Is Matrix Gla Protein Associated with Vascular Calcification? A Systematic Review

Abstract
:1. Introduction
2. Methodology
2.1. Search Strategy
2.2. Selection of Studies
2.3. Study Selection and Data Extraction
2.4. Risk of Bias Assessment
2.5. Data Extraction and Data Analysis
3. Results
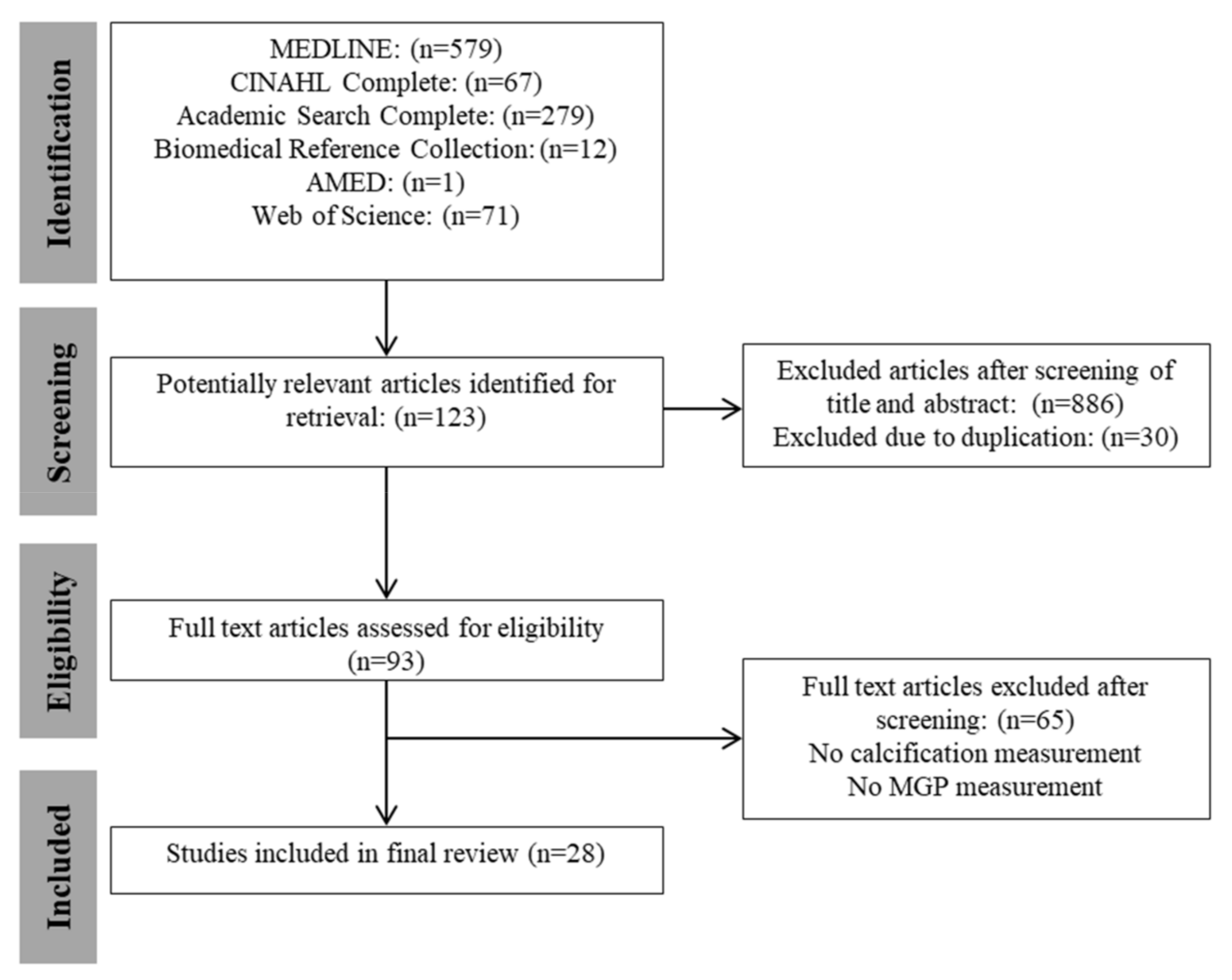
3.1. Literature Search
3.2. Risk of Bias Assessment
3.3. Study Characteristics
3.3.1. Study Population
3.3.2. Calcification Measurement
3.3.3. MGP Measurement
3.4. Summary of Study Cohorts
3.4.1. Atherosclerosis
3.4.2. Chronic Kidney Disease
3.4.3. Vitamin K Antagonists
3.4.4. Diabetes
3.4.5. Healthy Participants
3.4.6. Vitamin K Supplementation
4. Discussion
4.1. MGP Species
4.2. Calcification Development
4.3. Study Designs
4.4. Future Research and Clinical Implications
4.5. Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Wu, X.H.; Chen, X.Y.; Fan, Y.H.; Leung, T.W.H.; Wong, K.S. High Extent of Intracranial Carotid Artery Calcification Is Associated with Downstream Microemboli in Stroke Patients. J. Stroke Cerebrovasc. Dis. 2017, 26, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Zettervall, S.L.; Marshall, A.P.; Fleser, P.; Guzman, R.J. Association of arterial calcification with chronic limb ischemia in patients with peripheral artery disease. J. Vasc. Surg. 2017, 67, 507–513. [Google Scholar] [CrossRef] [PubMed]
- London, G.M.; Guérin, A.P.; Marchais, S.J.; Métivier, F.; Pannier, B.; Adda, H. Arterial media calcification in end-stage renal disease: Impact on all-cause and cardiovascular mortality. Nephrol. Dial. Transplant. 2003, 18, 1731–1740. [Google Scholar] [CrossRef] [PubMed]
- Guzman, R.J.; Brinkley, D.; Schumacher, P.; Donahue, R.M.; Beavers, H.; Qin, X. Tibial artery calcification as a marker of amputation risk in patients with PAD. J. Am. Coll. Cardiol. 2008, 51, 1967–1974. [Google Scholar] [CrossRef] [PubMed]
- Chatrou, M.L.L.; Reutelingsperger, C.P.; Schurgers, L.J. Role of vitamin K-dependent proteins in the arterial vessel wall. Hamostaseologie 2011, 31, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Price, P.A.; Otsuka, A.A.; Poser, J.W.; Kristaponis, J.; Raman, N. Characterization of a gamma-carboxyglutamic acid-containing protein from bone. Proc. Natl. Acad. Sci. USA 1976, 73, 1447–1451. [Google Scholar] [CrossRef] [PubMed]
- Speer, M.Y.; Yang, H.Y.; Brabb, T.; Leaf, E.; Look, A.; Lin, W.L.; Frutkin, A.; Dichek, D.; Giachelli, C.M. Smooth muscle cells give rise to osteochondrogenic precursors and chondrocytes in calcifying arteries. Circ. Res. 2009, 104, 733–741. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Jumabay, M.; Ly, A.; Radparvar, M.; Cubberly, M.R.; Boström, K.I. A role for the endothelium in vascular calcification. Circ. Res. 2013, 113, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Schurgers, L.J.; Spronk, H.M.; Skepper, J.N.; Hackeng, T.; Shanahan, C.; Vermeer, C.; Weissberg, P.; Proudfoot, D. Post-translational modifications regulate matrix Gla protein function: Importance for inhibition of vascular smooth muscle cell calcification. J. Thromb. Haemost. 2007, 5, 2503–2511. [Google Scholar] [CrossRef] [PubMed]
- Willems, B.A.G.; Vermeer, C.; Reutelingsperger, C.P.M.; Schurgers, L.J. The realm of vitamin K dependent proteins: Shifting from coagulation toward calcification. Mol. Nutr. Food Res. 2014, 58, 1620–1635. [Google Scholar] [CrossRef] [PubMed]
- Dalager, S.; Falk, E.; Kristensen, I.B.; Paaske, W.P. Plaque in superficial femoral arteries indicates generalized atherosclerosis and vulnerability to coronary death: An autopsy study. J. Vasc. Surg. 2008, 47, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Ammirati, E.; Moroni, F.; Norata, G.D.; Magnoni, M.; Camici, P.G. Markers of inflammation associated with plaque progression and instability in patients with carotid atherosclerosis. Mediat. Inflamm. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Mayer, O.; Seidlerová, J.; Bruthans, J.; Filipovský, J.; Timoracká, K.; Vaněk, J.; Černá, L.; Wohlfahrt, P.; Cífková, R.; Theuwissen, E.; et al. Desphospho-uncarboxylated matrix Gla-protein is associated with mortality risk in patients with chronic stable vascular disease. Atherosclerosis 2014, 235, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Liabeuf, S.; Bourron, O.; Olivier, B.; Vemeer, C.; Theuwissen, E.; Magdeleyns, E.; Aubert, C.E.; Brazier, M.; Mentaverri, R.; Hartemann, A.; et al. Vascular calcification in patients with type 2 diabetes: The involvement of matrix Gla protein. Cardiovasc. Diabetol. 2014, 13, 85. [Google Scholar] [CrossRef] [PubMed]
- Parker, B.D.; Schurgers, L.J.; Vermeer, C.; Schiller, N.B.; Whooley, M.A.; Ix, J.H. The association of uncarboxylated matrix Gla protein with mitral annular calcification differs by diabetes status: The Heart and Soul study. Atherosclerosis 2010, 210, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Schurgers, L.J.; Joosen, I.A.; Laufer, E.M.; Chatrou, M.L.L.; Herfs, M.; Winkens, M.H.M.; Westenfeld, R.; Veulemans, V.; Krueger, T.; Shanahan, C.M.; et al. Vitamin K-Antagonists Accelerate Atherosclerotic Calcification and Induce a Vulnerable Plaque Phenotype. PLoS ONE 2012, 7, e43229. [Google Scholar] [CrossRef] [PubMed]
- Schurgers, L.J.; Barreto, D.V.; Barreto, F.C.; Liabeuf, S.; Renard, C.; Magdeleyns, E.J.; Vermeer, C.; Choukroun, G.; Massy, Z.A. The circulating inactive form of matrix Gla protein is a surrogate marker for vascular calcification in chronic kidney disease: A preliminary report. Clin. J. Am. Soc. Nephrol. 2010, 5, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Schlieper, G.; Westenfeld, R.; Kruger, T.; Cranenburg, E.C.; Magdeleyns, E.J.; Brandenburg, V.M.; Djuric, Z.; Damjanovic, T.; Ketteler, M.; Vermeer, C.; et al. Circulating Nonphosphorylated Carboxylated Matrix Gla Protein Predicts Survival in ESRD. J. Am. Soc. Nephrol. 2011, 22, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Ueland, T.; Dahl, C.P.; Gullestad, L.; Aakhus, S.; Broch, K.; Skardal, R.; Vermeer, C.; Aukrust, P.; Schurgers, L.J. Circulating levels of non-phosphorylated undercarboxylated matrix Gla protein are associated with disease severity in patients with chronic heart failure. Clin. Sci. 2011, 121, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Schurgers, L.J.; Teunissen, K.J.F.; Knapen, M.H.J.; Kwaijtaal, M.; van Diest, R.; Appels, A.; Reutelingsperger, C.P.; Cleutjens, J.P.M.; Vermeer, C. Novel conformation-specific antibodies against matrix γ-carboxyglutamic acid (Gla) protein: Undercarboitylated matrix Gla protein as marker for vascular calcification. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1629–1633. [Google Scholar] [CrossRef] [PubMed]
- Agustina, M.; Fernando, A.; Laura, G.; Luz, G.; Nancy, H.L.; Ana, M.B.; Gustavo, H.I.; Marta, F.; Nora, V.; Silvia, I.V.; et al. Women’s preferences and mode of delivery in public and private hospitals: A prospective cohort study. BMC Pregnancy Childb. 2016, 16, 34. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef] [PubMed]
- Torii, S.; Ikari, Y.; Tanabe, K.; Kakuta, T.; Hatori, M.; Shioi, A.; Okano, T. Plasma phylloquinone, menaquinone-4 and menaquinone-7 levels and coronary artery calcification. J. Nutr. Sci. 2016, 5, e48. [Google Scholar] [CrossRef] [PubMed]
- Kurnatowska, I.; Grzelak, P.; Masajtis-Zagajewska, A.; Kaczmarska, M.; Stefańczyk, L.; Vermeer, C.; Maresz, K.; Nowicki, M. Effect of vitamin K2 on progression of atherosclerosis and vascular calcification in non-dialyzed patients with chronic kidney disease stage 3–5. Pol. Arch. Med. Wewn. 2015, 125, 631–640. [Google Scholar] [PubMed]
- Koos, R.; Krueger, T.; Westenfeld, R.; Kühl, H.P.; Brandenburg, V.; Mahnken, A.H.; Stanzel, S.; Vermeer, C.; Cranenburg, E.C.M.; Floege, J.; et al. Relation of circulating matrix Gla-protein and anticoagulation status in patients with aortic valve calcification. Thromb. Haemost. 2009, 101, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Delanaye, P.; Krzesinski, J.-M.; Warling, X.; Moonen, M.; Smelten, N.; Médart, L.; Pottel, H.; Cavalier, E. Dephosphorylated-uncarboxylated Matrix Gla protein concentration is predictive of vitamin K status and is correlated with vascular calcification in a cohort of hemodialysis patients. BMC Nephrol. 2014, 15, 145. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, C.J.; Shea, M.K.; Price, P.A.; Gagnon, D.R.; Wilson, P.W.F.; Larson, M.G.; Kiel, D.P.; Hoffmann, U.; Ferencik, M.; Clouse, M.E.; et al. Matrix Gla protein is associated with risk factors for atherosclerosis but not with coronary artery calcification. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 2769–2774. [Google Scholar] [CrossRef] [PubMed]
- Canfield, A.E.; Farrington, C.; Dziobon, M.D.; Boot-Handford, R.P.; Heagerty, A.M.; Kumar, S.N.; Roberts, I.S.D. The involvement of matrix glycoproteins in vascular calcification and fibrosis: An immunohistochemical study. J. Pathol. 2002, 196, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Shroff, R.C.; Shah, V.; Hiorns, M.P.; Schoppet, M.; Hofbauer, L.C.; Hawa, G.; Schurgers, L.J.; Singhal, A.; Merryweather, I.; Brogan, P.; et al. The circulating calcification inhibitors, fetuin-A and osteoprotegerin, but not Matrix Gla protein, are associated with vascular stiffness and calcification in children on dialysis. Nephrol. Dial. Transplant. 2008, 23, 3263–3271. [Google Scholar] [CrossRef] [PubMed]
- Rennenberg, R.J.M.W.; de Leeuw, P.W.; Kessels, A.G.H.; Schurgers, L.J.; Vermeer, C.; van Engelshoven, J.M.A.; Kemerink, G.J.; Kroon, A.A. Calcium scores and matrix Gla protein levels: Association with vitamin K status. Eur. J. Clin. Investig. 2010, 40, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Rennenberg, R.J.M.W.; van Varik, B.J.; Schurgers, L.J.; Hamulyak, K.; Cate, H.T.; Leiner, T.; Vermeer, C.; de Leeuw, P.W.; Kroon, A.A. Chronic coumarin treatment is associated with increased extracoronary arterial calcification in humans. Blood 2010, 115, 5121–5123. [Google Scholar] [CrossRef] [PubMed]
- Chatrou, M.L.L.; Cleutjens, J.P.; van Vusse, G.J.D.; Roijers, R.B.; Mutsaers, P.H.A.; Schurgers, L.J. Intra-section analysis of human coronary arteries reveals a potential role for micro-calcifications in macrophage recruitment in the early stage of atherosclerosis. PLoS ONE 2015, 10, e0142335. [Google Scholar] [CrossRef] [PubMed]
- Xiao, D.M.; Wu, Q.; Fan, W.F.; Ye, X.W.; Niu, J.Y.; Gu, Y. Effect of serum FGF-23, MGP and fetuin-A on calcium-phosphate metabolism in maintenance hemodialysis patients. Hemodial. Int. 2013, 17, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Jono, S.; Ikari, Y.; Vermeer, C.; Dissel, P.; Hasegawa, K.; Shioi, A.; Taniwaki, H.; Kizu, A.; Nishizawa, Y.; Saito, S. Matrix Gla protein is associated with coronary artery calcification as assessed by electron-beam computed tomography. Thromb. Haemost. 2004, 91, 790–794. [Google Scholar] [CrossRef] [PubMed]
- Pencak, P.; Czerwieńska, B.; Ficek, R.; Wyskida, K.; Kujawa-Szewieczek, A.; Olszanecka-Glinianowicz, M.; Więcek, A.; Chudek, J. Calcification of coronary arteries and abdominal aorta in relation to traditional and novel risk factors of atherosclerosis in hemodialysis patients. BMC Nephrol. 2013, 14, 10. [Google Scholar] [CrossRef] [PubMed]
- Cranenburg, E.C.M.; Brandenburg, V.M.; Vermeer, C.; Stenger, M.; Mühlenbruch, G.; Mahnken, A.H.; Gladziwa, U.; Ketteler, M.; Schurgers, L.J. Uncarboxylated matrix Gla protein (ucMGP) is associated with coronary artery calcification in haemodialysis patients. Thromb. Haemost. 2009, 101, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chen, J.; Zhang, Y.; Yu, W.; Zhang, C.; Gong, L.; Shao, L.; Lu, J.; Gao, Y.; Chen, X.; et al. Common genetic variants of MGP are associated with calcification on the arterial wall but not with calcification present in the atherosclerotic plaques. Circ. Cardiovasc. Genet. 2013, 6, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Dalmeijer, G.W.; van der Schouw, Y.T.; Vermeer, C.; Magdeleyns, E.J.; Schurgers, L.J.; Beulens, J.W.J. Circulating matrix Gla protein is associated with coronary artery calcification and vitamin K status in healthy women. J. Nutr. Biochem. 2013, 24, 624–628. [Google Scholar] [CrossRef] [PubMed]
- Petkovic, N.; Maric, R.; Gajanin, R.; Batinic, D.; Cuk, M.; Ristic, S.; Djukanovic, L. Prevalence and risk factors of vascular calcification in pre-dialysis patients with Balkan endemic nephropathy. Srp. Arh. Celok. Lek. 2016, 144, 608–614. [Google Scholar] [CrossRef]
- Moe, S.M.; Reslerova, M.; Ketteler, M.; O’Neill, K.; Duan, D.; Koczman, J.; Westenfeld, R.; Jahnen-Dechent, W.; Chen, N.X. Role of calcification inhibitors in the pathogenesis of vascular calcification in chronic kidney disease (CKD). Kidney Int. 2005, 67, 2295–2304. [Google Scholar] [CrossRef] [PubMed]
- Aoun, M.; Makki, M.; Azar, H.; Matta, H.; Chelala, D.N. High Dephosphorylated-Uncarboxylated MGP in Hemodialysis patients: Risk factors and response to vitamin K2, A pre-post intervention clinical trial. BMC Nephrol. 2017, 18, 191. [Google Scholar] [CrossRef] [PubMed]
- Shea, M.K.; O’Donnell, C.J.; Vermeer, C.; Magdeleyns, E.J.P.; Crosier, M.D.; Gundberg, C.M.; Ordovas, J.M.; Kritchevsky, S.B.; Booth, S.L.; Donnell, C.J.O.; et al. Circulating Uncarboxylated Matrix Gla Protein Is Associated with Vitamin K Nutritional Status, but Not Coronary Artery Calcium, in Older Adults 1–4. J. Nutr. 2011, 141, 1529–1534. [Google Scholar] [CrossRef] [PubMed]
- Ikari, Y.; Torii, S.; Shioi, A.; Okano, T. Impact of menaquinone-4 supplementation on coronary artery calcification and arterial stiffness: An open label single arm study. Nutr. J. 2015, 15, 53. [Google Scholar] [CrossRef] [PubMed]
- Shea, M.K.; Donnell, C.J.O.; Hoffmann, U.; Dallal, G.E.; Dawson-Hughes, B.; Price, P.A.; Williamson, M.K.; Booth, S.L.; O’Donnell, C.J.; Ordovas, J.M. Vitamin K supplementation and progression of coronary artery calcium in older men and women. Am. J. Clin. Nutr. 2009, 89, 1799–1807. [Google Scholar] [CrossRef] [PubMed]
- Meuwese, C.L.; Olauson, H.; Qureshi, A.R.; Ripsweden, J.; Barany, P.; Vermeer, C.; Drummen, N.; Stenvinkel, P. Associations between thyroid hormones, calcification inhibitor levels and vascular calcification in end-stage renal disease. PLoS ONE 2015, 10, e0132353. [Google Scholar] [CrossRef] [PubMed]
- Theuwissen, E.; Smit, E.; Vermeer, C. The Role of Vitamin K in Soft-Tissue Calcification. Adv. Nutr. 2012, 3, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Lomashvili, K.A.; Wang, X.; Wallin, R.; O’Neill, W.C. Matrix Gla protein metabolism in vascular smooth muscle and role in uremic vascular calcification. J. Biol. Chem. 2011, 286, 28715–28722. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, W.; Obeid, R. Vitamins in the Prevention of Human Diseases; De Gruyter Gmbh & Co. KG: Berlin, Germany; New York, NY, USA, 2011. [Google Scholar]
- Price, P.A.; Thomas, G.R.; Pardini, A.W.; Figueira, W.F.; Caputo, J.M.; Williamson, M.K. Discovery of a high molecular weight complex of calcium, phosphate, fetuin, and matrix γ-carboxyglutamic acid protein in the serum of etidronate-treated rats. J. Biol. Chem. 2002, 277, 3926–3934. [Google Scholar] [CrossRef] [PubMed]
- Merx, M.W.; Schäfer, C.; Westenfeld, R.; Brandenburg, V.; Hidajat, S.; Weber, C.; Ketteler, M.; Jahnen-Dechent, W. Myocardial Stiffness, Cardiac Remodeling, and Diastolic Dysfunction in Calcification-Prone Fetuin-A-Deficient Mice. J. Am. Soc. Nephrol. 2005, 16, 3357–3364. [Google Scholar] [CrossRef] [PubMed]
- Price, P.A.; Nguyen, T.M.T.; Williamson, M.K. Biochemical characterization of the serum fetuin-mineral complex. J. Biol. Chem. 2003, 278, 22153–22160. [Google Scholar] [CrossRef] [PubMed]
- Schurgers, L.J.; Uitto, J.; Reutelingsperger, C.P. Vitamin K-dependent carboxylation of matrix Gla-protein: A crucial switch to control ectopic mineralization. Trends Mol. Med. 2013, 19, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, J.L.; Joannides, A.J.; Skepper, J.N.; Mcnair, R.; Schurgers, L.J.; Proudfoot, D.; Jahnen-Dechent, W.; Weissberg, P.L.; Shanahan, C.M. Human vascular smooth muscle cells undergo vesicle-mediated calcification in response to changes in extracellular calcium and phosphate concentrations: A potential mechanism for accelerated vascular calcification in ESRD. J. Am. Soc. Nephrol. 2004, 15, 2857–2867. [Google Scholar] [CrossRef] [PubMed]
- Van Gorp, R.H.; Schurgers, L.J. New insights into the pros and cons of the clinical use of vitamin K antagonists (VKAs) versus direct oral anticoagulants (DOACs). Nutrients 2015, 7, 9538–9557. [Google Scholar] [CrossRef] [PubMed]
- Criqui, M.H.; Knox, J.B.; Denenberg, J.O.; Forbang, N.I.; McClelland, R.L.; Novotny, T.E.; Sandfort, V.; Waalen, J.; Blaha, M.J.; Allison, M.A. Coronary Artery Calcium Volume and Density: Potential Interactions and Overall Predictive Value: The Multi-Ethnic Study of Atherosclerosis. JACC Cardiovasc. Imaging 2017, 10, 845–854. [Google Scholar] [CrossRef] [PubMed]
- Laclaustra, M.; Casasnovas, J.A.; Fernández-Ortiz, A.; Fuster, V.; León-Latre, M.; Jiménez-Borreguero, L.J.; Pocovi, M.; Hurtado-Roca, Y.; Ordovas, J.M.; Jarauta, E.; et al. Femoral and carotid subclinical atherosclerosis association with risk factors and coronary calcium: The AWHS study. J. Am. Coll. Cardiol. 2016, 67, 1263–1274. [Google Scholar] [CrossRef] [PubMed]
- Demer, L.L.; Tintut, Y.; Nguyen, K.L.; Hsiai, T.; Lee, J.T. Rigor and Reproducibility in Analysis of Vascular Calcification. Circ. Res. 2017, 120, 1240–1242. [Google Scholar] [CrossRef] [PubMed]
- Barrett, H.E.; Cunnane, E.M.; O’Brien, J.M.; Moloney, M.A.; Kavanagh, E.G.; Walsh, M.T. On the effect of computed tomography resolution to distinguish between abdominal aortic aneurysm wall tissue and calcification: A proof of concept. Eur. J. Radiol. 2017, 95, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Herisson, F.; Heymann, M.-F.; Chétiveaux, M.; Charrier, C.; Battaglia, S.; Pilet, P.; Rouillon, T.; Krempf, M.; Lemarchand, P.; Heymann, D.; et al. Carotid and femoral atherosclerotic plaques show different morphology. Atherosclerosis 2011, 216, 348–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irkle, A.; Vesey, A.T.; Lewis, D.Y.; Skepper, J.N.; Bird, J.L.; Dweck, M.R.; Joshi, F.R.; Gallagher, F.A.; Warburton, E.A.; Bennett, M.R.; et al. Identifying active vascular microcalcification by 18F-sodium fluoride positron emission tomography. Nat. Commun. 2015, 6, 7495. [Google Scholar] [CrossRef] [PubMed]
- Kurnatowska, I.; Grzelak, P.; Masajtis-Zagajewska, A.; Kaczmarska, M.; Stefańczyk, L.; Vermeer, C.; Maresz, K.; Nowicki, M. Plasma Desphospho-Uncarboxylated Matrix Gla Protein as a Marker of Kidney Damage and Cardiovascular Risk in Advanced Stage of Chronic Kidney Disease. Kidney Blood Press. Res. 2016, 41, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Shanahan, C.M.; Proudfoot, D.; Farzaneh-Far, A.; Weissberg, P.L. The role of Gla proteins in vascular calcification. Crit. Rev. Eukaryot. Gene Expr. 1998, 8, 357–375. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Study Participation and Sample Size | Risk Factor Measure | Outcome Measure | Statistical Analyses and Reporting | Confounding | Overall Risk of Bias | |
|---|---|---|---|---|---|---|---|
| Athero | [21] | High | Low | Low | Moderate | High | High |
| [23] | Low | Low | Low | High | High | High | |
| [24] | Low | Low | Low | low | Low | Low | |
| [18] | High | Low | Low | High | High | High | |
| [25] | Low | Low | Low | low | Moderate | Moderate | |
| [22] | Moderate | Low | Low | High | High | High | |
| CKD | [26] | High | Low | Low | High | High | High |
| [27] | Low | Low | Low | Low | Low | Low | |
| [28] | Low | Low | Low | High | High | High | |
| [29] | High | Low | Low | High | High | High | |
| [30] | Low | Low | Low | Low | Low | Low | |
| [16] | Low | Low | Low | low | Low | Low | |
| [15] | Low | Low | Low | Low | Low | Low | |
| [31] | High | Low | Low | Low | Low | Low | |
| [32] | Low | Low | Low | High | High | High | |
| [33] | High | Low | Low | High | High | High | |
| VKA | [34] | High | Moderate | Low | Low | Low | Moderate |
| Diabetes | [12] | Low | Low | Low | Low | Low | Low |
| [13] | Low | Low | Low | Low | Low | Low | |
| Healthy | [35] | Low | Low | Low | Low | Low | Low |
| [36] | Low | Low | Low | Low | Low | Low | |
| [37] | High | Moderate | Low | Low | Low | Moderate | |
| [38] | Low | Low | Low | Low | Low | Low | |
| VK sup | [39] | Low | Low | Low | High | High | High |
| [40] | Low | Low | Low | High | High | High | |
| [41] | Low | Low | Low | High | High | High | |
| [42] | Low | Low | Low | Low | Low | Low | |
| [43] | Low | Low | Low | High | High | High |
| Author | Study | Population | Outcome Measure | |||||
|---|---|---|---|---|---|---|---|---|
| Study Design | Cohort | Age (Years) | Sex Male % | Calcification Measurement Method | Calcification Location | MGP Fraction | Main Findings | |
| [32] | Cross sectional | Human autopsy patients (n = 6) from non-cardiac causes | 47–86 years | NR | 3-MeV proton micro beam distribution of micro-calcifications | Coronary | t-ucMGP cMGP Immuno-histochemistry | Micro-calcification correlated with accumulation of t-ucMGP, but not cMGP. |
| [37] | Cross sectional | Control (n = 725); CAW (n = 585); AW (n = 454); CAP (n = 675) | Control 54.9 ± 7.6 CAW 56.8 ± 8.4 AW 57 ± 7.3 CAP 54.2 ± 6.7 | Control 70.6% CAW 70.4% AW 70.9% CAP 72.7% | MDCTA 64-slice Agatston score | CAW AW CAP | MGP | A lack of correlation between MGP levels and calcification in any location. |
| [25] | Cross sectional | Calcific aortic valve disease (n = 191) Control (n = 35) | 71 ± 9 (39–89) | 71% | Non-enhanced MSCT 16-slice Agatston score | Aortic valve Coronary | t-ucMGP | No correlation was found between serum t-ucMGP levels and Agatston aortic valve calcification scores in the patient group. |
| [20] | Cross sectional | Atherosclerotic carotid arteries (n = 10), non-diseased carotid artery (n = 5) and lower limb arteries (n = 6) | 73.2 ± 31.47 | 62% | Alizarin red/Von Kossa staining | Carotid peripheral | MGP t-MGP GluMGP GlaMGP | Advanced carotid plaques (vesicular structures) were present, at the interface of calcium crystal and surrounding tissues mainly co-localizing with GluMGP. In the peripheral arteries, t-MGP was localized in the non-calcified areas and GluMGP was associated with areas of calcification. |
| [34] | Cross sectional | Patients with stable chest pain/signs of myocardial infarction (n = 115) | 64 ± 11 | 60% | EBCT Agatston score | Coronary | MGP | Serum MGP levels were inversely correlated with the severity of coronary CAC scores and found to be independently associated with CAC scores. |
| [28] | Cross sectional | Autopsy patients (n = 10) Atheromatous aortic and coronary artery (n = 45) Normal artery (n = 4) | 44–80 | NR | Von Kossa staining | Coronary Aorta | MGP Immunohisto-chemistry | MGP was associated with calcified deposits and sites of early calcification in calciphylaxis and atherosclerosis, and was not detected in normal vessels or in vessels with fibrointimal proliferation. |
| Author | Study | Population | Outcome Measure | Main Findings | ||||
|---|---|---|---|---|---|---|---|---|
| Study Design | Cohort | Age (Years) | Sex Male % | Calc Measure Method | Calcification Location | MGP Fraction | ||
| [39] | Cross sectional | Stage V CKD pre dialysis—Balkan endemic nephropathy as primary kidney disease (n = 15) and other kidney diseases (n = 17) | BEN: 71.7 ± 6.1 Other: 54.7 ± 11.1 | BEN: 73% Other: 53% | Radio graphic film Adrago calc score | Iliac Femoral Radial Digital | MGP Immunohistochemistry | No significant difference was found between patients with vascular calcification scores of <4 and ≥4 in the expression of MGP in the wall of the radial artery. |
| [45] | Cross sectional | ESRD patients (n = 97) | 45.1 ± 14 | 64% | MDCT 64-slice scans Agatston score | Coronary | t-ucMGP dp-ucMGP | t-ucMGP and dp-ucMGP levels were not associated with CAC scores. |
| [26] | Cross sectional | Patient on hemodialysis (n = 160) (23 VKA; 137 no VKA) | 72 59–81 | 46% | Lateral X-ray radiography (Kauppila method) | Not specified | dp-ucMGP | dp-ucMGP levels were much higher in patients being treated with VKA, and little overlap was found with those not being treated. dp-ucMGP significantly correlated with calcification score. |
| [33] | Cross sectional | Patient on hemodialysis (n = 64) | 60.6 ± 11.3 | 46.87% | 64-slice spiral CT Agatston score | Coronary | MGP | CAC scores were classified into tertiles which revealed a significant positive relationship between increasing CAC and MGP levels. |
| [35] | Cross sectional | Patient on hemodialysis (n = 104); healthy controls (n = 14) | Pt. 50.3–56.9 Ctrl. 45.1–64.1 | 54% | 64-row MSCT Agatston score | Coronary Abdominal aorta | MGP | CAC score was significantly associated with MGP but the AAC score was not associated with MGP levels. |
| [18] | Prospective analysis | Patient on hemodialysis (warfarin excluded) (n = 188) Control group (n = 98) | Pts. 59 ± 11 Ctrl. 58 ± 15 | 54% | X-ray/ultrasound Adragao score Extended composite score | Pelvis Hands Av-fistula Carotid mitral aortic valve | dp-ucMGP dp-cMGP | Dp-cMGP levels were not associated with vascular or valvular calcifications at single sites. Using calcification scores, lower dp-cMGP levels correlated with extensive calcification compared with patients with fewer calcifications. Dp-ucMGP levels did not correlate with the extent of vascular calcifications. |
| [17] | Cross sectional | Caucasian CKD patients (n = 107) | 67 ± 13 | 60% | Multi slice spiral CT Kauppila score | Aorta | dp-ucMGP | A positive, statistically significant association was found between the aortic calcium score and plasma dp-ucMGP level. |
| [36] | Cross sectional | ESRD [CKD stage V] (n = 40) | 36–87 | 42.50% | MSCT 16-slice MSCT Agatston score | Coronary aortic valve | t-ucMGP | T-ucMGP levels had a significant association with CAC scores. T-ucMGP levels were significantly lower in patients in the intermediate and high CAC groups in comparison with patients with low CAC scores. |
| [29] | Cross sectional | Children on dialysis for ≥3 months (n = 61) | 13.4 ± 4.1 | 60.60% | 16-slice spiral CT Agatston score | Epicardial coronary cardiac valves Aorta | t-ucMGP | T-ucMGP levels in children on dialysis were significantly lower compared to healthy controls but no significant associations were found between t-ucMGP and calcification scores. |
| [40] | Cross sectional | Patients on hemodialysis (n = 30) Renal transplant (n = 38) | NR | NR | Quad-slice technique CT total coronary artery calcification score | Coronary aorta | MGP | No correlation was found between MGP levels and calcification of the coronary arteries or aorta. No difference was found in MGP levels between patients with and without calcification. |
| Author | Study | Population | Outcome Measure | Main Findings | ||||
|---|---|---|---|---|---|---|---|---|
| Study Design | Cohort | Age (Years) | Sex Male % | Calc Measure Method | Calc Location | MGP Fraction | ||
| [34] | Cross sectional | Patients on coumarins (n = 19) Control (n = 18) | Patients 48 (33–56) Control46 (36–53) | 64.8% | Soft-tissue 50-kV X-ray based on visibility | Femoral | dp-ucMGP | Coumarin use and dp-ucMGP were associated with femoral artery calcification. |
| Author | Study | Population | Outcome Measure | Main Findings | ||||
|---|---|---|---|---|---|---|---|---|
| Study Design | Cohort | Age (Years) | Sex Male % | Calc Measure Method | Calc Location | MGP Fraction | ||
| [14] | Cross sectional | Type 2 diabetics (n = 198) | 64 ± 8 | 80% | MSCT 128-slice Agatston score | Popliteal Tibial Peroneal | dp-ucMGP t-ucMGP | dp-ucMGP levels were a positive risk factor for an elevated calcification score and independent predictor of peripheral arterial calcification. t-ucMGP appeared to protect against calcification development. |
| [15] | Cross sectional | Outpatients with stable CVD (n = 839) | 68 ± 11 | 81% | Echocardiography Echo-dense structure | Mitral annular | t-ucMGP | A higher concentration of t-ucMGP was associated with lower odds of MAC in persons without diabetes. A higher concentration of t-ucMGP was associated with higher odds of MAC in persons with diabetes for patients with stable CVD. |
| Author | Study | Population | Outcome Measure | Main Findings | ||||
|---|---|---|---|---|---|---|---|---|
| Study Design | Cohort | Age (Years) | Sex Male % | Calcification Measurement Method | Calc Location | MGP Fraction | ||
| [38] | Cross sectional | Post-menopausal women (n = 200) | 66.9 ± 5.5 | 0% | MDCT Agatston score Total volume score | Coronary | t-ucMGP dp-cMGP dp-ucMGP | High t-ucMGP levels were significantly associated with lower CAC. dp-cMGP was not associated with CAC. Low vitamin K-status was associated with high dp-ucMGP concentrations but dp-ucMGP was not associated with CAC in women. |
| [42] | Cross sectional/Longitudinal | Healthy participants no clinical cardiovascular disease (n = 452) | 68.25 (66–70) | 41% | MSCT 8 slice Agatston score | Coronary | dp-ucMGP | Plasma ucMGP was not associated with CAC in healthy older adults. |
| [30] | Cross sectional | Hypertensive patients (n = 36) | 53 ± 10 | 52.7% | High-resolution CT Agatston score Z-score (total calcium) | Carotid Abdominal aorta Coronary | t-ucMGP | No significant correlation between ucMGP and calc sub scores or total calc z-score. A positive association was identified between total arterial calcium score and lower t-ucMGP. |
| [27] | Cross sectional | Framingham Offspring Study A: (n = 2056) B: (n = 452) | A: 57.5 ± 9 B: 68.5 ± 6 | A: 51% B: 41% | A: EBCT B: MDCT Agatston score | Coronary | MGP | No association between MGP and CAC after adjustment for CHD risk score in the groups A or B. |
| Author | Study | Population | Outcome Measure | Main Findings | |||||
|---|---|---|---|---|---|---|---|---|---|
| Study Design | Cohort | Supplement | Age (Years) | Sex Male % | Calc Measure Method | Calc Location | MGP Fraction | ||
| [41] | Prospective, pre-post intervention clinical trial | Hemodialysis patients (n = 50) | 360 μg of menaquinone MK-7 once daily | 71.50 (med 56.75; IQR 79.25) | 30% | X-ray Aortic calcification Severity score (AC-24) | Abdominal aorta | dp-ucMGP | At baseline, dp-ucMGP increased linearly with the increasing calcification score. No correlation between baseline calcification scores and dp-ucMGP drop. |
| [43] | Longitudinal | Cardiovascular disease (n = 26) | 15 mg of menaquinone -4 (Vitmain K2) 3 times daily | 69 ± 8 | 35% | MSCT 64-slice scanner Agatston score | Coronary | t-ucMGP | CAC significantly increased despite the MK-4 treatment |
| [24] | Prospective, randomized, and double-blind | Non-dialyzed with CKD stages 3–5 (n = 42) | 10 μg of cholecalciferol (D n = 12)/90 μg (menaquinone, MK-7) with 10 μg of cholecalciferol (K + D n = 28) | D: 55.4 ± 15.2 K + D; 59.4 ± 9.6 | D; 61.5% K + D; 52% | MSCT Agatston score | Coronary | MGP dp-ucMGP | CAC significantly increased in both groups at the end of treatment period. Vitamin K2 does not significantly affect the progression of calc but does significantly change dp-ucMGP levels. |
| [44] | Double-blind, randomized controlled trial | Healthy men and postmenopausal women subjects (n = 388): treatment group (n = 200), control group (n = 188) | 500 µg phylloquinone (Vitamin K1)/control group received multivitamin formulation without phylloquinone once daily | 68 ± 65 | 40% | MSCT 8-slice Agatston score | Coronary | MGP | No difference in CAC progression between the phylloquinone group and control group. Neither baseline nor change in MGP concentrations predicted the change in CAC. Phylloquinone supplementation slowed CAC progression older adults with pre-existing CAC, independent of its effect on MGP concentrations. |
| [23] | Cross sectional | Patients with CVD (n = 103) | NR | 64 ± 13 | 57% | MSCT 64-sliceAgatston score | Coronary | t-ucMGP | Coronary CAC score was inversely related to t-ucMGP. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barrett, H.; O’Keeffe, M.; Kavanagh, E.; Walsh, M.; O’Connor, E.M. Is Matrix Gla Protein Associated with Vascular Calcification? A Systematic Review. Nutrients 2018, 10, 415. https://doi.org/10.3390/nu10040415
Barrett H, O’Keeffe M, Kavanagh E, Walsh M, O’Connor EM. Is Matrix Gla Protein Associated with Vascular Calcification? A Systematic Review. Nutrients. 2018; 10(4):415. https://doi.org/10.3390/nu10040415
Chicago/Turabian StyleBarrett, Hilary, Mary O’Keeffe, Eamon Kavanagh, Michael Walsh, and Eibhlís M. O’Connor. 2018. "Is Matrix Gla Protein Associated with Vascular Calcification? A Systematic Review" Nutrients 10, no. 4: 415. https://doi.org/10.3390/nu10040415
APA StyleBarrett, H., O’Keeffe, M., Kavanagh, E., Walsh, M., & O’Connor, E. M. (2018). Is Matrix Gla Protein Associated with Vascular Calcification? A Systematic Review. Nutrients, 10(4), 415. https://doi.org/10.3390/nu10040415