Pre-Sleep Low Glycemic Index Modified Starch Does Not Improve Next-Morning Fuel Selection or Running Performance in Male and Female Endurance Athletes

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. General Procedures
2.3. Supplementation
2.4. Familiarization Protocol
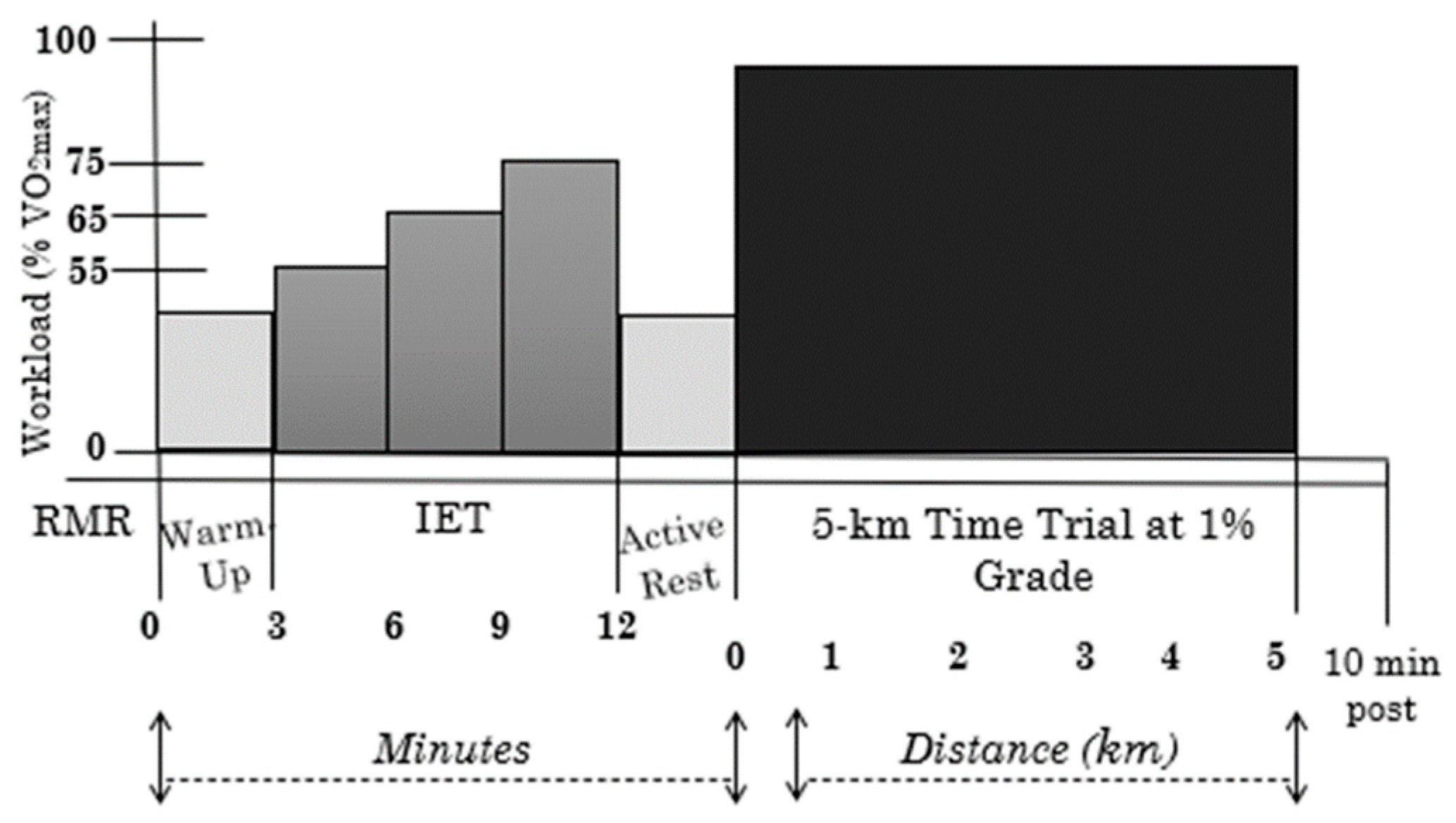
2.5. Experimental Protocol
2.6. Incremental Exercise Test and 5-km Time Trial
2.7. Statistical Analysis
3. Results
3.1. Participants
3.2. Effects of Supplement on Baseline Measures
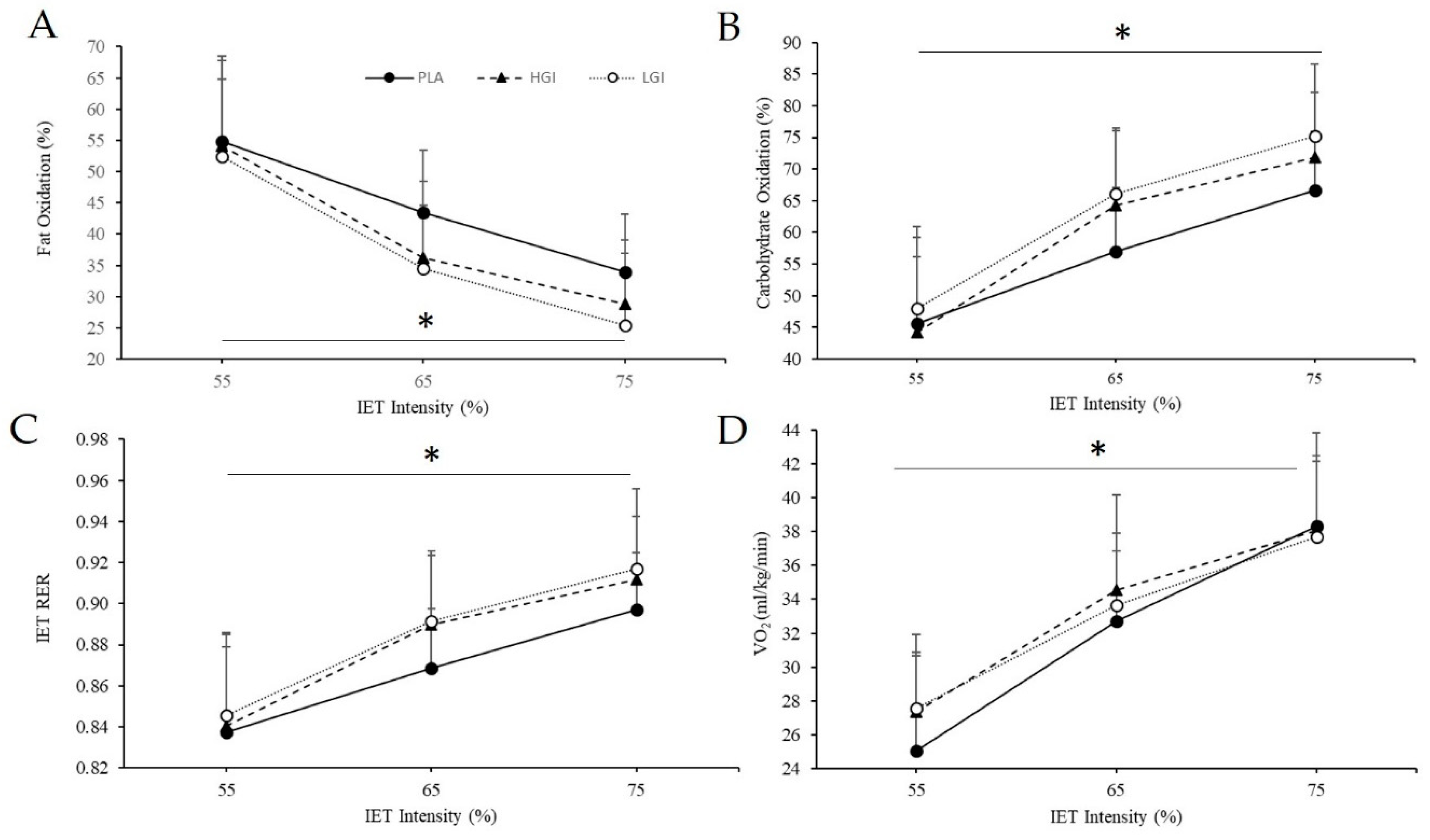
3.3. Effects of Supplement on the Response to the Incremental Exercise Test (IET)
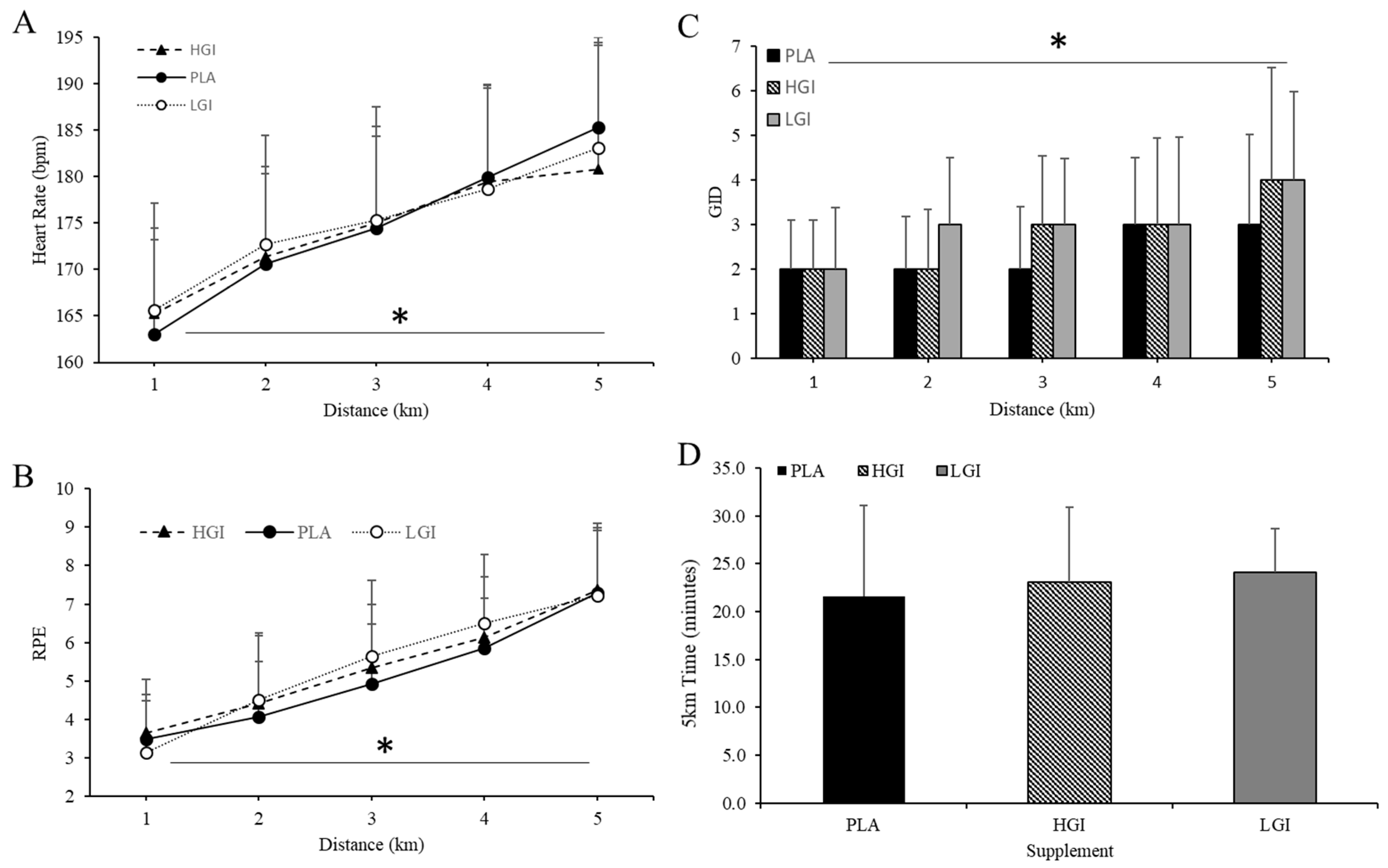
3.4. Effect of Supplement on 5-km TT
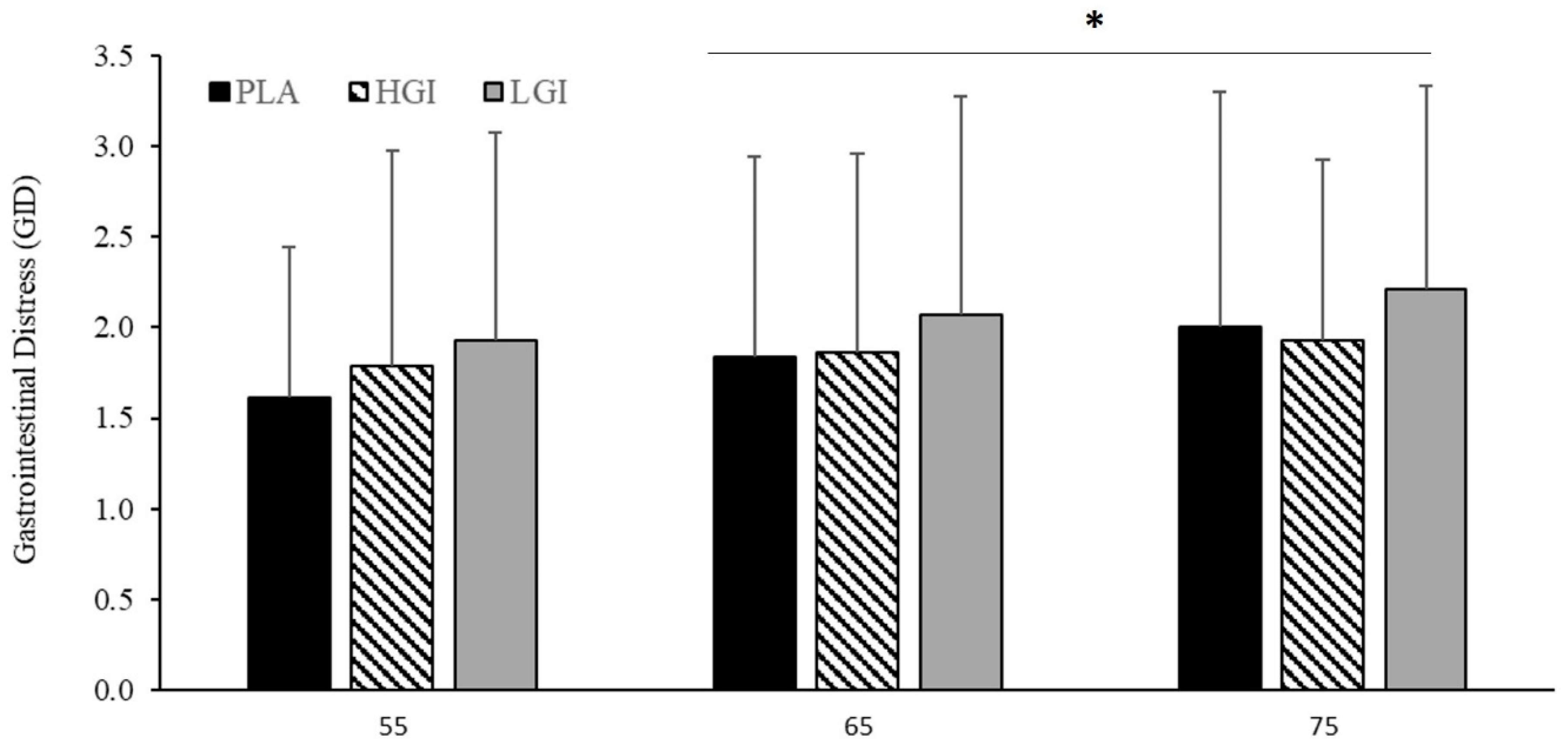
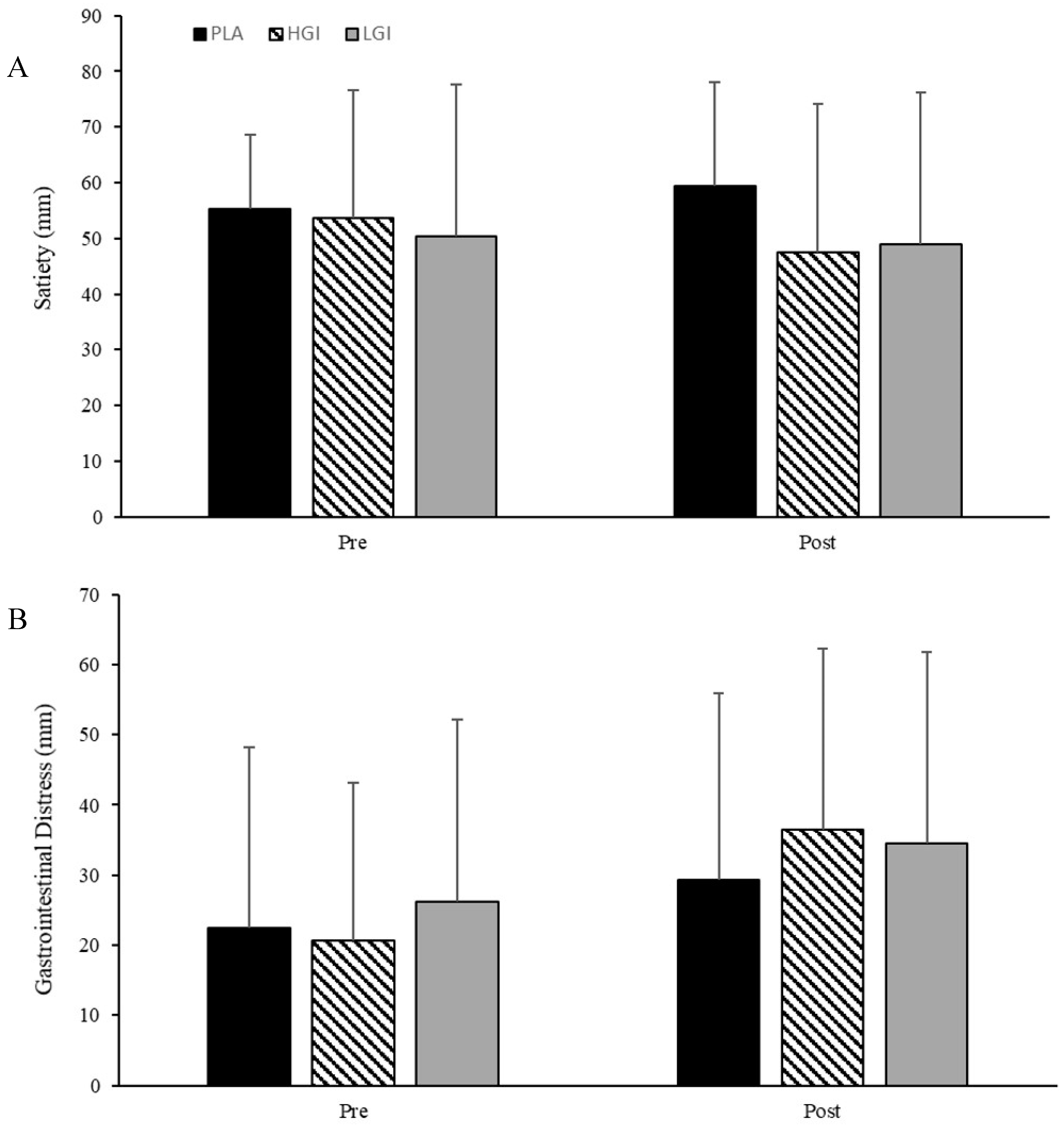
3.5. Effect of Supplement on Perceptual Responses of GID and Satiety to Exercise
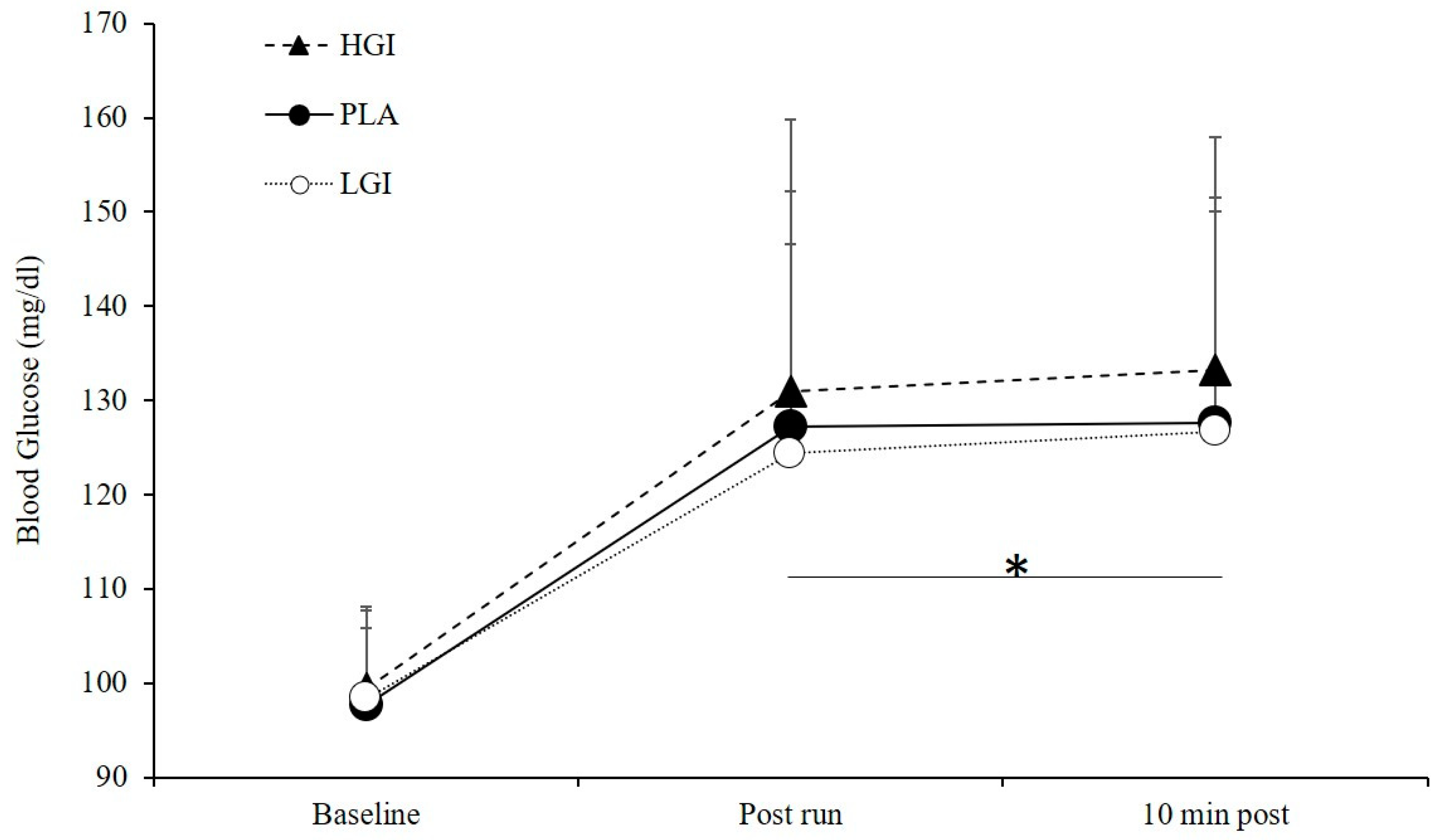
3.6. Blood Glucose (BG)
4. Discussion
Experimental Considerations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chryssanthopoulos, C.; Williams, C. Pre-exercise carbohydrate meal and endurance running capacity when carbohydrates are ingested during exercise. Int. J. Sports Med. 1997, 18, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Chryssanthopoulos, C.; Williams, C.; Nowitz, A.; Kotsiopoulou, C.; Vleck, V. The effect of a high carbohydrate meal on endurance running capacity. Int. J. Sport Nutr. Exerc. Metab. 2002, 12, 157. [Google Scholar] [CrossRef] [PubMed]
- Heung-Sang Wong, S.; Sun, F.; Chen, Y.; Li, C.; Zhang, Y.; Ya-Jun Huang, W. Effect of pre-exercise carbohydrate diets with high vs low glycemic index on exercise performance: A meta-analysis. Nutr. Rev. 2017, 75, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Neufer, P.D.; Costill, D.L.; Flynn, M.G.; Kirwan, J.P.; Mitchell, J.B.; Houmard, J. Improvements in exercise performance: Effects of carbohydrate feedings and diet. J. Appl. Physiol. 1987, 62, 983–988. [Google Scholar] [CrossRef]
- Thomas, D.; Brotherhood, J.; Brand, J. Carbohydrate feeding before exercise: Effect of glycemic index. Int. J. Sports Med. 1991, 12, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Wright, D.A.; Sherman, W.M.; Dernbach, A.R. Carbohydrate feedings before, during, or in combination improve cycling endurance performance. J. Appl. Physiol. 1991, 71, 1082–1088. [Google Scholar] [CrossRef] [PubMed]
- Ho, G.W.K. Lower gastrointestinal distress in endurance athletes. Curr. Sports Med. Rep. 2009, 8, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Peters, H.P.; Bos, M.; Seebregts, L.; Akkermans, L.M.; Henegouwen, G.v.B.; Bol, E.; Mosterd, W.L.; Vries, W.R. Gastrointestinal symptoms in long-distance runners, cyclists, and triathletes: Prevalence, medication, and etiology. Am. J. Gastroenterol. 1999, 94, 1570–1581. [Google Scholar] [CrossRef]
- Peters, H.P.; Zweers, M.; Backx, F.; Bol, E.; Hendriks Mosterd, W.L.; De Vries, W.R. Gastrointestinal symptoms during long-distance walking. Med. Sci. Sports Exerc. 1999, 31, 767–773. [Google Scholar] [CrossRef]
- Pfeiffer, B.; Stellingwerff, T.; Hodgson, A.B.; Randell, R.; Pöttgen, K.; Res, P.; Jeukendrup, A.E. Nutritional intake and gastrointestinal problems during competitive endurance events. Med. Sci. Sports Exerc. 2012, 44, 344–351. [Google Scholar] [CrossRef] [Green Version]
- Rehrer, N.J.; van Kemenade, M.; Meester, W.; Brouns, F.; Saris, W.H. Gastrointestinal complaints in relation to dietary intake in triathletes. Int. J. Sport Nutr. Exerc. Metab. 1992, 2, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Jeukendrup, A.E. Carbohydrate intake during exercise and performance. Nutrition 2004, 20, 669–677. [Google Scholar] [CrossRef] [PubMed]
- Halson, S.L.; Lancaster, G.I.; Achten, J.; Gleeson, M.; Jeukendrup, A.E. Effects of carbohydrate supplementation on performance and carbohydrate oxidation after intensified cycling training. J. Appl. Physiol. 2004, 97, 1245–1253. [Google Scholar] [CrossRef] [Green Version]
- Lehmann, U.; Robin, F. Slowly digestible starch—Its structure and health implications: A review. Trends Food Sci. Technol. 2007, 18, 346–355. [Google Scholar] [CrossRef]
- Baur, D.A.; de Vargas Fernanda, C.S.; Bach, C.W.; Garvey, J.A.; Ormsbee, M.J. Slow-absorbing modified starch before and during prolonged cycling increases fat oxidation and gastrointestinal distress without changing performance. Nutrients 2016, 8, 392. [Google Scholar] [CrossRef] [Green Version]
- Bennard, P.; Doucet, E. Acute effects of exercise timing and breakfast meal glycemic index on exercise-induced fat oxidation. Appl. Physiol. Nutr. Metab. 2006, 31, 502–511. [Google Scholar] [CrossRef]
- Roberts, M.D.; Lockwood, C.; Dalbo, V.J.; Volek, J.; Kerksick, C.M. Ingestion of a high-molecular-weight hydrothermally modified waxy maize starch alters metabolic responses to prolonged exercise in trained cyclists. Nutrition 2011, 27, 659–665. [Google Scholar] [CrossRef]
- Sun, F.; O’Reilly, J.; Li, L.; Wong, S.H. Effect of the glycemic index of pre-exercise snack bars on substrate utilization during subsequent exercise. Int. J. Food Sci. Nutr. 2013, 64, 1001–1006. [Google Scholar] [CrossRef]
- Moore, L.J.S.; Midgley, A.W.; Thurlow, S.; Thomas, G.; Mc Naughton, L.R. Effect of the glycaemic index of a pre-exercise meal on metabolism and cycling time trial performance. J. Sci. Med. Sport 2009, 13, 182–188. [Google Scholar] [CrossRef]
- Backhouse, S.H.; Williams, C.; Stevenson, E.; Nute, M. Effects of the glycemic index of breakfast on metabolic responses to brisk walking in females. Eur. J. Clin. Nutr. 2007, 61, 590–596. [Google Scholar] [CrossRef] [Green Version]
- Baur, D.A.; Willingham, B.D.; Smith, K.A.; Kisiolek, J.N.; Morrissey, M.C.; Saracino, P.G.; Ragland, T.J.; Ormsbee, M.J. Adipose Lipolysis Unchanged by Preexercise Carbohydrate Regardless of Glycemic Index. Med. Sci. Sports Exerc. 2018, 50, 827–836. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, E.; Williams, C.; Nute, M.; Humphrey, L.; Witard, O. Influence of the glycaemic index of an evening meal on substrate oxidation following breakfast and during exercise the next day in healthy women. Eur. J. Clin. Nutr. 2008, 62, 608–616. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, E.; Williams, C.; Nute, M.; Swaile, P.; Tsui, M. The effect of the glycemic index of an evening meal on the metabolic responses to a standard high glycemic index breakfast and subsequent exercise in men. Int. J. Sport Nutr. Exerc. Metab. 2005, 15, 308–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The UCAN Company. SuperStarch®. Available online: https://www.generationucan.com/superstarch/ (accessed on 22 April 2019).
- Bhattacharya, K.; Orton, R.; Qi, X.; Mundy, H.; Morley, D.; Champion, M.; Eaton, S.; Tester, R.; Lee, P. A novel starch for the treatment of glycogen storage diseases. J. Inherit. Metab. Dis. 2007, 30, 350–357. [Google Scholar] [CrossRef]
- Correia, C.E.; Bhattacharya, K.; Lee, P.J.; Shuster, J.J.; Theriaque, D.W.; Shankar, M.N.; Smit, G.P.A.; Weinstein, D.A. Use of modified cornstarch therapy to extend fasting in glycogen storage disease types Ia and Ib. Am. J. Clin. Nutr. 2008, 88, 1272–1276. [Google Scholar] [PubMed]
- Johannsen, N.M.; Sharp, R.L. Effect of pre-exercise ingestion of modified cornstarch on substrate oxidation during endurance exercise. Int. J. Sport Nutr. Exerc. Metab. 2007, 17, 232. [Google Scholar] [CrossRef] [Green Version]
- Ormsbee, M.J.; Contreras, R.J.; Spicer, M.T.; Miller, E.A.; Eckel, L.A.; Baur, D.A.; Gorman, K.A.; Panton, L.B. Nighttime feeding likely alters morning metabolism but not exercise performance in female athletes. Appl. Physiol. Nutr. Metab. 2016, 41, 719–727. [Google Scholar] [CrossRef]
- Tseh, W.; Caputo, J.L.; Keefer, D.J. Validity and reliability of the BOD POD® S/T tracking system. Int. J. Sports Med. 2010, 10, 704–708. [Google Scholar] [CrossRef]
- Crouter, S.E.; Antczak, A.; Hudak, J.R.; DellaValle, D.M.; Haas, J.D. Accuracy and reliability of the ParvoMedics TrueOne 2400 and MedGraphics VO2000 metabolic systems. Eur. J. Appl. Physiol. 2006, 98, 139–151. [Google Scholar] [CrossRef]
- Averbuch, M.; Katzper, M. Assessment of visual analog versus categorical scale for measurement of osteoarthritis pain. J. Clin. Pharm. 2004, 44, 368–372. [Google Scholar] [CrossRef]
- Bijur, P.E.; Silver, W.; Gallagher, E.J. Reliability of the visual analog scale for measurement of acute pain. Acad. Emerg. Med. 2001, 8, 1153–1157. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, E.J.; Bijur, P.E.; Latimer, C.; Silver, W. Reliability and validity of a visual analog scale for acute abdominal pain in the ED. Am. J. Emerg. Med. 2002, 20, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Frayn, K.N. Calculation of substrate oxidation rates in vivo from gaseous exchange. J. Appl. Physiol. 1983, 55, 628–634. [Google Scholar] [CrossRef] [Green Version]
- Halldorsdottir, S.; Warchal-Windham, M.E.; Wallace, J.F.; Pardo, S.; Parkes, J.L.; Simmons, D.A. Accuracy evaluation of five blood glucose monitoring systems: The north american comparator trial. J. Diabetes Sci. Technol. 2013, 7, 1294–1304. [Google Scholar] [CrossRef] [Green Version]
- Jäger, R.; Kerksick, C.M.; Campbell, B.I.; Cribb, P.J.; Wells, S.D.; Skwiat, T.M.; Purpura, M.; Ziegenfuss, T.N.; Ferrando, A.A.; Arent, S.M.; et al. International society of sports nutrition position stand: Protein and exercise. J. Int. Soc. Sports Nutr. 2017, 14, 20. [Google Scholar] [CrossRef] [Green Version]
- Laursen, P.B.; Francis, G.T.; Abbiss, C.R.; Newton, M.J.; Nosaka, K. Reliability of time-to-exhaustion versus time-trial running tests in runners. Med. Sci. Sports Exerc. 2007, 39, 1374–1379. [Google Scholar] [CrossRef]
- Jones, A.M.; Doust, J.H. A 1% treadmill grade most accurately reflects the energetic cost of outdoor running. J. Sports Sci. 2007, 14, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Kirwan, J.P.; Cyr-Campbell, D.; Campbell, W.W.; Scheiber, J.; Evans, W.J. Effects of moderate and high glycemic index meals on metabolism and exercise performance. Metabolism 2001, 50, 849–855. [Google Scholar] [CrossRef]
- Sherman, W.M.; Peden, M.C.; Wright, D.A. Carbohydrate feedings 1 h before exercise improves cycling performance. Am. J. Clin. Nutr. 1991, 54, 866–870. [Google Scholar] [CrossRef] [Green Version]
- Sparks, M.; Selig, S.; Febbraio, M. Pre-exercise carbohydrate ingestion: Effect of the glycemic index on endurance exercise performance. Med. Sci. Sports Exerc. 1998, 30, 844–849. [Google Scholar] [CrossRef]
- Wee, S.L.; Williams, C.; Gray, S.; Horabin, J. Influence of high and low glycemic index meals on endurance running capacity. Med. Sci. Sports Exerc. 1999, 31, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Williams, C. A low glycemic index meal before exercise improves endurance running capacity in men. Int. J. Sport Nutr. Exerc. Metab. 2006, 16, 510–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, L.J.S.; Midgley, A.W.; Thomas, G.; Thurlow, S.; McNaughton, L.R. The effects of low- and high-glycemic index meals on time trial performance. Int. J. Sports Physiol. Perform. 2009, 4, 331–344. [Google Scholar] [CrossRef]
- DeMarco, H.M.; Sucher, K.P.; Cisar, C.J.; Butterfield, G.E. Pre-exercise carbohydrate meals: Application of glycemic index. Med. Sci. Sports Exerc. 1999, 31, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.H.S.; Siu, P.M.; Lok, A.; Chen, Y.J.; Morris, J.; Lam, C.W. Effect of the glycaemic index of pre-exercise carbohydrate meals on running performance. Eur. J. Sport Sci. 2008, 8, 23–33. [Google Scholar] [CrossRef]
- Febbraio, M.A.; Keenan, J.; Angus, D.J.; Campbell, S.E.; Garnham, A.P. Pre-exercise carbohydrate ingestion, glucose kinetics, and muscle glycogen use: Effect of the glycemic index. J. Appl. Physiol. 2000, 89, 1845–1851. [Google Scholar] [CrossRef] [Green Version]
- Jentjens, R.; Jeukendrup, A. Effects of pre-exercise ingestion of trehalose, galactose and glucose on subsequent metabolism and cycling performance. Eur. J. Appl. Physiol. 2003, 88, 459–465. [Google Scholar] [CrossRef]
- Kern, M.; Heslin, C.J.; Rezende, R.S. Metabolic and performance effects of raisins versus sports gel as pre-exercise feedings in cyclists. J. Strength Cond. Res. 2007, 21, 1204. [Google Scholar]
- Stannard, S.R.; Constantini, N.W.; Miller, J.C. The Effect of Glycemic Index on Plasma Glucose and Lactate Levels during Incremental Exercise. Int. J. Sport Nutr. Exerc. Metab. 2000, 10, 51–61. [Google Scholar] [CrossRef]
- Romijn, J.A.; Coyle, E.F.; Sidossis, L.S.; Gastaldelli, A.; Horowitz, J.F.; Endert, E.; Wolfe, R.R. Regulation of endogenous fat and carbohydrate metabolism in relation to exercise intensity and duration. Am. J. Physiol. Endocrinol. Metab. 1993, 265, E380–E391. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.J.; Wong, S.H.S.; Chan, C.O.W.; Wong, C.K.; Lam, C.W.; Siu, P.M.F. Effects of glycemic index meal and CHO-electrolyte drink on cytokine response and run performance in endurance athletes. J. Sci. Med. Sport 2008, 12, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Chryssanthopoulos, C.; Hennessy, L.C.; Williams, C. The influence of pre-exercise glucose ingestion on endurance running capacity. Br. J. Sports Med. 1994, 28, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Koivisto, V.A.; Karonen, S.L.; Nikkila, E.A. Carbohydrate ingestion before exercise: Comparison of glucose, fructose, and sweet placebo. J. Appl. Physiol. 1981, 51, 783–787. [Google Scholar] [CrossRef] [PubMed]
- Marmy-Conus, N.; Fabris, S.; Proietto, J.; Hargreaves, M. Pre-exercise glucose ingestion and glucose kinetics during exercise. J. Appl. Physiol. 1996, 81, 853–857. [Google Scholar] [CrossRef] [PubMed]
- Ahlborg, G.; Felig, P.; Hagenfeldt, L.; Hendler, R.; Wahren, J. Substrate turnover during prolonged exercise in man. Splanchnic and leg metabolism of glucose, free fatty acids, and amino acids. J. Clin. Investig. 1974, 53, 1080–1090. [Google Scholar] [CrossRef] [PubMed]
- Gollnick, P.D.; Piehl, K.; Saltin, B. Selective glycogen depletion pattern in human muscle fibres after exercise of varying intensity and at varying pedalling rates. J. Physiol. 1974, 241, 45–57. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Combined | Male | Female |
|---|---|---|---|
| Sex (n, M/F) | 14 | 8 | 6 |
| Age (years) | 28 ± 9 | 29 ± 9 | 27 ± 10 |
| Height (cm) | 169.3 ± 10.4 | 176.0 ± 7.1 | 160.4 ± 6.8 * |
| Weight (kg) | 64.3 ± 9.8 | 70.1 ± 7.8 | 56.5 ± 6.2 * |
| Body fat (%) | 18.9 ± 5.6 | 14.7 ± 3.5 | 23.9 ± 2.5 * |
| VO2peak (mL·kg−1·min−1) | 55.4 ± 6.9 | 59.5 ± 5.5 | 49.9 ± 4.3 * |
| Supplement | ||||
|---|---|---|---|---|
| Variable | PLA | HGI | LGI | p Value |
| Visual Analogue Scale (VAS) (mm) | ||||
| Gastrointestinal Distress (GID) | 22.4 ± 25.8 | 20.6 ± 22.5 | 26.2 ± 26.0 | 0.59 |
| Satiety | 55.3 ± 13.3 | 53.6 ± 23.0 | 50.3 ± 27.2 | 0.73 |
| Substrate Oxidation | ||||
| FAT (%) | 47.3 ± 9.5 | 41.4 ± 16.8 | 42.7 ± 17.8 | 0.16 |
| Carbohydrate (CHO) (%) | 53.2 ± 9.6 | 59.1 ± 16.9 | 57.8 ± 18.0 | 0.16 |
| VO2 (mL/kg/min) | 3.9 ± 0.4 | 3.8 ± 0.4 | 3.8 ± 0.4 | 0.84 |
| Resting Energy Expenditure (REE) (kcal·day−1) | 1689 ± 278 | 1701 ± 308 | 1732 ± 287 | 0.72 |
| HR (bpm) | 57.7 ± 8.8 | 57.3 ± 10.6 | 59.9 ± 10.0 | 0.06 |
| Blood Glucose (BG) (mg·dL−1) | 97.7 ± 8.1 | 99.4 ± 8.8 | 98.4 ± 9.3 | 0.85 |
| Urine Specific Gravity (USG) (a.u.) | 1.02 ± 0.01 | 1.02 ± 0.01 | 1.02 ± 0.01 | 0.91 |
| Sleep (h) | 7.2 ± 0.8 | 7.2 ± 0.9 | 6.9 ± 1.2 | 0.68 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dudar, M.D.; Bode, E.D.; Fishkin, K.R.; Brown, R.A.; Carre, M.M.; Mills, N.R.; Ormsbee, M.J.; Ives, S.J. Pre-Sleep Low Glycemic Index Modified Starch Does Not Improve Next-Morning Fuel Selection or Running Performance in Male and Female Endurance Athletes. Nutrients 2020, 12, 2888. https://doi.org/10.3390/nu12092888
Dudar MD, Bode ED, Fishkin KR, Brown RA, Carre MM, Mills NR, Ormsbee MJ, Ives SJ. Pre-Sleep Low Glycemic Index Modified Starch Does Not Improve Next-Morning Fuel Selection or Running Performance in Male and Female Endurance Athletes. Nutrients. 2020; 12(9):2888. https://doi.org/10.3390/nu12092888
Chicago/Turabian StyleDudar, Monique D., Emilie D. Bode, Karly R. Fishkin, Rochelle A. Brown, Madeleine M. Carre, Noa R. Mills, Michael J. Ormsbee, and Stephen J. Ives. 2020. "Pre-Sleep Low Glycemic Index Modified Starch Does Not Improve Next-Morning Fuel Selection or Running Performance in Male and Female Endurance Athletes" Nutrients 12, no. 9: 2888. https://doi.org/10.3390/nu12092888
APA StyleDudar, M. D., Bode, E. D., Fishkin, K. R., Brown, R. A., Carre, M. M., Mills, N. R., Ormsbee, M. J., & Ives, S. J. (2020). Pre-Sleep Low Glycemic Index Modified Starch Does Not Improve Next-Morning Fuel Selection or Running Performance in Male and Female Endurance Athletes. Nutrients, 12(9), 2888. https://doi.org/10.3390/nu12092888