Mindful Eating and Active Living: Development and Implementation of a Multidisciplinary Pediatric Weight Management Intervention


Abstract
:1. Introduction
2. Description of MEALs Using the TIDieR Checklist
2.1. BRIEF NAME: Provide the Name or a Phrase that Describes the Intervention
2.2. WHY: Describe Any Rationale, Theory, or Goal of the Elements Essential to the Intervention
2.3. WHAT: Describe Materials and Procedures
2.4. WHO PROVIDED: Describe the Expertise, Background, and Specific Training Given to Each Category of Intervention Provider
2.5. HOW: Describe the Modes of Delivery of the Intervention
2.6. WHERE: Describe the Type(s) of Location(s) Where the Intervention Occurred, Including Any Necessary Infrastructure or Relevant Features
2.7. WHEN and HOW MUCH: Describe the Number of Times the Intervention Was Delivered and over What Period of Time
2.8. TAILORING: If the Intervention Was Planned to Be Personalized, Titrated or Adapted, then Describe What, Why, When, and How
2.9. MODIFICATIONS: If the Intervention Was Modified during the Course of the Study, Describe the Changes (What, Why, When, and How)
2.10. HOW WELL: Planned and Actual Fidelity to the Intervention
3. Discussion
3.1. Modifications and Suggestions Based on Lessons Learned
3.1.1. Costs and Resources
3.1.2. Balanced Approachability of Recipes
3.1.3. Engagement of the Dyad
3.1.4. Group Support and Discussion
3.1.5. Personnel Concerns
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ogden, C.L.; Carroll, M.D.; Lawman, H.G.; Fryar, C.D.; Kruszon-Moran, D.; Kit, B.K.; Flegal, K.M. Trends in Obesity Prevalence Among Children and Adolescents in the United States, 1988–1994 Through 2013–2014. JAMA 2016, 315, 2292–2299. [Google Scholar] [CrossRef] [PubMed]
- Daniels, S.R. The consequences of childhood overweight and obesity. Future Child 2006, 16, 47–67. [Google Scholar] [CrossRef] [PubMed]
- Pulgaron, E.R. Childhood obesity: A review of increased risk for physical and psychological comorbidities. Clin. Ther. 2013, 35, A18–A32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skinner, A.C.; Ravanbakht, S.N.; Skelton, J.A.; Perrin, E.M.; Armstrong, S.C. Prevalence of Obesity and Severe Obesity in US Children, 1999–2016. Pediatrics 2018, 141, e20173459. [Google Scholar] [CrossRef] [Green Version]
- Grossman, D.C.; Bibbins-Domingo, K.; Curry, S.J.; Barry, M.J.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W.; Kemper, A.R.; Krist, A.H.; Kurth, A.E. Screening for obesity in children and adolescents: US Preventive Services Task Force recommendation statement. JAMA 2017, 317, 2417–2426. [Google Scholar]
- Brennan, L.K.; Brownson, R.C.; Orleans, C.T. Childhood obesity policy research and practice: Evidence for policy and environmental strategies. Am. J. Prev. Med. 2014, 46, e1–e16. [Google Scholar] [CrossRef] [Green Version]
- Skelton, J.; Beech, B. Attrition in paediatric weight management: A review of the literature and new directions. Obes. Rev. 2011, 12, e273–e281. [Google Scholar] [CrossRef]
- Kamath, C.C.; Vickers, K.S.; Ehrlich, A.; McGovern, L.; Johnson, J.; Singhal, V.; Paulo, R.; Hettinger, A.; Erwin, P.J.; Montori, V.M. Clinical review: Behavioral interventions to prevent childhood obesity: A systematic review and metaanalyses of randomized trials. J. Clin Endocrinol. Metab. 2008, 93, 4606–4615. [Google Scholar] [CrossRef] [Green Version]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of obesity and trends in body mass index among US children and adolescents, 1999–2010. JAMA 2012, 307, 483–490. [Google Scholar] [CrossRef] [Green Version]
- Skinner, A.C.; Perrin, E.M.; Skelton, J.A. Prevalence of Obesity and Severe Obesity in US Children, 1999–2014. Obesity 2016, 24, 1116–1123. [Google Scholar] [CrossRef] [Green Version]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2014, 311, 806–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cameron, A.J.; Spence, A.C.; Laws, R.; Hesketh, K.D.; Lioret, S.; Campbell, K.J. A review of the relationship between socioeconomic position and the early-life predictors of obesity. Curr. Obes. Rep. 2015, 4, 350–362. [Google Scholar] [CrossRef] [PubMed]
- Beech, B.M.; Fitzgibbon, M.L.; Resnicow, K.; Whitt-Glover, M.C. The impact of socioeconomic factors and the built environment on childhood and adolescent obesity. Child. Obes. 2011, 7, 19–24. [Google Scholar] [CrossRef]
- Wilson, D.K. New perspectives on health disparities and obesity interventions in youth. J. Pediatric Psychol. 2009, 34, 231–244. [Google Scholar] [CrossRef]
- Beech, B.M.; Bruce, M.A.; Thorpe, R. Pediatric Obesity Risk Factors among African American Youth. Obes. Child. Adolesc. 2018, 2, 179. [Google Scholar]
- Kumanyika, S.K. Environmental influences on childhood obesity: Ethnic and cultural influences in context. Physiol. Behav. 2008, 94, 61–70. [Google Scholar] [CrossRef]
- Hersch, D.; Perdue, L.; Ambroz, T.; Boucher, J.L. Peer reviewed: The impact of cooking classes on food-related preferences, attitudes, and behaviors of school-aged children: A systematic review of the evidence, 2003–2014. Prev. Chronic Dis. 2014, 11. [Google Scholar]
- Robson, S.M.; Stough, C.O.; Stark, L.J. The impact of a pilot cooking intervention for parent-child dyads on the consumption of foods prepared away from home. Appetite 2016, 99, 177–184. [Google Scholar] [CrossRef]
- Kyrou, I.; Tsigos, C. Stress hormones: Physiological stress and regulation of metabolism. Curr. Opin. Pharm. 2009, 9, 787–793. [Google Scholar] [CrossRef]
- Katterman, S.N.; Kleinman, B.M.; Hood, M.M.; Nackers, L.M.; Corsica, J.A. Mindfulness meditation as an intervention for binge eating, emotional eating, and weight loss: A systematic review. Eat. Behav. 2014, 15, 197–204. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Lawlor, M.S.; Schonert-Reichl, K.A.; Gadermann, A.M.; Zumbo, B.D. A validation study of the mindful attention awareness scale adapted for children. Mindfulness 2014, 5, 730–741. [Google Scholar] [CrossRef]
- Grossman, P.; Niemann, L.; Schmidt, S.; Walach, H. Mindfulness-based stress reduction and health benefits: A meta-analysis. J. Psychosom. Res. 2004, 57, 35–43. [Google Scholar] [CrossRef]
- Gainey, A.; Himathongkam, T.; Tanaka, H.; Suksom, D. Effects of Buddhist walking meditation on glycemic control and vascular function in patients with type 2 diabetes. Complement. Ther. Med. 2016, 26, 92–97. [Google Scholar] [CrossRef]
- Shomaker, L.B.; Bruggink, S.; Pivarunas, B.; Skoranski, A.; Foss, J.; Chaffin, E.; Dalager, S.; Annameier, S.; Quaglia, J.; Brown, K.W. Pilot randomized controlled trial of a mindfulness-based group intervention in adolescent girls at risk for type 2 diabetes with depressive symptoms. Complement. Ther. Med. 2017, 32, 66–74. [Google Scholar] [CrossRef]
- Dallman, M.F. Stress-induced obesity and the emotional nervous system. Trends Endocrinol. Metab. 2010, 21, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Ludwig, D.S.; Kabat-Zinn, J. Mindfulness in medicine. JAMA 2008, 300, 1350–1352. [Google Scholar] [CrossRef]
- Cotterill, S.; Knowles, S.; Martindale, A.-M.; Elvey, R.; Howard, S.; Coupe, N.; Wilson, P.; Spence, M. Getting messier with TIDieR: Embracing context and complexity in intervention reporting. BMC Med. Res. Methodol. 2018, 18, 12. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomized trials. Ann. Intern. Med. 2010, 152, 726–732. [Google Scholar] [CrossRef] [Green Version]
- Pluhar, E.I.; Kamody, R.C.; Sanchez, J.; Thurston, I.B.; Burton, T.E. Description of an intervention to treat binge-eating behaviors among adolescents: Applying the Template for Intervention Descriptions and Replication. Int. J. Eat Disord. 2018, 51, 1128–1133. [Google Scholar] [CrossRef] [PubMed]
- Bartholomew, L.K.; Parcel, G.S.; Kok, G. Intervention mapping: A process for developing theory and evidence-based health education programs. Health Educ. Behav. 1998, 25, 545–563. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the public health impact of health promotion interventions: The RE-AIM framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, S.A.; Garrett, K.E. The use of logic models by community-based initiatives. Eval. Program Plan. 2005, 28, 167–172. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.-W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jerić, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A. SPIRIT 2013 statement: Defining standard protocol items for clinical trials. Ann. Intern. Med. 2013, 158, 200–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burton, E.T.; Smith, W.A.; Thurston, I.B.; Gray, E.; Perry, V.; Jogal, S.; Han, J.C. Interdisciplinary Management of Pediatric Obesity: Lessons Learned in the Midsouth. Clin. Pediatrics 2018, 57, 509–518. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Design and Nature; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An ecological perspective on health promotion programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef]
- Ohri-Vachaspati, P.; DeLia, D.; DeWeese, R.S.; Crespo, N.C.; Todd, M.; Yedidia, M.J. The relative contribution of layers of the Social Ecological Model to childhood obesity. Public Health Nutr. 2015, 18, 2055–2066. [Google Scholar] [CrossRef] [Green Version]
- van der Horst, K.; Ferrage, A.; Rytz, A. Involving children in meal preparation. Effects on food intake. Appetite 2014, 79, 18–24. [Google Scholar] [CrossRef]
- Fulkerson, J.A.; Rydell, S.; Kubik, M.Y.; Lytle, L.; Boutelle, K.; Story, M.; Neumark-Sztainer, D.; Dudovitz, B.; Garwick, A. Healthy Home Offerings via the Mealtime Environment (HOME): Feasibility, acceptability, and outcomes of a pilot study. Obesity 2010, 18, S69–S74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilfley, D.E.; Saelens, B.E.; Stein, R.I.; Best, J.R.; Kolko, R.P.; Schechtman, K.B.; Wallendorf, M.; Welch, R.R.; Perri, M.G.; Epstein, L.H. Dose, content, and mediators of family-based treatment for childhood obesity: A multisite randomized clinical trial. JAMA Pediatrics 2017, 171, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social cognitive theory: An agentic perspective. Annu. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Resnicow, K.; Davis-Hearn, M.; Smith, M.; Baranowski, T.; Lin, L.S.; Baranowski, J.; Doyle, C.; Wang, D.T. Social-cognitive predictors of fruit and vegetable intake in children. Health Psychol. 1997, 16, 272. [Google Scholar] [CrossRef]
- Anderson, E.S.; Winett, R.A.; Wojcik, J.R. Social-cognitive determinants of nutrition behavior among supermarket food shoppers: A structural equation analysis. Health Psychol. 2000, 19, 479. [Google Scholar] [CrossRef]
- Van Dam, N.T.; Earleywine, M.; Borders, A. Measuring mindfulness? An item response theory analysis of the Mindful Attention Awareness Scale. Personal. Individ. Differ. 2010, 49, 805–810. [Google Scholar] [CrossRef]
- Troped, P.J.; Wiecha, J.L.; Fragala, M.S.; Matthews, C.E.; Finkelstein, D.M.; Kim, J.; Peterson, K.E. Reliability and validity of YRBS physical activity items among middle school students. Med. Sci. Sports Exerc. 2007, 39, 416–425. [Google Scholar] [CrossRef]
- Brener, N.D.; Kann, L.; McManus, T.; Kinchen, S.A.; Sundberg, E.C.; Ross, J.G. Reliability of the 1999 youth risk behavior survey questionnaire. J. Adolesc. Health 2002, 31, 336–342. [Google Scholar] [CrossRef]
- Ware, J.E., Jr. SF-36 health survey update. Spine 2000, 25, 3130–3139. [Google Scholar] [CrossRef]
- Varni, J.W.; Burwinkle, T.M.; Seid, M.; Skarr, D. The PedsQL™* 4.0 as a pediatric population health measure: Feasibility, reliability, and validity. Ambul. Pediatrics 2003, 3, 329–341. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. Perceived stress scale. J. Health Soc. Behav. 1993, 24, 385–396. [Google Scholar] [CrossRef]
- Brown, K.W.; West, A.M.; Loverich, T.M.; Biegel, G.M. Assessing adolescent mindfulness: Validation of an Adapted Mindful Attention Awareness Scale in adolescent normative and psychiatric populations. Psychol. Assess. 2011, 23, 1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parfenoff, S.H.; Jose, P.E. Measuring Daily Stress in Children. Paper presented at the Biennial Meeting of the Society for Research in Child Development, Kansas City, MO, USA, 1989. ERIC Document Reproduction Service No. ED314206. [Google Scholar]
- Kabat-Zinn, J.; Hanh, T.N. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Delta: Atlanta, GA, USA, 2009. [Google Scholar]
- Linehan, M. DBT Skills Training Manual, 2nd ed.; Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Seo, D.-C.; Sa, J. A meta-analysis of obesity interventions among US minority children. J. Adolesc. Health 2010, 46, 309–323. [Google Scholar] [CrossRef] [PubMed]
- Barr-Anderson, D.J.; Adams-Wynn, A.W.; DiSantis, K.I.; Kumanyika, S. Family-focused physical activity, diet and obesity interventions in African–American girls: A systematic review. Obes. Rev. 2013, 14, 29–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barr-Anderson, D.; Singleton, C.; Cotwright, C.; Floyd, M.; Affuso, O. Outside-of-school time obesity prevention and treatment interventions in African American youth. Obes. Rev. 2014, 15, 26–45. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Education | Exposure | Experiential | ||
|---|---|---|---|---|
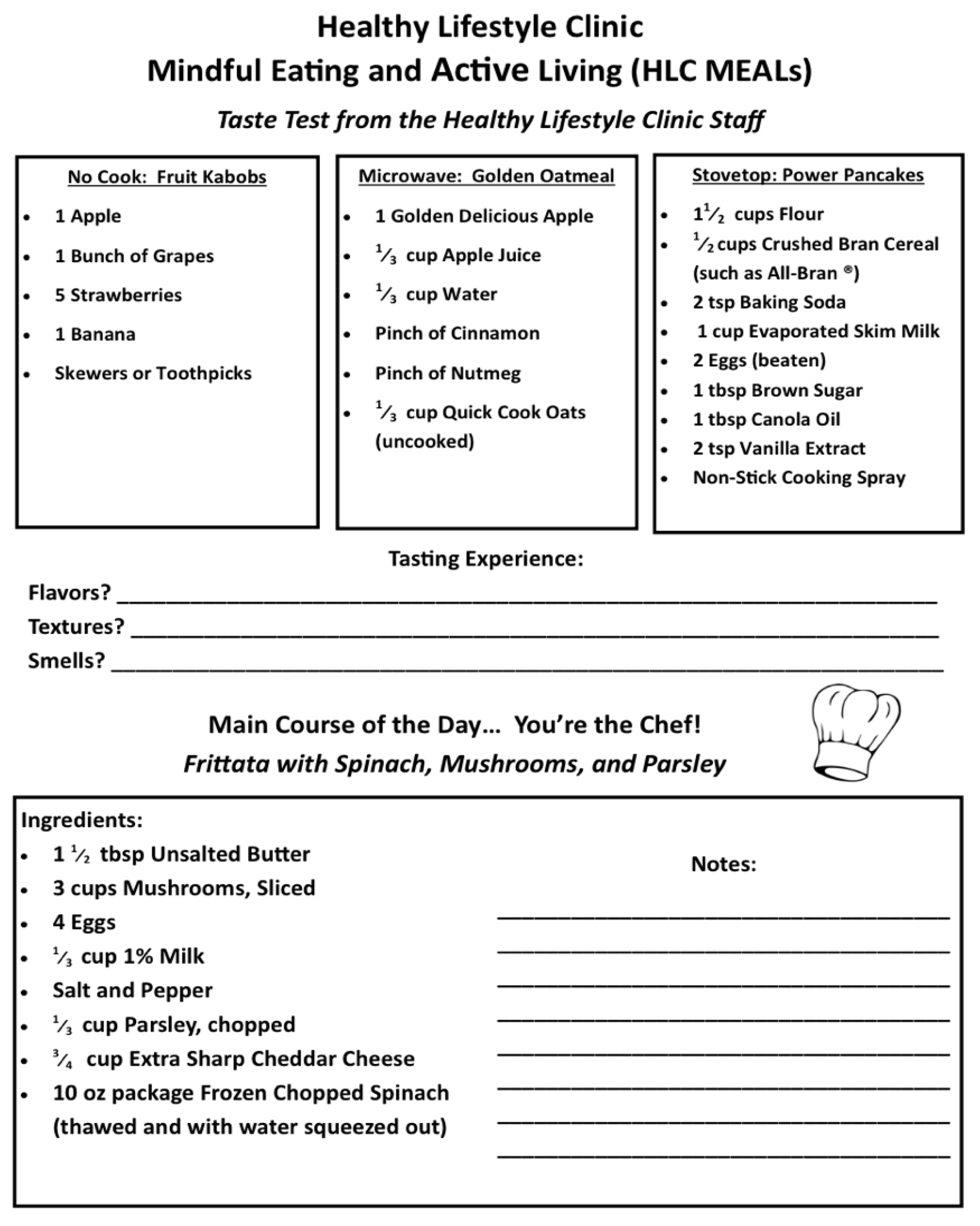
| Session 1: Breakfast | Topic: Behavioral Health
| No Cook | Fruit Kabobs fresh fruit arranged on a skewer | Breakfast Frittata Eggs baked with spinach and mushrooms, garnished with cheese. |
| Microwave | Golden Oatmeal apples, cinnamon, and oats served warm | |||
| Stove/Oven | Power Pancakes fluffy griddle cakes made from bran and whole wheat flour | |||
| Session 2: Lunch | Topic: Nutrition
| No Cook | Peach Banana Freeze blended smoothie of frozen fruit, spinach, and almond milk | Roasted Vegetable Pizza Oven-roasted yellow and zucchini squash on whole wheat flatbread. Served with green salad and participant-prepared vinaigrette. |
| Microwave | Sweet Potato Chips thinly sliced yams crisped in the microwave | |||
| Stove/Oven | Roasted Almonds warmed nuts tossed with rosemary | |||
| Session 3: Dinner | Topic: Exercise
| No Cook | Hummus and Crudités prepared hummus accompanied by carrot and celery sticks | Tuna Cakes Pan seared water-packed tuna patties accompanied by low-sodium French- style green beans from a can and frozen sweet potato fries. For dessert, Greek yogurt-based cheesecake square with berries. |
| Microwave | Beans and Rice black beans mixed with brown rice and tomato salsa | |||
| Stove/Oven | Chicken Taco spiced and grilled chicken breast served on a corn tortilla | |||
| Measurements | Description | Baseline | MEALs Sessions | Post Session Follow up | |||||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 0 Months | 3 Months | 6 Months | ||||
| Participants | Informed Consent | X | |||||||
| Anthropometrics | Height and weight | X | X | X | X | ||||
| Body Composition | Bioelectrical impedance (InBody 770) | X | X | X | X | ||||
| Vital Signs | Heart rate and blood pressure | X | X | X | X | ||||
| Caregiver Surveys | Family Demographic Information | X | X | X | X | ||||
| Mindfulness Attention Awareness Scale (MAAS) [47] | 15-item survey on day to day experiences and awareness | X | X | X | X | ||||
| Attitudes, Knowledge, Behaviors [48,49] | 22 questions about health and lifestyle choices | X | X | X | X | ||||
| SF-36v2 Health Survey [50] | 11- item health-related quality of life survey | X | X | X | X | ||||
| Pediatric Quality of Life Inventory, Parent Report [51] | 23-item caregiver report on child’s health-related quality of life | X | X | X | X | ||||
| Perceived Stress Scale [52] | 10-item appraisal of life situations as stressful | X | X | X | X | ||||
| Youth Surveys | MAAS-Child or Adolescent [22,53] | 15 question survey on day to day experiences and awareness. | X | X | X | X | |||
| Attitudes, Knowledge Behaviors [48,49] | 22 questions about health and lifestyle choices | X | X | X | X | ||||
| Pediatric Quality of Life Inventory, Self Report [51] | 11 question health related quality of life survey | X | X | X | X | ||||
| Hassles Scale for Children [54] | 49-item measure of children’s daily stress | X | X | X | X | ||||
| Post intervention questions | 8 questions about feasibility, and quality improvement | X | |||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burton, E.T.; Smith, W.A. Mindful Eating and Active Living: Development and Implementation of a Multidisciplinary Pediatric Weight Management Intervention. Nutrients 2020, 12, 1425. https://doi.org/10.3390/nu12051425
Burton ET, Smith WA. Mindful Eating and Active Living: Development and Implementation of a Multidisciplinary Pediatric Weight Management Intervention. Nutrients. 2020; 12(5):1425. https://doi.org/10.3390/nu12051425
Chicago/Turabian StyleBurton, E. Thomaseo, and Webb A. Smith. 2020. "Mindful Eating and Active Living: Development and Implementation of a Multidisciplinary Pediatric Weight Management Intervention" Nutrients 12, no. 5: 1425. https://doi.org/10.3390/nu12051425
APA StyleBurton, E. T., & Smith, W. A. (2020). Mindful Eating and Active Living: Development and Implementation of a Multidisciplinary Pediatric Weight Management Intervention. Nutrients, 12(5), 1425. https://doi.org/10.3390/nu12051425