cut-off (n 55) | 5.42 ± 3.00 | |||
| MetS (parameters) | ||||
| WC | Yes (n 87) | 9.88 ± 2.06 | <0.001 | |
| No (n 50) | 5.56 ± 3.18 | |||
| SBP/DBP | Yes (n 37) | 10.49 ± 1.72 | <0.001 | |
| No (n 100) | 7.50 ± 3.33 | |||
| Fasting Glucose | Yes (n 43) | 11.29 ± 1.22 | <0.001 | |
| No (n 94) | 6.94 ± 2.98 | |||
| HDL cholesterol | Yes (n 59) | 10.13 ± 2.09 | <0.001 | |
| No (n 78) | 6.93 ± 3.33 | |||
| Triglycerides | Yes (n 45) | 10.28 ± 2.20 | <0.001 | |
| No (n 92) | 7.34 ± 3.27 | |||
| MetS (presence/absence) | Yes (n 53) | 10.65 ± 1.62 | <0.001 | |
| No (n 84) | 6.82 ± 3.17 | |||
| Parameters | Circulating Levels of TMAO (µM) | Circulating Levels of TMAO (µM) | ||
|---|---|---|---|---|
| Simple Correlation | After Adjusting | |||
| r | p-value | r | p-value | |
| Age (years) | 0.103 | 0.232 | 0.169 | 0.054 |
| Anthropometric measurements | ||||
| BMI (kg/m2) | 0.737 | <0.001 | - | - |
| WC (cm) | 0.670 | <0.001 | −0.055 | 0.538 |
| Blood pressure | ||||
| SBP (mmHg) | 0.600 | <0.001 | 0.273 | 0.002 |
| DBP (mmHg) | 0.532 | <0.001 | 0.149 | 0.091 |
| Metabolic profile | ||||
| Fasting Glucose (mg/dL) | 0.656 | <0.001 | 0.034 | 0.700 |
| Insulin (µU/mL) | 0.668 | <0.001 | 0.202 | 0.021 |
| Total cholesterol (mg/dL) | 0.628 | <0.001 | 0.236 | 0.007 |
| HDL cholesterol (mg/dL) | −0.568 | <0.001 | −0.180 | 0.041 |
| LDL cholesterol (mg/dL) | 0.663 | <0.001 | 0.356 | <0.001 |
| Triglycerides (mg/dL) | 0.535 | <0.001 | 0.224 | 0.010 |
| ALT (U/L) | 0.376 | 0.001 | 0.065 | 0.461 |
| AST (U/L) | 0.506 | <0.001 | 0.176 | 0.046 |
| γGT (U/L) | 0.396 | 0.001 | 0.086 | 0.333 |
| Cardio-metabolic indices | ||||
| HoMA-IR | 0.699 | <0.001 | 0.211 | 0.016 |
| VAI | 0.549 | <0.001 | 0.255 | 0.003 |
| FLI | 0.820 | <0.001 | 0.604 | <0.001 |
| Nutritional parameter | ||||
| Total energy intake (kcal) | 0.592 | <0.001 | - | - |
| Parameters | Circulating Levels of TMAO (µM) | ||||
|---|---|---|---|---|---|
| OR | p-value | 95% IC | R2 | ||
| Gender | 1.15 | 0.015 | 1.029–1.295 | 0.047 | |
| Smoking | 1.26 | 0.001 | 1.110–1.423 | 0.108 | |
| Physical activity | 0.67 | <0.001 | 0.576–0.788 | 0.240 | |
| BMI categories | |||||
| Normal weight | 0.05 | 0.001 | 0.009–0.297 | 0.604 | |
| Overweight | 0.27 | <0.001 | 0.011–1.121 | 0.209 | |
| Grade I obesity | 0.18 | <0.001 | 0.010–0.099 | 0.237 | |
| Grade II obesity | 1.25 | <0.001 | 0.995–1.565 | 0.033 | |
| Grade III obesity | 9.59 | <0.001 | 3.946–23.344 | 0.561 | |
| HoMA-IR | 2.82 | <0.001 | 1.937–4.116 | 0.458 | |
| VAI | 1.58 | <0.001 | 1.308–1.912 | 0.248 | |
| FLI | 4.31 | <0.001 | 2.353–7.874 | 0.536 | |
| MetS (single parameters) | |||||
| WC | 1.88 | <0.001 | 1.490–2.375 | 0.378 | |
| SBP/DBP | 1.64 | <0.001 | 1.304–2.065 | 0.201 | |
| Fasting Glucose | 5.84 | <0.001 | 3.161–10.804 | 0.538 | |
| HDL cholesterol | 1.61 | <0.001 | 1.320–1.953 | 0.254 | |
| Triglycerides | 1.57 | 0.001 | 1.278–1.919 | 0.205 | |
| MetS (presence/absence) | 2.36 | <0.001 | 1.727–3.227 | 0.389 | |
| Parameters | Multiple Regression Analysis | |||
|---|---|---|---|---|
| Model 1 | R2 | β | t | p-value |
| FLI | 0.672 | 0.820 | 16.63 | <0.001 |
| Variables excluded: HoMA-IR and VAI | ||||
| Model 2 | ||||
| FLI | 0.469 | 0.685 | 9.2 | <0.001 |
| Variables excluded: MetS | ||||
| Parameters | Methodology | Participants | Effects | Hypothesis | Studies | Concordance |
|---|---|---|---|---|---|---|
| Nascent Metabolic Syndrome (MetS) | Case-control clinical study | 30 patients 20 controls | TMAO with a trend of positive correlation | TMAO levels rise only after MetS has advanced to the later stages including T2DM and/or CVD | [9] | Yes |
| HoMA-IR | Case-control clinical study | 30 patients 20 controls | TMAO not significantly correlated | No major role for TMAO in glucose metabolism or insulin sensitivity | [9] | No |
| Intervention Program | 220 subjects | A negative correlation between circulating TMAO levels insulin sensitivity | In obese, hyperglycemic humans FMO3 expression and TMAO levels are increased in hepatic insulin resistance. | [12] | Yes | |
| NAFLD | Experimental study | Mouse strain 129S6, documented for its susceptibility to IR or NAFLD | Mice 129S6 fed with a high-fat diet showed a high urinary excretion of TMAO associated with insulin resistance and NAFLD | A high-fat diet reduces the conversion and the bioavailability of choline by microbiota, causing NAFLD | [44] | Yes |
| Experimental study | Male ob/ob mice and their lean, wild-type C57BL/6J controls | Liver insulin receptor knockout mice with selective hepatic insulin resistance have increased circulating TMAO levels associated with a strong up-regulation of the TMAO-producing enzyme FMO3 in the liver | TMAO may block the hepatic insulin signaling pathway promoting the development of fatty liver | [11] | Yes | |
| Case-control study (CCS) and cross-sectional study (CSS) | 60 adult patients and 35 controls for CCS 1.628participants for CSS | TMAO is an independent risk marker for NAFLD in humans. in both the CCS and CSS studies | TMAO decreases the total bile acid pool size and influences the hepatic triglycerides levels, as a potential risk factor for fatty liver disease | [13] | Yes | |
| Intervention Program | 220 subjects | A positive correlation between circulating TMAO levels and liver fat content | Fasting levels of TMAO are regulated by hepatic FMO3 | [12] | Yes | |
| Cross-sectional study | One hundred middle-aged men | A strong positive association between liver function and a pattern of amino acids, which included TMAO | A pattern of amino acids, included TMAO, are regulated by liver enzymes | [18] | Yes | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barrea, L.; Annunziata, G.; Muscogiuri, G.; Di Somma, C.; Laudisio, D.; Maisto, M.; De Alteriis, G.; Tenore, G.C.; Colao, A.; Savastano, S. Trimethylamine-N-oxide (TMAO) as Novel Potential Biomarker of Early Predictors of Metabolic Syndrome. Nutrients 2018, 10, 1971. https://doi.org/10.3390/nu10121971
Barrea L, Annunziata G, Muscogiuri G, Di Somma C, Laudisio D, Maisto M, De Alteriis G, Tenore GC, Colao A, Savastano S. Trimethylamine-N-oxide (TMAO) as Novel Potential Biomarker of Early Predictors of Metabolic Syndrome. Nutrients. 2018; 10(12):1971. https://doi.org/10.3390/nu10121971
Chicago/Turabian StyleBarrea, Luigi, Giuseppe Annunziata, Giovanna Muscogiuri, Carolina Di Somma, Daniela Laudisio, Maria Maisto, Giulia De Alteriis, Gian Carlo Tenore, Annamaria Colao, and Silvia Savastano. 2018. "Trimethylamine-N-oxide (TMAO) as Novel Potential Biomarker of Early Predictors of Metabolic Syndrome" Nutrients 10, no. 12: 1971. https://doi.org/10.3390/nu10121971
APA StyleBarrea, L., Annunziata, G., Muscogiuri, G., Di Somma, C., Laudisio, D., Maisto, M., De Alteriis, G., Tenore, G. C., Colao, A., & Savastano, S. (2018). Trimethylamine-N-oxide (TMAO) as Novel Potential Biomarker of Early Predictors of Metabolic Syndrome. Nutrients, 10(12), 1971. https://doi.org/10.3390/nu10121971