The Relationship between Abdominal Fat Phenotypes and Insulin Resistance in Non-Obese Individuals after Acute Pancreatitis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Clinic Visit
2.3. Quantification of Abdominal Fat Phenotypes
2.3.1. Imaging Protocol
2.3.2. Intra-Pancreatic Fat Deposition
2.3.3. Intra-Hepatic Fat Deposition
2.3.4. Skeletal Muscle Fat Deposition
2.3.5. Subcutaneous and Visceral Fat Volumes
2.4. Laboratory Data
2.5. Indices of Insulin Sensitivity
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
3.2. Abdominal Fat Phenotypes in the Study Groups
3.3. Associations between Abdominal Fat Phenotypes and Indices of Insulin Sensitivity in the Study Groups
3.3.1. Intra-Pancreatic Fat Deposition
3.3.2. Intra-Hepatic Fat Deposition
3.3.3. Skeletal Muscle Fat Deposition
3.3.4. Visceral Fat Volume
3.3.5. Subcutaneous Fat Volume
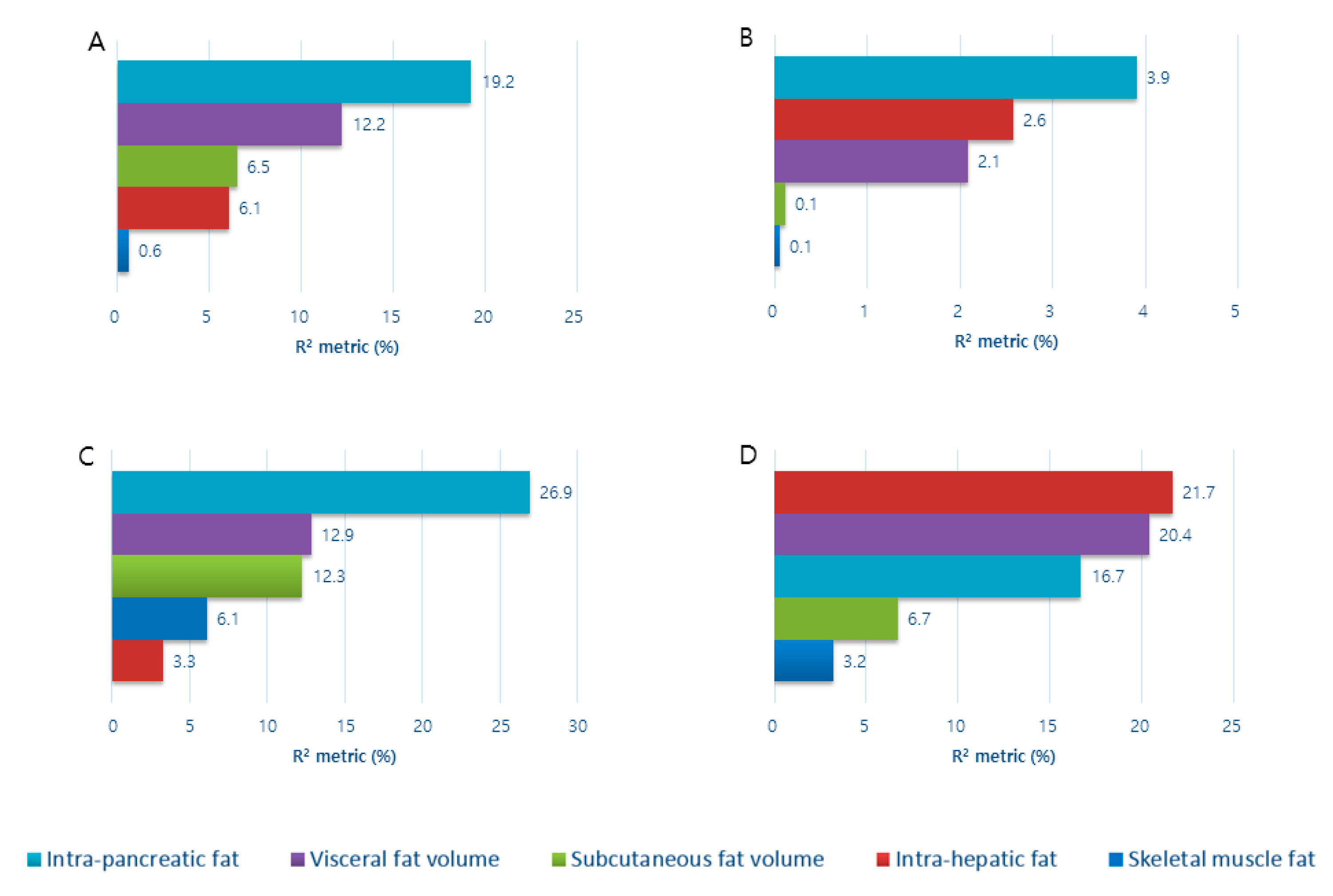
3.4. Contribution of Abdominal Fat Phenotypes to Indices of Insulin Sensitivity in the Study Groups
4. Discussion
Author Contributions
Acknowledgments
Funding
Conflicts of Interest
References
- Das, S.L.; Kennedy, J.I.; Murphy, R.; Phillips, A.R.; Windsor, J.A.; Petrov, M.S. Relationship between the exocrine and endocrine pancreas after acute pancreatitis. World J. Gastroenterol. 2014, 20, 17196–17205. [Google Scholar] [CrossRef] [PubMed]
- Das, S.L.; Singh, P.P.; Phillips, A.R.; Murphy, R.; Windsor, J.A.; Petrov, M.S. Newly diagnosed diabetes mellitus after acute pancreatitis: A systematic review and meta-analysis. Gut 2014, 63, 818–831. [Google Scholar] [CrossRef] [PubMed]
- Pendharkar, S.A.; Mathew, J.; Petrov, M.S. Age- and sex-specific prevalence of diabetes associated with diseases of the exocrine pancreas: A population-based study. Dig. Liver Dis. 2017, 49, 540–544. [Google Scholar] [CrossRef] [PubMed]
- Pendharkar, S.A.; Singh, R.G.; Chand, S.K.; Cervantes, A.; Petrov, M.S. Pro-inflammatory cytokines after an episode of acute pancreatitis: Associations with fasting gut hormone profile. Inflamm. Res. 2018, 67, 339–350. [Google Scholar] [CrossRef]
- Cho, J.; Walia, M.; Scragg, R.; Petrov, M.S. Frequency and risk factors for mental disorders following pancreatitis: A nationwide cohort study. Curr. Med. Res. Opin. 2019, 35, 1157–1164. [Google Scholar] [CrossRef]
- Petrov, M.S. Panorama of mediators in postpancreatitis diabetes mellitus. Curr. Opin. Gastroenterol. 2020, 36, 443–451. [Google Scholar] [CrossRef]
- Bharmal, S.H.; Cho, J.; Alarcon Ramos, G.C.; Ko, J.; Stuart, C.E.; Modesto, A.E.; Singh, R.G.; Petrov, M.S. Trajectories of glycaemia following acute pancreatitis: A prospective longitudinal cohort study with 24 months follow-up. J. Gastroenterol. 2020, 55, 775–788. [Google Scholar] [CrossRef]
- Bharmal, S.H.; Cho, J.; Stuart, C.E.; Alarcon Ramos, G.C.; Ko, J.; Petrov, M.S. Oxyntomodulin may distinguish new-onset diabetes after acute pancreatitis from type 2 diabetes. Clin. Transl. Gastroenterol. 2020, 11, e00132. [Google Scholar] [CrossRef]
- Woodmansey, C.; McGovern, A.P.; McCullough, K.A.; Whyte, M.B.; Munro, N.M.; Correa, A.C.; Gatenby, P.A.; Jones, S.A.; De Lusignan, S. Incidence, demographics, and clinical characteristics of diabetes of the exocrine pancreas (Type 3c): A retrospective cohort study. Diabetes Care 2017, 40, 1486–1493. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.; Scragg, R.; Petrov, M.S. Postpancreatitis diabetes confers higher risk for pancreatic cancer than type 2 diabetes: Results from a nationwide cancer registry. Diabetes Care 2020, 43, 2106–2112. [Google Scholar] [CrossRef]
- Cho, J.; Scragg, R.; Petrov, M.S. Risk of mortality and hospitalization after post-pancreatitis diabetes mellitus vs type 2 diabetes mellitus: A population-based matched cohort study. Am. J. Gastroenterol. 2019, 114, 804–812. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.; Scragg, R.; Pandol, S.J.; Goodarzi, M.O.; Petrov, M.S. Antidiabetic medications and mortality risk in individuals with pancreatic cancer-related diabetes and postpancreatitis diabetes: A nationwide cohort study. Diabetes Care 2019, 42, 1675–1683. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.; Scragg, R.; Petrov, M.S. Use of insulin and the risk of progression of pancreatitis: A population-based cohort study. Clin. Pharmacol. Ther. 2020, 107, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Lankisch, P.G.; Schirren, C.A. Increased body weight as a prognostic parameter for complications in the course of acute pancreatitis. Pancreas 1990, 5, 626–629. [Google Scholar] [CrossRef]
- Aune, D.; Mahamat-Saleh, Y.; Norat, T.; Riboli, E. High body mass index and central adiposity is associated with increased risk of acute pancreatitis: A meta-analysis. Dig. Dis. Sci. 2020. [Google Scholar] [CrossRef]
- Petrov, M.S. Abdominal fat: A key player in metabolic acute pancreatitis. Am. J. Gastroenterol. 2013, 108, 140–142. [Google Scholar] [CrossRef]
- Singh, R.G.; Pendharkar, S.A.; Cervantes, A.; Cho, J.; Miranda-Soberanis, V.; Petrov, M.S. Abdominal obesity and insulin resistance after an episode of acute pancreatitis. Dig. Liver Dis. 2018, 50, 1081–1087. [Google Scholar] [CrossRef]
- Shulman, G.I. Ectopic fat in insulin resistance, dyslipidemia, and cardiometabolic disease. N. Engl. J. Med. 2014, 371, 1131–1141. [Google Scholar] [CrossRef]
- Petrov, M.S. Skeletal muscle: A new piece in the pancreatitis puzzle. United Eur. Gastroenterol. J. 2019, 7, 1283–1284. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.G.; Yoon, H.D.; Wu, L.M.; Lu, J.; Plank, L.D.; Petrov, M.S. Ectopic fat accumulation in the pancreas and its clinical relevance: A systematic review, meta-analysis, and meta-regression. Metabolism 2017, 69, 1–13. [Google Scholar] [CrossRef]
- Gudipaty, L.; Rosenfeld, N.K.; Fuller, C.S.; Cuchel, M.; Rickels, M.R. Different β-cell secretory phenotype in non-obese compared to obese early type 2 diabetes. Diabetes Metab. Res. Rev. 2020, 36, e3295. [Google Scholar] [CrossRef] [PubMed]
- Suraamornkul, S.; Kwancharoen, R.; Ovartlarnporn, M.; Rawdaree, P.; Bajaj, M. Insulin clamp-derived measurements of insulin sensitivity and insulin secretion in lean and obese asian type 2 diabetic patients. Metab. Syndr. Relat. Disord. 2010, 8, 113–117. [Google Scholar] [CrossRef] [PubMed]
- DeSouza, S.V.; Priya, S.; Cho, J.; Singh, R.G.; Petrov, M.S. Pancreas shrinkage following recurrent acute pancreatitis: An MRI study. Eur. Radiol. 2019, 29, 3746–3756. [Google Scholar] [CrossRef] [PubMed]
- Cervantes, A.; Singh, R.G.; Kim, J.U.; DeSouza, S.V.; Petrov, M.S. Relationship of anthropometric indices to abdominal body composition: A multi-ethnic New Zealand magnetic resonance imaging study. J. Clin. Med. Res. 2019, 11, 435–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, R.G.; Nguyen, N.N.; Cervantes, A.; Alarcon Ramos, G.C.; Cho, J.; Petrov, M.S. Associations between intra-pancreatic fat deposition and circulating levels of cytokines. Cytokine 2019, 120, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.G.; Nguyen, N.N.; DeSouza, S.V.; Pendharkar, S.A.; Petrov, M.S. Comprehensive analysis of body composition and insulin traits associated with intra-pancreatic fat deposition in healthy individuals and people with new-onset prediabetes/diabetes after acute pancreatitis. Diabetes Obes. Metab. 2019, 21, 417–423. [Google Scholar] [CrossRef]
- Petrov, M.S. Diabetes of the exocrine pancreas: American Diabetes Association-compliant lexicon. Pancreatology 2017, 17, 523–526. [Google Scholar] [CrossRef]
- Petrov, M.S.; Yadav, D. Global epidemiology and holistic prevention of pancreatitis. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 175–184. [Google Scholar] [CrossRef]
- Bharmal, S.H.; Pendharkar, S.; Singh, R.G.; Cho, J.; Petrov, M.S. Glucose counter-regulation after acute pancreatitis. Pancreas 2019, 48, 670–681. [Google Scholar] [CrossRef]
- Dellinger, E.P.; Forsmark, C.E.; Layer, P.; Lévy, P.; Maraví-Poma, E.; Petrov, M.S.; Shimosegawa, T.; Siriwardena, A.K.; Uomo, G.; Whitcomb, D.C.; et al. Determinant-based classification of acute pancreatitis severity: An international multidisciplinary consultation. Ann. Surg. 2012, 256, 875–880. [Google Scholar] [CrossRef]
- American Diabetes Association Classification and diagnosis of diabetes: Standards of medical care in diabetes—2020. Diabetes Care 2020, 43, S14–S31. [CrossRef] [PubMed] [Green Version]
- Singh, R.G.; Cervantes, A.; Kim, J.U.; Nguyen, N.N.; DeSouza, S.V.; Dokpuang, D.; Lu, J.; Petrov, M.S. Intrapancreatic fat deposition and visceral fat volume are associated with the presence of diabetes after acute pancreatitis. Am. J. Physiol. Gastrointest. Liver Physiol. 2019, 316, G806–G815. [Google Scholar] [CrossRef] [PubMed]
- Al-Mrabeh, A.; Hollingsworth, K.G.; Steven, S.; Tiniakos, D.; Taylor, R. Quantification of intrapancreatic fat in type 2 diabetes by MRI. PLoS ONE 2017, 12, e0174660. [Google Scholar] [CrossRef] [Green Version]
- Crane, J.C.; Olson, M.P.; Nelson, S.J. SIVIC: Open-source, standards-based software for DICOM MR spectroscopy workflows. Int. J. Biomed. Imaging 2013, 2013. [Google Scholar] [CrossRef] [PubMed]
- Kiefer, L.S.; Fabian, J.; Lorbeer, R.; Machann, J.; Storz, C.; Kraus, M.S.; WinTermeyer, E.K.; Schlett, C.; Roemer, F.; Nikolaou, K.; et al. Inter- and intra-observer variability of an anatomical landmark-based, manual segmentation method by MRI for the assessment of skeletal muscle fat content and area in subjects from the general population. Br. J. Radiol. 2018, 91, 20180019. [Google Scholar] [CrossRef]
- Schneider, C.; Rasband, W.; Eliceiri, K. NIH Image to ImageJ: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Modesto, A.E.; Stuart, C.E.; Cho, J.; Ko, J.; Singh, R.G.; Petrov, M.S. Psoas muscle size as a magnetic resonance imaging biomarker of progression of pancreatitis. Eur. Radiol. 2020, 30, 2902–2911. [Google Scholar] [CrossRef]
- Irlbeck, T.; Massaro, J.M.; Bamberg, F.; O’Donnell, C.J.; Hoffmann, U.; Fox, C.S. Association between single-slice measurements of visceral and abdominal subcutaneous adipose tissue with volumetric measurements: The Framingham Heart study. Int. J. Obes. 2010, 34, 781–787. [Google Scholar] [CrossRef] [Green Version]
- Stuart, C.E.; Ko, J.; Alarcon Ramos, G.C.; Modesto, A.E.; Cho, J.; Petrov, M.S. Associations between cannabis use, abdominal fat phenotypes and insulin traits. J. Clin. Med. Res. 2020, 12, 377–388. [Google Scholar] [CrossRef]
- Pendharkar, S.A.; Singh, R.G.; Cervantes, A.; Desouza, S.V.; Bharmal, S.H.; Petrov, M.S. Gut hormone responses to mixed meal test in new-onset prediabetes/diabetes after acute pancreatitis. Horm. Metab. Res. 2019, 51, 191–199. [Google Scholar] [CrossRef]
- Pendharkar, S.A.; Singh, R.G.; Bharmal, S.H.; Drury, M.; Petrov, M.S. Pancreatic hormone responses to mixed meal test in new-onset prediabetes/diabetes after non-necrotizing acute pancreatitis. J. Clin. Gastroenterol. 2020, 54, e11–e20. [Google Scholar] [CrossRef]
- Yu, X.; Wang, L.; Zhang, W.; Ming, J.; Jia, A.; Xu, S.; Li, Q.; Ji, Q. Fasting triglycerides and glucose index is more suitable for the identification of metabolically unhealthy individuals in the Chinese adult population: A nationwide study. J. Diabetes Investig. 2019, 10, 1050–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grömping, U. Relative importance for linear regression in R: The package relaimpo. J. Stat. Softw. 2006, 17, 1–27. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.G.; Yoon, H.D.; Poppitt, S.D.; Plank, L.D.; Petrov, M.S. Ectopic fat accumulation in the pancreas and its biomarkers: A systematic review and meta-analysis. Diabetes Metab. Res. Rev. 2017, 33, 182–248. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.G.; Pendharkar, S.A.; Plank, L.D.; Petrov, M.S. Role of human lipocalin proteins in abdominal obesity after acute pancreatitis. Peptides 2017, 91, 1–7. [Google Scholar] [CrossRef]
- Jo, Y.J.; Park, J.Y.; Kim, S.H.; Kim, S.H.; Kim, Y.S.; Son, B.K.; Lee, J.S.; Jang, E.C.; Jun, D.W.; Han, J.H.; et al. Clinical implications of fatty pancreas: Correlations between fatty pancreas and metabolic syndrome. World J. Gastroenterol. 2009, 15, 1869. [Google Scholar] [CrossRef]
- Fernandez-Real, J.M.; Broch, M.; Vendrell, J.; Ricart, W. Insulin resistance, inflammation, and serum fatty acid composition. Diabetes Care 2003, 26, 1362–1368. [Google Scholar] [CrossRef] [Green Version]
- Gulen, M.; Guven, A.; Ozlem, Y.; Hismigullari, A. Histopathological changes in rat pancreas and skeletal muscle associated with high fat diet induced insulin resistance. Biotech. Histochem. 2015, 90, 495–505. [Google Scholar] [CrossRef]
- Singh, R.G.; Nguyen, N.N.; Cervantes, A.; Cho, J.; Petrov, M.S. Serum lipid profile as a biomarker of intra-pancreatic fat deposition: A nested cross-sectional study. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 956–964. [Google Scholar] [CrossRef]
- Sreedhar, U.L.; DeSouza, S.V.; Park, B.; Petrov, M.S. A systematic review of intra-pancreatic fat deposition and pancreatic carcinogenesis. J. Gastrointest. Surg. 2019. [Google Scholar] [CrossRef]
- Bonal, C.; Thorel, F.; Ait-Lounis, A.; Reith, W.; Trumpp, A.; Herrera, P.L. Pancreatic inactivation of c-Myc decreases acinar mass and transdifferentiates acinar cells into adipocytes in mice. Gastroenterology 2009, 136, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Ho, T.W.; Wu, J.M.; Kuo, T.C.; Yang, C.Y.; Lai, H.S.; Hsieh, S.H.; Lai, F.; Tien, Y.W. Change of both endocrine and exocrine insufficiencies after acute pancreatitis in non-diabetic patients. Medicine 2015, 94, e1123. [Google Scholar] [CrossRef] [PubMed]
- Barreto, S.G.; Carati, C.J.; Toouli, J.; Saccone, G.T.P. The islet-acinar axis of the pancreas: More than just insulin. Am. J. Physiol. Gastrointest. Liver Physiol. 2010, 299, 10–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szczepaniak, L.S.; Victor, R.G.; Mathur, R.; Nelson, M.D.; Szczepaniak, E.W.; Tyer, N.; Chen, I.; Unger, R.H.; Bergman, R.N.; Lingvay, I. Pancreatic steatosis and its relationship to β-cell dysfunction in humans: Racial and ethnic variations. Diabetes Care 2012, 35, 2377–2383. [Google Scholar] [CrossRef] [Green Version]
- Petrov, M.S. Harnessing analytic morphomics for early detection of pancreatic cancer. Pancreas 2018, 47, 1051–1054. [Google Scholar] [CrossRef]
- Alizargar, J.; Bai, C.H.; Hsieh, N.C.; Wu, S.F.V. Use of the triglyceride-glucose index (TyG) in cardiovascular disease patients. Cardiovasc. Diabetol. 2020, 19, 2–4. [Google Scholar] [CrossRef] [Green Version]
- Chamroonkiadtikun, P.; Ananchaisarp, T.; Wanichanon, W. The triglyceride-glucose index, a predictor of type 2 diabetes development: A retrospective cohort study. Prim. Care Diabetes 2020, 14, 161–167. [Google Scholar] [CrossRef]
- Heise, T.; Zijlstra, E.; Nosek, L.; Heckermann, S.; Plum-Mörschel, L.; Forst, T. Euglycaemic glucose clamp: What it can and cannot do, and how to do it. Diabetes Obes. Metab. 2016, 18, 962–972. [Google Scholar] [CrossRef]
- Chu, A.Y.; Deng, X.; Fisher, V.A.; Drong, A.; Zhang, Y.; Feitosa, M.F.; Liu, C.T.; Weeks, O.; Choh, A.C.; Duan, Q.; et al. Multiethnic genome-wide meta-analysis of ectopic fat depots identifies loci associated with adipocyte development and differentiation. Nat. Genet. 2017, 49, 125–130. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristic | Healthy Controls (n = 32) | T2DM (n = 20) | NODAP (n = 26) | p * |
|---|---|---|---|---|
| Age (years) | 46.0 (29.5–63.0) | 59.5 (49.5–72.0) | 58.0 (47.0–66.0) | 0.036 |
| Men, n (%) | 19 (54.3) | 16 (76.2) | 19 (70.1) | 0.195 |
| Body mass index (kg/m2) | 23.6 (21.6–26.6) | 26.4 (24.2–28.1) | 24.7 (22.3–27.1) | 0.009 |
| Triglycerides (mmol/L) | 0.9 (0.6–1.2) | 1.5 (0.9–2.0) | 1.5 (1.1–2.4) | 0.044 |
| Total cholesterol (mmol/L) | 4.5 (3.7–5.5) | 3.6 (4.5–5.4) | 5.0 (4.1–5.4) | 0.431 |
| HDL cholesterol (mmol/L) | 1.3 (0.9–1.8) | 1.3 (1.0–1.6) | 1.3 (1.1–1.6) | 0.791 |
| LDL cholesterol (mmol/L) | 2.7 (2.0–3.3) | 2.8 (2.1–3.2) | 2.6 (2.3–3.4) | 0.624 |
| Glycated hemoglobin A1c (mmol/mol) | 33.0 (31.0–35.0) | 41.0 (38.5–9.5) | 38.5 (36.0–41.1) | <0.001 |
| Fasting plasma glucose (mmol/L) | 4.8 (4.2–5.3) | 10.8 (8.9–19.4) | 8.4 (4.8–14.3) | <0.001 |
| Index | Healthy Controls | T2DM | NODAP | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | S.E. | p | R2 | β | S.E. | p | R2 | β | S.E. | p | R2 | |
| HOMA-IS | ||||||||||||
| Model 1 | −0.057 | 0.109 | 0.608 | 0.013 | −0.035 | 0.041 | 0.406 | 0.037 | −0.186 | 0.060 | 0.005 | 0.285 |
| Model 2 | −0.092 | 0.116 | 0.438 | −0.038 | 0.043 | 0.398 | −0.204 | 0.074 | 0.011 | |||
| Model 3 | −0.080 | 0.136 | 0.565 | −0.015 | 0.042 | 0.721 | −0.199 | 0.082 | 0.024 | |||
| Raynaud index | ||||||||||||
| Model 1 | 0.030 | 0.244 | 0.902 | 0.001 | −0.384 | 0.714 | 0.597 | 0.015 | −5.271 | 2.330 | 0.033 | 0.176 |
| Model 2 | 0.074 | 0.249 | 0.768 | −0.453 | 0.756 | 0.557 | −6.726 | 2.806 | 0.026 | |||
| Model 3 | 0.102 | 0.272 | 0.711 | −0.274 | 0.798 | 0.736 | −7.147 | 3.101 | 0.032 | |||
| Matsuda index | ||||||||||||
| Model 1 | 1.320 | 5.291 | 0.806 | 0.004 | 0.714 | 2.529 | 0.787 | 0.023 | −7.451 | 2.016 | 0.002 | 0.477 |
| Model 2 | 2.147 | 5.814 | 0.718 | 0.459 | 3.149 | 0.891 | −8.648 | 2.561 | 0.011 | |||
| Model 3 | 1.503 | 6.447 | 0.820 | 2.096 | 1.681 | 0.303 | −7.904 | 3.003 | 0.022 | |||
| TyG | ||||||||||||
| Model 1 | 0.036 | 0.056 | 0.532 | 0.017 | 0.178 | 0.159 | 0.277 | 0.065 | 0.324 | 0.091 | 0.002 | 0.357 |
| Model 2 | 0.048 | 0.049 | 0.338 | 0.182 | 0.170 | 0.299 | 0.354 | 0.106 | 0.003 | |||
| Model 3 | 0.032 | 0.053 | 0.547 | 0.058 | 0.158 | 0.720 | 0.379 | 0.11 | 0.004 | |||
| Index | Healthy Controls | T2DM | NODAP | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | S.E. | p | R2 | β | S.E. | p | R2 | β | S.E. | p | R2 | |
| HOMA-IS | ||||||||||||
| Model 1 | 0.011 | 0.034 | 0.740 | 0.005 | −0.002 | 0.003 | 0.589 | 0.017 | −0.051 | 0.024 | 0.046 | 0.150 |
| Model 2 | 0.005 | 0.036 | 0.888 | −0.002 | 0.004 | 0.625 | −0.048 | 0.027 | 0.087 | |||
| Model 3 | −0.009 | 0.042 | 0.833 | −0.001 | 0.003 | 0.681 | −0.048 | 0.027 | 0.085 | |||
| Raynaud index | ||||||||||||
| Model 1 | 0.072 | 0.077 | 0.358 | 0.033 | −0.035 | 0.058 | 0.555 | 0.020 | −1.216 | 0.920 | 0.198 | 0.065 |
| Model 2 | 0.086 | 0.077 | 0.277 | −0.032 | 0.060 | 0.596 | −1.336 | 1.018 | 0.202 | |||
| Model 3 | 0.095 | 0.086 | 0.279 | −0.029 | 0.061 | 0.637 | −1.341 | 1.035 | 0.208 | |||
| Matsuda index | ||||||||||||
| Model 1 | −0.687 | 1.380 | 0.625 | 0.015 | 0.312 | 0.296 | 0.341 | 0.181 | −1.768 | 0.904 | 0.069 | 0.203 |
| Model 2 | −0.564 | 1.472 | 0.707 | 0.491 | 0.555 | 0.441 | −1.482 | 1.092 | 0.198 | |||
| Model 3 | −0.411 | 1.782 | 0.821 | 0.053 | 0.467 | 0.920 | −1.586 | 1.084 | 0.169 | |||
| TyG | ||||||||||||
| Model 1 | −0.013 | 0.020 | 0.527 | 0.016 | 0.007 | 0.013 | 0.603 | 0.016 | 0.014 | 0.031 | <0.001 | 0.461 |
| Model 2 | −0.008 | 0.018 | 0.674 | 0.007 | 0.014 | 0.637 | 0.128 | 0.034 | 0.001 | |||
| Model 3 | 0.001 | 0.020 | 0.945 | 0.005 | 0.012 | 0.659 | 0.129 | 0.034 | 0.001 | |||
| Index | Healthy Controls | T2DM | NODAP | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | S.E. | p | R2 | β | S.E. | p | R2 | β | S.E. | p | R2 | |
| HOMA-IS | ||||||||||||
| Model 1 | −0.004 | 0.031 | 0.894 | 0.001 | 0.002 | 0.010 | 0.874 | 0.001 | 0.004 | 0.020 | 0.846 | 0.002 |
| Model 2 | −0.045 | 0.043 | 0.309 | 0.014 | 0.018 | 0.464 | 0.008 | 0.035 | 0.816 | |||
| Model 3 | −0.040 | 0.046 | 0.399 | 0.006 | 0.018 | 0.722 | 0.019 | 0.036 | 0.604 | |||
| Raynaud index | ||||||||||||
| Model 1 | −0.064 | 0.068 | 0.358 | 0.033 | 0.014 | 0.175 | 0.938 | <0.001 | 0.170 | 0.723 | 0.816 | 0.002 |
| Model 2 | −0.031 | 0.096 | 0.754 | 0.278 | 0.313 | 0.387 | 0.822 | 1.262 | 0.521 | |||
| Model 3 | −0.028 | 0.100 | 0.782 | 0.223 | 0.325 | 0.503 | 1.066 | 1.324 | 0.430 | |||
| Matsuda index | ||||||||||||
| Model 1 | −1.420 | 1.266 | 0.279 | 0.072 | 1.062 | 0.957 | 0.310 | 0.170 | 0.592 | 0.819 | 0.557 | 0.024 |
| Model 2 | −1.919 | 2.157 | 0.389 | 4.140 | 1.022 | 0.016 | 0.628 | 1.520 | 0.686 | |||
| Model 3 | −2.067 | 2.504 | 0.243 | 2.943 | 1.830 | 0.206 | 1.118 | 1.169 | 0.490 | |||
| TyG | ||||||||||||
| Model 1 | −0.012 | 0.018 | 0.556 | 0.014 | −0.0363 | 0.041 | 0.397 | 0.042 | −0.031 | 0.031 | 0.322 | 0.041 |
| Model 2 | 0.020 | 0.022 | 0.375 | −0.123 | 0.079 | 0.139 | −0.014 | 0.051 | 0.793 | |||
| Model 3 | 0.015 | 0.023 | 0.504 | −0.092 | 0.069 | 0.203 | −0.024 | 0.054 | 0.665 | |||
| Index | Healthy Controls | T2DM | NODAP | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | S.E. | p | R2 | β | S.E. | p | R2 | β | S.E. | p | R2 | |
| HOMA-IS | ||||||||||||
| Model 1 | −0.018 | 0.292 | 0.950 | <0.001 | −0.150 | 0.068 | 0.039 | 0.206 | −0.456 | 0.120 | 0.031 | 0.172 |
| Model 2 | 0.022 | 0.333 | 0.949 | −0.186 | 0.081 | 0.037 | −0.444 | 0.229 | 0.067 | |||
| Model 3 | 0.144 | 0.375 | 0.705 | −0.154 | 0.080 | 0.072 | −0.409 | 0.237 | 0.099 | |||
| Raynaud index | ||||||||||||
| Model 1 | 0.238 | 0.069 | 0.732 | 0.005 | −2.224 | 1.211 | 0.082 | 0.151 | −10.998 | 7.605 | 0.161 | 0.077 |
| Model 2 | 0.598 | 0.742 | 0.428 | −2.751 | 1.464 | 0.078 | −12.773 | 8.673 | 0.154 | |||
| Model 3 | 0.797 | 0.829 | 0.347 | −2.542 | 1.537 | 0.118 | −12.364 | 9.067 | 0.187 | |||
| Matsuda index | ||||||||||||
| Model 1 | 5.535 | 12.654 | 0.668 | 0.012 | −7.577 | 3.994 | 0.107 | 0.375 | −23.061 | 8.034 | 0.012 | 0.355 |
| Model 2 | 4.132 | 14.863 | 0.785 | −9.099 | 5.814 | 0.193 | −28.311 | 12.408 | 0.040 | |||
| Model 3 | 2.477 | 16.795 | 0.885 | −2.757 | 5.570 | 0.655 | −27.023 | 13.948 | 0.077 | |||
| TyG | ||||||||||||
| Model 1 | 0.171 | 0.176 | 0.341 | 0.035 | 0.348 | 0.107 | 0.024 | 0.254 | 1.200 | 0.249 | <0.001 | 0.491 |
| Model 2 | 0.062 | 0.175 | 0.725 | 0.744 | 0.316 | 0.031 | 1.130 | 0.287 | 0.001 | |||
| Model 3 | −0.035 | 0.191 | 0.858 | 0.566 | 0.288 | 0.068 | 1.129 | 0.300 | 0.001 | |||
| Index | Healthy Controls | T2DM | NODAP | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | S.E. | p | R2 | β | S.E. | p | R2 | β | S.E. | p | R2 | ||
| HOMA-IS | |||||||||||||
| Model 1 | 0.198 | 0.196 | 0.323 | 0.044 | 0.068 | 0.071 | 0.354 | 0.045 | −0.429 | 0.199 | 0.041 | 0.041 | |
| Model 2 | 0.167 | 0.212 | 0.441 | 0.070 | 0.090 | 0.448 | −0.506 | 0.202 | 0.020 | ||||
| Model 3 | 0.156 | 0.217 | 0.480 | 0.037 | 0.085 | 0.669 | −0.4882 | 0.206 | 0.029 | ||||
| Raynaud index | |||||||||||||
| Model 1 | 0.021 | 0.465 | 0.964 | <0.001 | 1.191 | 1.228 | 0.344 | 0.047 | −14.182 | 7.277 | 0.062 | 0.132 | |
| Model 2 | −0.082 | 0.485 | 0.867 | 1.253 | 1.153 | 0.428 | −15.249 | 7.745 | 0.061 | ||||
| Model 3 | −0.089 | 0.497 | 0.859 | 1.001 | 1.593 | 0.539 | −14.956 | 8.003 | 0.075 | ||||
| Matsuda index | |||||||||||||
| Model 1 | 3.809 | 9.310 | 0.688 | 0.010 | 5.884 | 4.586 | 0.247 | 0.215 | −20.765 | 9.198 | 0.039 | 0.254 | |
| Model 2 | 4.974 | 10.007 | 0.627 | 6.144 | 6.212 | 0.379 | −22.220 | 8.726 | 0.024 | ||||
| Model 3 | 5.841 | 10.500 | 0.588 | 2.925 | 4.375 | 0.543 | −21.074 | 9.105 | 0.039 | ||||
| TyG | |||||||||||||
| Model 1 | 0.001 | 0.121 | 0.994 | <0.001 | −0.341 | 0.272 | 0.225 | 0.081 | 0.629 | 0.325 | 0.065 | 0.135 | |
| Model 2 | 0.075 | 0.112 | 0.509 | −0.352 | 0.344 | 0.322 | 0.812 | 0.295 | 0.012 | ||||
| Model 3 | 0.086 | 0.111 | 0.444 | −0.193 | 0.305 | 0.536 | 0.797 | 0.304 | 0.016 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ko, J.; Skudder-Hill, L.; Cho, J.; Bharmal, S.H.; Petrov, M.S. The Relationship between Abdominal Fat Phenotypes and Insulin Resistance in Non-Obese Individuals after Acute Pancreatitis. Nutrients 2020, 12, 2883. https://doi.org/10.3390/nu12092883
Ko J, Skudder-Hill L, Cho J, Bharmal SH, Petrov MS. The Relationship between Abdominal Fat Phenotypes and Insulin Resistance in Non-Obese Individuals after Acute Pancreatitis. Nutrients. 2020; 12(9):2883. https://doi.org/10.3390/nu12092883
Chicago/Turabian StyleKo, Juyeon, Loren Skudder-Hill, Jaelim Cho, Sakina H. Bharmal, and Maxim S. Petrov. 2020. "The Relationship between Abdominal Fat Phenotypes and Insulin Resistance in Non-Obese Individuals after Acute Pancreatitis" Nutrients 12, no. 9: 2883. https://doi.org/10.3390/nu12092883
APA StyleKo, J., Skudder-Hill, L., Cho, J., Bharmal, S. H., & Petrov, M. S. (2020). The Relationship between Abdominal Fat Phenotypes and Insulin Resistance in Non-Obese Individuals after Acute Pancreatitis. Nutrients, 12(9), 2883. https://doi.org/10.3390/nu12092883