Nutritional Interventions to Improve Clinical Outcomes in Ovarian Cancer: A Systematic Review of Randomized Controlled Trials

 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.1.1. Studies
2.1.2. Participants
2.1.3. Interventions
2.1.4. Outcomes
2.2. Information Sources and Search Strategy
2.2.1. Electronic Searches
2.2.2. Hand Searches
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias and Quality Assessment
2.6. Data Synthesis
3. Results
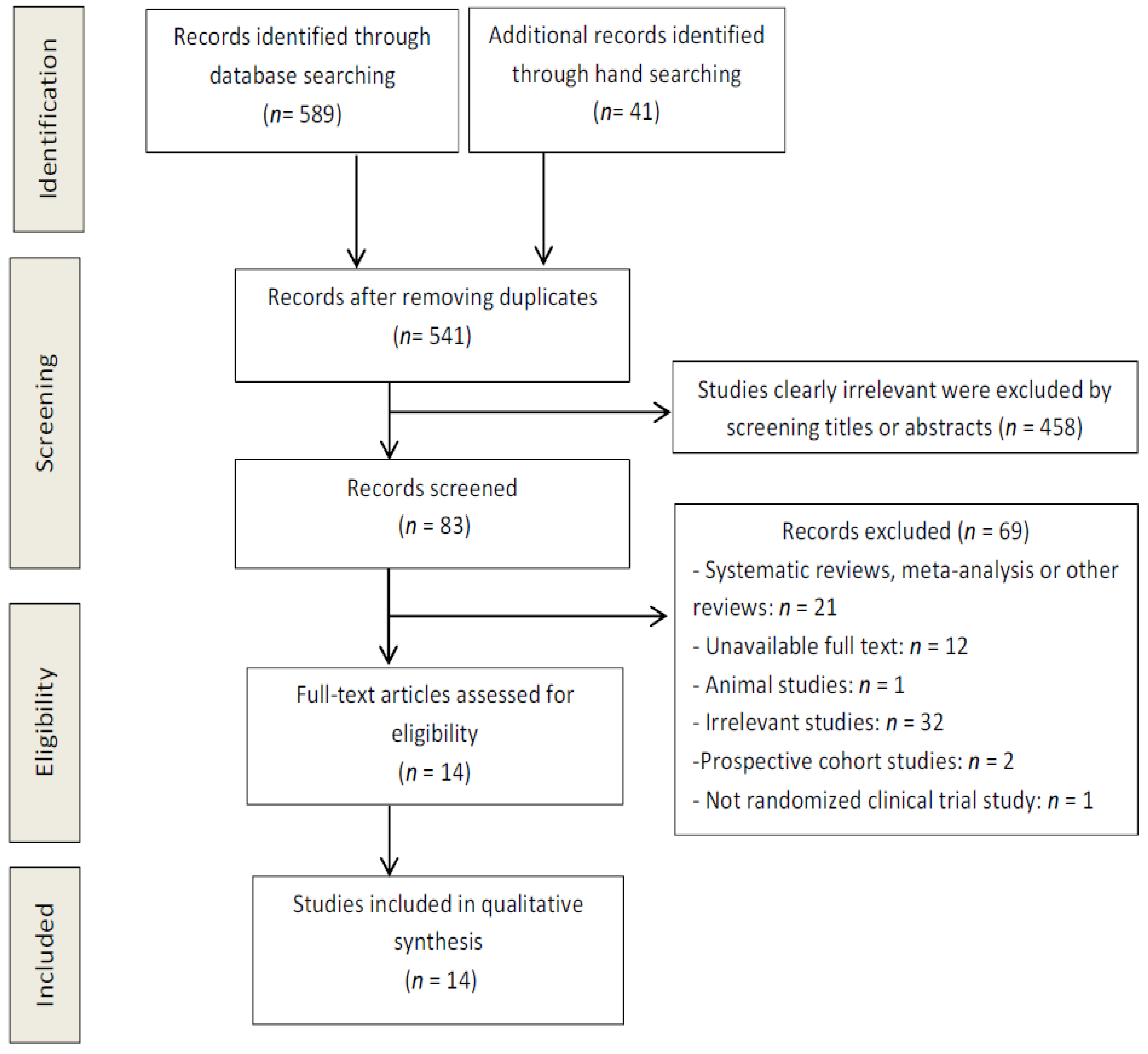
3.1. Study Selection
3.2. Study Characteristics
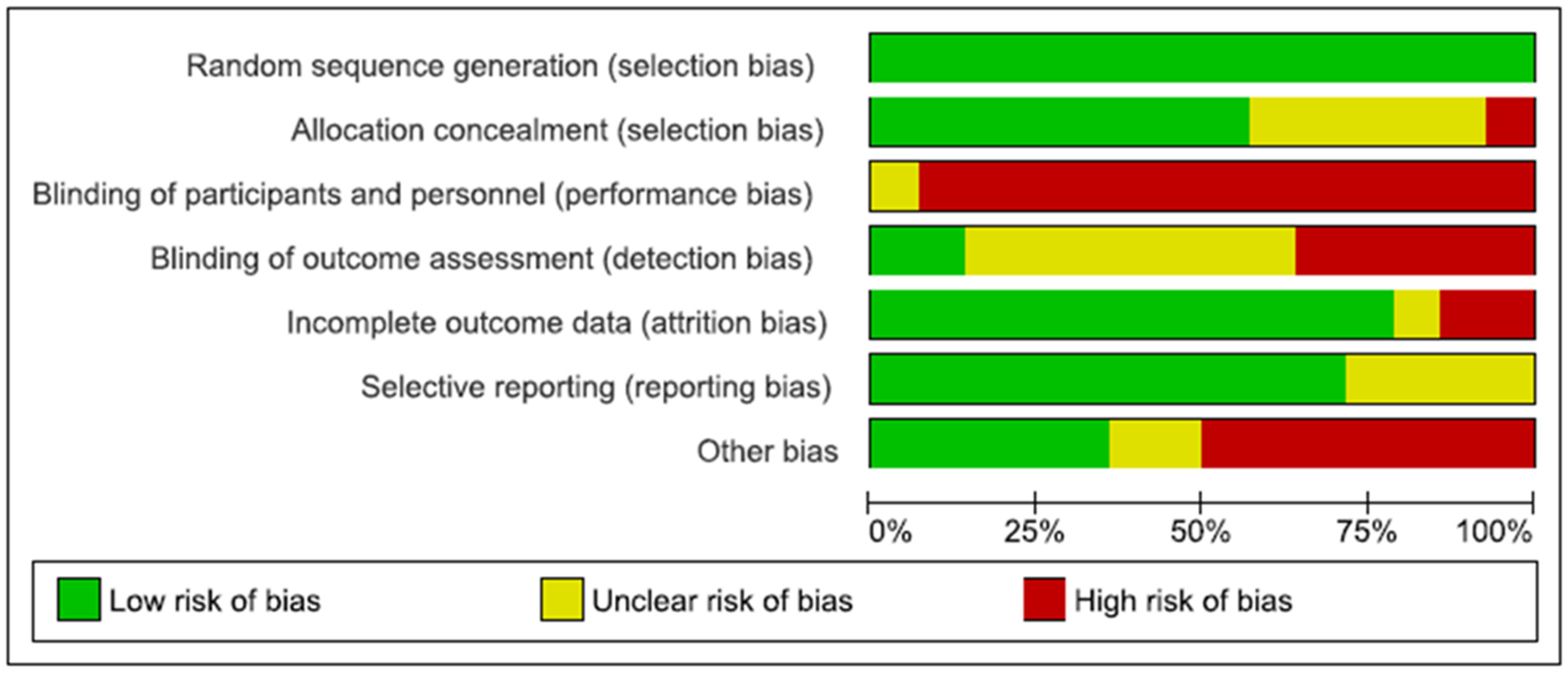
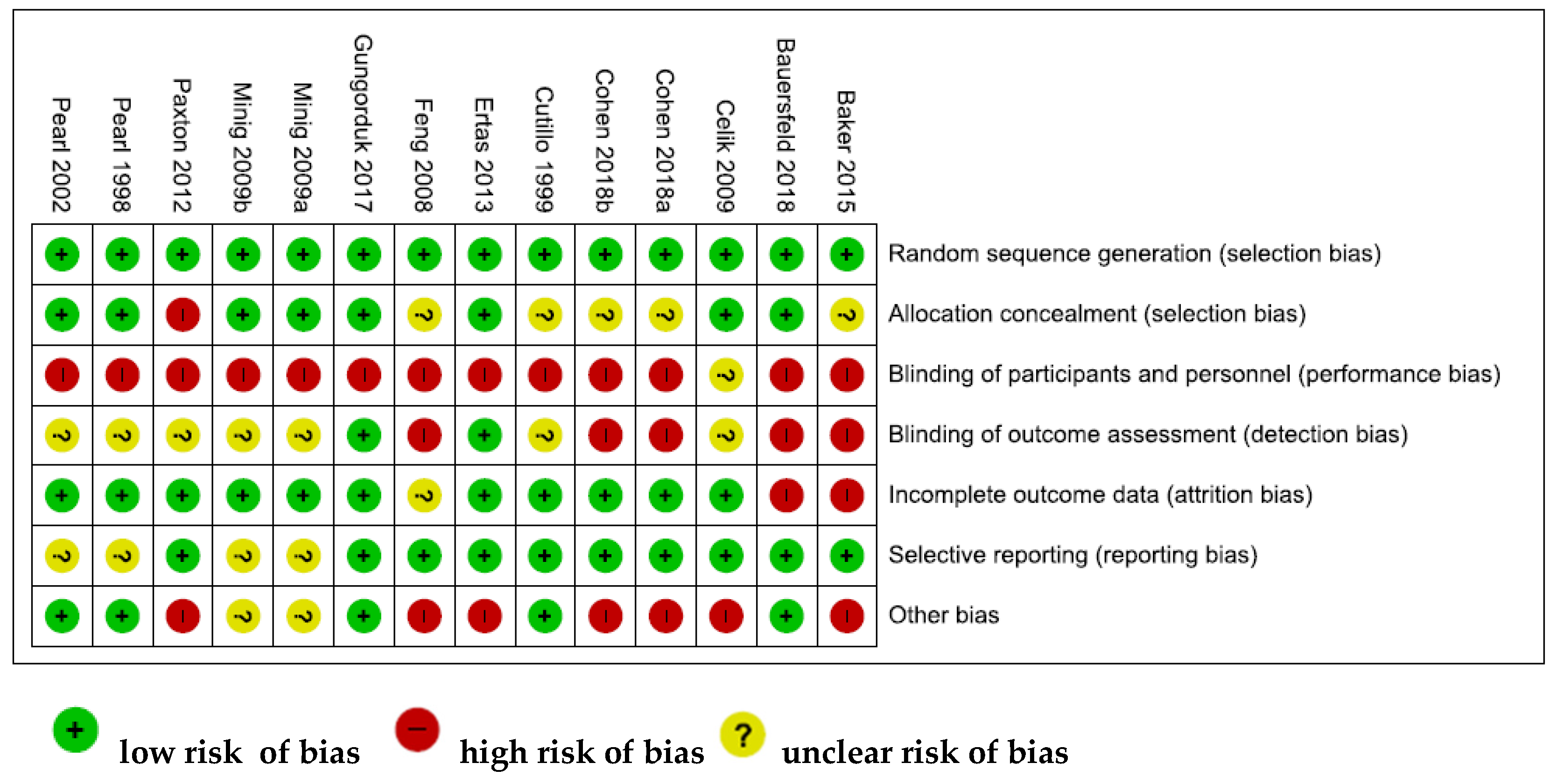
3.3. Study Quality Assessment
3.4. Summary of Findings
3.4.1. Effects of Nutritional Interventions on Overall Survival
3.4.2. Effects of Nutritional Interventions on LOS
3.4.3. Effects of Nutritional Interventions on Postoperative Clinical Outcomes
3.4.4. Effects of Nutritional Interventions on Postoperative Complications
3.4.5. Effects of Nutritional Interventions on Dietary Intake and Anthropometric Measures
3.4.6. Effects of Nutritional Interventions on QoL
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Hunn, J.; Rodriguez, G.C. Ovarian cancer: Etiology, risk factors, and epidemiology. Clin. Obstet. Gynecol. 2012, 55, 3–23. [Google Scholar] [CrossRef]
- Yancik, R. Ovarian cancer. Age contrasts in incidence, histology, disease stage at diagnosis, and mortality. Cancer 1993, 71, 517–523. [Google Scholar] [CrossRef]
- Laky, B.; Janda, M.; Cleghorn, G.; Obermair, A. Comparison of different nutritional assessments and body-composition measurements in detecting malnutrition among gynecologic cancer patients. Am. J. Clin. Nutr. 2008, 87, 1678–1685. [Google Scholar] [CrossRef]
- Yim, G.W.; Eoh, K.J.; Kim, S.W.; Nam, E.J.; Kim, Y.T. Malnutrition identified by the nutritional risk index and poor prognosis in advanced epithelial ovarian carcinoma. Nutr. Cancer 2016, 68, 772–779. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Arends, J. The causes and consequences of cancer-associated malnutrition. Eur. J. Oncol. Nurs. 2005, 9, S51–S63. [Google Scholar] [CrossRef]
- Read, J.A.; Beale, P.J.; Volker, D.H.; Smith, N.; Childs, A.; Clarke, S.J. Nutrition intervention using an eicosapentaenoic acid (EPA)-containing supplement in patients with advanced colorectal cancer. Effects on nutritional and inflammatory status: A phase II trial. Support Care. Cancer 2017, 15, 301–307. [Google Scholar] [CrossRef]
- Hertlein, L.; Kirschenhofer, A.; Fürst, S.; Beer, D.; Göß, C.; Lenhard, M.; Friese, K.; Burges, A.; Rittler, P. Malnutrition and clinical outcome in gynecologic patients. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 174, 137–140. [Google Scholar] [CrossRef]
- Geisler, J.P.; Linnemeier, G.C.; Thomas, A.J.; Manahan, K.J. Nutritional assessment using prealbumin as an objective criterion to determine whom should not undergo primary radical cytoreductive surgery for ovarian cancer. Gynecol. Oncol. 2007, 106, 128–131. [Google Scholar] [CrossRef]
- Kathiresan, A.S.; Brookfield, K.F.; Schuman, S.I.; Lucci, J.A., 3rd. Malnutrition as a predictor of poor postoperative outcomes in gynecologic cancer patients. Arch. Gynecol. Obstet. 2011, 284, 445–451. [Google Scholar] [CrossRef]
- Gupta, D.; Lis, C.G.; Vashi, P.G.; Lammersfeld, C.A. Impact of improved nutritional status on survival in ovarian cancer. Support Care. Cancer 2010, 18, 373–381. [Google Scholar] [CrossRef]
- Uccella, S.; Mele, M.C.; Quagliozzi, L.; Rinninella, E.; Nero, C.; Cappuccio, S.; Cintoni, M.; Gasbarrini, A.; Scambia, G.; Fagotti, A. Assessment of preoperative nutritional status using BIA-derived phase angle (PhA) in patients with advanced ovarian cancer: Correlation with the extent of cytoreduction and complications. Gynecol. Oncol. 2018, 149, 263–269. [Google Scholar] [CrossRef]
- Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. Available online: www.cochrane-handbook.org (accessed on 4 February 2019).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339. [Google Scholar] [CrossRef]
- Pearl, M.L.; Valea, F.A.; Fischer, M.; Mahler, L.; Chalas, E. A randomized controlled trial of early postoperative feeding in gynecologic oncology patients undergoing intra-abdominal surgery. Obstet. Gynecol. 1998, 92, 94–97. [Google Scholar] [CrossRef]
- Cutillo, G.; Maneschi, F.; Franchi, M.; Giannice, R.; Scambia, G.; Benedetti-Panici, P. Early feeding compared with nasogastric decompression after major oncologic gynecologic surgery: A randomized study. Obstet. Gynecol. 1999, 93, 41–45. [Google Scholar] [CrossRef]
- Pearl, M.L.; Frandina, M.; Mahler, L.; Valea, F.A.; Di Silvestro, P.A.; Chalas, E. A randomized controlled trial of a regular diet as the first meal in gynecologic oncology patients undergoing intraabdominal surgery. Obstet. Gynecol. 2002, 100, 230–234. [Google Scholar]
- Feng, S.; Chen, L.; Wang, G.; Chen, A.; Qiu, Y. Early oral intake after intra-abdominal gynecological oncology surgery. Cancer Nurs. 2008, 31, 209–213. [Google Scholar] [CrossRef]
- Celik, J.B.; Gezginc, K.; Ozcelik, K.; Celik, C. The role of immunonutrition in gynecologic oncologic surgery. Eur. J. Gynaecol. Oncol. 2009, 30, 418–421. [Google Scholar]
- Minig, L.; Biffi, R.; Zanagnolo, V.; Attanasio, A.; Beltrami, C.; Bocciolone, L.; Botteri, E.; Colombo, N.; Iodice, S.; Landoni, F.; et al. Early oral versus “traditional” postoperative feeding in gynecologic oncology patients undergoing intestinal resection: A randomized controlled trial. Ann. Surg. Oncol. 2009, 16, 1660–1668. [Google Scholar] [CrossRef]
- Minig, L.; Biffi, R.; Zanagnolo, V.; Attanasio, A.; Beltrami, C.; Bocciolone, L.; Botteri, E.; Colombo, N.; Iodice, S.; Landoni, F.; et al. Reduction of postoperative complication rate with the use of early oral feeding in gynecologic oncologic patients undergoing a major surgery: A randomized controlled trial. Ann. Surg. Oncol. 2009, 16, 3101–3110. [Google Scholar] [CrossRef]
- Ertas, I.E.; Gungorduk, K.; Ozdemir, A.; Solmaz, U.; Dogan, A.; Yildirim, Y. Influence of gum chewing on postoperative bowel activity after complete staging surgery for gynecological malignancies: A randomized controlled trial. Gynecol. Oncol. 2013, 131, 118–122. [Google Scholar] [CrossRef]
- Baker, J.; Janda, M.; Graves, N.; Bauer, J.; Banks, M.; Garrett, A.; Chetty, N.; Crandon, A.J.; Land, R.; Nascimento, M.; et al. Quality of life after early enteral feeding versus standard care for proven or suspected advanced epithelial ovarian cancer: Results from a randomised trial. Gynecol. Oncol. 2015, 137, 516–522. [Google Scholar] [CrossRef] [Green Version]
- Güngördük, K.; Özdemir, İ.A.; Güngördük, Ö.; Gülseren, V.; Gokçü, M.; Sancı, M. Effects of coffee consumption on gut recovery after surgery of gynecological cancer patients: A randomized controlled trial. Am. J. Obstet. Gynecol. 2017, 216, e1–e145. [Google Scholar] [CrossRef]
- Bauersfeld, S.P.; Kessler, C.S.; Wischnewsky, M.; Jaensch, A.; Steckhan, N.; Stange, R.; Kunz, B.; Brückner, B.; Sehouli, J.; Michalsen, A. The effects of short-term fasting on quality of life and tolerance to chemotherapy in patients with breast and ovarian cancer: A randomized cross-over pilot study. BMC Cancer 2018, 18, 476. [Google Scholar] [CrossRef]
- Cohen, C.W.; Fontaine, K.R.; Arend, R.C.; Alvarez, R.D.; Leath, C.A.; Huh, W.K.; Bevis, K.S.; Kim, K.H.; Straughn, J.M., Jr.; Gower, B.A. A Ketogenic Diet Reduces Central Obesity and Serum Insulin in Women with Ovarian or Endometrial Cancer. J. Nutr. 2018, 148, 1253–1260. [Google Scholar] [CrossRef]
- Cohen, C.W.; Fontaine, K.R.; Arend, R.C.; Soleymani, T.; Gower, B.A. Favorable Effects of a Ketogenic Diet on Physical Function, Perceived Energy, and Food Cravings in Women with Ovarian or Endometrial Cancer: A Randomized, Controlled Trial. Nutrients 2018, 10, 1187. [Google Scholar] [CrossRef]
- Paxton, R.J.; Garcia-Prieto, C.; Berglund, M.; Hernandez, M.; Hajek, R.A.; Handy, B.; Brown, J.; Jones, L.A. A randomized parallel-group dietary study for stages II-IV ovarian cancer survivors. Gynecol. Oncol. 2012, 124, 410–416. [Google Scholar] [CrossRef]
- Andreyev, H.J.; Norman, A.R.; Oates, J.; Cunningham, D. Why do patients with weight loss have a worse outcome when undergoing chemotherapy for gastrointestinal malignancies? Eur. J. Cancer 1998, 34, 503–509. [Google Scholar] [CrossRef]
- Triarico, S.; Rinninella, E.; Cintoni, M.; Capozza, M.A.; Mastrangelo, S.; Mele, M.C.; Ruggiero, A. Impact of malnutrition on survival and infections among pediatric patients with cancer: A retrospective study. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1165–1175. [Google Scholar] [CrossRef]
- Rinninella, E.; Cintoni, M.; De Lorenzo, A.; Addolorato, G.; Vassallo, G.; Moroni, R.; Miggiano, G.A.D.; Gasbarrini, A.; Mele, M.C. Risk, prevalence, and impact of hospital malnutrition in a Tertiary Care Referral University Hospital: A cross-sectional study. Intern. Emerg. Med. 2018, 13, 689–697. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Rossi Fanelli, F.; Molfino, A. Perspectives of health care professionals on cancer cachexia: Results from three global surveys. Ann. Oncol. 2016, 27, 2230–2236. [Google Scholar] [CrossRef]
- Laviano, A.; Di Lazzaro, L.; Koverech, A. Nutrition support and clinical outcome in advanced cancer patients. Proc. Nutr. Soc. 2018, 77, 388–393. [Google Scholar] [CrossRef] [Green Version]
- Uccella, S.; Mariani, A.; Wang, A.H.; Vierkant, R.A.; Cliby, W.A.; Robien, K.; Anderson, K.E.; Cerhan, J.R. Intake of coffee, caffeine and other methylxanthines and risk of Type I vs. Type II endometrial cancer. Br. J. Cancer 2013, 109, 1908–1913. [Google Scholar] [CrossRef]
- Uccella, S.; Mariani, A.; Wang, A.H.; Vierkant, R.A.; Robien, K.; Anderson, K.E.; Cerhan, J.R. Dietary and supplemental intake of one-carbon nutrients and the risk of type I and type II endometrial cancer: A prospective cohort study. Ann. Oncol. 2011, 22, 2129–2136. [Google Scholar] [CrossRef]
- Billson, H.A.; Holland, C.; Curwell, J.; Davey, V.L.; Kinsey, L.; Lawton, L.J.; Whitworth, A.J.; Burden, S. Perioperative nutrition interventions for women with ovarian cancer. Cochrane Database Syst. Rev. 2013, 9, CD009884. [Google Scholar] [CrossRef]
- Longo, V.D.; Mattson, M.P. Fasting: Molecular mechanisms and clinical applications. Cell Metab. 2014, 19, 181–192. [Google Scholar] [CrossRef]
- Safdie, F.; Brandhorst, S.; Wei, M.; Wang, W.; Lee, C.; Hwang, S.; Conti, P.S.; Chen, T.C.; Longo, V.D. Fasting enhances the response of glioma to chemo- and radiotherapy. PLoS One 2012, 7, e44603. [Google Scholar] [CrossRef]
- Vernieri, C.; Signorelli, D.; Galli, G.; Ganzinelli, M.; Moro, M.; Fabbri, A.; Tamborini, E.; Marabese, M.; Caiola, E.; Broggini, M.; et al. Exploiting FAsting-mimicking Diet and MEtformin to Improve the Efficacy of Platinum-pemetrexed Chemotherapy in Advanced LKB1-inactivated Lung Adenocarcinoma: The FAME Trial. Clin. Lung Cancer 2018, 18, 30335–30338. [Google Scholar] [CrossRef]
- Wallace, T.C.; Bultman, S.; D’Adamo, C.; Daniel, C.R.; Debelius, J.; Ho, E.; Eliassen, H.; Lemanne, D.; Mukherjee, P.; Seyfried, T.N.; et al. Personalized Nutrition in Disrupting Cancer—Proceedings From the 2017 American College of Nutrition Annual Meeting. J. Am. Coll. Nutr. 2019, 38, 1–14. [Google Scholar] [CrossRef]
- ClinicalTrials.gov Identifier: NCT02126449. US National library of Medicine. Available online: https://clinicaltrials.gov/ct2/show/NCT02126449 (accessed on 1 December 2018).
- ClinicalTrials.gov Identifier: NCT03340935. US National library of Medicine. Available online: https://clinicaltrials.gov/ct2/show/NCT03340935 (accessed on 1 December 2018).
- ClinicalTrials.gov Identifier: NCT03454282. US National library of Medicine. Available online: https://clinicaltrials.gov/ct2/show/NCT03454282 (accessed on 1 December 2018).
- ClinicalTrials.gov Identifier: NCT03595540. US National library of Medicine. Available online: https://clinicaltrials.gov/ct2/show/NCT03595540 (accessed on 1 December 2018).
- ClinicalTrials.gov Identifier: NCT03700437. US National library of Medicine. Available online: https://clinicaltrials.gov/ct2/show/NCT03700437 (accessed on 1 December 2018).
- ClinicalTrials.gov Identifier: NCT03709147. US National library of Medicine. Available online: https://clinicaltrials.gov/ct2/show/NCT03709147 (accessed on 1 December 2018).
- ClinicalTrials.gov Identifier: NCT03811587. US National library of Medicine. Available online: https://clinicaltrials.gov/ct2/show/NCT03811587 (accessed on 1 December 2018).
- Caccialanza, R.; Aprile, G.; Cereda, E.; Pedrazzoli, P. Fasting in oncology: A word of caution. Nat. Rev. Cancer 2019. [Google Scholar] [CrossRef]
- Caccialanza, R.; Pedrazzoli, P.; Cereda, E.; Gavazzi, C.; Pinto, C.; Paccagnella, A.; Beretta, G.D.; Nardi, M.; Laviano, A.; Zagonel, V. Nutritional Support in Cancer Patients: A Position Paper from the Italian Society of Medical Oncology (AIOM) and the Italian Society of Artificial Nutrition and Metabolism (SINPE). J. Cancer 2016, 7, 131–135. [Google Scholar] [CrossRef]
- Caccialanza, R.; Cereda, E.; De Lorenzo, F.; Farina, G.; Pedrazzoli, P.; AIOM-SINPE-FAVO Working Group. To fast, or not to fast before chemotherapy, that is the question. BMC Cancer 2018, 18, 337. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| MEDLINE | |
|---|---|
| Set | Search Terms |
| 1 | diet*[TextWord] OR diet therapy[MeSHTerms] OR therapy nutrition[MeSHTerms] OR eat*[TextWord] OR food*[TextWord] OR feed*[TextWord] OR meal*[TextWord] OR nutriment*[TextWord] or nutritional advice*[TextWord] OR nutritional counseling*[TextWord] OR nutritional support*[TextWord] OR nutritional intervention*[TextWord] |
| 2 | ovar* [TextWord] OR ovary [MeSHTerms] |
| 3 | cancer*[TextWord] OR oncology[TextWord] OR tumour*[TextWord] OR tumor*[TextWord] OR malignan*[TextWord] OR carcinoma[TextWord] OR neoplasm*[TextWord] |
| 4 | 2 AND 3 |
| 5 | 1 AND 4 |
| 6 | 5 and Refined by: Publication Type: “Randomized Controlled Trial” |
| 7 | 6 and Refined by: Subjects: “Humans” |
| WEB OF SCIENCE | |
| Set | Search Terms |
| 1 | Topic: (diet* OR eat* OR food* OR feed* OR meal* OR nutriment* or nutritional advice* OR nutritional therapy* OR nutritional support* OR nutritional intervention*) |
| 2 | Topic: (Ovarian OR Ovary) |
| 3 | Topic: (cancer* OR oncology OR tumour* OR tumor* OR malignan* OR carcinoma OR neoplasm*) |
| 4 | 1 AND 2 AND 3 |
| 5 | #4 AND Refined by: Topic: (randomised controlled trial* OR randomised controlled clinical trial* OR randomised controlled study OR randomised controlled clinical study OR randomized controlled trial* OR randomized controlled clinical trial* OR randomized controlled stud* OR randomized controlled clinical stud* OR randomised-controlled trial* OR randomised-controlled clinical trial* OR randomised-controlled study OR randomised-controlled clinical study OR randomized-controlled trial* OR randomized-controlled clinical trial* OR randomized-controlled stud* OR randomized-controlled clinical stud*) |
| COCHRANE | |
| Set | Search Terms |
| 1 | Title Abstract Keyword: diet* OR eat* OR food* OR feed* OR meal* OR nutriment* or nutritional advice* OR nutritional therapy* OR nutritional support* OR nutritional intervention* |
| 2 | Title Abstract Keyword: ovarian OR ovary |
| 3 | Title Abstract Keyword: cancer* OR oncology OR tumour* OR tumor* OR malignan* OR carcinoma OR neoplasm* |
| 4 | 1 AND 2 AND 3 |
| Study ID | Study Design | Cancer Types with % Ovarian Cancer | Sample Size | Time of Intervention | Type of Nutritional Intervention | Comparison | Outcomes Measures | Results |
|---|---|---|---|---|---|---|---|---|
| Pearl et al. 1998 [15] | RCT | Ovarian (32.3%), cervical, uterine and benign cancers | n = 195 | Post-operation on the first postoperative day | EOF: Clear liquid diet | TOF: Nothing by mouth until bowel sounds, the passage of stool or flatus |
| -No significant differences between the two groups in:
-Significantly reduction in the EOF group of:
|
| Cutillo et al. 1999 [16] | RCT with parallel arm design | Ovarian (48.3%) and other gynecologic cancers | n = 122 | Post-operation on the first postoperative day | EOF: Clear-fluid diet, passing to a semiliquid fiberless diet within the next 24 h | Nasogastric decompression followed by feeding at the first passage of flatus |
| -No significant differences between the two groups in incidence of nausea and vomiting. -Significant reduction in the EOF group of:
|
| Pearl et al. 2002 [17] | RCT | Ovarian (33%), cervical, uterine and benign cancers | n = 245 | Post-operation on the first postoperative day | EOF: Regular diet | EOF: Clear liquid diet |
| -No significant differences between the two groups in:
|
| Feng et al. 2008 [18] | RCT | Ovarian (18.3%) and other gynecologic cancers | n = 60 | Post-operation on the first 6 postoperative hours | Semiliquid diet followed by regular diet | Clear-liquid diet tosemiliquid diet toregular diet |
| -Significant reduction (p < 0.05) in clear feeds group of:
|
| Celik et al. 2009 [19] | RCT with parallel arm design | Ovarian (32%) and other gynecologic cancers | n = 50 | Pre-operation on the last 2 preoperative days post-operation on the first 7 postoperative days | IEN | Standardenteral nutrition |
| -No significant differences between the two groups in:
|
| Minig et al. 2009a [20] | RCT | Ovarian cancer (87.5%) | n = 40 | Post-operation during the first 24 postoperative hours | EOF: Clear liquid diet | TOF: Nothing by mouth until the resumption of normal bowel function |
| -Significant reduction of LOS (p = 0.022) in EOF group vs TOF group. -No significant differences between both groups in:
|
| Minig et al. 2009b [21] | RCT | Ovarian (58%), endometrial, cervix and other cancers | n = 143 | Post-operation during the first 24 postoperative hours | EOF: Clear liquid diet | TOF: Nothing by mouth until the resumption of normal bowel function |
| -Significant reduction of LOS in the EOF group (p = 0.006). -Significant higher overall postoperative (p = 0.003) and infective complications (p = 0.017) in the TOF group compared to the EOF group. -Significant higher mean level of postoperative satisfaction (p < 0.001) in the EOF group. -No differences between both groups in:
|
| Ertas et al. 2013 [22] | RCT | Ovarian (36.9%), endometrial and cervix cancers | n = 149 | Post-operation on the first postoperative morning until the first passage of flatus | Chewing-gum 3 times/day | Control |
| -Significant reduction (p < 0.001) in patients who chewed gum compared to controls of:
|
| Baker et al. 2015 [23] | RCT | Ovarian cancer (100%) | n = 109 | Post-operationon the first postoperative day | Early enteral feeding: standard fiber (20P:30F:50C) 125 kJ/kg body weight.Until adequate oral intake could be maintained: 65–75% of the daily nutritional requirements. | Standard oral diet |
| -No significant differences between both groups in:
|
| Güngördüket al. 2017 [24] | RCT | Ovarian (39.5%), endometrial, cervical and fallopian cancers | n = 114 | Post-operationon the first morning after surgery | 3 cups of caffeinated coffee daily (100 mL at 10:00 AM, 3:00 PM and /:00 PM) | Routine care without coffee consumption |
| -Significant reduction (p < 0.001) in patients who consumed coffee compared with controls in:
|
| Bauersfeld et al. 2018 [25] | RCT with cross-over design | Ovarian (11.7%) and breast cancers | n = 34 | During CT | Group ASTF* of 60 h (36 h before to 24 h after CT) during the first three of scheduled 6 CTsthenstandard Mediterranean diet during the last three of scheduled 6 CTs. | Group BStandard Mediterranean diet during the first three of scheduled 6 CTsthenSTF* of 60 h (36 h before to 24 h after CT) during the first three of scheduled 6 CTs |
| -In the group A, significant improvements during fasted periods compared to standard diet in:
|
| Cohen et al. 2018 [26] | RCT | Ovarian (62.2%) and endometrial cancers | n = 45 | During (n = 11) or post-CT | KD diet (70:25:5 energy from fat, protein, and carbohydrate) | ACS diet: high fiber, lower fat |
| -Significant reduction in the KD group compared to the ACS group of:
|
| Cohen et al. 2018 [27] | RCT with parallel arm design | Ovarian (62.2%) and endometrial cancers | n = 45 | During CT (n = 11) or post-CT | KD diet (70:25:5 energy from fat, protein, and carbohydrate) | ACS diet: moderate- to high-carbohydrate, high fiber, low fat |
| -No significant differences between both groups in
|
| Paxton et al. 2012 [28] | RCT with parallel arm design | Ovarian cancer (100%) | n = 52 | Post-CT≥6 months | LFHF group | FVJC group |
| -Significant improvements in both groups (p < 0.01) in:
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rinninella, E.; Fagotti, A.; Cintoni, M.; Raoul, P.; Scaletta, G.; Quagliozzi, L.; Miggiano, G.A.D.; Scambia, G.; Gasbarrini, A.; Mele, M.C. Nutritional Interventions to Improve Clinical Outcomes in Ovarian Cancer: A Systematic Review of Randomized Controlled Trials. Nutrients 2019, 11, 1404. https://doi.org/10.3390/nu11061404
Rinninella E, Fagotti A, Cintoni M, Raoul P, Scaletta G, Quagliozzi L, Miggiano GAD, Scambia G, Gasbarrini A, Mele MC. Nutritional Interventions to Improve Clinical Outcomes in Ovarian Cancer: A Systematic Review of Randomized Controlled Trials. Nutrients. 2019; 11(6):1404. https://doi.org/10.3390/nu11061404
Chicago/Turabian StyleRinninella, Emanuele, Anna Fagotti, Marco Cintoni, Pauline Raoul, Giuseppe Scaletta, Lorena Quagliozzi, Giacinto Abele Donato Miggiano, Giovanni Scambia, Antonio Gasbarrini, and Maria Cristina Mele. 2019. "Nutritional Interventions to Improve Clinical Outcomes in Ovarian Cancer: A Systematic Review of Randomized Controlled Trials" Nutrients 11, no. 6: 1404. https://doi.org/10.3390/nu11061404
APA StyleRinninella, E., Fagotti, A., Cintoni, M., Raoul, P., Scaletta, G., Quagliozzi, L., Miggiano, G. A. D., Scambia, G., Gasbarrini, A., & Mele, M. C. (2019). Nutritional Interventions to Improve Clinical Outcomes in Ovarian Cancer: A Systematic Review of Randomized Controlled Trials. Nutrients, 11(6), 1404. https://doi.org/10.3390/nu11061404