
Associations between Children’s Genetic Susceptibility to Obesity, Infant’s Appetite and Parental Feeding Practices in Toddlerhood

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
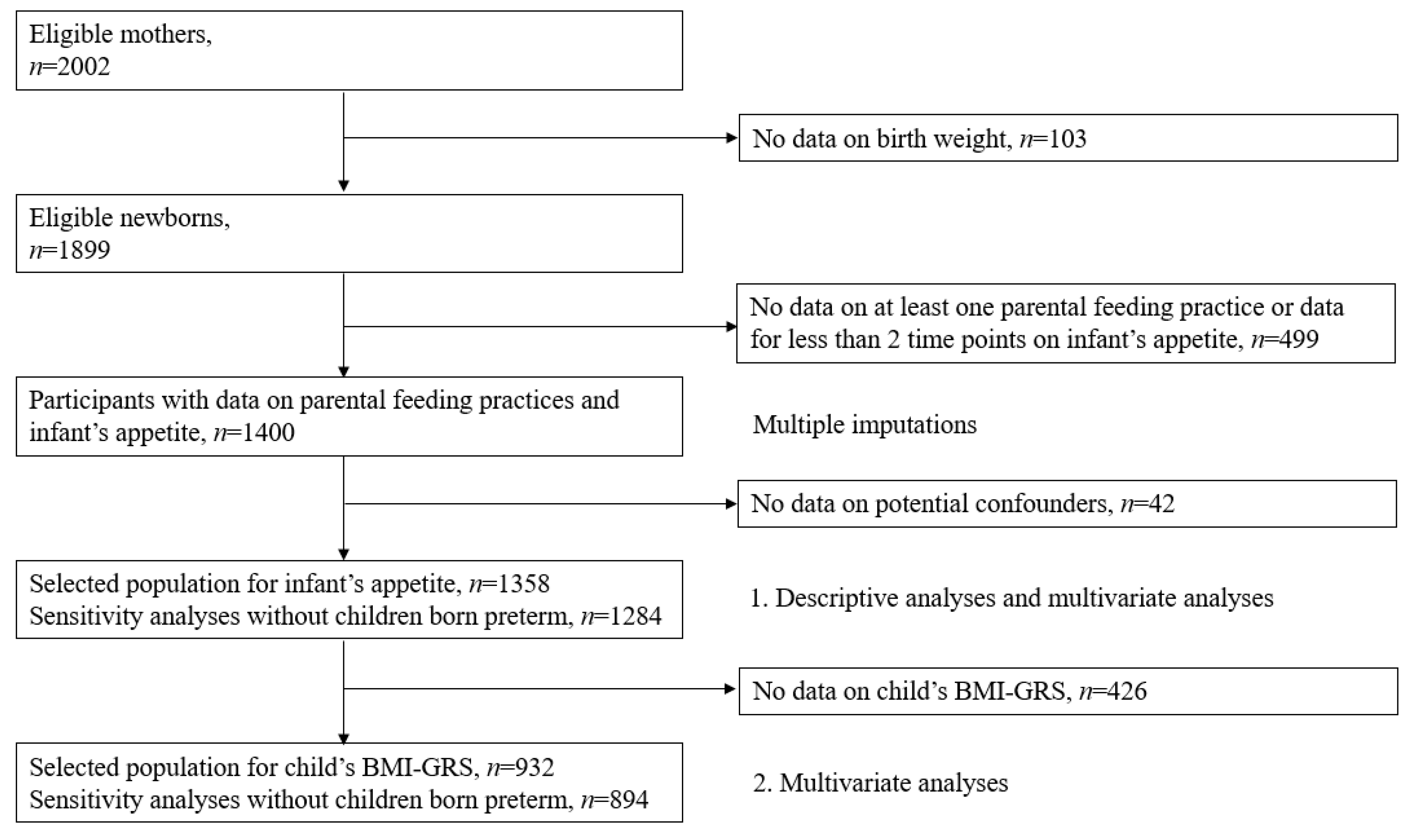
2.1. Study Population
2.2. Infant’s Appetite
2.3. Children’s Genetic Susceptibility to Obesity
2.4. Parental Feeding Practices
2.5. Potential Confounders
2.6. Sample Selection
2.7. Statistical Analyses
2.7.1. Main Analyses
2.7.2. Sensitivity Analyses
3. Results
3.1. Infant’s Appetite and Parental Feeding Practices at 2 Years
3.2. Child’s BMI-GRS and Parental Feeding Practices at 2 Years
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 25 June 2020).
- Reilly, J.J.; Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int. J. Obes. 2011, 35, 891–898. [Google Scholar] [CrossRef] [Green Version]
- Goodarzi, M.O. Genetics of obesity: What genetic association studies have taught us about the biology of obesity and its complications. Lancet Diabetes Endocrinol. 2018, 6, 223–236. [Google Scholar] [CrossRef]
- Wood, A.C. Gene-Environment Interplay in Child Eating Behaviors: What the Role of “Nature” Means for the Effects of “Nurture”. Curr. Nutr. Rep. 2018, 7, 294–302. [Google Scholar] [CrossRef]
- Day, F.R.; Loos, R.J. Developments in obesity genetics in the era of genome-wide association studies. J. Nutr. Nutr. 2011, 4, 222–238. [Google Scholar] [CrossRef]
- De Lauzon-Guillain, B.; Koudou, Y.A.; Botton, J.; Forhan, A.; Carles, S.; Pelloux, V.; Clément, K.; Ong, K.K.; Charles, M.A.; Heude, B. Association between genetic obesity susceptibility and mother-reported eating behaviour in children up to 5 years. Pediatr. Obes. 2019, 14, e12496. [Google Scholar] [CrossRef] [PubMed]
- Kral, T.V.; Faith, M.S. Influences on child eating and weight development from a behavioral genetics perspective. J. Pediatr. Psychol. 2009, 34, 596–605. [Google Scholar] [CrossRef] [Green Version]
- Rodenburg, G.; Kremers, S.P.; Oenema, A.; van de Mheen, D. Associations of children’s appetitive traits with weight and dietary behaviours in the context of general parenting. PLoS ONE 2012, 7, e50642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quah, P.L.; Chan, Y.H.; Aris, I.M.; Pang, W.W.; Toh, J.Y.; Tint, M.T.; Broekman, B.F.; Saw, S.M.; Kwek, K.; Godfrey, K.M.; et al. Prospective associations of appetitive traits at 3 and 12 months of age with body mass index and weight gain in the first 2 years of life. BMC Pediatr. 2015, 15, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Jaarsveld, C.H.; Llewellyn, C.H.; Johnson, L.; Wardle, J. Prospective associations between appetitive traits and weight gain in infancy. Am. J. Clin. Nutr. 2011, 94, 1562–1567. [Google Scholar] [CrossRef]
- Brown, C.L.; Vander Schaaf, E.B.; Cohen, G.M.; Irby, M.B.; Skelton, J.A. Association of Picky Eating and Food Neophobia with Weight: A Systematic Review. Child. Obes. 2016, 12, 247–262. [Google Scholar] [CrossRef] [Green Version]
- Savage, J.S.; Fisher, J.O.; Birch, L.L. Parental influence on eating behavior: Conception to adolescence. J. Law Med. Ethics 2007, 35, 22–34. [Google Scholar] [CrossRef] [Green Version]
- Ventura, A.K.; Birch, L.L. Does parenting affect children’s eating and weight status? Int. J. Behav. Nutr. Phys. Act. 2008, 5, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, R.; Ogden, J. Children’s eating attitudes and behaviour: A study of the modelling and control theories of parental influence. Health Educ. Res. 2004, 19, 261–271. [Google Scholar] [CrossRef] [Green Version]
- Carper, J.L.; Orlet Fisher, J.; Birch, L.L. Young girls’ emerging dietary restraint and disinhibition are related to parental control in child feeding. Appetite 2000, 35, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Yelverton, C.A.; Geraghty, A.A.; O’Brien, E.C.; Killeen, S.L.; Horan, M.K.; Donnelly, J.M.; Larkin, E.; Mehegan, J.; McAuliffe, F.M. Breastfeeding and maternal eating behaviours are associated with child eating behaviours: Findings from the ROLO Kids Study. Eur. J. Clin. Nutr. 2021, 75, 670–679. [Google Scholar] [CrossRef]
- Taveras, E.M.; Scanlon, K.S.; Birch, L.; Rifas-Shiman, S.L.; Rich-Edwards, J.W.; Gillman, M.W. Association of breastfeeding with maternal control of infant feeding at age 1 year. Pediatrics 2004, 114, e577–e583. [Google Scholar] [CrossRef] [Green Version]
- Rhee, K.E.; Coleman, S.M.; Appugliese, D.P.; Kaciroti, N.A.; Corwyn, R.F.; Davidson, N.S.; Bradley, R.H.; Lumeng, J.C. Maternal feeding practices become more controlling after and not before excessive rates of weight gain. Obesity 2009, 17, 1724–1729. [Google Scholar] [CrossRef]
- Fisher, J.O.; Birch, L.L. Restricting access to foods and children’s eating. Appetite 1999, 32, 405–419. [Google Scholar] [CrossRef] [PubMed]
- Blissett, J.; Bennett, C. Cultural differences in parental feeding practices and children’s eating behaviours and their relationships with child BMI: A comparison of Black Afro-Caribbean, White British and White German samples. Eur. J. Clin. Nutr. 2013, 67, 180–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardel, M.; Willig, A.L.; Dulin-Keita, A.; Casazza, K.; Beasley, T.M.; Fernandez, J.R. Parental feeding practices and socioeconomic status are associated with child adiposity in a multi-ethnic sample of children. Appetite 2012, 58, 347–353. [Google Scholar] [CrossRef] [Green Version]
- Gubbels, J.S.; Gerards, S.M.; Kremers, S.P. The association of parenting practices with toddlers’ dietary intake and BMI, and the moderating role of general parenting and child temperament. Public Health Nutr. 2020, 23, 1–9. [Google Scholar] [CrossRef]
- Fisher, J.O.; Birch, L.L. Parents’ restrictive feeding practices are associated with young girls’ negative self-evaluation of eating. J. Am. Diet. Assoc. 2000, 100, 1341–1346. [Google Scholar] [CrossRef] [Green Version]
- Jansen, E.; Mulkens, S.; Jansen, A. Do not eat the red food!: Prohibition of snacks leads to their relatively higher consumption in children. Appetite 2007, 49, 572–577. [Google Scholar] [CrossRef]
- Faith, M.S.; Scanlon, K.S.; Birch, L.L.; Francis, L.A.; Sherry, B. Parent-child feeding strategies and their relationships to child eating and weight status. Obes. Res. 2004, 12, 1711–1722. [Google Scholar] [CrossRef]
- Galloway, A.T.; Fiorito, L.M.; Francis, L.A.; Birch, L.L. ‘Finish your soup’: Counterproductive effects of pressuring children to eat on intake and affect. Appetite 2006, 46, 318–323. [Google Scholar] [CrossRef] [Green Version]
- Webber, L.; Cooke, L.; Hill, C.; Wardle, J. Associations between children’s appetitive traits and maternal feeding practices. J. Am. Diet. Assoc. 2010, 110, 1718–1722. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.; Andrianopoulos, N.; Hesketh, K.; Ball, K.; Crawford, D.; Brennan, L.; Corsini, N.; Timperio, A. Parental use of restrictive feeding practices and child BMI z-score. A 3-year prospective cohort study. Appetite 2010, 55, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Farrow, C.V.; Blissett, J. Controlling feeding practices: Cause or consequence of early child weight? Pediatrics 2008, 121, e164–e169. [Google Scholar] [CrossRef] [PubMed]
- Afonso, L.; Lopes, C.; Severo, M.; Santos, S.; Real, H.; Durao, C.; Moreira, P.; Oliveira, A. Bidirectional association between parental child-feeding practices and body mass index at 4 and 7 y of age. Am. J. Clin. Nutr. 2016, 103, 861–867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, E.; Williams, K.E.; Mallan, K.M.; Nicholson, J.M.; Daniels, L.A. Bidirectional associations between mothers’ feeding practices and child eating behaviours. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, P.W.; Tharner, A.; van der Ende, J.; Wake, M.; Raat, H.; Hofman, A.; Verhulst, F.C.; van Ijzendoorn, M.H.; Jaddoe, V.W.; Tiemeier, H. Feeding practices and child weight: Is the association bidirectional in preschool children? Am. J. Clin. Nutr. 2014, 100, 1329–1336. [Google Scholar] [CrossRef] [Green Version]
- Shloim, N.; Edelson, L.R.; Martin, N.; Hetherington, M.M. Parenting Styles, Feeding Styles, Feeding Practices, and Weight Status in 4-12 Year-Old Children: A Systematic Review of the Literature. Front. Psychol. 2015, 6, 1849. [Google Scholar] [CrossRef] [Green Version]
- Webber, L.; Cooke, L.; Hill, C.; Wardle, J. Child adiposity and maternal feeding practices: A longitudinal analysis. Am. J. Clin. Nutr. 2010, 92, 1423–1428. [Google Scholar] [CrossRef]
- Derks, I.P.; Tiemeier, H.; Sijbrands, E.J.; Nicholson, J.M.; Voortman, T.; Verhulst, F.C.; Jaddoe, V.W.; Jansen, P.W. Testing the direction of effects between child body composition and restrictive feeding practices: Results from a population-based cohort. Am. J. Clin. Nutr. 2017, 106, 783–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eichler, J.; Schmidt, R.; Poulain, T.; Hiemisch, A.; Kiess, W.; Hilbert, A. Stability, Continuity, and Bi-Directional Associations of Parental Feeding Practices and Standardized Child Body Mass Index in Children from 2 to 12 Years of Age. Nutrients 2019, 11, 1751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faith, M.S.; Carnell, S.; Kral, T.V. Genetics of food intake self-regulation in childhood: Literature review and research opportunities. Hum. Hered. 2013, 75, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Dalle Molle, R.; Fatemi, H.; Dagher, A.; Levitan, R.D.; Silveira, P.P.; Dubé, L. Gene and environment interaction: Is the differential susceptibility hypothesis relevant for obesity? Neurosci. BioBehav. Rev. 2017, 73, 326–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heude, B.; Forhan, A.; Slama, R.; Douhaud, L.; Bedel, S.; Saurel-Cubizolles, M.J.; Hankard, R.; Thiebaugeorges, O.; De Agostini, M.; Annesi-Maesano, I.; et al. Cohort Profile: The EDEN mother-child cohort on the prenatal and early postnatal determinants of child health and development. Int. J. Epidemiol. 2016, 45, 353–363. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Zhao, J.H.; Luan, J.; Luben, R.N.; Rodwell, S.A.; Khaw, K.T.; Ong, K.K.; Wareham, N.J.; Loos, R.J. Cumulative effects and predictive value of common obesity-susceptibility variants identified by genome-wide association studies. Am. J. Clin. Nutr. 2010, 91, 184–190. [Google Scholar] [CrossRef] [Green Version]
- Speliotes, E.K.; Willer, C.J.; Berndt, S.I.; Monda, K.L.; Thorleifsson, G.; Jackson, A.U.; Lango Allen, H.; Lindgren, C.M.; Luan, J.; Mägi, R.; et al. Association analyses of 249,796 individuals reveal 18 new loci associated with body mass index. Nat. Genet. 2010, 42, 937–948. [Google Scholar] [CrossRef] [Green Version]
- Elks, C.E.; Heude, B.; de Zegher, F.; Barton, S.J.; Clement, K.; Inskip, H.M.; Koudou, Y.; Cooper, C.; Dunger, D.B.; Ibanez, L.; et al. Associations between genetic obesity susceptibility and early postnatal fat and lean mass: An individual participant meta-analysis. JAMA Pediatr. 2014, 168, 1122–1130. [Google Scholar] [CrossRef]
- Musher-Eizenman, D.; Holub, S. Comprehensive Feeding Practices Questionnaire: Validation of a new measure of parental feeding practices. J. Pediatr. Psychol. 2007, 32, 960–972. [Google Scholar] [CrossRef]
- Musher-Eizenman, D.R.; de Lauzon-Guillain, B.; Holub, S.C.; Leporc, E.; Charles, M.A. Child and parent characteristics related to parental feeding practices. A cross-cultural examination in the US and France. Appetite 2009, 52, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Botton, J.; Heude, B.; Maccario, J.; Ducimetière, P.; Charles, M.A. Postnatal weight and height growth velocities at different ages between birth and 5 y and body composition in adolescent boys and girls. Am. J. Clin. Nutr. 2008, 87, 1760–1768. [Google Scholar] [CrossRef] [Green Version]
- Howe, T.H.; Sheu, C.F.; Wang, T.N. Feeding Patterns and Parental Perceptions of Feeding Issues of Preterm Infants in the First 2 Years of Life. Am. J. Occup. Ther. 2019, 73, 7302205030. [Google Scholar] [CrossRef]
- Eekhout, I.; van de Wiel, M.A.; Heymans, M.W. Methods for significance testing of categorical covariates in logistic regression models after multiple imputation: Power and applicability analysis. BMC Med. Res. Methodol. 2017, 17, 129. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.O.; Birch, L.L. Restricting access to palatable foods affects children’s behavioral response, food selection, and intake. Am. J. Clin. Nutr. 1999, 69, 1264–1272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, S.O.; Frazier-Wood, A.C. Satiety and the Self-Regulation of Food Take in Children: A Potential Role for Gene-Environment Interplay. Curr. Obes. Rep. 2016, 5, 81–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodgers, R.F.; Paxton, S.J.; Massey, R.; Campbell, K.J.; Wertheim, E.H.; Skouteris, H.; Gibbons, K. Maternal feeding practices predict weight gain and obesogenic eating behaviors in young children: A prospective study. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 24. [Google Scholar] [CrossRef] [Green Version]
- Quah, P.L.; Ng, J.C.; Fries, L.R.; Chan, M.J.; Aris, I.M.; Lee, Y.S.; Yap, F.; Godfrey, K.M.; Chong, Y.S.; Shek, L.P.; et al. Longitudinal Analysis Between Maternal Feeding Practices and Body Mass Index (BMI): A Study in Asian Singaporean Preschoolers. Front. Nutr. 2019, 6, 32. [Google Scholar] [CrossRef]
- Selzam, S.; McAdams, T.A.; Coleman, J.R.I.; Carnell, S.; O’Reilly, P.F.; Plomin, R.; Llewellyn, C.H. Evidence for gene-environment correlation in child feeding: Links between common genetic variation for BMI in children and parental feeding practices. PLoS Genet. 2018, 14, e1007757. [Google Scholar] [CrossRef] [Green Version]
- Reed, Z.E.; Micali, N.; Bulik, C.M.; Davey Smith, G.; Wade, K.H. Assessing the causal role of adiposity on disordered eating in childhood, adolescence, and adulthood: A Mendelian randomization analysis. Am. J. Clin. Nutr. 2017, 106, 764–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors Influencing Children’s Eating Behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maynard, L.M.; Galuska, D.A.; Blanck, H.M.; Serdula, M.K. Maternal perceptions of weight status of children. Pediatrics 2003, 111, 1226–1231. [Google Scholar]
- Zhou, Z.; Liew, J.; Yeh, Y.C.; Perez, M. Appetitive Traits and Weight in Children: Evidence for Parents’ Controlling Feeding Practices as Mediating Mechanisms. J. Genet. Psychol. 2020, 181, 1–13. [Google Scholar] [CrossRef]
- Steinsbekk, S.; Belsky, J.; Wichstrøm, L. Parental Feeding and Child Eating: An Investigation of Reciprocal Effects. Child. Dev. 2016, 87, 1538–1549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blissett, J.; Haycraft, E.; Farrow, C. Inducing preschool children’s emotional eating: Relations with parental feeding practices. Am. J. Clin. Nutr. 2010, 92, 359–365. [Google Scholar] [CrossRef] [Green Version]
- Jansen, P.W.; Derks, I.P.M.; Mou, Y.; van Rijen, E.H.M.; Gaillard, R.; Micali, N.; Voortman, T.; Hillegers, M.H.J. Associations of parents’ use of food as reward with children’s eating behaviour and BMI in a population-based cohort. Pediatr. Obes. 2020, 15, e12662. [Google Scholar] [CrossRef]
- de Lauzon-Guillain, B.; Clifton, E.A.; Day, F.R.; Clement, K.; Brage, S.; Forouhi, N.G.; Griffin, S.J.; Koudou, Y.A.; Pelloux, V.; Wareham, N.J.; et al. Mediation and modification of genetic susceptibility to obesity by eating behaviors. Am. J. Clin. Nutr. 2017, 106, 996–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| % (n), Mean (SD) or Median (Q1–Q3) | |||
|---|---|---|---|
| Maternal Characteristics | |||
| Center | |||
| Poitiers | 46.8% (636) | ||
| Nancy | 53.2% (722) | ||
| Age at delivery (years) | 29.9 (4.7) | ||
| Primiparous | 47.2% (641) | ||
| Education level | |||
| <High school diploma | 23.1% (314) | ||
| High school diploma | 17.7% (240) | ||
| 2 years university degree | 23.2% (315) | ||
| 5 years university degree | 36.0% (489) | ||
| Household income (€/month) | |||
| ≤1500 | 12.6% (171) | ||
| 1501–2300 | 29.2% (397) | ||
| 2301–3000 | 28.1% (382) | ||
| >3000 | 30.0% (408) | ||
| Smoker status during pregnancy | 22.0% (299) | ||
| BMI before pregnancy (kg/m2) | 23.1 (4.4) | ||
| Parental Feeding Practices a | |||
| Restriction for health | 3.4 (1.0) | ||
| Restriction for weight | 1.7 (0.6) | ||
| Pressure to eat | 2.3 (0.8) | ||
| Food as a reward | 1.33 (1.00–1.66) | ||
| Emotional feeding | 1.33 (1.00–1.66) | ||
| Child Characteristics | |||
| Boys | 52.1% (707) | ||
| Birth weight (kg) | 3.3 (0.5) | ||
| Gestational age (weeks) | 39.2 (1.7) | ||
| Pre-term birth (<37 weeks) | 5.4% (74) | ||
| Any breastfeeding duration, months | |||
| <1 | 33.3% (452) | ||
| 1 to <4 | 31.0% (421) | ||
| ≥4 | 35.7% (485) | ||
| BMI genetic risk score (0–32 score) | 13.7 (2.5) | ||
| WHO weight for length z-score at 2 years | 0.2 (1.7) | ||
| 4 Months | 8 Months | 12 Months | 24 Months | ||
|---|---|---|---|---|---|
| Infant appetite | |||||
| Needs to be stimulated | 2.7% (36) | 2.7% (36) | 4.8% (62) | 6.6% (90) | |
| Normal appetite | 93.4% (1239) | 95.2% (1252) | 92.0% (1188) | 88% (1194) | |
| Always hungry | 3.9% (52) | 2.1% (27) | 3.3% (42) | 5.4% (73) | |
| 4-to-24-month appetite | |||||
| Low appetite | 11.1% (151) | ||||
| Normal appetite | 77.7% (1055) | ||||
| High appetite | 11.2% (152) | ||||
| Restriction for Health | Restriction for Weight | Pressure to Eat | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Boys | Girls | Boys | Girls | |||||||||
| β [95% CI] | p | β [95% CI] | p | β [95% CI] | p | β [95% CI] | p | β [95% CI] | p | |||
| Unadjusted model | ||||||||||||
| 4-to-24-month appetite | 0.7 | <0.001 | 0.06 | <0.001 | 0.02 | |||||||
| N | 707 | 651 | 707 | 651 | 1358 | |||||||
| Low appetite | 0.07 [−0.19; 0.34] | −0.21 [−0.44; 0.02] | −0.17 [−0.32; −0.01] | −0.12 [−0.26; 0.01] | 0.15 [0.01; 0.29] | |||||||
| Normal appetite | 0 [Ref] | 0 [Ref] | 0 [Ref] | 0 [Ref] | 0 [Ref] | |||||||
| High appetite | −0.07 [−0.29; 0.15] | 0.47 [0.19; 0.76] | 0.06 [−0.07; 0.20] | 0.48 [0.32; 0.65] | 0.15 [0.01; 0.29] | |||||||
| Main analyses * | ||||||||||||
| 4-to-24-month appetite | 0.7 | <0.001 | 0.06 | <0.001 | 0.03 | |||||||
| N | 707 | 651 | 707 | 651 | 1358 | |||||||
| Low appetite | 0.06 [−0.21; 0.33] | −0.22 [−0.46; 0.01] | −0.17 [−0.32; −0.01] | −0.12 [−0.25; 0.01] | 0.15 [0.01; 0.28] | |||||||
| Normal appetite | 0 [Ref] | 0 [Ref] | 0 [Ref] | 0 [Ref] | 0 [Ref] | |||||||
| High appetite | −0.07 [−0.29; 0.16] | 0.44 [0.16; 0.72] | 0.07 [−0.07; 0.20] | 0.46 [0.30; 0.62] | 0.14 [0.00; 0.28] | |||||||
| Sensitivity analyses * | ||||||||||||
| 4-to-24-month appetite, without children born preterm | 0.5 | 0.001 | 0.1 | <0.001 | 0.03 | |||||||
| N | 667 | 617 | 667 | 617 | 1284 | |||||||
| Low appetite | 0.07 [−0.20; 0.35] | −0.13 [−0.37; 0.11] | −0.16 [−0.33; 0.00] | −0.11 [−0.25; 0.02] | 0.16 [0.01; 0.30] | |||||||
| Normal appetite | 0 [Ref] | 0 [Ref] | 0 [Ref] | 0 [Ref] | 0 [Ref] | |||||||
| High appetite | −0.12 [−0.36; 0.12] | 0.50 [0.21; 0.78] | 0.01 [−0.13; 0.15] | 0.49 [0.33; 0.65] | 0.14 [−0.01; 0.28] | |||||||
| 4-to-24-month appetite, further adjusted for WHO weight-for-length z-score | 0.7 | 0.009 | 0.5 | <0.001 | 0.02 | |||||||
| N | 707 | 651 | 707 | 651 | 1358 | |||||||
| Low appetite | 0.06 [−0.21; 0.33] | −0.17 [−0.41; 0.06] | −0.09 [−0.25; 0.07] | −0.06 [−0.20; 0.07] | 0.10 [−0.04; 0.24] | |||||||
| Normal appetite | 0 [Ref] | 0 [Ref] | 0 [Ref] | 0 [Ref] | 0 [Ref] | |||||||
| High appetite | −0.07 [−0.29; 0.16] | 0.38 [0.09; 0.67] | 0.00 [−0.13; 0.13] | 0.40 [0.24; 0.56] | 0.19 [0.05; 0.33] | |||||||
| 4-to-12-month appetite | 0.5 | 0.001 | 0.09 | 0.04 | 0.2 | |||||||
| N | 707 | 651 | 707 | 651 | 1358 | |||||||
| Low appetite | −0.05 [−0.40; 0.31] | −0.36 [−0.63; −0.09] | −0.24 [−0.45; −0.03] | −0.09 [−0.25; 0.06] | 0.01 [−0.16; 0.18] | |||||||
| Normal appetite | 0 [Ref] | 0 [Ref] | 0 [Ref] | 0 [Ref] | 0 [Ref] | |||||||
| High appetite | −0.15 [−0.41; 0.11] | 0.46 [0.10; 0.82] | −0.04 [−0.19; 0.12] | 0.32 [0.11; 0.52] | 0.15 [−0.02; 0.32] | |||||||
| 4-to-24-month appetite, multiple imputation | 0.8 | 0.001 | 0.04 | <0.001 | 0.04 | |||||||
| N | 729 | 671 | 729 | 671 | 1400 | |||||||
| Low appetite | 0.04 [−0.23; 0.31] | −0.22 [−0.45; 0.02] | −0.17 [−0.33; −0.01] | −0.11 [−0.24; 0.02] | 0.13 [0.00; 0.27] | |||||||
| Normal appetite | 0 [Ref] | 0 [Ref] | 0 [Ref] | 0 [Ref] | 0 [Ref] | |||||||
| High appetite | −0.07 [−0.30; 0.15] | 0.43 [0.15; 0.72] | 0.07 [−0.06; 0.20] | 0.45 [0.29; 0.61] | 0.13 [−0.01; 0.27] | |||||||
| Emotional Feeding (Ref = Normal) | ||||||
|---|---|---|---|---|---|---|
| Boys | Girls | |||||
| High | p | High | p | |||
| Unadjusted Model | ||||||
| 4-to-24-month appetite | 0.002 | 0.5 | ||||
| N | 707 | 651 | ||||
| Low appetite | 1.47 [0.85; 2.53] | 0.79 [0.51; 1.25] | ||||
| Normal appetite | 1 [Ref] | 1 [Ref] | ||||
| High appetite | 2.29 [1.41; 3.72] | 1.20 [0.68; 2.11] | ||||
| Main analyses * | ||||||
| 4-to-24-month appetite | 0.004 | 0.5 | ||||
| N | 707 | 651 | ||||
| Low appetite | 1.48 [0.85; 2.58] | 0.79 [0.50; 1.27] | ||||
| Normal appetite | 1 [Ref] | 1 [Ref] | ||||
| High appetite | 2.24 [1.36; 3.68] | 1.13 [0.63; 2.02] | ||||
| Sensitivity analyses * | ||||||
| 4-to-24-month appetite, without children born preterm | 0.006 | 0.7 | ||||
| N | 667 | 617 | ||||
| Low appetite | 1.49 [0.84; 2.64] | 0.82 [0.50; 1.35] | ||||
| Normal appetite | 1 [Ref] | 1 [Ref] | ||||
| High appetite | 2.26 [1.33; 3.85] | 1.05 [0.58; 1.89] | ||||
| 4-to-24-month appetite, further adjusted for WHO weight-for-length z-score | 0.005 | 0.7 | ||||
| N | 707 | 651 | ||||
| Low appetite | 1.54 [0.88; 2.72] | 0.83 [0.52; 1.35] | ||||
| Normal appetite | 1 [Ref] | 1 [Ref] | ||||
| High appetite | 2.16 [1.31; 3.57] | 1.06 [0.59; 1.91] | ||||
| 4-to-12-month appetite | 0.02 | 0.5 | ||||
| N | 707 | 651 | ||||
| Low appetite | 1.40 [0.66; 2.95] | 0.79 [0.46; 1.35] | ||||
| Normal appetite | 1 [Ref] | 1 [Ref] | ||||
| High appetite | 2.32 [1.28; 4.22] | 1.29 [0.61; 2.71] | ||||
| 4-to-24-month appetite, multiple imputation | 0.006 | 0.5 | ||||
| N | 729 | 671 | ||||
| Low appetite | 1.04 [0.70; 1.53] | 0.81 [0.58; 1.14] | ||||
| Normal appetite | 1 [Ref] | 1 [Ref] | ||||
| High appetite | 1.41 [0.99; 2.01] | 1.14 [0.77; 1.69] | ||||
| Restriction for Health | Restriction for Weight | Pressure to Eat | |||||
|---|---|---|---|---|---|---|---|
| β [95% CI] | p | β [95% CI] | p | β [95% CI] | p | ||
| Unadjusted model | |||||||
| Child BMI-GRS, per risk allele (n = 932) | −0.01 [−0.03; 0.02] | 0.6 | 0.01 [−0.01; 0.02] | 0.3 | 0.01 [−0.01; 0.03] | 0.3 | |
| Main analyses * | |||||||
| Child BMI-GRS, per risk allele (n = 932) | −0.01 [−0.03; 0.02] | 0.7 | 0.01 [−0.01; 0.02] | 0.3 | 0.01 [−0.01; 0.03] | 0.3 | |
| Sensitivity analyses * | |||||||
| Child weighted BMI-GRS, per risk allele (n = 932) | −0.01 [−0.03; 0.01] | 0.5 | 0.01 [−0.01; 0.02] | 0.4 | 0.01 [−0.01; 0.02] | 0.6 | |
| Child BMI-GRS without children born preterm, per risk allele (n = 894) | −0.01 [−0.03; 0.02] | 0.7 | 0.01 [−0.01; 0.03] | 0.2 | 0.01 [−0.01; 0.03] | 0.4 | |
| Child BMI-GRS, per risk allele, after multiple imputation (n = 1342) a | 0.00 [−0.03; 0.02] | 0.7 | 0.01 [−0.01; 0.02] | 0.3 | 0.02 [0.00; 0.03] | 0.08 | |
| Emotional Feeding | |||
|---|---|---|---|
| OR [95% CI] | p | ||
| Unadjusted model | |||
| Child BMI-GRS, per risk allele (n = 932) | 1.00 [0.95; 1.05] | 1 | |
| Main analyses * | |||
| Child BMI-GRS, per risk allele (n = 932) | 1.00 [0.95; 1.05] | 0.9 | |
| Sensitivity analyses * | |||
| Child weighted BMI-GRS, per risk allele (n = 932) | 1.01 [0.97; 1.06] | 0.6 | |
| Child BMI-GRS without children born preterm, per risk allele (n = 894) | 1.01 [0.95; 1.06] | 0.8 | |
| Child BMI-GRS, per risk allele, after multiple imputation (n = 1342) a | 1.00 [0.95; 1.04] | 0.9 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guivarch, C.; Charles, M.-A.; Forhan, A.; Ong, K.K.; Heude, B.; de Lauzon-Guillain, B. Associations between Children’s Genetic Susceptibility to Obesity, Infant’s Appetite and Parental Feeding Practices in Toddlerhood. Nutrients 2021, 13, 1468. https://doi.org/10.3390/nu13051468
Guivarch C, Charles M-A, Forhan A, Ong KK, Heude B, de Lauzon-Guillain B. Associations between Children’s Genetic Susceptibility to Obesity, Infant’s Appetite and Parental Feeding Practices in Toddlerhood. Nutrients. 2021; 13(5):1468. https://doi.org/10.3390/nu13051468
Chicago/Turabian StyleGuivarch, Claire, Marie-Aline Charles, Anne Forhan, Ken K. Ong, Barbara Heude, and Blandine de Lauzon-Guillain. 2021. "Associations between Children’s Genetic Susceptibility to Obesity, Infant’s Appetite and Parental Feeding Practices in Toddlerhood" Nutrients 13, no. 5: 1468. https://doi.org/10.3390/nu13051468
APA StyleGuivarch, C., Charles, M. -A., Forhan, A., Ong, K. K., Heude, B., & de Lauzon-Guillain, B. (2021). Associations between Children’s Genetic Susceptibility to Obesity, Infant’s Appetite and Parental Feeding Practices in Toddlerhood. Nutrients, 13(5), 1468. https://doi.org/10.3390/nu13051468