
Associations between Circulating Markers of Cholesterol Homeostasis and Macrovascular Events among Patients Undergoing Hemodialysis

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
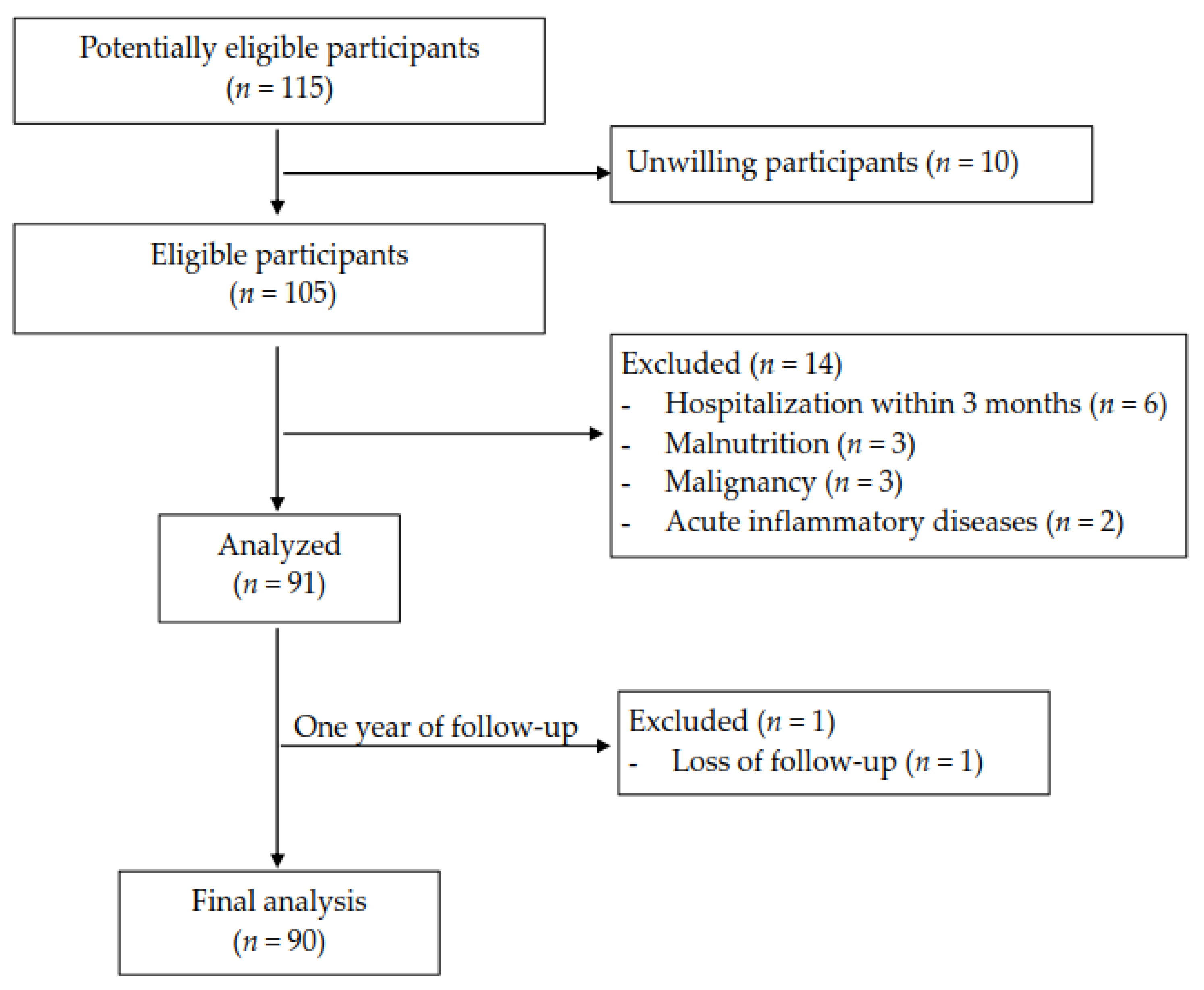
2.1. Study Design and Participants
2.2. Definition and Assessment of Macrovascular Events
2.3. Biochemistry
2.4. Measurements of Circulating Markers of Cholesterol Homeostasis
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Circulating Markers of Cholesterol Homeostasis in HD Patients
3.2. Differences between HD Patients with and without Macrovascular Events
3.3. Correlations of Cholesterol Homeostasis Markers
3.4. Predictions of Macrovascular Events in HD Patients by Cholesterol Homeostasis Markers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hou, F.; Jiang, J.; Chen, J.; Yu, X.; Zhou, Q.; Chen, P.; Mei, C.; Xiong, F.; Shi, W.; Zhou, W.; et al. China collaborative study on dialysis: A multi-centers cohort study on cardiovascular diseases in patients on maintenance dialysis. BMC Nephrol. 2012, 13, 94. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.H.; Hung, S.Y.; Sung, J.M.; Hung, K.Y.; Wang, J.D. Risk of stroke in long-term dialysis patients compared with the general population. Am. J. Kidney Dis 2014, 63, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.-C.; Lee, Y.-T.; Li, L.-C.; Ng, H.-Y.; Kuo, W.-H.; Lin, P.-T.; Liao, Y.-C.; Chiou, T.T.-Y.; Lee, C.-T. The Number of Comorbidities Predicts Renal Outcomes in Patients with Stage 3–5 Chronic Kidney Disease. J. Clin. Med. 2018, 7, 493. [Google Scholar] [CrossRef] [Green Version]
- De Jager, D.J.; Grootendorst, D.C.; Jager, K.J.; Van Dijk, P.C.; Tomas, L.M.J.; Ansell, D.; Collart, F.; Finne, P.; Heaf, J.G.; De Meester, J.; et al. Cardiovascular and Noncardiovascular Mortality Among Patients Starting Dialysis. JAMA 2009, 302, 1782–1789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United States Renal Data System. 2020 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2020.
- Chang, T.Y.; Chang, C.C.; Ohgami, N.; Yamauchi, Y. Cholesterol sensing, trafficking, and esterification. Annu. Rev. Cell Dev. Biol. 2006, 22, 129–157. [Google Scholar] [CrossRef]
- Tabas, I. Consequences of cellular cholesterol accumulation: Basic concepts and physiological implications. J. Clin. Investig. 2002, 110, 905–911. [Google Scholar] [CrossRef]
- Ikonen, E. Cellular cholesterol trafficking and compartmentalization. Nat. Rev. Mol. Cell Biol. 2008, 9, 125–138. [Google Scholar] [CrossRef] [PubMed]
- Kruit, J.K.; Groen, A.K.; van Berkel, T.J.; Kuipers, F. Emerging roles of the intestine in control of cholesterol metabolism. World J. Gastroenterol. 2006, 12, 6429–6439. [Google Scholar] [CrossRef]
- Cohen, D.E. Balancing cholesterol synthesis and absorption in the gastrointestinal tract. J. Clin. Lipidol. 2008, 2, S1–S3. [Google Scholar] [CrossRef] [Green Version]
- Miettinen, T.A.; Tilvis, R.S.; Kesäniemi, Y.A. Serum cholestanol and plant sterol levels in relation to cholesterol metabolism in middle-aged men. Metabolism 1989, 38, 136–140. [Google Scholar] [CrossRef]
- Miettinen, T.A.; Tilvis, R.S.; Kesäniemi, Y.A. Serum plant sterols and cholesterol precursors reflect cholesterol absorption and synthesis in volunteers of a randomly selected male population. Am. J. Epidemiol. 1990, 131, 20–31. [Google Scholar] [CrossRef] [Green Version]
- Simonen, P.; Gylling, H.; Miettinen, T.A. The validity of serum squalene and non-cholesterol sterols as surrogate markers of cholesterol synthesis and absorption in type 2 diabetes. Atherosclerosis 2008, 197, 883–888. [Google Scholar] [CrossRef]
- Matthan, N.R.; Raeini-Sarjaz, M.; Lichtenstein, A.H.; Ausman, L.M.; Jones, P.J. Deuterium uptake and plasma cholesterol precursor levels correspond as methods for measurement of endogenous cholesterol synthesis in hypercholesterolemic women. Lipids 2000, 35, 1037–1044. [Google Scholar] [CrossRef]
- Sauter, G.; Berr, F.; Beuers, U.; Fischer, S.; Paumgartner, G. Serum concentrations of 7alpha-hydroxy-4-cholesten-3-one reflect bile acid synthesis in humans. Hepatology 1996, 24, 123–126. [Google Scholar] [CrossRef]
- Igel-Korcagova, A.; Raab, P.; Brensing, K.A.; Pöge, U.; Klehr, H.U.; Igel, M.; von Bergmann, K.; Sudhop, T. Cholesterol metabolism in patients with chronic renal failure on hemodialysis. J. Nephrol. 2003, 16, 850–854. [Google Scholar]
- Rogacev, K.S.; Pinsdorf, T.; Weingärtner, O.; Gerhart, M.K.; Welzel, E.; van Bentum, K.; Popp, J.; Menzner, A.; Fliser, D.; Lütjohann, D.; et al. ; et al. Cholesterol synthesis, cholesterol absorption, and mortality in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2012, 7, 943–948. [Google Scholar] [CrossRef] [Green Version]
- Haroon, S.; Davenport, A. Choosing a dialyzer: What clinicians need to know. Hemodial. Int. 2018, 22, S65–S74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knopfholz, J.; Disserol, C.C.D.; Pierin, A.J.; Schirr, F.L.; Streisky, L.; Takito, L.L.; Ledesma, P.M.; Faria-Neto, J.R.; Olandoski, M.; Da Cunha, C.L.P.; et al. Validation of the Friedewald Formula in Patients with Metabolic Syndrome. Cholesterol 2014, 2014, 261878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthan, N.R.; Giovanni, A.; Schaefer, E.J.; Brown, B.G.; Lichtenstein, A.H. Impact of simvastatin, niacin, and/or antioxidants on cholesterol metabolism in cad patients with low hdl. J. Lipid Res. 2003, 44, 800–806. [Google Scholar] [CrossRef] [Green Version]
- Fellstrom, B.C.; Jardine, A.G.; Schmieder, R.E.; Holdaas, H.; Bannister, K.; Beutler, J.; Chae, D.W.; Chevaile, A.; Cobbe, S.M.; Gronhagen-Riska, C.; et al. Rosuvastatin and cardiovascular events in patients undergoing hemodialysis. N. Engl. J. Med. 2009, 360, 1395–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wanner, C.; Krane, V.; Marz, W.; Olschewski, M.; Mann, J.F.; Ruf, G.; Ritz, E.; German, D.; Dialysis Study, I. Atorvastatin in patients with type 2 diabetes mellitus undergoing hemodialysis. N. Engl. J. Med. 2005, 353, 238–248. [Google Scholar] [CrossRef]
- Cholesterol Treatment Trialists’ (CTT) Collaboration. Efficacy and safety of more intensive lowering of LDL cholesterol: A meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 2010, 376, 1670–1681. [Google Scholar] [CrossRef] [Green Version]
- Berge, K.E.; Tian, H.; Graf, G.A.; Yu, L.; Grishin, N.V.; Schultz, J.; Kwiterovich, P.; Shan, B.; Barnes, R.; Hobbs, H.H. Accumulation of dietary cholesterol in sitosterolemia caused by mutations in adjacent abc transporters. Science 2000, 290, 1771–1775. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.H.; Lu, K.; Hazard, S.; Yu, H.; Shulenin, S.; Hidaka, H.; Kojima, H.; Allikmets, R.; Sakuma, N.; Pegoraro, R.; et al. Identification of a gene, abcg5, important in the regulation of dietary cholesterol absorption. Nat. Genet. 2001, 27, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Assmann, G.; Cullen, P.; Erbey, J.; Ramey, D.R.; Kannenberg, F.; Schulte, H. Plasma sitosterol elevations are associated with an increased incidence of coronary events in men: Results of a nested case-control analysis of the prospective cardiovascular münster (procam) study. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 13–21. [Google Scholar] [CrossRef]
- Matthan, N.R.; Pencina, M.; LaRocque, J.M.; Jacques, P.F.; D’Agostino, R.B.; Schaefer, E.J.; Lichtenstein, A.H. Alterations in cholesterol absorption/synthesis markers characterize framingham offspring study participants with chd. J. Lipid Res. 2009, 50, 1927–1935. [Google Scholar] [CrossRef] [Green Version]
- Rajaratnam, R.A.; Gylling, H.; Miettinen, T.A. Independent association of serum squalene and noncholesterol sterols with coronary artery disease in postmenopausal women. J. Am. Coll. Cardiol. 2000, 35, 1185–1191. [Google Scholar] [CrossRef] [Green Version]
- Glueck, C.J.; Speirs, J.; Tracy, T.; Streicher, P.; Illig, E.; Vandegrift, J. Relationships of serum plant sterols (phytosterols) and cholesterol in 595 hypercholesterolemic subjects, and familial aggregation of phytosterols, cholesterol, and premature coronary heart disease in hyperphytosterolemic probands and their first-degree relatives. Metabolism 1991, 40, 842–848. [Google Scholar] [PubMed]
- Pinedo, S.; Vissers, M.N.; von Bergmann, K.; Elharchaoui, K.; Lütjohann, D.; Luben, R.; Wareham, N.J.; Kastelein, J.J.; Khaw, K.T.; Boekholdt, S.M. Plasma levels of plant sterols and the risk of coronary artery disease: The prospective epic-norfolk population study. J. Lipid Res. 2007, 48, 139–144. [Google Scholar] [CrossRef]
- Fassbender, K.; Lütjohann, D.; Dik, M.G.; Bremmer, M.; König, J.; Walter, S.; Liu, Y.; Letièmbre, M.; von Bergmann, K.; Jonker, C. Moderately elevated plant sterol levels are associated with reduced cardiovascular risk--the lasa study. Atherosclerosis 2008, 196, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Wilund, K.R.; Yu, L.; Xu, F.; Vega, G.L.; Grundy, S.M.; Cohen, J.C.; Hobbs, H.H. No association between plasma levels of plant sterols and atherosclerosis in mice and men. Arterioscler Thromb. Vasc. Biol. 2004, 24, 2326–2332. [Google Scholar] [CrossRef] [Green Version]
- Weingärtner, O.; Lütjohann, D.; Meyer, S.; Fuhrmann, A.; Cremers, B.; Seiler-Mußler, S.; Schött, H.F.; Kerksiek, A.; Friedrichs, S.; Ulbricht, U.; et al. Low serum lathosterol levels associate with fatal cardiovascular disease and excess all-cause mortality: A prospective cohort study. Clin. Res. Cardiol. 2019, 108, 1381–1385. [Google Scholar] [CrossRef]
- Drukker, A.; Levy, E.; Bronza, N.; Stankiewicz, H.; Goldstein, R. Impaired intestinal fat absorption in chronic renal failure. Nephron 1982, 30, 154–160. [Google Scholar] [CrossRef]
- Björkhem, I.; Miettinen, T.; Reihnér, E.; Ewerth, S.; Angelin, B.; Einarsson, K. Correlation between serum levels of some cholesterol precursors and activity of hmg-coa reductase in human liver. J. Lipid Res. 1987, 28, 1137–1143. [Google Scholar] [CrossRef]
- Kempen, H.J.; Glatz, J.F.; Gevers Leuven, J.A.; van der Voort, H.A.; Katan, M.B. Serum lathosterol concentration is an indicator of whole-body cholesterol synthesis in humans. J. Lipid Res. 1988, 29, 1149–1155. [Google Scholar] [CrossRef]
- Baigent, C.; Landray, M.J.; Reith, C.; Emberson, J.; Wheeler, D.C.; Tomson, C.; Wanner, C.; Krane, V.; Cass, A.; Craig, J.; et al. The effects of lowering ldl cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (study of heart and renal protection): A randomised placebo-controlled trial. Lancet 2011, 377, 2181–2192. [Google Scholar] [CrossRef] [Green Version]
- Lupattelli, G.; Pirro, M.; Mannarino, M.R.; Siepi, D.; Roscini, A.R.; Schillaci, G.; Mannarino, E. Visceral fat positively correlates with cholesterol synthesis in dyslipidaemic patients. Eur. J. Clin. Investig. 2012, 42, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Mashnafi, S.; Plat, J.; Mensink, R.P.; Baumgartner, S. Non-Cholesterol Sterol Concentrations as Biomarkers for Cholesterol Absorption and Synthesis in Different Metabolic Disorders: A Systematic Review. Nutrients 2019, 11, 124. [Google Scholar] [CrossRef] [Green Version]
- Simonen, P.P.; Gylling, H.; Miettinen, T.A. Body weight modulates cholesterol metabolism in non-insulin dependent type 2 diabetics. Obes. Res. 2002, 10, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Simonen, P.; Gylling, H.; Howard, A.N.; Miettinen, T.A. Introducing a new component of the metabolic syndrome: Low cholesterol absorption. Am. J. Clin. Nutr. 2000, 72, 82–88. [Google Scholar] [CrossRef] [Green Version]
- Anderson, G.H.; Woodend, D. Effect of glycemic carbohydrates on short-term satiety and food intake. Nutr. Rev. 2003, 61, S17–S26. [Google Scholar] [CrossRef]
- Katan, M.B.; Grundy, S.M.; Jones, P.; Law, M.; Miettinen, T.; Paoletti, R. Efficacy and safety of plant stanols and sterols in the management of blood cholesterol levels. Mayo Clin. Proc. 2003, 78, 965–978. [Google Scholar] [CrossRef] [Green Version]
- Kendrick, J.; Chonchol, M.B. Nontraditional risk factors for cardiovascular disease in patients with chronic kidney disease. Nat. Clin. Pract. Nephrol. 2008, 4, 672–681. [Google Scholar] [CrossRef] [PubMed]
- Yao, Q.; Pecoits-Filho, R.; Lindholm, B.; Stenvinkel, P. Traditional and non-traditional risk factors as contributors to atherosclerotic cardiovascular disease in end-stage renal disease. Scand. J. Urol. Nephrol. 2004, 38, 405–416. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | HD (n = 90) | Healthy Control (n = 9) | p |
|---|---|---|---|
| Age, years | 65 ± 7 | 62 ± 11 | 0.196 |
| Sex | 1.000 | ||
| Female | 45 (50.0%) | 4 (44.4%) | |
| Male | 45 (50.0%) | 5 (55.6%) | |
| BMI, kg/m2 | 22.6 ± 4.0 | 22.1 ± 3.1 | 0.766 |
| Systolic blood pressure, mmHg | 137 ± 30 | N/A | |
| Diastolic blood pressure, mmHg | 67 ± 14 | N/A | |
| Dialysis vintage, years | 10.4 ± 7.49 | N/A | – |
| Diabetes | 16 (17.8%) | 0 (0 %) | – |
| Etiologies of renal failure | – | ||
| Primary kidney disease | 37 (41.1%) | N/A | |
| Systemic disease | 37 (41.1%) | N/A | |
| Others | 16 (17.8%) | N/A | |
| Desmosterol, 102 mmol/mol cholesterol | 61.6 ± 86.5 | 65.2 ± 39.9 | 0.523 |
| Lathosterol, 102 mmol/mol cholesterol | 111.6 ± 95.9 | 157.2 ± 136.3 | 0.499 |
| Campesterol, 102 mmol/mol cholesterol | 330.0 ± 179.5 | 207.9 ± 91.4 | 0.023 |
| Sitosterol, 102 mmol/mol cholesterol | 218.4 ± 128.4 | 168.3 ± 89.0 | 0.199 |
| Cholesterol metabolic balance score | 0.4 ± 0.3 | 0.7 ± 0.6 | 0.109 |
| Laboratory measurements | |||
| Hemoglobin, g/dL | 10.7 ± 1.3 | 13.5 ± 1.9 | <0.001 |
| Albumin, g/dL | 3.9 ± 0.3 | 4.3 ± 0.3 | 0.015 |
| BUN, mg/dL * | 69.0 (57.0–83.0) | 14.0 (13.0–16.0) | <0.001 |
| Cr, mg/dL | 10.4 ± 2.1 | 1.0 ± 0.4 | <0.001 |
| Total Cholesterol, mg/dL * | 153.5 (136.0–183.0) | 191.0 (177.0–199.0) | 0.005 |
| Triglyceride, mg/dL * | 114.5 (84.0 –165.0) | 117.0 (84.0–131.0) | 0.789 |
| HDL-C, mg/dL | 45.4 ± 15.3 | 52.1 ± 9.6 | 0.049 |
| LDL-C, mg/dL | 90.2 ± 34.6 | 122.3 ± 41.1 | 0.005 |
| Variables | With Events (n = 14) | Without Events (n = 76) | p |
|---|---|---|---|
| Age, years | 69 ± 8 | 64 ± 6 | <0.001 |
| Sex | 0.144 | ||
| Female | 4 (28.6%) | 41 (53.9%) | |
| Male | 10 (71.4%) | 35 (46.1%) | |
| BMI, kg/m2 | 24.0 ± 6.0 | 22.3 ± 3.3 | <0.001 |
| Systolic blood pressure, mmHg | 136 ± 30 | 154 ± 24 | 0.094 |
| Diastolic blood pressure, mmHg | 67 ± 15 | 68 ± 10 | 0.528 |
| Dialysis vintage, years | 11.4 ± 9.1 | 10.2 ± 7.2 | <0.001 |
| Diabetes | 3 (21.4%) | 13 (17.1%) | 0.709 |
| Desmosterol, 102 mmol/mol cholesterol | 61.7 ± 49.6 | 61.5 ± 91.9 | 0.925 |
| Lathosterol, 102 mmol/mol cholesterol | 99.1 ± 108.0 | 113.9 ± 94.1 | 0.214 |
| Campesterol, 102 mmol/mol cholesterol | 298.1 ± 139.7 | 335.9 ± 186.0 | 0.652 |
| Sitosterol, 102 mmol/mol cholesterol | 199.2 ± 83.5 | 221.9 ± 135.2 | 0.854 |
| Cholesterol metabolic balance score | 0.4 ± 0.4 | 0.4 ± 0.3 | 0.544 |
| Laboratory measurements | |||
| Hemoglobin, g/dL | 10.7 ± 1.3 | 10.7 ± 1.3 | 0.982 |
| Albumin, g/dL | 3.9 ± 0.4 | 3.9 ± 0.3 | 0.551 |
| BUN, mg/dL | 75.0 (64.0–84.0) | 68.0 (56.0–80.0) | 0.319 |
| Cr, mg/dL | 10.5 ± 2.3 | 10.4 ± 2.0 | 0.555 |
| Total Cholesterol, mg/dL * | 141.5 (137.0–164.0) | 158.0 (136.0–186) | 0.157 |
| Triglyceride, mg/dL * | 110.0 (100.0–136.0) | 117.0 (82.0–167.0) | 0.925 |
| HDL-C, mg/dL | 39.9 ± 11.7 | 46.4 ± 15.7 | 0.148 |
| LDL-C, mg/dL | 81.1 ± 20.0 | 91.9 ± 36.6 | 0.395 |
| Variables | Desmosterol | Lathosterol | Campesterol | Sitosterol | Cholesterol Metabolic Balance Score |
|---|---|---|---|---|---|
| Age | −0.15 | −0.18 | −0.16 | −0.13 | −0.08 |
| BMI | −0.07 | 0.32 ** | −0.21 * | −0.30 ** | 0.33 ** |
| Desmosterol | – | 0.40 **** | 0.18 | 0.12 | 0.42 **** |
| Lathosterol | 0.40 **** | – | 0.07 | −0.02 | 0.65 **** |
| Campesterol | 0.18 | 0.07 | – | 0.85 **** | −0.40 *** |
| Sitosterol | 0.12 | −0.02 | 0.85 **** | – | −0.42 **** |
| Cholesterol metabolic balance score | 0.42 **** | 0.65 **** | −0.40 *** | −0.42 **** | – |
| Albumin | −0.07 | 0.14 | −0.11 | −0.03 | 0.08 |
| Total Cholesterol | −0.17 | −0.23 * | −0.18 | −0.16 | −0.11 |
| Triglyceride | −0.18 | 0.06 | −0.28 ** | −0.32 ** | 0.13 |
| HDL-C | 0.15 | −0.14 | 0.18 | 0.22 * | −0.18 |
| LDL-C | −0.19 | −0.23 * | −0.16 | −0.14 | −0.11 |
| Variables | Unadjusted | Full-Adjusted | ||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Desmosterol | 1.000 (0.989–1.006) | 0.994 | 0.997 (0.968–1.008) | 0.699 |
| Lathosterol | 0.998 (0.989–1.004) | 0.598 | 0.997 (0.979–1.011) | 0.697 |
| Campesterol | 0.999 (0.995–1.002) | 0.470 | 1.000 (0.988–1.011) | 0.939 |
| Sitosterol | 0.998 (0.992–1.003) | 0.544 | 1.001 (0.985–1.015) | 0.898 |
| Cholesterol metabolic balance score | 1.012 (0.132–4.993) | 0.989 | 9.003 (0.013–4621.542) | 0.467 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, W.-C.; Kuo, W.-H.; Moi, S.-H.; Chiu, B.; Chen, J.-B.; Yang, C.-H. Associations between Circulating Markers of Cholesterol Homeostasis and Macrovascular Events among Patients Undergoing Hemodialysis. Nutrients 2021, 13, 1014. https://doi.org/10.3390/nu13031014
Lee W-C, Kuo W-H, Moi S-H, Chiu B, Chen J-B, Yang C-H. Associations between Circulating Markers of Cholesterol Homeostasis and Macrovascular Events among Patients Undergoing Hemodialysis. Nutrients. 2021; 13(3):1014. https://doi.org/10.3390/nu13031014
Chicago/Turabian StyleLee, Wen-Chin, Wei-Hung Kuo, Sin-Hua Moi, Barry Chiu, Jin-Bor Chen, and Cheng-Hong Yang. 2021. "Associations between Circulating Markers of Cholesterol Homeostasis and Macrovascular Events among Patients Undergoing Hemodialysis" Nutrients 13, no. 3: 1014. https://doi.org/10.3390/nu13031014
APA StyleLee, W. -C., Kuo, W. -H., Moi, S. -H., Chiu, B., Chen, J. -B., & Yang, C. -H. (2021). Associations between Circulating Markers of Cholesterol Homeostasis and Macrovascular Events among Patients Undergoing Hemodialysis. Nutrients, 13(3), 1014. https://doi.org/10.3390/nu13031014