
Excessive Vitamin A Supplementation Increased the Incidence of Acute Respiratory Tract Infections: A Systematic Review and Meta-Analysis




Abstract
:1. Introduction
2. Materials and Methods
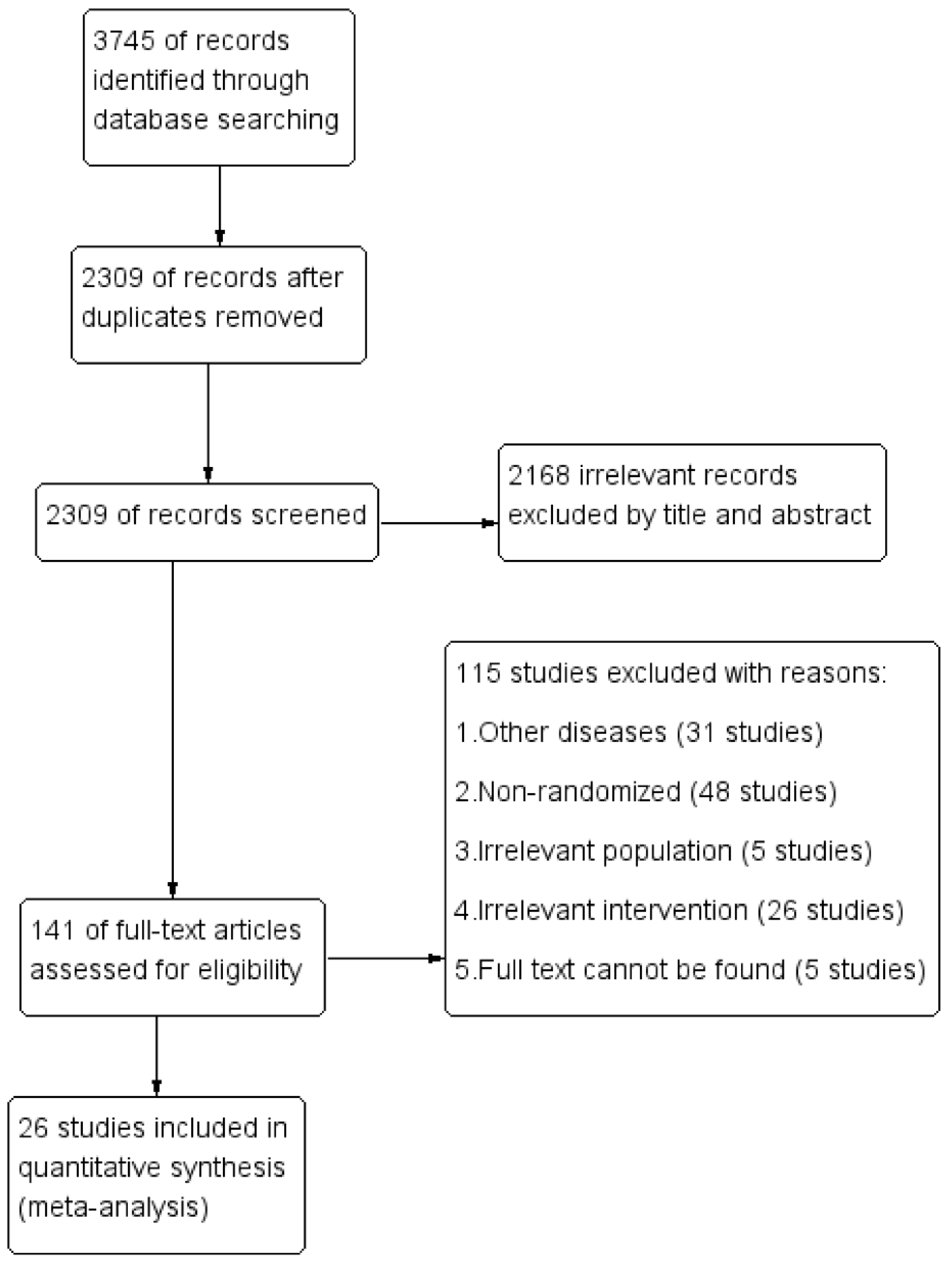
2.1. Search Strategy and Study Selection
2.2. Inclusion/Exclusion Criteria
2.3. Definition of Outcomes
2.4. Data Extraction and Quality Assessment
2.5. Data Synthesis and Analysis
3. Results
3.1. Baseline Characteristics of Included Studies
3.2. Association between Vitamin A and ARTI
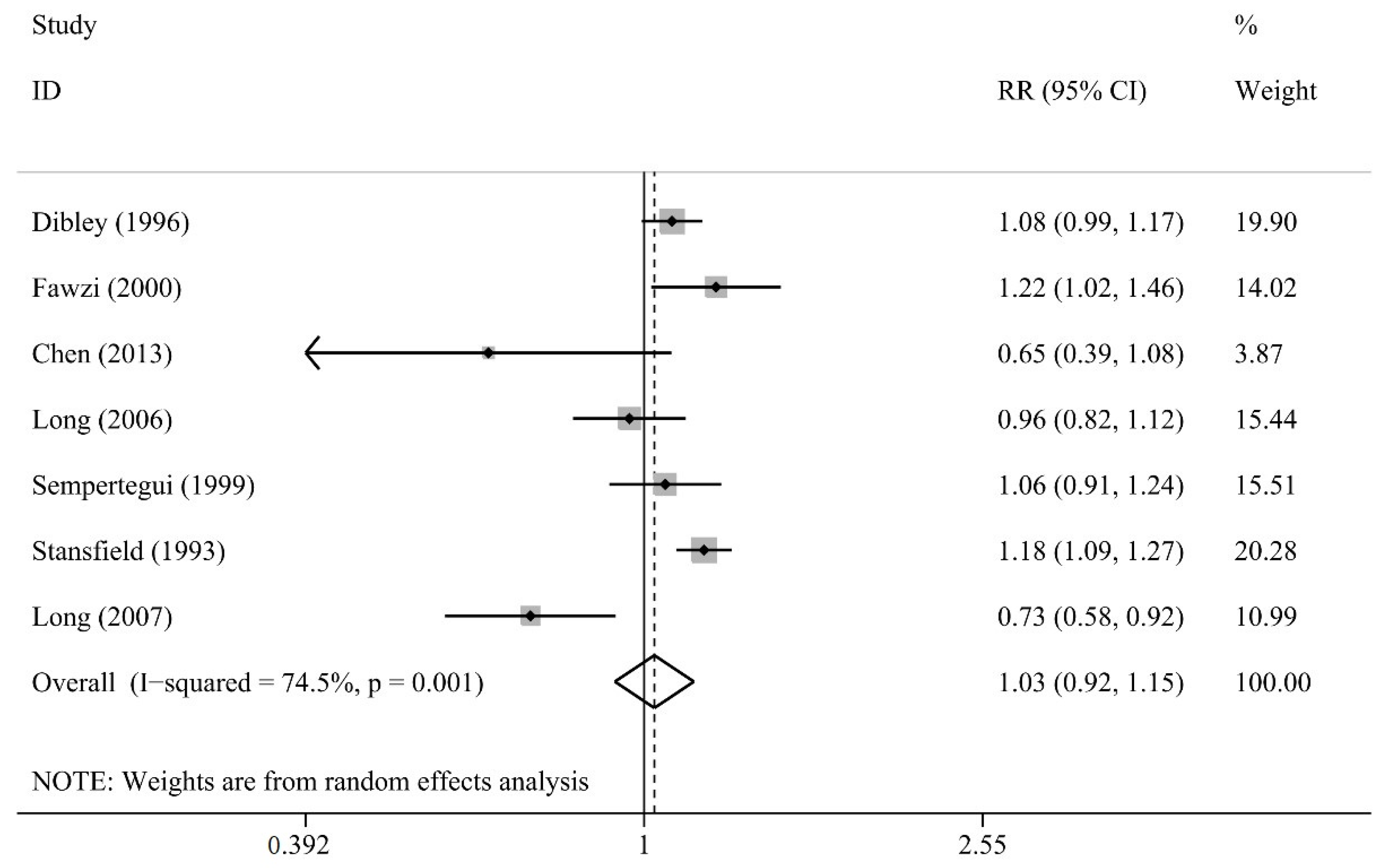
3.2.1. Incidence of ARTI
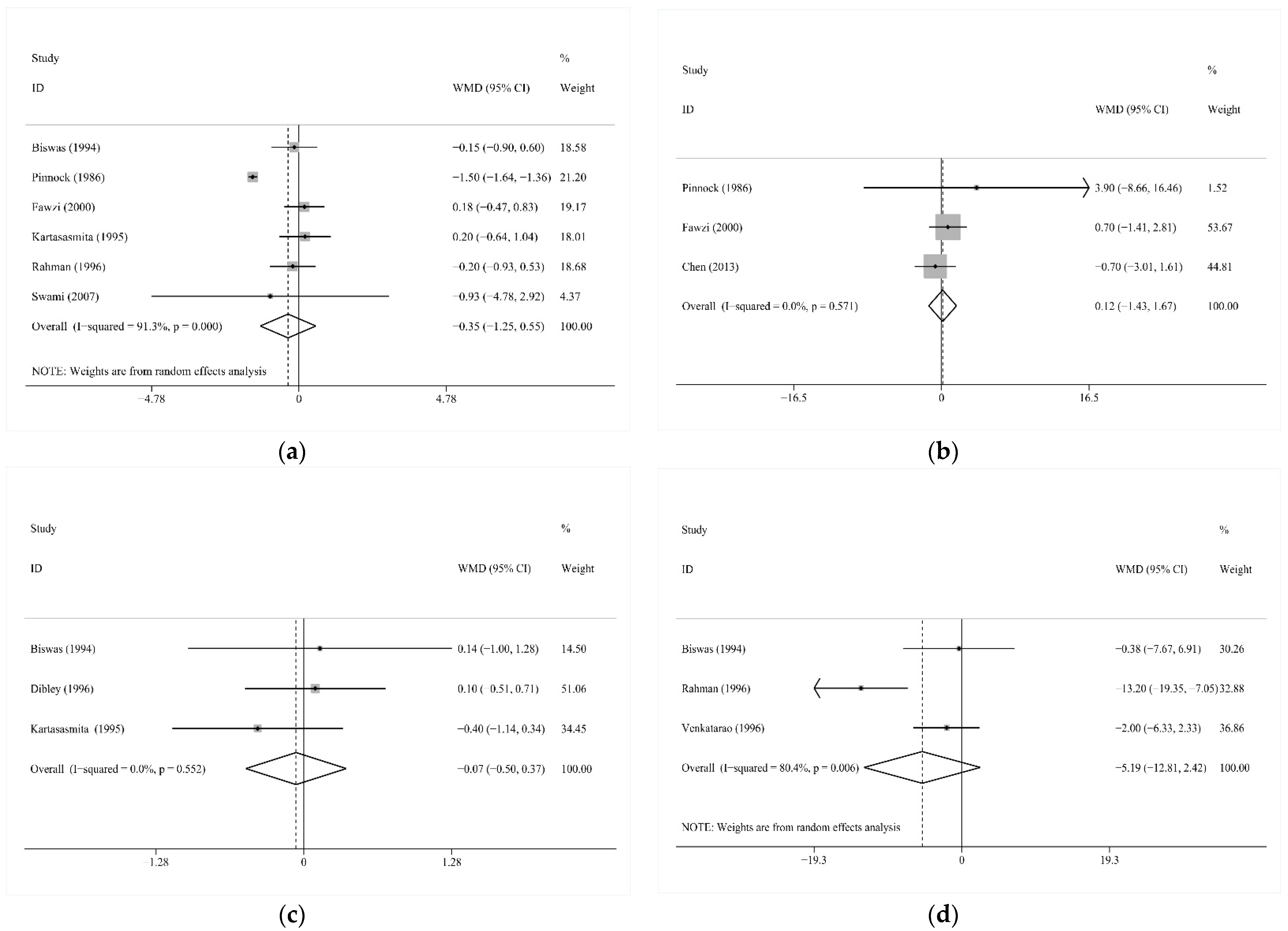
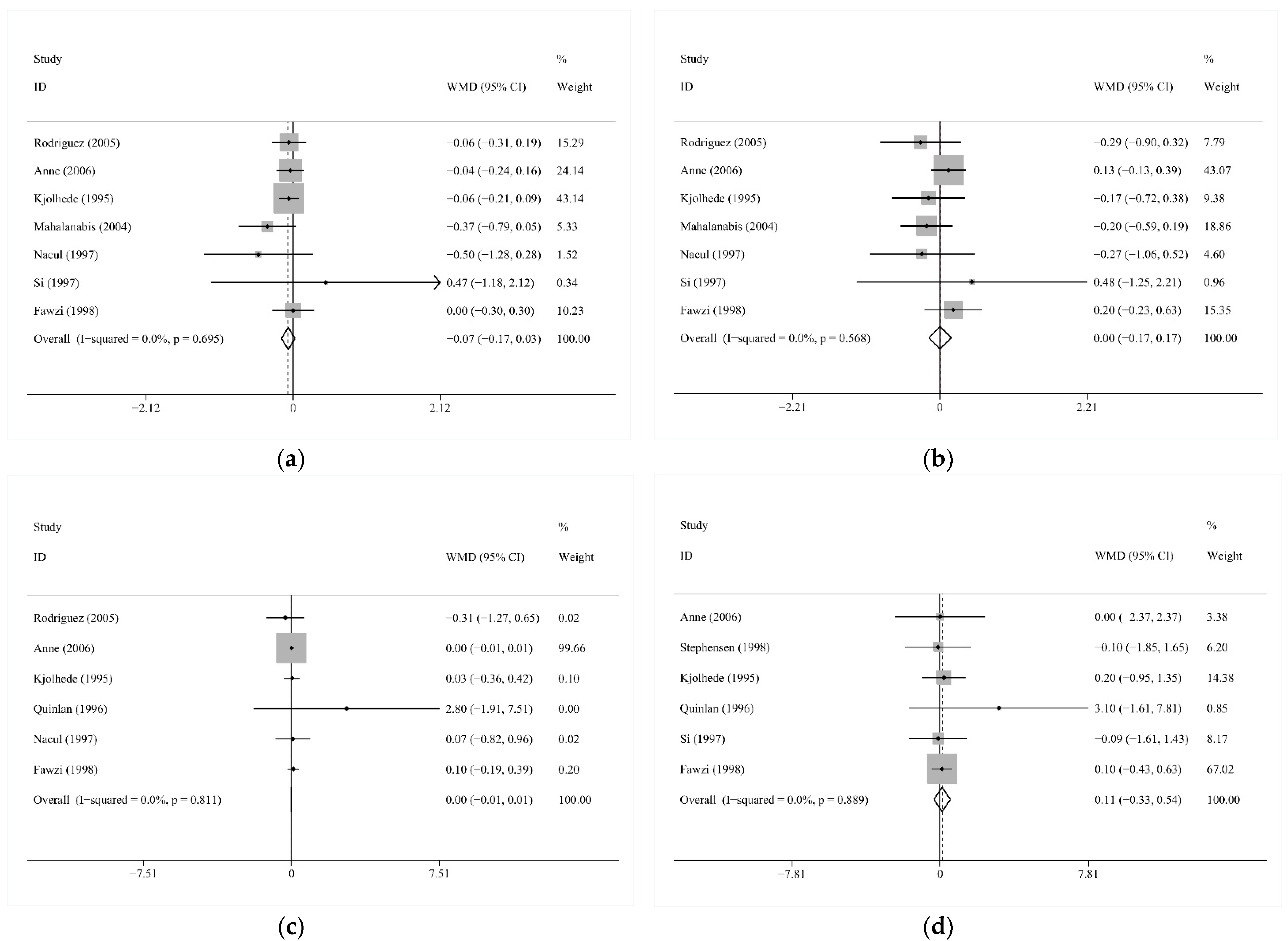
3.2.2. The Severity of ARTI
3.3. Association between Vitamin A and LRTI
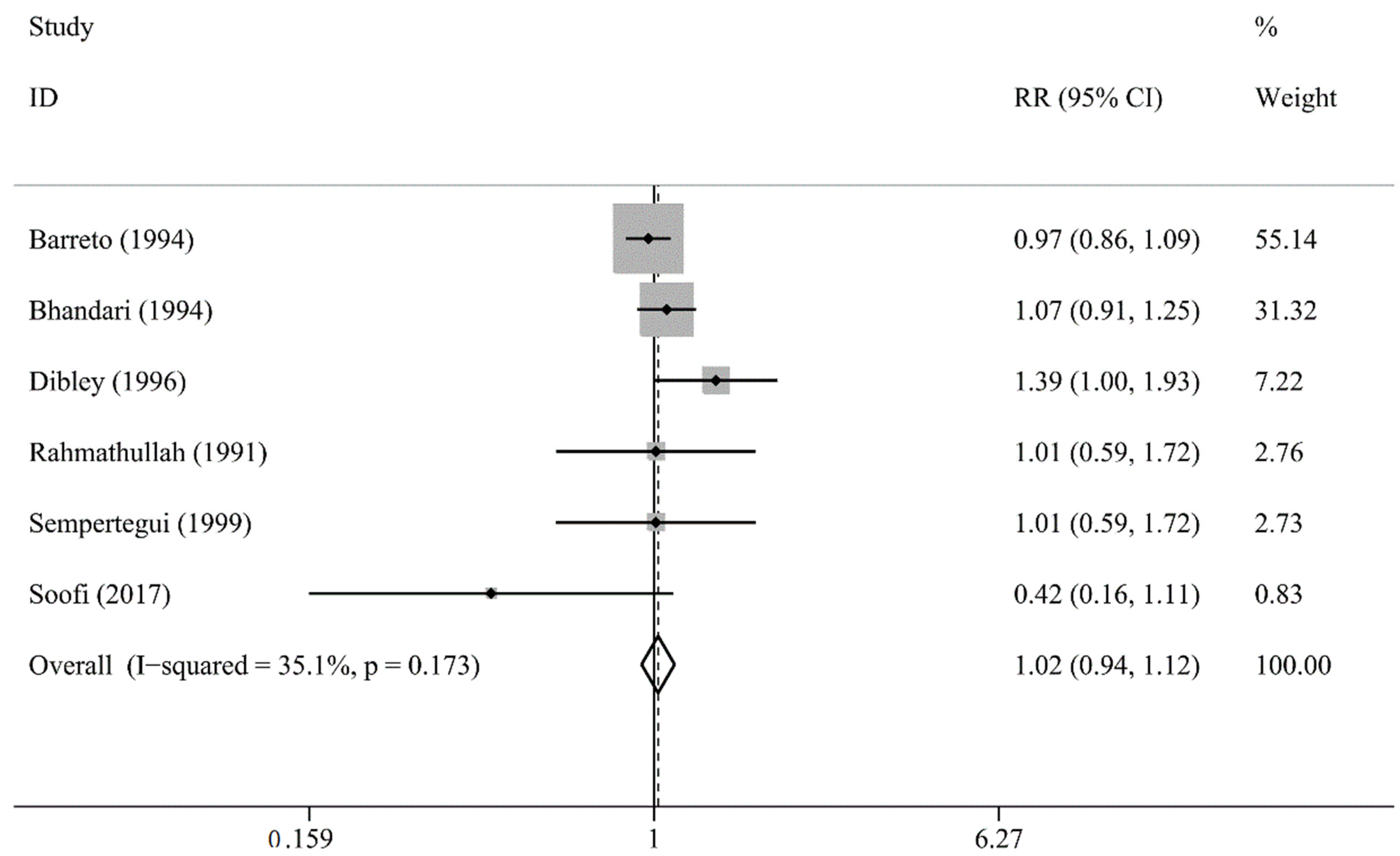
3.3.1. Incidence of LRTI
3.3.2. The Severity of LRTI
3.4. Subgroup Analysis
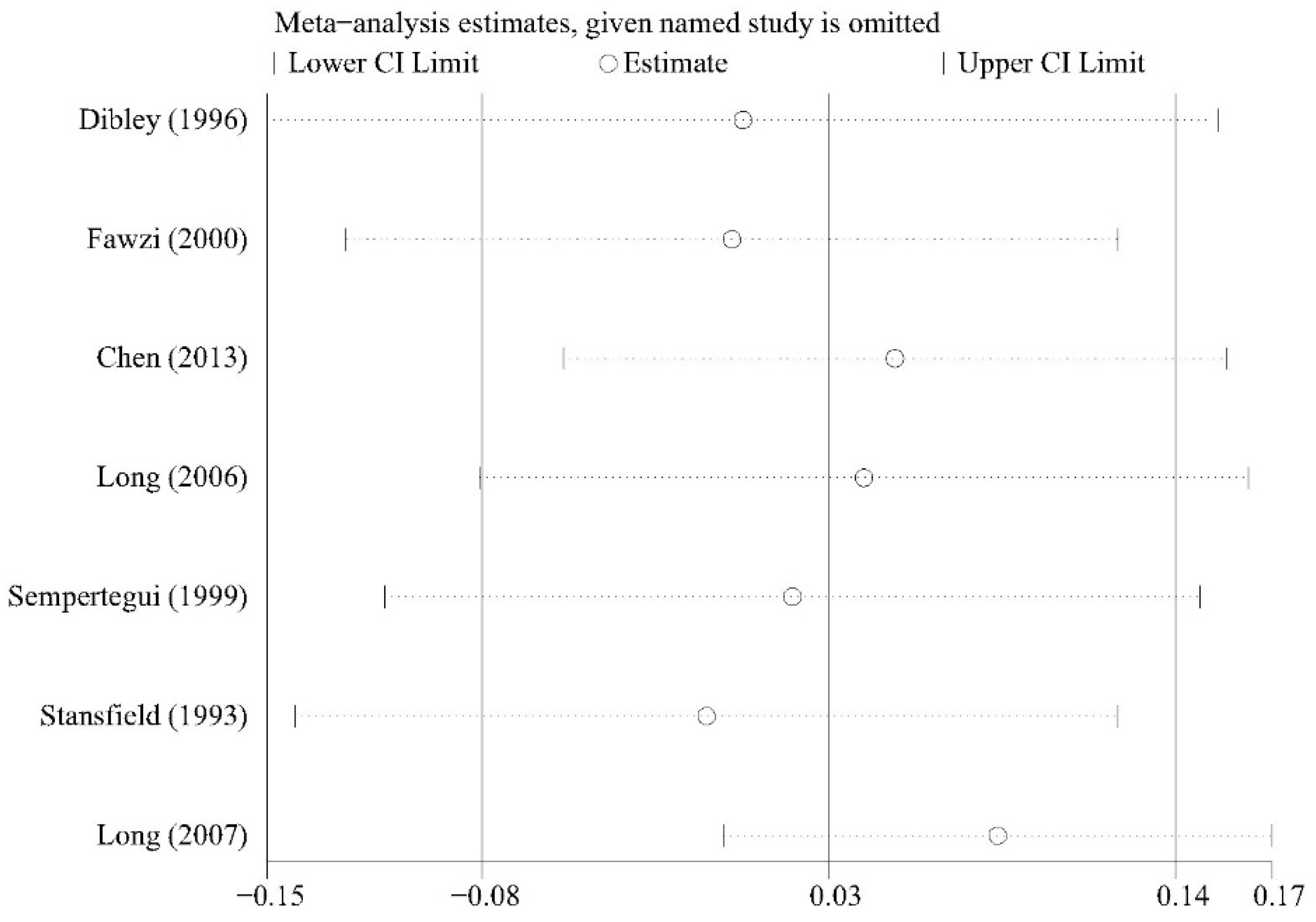
3.5. Sensitivity Analysis
3.6. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- Kardos, P.; Malek, F.A. Common Cold—An Umbrella Term for Acute Infections of Nose, Throat, Larynx and Bronchi. Pneumologia 2016, 71, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Hawke, K.; Van Driel, M.L.; Buffington, B.J.; McGuire, T.M.; King, D. Homeopathic medicinal products for preventing and treating acute respiratory tract infections in children. Cochrane Database Syst. Rev. 2018, 9, CD005974. [Google Scholar] [CrossRef]
- Black, R.E.; Cousens, S.; Johnson, H.L.; Lawn, J.; Rudan, I.; Bassani, D.; Jha, P.; Campbell, H.; Walker, C.F.; Cibulskis, R.; et al. Global, regional, and national causes of child mortality in 2008: A systematic analysis. Lancet 2010, 375, 1969–1987. [Google Scholar] [CrossRef]
- Causes of Death: Our World in Data. Available online: https://ourworldindata.org/causes-of-death (accessed on 1 February 2018).
- Wang, X.; Li, Y.; O′Brien, K.L.; Madhi, S.A.; Widdowson, M.-A.; Byass, P.; Omer, S.B.; Abbas, Q.; Ali, A.; Amu, A.; et al. Global burden of respiratory infections associated with seasonal influenza in children under 5 years in 2018: A systematic review and modelling study. Lancet Glob. Heal. 2020, 8, e497–e510. [Google Scholar] [CrossRef] [Green Version]
- Calder, P.C.; Carr, A.C.; Gombart, A.F.; Eggersdorfer, M. Optimal Nutritional Status for a Well-Functioning Immune System Is an Important Factor to Protect against Viral Infections. Nutrients 2020, 12, 1181. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.J.L.; Vos, T.; Lozano, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2197–2223. [Google Scholar] [CrossRef]
- Borel, P.; Desmarchelier, C. Genetic Variations Associated with Vitamin A Status and Vitamin A Bioavailability. Nutrients 2017, 9, 246. [Google Scholar] [CrossRef]
- Cañete, A.; Cano, E.; Muñoz-Chápuli, R.; Carmona, R. Role of Vitamin A/Retinoic Acid in Regulation of Embryonic and Adult Hematopoiesis. Nutrients 2017, 9, 159. [Google Scholar] [CrossRef] [Green Version]
- WHO Guidelines Approved by the Guidelines Review Committee. In Guideline: Vitamin A Supplementation in Infants and Children 6–59 Months of Age; World Health Organization. Available online: https://www.ncbi.nlm.nih.gov/books/NBK185172/ (accessed on 1 October 2021).
- Mahalanabis, D.; Lahiri, M.; Paul, D.; Gupta, S.; Gupta, A.; Wahed, M.A.; Khaled, M.A. Randomized, double-blind, placebo-controlled clinical trial of the efficacy of treatment with zinc or vitamin A in infants and young children with severe acute lower respiratory infection. Am. J. Clin. Nutr. 2004, 79, 430–436. [Google Scholar] [CrossRef] [Green Version]
- Grotto, I.; Mimouni, M.; Gdalevich, M.; Mimouni, D. Vitamin A supplementation and childhood morbidity from diarrhea and respiratory infections: A meta-analysis. J. Pediatr. 2003, 142, 297–304. [Google Scholar] [CrossRef]
- Chen, K.; Chen, X.-R.; Zhang, L.; Luo, H.-Y.; Gao, N.; Wang, J.; Fu, G.-Y.; Mao, M. Effect of simultaneous supplementation of vitamin A and iron on diarrheal and respiratory tract infection in preschool children in Chengdu City, China. Nutrients 2013, 29, 1197–1203. [Google Scholar] [CrossRef] [PubMed]
- Swami, H.M.; Thakur, J.S.; Bhatia, S.P.S. Impact of mass supplementation of vitamin A. Indian J. Pediatr. 2007, 74, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Sempértegui, F.; Estrella, B.; Camaniero, V.; Betancourt, V.; Izurieta, R.; Ortiz, W.; Fiallo, E.; Troya, S.; Rodríguez, A.; Griffiths, J.K.; et al. The beneficial effects of weekly low-dose vitamin A supplementation on acute lower respiratory infections and diarrhea in Ecuadorian children. Pediatrics 1999, 104, e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, A.B.; Torzillo, P.J.; Stewart, P.M.; Boyce, N.C.; White, A.V.; Wheaton, G.R.; Purdie, D.M.; Wakerman, J.; Valery, P.C. Zinc and vitamin A supplementation in Indigenous Australian children hospitalised with lower respiratory tract infection: A randomised controlled trial. Med. J. Aust. 2006, 184, 107–112. [Google Scholar] [CrossRef]
- Kjolhede, C.L.; Chew, F.J.; Gadomski, A.M.; Marroquin, D.P. Clinical trial of vitamin A as adjuvant treatment for lower respiratory tract infections. J. Pediatr. 1995, 126, 807–812. [Google Scholar] [CrossRef]
- Quinlan, K.P. Vitamin A and Respiratory Syncytial Virus Infection. Arch. Pediatr. Adolesc. Med. 1996, 150, 25–30. [Google Scholar] [CrossRef]
- Fawzi, W.W.; Mbise, R.L.; Fataki, M.R.; Herrera, M.G.; Kawau, F.; Hertzmark, E.; Spiegelman, D.; Ndossi, G. Vitamin A supplementation and severity of pneumonia in children admitted to the hospital in Dar es Salaam, Tanzania. Am. J. Clin. Nutr. 1998, 68, 187–192. [Google Scholar] [CrossRef]
- Nacul, L.; Kirkwood, B.R.; Arthur, P.; Morris, S.S.; Magalhães, M.; Fink, M.C.D.S. Randomised, double blind, placebo controlled clinical trial of efficacy of vitamin A treatment in non-measles childhood pneumonia. BMJ 1997, 315, 505–510. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez, A.; Hamer, D.H.; Rivera, J.; Acosta, M.; Salgado, G.; Gordillo, M.; Cabezas, M.; Naranjo-Pinto, C.; Leguísamo, J.; Gómez, D.; et al. Effects of moderate doses of vitamin A as an adjunct to the treatment of pneumonia in underweight and normal-weight children: A randomized, double-blind, placebo-controlled trial. Am. J. Clin. Nutr. 2005, 82, 1090–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Si, N.; Grytter, C.; Vy, N.; Hue, N.; Pedersen, F. High dose vitamin A supplementation in the course of pneumonia in Vietnamese children. Acta Paediatr. 1997, 86, 1052–1055. [Google Scholar] [CrossRef] [PubMed]
- Stephensen, C.B.; Franchi, L.M.; Hernandez, H.; Campos, M.; Gilman, R.H.; Alvarez, J.O. Adverse Effects of High-dose Vitamin A Supplements in Children Hospitalized With Pneumonia. Pediatrics 1998, 101, e3. [Google Scholar] [CrossRef] [Green Version]
- Soofi, S.; Ariff, S.; Sadiq, K.; Habib, A.; Bhatti, Z.; Ahmad, I.; Hussain, M.; Ali, N.; Cousens, S.; A Bhutta, Z. Evaluation of the uptake and impact of neonatal vitamin A supplementation delivered through the Lady Health Worker programme on neonatal and infant morbidity and mortality in rural Pakistan: An effectiveness trial. Arch. Dis. Child. 2016, 102, 216–223. [Google Scholar] [CrossRef]
- Bhandari, N.; Bhan, M.K.; Sazawal, S. Impact of massive dose of vitamin A given to preschool children with acute diarrhoea on subsequent respiratory and diarrhoeal morbidity. BMJ 1994, 309, 1404–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biswas, R.; Biswas, A.B.; Manna, B.; Bhattacharya, S.K.; Dey, R.; Sarkar, S. Effect of vitamin A supplementation on diarrhoea and acute respiratory tract infection in children. Eur. J. Epidemiol. 1994, 10, 57–61. [Google Scholar] [CrossRef]
- Rahmathullah, L.; Underwood, B.A.; Thulasiraj, R.D.; Milton, R.C. Diarrhea, respiratory infections, and growth are not affected by a weekly low-dose vitamin A supplement: A masked, controlled field trial in children in southern India. Am. J. Clin. Nutr. 1991, 54, 568–577. [Google Scholar] [CrossRef]
- Dibley, M.J.; Sadjimin, T.; Kjolhede, C.L.; Moulton, L. Vitamin A Supplementation Fails to Reduce Incidence of Acute Respiratory Illness and Diarrhea in Preschool-Age Indonesian Children. J. Nutr. 1996, 126, 434–442. [Google Scholar] [CrossRef] [Green Version]
- Barreto, M.; Farenzena, G.; Fiaccone, R.; Santos, L.; Assis, A.; Araújo, M.; Santos, P. Effect of vitamin A supplementation on diarrhoea and acute lower-respiratory-tract infections in young children in Brazil. Lancet 1994, 344, 228–231. [Google Scholar] [CrossRef] [Green Version]
- Venkatarao, T.; Ramakrishnan, R.; Nair, N.G.; Radhakrishnan, S.; Sundaramoorthy, L.; Koya, P.K.; Kumar, S.K. Effect of vitamin A supplementation to mother and infant on morbidity in infancy. Indian Pediatr. 1996, 33, 279–286. [Google Scholar]
- Long, K.Z.; Montoya, Y.; Hertzmark, E.; Santos, J.I.; Rosado, J.L. A double-blind, randomized, clinical trial of the effect of vitamin A and zinc supplementation on diarrheal disease and respiratory tract infections in children in Mexico City, Mexico. Am. J. Clin. Nutr. 2006, 83, 693–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, K.Z.; Rosado, J.L.; Dupont, H.L.; Hertzmark, E.; Santos, J.I. Supplementation with vitamin A reduces watery diarrhoea and respiratory infections in Mexican children. Br. J. Nutr. 2007, 97, 337–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinnock, C.B.; Douglas, R.M.; Badcock, N.R. Vitamin A status in children who are prone to respiratory tract infections. J. Paediatr. Child Health 1986, 22, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Kartasasmita, C.; Rosmayudi, O.; Deville, W.; Demedts, M. Plasma retinol level, vitamin A supplementation and acute respiratory infections in children of 1–5 years old in a developing country. Tuber. Lung Dis. 1995, 76, 563–569. [Google Scholar] [CrossRef]
- Rahman, M.M.; Mahalanabis, D.; Alvarez, J.O.; Wahed, M.A.; Islam, M.A.; Habte, D.; Khaled, M.A. Acute Respiratory Infections Prevent Improvement of Vitamin A Status in Young Infants Supplemented with Vitamin A. J. Nutr. 1996, 126, 628–633. [Google Scholar] [CrossRef] [Green Version]
- Stansfield, S.; Pierre-Louis, M.; Augustin, A.; Lerebours, G. Vitamin A supplementation and increased prevalence of childhood diarrhoea and acute respiratory infections. Lancet 1993, 342, 578–582. [Google Scholar] [CrossRef]
- Fawzi, W.W.; Mbise, R.; Spiegelman, D.; Fataki, M.; Hertzmark, E.; Ndossi, G. Vitamin A supplements and diarrheal and respiratory tract infections among children in Dar es Salaam, Tanzania. J. Pediatr. 2000, 137, 660–667. [Google Scholar] [CrossRef]
- Brown, N.; Roberts, C. Vitamin A for acute respiratory infection in developing countries: A meta-analysis. Acta Paediatr. 2004, 93, 1437–1442. [Google Scholar] [CrossRef]
- Imdad, A.; Mayo-Wilson, E.; Herzer, K.; A Bhutta, Z. Vitamin A supplementation for preventing morbidity and mortality in children from six months to five years of age. Cochrane Database Syst. Rev. 2017, 2017, CD008524. [Google Scholar] [CrossRef]
- Bates, C. Vitamin A. Lancet 1995, 345, 31–35. [Google Scholar] [CrossRef]
- Stephensen, C.B. Vitamin A, Infection, and Immune Function. Annu. Rev. Nutr. 2001, 21, 167–192. [Google Scholar] [CrossRef]
- Larange, A.; Cheroutre, H. Retinoic Acid and Retinoic Acid Receptors as Pleiotropic Modulators of the Immune System. Annu. Rev. Immunol. 2016, 34, 369–394. [Google Scholar] [CrossRef] [PubMed]
- Wirth, J.P.; Petry, N.; Tanumihardjo, S.A.; Rogers, L.M.; McLean, E.; Greig, A.; Garrett, G.S.; Klemm, R.D.W.; Rohner, F. Vitamin A Supplementation Programs and Country-Level Evidence of Vitamin A Deficiency. Nutrients 2017, 9, 190. [Google Scholar] [CrossRef] [PubMed]
- Surman, S.L.; Penkert, R.R.; Sealy, R.E.; Jones, B.G.; Marion, T.N.; Vogel, P.; Hurwitz, J.L. Consequences of Vitamin A Deficiency: Immunoglobulin Dysregulation, Squamous Cell Metaplasia, Infectious Disease, and Death. Int. J. Mol. Sci. 2020, 21, 5570. [Google Scholar] [CrossRef] [PubMed]
- Michaëlsson, K.; Lithell, H.; Vessby, B.; Melhus, H. Serum Retinol Levels and the Risk of Fracture. N. Engl. J. Med. 2003, 348, 287–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, L.S.; Harnack, L.J.; Lazovich, D.; Folsom, A.R. Vitamin A intake and the risk of hip fracture in postmenopausal women: The Iowa Women’s Health Study. Osteoporos. Int. 2004, 15, 552–559. [Google Scholar] [CrossRef] [Green Version]
- Coghlan, D.; Cranswick, N.E. Complementary medicine and vitamin A toxicity in children. Med. J. Aust. 2001, 175, 223–224. [Google Scholar] [CrossRef] [PubMed]
- Borel, P.; Desmarchelier, C.; Nowicki, M.; Bott, R. A Combination of Single-Nucleotide Polymorphisms Is Associated with Interindividual Variability in Dietary β-Carotene Bioavailability in Healthy Men. J. Nutr. 2015, 145, 1740–1747. [Google Scholar] [CrossRef] [Green Version]
- Bohn, T.; Desmarchelier, C.; Dragsted, L.O.; Nielsen, C.S.; Stahl, W.; Rühl, R.; Keijer, J.; Borel, P. Host-related factors explaining interindividual variability of carotenoid bioavailability and tissue concentrations in humans. Mol. Nutr. Food Res. 2017, 61, 61. [Google Scholar] [CrossRef] [PubMed]
- Bohn, T.; Desmarchelier, C.; El, S.N.; Keijer, J.; Van Schothorst, E.; Rühl, R.; Borel, P. β-Carotene in the human body: Metabolic bioactivation pathways—From digestion to tissue distribution and excretion. Proc. Nutr. Soc. 2019, 78, 68–87. [Google Scholar] [CrossRef] [Green Version]
- von Lintig, J.; Moon, J.; Lee, J.; Ramkumar, S. Carotenoid metabolism at the intestinal barrier. Biochim. Biophys. Acta Mol. Cell Biol. Lipids 2020, 1865, 158580. [Google Scholar] [CrossRef] [PubMed]
- Widjaja-Adhi, M.A.K.; Lobo, G.P.; Golczak, M.; Von Lintig, J. A genetic dissection of intestinal fat-soluble vitamin and carotenoid absorption. Hum. Mol. Genet. 2015, 24, 3206–3219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sommer, A.; Djunaedi, E.; Loeden, A.; Tarwotjo, I.; West, K.; Tilden, R.; Mele, L. The Aceh Study Group impact of vitamin a supplementation on childhood mortality. Lancet 1986, 327, 1169–1173. [Google Scholar] [CrossRef]
- Sommer, A.; Hussaini, G.; Tarwotjo, I.; Susanto, D. Increased mortality in children with mild vitamin a deficiency. Lancet 1983, 322, 585–588. [Google Scholar] [CrossRef]
- Cristea, I.A.; Gentili, C. Publication Bias in Trials with and Without Null Findings. JAMA 2019, 322, 1213–1214. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author/Location/Year | Age Range (Month) | Baseline Serum Retionl Status (μmol/L) | Intervention and Duration | Number per Limb | Outcome Measures | Overall Mortality of Study | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| IT | CT | <1 Year | >1 Year | IT | CT | Total | IT | CT | |||
| Anne/Australia/2006 | <132 | 0.50 | 0.80 | 50,000 IU on Days 1 and 5 | 100,000 IU on Days 1 and 5 | 108 | 107 | Days to normalization of SpO2; Days to resolution of fever; Days for respiratory rate to settle; Days in hospital | 0 | 0 | 0 |
| Kjolhede/Guatemala/1995 | 3–48 | 0.92 | 0.87 | 100,000 IU on admission | 200,000 IU on admission | 132 | 131 | Days to normalization of SpO2; Days to resolution of fever; Days for respiratory rate to settle; Days in hospital | 4 | 2 | 2 |
| Mahalanabis/India/2004 | 2–24 | 0.71 ± 0.53 | 0.71 ± 0.62 | 33,333 IU twice daily for 4 d | 33,333 IU twice daily for 4 d | 38 | 38 | Days to resolution of fever; Days for respiratory rate to settle | 1 | 1 | 0 |
| Quinlan/Chicago/1996 | 2–58 | - | 100,000 IU on admission | 100,000 IU on admission | 21 | 11 | Days to normalization of SpO2; Days in hospital | 0 | 0 | 0 | |
| Fawzi/Tanzanian/1998 | 6–60 | - | - | 200,000 IU over 2 d | 400,000 IU over 2 d | 346 | 341 | Days to normalization of SpO2; Days to resolution of fever; Days for respiratory rate to settle; Days in hospital | 21 | 13 | 8 |
| Nacul/Brazil/1997 | 6–59 | 0.45 ± 0.34 | 0.38 ± 0.28 | 200,000 IU over 2 d | 400,000 IU over 2 d | 239 | 233 | Days to normalization of SpO2; Days to resolution of fever; Days for respiratory rate to settle | 4 | 2 | 2 |
| Rodríguez/Ecuador/2005 | 2–59 | 1.26 ± 0.54 | 1.35 ± 0.59 | 50,000 IU on admission | 100,000 IU on admission | 121 | 118 | Days to normalization of SpO2; Days to resolution of fever; Days for respiratory rate to settle | 5 | 2 | 3 |
| Si/Vietnam/1997 | 1–59 | - | - | 200,000 IU over 2 d | 400,000 IU over 2 d | 279 | 309 | Days to resolution of fever; Days for respiratory rate to settle; Days in hospital | 4 | 1 | 3 |
| Stephensen/Peru/1998 | 3–120 | 0.24 ± 0.17 | 0.31 ± 0.24 | 100,000 IU on admission and 50,000 IU the nextday | 200,000 IU onadmission and 100,000 IU the next day | 48 | 47 | Days in hospital | 0 | 0 | 0 |
| Bhandari/Govindpuri/1994 | 12–60 | - | - | - | 200,000 IU on admission | 422 | 420 | Incidence of Acute lower respiratory tract Infection | - | - | - |
| Biswas/Calcutta/1994 | 12–71 | - | - | - | 200,000 IU on admission | 91 | 83 | Mean number of episodes; Mean duration per episode; Mean duration per child | 0 | 0 | 0 |
| Rahmathullah/India/1991 | 6–60 | - | - | 8375 IU/week, 52 weeks | 8375 IU/week, 52 weeks | 7655 | 7764 | Incidence of Acute lower respiratory tract Infection | - | - | - |
| Dibley/Indonesian/1996 | 6–47 | - | - | 103,000 IU/4 months, 2 years | 206,000 IU/4 months, 2 years | 396 | 386 | Incidence of Acute lower respiratory tract Infection; Incidence of Acute respiratory tract infection | 1 | 0 | 1 |
| Chen/China/2013 | 36–72 | 1.15 ± 0.30 | 1.14 ± 0.27 | - | 200,000 IU on admission | 95 | 104 | Incidence of Acute respiratory tract infection; Cough (days) | - | - | - |
| Barreto/Brazil/1994 | 6–48 | - | - | 100,000 IU/4 months, 1 year | 200,000 IU/4 months, 1 year | 620 | 620 | Incidence of Acute lower respiratory tract Infection; Cough (days) | 4 | 2 | 2 |
| Venkatarao/India/1996 | 0–12 | - | - | 200,000 IU at 6 months old | - | 311 | 297 | Mean duration per child | 12 | 3 | 9 |
| Long/Mexico/2006 | 6–15 | - | - | 20,000 IU/2 months, 1 year | 45,000 IU/2 months, 1 year | 180 | 183 | Incidence of Acute lower respiratory tract Infection | - | - | - |
| Pinnock/Adelaide/1986 | 12–48 | 4.21 ± 0.15 | 4.08 ± 0.17 | - | 1500 IU/day, 5 months | 76 | 71 | Mean number of episodes; Cough (days) | - | - | - |
| Kartasasmita/India/1995 | 12–54 | 2.71 ± 0.65 | 1.60 ± 0.59 | - | 200,000 IU on admission and 6 months | 126 | 143 | Mean number of episodes; Mean duration per episode | - | - | - |
| Rahman/Bangladesh/1996 | 2.5 | 0.43 ± 0.24 | 0.42 ± 0.20 | 50,000 IU on 4 week, 8 week | - | 84 | 81 | Mean number of episodes; Mean duration per child | - | - | - |
| Sempertegui/Ecuador/1999 | 6–36 | 3.40 ± 0.93 | 3.49 ± 0.91 | 10,000 IU/week, 40 weeks | 10,000 IU/week, 40 weeks | 200 | 200 | Incidence of Acute lower respiratory tract Infection; Incidence of Acute respiratory tract infection | - | - | - |
| Stansfield/Haiti/1993 | 6–83 | - | - | 100,000 IU/4 months, 1 year | 200,000 IU/4 months, 1 year | 8351 | 6993 | Incidence of Acute respiratory tract infection | 72 | 36 | 36 |
| Fawzi/Tanzania/2000 | 6–60 | - | - | 100,000 IU/4 months, 1 year | 200,000 IU/4 months, 1 year | 289 | 285 | Mean number of episodes; Cough (days); Incidence of Acute respiratory tract infection | - | - | - |
| Swami/Chandigarh/2007 | 12–60 | - | - | - | 200,000 IU on admission | 276 | 252 | Mean number of episodes | 2 | 0 | 2 |
| Long/Mexican/2007 | 6–15 | - | - | 20,000 IU/2 months, 1 year | 45,000 IU/2 months, 1 year | 97 | 98 | Incidence of Acute respiratory tract infection | - | - | - |
| Soofi/Pakistan/2017 | 0–1 | - | - | 50,000 IU on admission | - | 5380 | 5648 | Incidence of Acute lower respiratory tract Infection | 243 | 128 | 115 |
| First Author | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Other Bias |
|---|---|---|---|---|---|---|---|
| Anne 2006 | low | low | low | unclear | low | low | low |
| Kjolhede 1995 | unclear | low | unclear | unclear | high | low | unclear |
| Mahalanabis 2004 | low | low | low | low | low | low | low |
| Quinlan 1996 | unclear | unclear | low | unclear | low | high | high |
| Fawzi 1998 | unclear | low | low | unclear | low | low | low |
| Nacul 1997 | low | low | low | low | low | low | low |
| Rodríguez 2005 | low | low | low | low | low | low | low |
| Si 1997 | unclear | unclear | low | unclear | unclear | unclear | high |
| Stephensen 1998 | low | low | low | unclear | low | unclear | low |
| Bhandari 1994 | low | low | low | low | low | low | low |
| Biswas 1994 | low | low | low | low | high | unclear | unclear |
| Rahmathullah 1991 | unclear | low | low | unclear | low | high | unclear |
| Dibley 1996 | low | low | low | unclear | unclear | high | high |
| Chen 2013 | unclear | high | low | unclear | low | unclear | high |
| Barreto 1994 | low | low | low | low | high | low | low |
| Venkatarao 1996 | unclear | low | high | high | high | unclear | high |
| Long 2006 | low | low | low | unclear | high | low | unclear |
| Pinnock 1986 | unclear | low | low | unclear | high | unclear | unclear |
| Kartasasmita 1995 | low | unclear | unclear | unclear | low | unclear | high |
| Rahman 1996 | unclear | low | low | unclear | high | low | high |
| Sempertegui 1999 | low | low | low | unclear | high | low | high |
| Stansfield 1993 | low | low | low | low | low | low | low |
| Fawzi 2000 | unclear | low | low | unclear | low | low | unclear |
| Swami 2007 | unclear | unclear | unclear | unclear | high | high | high |
| Long 2007 | low | low | low | unclear | low | unclear | unclear |
| Soofi 2017 | low | low | low | low | low | unclear | unclear |
| Subgroup | Number of Studies | RR | 95%CI | p | Heterogeneity | ||
|---|---|---|---|---|---|---|---|
| I2 | p | ||||||
| dose | |||||||
| high | 4 | 1.131 | (1.065, 1.200) | <0.001 | 19.3% | 0.294 | |
| standard | 3 | 0.815 | (0.643, 1.032) | 0.090 | 59.4% | 0.085 | |
| frequency | |||||||
| low | 1 | 0.650 | (0.392, 1.078) | 0.095 | |||
| medium | 3 | 1.143 | (1.066, 1.225) | <0.001 | 32.0% | 0.230 | |
| high | 3 | 0.923 | (0.764, 1.115) | 0.406 | 70.3% | 0.035 | |
| area | |||||||
| Asia | 2 | 0.893 | (0.552, 1.446) | 0.645 | 73.5% | 0.052 | |
| Other areas | 5 | 1.033 | (0.893, 1.195) | 0.658 | 79.2% | 0.001 | |
| Nutritional status | |||||||
| stunted | 3 | 0.821 | (0.457, 1.474) | 0.509 | 59.7% | 0.083 | |
| wasted | 2 | 0.589 | (0.208, 1.668) | 0.319 | 52.3% | 0.148 | |
| normal | 3 | 1.656 | (1.302, 2.106) | <0.001 | 14.9% | 0.309 | |
| Subgroup | Number of Studies | WMD | 95%CI | p | Heterogeneity | ||
|---|---|---|---|---|---|---|---|
| I2 | p | ||||||
| dose | |||||||
| standard | 4 | −0.683 | (−1.684, 0.318) | 0.181 | 86.9% | <0.001 | |
| high | 2 | 0.188 | (−0.327, 0.702) | 0.475 | 0.0% | 0.971 | |
| frequency | |||||||
| low | 4 | −0.081 | (−0.522, 0.360) | 0.719 | 0.0% | 0.860 | |
| median | 1 | 0.180 | (−0.473, 0.833) | 0.589 | |||
| high | 1 | −1.500 | (−1.643, 1.357) | <0.001 | |||
| area | |||||||
| Asia | 4 | −0.081 | (−0.522, 0.360) | 0.719 | 0.0% | 0.860 | |
| Other areas | 2 | −0.691 | (−2.337, 0.954) | 0.410 | 95.9% | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Lu, Y.; Wang, S.; Yang, L.; Xia, H.; Sun, G. Excessive Vitamin A Supplementation Increased the Incidence of Acute Respiratory Tract Infections: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 4251. https://doi.org/10.3390/nu13124251
Zhang Y, Lu Y, Wang S, Yang L, Xia H, Sun G. Excessive Vitamin A Supplementation Increased the Incidence of Acute Respiratory Tract Infections: A Systematic Review and Meta-Analysis. Nutrients. 2021; 13(12):4251. https://doi.org/10.3390/nu13124251
Chicago/Turabian StyleZhang, Yihan, Yifei Lu, Shaokang Wang, Ligang Yang, Hui Xia, and Guiju Sun. 2021. "Excessive Vitamin A Supplementation Increased the Incidence of Acute Respiratory Tract Infections: A Systematic Review and Meta-Analysis" Nutrients 13, no. 12: 4251. https://doi.org/10.3390/nu13124251
APA StyleZhang, Y., Lu, Y., Wang, S., Yang, L., Xia, H., & Sun, G. (2021). Excessive Vitamin A Supplementation Increased the Incidence of Acute Respiratory Tract Infections: A Systematic Review and Meta-Analysis. Nutrients, 13(12), 4251. https://doi.org/10.3390/nu13124251