Food Addiction in a Group of Italian Adolescents Diagnosed for Eating Disorder

 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Study Design
2.2. Psychometric Measures
2.2.1. Multidimensional Anxiety Scale for Children 2
2.2.2. Children Depression Inventory 2
2.2.3. Youth Self-Report
2.2.4. Eating Disorder Inventory-3
2.2.5. Eating Attitudes Test–26
2.2.6. Yale Food Addiction Scale 2.0
- No Food Addiction = 1 or fewer symptoms/Does not meet criteria for impairment/distress criteria;
- Mild Food Addiction = 2 or 3 symptoms and impairment/distress criteria;
- Moderate Food Addiction = 4 or 5 symptoms and impairment/distress criteria;
- Severe Food Addiction = 6 or more symptoms and impairment/distress criteria.
2.2.7. Body Uneasiness Test
2.3. Statistical Analysis
2.4. Ethics Approval
3. Results
3.1. Subjects
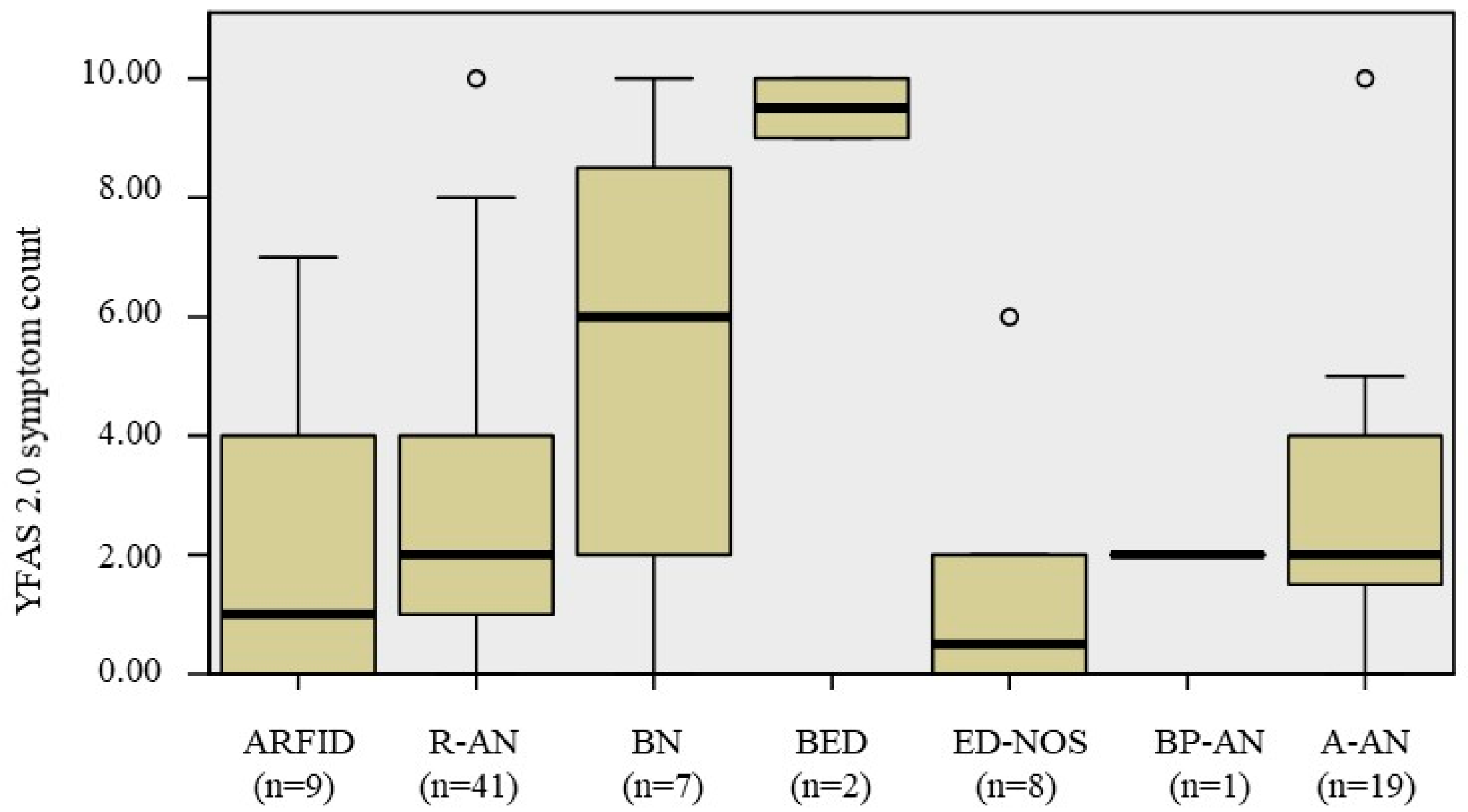
3.2. FA in the Different Subgroups of EDs
3.3. FA and Patients’ Characteristics
3.4. FA and Psychopathology and Eating Pattern
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviation
| A-AN | Atypical Anorexia Nervosa |
| ARFID | Avoidant Restrictive Food Intake Disorder |
| BED | Binge Eating Disorder |
| BMI | Body Mass Index |
| BN | Bulimia Nervosa |
| BP-AN | Binge Purging Anorexia Nervosa |
| CDI 2 | Child Depression Inventory 2 |
| DSM–5 | Diagnostic and Statistical Manual of Mental Disorders 5th Edition |
| DSM–IV | Diagnostic and Statistical Manual of Mental Disorders 4th Edition |
| EAT-26 | Eating Attitude Test 26 |
| EDI-3 | Eating Disorders Inventory 3 |
| ED-NOS | Eating Disorder Not Otherwise Specified |
| EDs | Eating Disorders, |
| IQR | Interquartile Range |
| MASC 2 | Multidimensional Anxiety Scale for Children. |
| R-AN | Restrictive Anorexia Nervosa |
| SRAD | Substance-Related and Addictive Disorders |
| YFAS | Yale Food Addiction Scale |
References
- Randolph, T.G. The descriptive features of food addiction; addictive eating and drinking. Q. J. Stud. Alcohol 1956, 17, 198–224. [Google Scholar] [CrossRef] [PubMed]
- Imperatori, C.; Fabbricatore, M.; Vumbaca, V.; Innamorati, M.; Contardi, A.; Farina, B. Food Addiction: Definition, measurement and prevalence in healthy subjects and in patients with eating disorders. Riv. Psichiatr. 2016, 51, 60–65. [Google Scholar] [PubMed]
- Gearhardt, A.; Corbin, W.; Brownell, K. Preliminary validation of the Yale Food Addiction Scale. Appetite 2009, 52, 430–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gearhardt, A.N.; White, M.A.; Masheb, R.M.; Morgan, P.T.; Crosby, R.D.; Grilo, C.M. An examination of the food addiction construct in obese patients with binge eating disorder. Int. J. Eat. Disord. 2012, 45, 657–663. [Google Scholar] [CrossRef] [Green Version]
- Meule, A.; Heckel, D.; Jurowich, C.F.; Vögele, C.; Kübler, A. Correlates of food addiction in obese individuals seeking bariatric surgery. Clin. Obes. 2014, 4, 228–236. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Development of the Yale Food Addiction Scale Version 2. Psychol. Addict. Behav. 2016, 30, 113–121. [Google Scholar] [CrossRef] [Green Version]
- Pursey, K.M.; Stanwell, P.; Gearhardt, A.N.; Collins, C.E.; Burrows, T.L. The prevalence of food addiction as assessed by the yale food addiction scale: A systematic review. Nutrients 2014, 6, 4552–4590. [Google Scholar] [CrossRef] [Green Version]
- Granero, R.; Jiménez-Murcia, S.; Gerhardt, A.N.; Agüera, Z.; Aymamí, N.; Gómez-Peña, M.; Lozano-Madrid, M.; Mallorquí-Bagué, N.; Mestre-Bach, G.; Neto-Antao, M.I.; et al. Validation of the Spanish version of the Yale Food Addiction Scale 2.0 (YFAS 2.0) and clinical correlates in a sample of eating disorder, gambling disorder, and healthy control participants. Front. Psychiatry 2018, 9, 1–11. [Google Scholar] [CrossRef]
- Albayrak, Ö.; Föcker, M.; Kliewer, J.; Esber, S.; Peters, T.; de Zwaan, M.; Hebebrand, J. Eating-related Psychopathology and Food Addiction in Adolescent Psychiatric Inpatients. Eur. Eat. Disord. Rev. 2017, 25, 214–220. [Google Scholar] [CrossRef]
- Granero, R.; Hilker, I.; Agüera, Z.; Jiménez-Murcia, S.; Sauchelli, S.; Islam, M.A.; Fagundo, A.B.; Sánchez, I.; Riesco, N.; Dieguez, C.; et al. Food Addiction in a Spanish Sample of Eating Disorders: DSM-5 Diagnostic Subtype Differentiation and Validation Data. Eur. Eat. Disord. Rev. 2014, 22, 389–396. [Google Scholar] [CrossRef]
- Aloi, M.; Rania, M.; Rodríguez Muñoz, R.C.; Jiménez Murcia, S.; Fernández-Aranda, F.; De Fazio, P.; Segura-Garcia, C. Validation of the Italian version of the Yale Food Addiction Scale 2.0 (I-YFAS 2.0) in a sample of undergraduate students. Eat. Weight Disord. 2017, 22, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Brunault, P.; Courtois, R.; Gearhardt, A.N.; Gaillard, P.; Journiac, K.; Cathelain, S.; Réveillère, C.; Ballon, N. Validation of the French Version of the DSM-5 Yale Food Addiction Scale in a Nonclinical Sample. Can. J. Psychiatry 2017, 62, 199–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauck, C.; Weiß, A.; Schulte, E.M.; Meule, A.; Ellrott, T. Prevalence of “Food Addiction” as Measured with the Yale Food Addiction Scale 2.0 in a Representative German Sample and Its Association with Sex, Age and Weight Categories. Obes. Facts 2017, 10, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Nunes-Neto, P.R.; Köhler, C.A.; Schuch, F.B.; Quevedo, J.; Solmi, M.; Murru, A.; Vieta, E.; Maes, M.; Stubbs, B.; Carvalho, A.F. Psychometric properties of the modified Yale food addiction scale 2.0 in a large Brazilian sample. Rev. Bras. Psiquiatr. 2018, 40, 444–448. [Google Scholar] [CrossRef] [Green Version]
- Khine, M.T.; Ota, A.; Gearhardt, A.N.; Fujisawa, A.; Morita, M.; Minagawa, A.; Li, Y.; Naito, H.; Yatsuya, H. Validation of the japanese version of the yale food addiction scale 2.0 (J-YFAS 2.0). Nutrients 2019, 11, 687. [Google Scholar] [CrossRef] [Green Version]
- Mies, G.W.; Treur, J.L.; Larsen, J.K.; Halberstadt, J.; Pasman, J.A.; Vink, J.M. The prevalence of food addiction in a large sample of adolescents and its association with addictive substances. Appetite 2017, 118, 97–105. [Google Scholar] [CrossRef]
- Zhao, Z.; Ma, Y.; Han, Y.; Liu, Y.; Yang, K.; Zhen, S.; Wen, D. Psychosocial correlates of food addiction and its association with quality of life in a non-clinical adolescent sample. Nutrients 2018, 10, 837. [Google Scholar] [CrossRef] [Green Version]
- Manzoni, G.M.; Rossi, A.; Pietrabissa, G.; Varallo, G.; Molinari, E.; Poggiogalle, E.; Donini, L.M.; Tarrini, G.; Melchionda, N.; Piccione, C.; et al. Validation of the Italian Yale Food Addiction Scale in postgraduate university students. Eat. Weight Disord. 2018, 23, 167–176. [Google Scholar] [CrossRef] [Green Version]
- Imperatori, C.; Fabbricatore, M.; Lester, D.; Manzoni, G.M.; Castelnuovo, G.; Raimondi, G.; Innamorati, M. Psychometric properties of the modified Yale Food Addiction Scale Version 2.0 in an Italian non-clinical sample. Eat. Weight Disord. 2019, 24, 37–45. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; Boswell, R.G.; White, M.A. The association of “food addiction” with disordered eating and body mass index. Eat. Behav. 2014, 15, 427–433. [Google Scholar] [CrossRef] [Green Version]
- Zanna, V.; Castiglioni, M.C.; Criscuolo, M.; Chianello, I.; Elisei, M.; Cinelli, G.; Laghi, F.; Mazzoni, S.; Vicari, S. Day-Hospital Multifocal Integrated Treatment for Anorexia Nervosa in Adolescents: A One-Year Follow-Up. J. Child Fam. Stud. 2017, 26, 1460–1471. [Google Scholar] [CrossRef]
- Birmaher, B.; Ehmann, M.; Axelson, D.A.; Goldstein, B.I.; Monk, K.; Kalas, C.; Kupfer, D.; Gill, M.K.; Leibenluft, E.; Bridge, J.; et al. Schedule for affective disorders and schizophrenia for school-age children (K-SADS-PL) for the assessment of preschool children—A preliminary psychometric study. J. Psychiatr. Res. 2009, 43, 680–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- March, J.S. Multidimensional Anxiety Scale for Children 2nd Edition (MASC 2); Multi-Health Systems: Toronto, ON, Canada, 2013. [Google Scholar]
- Paloscia, C.; Giangregorio, A.; Guerini, R.; Melchiori, F.M. MASC 2—Multidimensional Anxiety Scale for Children-Second Edition—Manuale Versione Italiana; Hogrefe: Firenze, Italy, 2017. [Google Scholar]
- Kovács, M. Children’s Depression Inventory 2TM(CDI 2) North Tonawanda; Multi-Health Systems: New York, NY, USA, 2010. [Google Scholar]
- Camuffo, M.; Cerutti, R.; Kovacs, M. CDI-2 Children’s Depression Inventory, 2nd ed.; Italian adaptation; Hogrefe: Firenze, Italy, 2018. [Google Scholar]
- Achenbach, T.; Rescorla, L. Manual for the ASEBA School-Age Forms & Profiles; University of Vermont, Research Center for Children, Youth, & Families: Burlington, VT, USA, 2001. [Google Scholar]
- Frigerio, A.; Monterosso, R. La valutazione su base empirica dei problemi emotivo-comportamentali in età evolutiva. Infanz. Adolesc. 2002, 1, 38–48. [Google Scholar]
- Garner, D. EDI-3, Eating Disorder Inventory-3: Professional Manual; Psychological Assessment Resources, Inc.: Lutz, FL, USA, 2004. [Google Scholar]
- Giannini, M.; Pannocchia, L.; Dalle Grave, R.; Muratori, F.; Viglione, V. EDI-3 Eating Disorders Inventory-Manuale. Adattamento Italiano; Giunti Organizzazioni Speciali (OS): Firenze, Italy, 2008. [Google Scholar]
- Dotti, A.; Lazzari, R. Validation and reliability of the Italian EAT-Eat. Weight Disord. 1998, 3, 188–194. [Google Scholar] [CrossRef]
- Cuzzolaro, M.; Vetrone, G.; Marano, G.; Batacchi, M.W. BUT: Una nuova scala per la valutazione del disagio relativo all’immagine del corpo. Psichiatr. Infanz. Adolesc. 1999, 66, 417–428. [Google Scholar]
- Meule, A.; Hermann, T.; Kübler, A. Food addiction in overweight and obese adolescents seeking weight-loss treatment. Eur. Eat. Disord. Rev. 2015, 23, 193–198. [Google Scholar] [CrossRef]
- Castellini, G.; Lo Sauro, C.; Mannucci, E.; Ravaldi, C.; Rotella, C.M.; Faravelli, C.; Ricca, V. Diagnostic crossover and outcome predictors in eating disorders according to DSM-IV and DSM-V proposed criteria: A 6-year follow-up study. Psychosom. Med. 2011, 73, 270–279. [Google Scholar] [CrossRef]
- Manjrekar, E.; Berenbaum, H.; Bhayani, N. Investigating the moderating role of emotional awareness in the association between urgency and binge eating. Eat. Behav. 2015, 17, 99–102. [Google Scholar] [CrossRef]
- Dorard, G.; Khorramian-Pour, M. Hyperphagie boulimique: Liens avec la personnalité et l’émotionnalité. Encephale 2017, 43, 114–119. [Google Scholar] [CrossRef]


{kind=link}
| Whole Sample (n = 87) | ARFID (n = 9) | R-AN (n = 41) | BN (n = 7) | BED (n = 2) | ED-NOS (n = 8) | BP-AN (n = 1) | A-AN (n = 19) | p * | |
|---|---|---|---|---|---|---|---|---|---|
| Age | 15.60 (2.8) | 14.10 (3.9) | 16.00 (2.40) | 16.30 (1.80) | 14.75 (-) | 16.10 (3.05) | 16.60 | 15.10 (3.20) | 0.000 |
| Gender (F) | 79 (90.8) | 5 (55.6) | 41 (100.0) | 7 (100.0) | 1 (50.0) | 6 (75.0) | 1 (100.0) | 18 (94.7) | - |
| Weight (kg) | 43.50 (11.80) | 38.60 (11.90) | 41.60 (8.40) | 54.20 (2.80) | 116.20 (-) | 38.9 (18.2) | 41.30 | 49.10 (11.60) | 0.003 |
| Height (cm) | 159.00 (9.50) | 160.50 (13.50) | 159.00 (7.50) | 157.00 (9.80) | 166.50 (-) | 157.00 (6.50) | 160.00 | 159.00 (11.0) | 0.259 |
| BMI (kg/cm2) a | 17.24 (3.55) | 14.98 (2.74) | 16.47 (2.87) | 21.58 (2.30) | 41.95 (-) | 15.81 (4.07) | 16.13 | 19.43 (2.61) | 0.000 |
| BMI percentile a | 10.00 (32.00) | 3.00 (15.5) | 4.0 (9.5) | 65.00 (43.0) | 99.0 (-) | 5.00 (16.3) | 1.0 | 40.00 (34.00) | 0.000 |
| Whole Sample (n = 87) | ARFID (n = 9) | R-AN (n = 41) | BN (n = 7) | BED (n = 2) | ED-NOS (n = 8) | BP-AN (n = 1) | A-AN (n = 19) | Test Value | p | V di Cramer a | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Food Addiction | |||||||||||
| Positive | 43 (49.4) | 3 (33.3) | 22 (53.7) | 4 (57.1) | 0 (0) | 3 (37.5) | 1 (100) | 10 (52.6) | 4.520 | 0.653 a | - |
| Severity | |||||||||||
| Mild | 15 (17.2) | 1 (11,1) | 8 (19,5) | 0 (0) | 0 (0) | 2 (25) | 1 (100) | 3 (15,8) | 9.630 | 0.416 a | - |
| Moderate | 12 (13.8) | 1 (11,1) | 7 (17,1) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 4 (21,1) | - | - | - |
| Severe | 16 (18.4) | 1 (11,1) | 7 (17,1) | 4 (57,1) | 0 (0) | 1 (12,5) | 0 (0) | 3 (15,8) | - | - | - |
| Yfas 2.0 Symptoms | |||||||||||
| Amount | 16 (18,40) | 1 (11.1) | 4 (9.8) | 5 (71.4) | 2 (100.0) | 1 (12.5) | 0 (0.0) | 3 (15.8) | 18.425 | 0.001a | 0.543 |
| Attemps | 22 (25,30) | 1 (11.1) | 12 (29.3) | 2 (28.6) | 2 (100.0) | 1 (12.5) | 0 (0.0) | 4 (21.1) | 6.862 | 0.300 a | -- |
| Time | 35 (40,20) | 4 (44.4) | 14 (34.1) | 4 (57.1) | 2 (100.0) | 2 (25.0) | 1 (100.0) | 8 (42.1) | 6.311 | 0.367 a | -- |
| Activities | 27 (31,00) | 2 (22.2) | 15 (36.6) | 4 (57.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 6 (31.6) | 7.676 | 0.227 a | -- |
| Consequences | 24 (27,60) | 2 (22.2) | 12 (29.3) | 4 (57.1) | 2 (100.0) | 1 (12.5) | 0 (0.0) | 3 (15.8) | 9.545 | 0.101 a | -- |
| Tolerance | 21 (24,10) | 2 (22.2) | 8 (19.5) | 3 (42.9) | 2 (100.0) | 1 (12.5) | 0 (0.0) | 5 (26.3) | 7.690 | 0.217 a | -- |
| Withdrawal | 44 (50,60) | 4 (44.4) | 18 (43.9) | 5 (71.4) | 2 (100.0) | 3 (37.5) | 0 (0.0) | 12 (63.2) | 6.325 | 0.363 a | -- |
| Problems | 28 (32,20) | 2 (22.2) | 15 (36.6) | 3 (42.9) | 2 (100.0) | 1 (12.5) | 1 (100.0) | 4 (21.1) | 8.816 | 0.141 a | -- |
| Obligations | 9 (10,30) | 0 (0.0) | 4 (9.8) | 1 (14.3) | 1 (50.0) | 0 (0.0) | 0 (0.0) | 3 (15.8) | 5.977 | 0.389 a | -- |
| Situations | 12 (13,80) | 1 (11.1) | 5 (12.2) | 2 (28.6) | 2 (100.0) | 0 (0.0) | 0 (0.0) | 2 (10.5) | 10.439 | 0.061 a | -- |
| Craving | 19 (21,80) | 1 (11.1) | 9 (22.0) | 4 (57.1) | 2 (100.0) | 1 (12.5) | 0 (0.0) | 2 (10.5) | 11.957 | 0.032a | 0.415 |
| Dependent Variable | Independent Variables | Coefficient (B) | 95% CI | p | Exp (B) | |
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| Food addiction | Age | 0.430 | 1.034 | 2.288 | 0.034 | 1.538 |
| EAT-26 | 0.046 | 1.009 | 1.087 | 0.015 | 1.047 | |
| Interoceptive Deficits (EDI-3) | 0.095 | 1.024 | 1.181 | 0.009 | 1.100 | |
| Constant | −9.662 | 0.005 | 0.000 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cinelli, G.; Criscuolo, M.; Bifone, C.; Chianello, I.; Castiglioni, M.C.; De Lorenzo, A.; Di Renzo, L.; Tozzi, A.E.; Vicari, S.; Zanna, V. Food Addiction in a Group of Italian Adolescents Diagnosed for Eating Disorder. Nutrients 2020, 12, 1524. https://doi.org/10.3390/nu12051524
Cinelli G, Criscuolo M, Bifone C, Chianello I, Castiglioni MC, De Lorenzo A, Di Renzo L, Tozzi AE, Vicari S, Zanna V. Food Addiction in a Group of Italian Adolescents Diagnosed for Eating Disorder. Nutrients. 2020; 12(5):1524. https://doi.org/10.3390/nu12051524
Chicago/Turabian StyleCinelli, Giulia, Michela Criscuolo, Costanza Bifone, Ilenia Chianello, Maria Chiara Castiglioni, Antonino De Lorenzo, Laura Di Renzo, Alberto Eugenio Tozzi, Stefano Vicari, and Valeria Zanna. 2020. "Food Addiction in a Group of Italian Adolescents Diagnosed for Eating Disorder" Nutrients 12, no. 5: 1524. https://doi.org/10.3390/nu12051524
APA StyleCinelli, G., Criscuolo, M., Bifone, C., Chianello, I., Castiglioni, M. C., De Lorenzo, A., Di Renzo, L., Tozzi, A. E., Vicari, S., & Zanna, V. (2020). Food Addiction in a Group of Italian Adolescents Diagnosed for Eating Disorder. Nutrients, 12(5), 1524. https://doi.org/10.3390/nu12051524