
Family Socioecological Correlates of Lifestyle Patterns in Early Childhood: A Cross-Sectional Study from the EDEN Mother–Child Cohort

 , , , ,
, , , ,  , , and
, , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Measurements
2.2.1. EBRBs
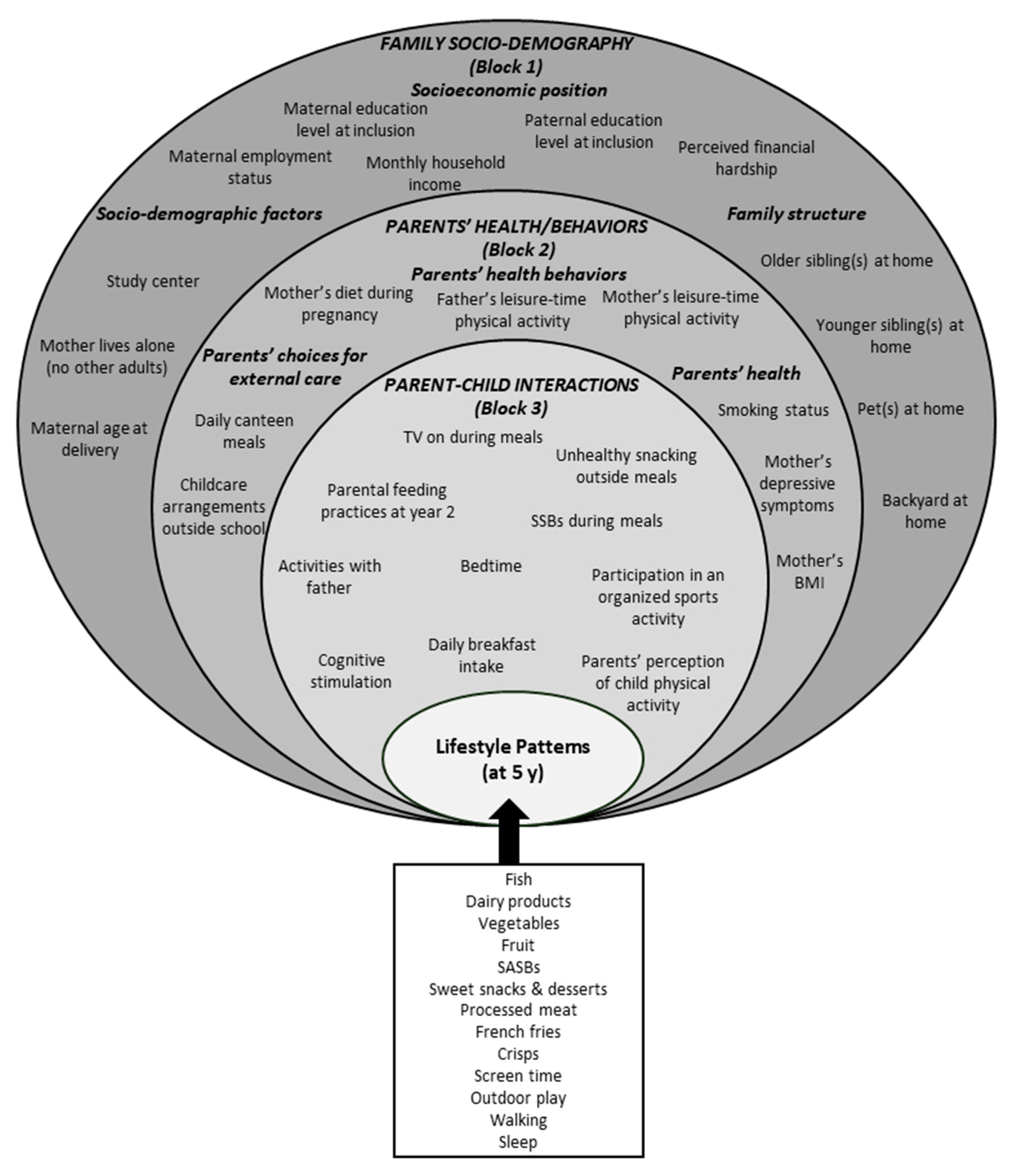
2.2.2. Family Socio-Ecological Correlates
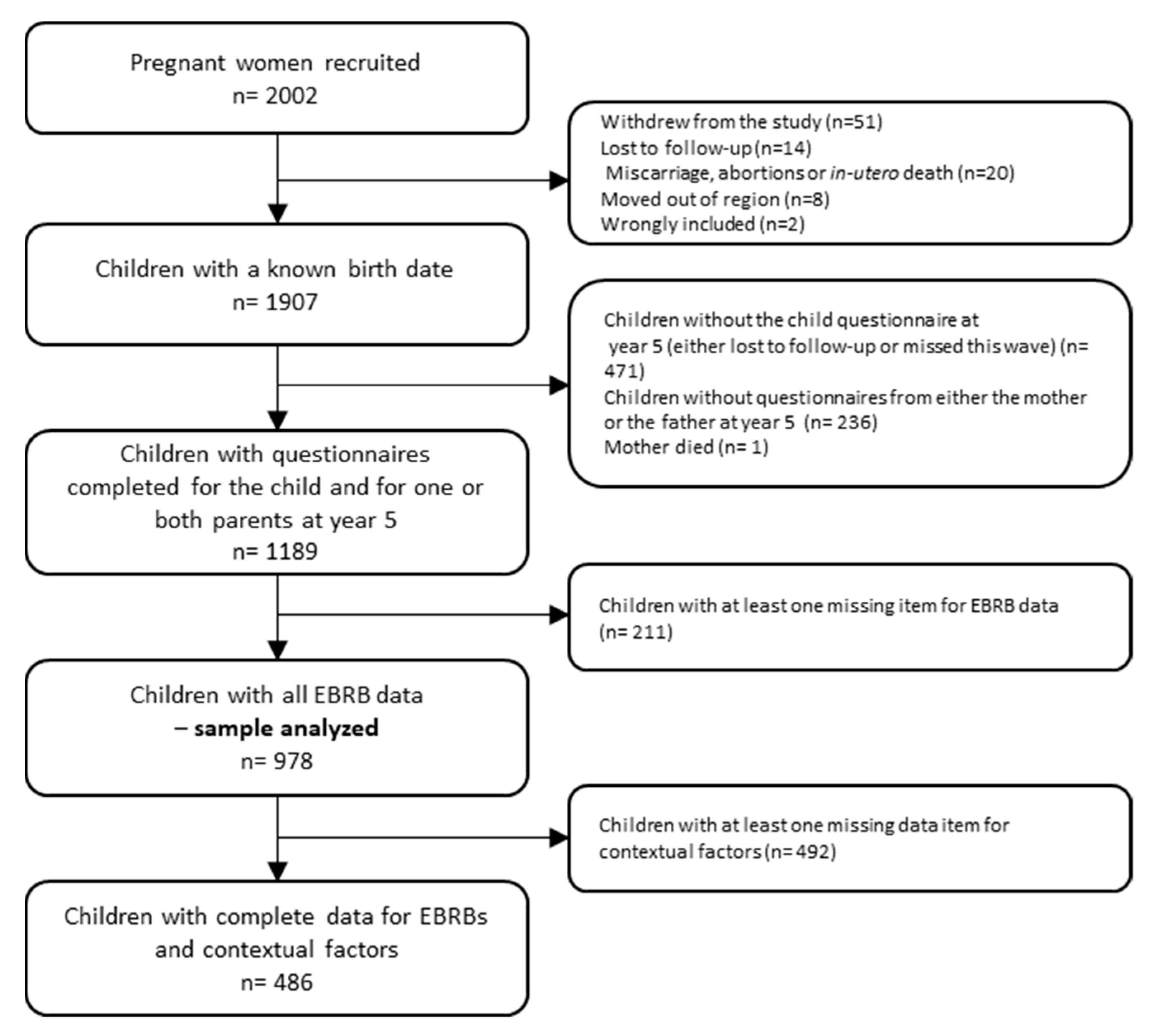
2.3. Study Sample
2.4. Statistical Analysis
2.4.1. Participant Characteristics
2.4.2. Lifestyle Patterns
2.4.3. Hierarchical Linear Regression
2.4.4. Handling Missing Data
3. Results
3.1. Participants Characteristics
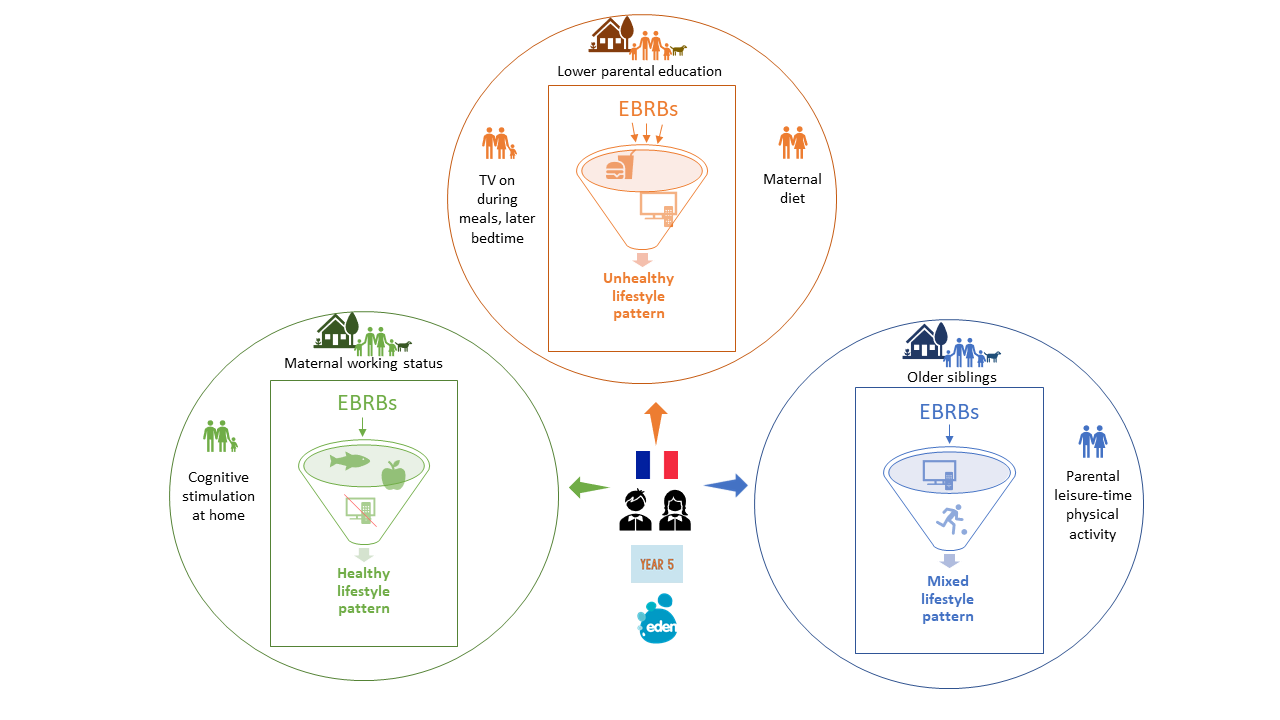
3.2. Lifestyle Patterns
3.3. Hierarchical Linear Regression
3.4. Sensitivity Analyses
4. Discussion
4.1. Lifestyle Patterns
4.2. Socio-Ecological Correlates of Lifestyle Patterns
4.2.1. Family Socio-Demography
4.2.2. Parents’ Health/Behaviors
4.2.3. Parent-Child Interactions
4.3. Public Health Implications
4.4. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Obesity and Overweight. Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 25 January 2021).
- Olds, T.; Maher, C.; Zumin, S.; Péneau, S.; Lioret, S.; Castetbon, K.; Bellisle; De Wilde, J.; Hohepa, M.; Maddison, R.; et al. Evidence that the prevalence of childhood overweight is plateauing: Data from nine countries. Pediatr. Obes. 2011, 6, 342–360. [Google Scholar] [CrossRef]
- Ayala-Marín, A.M.; Iguacel, I.; De Miguel-Etayo, P.; Moreno, L.A. Consideration of Social Disadvantages for Understanding and Preventing Obesity in Children. Front. Public Health 2020, 8, 423. [Google Scholar] [CrossRef]
- Reilly, J.J.; Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int. J. Obes. 2011, 35, 891–898. [Google Scholar] [CrossRef] [Green Version]
- Poorolajal, J.; Sahraei, F.; Mohamdadi, Y.; Doosti-Irani, A.; Moradi, L. Behavioral factors influencing childhood obesity: A systematic review and meta-analysis. Obes. Res. Clin. Pract. 2020, 14, 109–118. [Google Scholar] [CrossRef]
- Prochaska, J.J.; Prochaska, J.O. A Review of Multiple Health Behavior Change Interventions for Primary Prevention. Am. J. Lifestyle Med. 2011, 5, 208–221. [Google Scholar] [CrossRef]
- Gubbels, J.S.; van Assema, P.; Kremers, S.P.J. Physical Activity, Sedentary Behavior, and Dietary Patterns among Children. Curr. Nutr. Rep. 2013, 2, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Leech, R.M.; A McNaughton, S.; Timperio, A. The clustering of diet, physical activity and sedentary behavior in children and adolescents: A review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 4. [Google Scholar] [CrossRef] [Green Version]
- D’Souza, N.J.; Kuswara, K.; Zheng, M.; Leech, R.; Downing, K.L.; Lioret, S.; Campbell, K.J.; Hesketh, K.D. A systematic review of lifestyle patterns and their association with adiposity in children aged 5–12 years. Obes. Rev. 2020, 21, e13029. [Google Scholar] [CrossRef]
- Liberali, R.; Del Castanhel, F.; Kupek, E.; De Assis, M.A.A. Latent Class Analysis of Lifestyle Risk Factors and Association with Overweight and/or Obesity in Children and Adolescents: Systematic Review. Child. Obes. 2021, 17, 2–15. [Google Scholar] [CrossRef]
- Johnson, S.S.; Paiva, A.L.; Cummins, C.O.; Johnson, J.L.; Dyment, S.J.; Wright, J.A.; Prochaska, J.O.; Prochaska, J.M.; Sherman, K. Transtheoretical Model-based multiple behavior intervention for weight management: Effectiveness on a population basis. Prev. Med. 2008, 46, 238–246. [Google Scholar] [CrossRef] [Green Version]
- Magee, C.A.; Lee, J.K.; Vella, S.A. Bidirectional Relationships between Sleep Duration and Screen Time in Early Childhood. JAMA Pediatr. 2014, 168, 465–470. [Google Scholar] [CrossRef] [Green Version]
- Kaar, J.L.; Schmiege, S.J.; Vadiveloo, M.; Simon, S.L.; Tovar, A. Sleep duration mediates the relationship between health behavior patterns and obesity. Sleep Health 2018, 4, 442–447. [Google Scholar] [CrossRef] [Green Version]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: London, UK; Cambridge, MA, USA, 1981. [Google Scholar]
- Davison, K.K.; Birch, L.L. Childhood overweight: A contextual model and recommendations for future research. Obes. Rev. 2001, 2, 159–171. [Google Scholar] [CrossRef]
- Niermann, C.Y.; Gerards, S.M.; Kremers, S.P. Conceptualizing Family Influences on Children’s Energy Balance-Related Behaviors: Levels of Interacting Family Environmental Subsystems (The LIFES Framework). Int. J. Environ. Res. Public Health 2018, 15, 2714. [Google Scholar] [CrossRef] [Green Version]
- Davison, K.K.; Gicevic, S.; Aftosmes-Tobio, A.; Ganter, C.; Simon, C.L.; Newlan, S.; Manganello, J.A. Fathers’ Representation in Observational Studies on Parenting and Childhood Obesity: A Systematic Review and Content Analysis. Am. J. Public Health 2016, 106, e14–e21. [Google Scholar] [CrossRef]
- Heude, B.; Forhan, A.; Slama, R.; Douhaud, L.; Bedel, S.; Saurel-Cubizolles, M.-J.; Hankard, R.; Thiebaugeorges, O.; De Agostini, M.; Annesi-Maesano, I.; et al. Cohort Profile: The EDEN mother-child cohort on the prenatal and early postnatal determinants of child health and development. Int. J. Epidemiol. 2016, 45, 353–363. [Google Scholar] [CrossRef] [Green Version]
- Deschamps, V.; De Lauzon-Guillain, B.; Lafay, L.; Borys, J.-M.; Charles, M.A.; Romon, M. Reproducibility and relative validity of a food-frequency questionnaire among French adults and adolescents. Eur. J. Clin. Nutr. 2007, 63, 282–291. [Google Scholar] [CrossRef] [Green Version]
- Saldanha-Gomes, C.; Marbac, M.; Sedki, M.; Cornet, M.; Plancoulaine, S.; Charles, M.-A.; Lioret, S.; Dargent-Molina, P. Clusters of diet, physical activity, television exposure and sleep habits and their association with adiposity in preschool children: The EDEN mother-child cohort. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 20. [Google Scholar] [CrossRef] [Green Version]
- Davison, K.K.; Jurkowski, J.M.; A Lawson, H. Reframing family-centred obesity prevention using the Family Ecological Model. Public Health Nutr. 2013, 16, 1861–1869. [Google Scholar] [CrossRef] [Green Version]
- Victora, C.; Huttly, S.R.; Fuchs, S.C.; Olinto, M.T. The role of conceptual frameworks in epidemiological analysis: A hierarchical approach. Int. J. Epidemiol. 1997, 26, 224–227. [Google Scholar] [CrossRef] [Green Version]
- Cislak, A.; Safron, M.; Pratt, M.; Gaspar, T.; Luszczynska, A. Family-related predictors of body weight and weight-related behaviours among children and adolescents: A systematic umbrella review. Child Care Health Dev. 2011, 38, 321–331. [Google Scholar] [CrossRef]
- Cattell, R.B. The Scree Test for The Number Of Factors. Multivar. Behav. Res. 1966, 1, 245–276. [Google Scholar] [CrossRef]
- De Senna, A.F.K.; Giugliani, C.; Avilla, J.; Bizon, A.M.B.L.; Martins, A.C.M.; Giugliani, E.R.J. Maternal satisfaction with breastfeeding in the first month postpartum and associated factors. Int. Breastfeed. J. 2020, 15, 72. [Google Scholar] [CrossRef]
- Mohammed, S.H.; Habtewold, T.D.; Esmaillzadeh, A. Household, maternal, and child related determinants of hemoglobin levels of Ethiopian children: Hierarchical regression analysis. BMC Pediatr. 2019, 19, 113. [Google Scholar] [CrossRef] [Green Version]
- Seaman, S.R.; White, I.; Copas, A.; Li, L. Combining Multiple Imputation and Inverse-Probability Weighting. Biometrics 2011, 68, 129–137. [Google Scholar] [CrossRef]
- Varshney, N.; Lee, S.; Temple, J.A.; Reynolds, A.J. Does early childhood education enhance parental school involvement in second grade? Evidence from Midwest Child-Parent Center Program. Child. Youth Serv. Rev. 2020, 117, 105317. [Google Scholar] [CrossRef]
- Hilmers, A.; Hilmers, D.C.; Dave, J. Neighborhood Disparities in Access to Healthy Foods and Their Effects on Environmental Justice. Am. J. Public Health 2012, 102, 1644–1654. [Google Scholar] [CrossRef]
- Chambers, E.C.; Pichardo, M.S.; Rosenbaum, E. Sleep and the Housing and Neighborhood Environment of Urban Latino Adults Living in Low-Income Housing: The AHOME Study. Behav. Sleep Med. 2014, 14, 169–184. [Google Scholar] [CrossRef] [Green Version]
- Aggio, D.; Gardner, B.; Roberts, J.; Johnstone, J.; Stubbs, B.; Williams, G.; Sánchez, G.F.L.; Smith, L. Correlates of children’s independent outdoor play: Cross-sectional analyses from the Millennium Cohort Study. Prev. Med. Rep. 2017, 8, 10–14. [Google Scholar] [CrossRef]
- Scharte, M.; Bolte, G.; For the GME Study Group. Increased health risks of children with single mothers: The impact of socio-economic and environmental factors. Eur. J. Public Health 2013, 23, 469–475. [Google Scholar] [CrossRef] [Green Version]
- Venn, D.; Strazdins, L. Your money or your time? How both types of scarcity matter to physical activity and healthy eating. Soc. Sci. Med. 2017, 172, 98–106. [Google Scholar] [CrossRef]
- Jong, J.K.-D.; De Vries, J.H.; Bleeker, S.E.; Jaddoe, V.W.V.; Hofman, A.; Raat, H.; Moll, H.A. Socio-demographic and lifestyle determinants of ‘Western-like’ and ‘Health conscious’ dietary patterns in toddlers. Br. J. Nutr. 2013, 109, 137–147. [Google Scholar] [CrossRef] [Green Version]
- North, K.; the Avon Longitudinal Study of Pregnancy and Childhood (ALSPAC) Study Team; Emmett, P. Multivariate analysis of diet among three-year-old children and associations with socio-demographic characteristics. Eur. J. Clin. Nutr. 2000, 54, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.; Lee, S. Does Maternal Employment Affect Parental Time Allocated to Children’s Food Consumption and Physical Activity? Evidence from the Korean Time Use Survey. Int. J. Hum. Ecol. 2012, 13, 53–67. [Google Scholar] [CrossRef] [Green Version]
- Felfe, C.; Hsin, A. Maternal work conditions and child development. Econ. Educ. Rev. 2012, 31, 1037–1057. [Google Scholar] [CrossRef] [Green Version]
- Rushing, C.; Powell, L. Family Dynamics of the Stay-at-Home Father and Working Mother Relationship. Am. J. Men’s Health 2014, 9, 410–420. [Google Scholar] [CrossRef]
- Kracht, C.L.; Sisson, S.B. Sibling influence on children’s objectively measured physical activity: A meta-analysis and systematic review. BMJ Open Sport Exerc. Med. 2018, 4, e000405. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Camara, S.; on behalf the EDEN mother-child cohort study group; de Lauzon-Guillain, B.; Heude, B.; Charles, M.-A.; Botton, J.; Plancoulaine, S.; Forhan, A.; Saurel-Cubizolles, M.-J.; Dargent-Molina, P.; et al. Multidimensionality of the relationship between social status and dietary patterns in early childhood: Longitudinal results from the French EDEN mother-child cohort. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 122. [Google Scholar] [CrossRef] [Green Version]
- Cleland, V.; Venn, A.; Fryer, J.; Dwyer, T.; Blizzard, L. Parental exercise is associated with Australian children’s extracurricular sports participation and cardiorespiratory fitness: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2005, 2, 3. [Google Scholar] [CrossRef] [Green Version]
- Beets, M.W.; Cardinal, B.J.; Alderman, B. Parental Social Support and the Physical Activity-Related Behaviors of Youth: A Review. Health Educ. Behav. 2010, 37, 621–644. [Google Scholar] [CrossRef]
- Crespo, N.C.; Corder, K.; Marshall, S.; Norman, G.J.; Patrick, K.; Sallis, J.F.; Elder, J.P. An Examination of Multilevel Factors That May Explain Gender Differences in Children’s Physical Activity. J. Phys. Act. Health 2013, 10, 982–992. [Google Scholar] [CrossRef]
- Ashman, A.M.; Collins, C.E.; Hure, A.J.; Jensen, M.; Oldmeadow, C. Maternal diet during early childhood, but not pregnancy, predicts diet quality and fruit and vegetable acceptance in offspring. Matern. Child Nutr. 2014, 12, 579–590. [Google Scholar] [CrossRef]
- E Borland, S.; and the SWS Study Group; Robinson, S.M.; Crozier, S.R.; Inskip, H.M. Stability of dietary patterns in young women over a 2-year period. Eur. J. Clin. Nutr. 2007, 62, 119–126. [Google Scholar] [CrossRef] [Green Version]
- Melchior, M.; Caspi, A.; Howard, L.M.; Ambler, A.P.; Bolton, H.; Mountain, N.; Moffitt, T.E. Mental health context of food insecurity: A representative cohort of families with young children. Pediatrics 2009, 124, e564–e572. [Google Scholar]
- Potts, R.; Sanchez, D. Television viewing and depression: No news is good news. J. Broadcast. Electron. Media 1994, 38, 79–90. [Google Scholar] [CrossRef]
- Connell, A.M.; Goodman, S.H. The association between psychopathology in fathers versus mothers and children’s internalizing and externalizing behavior problems: A meta-analysis. Psychol. Bull. 2002, 128, 746–773. [Google Scholar] [CrossRef]
- Loth, K.A. Associations between Food Restriction and Pressure-to-Eat Parenting Practices and Dietary Intake in Children: A Selective Review of the Recent Literature. Curr. Nutr. Rep. 2016, 5, 61–67. [Google Scholar] [CrossRef]
- Ogden, J.; Reynolds, R.; Smith, A. Expanding the concept of parental control: A role for overt and covert control in children’s snacking behaviour? Appetite 2006, 47, 100–106. [Google Scholar] [CrossRef] [Green Version]
- Rodenburg, G.; Kremers, S.P.J.; Oenema, A.; Van De Mheen, D. Associations of parental feeding styles with child snacking behaviour and weight in the context of general parenting. Public Health Nutr. 2014, 17, 960–969. [Google Scholar] [CrossRef] [Green Version]
- Saegert, S.; Winkel, G.H. Environmental Psychology. Annu. Rev. Psychol. 1990, 41, 441–477. [Google Scholar] [CrossRef]
- Duch, H.; Fisher, E.M.; Ensari, I.; Harrington, A. Screen time use in children under 3 years old: A systematic review of correlates. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 102. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Hale, L.; Chang, A.-M.; Nahmod, N.G.; Master, L.; Berger, L.M.; Buxton, O.M. Longitudinal associations of childhood bedtime and sleep routines with adolescent body mass index. Sleep 2019, 42, zsy202. [Google Scholar] [CrossRef]
- Backholer, K.; Beauchamp, A.; Ball, K.; Turrell, G.; Martin, J.; Woods, J.; Peeters, A. A Framework for Evaluating the Impact of Obesity Prevention Strategies on Socioeconomic Inequalities in Weight. Am. J. Public Health 2014, 104, e43–e50. [Google Scholar] [CrossRef]
- Beauchamp, A.; Backholer, K.; Magliano, D.; Peeters, A. The effect of obesity prevention interventions according to socioeconomic position: A systematic review. Obes. Rev. 2014, 15, 541–554. [Google Scholar] [CrossRef]
- Wang, C.-M.; Qu, H.-Y.; Xu, H.-M. Relationship between social support and self-efficacy in women psychiatrists. Chin. Nurs. Res. 2015, 2, 103–106. [Google Scholar] [CrossRef]
- Sallis, J.F.; Saelens, B.E. Assessment of Physical Activity by Self-Report: Status, Limitations, and Future Directions. Res. Q. Exerc. Sport 2000, 71, 1–14. [Google Scholar] [CrossRef]
- Reilly, J.J.; Penpraze, V.; Hislop, J.; Davies, G.; Grant, S.; Paton, J. Objective measurement of physical activity and sedentary behaviour: Review with new data. Arch. Dis. Child. 2008, 93, 614–619. [Google Scholar] [CrossRef]
- Lioret, S.; Campbell, K.J.; McNaughton, S.A.; Cameron, A.J.; Salmon, J.; Abbott, G.; Hesketh, K.D. Lifestyle Patterns Begin in Early Childhood, Persist and Are Socioeconomically Patterned, Confirming the Importance of Early Life Interventions. Nutrients 2020, 12, 724. [Google Scholar] [CrossRef] [Green Version]
- Leech, R.; McNaughton, S.; Timperio, A. Clustering of diet, physical activity and sedentary behaviour among Australian children: Cross-sectional and longitudinal associations with overweight and obesity. Int. J. Obes. 2015, 39, 1079–1085. [Google Scholar] [CrossRef]
- Prochaska, J.J.; Spring, B.; Nigg, C.R. Multiple health behavior change research: An introduction and overview. Prev. Med. 2008, 46, 181–188. [Google Scholar] [CrossRef] [Green Version]
- Cameron, A.J.; Ball, K.; Hesketh, K.D.; McNaughton, S.A.; Salmon, J.; Crawford, D.A.; Lioret, S.; Campbell, K.J. Variation in outcomes of the Melbourne Infant, Feeding, Activity and Nutrition Trial (InFANT) Program according to maternal education and age. Prev. Med. 2014, 58, 58–63. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Weighted Mean or % (95% CI) | |||
|---|---|---|---|
| All (n = 978) | Girls n = 459 | Boys n = 519 | |
| BLOCK 1: FAMILY SOCIO-DEMOGRAPHY | |||
| Maternal education level at inclusion | |||
| <High school diploma | 29.3 (25.8; 32.7) | 27.9 (22.8; 32.9) | 30.5 (25.8; 35.2) |
| High school diploma to 2-year university degree | 39.3 (36.1; 42.5) | 40.9 (36.1; 45.7) | 37.9 (33.5; 42.3) |
| ≥3-year university degree | 31.4 (28.6; 34.3) | 31.2 (27.0; 35.4) | 31.6 (27.7; 35.6) |
| Paternal education level at inclusion | |||
| <High school diploma | 37.2 (33.7; 40.7) | 36.2 (31.0; 41.4) | 38.1 (33.4; 42.9) |
| High school diploma to 2-year university degree | 38.9 (35.6; 42.3) | 38.3 (33.4; 43.3) | 39.5 (34.9; 44.0) |
| ≥3-year university degree | 23.9 (21.2; 26.5) | 25.5 (21.4; 29.5) | 22.4 (18.9; 25.9) |
| Monthly household income | |||
| <2300 EUR | 27.8 (24.5; 31) | 25.1 (20.4; 29.8) | 30.2 (25.6; 34.7) |
| 2301 EUR to 3800 EUR | 45.7 (42.4; 49.1) | 47.4 (42.5; 52.2) | 44.3 (39.7; 48.9) |
| >3800 EUR | 26.5 (23.7; 29.2) | 27.5 (23.4; 31.7) | 25.5 (21.8; 29.2) |
| Perceived financial hardship | |||
| At least one | 18.1 (15.2; 20.9) | 17.4 (13.3; 21.5) | 18.6 (14.7; 22.6) |
| Maternal employment status | |||
| Not employed | 21.7 (18.8; 24.7) | 20.7 (16.6; 24.9) | 22.7 (18.4; 26.9) |
| Employed part-time | 29.1 (26.1; 32.2) | 31.3 (26.6; 35.9) | 27.2 (23.2; 31.2) |
| Employed full-time | 49.2 (45.8; 52.5) | 48.0 (43.1; 52.9) | 50.1 (45.6; 54.8) |
| Study center | |||
| Nancy | 50.1 (46.7; 53.4) | 52.8 (47.9; 57.7) | 47.6 (43.0; 52.2) |
| Maternal age at delivery | |||
| <27 y | 26.8 (23.6; 29.9) | 26.0 (21.4; 30.6) | 27.5 (23.1; 31.9) |
| 27 to 33 y | 48.0 (44.6; 51.3) | 49.4 (44.5; 54.3) | 46.7 (42.1; 51.3) |
| >33 y | 25.2 (22.5; 28.0) | 24.6 (20.7; 28.6) | 25.8 (22.1; 29.6) |
| Mother lives alone (no other adult) | |||
| Yes | 7.8 (5.8; 9.8) | 7.8 (4.8; 10.8) | 7.8 (5.1; 10.4) |
| Younger siblings at home | |||
| At least one | 46.3 (43.0; 49.7) | 46.5 (41.6; 51.5) | 46.1 (41.5; 50.7) |
| Older siblings at home | |||
| At least one | 55.5 (52.3; 58.8) | 55.0 (50.2; 59.8) | 56.0 (51.5; 60.5) |
| Pets at home | |||
| At least one dog | 29.7 (26.6; 32.9) | 29.1 (24.5; 33.7) | 30.3 (26.0; 34.6) |
| No dog but other animals | 31.7 (28.6; 34.9) | 32.8 (28.1; 37.4) | 30.8 (26.6; 35.0) |
| No pets | 38.6 (35.3; 41.7) | 38.1 (33.5; 42.8) | 38.9 (34.4; 43.3) |
| Backyard at home | |||
| Yes | 89.8 (87.4; 92.2) | 88.6 (84.9; 92.3) | 90.9 (88.0; 93.8) |
| BLOCK 2: PARENTS’ HEALTH/BEHAVIORS | |||
| Mother’s diet during pregnancy (PCA scores) | |||
| Healthy | −0.03 (−0.10; 0.03) | −0.04 (−0.14; 0.06) | −0.03 (−0.11; 0.06) |
| Western | −0.02 (−0.10; 0.05) | −0.03 (−0.13; 0.07) | −0.02 (−0.13; 0.0) |
| Mother’s leisure-time physical activity | |||
| 0 h/week | 58.4 (55.2; 61.7) | 61.0 (56.3; 65.7) | 56.1 (51.6; 60.6) |
| >0 to 2 h/week | 27.5 (24.6; 30.4) | 27.1 (23.0; 31.3) | 27.8 (23.9; 31.7) |
| >2 h/week | 14.1 (11.8; 16.3) | 11.8 (8.9; 14.8) | 16.1 (12.8; 19.4) |
| Father’s leisure-time physical activity | |||
| 0 h/week | 50.9 (47.5; 54.4) | 54.1 (49.1; 59.0) | 48.1 (43.3; 52.9) |
| >0 to 2 h/week | 18.4 (15.7; 21.1) | 17.5 (13.8; 21.3) | 19.1 (15.4; 22.9) |
| >2 h/week | 30.7 (27.6; 33.9) | 28.4 (24.0; 32.9) | 32.8 (28.4; 37.2) |
| Mother’s BMI | |||
| >30 kg/m2 | 15.8 (13.3; 18.3) | 16.8 (13.1; 20.6) | 14.9 (11.6; 18.3) |
| 25 to 30 kg/m2 | 23.9 (20.9; 26.8) | 24.6 (20.2; 29.0) | 23.2 (19.2; 27.2) |
| <25 kg/m2 | 60.3 (57.0; 63.6) | 58.6 (53.7; 63.5) | 61.8 (57.3; 66.4) |
| Mother’s depression symptoms (CES-D score) | 9.57 (9.02; 10.13) | 9.84 (9.00; 10.69) | 9.33 (8.59; 10.06) |
| Smoking status | |||
| At least one parent smokes | 47.5 (44.1; 50.9) | 48.3 (43.3; 53.3) | 46.8 (42.1; 51.5) |
| Childcare arrangements outside school | |||
| Outside school hours care services | 36.1 (32.9; 39.2) | 34.0 (29.5; 38.5) | 37.9 (33.6; 42.3) |
| Neighbor or employee | 23.4 (20.6; 26.2) | 28.1 (23.7; 32.5) | 19.2 (15.8; 22.7) |
| Mother, father (parents) or family | 40.5 (37.2; 43.9) | 37.9 (33.0; 42.8) | 42.8 (38.2; 47.4) |
| Daily canteen meals | |||
| Yes | 53.7 (50.3; 57.1) | 55.3 (50.3; 60.4) | 52.3 (47.7; 56.9) |
| BLOCK 3: PARENT-CHILD INTERACTIONS | |||
| Parental feeding practices at year 2 | |||
| Child control (Lack of parental control) | |||
| T3 (tertile range: 2.66 to 5) | 28.9 (25.8; 32.1) | 26.8 (22.4; 31.4) | 30.8 (26.4; 35.3) |
| Food as reward | |||
| T3 (tertile range: 1.66 to 4) | 32.0 (28.7; 35.4) | 34.3 (29.4; 39.3) | 30.0 (25.4; 34.5) |
| Food restrictions for health | |||
| T3 (tertile range: 4.25 to 5) | 37.9 (34.4; 41.4) | 36.8 (31.6; 41.9) | 38.8 (34.0; 43.6) |
| Pressure to eat | |||
| T3 (tertile range: 3 to 4.66) | 33.3 (29.9; 36.8) | 32.9 (28.0; 37.7) | 33.8 (29.1; 38.4) |
| Daily breakfast intake | |||
| Yes | 91.9 (90.0; 93.8) | 91.3 (88.2; 94.3) | 92.5 (90.1; 94.8) |
| TV on during meals | |||
| Often or always | 33.0 (29.8; 36.3) | 31.9 (27.1; 36.6) | 34.2 (29.7; 38.6) |
| Sometimes | 32.7 (29.5; 35.8) | 33.2 (28.6; 37.7) | 32.2 (27.9; 36.5) |
| Never | 34.3 (31.2; 37.3) | 35.0 (30.4; 39.5) | 33.6 (29.4; 37.8) |
| Unhealthy snacking outside meals | |||
| Often or always | 18.8 (15.9; 21.6) | 18.0 (13.9; 22.0) | 19.5 (15.6; 23.4) |
| Sometimes | 58.0 (54.7; 61.4) | 56.6 (51.7; 61.5) | 59.3 (54.8; 63.9) |
| Never | 23.2 (20.5; 25.9) | 25.5 (21.3; 29.7) | 21.2 (17.7; 24.7) |
| SASBs during meals | |||
| Yes | 20.1 (17.2; 23.0) | 18.3 (14.1; 22.4) | 21.7 (17.8; 25.7) |
| Parents’ perception of child physical activity | |||
| More active than other children | 17.9 (15.3; 20.6) | 12.1 (8.7; 15.5) | 23.1 (19.2; 27.0) |
| Participation in an organized sports activity | |||
| Yes | 55.4 (52; 58.7) | 60.2 (55.3; 65.1) | 51.0 (46.4; 55.6) |
| Bedtime (hours and minutes) | 20 h 42 min (20 h 40 min; 20 h 44 min) | 20 h 42 min (20 h 39 min; 20 h 44 min) | 20 h 43 min (20 h 40; 20 h 45 min) |
| Cognitive stimulation (HOME score) | 17.10 (16.92; 17.26) | 17.10 (16.82; 17.31) | 17.12 (16.89; 17.34) |
| Activity with the father (PCA scores) | |||
| Everyday care with leisure time | 0.00 (−0.08; 0.07) | −0.10 (−0.17; 0.05) | 0.04 (−0.05; 0.15) |
| Everyday care without active leisure time | −0.07 (−0.15; 0.01) | −0.01 (−0.12; 0.10) | −0.12 (−0.24; −0.01) |
| Girls (n = 459) | Boys (n = 519) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| EBRB Distribution | PCA Factor Loadings | EBRB Distribution | PCA Factor Loadings | ||||||
| Mean (SD) | Unhealthy | Healthy | Mixed | Mean (SD) | Unhealthy | Healthy | Mixed | p | |
| Fish (times/week) | 1.94 (1.47) | 0.16 | 0.60 | −0.01 | 1.96 (1.41) | 0.00 | 0.59 | 0.04 | 0.84 |
| Dairy products(times/week) | 15.90 (6.77) | 0.03 | 0.37 | −0.04 | 16.26 (6.85) | 0.11 | 0.21 | 0.22 | 0.40 |
| Vegetables (times/week) | 8.14 (5.51) | −0.23 | 0.72 | −0.03 | 7.85 (5.17) | −0.08 | 0.73 | −0.06 | 0.39 |
| Fruit (times/week) | 7.94 (5.04) | −0.09 | 0.77 | 0.07 | 8.15(4.99) | −0.01 | 0.71 | −0.02 | 0.50 |
| SASBs (times/week) | 5.71 (4.92) | 0.43 | 0.07 | 0.20 | 6.90 (5.98) | 0.62 | 0.09 | 0.09 | <0.001 |
| Sweet snacks & desserts (times/week) | 10.44 (5.90) | 0.66 | −0.06 | 0.05 | 10.98 (6.30) | 0.64 | −0.04 | 0.09 | 0.16 |
| Processed meat (times/week) | 0.99 (1.20) | 0.57 | 0.02 | 0.11 | 1.15 (1.38) | 0.56 | 0.13 | −0.04 | 0.07 |
| French fries (times/week) | 0.95 (0.99) | 0.73 | −0.02 | 0.01 | 1.06 (0.99) | 0.50 | −0.02 | 0.15 | 0.07 |
| Crisps (times/week) | 0.81 (0.86) | 0.67 | −0.06 | −0.07 | 0.79(0.86) | 0.55 | −0.07 | −0.17 | 0.86 |
| Screen time (hours/day) | 1.26 (0.83) | 0.27 | −0.23 | 0.53 | 1.37(0.80) | 0.52 | −0.34 | 0.25 | 0.03 |
| Outdoor play (standardized by season) | −0.13 (0.94) | −0.03 | 0.11 | 0.68 | 0.07(1.05) | 0.00 | −0.11 | 0.73 | 0.002 |
| Walking (hours/day) | 0.69 (0.45) | −0.07 | 0.09 | 0.79 | 0.73(0.51) | 0.12 | −0.01 | 0.77 | 0.12 |
| Sleep (hours/day) | 10.89 (0.46) | −0.15 | 0.09 | −0.30 | 10.86(0.49) | −0.37 | 0.14 | 0.34 | 0.23 |
| % variance explained | 17.8 | 12.8 | 10.6 | 17.2 | 11.8 | 10.6 | |||
| Component label (i.e., lifestyle pattern label) | Discretionary Consumption, Low Vegetables, High Screen | Fish, Dairy products, Fruit & Vegetables, Low Screen | SASBs, High Screen, Outdoor Play, Walking, Low Sleep | Discretionary Consumption, High Screen, Low Sleep | Fish, Dairy products, Fruit & Vegetables, Low Screen | Dairy products, High Screen, Outdoor Play, Walking, High Sleep | |||
| Girls (n = 459) Discretionary Consumption, Low Vegetables, High Screen | Boys (n = 519) Discretionary Consumption, High Screen, Low Sleep | |||
|---|---|---|---|---|
| β (95% CI) | p | β (95% CI) | p | |
| MODEL 1: FAMILY SOCIO-DEMOGRAPHY | ||||
| Maternal education level at inclusion | 0.16 | 0.007 | ||
| <HS diploma vs. ≥3-y university degree | 0.25 (−0.07; 0.58) | 0.33 (0.04; 0.62) | ||
| ≥HS diploma to 2-y university degree vs. ≥3-y university degree | 0.02 (−0.23; 0.28) | −0.04 (−0.27; 0.20) | ||
| Paternal education level at inclusion | 0.024 | 0.031 | ||
| <HS diploma vs. ≥3-y university degree | 0.35 (0.04; 0.66) | 0.27 (−0.02; 0.57) | ||
| ≥HS diploma to 2-y university degree vs. ≥3-y university degree | 0.08 (−0.19; 0.36) | 0.03 (−0.23; 0.29) | ||
| Monthly household income | 0.66 | 0.16 | ||
| 2300 EUR vs. 3800 EUR | −0.09 (−0.41; 0.23) | 0.29 (−0.01; 0.60) | ||
| 2301 EUR to 3800 EUR vs. 3800 EUR | 0.03 (−0.21; 0.28) | 0.17 (−0.07; 0.42) | ||
| Perceived financial hardship 1 | ||||
| At least one vs. No | ||||
| Maternal employment status | 0.33 | 0.60 | ||
| Not employed vs. Employed full-time | 0.18 (−0.09; 0.45) | 0.07 (−0.17; 0.32) | ||
| Employed part-time vs. Employed full-time | 0.12 (−0.10; 0.34) | −0.06 (−0.27; 0.15) | ||
| Study center | ||||
| Nancy vs. Poitiers | −0.09 (−0.27; 0.09) | 0.33 | ||
| Maternal age at delivery | 0.10 | |||
| <27 y vs. >33 y | 0.10 (−0.14; 0.35) | |||
| 27 to 33 y vs. >33 y | −0.12 (−0.34; 0.09) | |||
| Mother lives alone (no other adults) | ||||
| Yes vs. No | ||||
| Younger siblings at home | ||||
| At least one vs. No | ||||
| Older siblings at home | ||||
| At least one vs. No | ||||
| Pets at home | 0.050 | 0.06 | ||
| At least one dog vs. No pets | 0.29 (0.05; 0.52) | 0.25 (0.03; 0.47) | ||
| No dog but other animals vs. No pets | 0.07 (−0.15; 0.29) | 0.19 (−0.02; 0.40) | ||
| Backyard at home | ||||
| Yes vs. No | −0.44 (−0.76; −0.12) | 0.007 | ||
| MODEL 2 2: PARENTS’ HEALTH/BEHAVIORS | ||||
| Mother’s diet during pregnancy (PCA scores) | ||||
| Healthy | 0.15 (0.05; 0.24) | 0.002 | ||
| Western | 0.38 (0.22; 0.54) | <0.001 | 0.40 (0.30; 0.49) | <0.001 |
| Mother’s leisure time physical activity | 0.70 | 0.67 | ||
| 0 h/week vs. >2 h/week | 0.09 (−0.21; 0.39) | 0.09 (−0.15; 0.33) | ||
| >0 to 2 h/week vs. >2 h/week | 0.01 (−0.30; 0.33) | 0.03 (−0.23; 0.28) | ||
| Father’s leisure time physical activity | 0.41 | 0.012 | ||
| 0 h/week vs. >2 h/week | 0.03 (−0.19; 0.26) | 0.20 (0.01; 0.40) | ||
| >0 to 2 h/week vs. >2 h/week | 0.16 (−0.12; 0.44) | −0.08 (−0.32; 0.16) | ||
| Mother’s BMI | 0.24 | |||
| >30 kg/m2 vs. <25 kg/m2 | 0.18 (−0.07; 0.44) | |||
| 25 to 30 kg/m2 vs. <25 kg/m2 | 0.07 (−0.15; 0.30) | |||
| Mother’s depression symptoms (CESD score) | 0.00 (−0.01; 0.01) | 0.45 | 0.01 (−0.01; 0.02) | 0.27 |
| Smoking status | ||||
| At least one parent vs. Neither parent | −0.03 (−0.22; 0.16) | 0.74 | 0.08 (−0.09; 0.26) | 0.35 |
| Childcare arrangements outside school | 0.57 | |||
| OSHC services vs. Mother, father, or family | −0.01 (−0.20; 0.18) | |||
| Neighbor or employee vs. parents or family | −0.11 (−0.34; 0.12) | |||
| Daily canteen meals | ||||
| Yes vs. No | ||||
| MODEL 3 2: PARENT-CHILD INTERACTIONS | ||||
| Parental feeding practices at year 2, (T3 vs. T1 + T2) | ||||
| Child control (Lack of parental control) | 0.19 (−0.01; 0.40) | 0.06 | 0.05 (−0.13; 0.22) | 0.60 |
| Food as reward | −0.05 (−0.24; 0.14) | 0.63 | 0.04 (−0.12; 0.21) | 0.62 |
| Food restrictions for health | −0.11 (−0.29; 0.07) | 0.22 | −0.08 (−0.24; 0.08) | 0.31 |
| Pressure to eat | ||||
| Daily breakfast intake | ||||
| Yes vs. No | ||||
| TV on during meals | 0.003 | <0.001 | ||
| Often or always vs. Never | 0.37 (0.13; 0.61) | 0.46 (0.26; 0.65) | ||
| Sometimes vs. Never | 0.31 (0.10; 0.53) | 0.38 (0.20; 0.56) | ||
| Unhealthy snacking outside meals | <0.001 | <0.001 | ||
| Often or always vs. Never | 0.69 (0.40; 0.99) | 0.57 (0.33; 0.81) | ||
| Sometimes vs. Never | 0.03 (−0.18; 0.24) | 0.04 (−0.14; 0.23) | ||
| SASBs during meals | ||||
| Yes vs. No | −0.11 (−0.35; 0.13) | 0.39 | 0.48 (0.30; 0.67) | <0.001 |
| Parents’ perception of child physical activity | ||||
| More active than vs. Less or as active as other children | ||||
| Participation in an organized sports activity | ||||
| Yes vs. No | −0.12 (−0.30; 0.06) | 0.19 | −0.09 (−0.24; 0.06) | 0.23 |
| Bedtime (Hours) | 0.24 (0.03; 0.45) | 0.024 | 0.30 (0.14; 0.46) | <0.001 |
| Cognitive stimulation (HOME score) | −0.02 (−0.05; 0.02) | 0.42 | ||
| Activities with the father (PCA scores) | ||||
| Everyday care with leisure time | ||||
| Everyday care without active leisure time | −0.04 (−0.12; 0.03) | 0.26 | ||
| Girls (n = 459) Fish, Dairy Products, Fruit & Vegetables, Low Screen | Boys (n = 519) Fish, Dairy Products, Fruit & Vegetables, Low Screen | |||
|---|---|---|---|---|
| β (95% CI) | p | β (95% CI) | p | |
| MODEL 1: FAMILY SOCIO-DEMOGRAPHY | ||||
| Maternal education level at inclusion | 0.10 | 0.20 | ||
| <HS diploma vs. ≥3-y university degree | −0.22 (−0.52; 0.09) | −0.27 (−0.56; 0.03) | ||
| ≥HS diploma to 2-y university degree vs. ≥3-y university degree | 0.05 (−0.20; 0.30) | −0.15 (−0.39; 0.09) | ||
| Paternal education level at inclusion | 0.51 | 0.06 | ||
| <HS diploma vs. ≥3-y university degree | −0.17 (−0.48; 0.14) | −0.32 (−0.63; −0.02) | ||
| ≥HS diploma to 2-y university degree vs. ≥3-y university degree | −0.14 (−0.41; 0.13) | −0.27 (−0.53; 0.00) | ||
| Monthly household income | 0.08 | 0.69 | ||
| 2300 EUR vs. 3800 EUR | −0.29 (−0.61; 0.03) | −0.08 (−0.41; 0.25) | ||
| 2301 EUR to 3800 EUR vs. 3800 EUR | −0.26 (−0.50; −0.02) | −0.10 (−0.35; 0.15) | ||
| Perceived financial hardship 1 | ||||
| At least one vs. No | ||||
| Maternal employment status | 0.034 | |||
| Not employed vs. Employed full-time | 0.31 (0.02; 0.60) | |||
| Employed part-time vs. Employed full-time | 0.17 (−0.06; 0.39) | |||
| Study center | ||||
| Nancy vs. Poitiers | ||||
| Maternal age at delivery | ||||
| <27 y vs. >33 y | ||||
| 27 to 33 y vs. > 33 y | ||||
| Mother lives alone (no other adults) | ||||
| Yes vs. No | 0.46 (0.09; 0.83) | 0.014 | −0.15 (−0.51; 0.22) | 0.43 |
| Younger siblings at home | ||||
| At least one vs. No | 0.09 (−0.10; 0.28) | 0.34 | ||
| Older siblings at home | ||||
| At least one vs. No | 0.15 (−0.03; 0.33) | 0.10 | ||
| Pets at home | ||||
| At least one dog vs. No pets | ||||
| No dog but other animals vs. No pets | ||||
| Backyard at home | ||||
| Yes vs. No | ||||
| MODEL 2 2: PARENTS’ HEALTH/BEHAVIORS | ||||
| Mother’s diet during pregnancy (PCA scores) | ||||
| Healthy | 0.28 (0.17; 0.39) | <0.001 | 0.28 (0.18; 0.38) | <0.001 |
| Western | −0.11 (−0.22; 0.01) | 0.06 | −0.05 (−0.15; 0.04) | 0.26 |
| Mother’s leisure time physical activity | 0.53 | 0.29 | ||
| 0 h/week vs. >2 h/week | −0.17 (−0.47; 0.11) | −0.20 (−0.45; 0.06) | ||
| >0 to 2 h/week vs. >2 h/week | −0.14 (−0.45; 0.17) | −0.15 (−0.43; 0.13) | ||
| Father’s leisure time physical activity | ||||
| 0 h/week vs. >2 h/week | ||||
| >0 to 2 h/week vs. >2 h/week | ||||
| Mother’s BMI | 0.70 | |||
| >30 kg/m2 vs. <25 kg/m2 | −0.01 (−0.27; 0.24) | |||
| 25 to 30 kg/m2 vs. <25 kg/m2 | −0.09 (−0.30; 0.13) | |||
| Mother’s depression symptoms (CESD score) | −0.01 (−0.02; 0.00) | 0.046 | ||
| Smoking status | ||||
| At least one parent vs. Neither parent | −0.17 (−0.36; 0.02) | 0.09 | 0.03 (−0.16; 0.21) | 0.78 |
| Childcare arrangements outside school | ||||
| OSHC services vs. Mother, father, or family | ||||
| Neighbor or employee vs. parents or family | ||||
| Daily canteen meals | ||||
| Yes vs. No | −0.07 (−0.25; 0.12) | 0.47 | ||
| MODEL 3 2: PARENT-CHILD INTERACTIONS | ||||
| Parental feeding practices at year 2, (T3 vs. T1 + T2) | ||||
| Child control (Lack of parental control) | −0.08 (−0.29; 0.13) | 0.47 | −0.04 (−0.24; 0.16) | 0.68 |
| Food as reward | −0.08 (−0.28; 0.12) | 0.42 | −0.14 (−0.34; 0.05) | 0.15 |
| Food restrictions for health | 0.13 (−0.08; 0.34) | 0.24 | 0.20 (0.01; 0.38) | 0.035 |
| Pressure to eat | ||||
| Daily breakfast intake | ||||
| Yes vs. No | 0.16 (−0.15; 0.46) | 0.32 | ||
| TV on during meals | <0.001 | 0.005 | ||
| Often or always vs. Never | −0.30 (−0.55; −0.06) | −0.19 (−0.42; 0.04) | ||
| Sometimes vs. Never | 0.22 (0.01; 0.44) | 0.08 (−0.13; 0.30) | ||
| Unhealthy snacking outside meals | 0.25 | 0.13 | ||
| Often or always vs. Never | −0.12 (−0.40; 0.17) | −0.11 (−0.40; 0.17) | ||
| Sometimes vs. Never | −0.18 (−0.38; 0.04) | −0.21 (−0.43; 0.00) | ||
| SASBs during meals | ||||
| Yes vs. No | −0.21 (−0.46; 0.04) | 0.10 | 0.03 (−0.18; 0.25) | 0.76 |
| Parents’ perception of child physical activity | ||||
| More active than vs. Less or as active as other children | −0.21 (−0.41; −0.01) | 0.042 | ||
| Participation in an organized sports activity | ||||
| Yes vs. No | 0.04 (−0.14; 0.22) | 0.67 | 0.23 (0.05; 0.40) | 0.01 |
| Bedtime (Hours) | −0.13 (−0.35; 0.08) | 0.23 | −0.36 (−0.54; −0.17) | <0.001 |
| Cognitive stimulation (HOME score) | 0.07 (0.03; 0.11) | 0.001 | 0.06 (0.02; 0.10) | 0.001 |
| Activities with the father (PCA scores) | ||||
| Everyday care with leisure time | ||||
| Everyday care without active leisure time | 0.06 (−0.03; 0.15) | 0.20 | ||
| Girls (n = 459) SASBs, High Screen, Outdoor Play, Walking, Low Sleep | Boys (n = 519) Dairy Products, High Screen, Outdoor Play, Walking, High Sleep | |||
|---|---|---|---|---|
| β (95% CI) | p | β (95% CI) | p | |
| MODEL 1: FAMILY SOCIO-DEMOGRAPHY | ||||
| Maternal education level at inclusion | <0.001 | 0.004 | ||
| <HS diploma vs. ≥3-y university degree | 0.71 (0.41; 1.01) | 0.39 (0.11; 0.68) | ||
| ≥HS diploma to 2-y university degree vs. 3-y university degree | 0.15 (−0.09; 0.39) | 0.02 (−0.20; 0.25) | ||
| Paternal education level at inclusion | 0.27 | 0.016 | ||
| <HS diploma vs. ≥3-y university degree | 0.21 (−0.09; 0.50) | 0.39 (0.10; 0.67) | ||
| ≥HS diploma to 2-y university degree vs. ≥3-y university degree | 0.07 (−0.20; 0.35) | 0.19 (−0.06; 0.44) | ||
| Monthly household income | 0.07 | 0.47 | ||
| 2300 EUR vs. 3800 EUR | 0.35 (0.05; 0.65) | 0.18 (−0.11; 0.47) | ||
| 2301 EUR to 3800 EUR vs. 3800 EUR | 0.19 (−0.04; 0.43) | 0.08 (−0.15; 0.32) | ||
| Perceived financial hardship 1 | ||||
| At least one vs. No | ||||
| Maternalemployment status | 0.13 | 0.17 | ||
| Not employed vs. Employed full-time | −0.22 (−0.49; 0.04) | 0.02 (−0.22; 0.26) | ||
| Employed part-time vs. Employed full-time | −0.18 (−0.38; 0.03) | −0.17 (−0.37; 0.03) | ||
| Study center | ||||
| Nancy vs. Poitiers | 0.26 (0.09; 0.44) | 0.003 | ||
| Maternal age at delivery | ||||
| <27y vs. >33 y | ||||
| 27 to 33 y vs. >33 y | ||||
| Mother lives alone (no other adults) | ||||
| Yes vs. No | ||||
| Younger siblings at home | ||||
| At least one vs. No | −0.05 (−0.26; 0.15) | 0.61 | ||
| Older siblings at home | ||||
| At least one vs. No | 0.21 (0.02; 0.41) | 0.033 | 0.17 (−0.01; 0.34) | 0.06 |
| Pets at home | 0.003 | 0.011 | ||
| At least one dog vs. No pets | 0.31 (0.09; 0.53) | 0.25 (0.04; 0.46) | ||
| No dog but other animals vs. No pets | −0.05 (−0.26; 0.16) | −0.06 (−0.27; 0.14) | ||
| Backyard at home | ||||
| Yes vs. No | ||||
| MODEL 2 2: PARENTS HEALTH/BEHAVIORS | ||||
| Mother’s diet during pregnancy (PCA scores) | ||||
| Healthy | ||||
| Western | 0.00 (−0.11; 0.12) | 0.96 | 0.01 (−0.08; 0.10) | 0.86 |
| Mother’s leisure time physical activity | 0.78 | <0.001 | ||
| 0 h/week vs. >2 h/week | 0.08 (−0.22; 0.37) | −0.47 (−0.72; −0.23) | ||
| >0 to 2 h/week vs. >2 h/week | 0.11 (−0.20; 0.42) | −0.42 (−0.68; −0.16) | ||
| Father’s leisure time physical activity | 0.40 | 0.017 | ||
| 0 h/week vs. >2 h/week | 0.06 (−0.16; 0.29) | −0.19 (−0.39; 0.00) | ||
| >0 to 2 h/week vs. >2 h/week | −0.11 (−0.39; 0.17) | −0.32 (−0.56; −0.08) | ||
| Mother’s BMI | 0.22 | 0.13 | ||
| >30 kg/m2 vs. <25 kg/m2 | 0.17 (−0.08; 0.42) | 0.17 (−0.07; 0.42) | ||
| 25 to 30 kg/m2 vs. <25 kg/m2 | 0.16 (−0.05; 0.38) | 0.18 (−0.02; 0.39) | ||
| Mother’s depression symptoms (CESD score) | 0.00 (−0.01; 0.01) | 0.50 | 0.00 (−0.01; 0.01) | 0.62 |
| Smoking status | ||||
| At least one parent vs. Neither parent | 0.07 (−0.12; 0.26) | 0.46 | 0.07 (−0.11; 0.24) | 0.43 |
| Childcare arrangements outside school | 0.25 | <0.001 | ||
| OSHC services vs. Mother, father, or family | −0.19 (−0.42; 0.04) | −0.39 (−0.60; −0.19) | ||
| Neighbor or employee vs. parents or family | −0.06 (−0.31; 0.18) | −0.24 (−0.48; 0.01) | ||
| Daily canteen meals | ||||
| Yes vs. No | −0.12 (−0.32; 0.08) | 0.23 | ||
| MODEL 3 2: PARENT-CHILD INTERACTIONS | ||||
| Parental feeding practices at year 2, (T3 vs. T1 + T2) | ||||
| Child control (Lack of parental control) | ||||
| Food as reward | 0.10 (−0.10; 0.29) | 0.33 | ||
| Food restrictions for health | ||||
| Pressure to eat | ||||
| Daily breakfast intake | ||||
| Yes vs. No | −0.46 (−0.77; −0.14) | 0.005 | ||
| TV on during meals | 0.44 | 0.86 | ||
| Often or always vs. Never | 0.14 (−0.10; 0.38) | 0.04 (−0.18; 0.26) | ||
| Sometimes vs. Never | 0.01 (−0.20; 0.23) | 0.06 (−0.15; 0.26) | ||
| Unhealthy snacking outside meals | 0.09 | 0.20 | ||
| Often or always vs. Never | −0.06 (−0.34; 0.22) | 0.23 (−0.04; 0.51) | ||
| Sometimes vs. Never | 0.17 (−0.04; 0.38) | 0.16 (−0.05; 0.36) | ||
| SASBs during meals | ||||
| Yes vs. No | 0.08 (−0.17; 0.33) | 0.53 | 0.16 (−0.04; 0.37) | 0.12 |
| Parents’ perception of child physical activity | ||||
| More active than vs. Less or as active as other children | 0.12 (−0.08; 0.31) | 0.24 | ||
| Participation in an organized sports activity | ||||
| Yes vs. No | −0.07 (−0.25; 0.10) | 0.42 | ||
| Bedtime (Hours) | 0.40 (0.19; 0.61) | <0.001 | −0.51 (−0.69; −0.32) | <0.001 |
| Cognitive stimulation (HOME score) | −0.01 (−0.05; 0.03) | 0.61 | ||
| Activities with the father (PCA scores) | ||||
| Everyday care with leisure time | ||||
| Everyday care without active leisure time | −0.08 (−0.18; 0.01) | 0.08 | −0.07 (−0.15; 0.01) | 0.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Descarpentrie, A.; Saldanha-Gomes, C.; Guivarch, C.; Dargent-Molina, P.; de Lauzon-Guillain, B.; Plancoulaine, S.; Charles, M.-A.; Chia, A.; Chong, M.F.F.; Vandentorren, S.; et al. Family Socioecological Correlates of Lifestyle Patterns in Early Childhood: A Cross-Sectional Study from the EDEN Mother–Child Cohort. Nutrients 2021, 13, 3803. https://doi.org/10.3390/nu13113803
Descarpentrie A, Saldanha-Gomes C, Guivarch C, Dargent-Molina P, de Lauzon-Guillain B, Plancoulaine S, Charles M-A, Chia A, Chong MFF, Vandentorren S, et al. Family Socioecological Correlates of Lifestyle Patterns in Early Childhood: A Cross-Sectional Study from the EDEN Mother–Child Cohort. Nutrients. 2021; 13(11):3803. https://doi.org/10.3390/nu13113803
Chicago/Turabian StyleDescarpentrie, Alexandra, Cécilia Saldanha-Gomes, Claire Guivarch, Patricia Dargent-Molina, Blandine de Lauzon-Guillain, Sabine Plancoulaine, Marie-Aline Charles, Airu Chia, Mary Foong Fong Chong, Stéphanie Vandentorren, and et al. 2021. "Family Socioecological Correlates of Lifestyle Patterns in Early Childhood: A Cross-Sectional Study from the EDEN Mother–Child Cohort" Nutrients 13, no. 11: 3803. https://doi.org/10.3390/nu13113803
APA StyleDescarpentrie, A., Saldanha-Gomes, C., Guivarch, C., Dargent-Molina, P., de Lauzon-Guillain, B., Plancoulaine, S., Charles, M. -A., Chia, A., Chong, M. F. F., Vandentorren, S., Heude, B., Bernard, J. Y., & Lioret, S. (2021). Family Socioecological Correlates of Lifestyle Patterns in Early Childhood: A Cross-Sectional Study from the EDEN Mother–Child Cohort. Nutrients, 13(11), 3803. https://doi.org/10.3390/nu13113803